shaping uhc policy for post 2015: opportunities & risks jeanette vega md, drph managing director...
TRANSCRIPT
Shaping UHC Policy for Post 2015:Opportunities & Risks
Jeanette Vega MD, DrPHManaging Director of Health
NHIS 10 Anniversary Conference Accra, November 4th, 2013

2
Universal Health Coverage (UHC) contribution to the Sustainable Development Goals
UHC: Definition and components
Health financing situation in Africa
Presentation Overview
Achievement of MDGs in the region
Concluding remarks
3
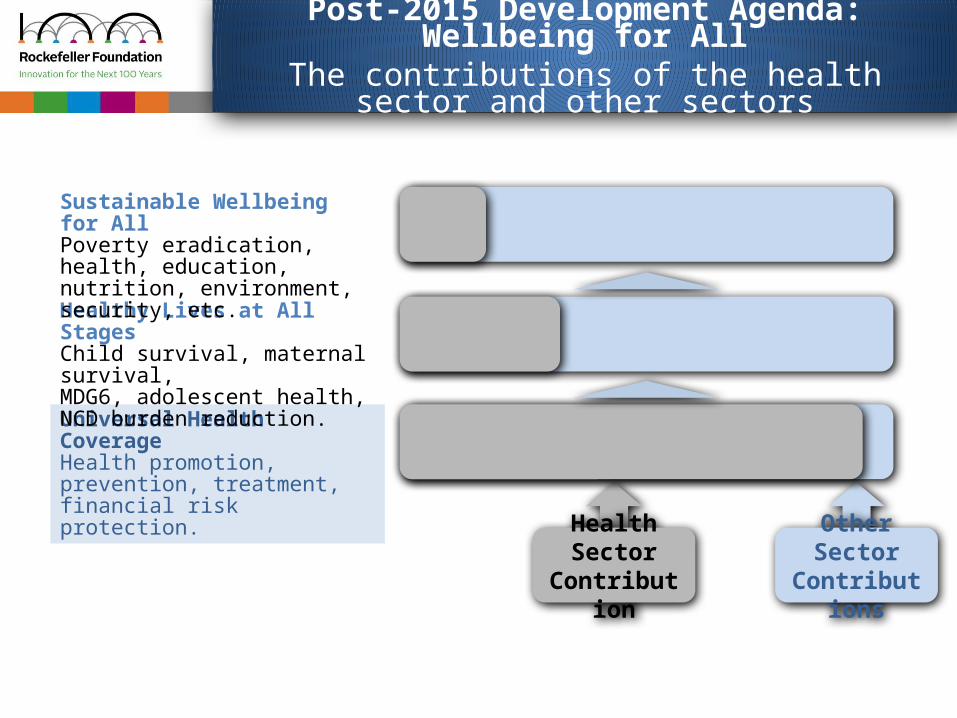
Universal Health CoverageHealth promotion, prevention, treatment, financial risk protection.
Healthy Lives at All StagesChild survival, maternal survival,MDG6, adolescent health, NCD burden reduction.
Sustainable Wellbeing for AllPoverty eradication, health, education, nutrition, environment, security, etc.
Health SectorContribution
Other Sector Contributions
Post-2015 Development Agenda: Wellbeing for AllThe contributions of the health sector and other sectors

4
Universal Health Coverage: What?
Indicators: 1. Financial protection2. Access
All people can access the health services they need without incurring financial hardship.
Definition:

5
Financing for UHC: Overall questions to be addressed by any country
How to alter the system in a way that– Reduces the gap between the need for and use of
services, across the population, – Improves quality of health services, – Improves financial protection…
… given our starting point in terms of– existing configuration of the health system, including coverage
arrangements,
– overall current and expected fiscal constraints, and
– other key contextual factors, such as labor market (informality), public administration structure (e.g. decentralization), geography and population density, politics, etc.?
1
2
6
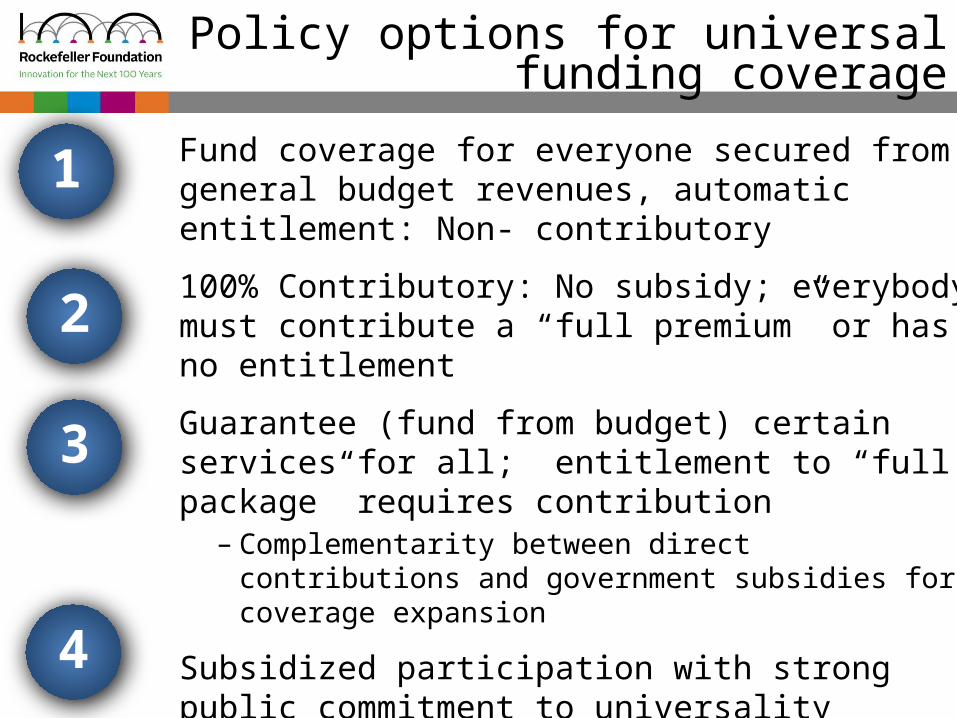
Policy options for universal funding coverage
Fund coverage for everyone secured from general budget revenues, automatic entitlement: Non- contributory
100% Contributory: No subsidy; everybody must contribute a “full premium” or has no entitlement
Guarantee (fund from budget) certain services for all; entitlement to “full package” requires contribution– Complementarity between direct contributions and
government subsidies for coverage expansion
Subsidized participation with strong public commitment to universality
1
2
3
4

7
Two conditions for financing UHC when using contributory arrangements
Subsidization: because some will be too poor or too sick to be able to afford coverage
Compulsory contribution: because some who can afford it are unwilling to pay for it
1
2
One without the other won’t work (subsidies alone not sufficient because rich/healthy will not join; and
compulsory without subsidies imposes a heavy burden on the poor and sick)

8
Some broad lessons on health financing policy
No country gets to UHC via voluntary health insurance
– Compulsory or automatic entitlement is essential, with subsidies
All countries with universal health coverage rely in whole or in part on general budget revenues
– Because there are always some who can’t contribute directly,
– And the larger the informal sector, the greater the need for using general revenues
Need to manage resources efficiently: Strategic purchasing is essential
– Move away from the extremes of provider payment methods – unmanaged fee-for-service and rigid line item budgets – as these contribute to system inefficiencies
1
2
3

9
Common elements of few countries that have high coverage with “voluntary”contributory schemes
Cost of the “premium” much less than the perceived value of the benefit, stimulating demand
– Substantial subsidies on the supply side and the demand side, and same benefit package as rest of population in the scheme
– Population aware that not being covered means risk of high out-of-pocket spending
Strong role of local governments– Strong incentives/instructions for local officials to inform people
and enroll them into the coverage program, (ie. Rwanda), and– Explicit role for local budgets to subsidize (ie China)
Very strong (authoritarian) governments able to implement these measures
10
ChadKenya
CongoGabon
Guinea
Nigeria
Guinea-Bissau
Burundi
Cameroon
Seych
elles
Benin
UgandaNiger
GambiaGhana
Mali
South Afric
a
Comoros
Lesotho
Togo
Malawi
Rwanda0
5
10
15
20
25
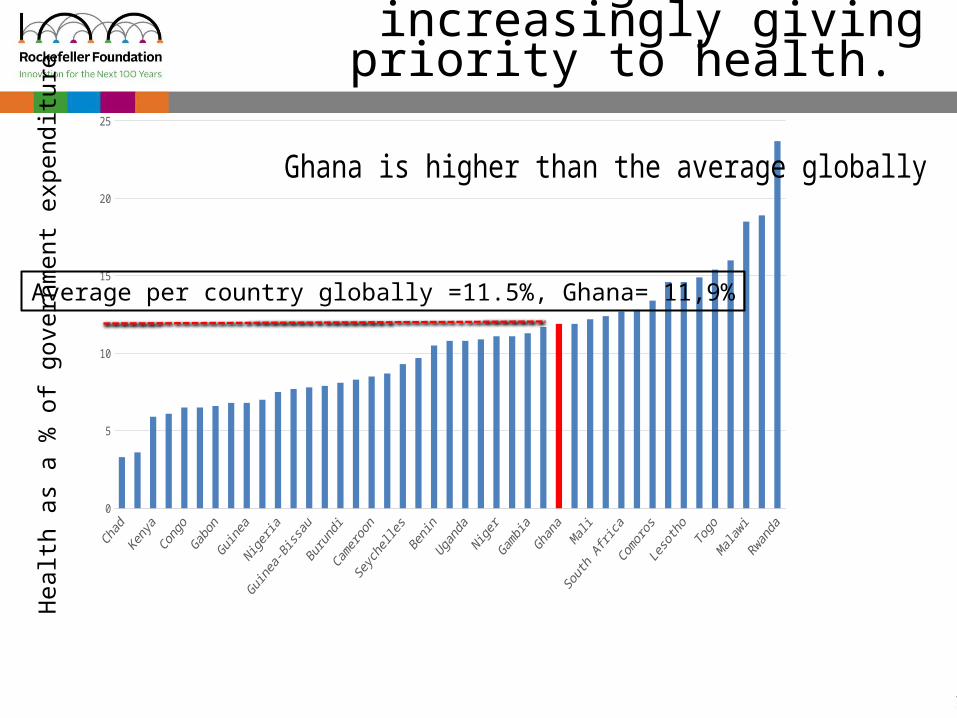
Ghana is higher than the average globally
Average per country globally =11.5%, Ghana= 11,9%
African governments increasingly giving priority to health.
Hea
lth a
s a
% o
f gov
ernm
ent e
xpen
ditu
re

11
African countries have low public spending on health relative to the size of the economy
Ghana is lower than the average globally =2.6%
Eritrea
Cameroon
Guinea
Guinea-Biss
auGabon
Kenya
C?te d'Ivoire
Nigeria
Angola
Mauritius
Gambia, The
Benin
Uganda
Equatorial G
uinea
Ghana
Ethiopia
Mozambique
Burundi
United Republic
of Tanza
niaNiger
Namibia
Botswana
Mali
Algeria
Mauritania
Burkina Faso
Sierra Le
one
Seychelle
s
Senegal
South Africa
Togo
Djibouti
Rwanda
Liberia
Malawi
Leso
tho0
1
2
3
4
5
6
7
8
9
10
Source: WHO estimates for 2011
Tota
l gov
ernm
ent e
xpen
ditu
res
on h
ealth
as
a %
of G
DP
Average per country globally= 3.9%
12
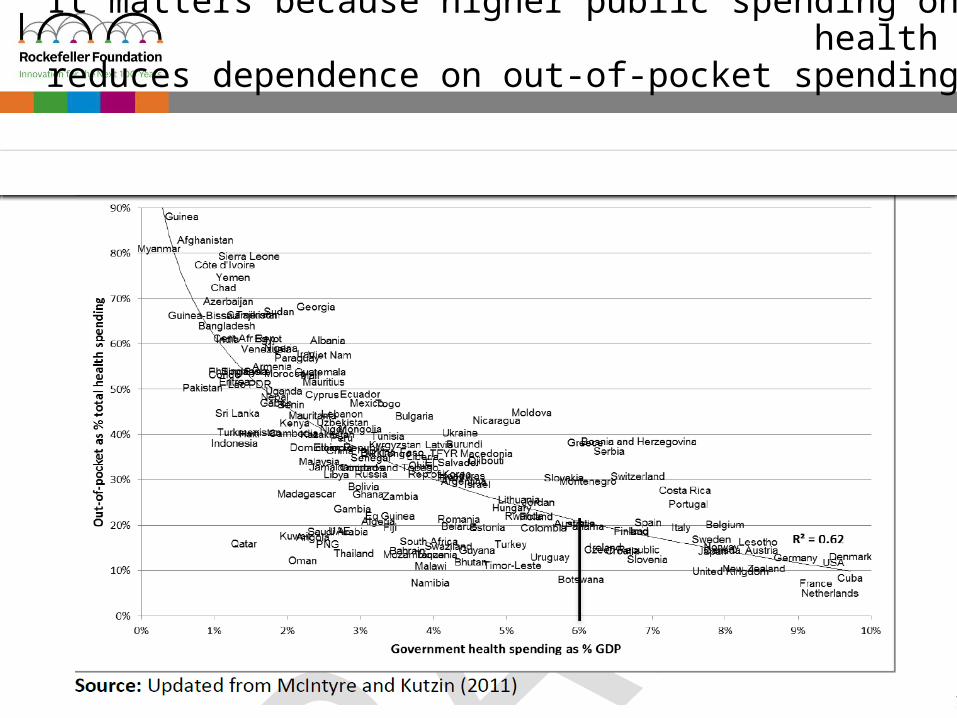
It matters because higher public spending on health reduces dependence on out-of-pocket spending
13
In summary: two critical issues to increase financial access coverage in Africa
All people can access the health services they need without incurring financial hardship.
How to increase overall fiscal space for health and increase health as a priority in the general budget
1
2
How to advance towards pre-paid Universal financial coverage

14
Achievement of MDGs in the region
15
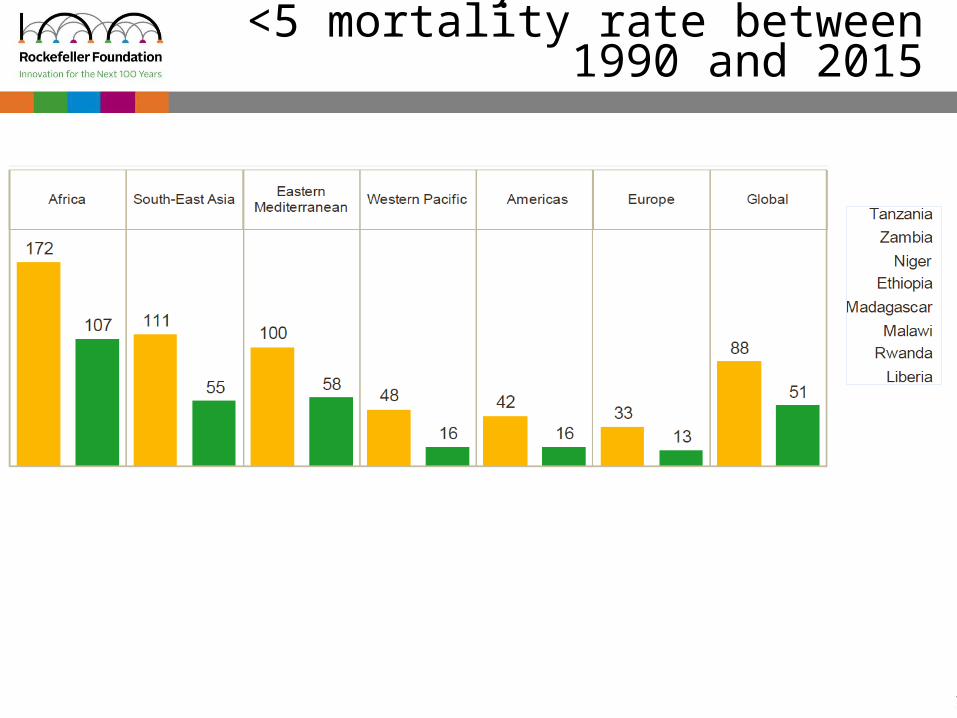
Reduce by two-thirds the <5 mortality rate between 1990 and 2015

16
Reduce by three quarter the maternal mortality rate between 1990- 2015
Target : 213 per 100,000 livebirthsOnly 2 countries
on track:EritreaEquatorial Guinea

17
Maternal health: Increase % of skilled birth attendance to 80%

18
One reason for no achievement has been the absence of UHC as a goal in the current objectives
Universal Health Coverage is an integrated, efficient approach to improve health outcomes. It is aspirational, but
there is growing global and national commitment to UHC.
UHC reflects health sector’s inherent responsibility to provide universal and equitable access to health that ensures improved health outcomes.
UHC links to other sectors, and enables healthy, sustainable development.
UHC is a recommitment to health as a human right.
1
2
3
19
Why UHC in the Post 2015 Development Agenda?
When designed with an equity, rights and fiscally prudent focus, UHC
is an accelerator towards better health outcomes and overall
social wellbeing.

20
MDGs + more ambitious health outcome targets. – E.g., ending preventable maternal and child deaths, universal
access to reproductive health, new HIV, TB, malaria targets, NCDs and their risks.
Universal health coverage emerging as the specific health sector contribution to health
Equity – realizing the right to health for all.
Recognition that achieving health outcome targets a require actions beyond the health sector – determinants of health.– E.g. income distribution, education and labor policies, food
security and nutrition, water and sanitation, urbanization.
Emerging Consensus on Health in the Post-2015 Development Agenda?
21
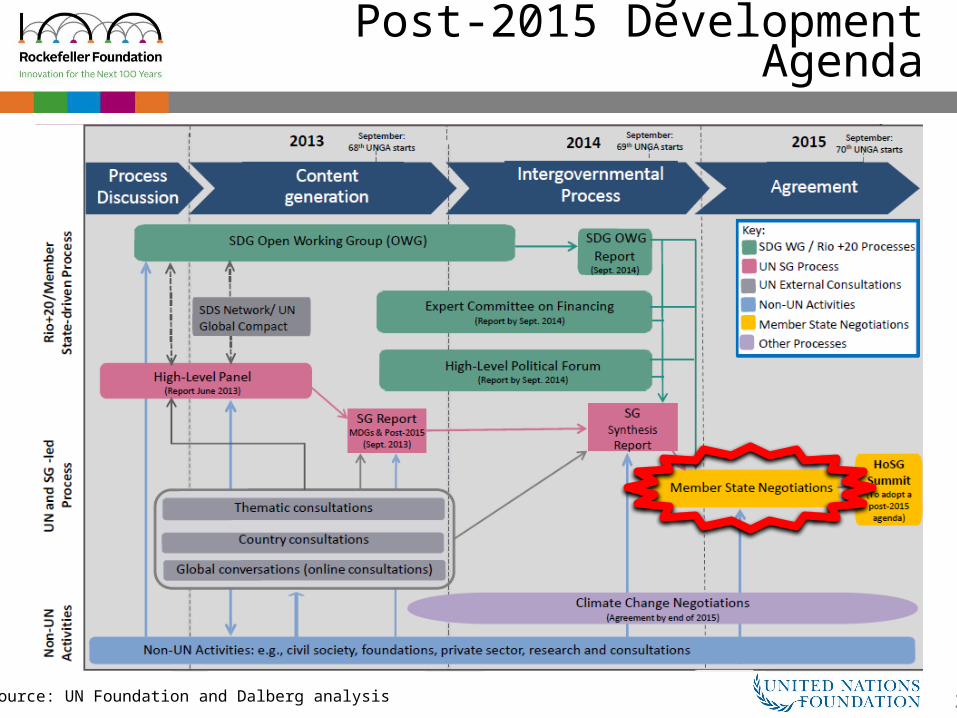
Processes Feeding Into the Post-2015 Development Agenda
Source: UN Foundation and Dalberg analysis