severity of cardiovascular disease outcomes among patients ... filed. neaton and the insight smart,...
TRANSCRIPT

D. Neaton and the INSIGHT SMART, ESPRIT Study Groups, and SILCAAT Scientific CommitteeAnna D. Nordell, Matthew McKenna, Álvaro H. Borges, Daniel Duprez, Jacqueline Neuhaus, James
of Inflammation and CoagulationSeverity of Cardiovascular Disease Outcomes Among Patients With HIV Is Related to Markers
Online ISSN: 2047-9980 Dallas, TX 75231
is published by the American Heart Association, 7272 Greenville Avenue,Journal of the American Heart AssociationThe doi: 10.1161/JAHA.114.000844
2014;3:e000844; originally published May 28, 2014;J Am Heart Assoc.
http://jaha.ahajournals.org/content/3/3/e000844World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://jaha.ahajournals.org/ahaoa/suppl/2014/06/27/jah3554.DC1.htmlData Supplement (unedited) at:
for more information. http://jaha.ahajournals.orgAccess publication. Visit the Journal at
is an online only OpenJournal of the American Heart AssociationSubscriptions, Permissions, and Reprints: The
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from
Severity of Cardiovascular Disease Outcomes Among Patients WithHIV Is Related to Markers of Inflammation and CoagulationAnna D. Nordell, BA; Matthew McKenna, BA; �Alvaro H. Borges, MD, MSc; Daniel Duprez, MD, PhD; Jacqueline Neuhaus, MS;James D. Neaton, PhD; for the INSIGHT SMART, ESPRIT Study Groups, and SILCAAT Scientific Committee*
Background-—In the general population, raised levels of inflammatory markers are stronger predictors of fatal than nonfatalcardiovascular disease (CVD) events. People with HIV have elevated levels of interleukin-6 (IL-6), high-sensitivity C-reactive protein(hsCRP), and D-dimer; HIV-induced activation of inflammatory and coagulation pathways may be responsible for their greater risk ofCVD. Whether the enhanced inflammation and coagulation associated with HIV is associated with more fatal CVD events has notbeen investigated.
Methods and Results-—Biomarkers were measured at baseline for 9764 patients with HIV and no history of CVD. Of thesepatients, we focus on the 288 that experienced either a fatal (n=74) or nonfatal (n=214) CVD event over a median of 5 years. Oddsratios (ORs) (fatal versus nonfatal CVD) (95% confidence intervals [CIs]) associated with a doubling of IL-6, D-dimer, hsCRP, and a1-unit increase in an IL-6 and D-dimer score, measured a median of 2.6 years before the event, were 1.39 (1.07 to 1.79), 1.40(1.10 to 1.78), 1.09 (0.93 to 1.28), and 1.51 (1.15 to 1.97), respectively. Of the 214 patients with nonfatal CVD, 23 died duringfollow-up. Hazard ratios (95% CI) for all-cause mortality were 1.72 (1.28 to 2.31), 1.73 (1.27 to 2.36), 1.44 (1.15 to 1.80), and 1.88(1.39 to 2.55), respectively, for IL-6, D-dimer, hsCRP, and the IL-6 and D-dimer score.
Conclusions-—Higher IL-6 and D-dimer levels reflecting enhanced inflammation and coagulation associated with HIV areassociated with a greater risk of fatal CVD and a greater risk of death after a nonfatal CVD event.
Clinical Trial Registration-—URL: http://www.clinicaltrial.gov Unique identifier: SMART: NCT00027352, ESPRIT: NCT00004978,SILCAAT: NCT00013611. ( J Am Heart Assoc. 2014;3:e000844 doi: 10.1161/JAHA.114.000844)
Key Words: cardiovascular disease • inflammation
O ver 15 years ago, an association between enhancedinflammation, as demonstrated by higher plasma levels
of C-reactive protein (CRP), and risk of coronary heart disease(CHD) in middle-aged men without previous cardiovascular
disease (CVD) was reported using data from the Multiple RiskFactor Intervention Trial (MRFIT).1 In MRFIT, CRP was stronglyrelated to CHD mortality, but was not related to nonfatalmyocardial infarction (MI). Importantly, most of the CHDdeaths occurred more than 10 years after the CRP measure-ment. This MRFIT observation that markers of inflammationare stronger predictors of fatal, as compared to nonfatal, CHDevents has been confirmed in other studies.2–4 Reasons forthis finding include the possibility that patients with higherinflammatory markers may have different underlying vasculardisease. It has been speculated that patients with greaterlevels of inflammation might be more likely to experience fatalarrhythmias that result in sudden death or have greater levelsof inflammation in unstable plaques.1–3 It is also possible thatlow-grade inflammation results in activation of the coagulationsystem, increasing the likelihood of fatal outcomes subse-quent to plaque rupture.4 Other reasons include a greaterpresence of other CVD risk factors among those with higherinflammatory biomarker levels that increased risk of death, orthe presence of other nonvascular conditions that areassociated with chronic inflammation and that lead to anincreased risk of fatal events.
From the Division of Biostatistics, School of Public Health, University ofMinnesota, Minneapolis, MN (A.D.N., M.M., J.N., J.D.N.); Department ofInfectious Diseases, Rigshospitalet and Copenhagen HIV Programme, Universityof Copenhagen, Copenhagen, Denmark (A.H.B.); Cardiovascular Division,University of Minnesota, Minneapolis, MN (D.D.).
Accompanying Table S1 is available at http://jaha.ahajournals.org/content/3/3/e000844/suppl/DC1
*A list of all INSIGHT SMART, ESPRIT Study Groups and the SILCAAT ScientificCommittee participants is provided in Data S1, available at http://jaha.ahajournals.org/content/3/3/e000844/suppl/DC1.
Correspondence to: James D. Neaton, PhD, Division of Biostatistics, 2221University Ave SE, Room 200, Minneapolis, MN 55414. E-mail: [email protected]
Received January 28, 2014; accepted April 23, 2014.
ª 2014 The Authors. Published on behalf of the American Heart Association,Inc., by Wiley Blackwell. This is an open access article under the terms of theCreative Commons Attribution-NonCommercial License, which permits use,distribution and reproduction in any medium, provided the original work isproperly cited and is not used for commercial purposes.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 1
ORIGINAL RESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

Patients with HIV may contribute to our understanding ofthese findings in the general population. They are in asustained inflammatory state even when taking suppressiveantiretroviral therapy (ART).5 Reasons for this inflammatorystate and the associated chronic state of immune activationhave been reviewed.6,7 Some key findings concerning HIV,inflammation, and CVD, which we and others have described,are: (1) compared to age- and gender-matched people in thegeneral population interleukin-6 (IL-6), high-sensitivity CRP(hsCRP), and D-dimer are elevated5; (2) patients with HIVappear to be at an increased risk of CVD, compared toindividuals without HIV8–12; and (3) IL-6, hsCRP, and D-dimermeasured several years beforehand are associated with all-cause mortality and fatal or nonfatal CVD.1,13 The results inthe reports by Kuller and Duprez, which utilized stored plasmaspecimens from the Strategies for Management of Antiretro-viral Therapy (SMART) trial,14,15 also suggested that thoughthe associations of these biomarkers with fatal or non-fatalCVD was similar to associations reported in general popula-tion studies, the association with all-cause mortality wasstronger than for CVD, even though the deaths in SMARTwere attributed to a number of different causes.
Collectively, these findings led us to formulate 2 hypoth-eses: (1) HIV-positive patients with higher levels of IL-6,hsCRP, and D-dimer, measured several years before the CVDevent, are more likely to experience a fatal, as compared to anonfatal, CVD event; and (2) mortality after nonfatal CVDevents is higher among HIV-positive patients with higher, ascompared to lower, levels of IL-6, hsCRP, and D-dimer, alsomeasured several years before the nonfatal event. Toinvestigate these hypotheses, we used data from SMARTand 2 other large international clinical trials of HIVtreatments.
Methods
Study PopulationsThis investigation included patients from 3 large internationalHIV treatment trials conducted by the International Networkfor Strategic Initiatives in Global HIV Trials, the SMARTtrial,14,15 the Evaluation of Subcutaneous Proleukin� in aRandomized International Trial (ESPRIT),16,17 and the Subcu-taneous Recombinant, Human Interleukin-2 in HIV-InfectedPatients with Low CD4+ Counts under Active AntiretroviralTherapy (SILCAAT) trial.17 These trials were carried out in 33,25, and 11 countries, respectively. The SMART studycompared continuous ART with intermittent ART among HIV-positive patients with a CD4+ cell count of more than 350cells/mm3. ESPRIT and SILCAAT compared IL-2 plus ARTversus ART alone among HIV-positive patients with CD4+
counts of 300 cells/mm3 or more and with CD4+ counts of 50
to 299 cells/mm3, respectively. All studies were approved byan institutional review committee and patients were includedonly after giving informed consent.
Biomarker MeasurementsIL-6, hsCRP, and D-dimer were measured at baseline, beforerandomization, in each trial using stored plasma for patientswho provided written consent. For patients in SMART, thesebiomarkers were measured at the Laboratory for ClinicalBiochemistry Research at the University of Vermont (Burling-ton). In the ESPRIT and SILCAAT trials, laboratory measure-ments were performed by SAIC-Frederick (Frederick, MD). Allsamples in both laboratories were analyzed blinded totreatment group and CVD event status. IL-6 was measuredby the same method at each laboratory (ChemiluminescentSandwich ELISA; R&D Sytems, Minneapolis, MN). D-dimerlevels were measured by ELISA on the Sta-R analyzer, LiatestD-DI (Diagnostic Stago, Parsippany, NJ), for patients in SMARTand on a VIDAS instrument (bioM�erieux Inc, Durham, NC) forpatients in ESPRIT and SILCAAT. hsCRP was measured byELISA by both laboratories. For SMART, a NBTMII nephelom-eter, N Antiserum to Human CRP (Siemens Diagnostics,Deerfield, IL), was used. For ESPRIT and SILCAAT, an R&DSystems ELISA assay was used. Twenty samples wereindependently analyzed at each laboratory for these biomar-ker levels. Table S1 summarizes the measurements made ateach laboratory. Lower limits of detection (LLOD) for IL-6,hsCRP, and D-dimer were 0.16 pg/mL, 0.16 lg/mL, and0.01 lg/mL for SMART. In ESPRIT and SILCAAT, LLOD were0.156 pg/mL, 0.078 lg/mL, and 0.045 lg/mL.
Baseline and Follow-up MeasurementsIn all 3 studies, the following baseline measurements wereobtained before randomization: age, sex, race, body massindex (BMI), CD4+ cell count, HIV-RNA, duration of ART, andprevious AIDS clinical event. In SMART and ESPRIT, additionalbaseline measurements were made, including hepatitis B/Ccoinfection, diabetes, and use of blood pressure and lipid-lowering medication. For patients in SMART, smoking statuswas assessed and blood lipids were measured. During follow-up, HIV RNA levels and CD4+ cell counts were recorded every4 months in each study.
EventsCVD events considered were deaths attributed to CVD,unwitnessed deaths that were not attributed to suicide, drugabuse, or violence, nonfatal MI, nonfatal stroke, and coronaryartery disease (CAD) requiring surgery. In SMART and ESPRIT,documentation of CVD events that was provided by the
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 2
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

clinical sites were reviewed by an endpoint review committeeusing prespecified criteria.18 Criteria for acute MI followed theuniversal definition of MI.19 CAD requiring surgery requireda procedure report, hospital discharge summary, or othermedical record from the hospitalization during which theprocedure was performed (coronary artery bypass graft,coronary artery stent implant, coronary artherectomy, orpercutaneous transluminal angioplasty). For strokes, 5 criteriawere considered: (1) acute onset with clinically compatiblecourse, including unequivocal objective findings of a localizingneurological deficit; (2) computed tomography (CT) or mag-netic resonance imaging (MRI) compatible with diagnosis ofstroke and current neurologic signs and symptoms; (3) strokediagnosed as cause of death at autopsy; (4) positive lumbarpuncture compatible with subarachnoid hemorrhage; and(5) death certificate or death note from medical record listingstroke as the cause of death. A participant was considered tohave experienced a stroke if the first and second criteria weremet, the third criterion was met, the first and fourth criteriawere met, or the first and fifth criteria were met. In SILCAAT,CVD events reported as serious adverse events were codedaccording to the Medical Dictionary for Regulatory Activities(MedRA; version 12.0). The following Standardized MedRAQuery codes were used for nonfatal stroke (20000082),nonfatal MI (20000047), and CAD requiring surgery(10068176, 10052086, 10057787, or 10063025). In all 3studies, cause of death was coded using documentation ofthe death provided by the clinical sites using the Coding ofDeath in HIV system.20
In addressing our first hypothesis, we defined fatal CVDevents as: (1) deaths attributable to CVD or unwitnesseddeaths for patients that did not experience a nonfatal MI orstroke before their death and (2) deaths within 28 days aftera nonfatal MI, stroke, or CAD. Patients who experienced MI,stroke, or CAD events and survived at least 28 days weredefined as having nonfatal CVD events.
For our second hypothesis, we considered any patient withan MI, stroke, or CAD event who survived at least 28 days.For this group of patients, we assessed subsequent risk of all-cause mortality.
Statistical AnalysesLogistic regression, including indicators for study the patientwas enrolled in (SMART, ESPRIT, SILCAAT), was used to studythe association of each biomarker with fatal CVD. In additionto considering each biomarker individually, we also consid-ered a combined IL-6 and D-dimer score used for predictingall-cause mortality among HIV patients with a suppressed viralload. Because of their independent association with all-causemortality, the IL-6 and D-dimer score was created in order toaccount for the contribution of both markers in a single
combined measure. This score was determined using thecontrol arms of SMART, ESPRIT, and SILCAAT (144 deaths)and was adjusted for age, gender, and study; IL-6 and D-dimerwere log2 transformed. The regression coefficients from thisCox model for IL-6 and D-dimer were then used to create theIL-6 and D-dimer score.21
In this investigation, the biomarkers were log2 transformedbecause their distributions were right-skewed. With thisapproach, a 1 log2 higher level of a biomarker correspondsto a doubling of the marker. Results are also cited for tertilesof each biomarker, which were defined using all of thepatients in the 3 studies that experienced a fatal or nonfatalCVD event. Other covariates, measured in each study, thatwere considered potential confounding factors were: timebetween biomarker measurement and the event, age, gender,race, baseline BMI, HIV RNA level, baseline CD4+ cell count,and earlier AIDS event at study entry. We also considered theinteraction between time between biomarker measurementand the event with the log-transformed biomarker. Insensitivity analyses, we adjusted for hepatitis B/C coinfec-tion, diabetes, and use of blood pressure and lipid-loweringmedication (SMART and ESPRIT) and then added smoking andthe ratio of total cholesterol to high-density lipoprotein (HDL)cholesterol (SMART only). We also carried out separateanalyses for patients in the control arms of the 3 studies.These patients were to receive continuous ART with a goal ofsuppressing HIV-RNA levels during follow-up. This is therecommended standard of care for patients with HIV.22
Cumulative mortality after a nonfatal CVD event wasestimated using the Kaplan-Meier method. Cox models thatincluded study indicators were used to study factors relatedto mortality for the 214 patients who experienced a nonfatalCVD event. Models included the same covariates as thelogistic model, as well as CD4+ cell counts and HIV-RNA levelsboth proximal to the nonfatal event. Hazard ratios (HRs) and95% confidence intervals (CIs) are cited. The proportionalhazards assumption was tested by including an interactionterm between each biomarker and log-transformed follow-uptime.
All analyses were performed using SAS statistical software(version 9.2; SAS Institute Inc., Cary, NC). P<0.05 wasconsidered significant.
ResultsAmong the 11 278 patients randomized in these trials (5472SMART, 4111 ESPRIT, and 1695 SILCAAT), 10 001 (89%) hadIL-6, hsCRP, and D-dimer measured on stored baseline plasmasamples for consenting patients (5017 SMART, 3570 ESPRIT,and 1414 SILCAAT). Of these, 9764 (98%) did not report ahistory of CVD at study entry (Figure). Over a median(interquartile range; IQR) follow-up of 5.0 (2.3, 7.1) years, 74
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 3
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from
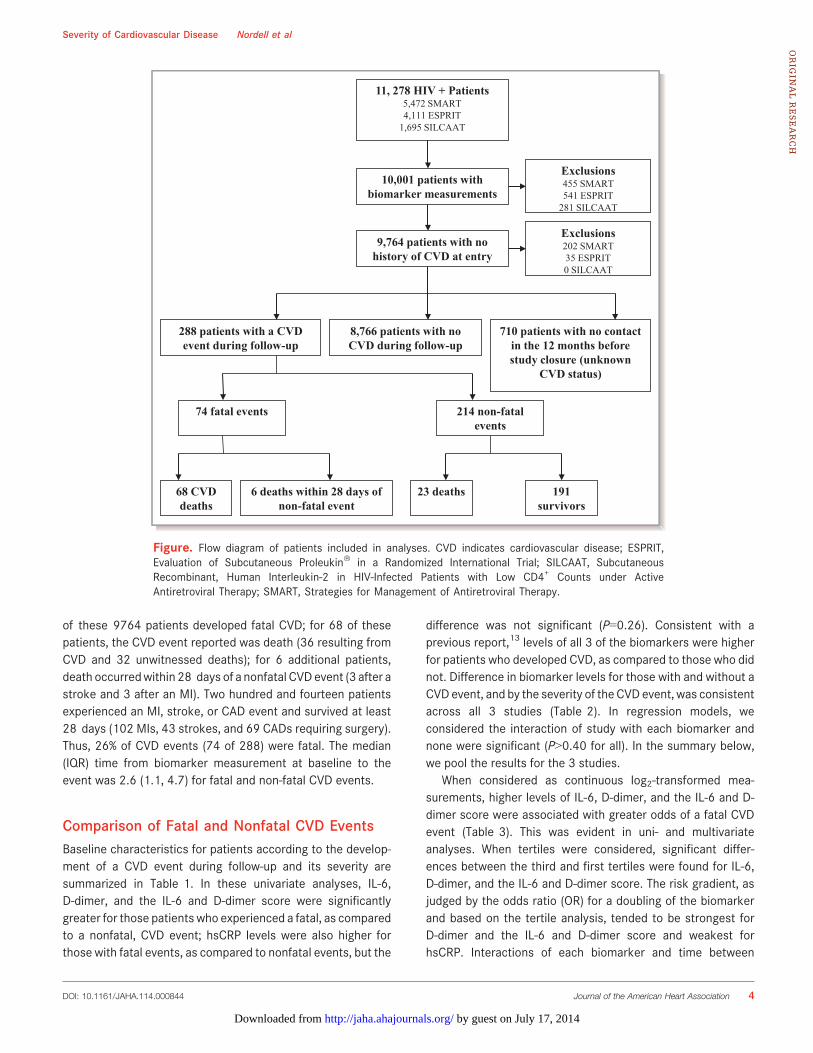
of these 9764 patients developed fatal CVD; for 68 of thesepatients, the CVD event reported was death (36 resulting fromCVD and 32 unwitnessed deaths); for 6 additional patients,death occurredwithin 28 days of a nonfatal CVD event (3 after astroke and 3 after an MI). Two hundred and fourteen patientsexperienced an MI, stroke, or CAD event and survived at least28 days (102 MIs, 43 strokes, and 69 CADs requiring surgery).Thus, 26% of CVD events (74 of 288) were fatal. The median(IQR) time from biomarker measurement at baseline to theevent was 2.6 (1.1, 4.7) for fatal and non-fatal CVD events.
Comparison of Fatal and Nonfatal CVD EventsBaseline characteristics for patients according to the develop-ment of a CVD event during follow-up and its severity aresummarized in Table 1. In these univariate analyses, IL-6,D-dimer, and the IL-6 and D-dimer score were significantlygreater for those patients who experienced a fatal, as comparedto a nonfatal, CVD event; hsCRP levels were also higher forthose with fatal events, as compared to nonfatal events, but the
difference was not significant (P=0.26). Consistent with aprevious report,13 levels of all 3 of the biomarkers were higherfor patients who developed CVD, as compared to those who didnot. Difference in biomarker levels for those with and without aCVD event, and by the severity of the CVD event, was consistentacross all 3 studies (Table 2). In regression models, weconsidered the interaction of study with each biomarker andnone were significant (P>0.40 for all). In the summary below,we pool the results for the 3 studies.
When considered as continuous log2-transformed mea-surements, higher levels of IL-6, D-dimer, and the IL-6 and D-dimer score were associated with greater odds of a fatal CVDevent (Table 3). This was evident in uni- and multivariateanalyses. When tertiles were considered, significant differ-ences between the third and first tertiles were found for IL-6,D-dimer, and the IL-6 and D-dimer score. The risk gradient, asjudged by the odds ratio (OR) for a doubling of the biomarkerand based on the tertile analysis, tended to be strongest forD-dimer and the IL-6 and D-dimer score and weakest forhsCRP. Interactions of each biomarker and time between
10,001 patients with biomarker measurements
9,764 patients with no history of CVD at entry
288 patients with a CVD event during follow-up
8,766 patients with no CVD during follow-up
710 patients with no contact in the 12 months before study closure (unknown
CVD status)
Exclusions455 SMART541 ESPRIT
281 SILCAAT
Exclusions202 SMART35 ESPRIT0 SILCAAT
214 non-fatal events
74 fatal events
68 CVD deaths
6 deaths within 28 days of non-fatal event
23 deaths 191survivors
11, 278 HIV + Patients5,472 SMART4,111 ESPRIT
1,695 SILCAAT
Figure. Flow diagram of patients included in analyses. CVD indicates cardiovascular disease; ESPRIT,Evaluation of Subcutaneous Proleukin� in a Randomized International Trial; SILCAAT, SubcutaneousRecombinant, Human Interleukin-2 in HIV-Infected Patients with Low CD4+ Counts under ActiveAntiretroviral Therapy; SMART, Strategies for Management of Antiretroviral Therapy.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 4
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

biomarker measurement and the event were also consideredand none were significant. Sensitivity analyses were per-formed, excluding the unwitnessed deaths, and results weresimilar to those in Table 3. For example, univariate ORs (95%CI) associated with a doubling of IL-6, D-dimer, hsCRP, andthe IL-6 and D-dimer score were 1.41 (1.03 to 1.92), 1.36(1.01 to 1.82), 1.13 (0.92 to 1.37), and 1.50 (1.08 to 2.07),respectively.
Considering the 206 patients (54 fatal and 152 nonfatalevents) in SMART and ESPRIT that had measurementsrecorded at baseline, we adjusted for 4 additional covariates:diabetes, hepatitis B/C coinfection, and use of blood pressureand lipid-lowering medication. Adjusted ORs were similar to
those shown in Table 3: for IL-6, D-dimer, hsCRP, and IL andD-dimer score, ORs (95% CIs) were 1.33 (95% CI, 0.95 to1.86), 1.43 (95% CI, 1.02 to 2.00), 1.18 (95% CI, 0.95 to1.47), and 1.49 (95% CI, 1.03 to 2.15), respectively.
For the 115 patients (31 fatal and 84 nonfatal events) inSMART for whom we could also adjust for smoking and total/HDL cholesterol, adjusted ORs were 1.10 (95% CI, 0.72 to1.67), 1.39 (95% CI, 0.90 to 2.15), 1.25 (95% CI, 0.91 to1.70), and 1.22 (95% CI, 0.78 to 1.93) for IL-6, D-dimer,hsCRP, and the IL-6 and D-dimer score, respectively.
In SMART, the OR associated with a doubling of IL-6 waslower than in analyses based on all 3 studies or based onSMART and ESPRIT. For all 5017 patients in SMART, median
Table 1. Baseline Characteristics for HIV-Positive Patients Who Experienced CVD Events According to Severity
No Event* Fatal CVD† Nonfatal CVD‡ P Value§
Baseline characteristics, n 9476 74 214
Age (y), median (IQR) 42 (36 to 48) 48 (41 to 54) 49 (42 to 54) 0.76
Sex (% female) 22 14 8 0.21
Race (% black) 19 23 16 0.20
BMI (kg/m2), median (IQR) 24.3 (22.1 to 27.0) 24.0 (22.1 to 27.0) 24.3 (22.1 to 27.1) 0.58
CD4+ cell count, (cells/mm3) median (IQR) 487 (367 to 669) 409 (331 to 644) 469 (356 to 633) 0.63
HIV-RNA<500 copies/mL, % 77 74 77 0.64
Earlier AIDS event, % 26 39 29 0.10
IL-6, (pg/mL) median (IQR) 1.8 (1.2 to 2.8) 3.1 (1.9 to 4.5) 2.3 (1.5 to 3.5) 0.01||
% highest tertile (<1.88)# 20 45 28
% middle tertile (1.88≤9<3.14)# 27 31 36
% lowest tertile (≥3.14)# 52 24 36 0.02¶
D-dimer, (lg/mL) median (IQR) 0.24 (0.15 to 0.37) 0.35 (0.24 to 0.61) 0.27 (0.17 to 0.45) 0.006||
% highest tertile (<0.22) 21 45 29
% middle tertile (0.22≤9< 0.41) 31 32 34
% lowest tertile (≥0.41) 47 23 37 0.03¶
hsCRP, (lg/mL) median (IQR) 1.6 (0.7 to 3.6) 3.1 (1.1. to 7.5) 2.2 (1.1 to 5.6) 0.26||
% highest tertile (<1.55) 21 39 31
% middle tertile (1.55≤9<4.17) 29 32 34
% lowest tertile (≥4.17) 50 28 35 0.49¶
IL-6 and D-dimer score median (IQR) �0.02 (�0.60 to 0.61) 0.85 (0.20 to 1.36) 0.30 (�0.20 to 0.89) 0.003
% highest tertile (<1.04) 19 51 27
% middle tertile (1.04≤9<1.75) 28 26 36
% lowest tertile (≥1.75) 53 23 37 0.001¶
BMI indicates body mass index; CVD, cardiovascular disease; hsCRP, high-sensitivity C-reactive protein; IQR, interquartile range.*No event measurements noted for completeness.†Deaths attributed to CVD and unwitnessed deaths not resulting from violence, suicide, or drug abuse that were not proceeded by a nonfatal event or deaths within 28 days of the nonfatalCVD event.‡Nonfatal myocardial infarction, coronary artery disease requiring surgery, or nonfatal stroke for participants that survived at least 28 days.§From a univariate logistic model comparing fatal and nonfatal CVD events (n=288).||P values reported based on log2-transformed biomarker measurement.¶P value based on 2 df chi-square test.#Tertiles were defined using all of the patients in the 3 studies that experienced a fatal or nonfatal CVD event.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 5
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

Table2.
Characteristicsof
SMAR
T,ES
PRIT,andSILC
AATPatie
ntsWith
andWith
outFatal/NonfatalC
VDEvents
SMAR
TES
PRIT
SILC
AAT
NoEvent
FatalC
VDNonfatalC
VDNoEvent
FatalC
VDNon-Fatal
CVD
NoEvent
FatalC
VDNon-Fatal
CVD
Baselinecharacteristics,
n4697
3286
3418
2691
1361
1637
Age(y),median(IQR)
43(37to
50)
50(47to
54)
50(43to
55)
40(35to
46)
44(38to
51)
48(41to
54)
40(36to
47)
49(43to
58)
47(41to
54)
Sex(%
female)
2722
1518
44
1613
3
Race
(%black)
2941
349
84
913
5
BMI,(kg/m2 )median
(IQR)
25.0
(22.5to
28.1)
24.0
(21.8to
30.1)
25.7
(22.3to
28.4)
23.7
(21.9to
25.9)
24.4
(23.1to
25.8)
23.9
(22.0to
26.0)
23.8
(21.7to
26.1)
23.0
(21.3to
26.9)
23.5
(22.1to
26.1)
BP-loweringdrug
use,
%17
4737
50
10N/A
NANA
Lipid-loweringdrug
use,
%14
1333
1013
20N/A
NANA
HepatitisBor
Ccoinfected,%
1731
1422
2915
N/A
NANA
CD4+
cellcount,(cells/
mm3 )median(IQR)
598(467
to794)
649(442
to874)
593(450
to838)
453(368
to581)
399(341
to516)
470(386
to582)
202(150
to255)
200(144
to269)
188(131
to249)
ART,
%84
8187
100
100
100
100
100
100
TimesincefirstAR
T,(y)
median(IQR)
6(4
to8)
7(5
to9)
6(4
to8)
4(2
to6)
5(2
to6)
6(4
to8)
4(2
to8)
3(1
to6)
5(3
to8)
BaselineHIV-RN
A<500
copies/mL,
%72
7272
8169
8182
8878
Earlier
AIDS
event,%
2441
3427
5823
326
32
Diabetes,%
613
212
86
N/A
NANA
Smoker,%
4153
52N/A
NANA
N/A
NANA
Total/HDL
cholesterol,
(mmol/L)median(IQR)
4.6(3.6
to5.9)
4.1(3.1
to5.5)
6.1(4.2
to8.1)
N/A
NANA
N/A
NANA
IL-6,(pg/mL)
median
(IQR)
1.7(1.1
to2.9)
4.1(2.0
to6.5)
2.6(1.8
to4.5)
1.9(1.3
to2.7)
2.7(2.1
to3.2)
2.2(1.5
to3.1)
1.80
(1.20to
2.70)
2.5(1.6
to3.6)
1.9(1.5
to2.9)
D-dimer,(lg/mL)
median(IQR)
0.20
(0.13to
0.37)
0.37
(0.21to
0.72)
0.27
(0.15to
0.49)
0.26
(0.19to
0.37)
0.33
(0.25to
0.48)
0.28
(0.19to
0.42)
0.25
(0.17to
0.36)
0.42
(0.30to
0.70)
0.27
(0.18to
0.42)
hsCR
P,(lg/mL)
median
(IQR)
1.7(0.7
to4.0)
5.9(1.3
to8.9)
2.6(1.4
to6.7)
1.5(0.7
to3.2)
2.4(1.0
to3.7)
1.7(1.0
to4.2)
1.4(0.6
to3.3)
3.5(2.3
to5.0)
2.3(1.0
to4.6)
IL-6
andD-dimer
score,
median(IQR)
�0.12(�
0.81
to0.64)
1.17
(0.16to
1.95)
0.51
( �0.08
to1.14)
0.09
(�0.39
to0.59)
0.56
(0.29to
0.92)
0.18
(�0.21
to0.78)
�0.03(�
0.53
to0.51)
0.61
(�0.22
to1.19)
00.15(�
0.25
to0.56)
ARTindicatesantiretroviraltherapy;B
P,bloodpressure;B
MI,body
massindex;CVD
,cardiovasculardisease;
ESPR
IT,E
valuationof
Subcutaneous
Proleukin�
inaRa
ndom
ized
InternationalTria
l;HDL,
high-density
lipoprotein;h
sCRP
,high-
sensitivity
C-reactiveprotein;
SILC
AAT,
Subcutaneous
Recombinant,Hum
anInterle
ukin-2
inHIV-In
fected
Patie
ntswith
LowCD4+
CountsunderAc
tiveAn
tiretroviralT
herapy;SM
ART,
Strategies
forManagem
entof
AntiretroviralT
herapy.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 6
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

(IQR) levels of IL-6 for smokers and nonsmokers were 1.98(1.19 to 3.23) and 1.65 (1.05 to 2.86), respectively (P<0.001for difference). To investigate whether the adjustment forsmoking led to the lower OR for SMART, we comparedunadjusted and smoking adjusted ORs for SMART partici-pants. In the unadjusted model, the OR associated with adoubling of IL-6 was 1.29 (95% CI, 0.93 to 1.80); in the modeladjusting for smoking, the OR was 1.30 (95% CI, 0.93 to1.81).
There were 134 patients in the control arms of the 3studies that experienced a CVD event (32 fatal and 102nonfatal). ORs were similar to those cited for all patients inTable 3, but CIs were wider as a result of the smaller numberof events. Adjusted ORs (fatal/nonfatal events) were 1.62(95% CI, 0.96 to 2.74), 1.40 (95% CI, 0.88 to 2.25), 1.11 (95%CI, 0.82 to 1.51), and 1.89 (95% CI, 1.05 to 3.41) for IL-6,D-dimer, hsCRP, and the IL-6 and D-dimer score, respectively.Interaction P values for treatment/control and each biomar-ker were all >0.59.
Biomarker Association With Mortality After aNonfatal CVD EventAmong the 214 patients who had a nonfatal CVD event, therewere 23 deaths (10.7%). Cumulative mortality 6 and
12 months after the nonfatal event for these patients, all ofwhom survived at least 28 days, was 2.9% and 4.0%,respectively.
In univariate analyses, higher levels of each of thebiomarkers were associated with an increased risk of death(Table 4). HRs were reduced with covariate adjustment, yetremained significant for all 4 biomarkers. There was noevidence that the proportional hazards assumption did nothold for each biomarker (interaction P values all >0.73).
DiscussionBased on our previous work and studies in the generalpopulation, we formulated 2 related hypotheses on theassociation of inflammatory and coagulation markers and theseverity of future CVD events in HIV-positive patients. Inanalyses that adjusted for HIV- and CVD-related factors, wefound that among HIV-positive patients who developed CVD:(1) those with higher levels of IL-6, D-dimer, and an IL-6 andD-dimer score, but not hsCRP, measured several years earlierwere significantly more likely to have a fatal CVD event and(2) the risk of death after an MI, stroke, or CAD event wassignificantly increased among HIV-positive patients withhigher baseline levels of IL-6, hsCRP, and an IL-6 and D-dimerscore, but not D-dimer. In this latter analysis, the biomarkers
Table 3. Unadjusted and Covariate Adjusted* Odds Ratios for Fatal CVD† (Versus Nonfatal CVD‡) According to Tertile andAssociated With a Doubling of Each Biomarker or 1-Unit Increase of IL-6 and D-Dimer Score
Biomarker
Lowest Tertile Middle Tertile Highest TertileOR Associated With Doubling ofBiomarker
OR OR 95% CI P Value OR 95% CI P Value Omnibus P Value§ OR 95% CI P Value
IL-6, pg/mL
Univariate 1.0 1.32 (0.66 to 2.64) 0.44 2.46 (1.25 to 4.87) 0.01 0.02 1.39 (1.07 to 1.79) 0.01
Adjusted 1.0 1.41 (0.69 to 2.88) 0.34 2.62 (1.26 to 5.46) 0.01 0.02 1.41 (1.07 to 1.86) 0.01
D-dimer (lg/mL)
Univariate 1.0 1.63 (0.80 to 3.33) 0.18 2.47 (1.25 to 4.85) 0.009 0.03 1.40 (1.10 to 1.78) 0.007
Adjusted 1.0 1.74 (0.80 to 3.75) 0.16 2.70 (1.27 to 5.75) 0.01 0.05 1.45 (1.10 to 1.92) 0.008
hsCRP (lg/mL)
Univariate 1.0 1.17 (0.60 to 2.29) 0.65 1.49 (0.77 to 2.88) 0.24 0.49 1.09 (0.93 to 1.28) 0.31
Adjusted 1.0 1.17 (0.59 to 2.33) 0.65 1.55 (0.78 to 3.10) 0.21 0.39 1.10 (0.93 to 1.30) 0.29
IL-6 and D-dimerscore
Univariate 1.0 1.15 (0.56 to 2.38) 0.71 3.07 (1.57 to 6.00) 0.001 0.001 1.51 (1.15 to 1.97) 0.003
Adjusted 1.0 1.20 (0.57 to 2.54) 0.64 3.67 (1.74 to 7.72) <0.001 <0.001 1.58 (1.17 to 2.13) 0.003
hsCRP indicates high-sensitivity C-reactive protein; OR, odds ratio.*Covariates include: study indicators, log-transformed time to event, age, gender, race, body mass index, HIV-RNA, baseline CD4+ cell count, and earlier AIDS at baseline.†Number of fatal CVD events=74.‡Number of nonfatal CVD events=214.§Based on 2 df chi-square test.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 7
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

were measured a median of 2.6 years before the nonfatalevent. To our knowledge, the prognostic importance of thesemarkers for fatal, as compared to nonfatal, CVD events hasnot been studied in the setting of HIV infection.
Considering the results based on the first hypothesis, ourfindings are consistent with studies in the general populationthat show an increased risk of more fatal CVD events forpatients with higher inflammatory markers. In MRFIT, higherCRP levels at baseline were significantly associated with CHDdeath, all of which occurred 11 to 17 years after the CRPmeasurement (P<0.001). No association (P=0.78) was foundbetween baseline CRP and nonfatal MIs, which occurred 6 to7 years after CRP measurement.1 In the PROSPER study, IL-6and CRP, measured at baseline in over 5000 patients, wereboth more strongly related to fatal CVD events than nonfatalCVD events.3 Engstr€om et al. measured 5 other inflammation-sensitive plasma proteins (ISPs)—fibrinogen, orosomucoid,a1-antirypsin, haptoglobin, and ceruloplasmin—6075 healthymen and found that, for men who subsequently developed acoronary event, fatal events were related to the number ofISPs measured at the baseline examination, which was anaverage of 12.9 years before the events.2
In addition to IL-6, D-dimer, a fibrin degradation productand marker of ongoing coagulation, was significantly associ-ated with severity of CVD disease. We have previously shownthat D-dimer is elevated among patients with HIV infection.5
The significant association of baseline D-dimer with severityof CVD outcomes may reflect activation of coagulationsystems in response to low-grade inflammation associatedwith HIV infection. It has been shown that HIV replicationalters the composition of extrinsic pathway coagulationfactors,23 and this cycle of inflammation and coagulationresulting from infection may increase the risk of progressiveorgan dysfunction and death.24,25
Higher levels of inflammatory markers and D-dimer for thosewith fatal CVD may also reflect greater underlying disease. Incross-sectional studies, higher D-dimer levels have beenassociated with severity of peripheral atherosclerosis.26,27
In an overview of 3 studies, higher levels of IL-6 measured atthe time of stroke diagnosis were associated with anincreased risk of a poor outcome, including death,28 andconcluded that IL-6 may be a general marker of diseaseseverity. Although we excluded HIV-positive patients with ahistory of CVD, recent cross-sectional comparisons ofHIV-positive men and women without a history of CVD withHIV-negative controls have found differences in vascularabnormalities.29–31 In 2 studies by the same group, those withHIV were found to have more noncalcified coronary plaque byCT angiography.29,30 Furthermore, in one of these studies,correlations between soluble CD163 and increased amount ofnoncalcified plaque suggests that monocyte and macrophageactivation may contribute to formation of vulnerable plaque inHIV-positive patients.30 Thus, it is possible that those withhigher inflammatory markers had more vulnerable plaquethan those who did not. In another study,31 HIV-positivepatients without a history of CVD had more structural andfunctional abnormalities based on cardiac MRI than HIV-negative patients.
Studies in the general population have reported that higherlevels of markers of inflammation measured at the time of anacute coronary event are related to subsequent mortality, butnot to recurrent coronary events.32–34 These observationsmay be related to the findings of our second hypothesis, thatmortality after nonfatal CVD events would be higher amongHIV-positive patients with higher, as compared to lower, levelsof IL-6, hsCRP, and D-dimer. For patients in the generalpopulation, De Servi et al. speculated that the highestinflammatory markers observed during an acute coronarysyndrome are more likely to be observed among patients whohad high levels before the event.35 If HIV patients who arealready in a state of ongoing immune activation with chroniclow-grade inflammation are at increased risk of an exagger-ated inflammatory response after their CVD event, as hasbeen suggested based on findings in the general population,3
this could explain the findings based on our second hypoth-esis. However, we cannot directly address this because
Table 4. Unadjusted and Covariate Adjusted* Hazard Ratios for All-Cause Mortality After Nonfatal CVD† (n=214) EventsAssociated With a Doubling of Biomarker or 1-Unit Increase in IL-6/D-Dimer Score
Biomarker
Median (IQR) Univariate Adjusted
Deaths (n=23) Survivors (n=191) HR 95% CI P Value HR 95% CI P Value
IL-6, pg/mL 3.1 (2.3 to 6.2) 2.2 (1.5 to 3.2) 1.72 (1.28 to 2.31) <0.001 1.85 (1.25 to 2.72) 0.002
D-dimer, lg/mL 0.47 (0.29 to 0.59) 0.27 (0.17 to 0.42) 1.73 (1.27 to 2.36) <0.001 1.76 (1.17 to 2.66) 0.007
hsCRP, lg/mL 5.3 (2.6 to 7.5) 2.0 (1.0 to 4.9) 1.44 (1.15 to 1.80) 0.001 1.39 (1.08 to 1.78) 0.01
IL-6 and D-dimer score 0.94 (0.37 to 1.57) 0.18 (�0.25 to 0.72) 1.88 (1.39 to 2.55) <0.001 2.01 (1.35 to 3.01) <0.001
CVD indicates cardiovascular disease; hsCRP, high-sensitivity C-reactive protein; HR, hazard ratio.*Covariates include: study indicators, log-transformed time to event, age, gender, race, body mass index, HIV-RNA at baseline and proximal to nonfatal CVD event, CD4+ cell count atbaseline and proximal to nonfatal CVD event, and earlier AIDS at baseline.†Number of deaths after a nonfatal CVD event=23, including deaths attributed to CVD and unwitnessed deaths not resulting from violence, suicide, or drug abuse.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 8
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from

biomarkers were not measured at the time of the nonfatalCVD event.
There are several limitations to our findings. Cause ofdeath was uncertain for many of the deaths. However,because sudden cardiac deaths account for most cardiac andmany non-AIDS deaths among HIV-positive individuals,36 wefound it reasonable to consider unwitnessed deaths notattributable to suicide, drug abuse, or violence as fatal CVD.In addition, we showed, in a sensitivity analysis, that resultsdid not differ when unwitnessed deaths were excluded fromthe logistic models. Another limitation was that importantCVD risk factors at baseline were not fully assessed and couldonly be partially adjusted for. ORs were reduced when onlySMART patients for whom smoking and blood lipids weremeasured at baseline were considered. Although IL-6 levelswere higher among smokers than nonsmokers in SMART, thepercentages of patients with fatal and nonfatal events whosmoked were similar (Table 2), and ORs from unadjusted andsmoking-adjusted models were also similar, suggesting thatsmoking was not an important confounding factor in studyingseverity of CVD events. We also did not measure thebiomarkers in the time period immediately before eventsoccurred or at the time of the event. Correlations amongmeasurements taken more remotely with those proximal tothe event may be informative. Finally, power for bothhypotheses was limited, particularly for the analysesrestricted to the subgroup of patients who participated inSMART, as well as for the patients in the control arms of the 3studies, and, as a consequence, CIs are wide for thoseanalyses. Strengths include the central measurement of thebiomarkers, excellent follow-up, and the uniqueness of thisinvestigation in HIV-positive patients.
ConclusionIn conclusion, we sought to assess the prognostic value ofinflammatory and coagulation markers for fatal outcomesamong patients with HIV who experience CVD events. Wefound that activated inflammatory and coagulation pathways,as demonstrated by higher IL-6 and D-dimer plasma levels,are associated with a greater risk of fatal, as compared tononfatal, CVD and a greater risk of death after a nonfatal CVDevent. These findings suggest that chronic inflammation andactivated coagulation associated with HIV leads to a pooroutcome when a CVD event occurs.
AcknowledgmentsThe authors acknowledge the SMART, ESPRIT, and SILCAAT patients.See N Engl J Med 2006;355:2283-2296 for the complete list ofSMART investigators and N Engl J Med 2009;361:1548-1559 for thecomplete list of ESPRIT and SILCAAT investigators.
Sources of FundingThis study was funded by the National Institutes of Health(Grant No.: U01AI46957 and U01AI068641 [ESPRIT andSMART]; U01AI042170 and U01AI46362 [SMART]). SILCAATwas supported by grants from Chiron and Novartis. Thefunding sources had no role in data collection, data analysis,or decisions to publish the results.
DisclosuresNone.
References1. Kuller LH, Tracy RP, Shaten J, Meilahn EN. Relation of C-reactive protein and
coronary heart disease in the MRFIT nested case-control study. Am JEpidemiol. 1996;144:537–547.
2. Engstr€om G, Hedblad B, Stavenow L, Tyd�en P, Lind P, Janzon L, Lindg€arde F.Fatality of future coronary events is related to inflammation-sensitive plasmaproteins a population-based prospective cohort study. Circulation.2004;110:27–31.
3. Sattar N, Murrary HM, Welsh P, Blauw GJ, Buckley BM, Cobbe S, de Craen AJM,Lowe GD, Jukema JW, Macfarlane PW, Murphy MB, Stott DJ, Westendorp RGJ,Shepherd J, Ford I, Packard CJ; for the Prospective Study of Pravastatin in theElderly at Risk (PROSPER) Study Group. Are markers of inflammation morestrongly associated with risk for fatal than for non-fatal vascular events?. PLoSMed. 2009;6:e1000099.
4. van Wijk DF, Boekholdt SM, Wareham NJ, Ahmadi-Abhari S, Kastelein JJ, StroesES, Khaw KT. C-reactive protein, fatal and nonfatal coronary artery disease,stroke, and peripheral artery disease in the prospective EPIC-Norfolk cohortstudy. Arterioscler Thromb Vasc Biol. 2013;33:2888–2894.
5. Neuhaus J, Jacobs DR, Baker JV, Calmy A, Duprez D, La Rosa A, Kuller LH, PettSL, Ristola M, Ross MJ, Shlipak MG, Tracy R, Neaton JD. Markers ofinflammation, coagulation, and renal function are elevated in adults with HIVinfection. J Infect Dis. 2010;201:1788–1795.
6. Catalfamo M, Le Saout C, Lane HC. The role of cytokines in the pathogenesisand treatment of HIV infection. Cytokine Growth Factor Rev. 2012;23:207–214.
7. Deeks SG, Tracy R, Douek DC. Systemic effects of inflammation on healthduring chronic hiv infection. Immunity. 2013;39:633–645.
8. Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardialinfarction rates and cardiovascular risk factors among patients with humanimmunodeficiency virus disease. J Clin Endocrinol Metab. 2007;92:2506–2512.
9. Lang S, Mary-Krause M, Cotte L, Gilquin J, Partisani M, Simon A, Boccara F,Bingham A, Costagliola D. Increased risk of myocardial infarction in HIV-infected patients in France, relative to the general population. AIDS.2010;24:1228–1230.
10. Obel N, Thomsen HF, Kronborg G, Larsen CS, Hildebrandt PR, Sørensen HT,Gerstoft J. Ischemic heart disease in HIV-infected and HIV-uninfected individ-uals: a population-based cohort study. Clin Infect Dis. 2007;44:1625–1631.
11. Currier JS, Taylor A, Boyd F, Dezii CM, Kawabata H, Burtcel B, Maa JF, HodderS. Coronary heart disease in HIV-infected individuals. J Acquir Immune DeficSyndr. 1999;33:506–512.
12. Freiberg MS, Chang CCH, Kuller LH, Skanderson M, Lowy E, Kraemer KL, ButtAA, Goetz MB, Leaf D, Oursler KA, Rimland D, Barradas MR, Brown S, Gilbert C,McGinnis K, Crothers K, Sico J, Crane H, Warner A, Gottlieb S, Gottdiener J,Tracy RP, Budoff M, Watson C, Armah KA, Doebler D, Bryant K, Justice AC. HIVinfection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;1–9.
13. Duprez DA, Neuhaus J, Kuller LH, Tracy R, Belloso W, De WITS, Drummond F,Lane HC, Ledergerber B, Lundgren J, Nixon D, Paton NI, Prineas RJ, Neaton JD;for the INSIGHT SMART Study Group. Inflammation, coagulation andcardiovascular disease in HIV-infected patients. PLoS One. 2012; 7: e44454.
14. SMART Study Group. CD4+ count-guided interruption of antiretroviral treat-ment. N Engl J Med. 2006;355:2283–2296.
15. SMART Study Group. Risk for opportunistic disease and death after reinitiatingcontinuous antiretroviral therapy in patients with HIV previously receivingepisodic therapy, a randomized trial. Ann Intern Med. 2008;149:289–299.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 9
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from
16. Emery S, Abrams DI, Cooper DA, Darbyshire JH, Lane HC, Lundgren JD, NeatonJD; the ESPRIT Study Group. The evaluation of subcutaneous proleukin (R)(interleukin-2) in a randomized international trial: rationale, design, andmethods of ESPRIT. Control Clin Trials. 2002;23:198–220.
17. The INSIGHT-ESPRIT Study Group and SILCAAT Scientific Committee. Interleu-kin-2 therapy in patientswith HIV infection.NEngl JMed. 2009;361:1548–1559.
18. Lifson AR, INSIGHT Endpoint Review Committee Writing Group, Belloso WH,Davey RT, Duprez D, Gatell JM, Hoy JF, Krum EA, Nelson R, Pederson C, PerezG, Price RW, Prineas RJ, Rhame FS, Sampson JH, Worley J; for the INSIGHTStudy Group. Development of diagnostic criteria for serious non-AIDS eventsin HIV clinical trials. HIV Clinical Trials. 2010; 11.4: 205–219.
19. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction.J Am Coll Cardiol. 2007;50:2173–2195.
20. Kowalska JD, Friis-Møller N, Kirk O, Bannister W, Mocroft A, Sabin C, Reiss P,Gill J, Lewden C, Phillips A, D-Arminio Monforte A, Law M, Sterne J, DeWit S,Lundgren JD; for the CoDe Working Group; the D: A: D Study Group. TheCoding Causes of Death in HIV (CoDe) Project: initial results and evaluation ofmethodology. Epidemiology. 2011;22:516–523.
21. Grund B, Baker J, Deeks S, Wolfson J, Wentworth D, Cozzi-Lepri A, Cohen C,Phillips A, Lundgren J, Neaton J; for the INSIGHT SMART/ESPRIT/SILCAATStudy Groups. Combined effect of interleukin-6 and D-dimer on the risk ofserious non-AIDS conditions: data from 3 prospective cohorts (Abstract 60).In: Program and abstracts of the 20th Conference on Retroviruses andOpportunistic Infections, Atlanta, GA; March 2013.
22. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for theUse of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Depart-ment of Health and Human Services. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentsgl.pdf. Accessed May 15, 2014.
23. Baker JV, Brummel-Ziedins K, Neuhaus J, Duprez D, Cummins N, Dalmau D,DeHovitz J, Lehmann C, Sullivan A, Woolley I, Kuller L, Neaton JD, Tracy RP. HIVreplication alters the composition of extrinsic pathway coagulation factors andincreases thrombin generation. J Am Heart Assoc. 2013;2:e000264.
24. Dellinger RP. Cardiovascular management of septic shock. Crit Care Med.2003;31:946–955.
25. Levi M, van der Poll T, B€uller HR. Bidirectional relation between inflammationand coagulation. Circulation. 2004;109:2698–2704.
26. Lassila R, Peltonen S, Lep€antalo M, Saarinen O, Kauhanen P, Manninen V.Severity of peripheral atherosclerosis is associated with fibrinogen and
degradation of cross-linked fibrin. Arterioscler Thromb Vasc Biol.1993;13:1738–1742.
27. Lee AJ, Fowkes FG, Lowe GD, Rumley A. Fibrin D-dimer, haemostatic factorsand peripheral arterial disease. Thromb Haemost. 1995;74:828–832.
28. Whiteley W, Jackson C, Lewis S, Lowe G, Rumley A, Sandercock P, Wardlaw J,Dennis M, Sudlow C. Inflammatory markers and poor outcome after stroke: aprospective cohort study and systematic review of interleukin-6. PLoS Med.2009;6:e1000145.
29. Zanni MV, Abbara S, Lo J, Wai B, Hark D, Marmarelis E, Grinspoon SK.Increased coronary atherosclerotic plaque vulnerability by coronary com-puted tomography angiography in HIV-infected men. AIDS. 2013;27:1263–1272.
30. Fitch KV, Srinivasa S, Abbara S, Burdo TH, Williams KC, Eneh P, Lo J, GrinspoonSK. Noncalcified coronary atherosclerotic plaque and immune activation inHIV-infected women. J Infect Dis. 2013;208:1737–1746.
31. Holloway CJ, Ntusi N, Suttie J, Mahmod M, Wainwright E, Clutton G, HancockG, Beak P, Tajar A, Piechnik SK, Schneider JE, Angus B, Clarke K, Dorrell L,Neubauer S. Comprehensive cardiac magnetic resonance imaging andspectroscopy reveal a high burden of myocardial disease in HIV patients.Circulation. 2013;128:814–822.
32. Lindahl B, Toss H, Siegbahn A, Venge P, Wallentin L. Markers of myocardialdamage and inflammation in relation to long-term mortality in unstablecoronary artery disease. N Engl J Med. 2000;343:1139–1147.
33. James SK, Armstrong P, Barnathan E, Califf R, Lindahl B, Siegbahn A, SimoonsML, Topol EJ, Venge P, Wallentin L. Troponin and C-reactive protein havedifferent relations to subsequent mortality and myocardial infarction afteracute coronary syndromea GUSTO-IV substudy. J Am Coll Cardiol. 2003;41:916–924.
34. Zamani P, Schwartz GG, Olsson AG, Rifai N, Bao W, Libby P, Ganz P, Kinlay S.Inflammatory biomarkers, death, and recurrent nonfatal coronary events afteran acute coronary syndrome in the MIRACL study. J Am Heart Assoc. 2013;2:e003103.
35. De Servi S, Mariani M, Mariani G, Mazzone A. C-reactive protein increase inunstable coronary disease cause or effect? J Am Coll Cardiol. 2005;46:1496–1502.
36. Tseng ZH, Secemsky EA, Dowdy D, Vittinghoff E, Moyers B, Wong JK, HavlirDV, Hsue PY. Sudden cardiac death in patients with human immunodeficiencyvirus infection. J Am Coll Cardiol. 2012;59:1891–1896.
DOI: 10.1161/JAHA.114.000844 Journal of the American Heart Association 10
Severity of Cardiovascular Disease Nordell et alORIG
INALRESEARCH
by guest on July 17, 2014http://jaha.ahajournals.org/Downloaded from
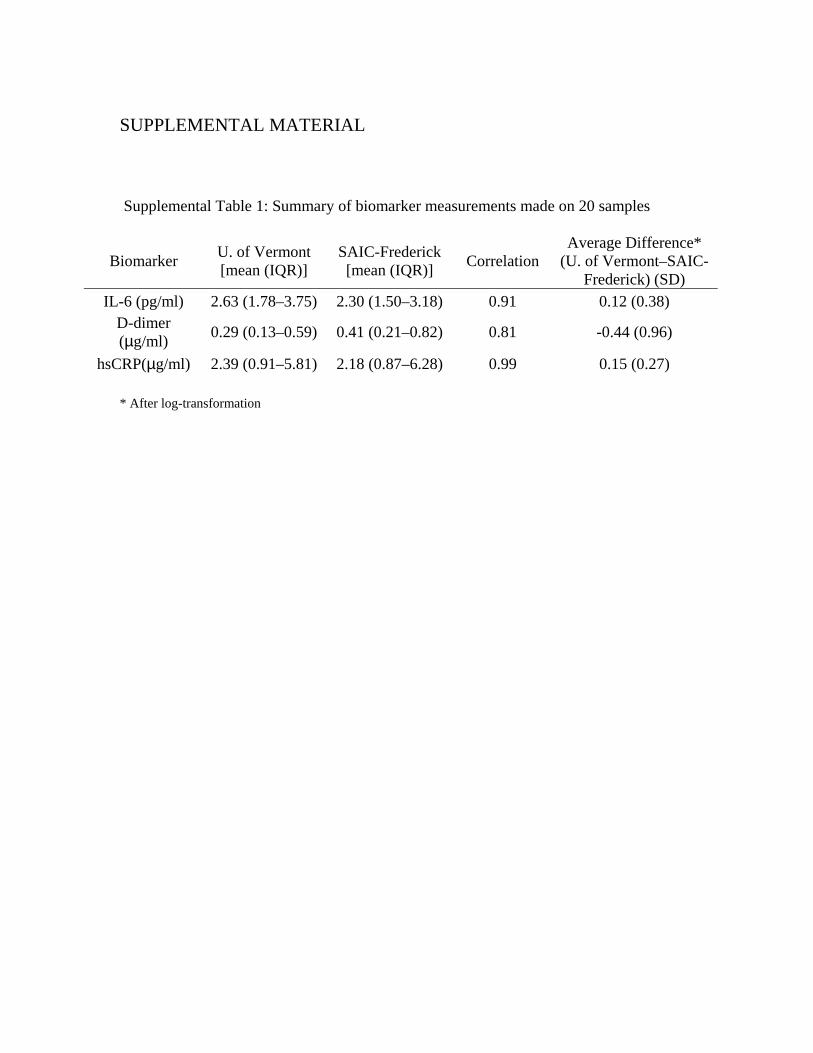
SUPPLEMENTAL MATERIAL Supplemental Table 1: Summary of biomarker measurements made on 20 samples
Biomarker U. of Vermont [mean (IQR)]
SAIC-Frederick [mean (IQR)]
Correlation Average Difference*
(U. of Vermont–SAIC-Frederick) (SD)
IL-6 (pg/ml) 2.63 (1.78–3.75) 2.30 (1.50–3.18) 0.91 0.12 (0.38) D-dimer (µg/ml)
0.29 (0.13–0.59) 0.41 (0.21–0.82) 0.81 -0.44 (0.96)
hsCRP(µg/ml) 2.39 (0.91–5.81) 2.18 (0.87–6.28) 0.99 0.15 (0.27)
* After log-transformation

SMART Study Group (see also N Eng J Med 2006; 355:2283-2296) Community Programs for Clinical Research on AIDS Chair’s Office and Operations Center: F. Gordin (group leader), E. Finley, D. Dietz, C. Chesson, M. Vjecha, B. Standridge, B. Schmetter, L. Grue, M. Willoughby, A. Demers; Regional Coordinating Centers Copenhagen: J.D. Lundgren, A. Phillips, U.B. Dragsted, K.B. Jensen, A. Fau, L. Borup, M. Pearson, P.O. Jansson, B.G. Jensen, T.L. Benfield; London: J.H. Darbyshire, A.G. Babiker, A.J. Palfreeman, S.L. Fleck, Y. Collaco-Moraes, B. Cordwell, W. Dodds, F. van Hooff, L. Wyzydrag; Sydney: D.A. Cooper, S. Emery, F.M. Drummond, S.A. Connor, C.S. Satchell, S. Gunn, S. Oka, M.A. Delfino, K. Merlin, C. McGinley; Statistical and Data Management Center Minneapolis: J.D. Neaton, G. Bartsch, A. DuChene, M. George, B. Grund, M. Harrison, C. Hogan (deceased), E. Krum, G. Larson, C. Miller, R. Nelson, J. Neuhaus, M.P. Roediger, T. Schultz, L. Thackeray; Electrocardiography Reading Center: R. Prineas, C. Campbell; End Point Review Committee: G. Perez (cochair), A. Lifson (cochair), D. Duprez, J. Hoy, C. Lahart, D. Perlman, R. Price, R. Prineas, F. Rhame, J. Sampson, J. Worley; NIAID Data and Safety Monitoring Board: M. Rein (chair), R. Der Simonian (executive secretary), B.A. Brody, E.S. Daar, N.N. Dubler, T.R. Fleming, D.J. Freeman, J.P. Kahn, K.M. Kim, G. Medoff, J.F. Modlin, R. Moellering, Jr., B.E. Murray, B. Pick, M.L. Robb, D.O. Scharfstein, J. Sugarman, A. Tsiatis, C. Tuazon, L. Zoloth; NIAID K. Klingman, S. Lehrman; SMART Clinical Site Investigators Argentina: J. Lazovski, W.H. Belloso, M.H. Losso, J.A. Benetucci, S. Aquilia, V. Bittar, E.P. Bogdanowicz, P.E. Cahn, A.D. Casiró, I. Cassetti, J.M. Contarelli, J.A. Corral, A. Crinejo, L. Daciuk,D.O. David, G. Guaragna, M.T. Ishida, A. Krolewiecki, H.E. Laplume, M.B. Lasala, L. Lourtau, S.H. Lupo, A. Maranzana, F. Masciottra, M. Michaan, L. Ruggieri, E. Salazar, M. Sánchez, C. Somenzini; Australia : J.F. Hoy, G.D. Rogers, A.M. Allworth, J.S.C. Anderson, J. Armishaw, K. Barnes, A. Carr, A. Chiam, J.C.P. Chuah, M.C. Curry, R.L. Dever, W.A. Donohue, N.C. Doong, D.E. Dwyer, J. Dyer, B. Eu, V.W. Ferguson, M.A.H. French, R.J. Garsia, J. Gold, J.H. Hudson, S. Jeganathan, P. Konecny, J. Leung, C.L. McCormack, M. McMurchie, N. Medland, R.J. Moore, M.B. Moussa, D. Orth, M. Piper, T. Read, J.J. Roney, N. Roth, D.R. Shaw, J. Silvers, D.J. Smith, A.C. Street, R.J. Vale, N.A. Wendt, H. Wood, D.W. Youds, J. Zillman; Austria: A. Rieger, V. Tozeau, A. Aichelburg, N. Vetter; Belgium: N. Clumeck, S. Dewit, A. de Roo, K. Kabeya, P. Leonard, L. Lynen, M. Moutschen, E. O’Doherty; Brazil: L.C. Pereira, Jr., T.N.L. Souza, M. Schechter, R. Zajdenverg, M.M.T.B. Almeida, F. Araujo, F. Bahia, C. Brites, M.M. Caseiro, J. Casseb, A. Etzel, G.G. Falco, E.C.J. Filho, S.R. Flint, C.R. Gonzales, J.V.R. Madruga, L.N. Passos, T. Reuter, L.C. Sidi, A.L.C. Toscano; Canada: D. Zarowny, E. Cherban, J. Cohen, B. Conway, C. Dufour, M. Ellis, A. Foster, D. Haase, H. Haldane, M. Houde, C. Kato, M. Klein, B. Lessard, A. Martel, C. Martel, N. McFarland, E. Paradis, A. Piche, R. Sandre, W. Schlech, S. Schmidt, F. Smaill, B. Thompson, S. Trottier, S. Vezina, S. Walmsley; Chile:

M.J. Wolff Reyes, R. Northland; Denmark: L. Ostergaard, C. Pedersen, H. Nielsen, L. Hergens, I.R. Loftheim, K.B. Jensen; Estonia: M. Raukas, K. Zilmer; Finland : J. Justinen, M. Ristola; France : P.M. Girard, R. Landman, S. Abel, S. Abgrall, K. Amat, L. Auperin, R. Barruet, A. Benalycherif, N. Benammar, M. Bensalem, M. Bentata, J.M. Besnier, M. Blanc, O. Bouchaud, A. Cabié, P. Chavannet, J.M. Chennebault, S. Dargere, X. de la Tribonniere, T. Debord, N. Decaux, J. Delgado, M. Dupon, J. Durant, V. Frixon-Marin, C. Genet, L. Gérard, J. Gilquin, B. Hoen, V. Jeantils, H. Kouadio, P. Leclercq, J.-D. Lelièvre, Y. Levy, C.P. Michon, P. Nau, J. Pacanowski, C. Piketty, I. Poizot-Martin, I. Raymond, D. Salmon, J.L. Schmit, M.A. Serini, A. Simon, S. Tassi, F. Touam, R. Verdon, P. Weinbreck, L. Weiss, Y. Yazdanpanah, P. Yeni; Germany: G. Fätkenheuer, S. Staszewski, F. Bergmann, S. Bitsch, J.R. Bogner, N. Brockmeyer, S. Esser, F.D. Goebel, M. Hartmann, H. Klinker, C. Lehmann, T. Lennemann, A. Plettenberg, A. Potthof, J. Rockstroh, B. Ross, A. Stoehr, J.C. Wasmuth, K. Wiedemeyer, R. Winzer; Greece: A. Hatzakis, G. Touloumi, A. Antoniadou, G.L. Daikos, A. Dimitrakaki, P. Gargalianos-Kakolyris, M. Giannaris, A. Karafoulidou, A. Katsambas, O. Katsarou, A.N. Kontos, T. Kordossis, M.K. Lazanas, P. Panagopoulos, G. Panos, V. Paparizos, V. Papastamopoulos, G. Petrikkos, H. Sambatakou, A. Skoutelis, N. Tsogas, G. Xylomenos; Ireland: C.J. Bergin, B. Mooka; Israel: S. Pollack, M.G. Mamorksy, N. Agmon-Levin, R. Karplus, E. Kedem, S. Maayan, E. Shahar, Z. Sthoeger, D. Turner, I. Yust; Italy : G. Tambussi, V. Rusconi, C. Abeli, M. Bechi, A. Biglino, S. Bonora, L. Butini, G. Carosi, S. Casari, A. Corpolongo, M. De Gioanni, G. Di Perri, M. Di Pietro, G. D’Offizi, R. Esposito, F. Mazzotta, M. Montroni, G. Nardini, S. Nozza, T. Quirino, E. Raise; Japan : M. Honda, M. Ishisaka; Lithuania : S. Caplinskas, V. Uzdaviniene; Luxembourg: J.C. Schmit, T. Staub; Morocco: H. Himmich, K. Marhoum El Filali; New Zealand: G.D. Mills, T. Blackmore, J.A. Masters, J. Morgan, A. Pithie; Norway: J. Brunn, V. Ormasssen; Peru : A. La Rosa, O. Guerra, M. Espichan, L. Gutierrez, F. Mendo, R. Salazar; Poland: B. Knytz, A. Horban, E. Bakowska, M. Beniowski, J. Gasiorowski, J. Kwiatkowski; Portugal: F. Antunes, R.S. Castro, M. Doroana, A. Horta, K. Mansinho, A.C. Miranda, I.V. Pinto, E. Valadas, J. Vera; Russia: A. Rakhmanova, E. Vinogradova, A. Yakovlev, N. Zakharova; South Africa: R. Wood, C. Orrel;

Spain: J. Gatell, J.A. Arnaiz, R. Carrillo, B. Clotet, D. Dalmau, A. González, Q. Jordano, A. Jou, H. Knobel, M. Larrousse, R. Mata, J.S. Moreno, E. Oretaga, J.N. Pena, F. Pulido, R. Rubio, J. Sanz, P. Viciana; Switzerland: B. Hirschel, R. Spycher, M. Battegay, E. Bernasconi, S. Bottone, M. Cavassini, A. Christen, C. Franc, H.J. Furrer, A. Gayet-Ageron, D. Genné, S. Hochstrasser, L. Magenta, C. Moens, N. Müller, R. Nüesch; Thailand: P. Phanuphak, K. Ruxrungtham, W. Pumpradit, P. Chetchotisakd, S. Dangthongdee, S. Kiertiburanakul, V. Klinbuayaem, P. Mootsikapun, S. Nonenoy, B. Piyavong, W. Prasithsirikul, P. Raksakulkarn; United Kingdom: B.G. Gazzard, J.G. Ainsworth, J. Anderson, B.J. Angus, T.J. Barber, M.G. Brook, C.D. Care, D.R. Chadwick, M. Chikohora, D.R. Churchill, D. Cornforth, D.H. Dockrell, P.J. Easterbrook, P.A. Fox, R. Fox, P.A. Gomez, M.M. Gompels, G.M. Harris, S. Herman, A.G.A. Jackson, S.P.R. Jebakumar, M.A. Johnson, G.R. Kinghorn, K.A. Kuldanek, N. Larbalestier, C. Leen, M. Lumsden, T. Maher, J. Mantell, R. Maw, S. McKernan, L. McLean, S. Morris, L. Muromba, C.M. Orkin, A.J. Palfreeman, B.S. Peters, T.E.A. Peto, S.D. Portsmouth, S. Rajamanoharan, A. Ronan, A. Schwenk, M.A. Slinn, C.J. Stroud, R.C. Thomas, M.H. Wansbrough-Jones, H.J. Whiles, D.J. White, E. Williams, I.G. Williams, M. Youle; United States: D.I. Abrams, E.A. Acosta, S. Adams, A. Adamski, L. Andrews, D. Antoniskis, D.R. Aragon, R. Arduino, R. Artz, J. Bailowitz, B.J. Barnett, C. Baroni, M. Barron, J.D. Baxter, D. Beers, M. Beilke, D. Bemenderfer, A. Bernard, C.L. Besch, M.T. Bessesen, J.T. Bethel, S. Blue, J.D. Blum, S. Boarden, R.K. Bolan, J.B. Borgman, I. Brar, B.K. Braxton, U.F. Bredeek, R. Brennan, D.E. Britt, J. Brockelman, S. Brown, V. Bruzzese, D. Bulgin-Coleman, D.E. Bullock, V. Cafaro, B. Campbell, S. Caras, J. Carroll, K.K. Casey, F. Chiang, G. Childress, R.B. Cindrich, C. Clark, M. Climo, C. Cohen, J. Coley, D.V. Condoluci, R. Contreras, J. Corser, J. Cozzolino, L.R. Crane, L. Daley, D. Dandridge, V. D’Antuono, J.G. Darcourt Rizo Patron, J.A. DeHovitz, E. DeJesus, J. Des-Jardin, M. Diaz-Linares, C. Dietrich, P. Dodson, E. Dolce, K. Elliott, D. Erickson, M. Estes, L.L. Faber, J. Falbo, M.J. Farrough, C.F. Farthing, P. Ferrell-Gonzalez, H. Flynn, C. Frank, M. Frank, K.F. Freeman, N. French, G. Friedland, N. Fujita, L. Gahagan, K. Genther, I. Gilson, M.B. Goetz, E. Goodwin, F. Graziano, C.K. Guity, P. Gulick, E.R. Gunderson, C.M. Hale, K. Hannah, H. Henderson, K. Hennessey, W.K. Henry, D.T. Higgins, S.L. Hodder, H.W. Horowitz, M. Howe-Pittman, J. Hubbard, R. Hudson, H. Hunter, C. Hutelmyer, M.T. Insignares, L. Jackson, L. Jenny, M. John, D.L. Johnson, G. Johnson, J. Johnson, L. Johnson, J. Kaatz, J. Kaczmarski, S. Kagan, C. Kantor, T. Kempner, K. Kieckhaus, N. Kimmel, B.M. Klaus, N. Klimas, J.R. Koeppe, J. Koirala, J. Kopka, J.R. Kostman, M.J. Kozal, A. Kumar, A. Labriola, H. Lampiris, C. Lamprecht, K.M. Lattanzi, J. Lee, J. Leggett, C. Long, A. Loquere, K. Loveless, C.J. Lucasti, R. Luskin-Hawk, M. MacVeigh, L.H. Makohon, S. Mannheimer, N.P. Markowitz, C. Marks, N. Martinez, C. Martorell, E. McFeaters, B. McGee, D.M. McIntyre, J. McKee, E. McManus, L.G. Melecio, D. Melton, S. Mercado, E. Merrifield, J.A. Mieras, M. Mogyoros, F.M. Moran, K. Murphy, D. Mushatt, S. Mutic, I. Nadeem, J.P. Nadler, R. Nahass, D. Nixon, S. O’Brien, A. Ognjan, M. O’Hearn, K. O’Keefe, P.C. Okhuysen, E. Oldfield, D. Olson, R. Orenstein, R. Ortiz, J. Osterberger, W. Owen, F. Parpart, V. Pastore-Lange, S. Paul, A. Pavlatos, D.D. Pearce, R. Pelz, G. Perez, S. Peterson, G. Pierone, Jr., D. Pitrak, S.L. Powers, H.C. Pujet, J.W. Raaum, J. Ravishankar, J. Reeder, N. Regevik, N.A. Reilly, C. Reyelt, J. Riddell IV, D. Rimland, M.L. Robinson, A.E. Rodriguez, M.C. Rodriguez-Barradas, V. Rodriguez Derouen, R. Roland, C. Rosmarin, W.L. Rossen, J.R. Rouff, J.H. Sampson, M. Sands, C. Savini, S. Schrader, M.M. Schulte, C. Scott, R. Scott, H. Seedhom, M. Sension, A. Sheble-Hall, A. Sheridan, J. Shuter, L.N. Slater, R. Slotten, D. Slowinski, M. Smith, S. Snap, D.M. States, M. Stewart, G. Stringer, J. Sullivan, K.K. Summers, K. Swanson, I.B. Sweeton, S. Szabo, E.M. Tedaldi, E.E. Telzak, Z. Temesgen, D. Thomas, M.A. Thompson, S. Thompson, C. Ting Hong Bong, C. Tobin, J. Uy, A. Vaccaro, L.M. Vasco, I. Vecino, G.K. Verlinghieri, F. Visnegarwala, B.H. Wade, V. Watson, S.E. Weis, J.A. Weise, S. Weissman, A.M. Wilkin, L. Williams, J.H. Witter, L. Wojtusic, T.J. Wright, V. Yeh, B. Young, C. Zeana, J. Zeh; Uruguay: E. Savio, M. Vacarezza.

ESPRIT and SILCAAT Study Groups (see also N Eng J Med 2009; 361: 1548-1559) Coordinating Centers: Copenhagen: B Aagaard, E Aragon, J Arnaiz, L Borup, B Clotet, U Dragsted, A Fau, D Gey, J Grarup, U Hengge, P Herrero, P Jansson, B Jensen, K Jensen, H Juncher, P Lopez, J Lundgren, C Matthews, D Mollerup, M Pearson, A Phillips, S Reilev, K Tillmann, S Varea. London: B Angus, A Babiker, B Cordwell, J Darbyshire, W Dodds, S Fleck, J Horton, F Hudson, Y Moraes, F Pacciarini, A Palfreeman, N Paton, N Smith, F van Hooff. Minneapolis: J Bebchuk, G Collins, E Denning, A DuChene, L Fosdick, M Harrison, K Herman-Lamin, E Krum, G Larson, J Neaton, R Nelson, K Quan, S Quan, T Schultz, G Thompson, D Wentworth, N Wyman. Sydney: C Carey, F Chan, D Cooper, B Cordwell, D Courtney-Rodgers, F Drummond, S Emery, M Harrod, S Jacoby, L Kearney, M Law, E Lin, S Pett, R Robson, N Seneviratne, M Stewart, E Watts. Washington: E Finley, F Gordin, A Sánchez, B Standridge, M Vjecha. Endpoint Review Committee: W Belloso, R Davey, D Duprez, J Gatell, J Hoy, A Lifson, C Pederson, G Perez, R Price, R Prineas, F Rhame, J Sampson, J Worley. Data and Safety Monitoring Board: J Modlin, V Beral, R Chaisson, T Fleming, C Hill, K Kim, B Murray, B Pick, M Seligmann, I Weller. National Institute of Allergy and Infectious Disease: K Cahill, L Fox, M Luzar, A Martinez, L McNay, J Pierson, J Tierney, S Vogel. International Drug Distribution (CTS Inc., Durham, North Carolina): V Costas, J Eckstrand. Specimen Repository (SAIC Frederick, Inc.): S Brown. Clinical Sites for ESPRIT and/or SILCAAT: Argentina: L Abusamra, E Angel, S Aquilia, W Belloso, J Benetucci, V Bittar, E Bogdanowicz, P Cahn, A Casiro, J Contarelli, J Corral, L Daciuk, D David, W Dobrzanski, A Duran, J Ebenrstejin, I Ferrari, D Fridman, V Galache, G Guaragna, S Ivalo, A Krolewiecki, I Lanusse, H Laplume, M Lasala, R Lattes, J Lazovski, G Lopardo, M Losso, L Lourtau, S Lupo, A Maranzana, C Marson, L Massera, G Moscatello, S Olivia, I Otegui, L Palacios, A Parlante, H Salomon, M Sanchez, C Somenzini, C Suarez, M Tocci, J Toibaro, C Zala. Australia: S Agrawal, P Ambrose, C Anderson, J Anderson, D Baker, K Beileiter, K Blavius, M Bloch, M Boyle, D Bradford, P Britton, P Brown, T Busic, A Cain, L Carrall, S Carson, I Chenoweth, J Chuah, F Clark, J Clemons, K Clezy, D Cooper, P Cortissos, N Cunningham, M Curry, L Daly, C D’Arcy-Evans, R Del Rosario, S Dinning, P Dobson, W Donohue, N Doong, C Downs, E Edwards, S Edwards, C Egan, W Ferguson, R Finlayson, C Forsdyke, L Foy, T Franic, A Frater, M French, D Gleeson, J Gold, P Habel, K Haig, S Hardy, R Holland, J Hoy, J Hudson, R Hutchison, N Hyland, R James, C Johnston, M Kelly, M King, K Kunkel, H Lau, J Leamy, D Lester, J Leung, A Lohmeyer, K Lowe, K MacRae, C Magness, O Martinez, H Maruszak, N Medland, S Miller, J Murray, P Negus, R Newman, M Ngieng, C Nowlan, J Oddy, N Orford, D Orth, J Patching, M Plummer, S Price, R Primrose, I Prone, H Ree, C Remington, R Richardson, S Robinson, G Rogers, J Roney, N Roth, D Russell, S Ryan, J Sarangapany, T Schmidt, K Schneider, C Shields, C Silberberg, D Shaw, J Skett, D Smith, T Meng Soo, D Sowden, A Street, B Kiem Tee, Jl Thomson, S Topaz, R Vale, C Villella, A Walker, A Watson, N Wendt, L Williams, D Youds. Austria: A Aichelburg, P Cichon, B Gemeinhart, A Rieger, B Schmied, V Touzeau-Romer, N Vetter. Belgium: R Colebunders, N Clumeck, A DeRoo, K Kabeya, E O'Doherty, S de Wit. Brazil:
C De Salles Amorim, C Basso, S Flint, E Kallas, G Levi, D Lewi, L Pereira Jr, M da Silva, T Souza, A Toscano. Canada (CTN): J Angel, M Arsenault, M Bast, B Beckthold, P Bouchard, I Chabot, R Clarke, J Cohen, P Coté, M Ellis, C Gagne, J Gill, M Houde, B Johnston, N Jubinville, C Kato, N Lamoureux, G Larson, J Latendre-Paquette, A Lindemulder, A McNeil, N McFarland, J Montaner, C Morrisseau, R O’Neill, G Page, A Piche, B Pongracz, H Preziosi, L Puri, A Rachlis, E Ralph, I Raymond, D Rouleau, JP Routy, R Sandre,T Seddon, S Shafran, C Sikora, F Smaill, D Stromberg, S Trottier, S Walmsley, K Weiss, K Williams, D Zarowny. Denmark: B Baadegaard, Å Bengaard Andersen, K Boedker, P Collins, J Gerstoft, L Jensen, H Moller, P Lehm Andersen, I Loftheim, L Mathiesen, H Nielsen, N Obel, C Pedersen, D Petersen, L Pors Jensen, F Trunk Black. France (ANRS): JP Aboulker, A Aouba, M Bensalem, H Berthe, C Blanc, M Bloch, D Bornarel, O Bouchaud, F Boue, E Bouvet, C Brancon, S Breaud, D Brosseau, A Brunet, C Capitant, C Ceppi, C Chakvetadze, C Cheneau, JM Chennebault, P De Truchis, AM Delavalle, JF Delfraissy, P Dellamonica, AM Delavalle, C Dumont, N Edeb, G Fabre, S Ferrando, A Foltzer, V Foubert, JA Gastaut, J Gerbe, PM Girard, C Goujard, B Hoen, P Honore, H Hue,T Hynh, C Jung, S Kahi, C Katlama, JM Lang, V Le Baut, B Lefebvre, N Leturque, Y Lévy, J Loison, G Maddi, A Maignan, C Majerholc, C de Boever, JL Meynard, C Michelet, C Michon, M Mole, E Netzer, G Pialoux, I Poizot-Martin, F Raffi, M Ratajczak, I Ravaux, J Reynes, D Salmon-Ceron, M Sebire, A Simon, L Tegna, D Tisne-Dessus, C Tramoni, JP Viard, M Vidal, C Viet-Peaucelle, L Weiss, A Zeng, D Zucman. Germany: A Adam, K Arastéh, G Behrens, F Bergmann, M Bickel, D Bittner, J Bogner, N Brockmeyer, N Darrelmann, M Deja, M Doerler, S Esser, G Faetkenheuer, S Fenske, S Gajetzki, D Gey, F Goebel, D Gorriahn, E Harrer, T Harrer, H Hartl, M Hartmann, S Heesch, W Jakob, H Jäger, H Klinker, G Kremer, C Ludwig, K Mantzsch, S Mauss, A Meurer, A Niedermeier, N Pittack, A Plettenberg, A Potthoff, M Probst, M Rittweger, J Rockstroh, B Ross, J Rotty, E Rund, T Ruzicka, Rt Schmidt, G Schmutz, E Schnaitmann, D Schuster, T Sehr, B Spaeth, S Staszewski, HJ Stellbrink, C Stephan, T Stockey, A Stoehr, K Tillmann, A Trein, T Vaeth, M Vogel, J Wasmuth, C Wengenroth, R Winzer, E Wolf. Ireland: F Mulcahy, Dl Reidy. Israel: Y Cohen, G Drora, I Eliezer, O Godo, E Kedem, E Magen, M Mamorsky, S Pollack, Z Sthoeger, H Vered, I Yust. Italy: F Aiuti, M Bechi, A Bergamasco, D Bertelli, R Bruno, L Butini, M Cagliuso, G Carosi, S Casari, V Chrysoula, G Cologni, V Conti, A Costantini, A Corpolongo, G D’Offizi, F Gaiottino, M Di Pietro, R Esposito, G Filice, M Francesco, E Gianelli, C Graziella, L Magenta, F Martellotta, R Maserati, F Mazzotta, G Murdaca, G Nardini, S Nozza, F Puppo, M Pogliaghi, D Ripamonti, C Ronchetti, S Rusconi, V Rusconi, P Sacchi, N Silvia, F Suter, G Tambussi, A Uglietti, M Vechi, B Vergani, F Vichi, P Vitiello. Japan: A Iwamoto,Y Kikuchi, N Miyazaki, M Mori, T Nakamura, T Odawara, S Oka, T Shirasaka, M Tabata, M Takano, C Ueta, D Watanabe, Y Yamamoto. Morocco: I Erradey, H Himmich, K Marhoum El Filali. The Netherlands: W Blok, R van Boxtel, K Brinkman H Doevelaar, A van Eeden, M Grijsen, M Groot, J Juttmann, M Kuipers, S Ligthart, P van der Meulen, J Lange, N Langebeek, S Ligthart, P Reiss, C Richter, M Schoemaker, L Schrijnders-Gudde, E Septer-Bijleveld, H Sprenger, J Vermeulen, R ten Kate, B van de Ven. Norway: J Bruun, D Kvale, A Maeland. Poland: E Bakowska, M Beniowski, A Boron-Kaczmarska, J Gasiorowski, A Horban, M Inglot, B Knysz, E Mularska, M Parczewski, M Pynka, W Rymer, A Szymczak.

Portugal: M Aldir, F Antunes, C Baptista, J da Conceicao Vera, M Doroana, K Mansinho, C Raquel A dos Santos, E Valadas, I Vaz Pinto. Singapore: E Chia, E Foo, F Karim, PL Lim, A Panchalingam, N Paton, A Quek. Spain: R Alcázar-Caballero, E Aragon, J Arnaiz, J Arribas, J Arrizabalaga, X de Barron, F Blanco, E Bouza, I Bravo, S Calvo, L Carbonero, I Carpena, M Castro, B Clotet, L Cortes, M del Toro, P Domingo, M Elias, J Espinosa, V Estrada, E Fernandez-Cruz, P Fernández, H Freud, M Fuster, A Garcia, G Garcia, R Garrido, J Gatell, P Gijón, J Gonzalez-García, I Gil, A González, J González-Lahoz, P López Grosso, M Gutierrez, E Guzmán, J Iribarren, M Jiménez, A Jou, J Juega, J Lopez, P Lopez, F Lozano, L Martín-Carbonero, R Mata, G Mateo, A Menasalvas, C Mirelles, J de Miguel Prieto, M Montes, A Moreno, J Moreno, V Moreno, R Muñoz, A Ocampo, E Ortega, L Ortiz, B Padilla, A Parras, A Paster, J Pedreira, J Peña, R Perea, B Portas, J Puig, F Pulido, M Rebollar, J de Rivera, V Roca, F Rodríguez- Arrondo, R Rubio, J Santos, J Sanz, G Sebastian, M Segovia, V Soriano, L Tamargo, S Varea, P Viciana, M von Wichmann. Sweden: G Bratt, A Hollander, P Olov Pehrson, I Petz, E Sandstrom, A Sönnerborg. Switzerland: E Bernasconi, V Gurtner. Thailand: U Ampunpong, C Auchieng, C Bowonwatanuwong, P Chanchai, P Chetchotisakd, T Chuenyan, C Duncombe, M Horsakulthai, P Kantipong, K Laohajinda, P Phanuphak, V Pongsurachet, S Pradapmook, K Ruxruntham, S Seekaew, A Sonjai, S Suwanagool, W Techasathit, S Ubolyam, J Wankoon. United Kingdom: I Alexander, D Dockrell, P Easterbrook, B Edwards, E Evans, M Fisher, R Fox, B Gazzard, G Gilleran, J Hand, L Heald, C Higgs, S Jebakumar, I Jendrulek, M Johnson, S Johnson, F Karim, G Kinghorn, K Kuldanek, C Leen, R Maw, S McKernan, L McLean, S Morris, M Murphy, S O'Farrell, E Ong, B Peters, C Stroud, M Wansbrough-Jones, J Weber, D White, I Williams, M Wiselka, T Yee. United States: S Adams, D Allegra, L Andrews, B Aneja, G Anstead, R Arduino, R Artz, J Bailowitz, S Banks, J Baxter, J Baum, D Benator, D Black, D Boh, T Bonam, M Brito, J Brockelman, S Brown, V Bruzzese, A Burnside Jr., V Cafaro, K Casey, L Cason, G Childress, Cl Clark, D Clifford, M Climo, D Cohn, P Couey, H Cuervo, R Davey Jr, S Deeks, M Dennis, M Diaz-Linares, D Dickerson, M Diez, J Di Puppo, P Dodson, D Dupre, R Elion, K Elliott, W El-Sadr, M Estes, J Fabre, M Farrough, J Flamm, S Follansbee, C Foster, C Frank, J Franz, G Frechette, G Freidland, J Frische, L Fuentes, C Funk, C Geisler, K Genther, M Giles, M Goetz, M Gonzalez, C Graeber, F Graziano, D Grice, B Hahn, C Hamilton, S Hassler, A Henson, S Hopper, M John, L Johnson, M Johnson, R Johnson, R Jones, J Kahn, M Kelly, N Klimas, M Kolber, S Koletar, A Labriola, R Larsen, F Lasseter, M Lederman, T Ling, T Lusch, R MacArthur, C Machado, L Makohon, J Mandelke, S Mannheimer, N Markowitz, M Martínez, N Martinez, M Mass, H Masur, D McGregor, D McIntyre, J McKee, D McMullen, M Mettinger, S Middleton, J Mieras, D Mildvan, P Miller, T Miller, V Mitchell, R Mitsuyasu, A Moanna, C Mogridge, F Moran, R Murphy, D Mushatt, R Nahass, D Nixon, S O'Brien, J Ojeda, P Okhuysen, M Olson, J Osterberger, W Owen, Sr. S Pablovich, S Patel, G Perez, G Pierone Jr., R Poblete, A Potter, E Preston, C Rappoport, N Regevik, M Reyelt, F. Rhame, L Riney, M Rodriguez-Barradas, M Rodriguez, Milagros Rodriguez, J Rodriguez, R Roland, C Rosmarin-DeStefano, W Rossen, J Rouff, M Saag, J Sampson, S Santiago, J Sarria, S Wirtz, U Schmidt, C Scott, A Sheridan, A Shin, S Shrader, G Simon, D Slowinski, K Smith, J Spotkov, C Sprague, D States, C Suh, J Sullivan, K Summers, B Sweeton, V Tan, T Tanner, E Tedaldi, Z Temesgen, D Thomas, M Thompson, C Tobin, N Toro, W Towner, K Upton, J Uy, S Valenti, C van der Horst, J Vita, J Voell, J Walker, T Walton, K Wason, V Watson, A Wellons, J Weise, M White, T Whitman, B Williams, N Williams, J Windham, M Witt, K Workowski, G Wortmann, T Wright, C Zelasky, B Zwickl.