setting priorities delivering best value managing scarcity: experience from tayside danny ruta
TRANSCRIPT

Setting Priorities
Delivering Best Value
Managing Scarcity: Experience from Tayside
Danny Ruta

The doctor-manager divide
‘In a resource allocation context, doctors (can be) caricatured as taking the role of patient advocate while managers take the corporate, strategic view. Delivery of efficient (and in the case of the NHS, equitable) health care requires doctors to take responsibility for resources and to consider the needs of populations while managers need to become more outcome and patient centred.’
Ruta, Mitton, Donaldson et al, BMJ 2005, in press

Programme Budgeting & Marginal Analysis (PBMA)
How resources are spent Costs and benefits of changes in spending Can operate at micro or macro level
PBMA asks five simple questions about resource
use

Programme Budgeting & Marginal Analysis (PBMA)
1. What are the total resources available for a programme?
2. On which services are these resources currently spent?
3. What services are candidates for receiving more or new resources (and what are the costs and potential benefits of putting resources into such growth areas)?

Programme Budgeting & Marginal Analysis (PBMA)
4. Can any existing services be provided as effectively, but with fewer resources, so releasing resources to fund items on the growth list?
5. If some growth areas still cannot be funded, are there any services which should receive fewer resources, or even be stopped, because greater benefit would be reached by funding the growth option as opposed to the existing service?
Questions 1&2 = the PB bit
Questions 3,4,5 = the MA bit

The ‘seven steps’ of PBMA
1. Determine the aim and scope of the exercise
2. Compile a programme budget (map of current activity and expenditure)
3. Form a marginal analysis advisory panel and stakeholder advisory groups
4. Determine locally relevant decision making criteria with input from decision makers and stakeholders

The ‘seven steps’ of PBMA
5. Advisory panel identifies options in terms of:
- Areas for service growth
- Areas for resource release through producing same level of output (or outcomes) but with less resources
- Areas for resource release through scaling back or stopping some services

The ‘seven steps’ of PBMA
6. Advisory panel makes recommendations in terms of:
- Funding growth areas with new resources
- Decisions to move resources released through increased productivity to areas of growth
- Trade-off decisions to move resources from one service to another if relative value is deemed greater
The ‘seven steps’ of PBMA
7. Validity checks with additional stakeholders and final decisions to inform budget planning process

1. Determine aim & scope of exercise
Example – Tayside Drugs & Alcohol
• Population < 500,000
• Dundee, Angus, Perth & Kinross councils
• 3 DAATs
• from NHS to LA led

1. Determine aim & scope of exercise
Example – Tayside Drugs & Alcohol
Aim:
“To examine current provision of drug and alcohol services across Tayside; and to propose opportunities for management, service and financial benefits or improvements.”

1. Determine aim & scope of exercise
Example – Tayside Drugs & Alcohol Scope:
• Covering only drugs and alcohol services specifically for people with drugs and alcohol problems;
• Covering services delivered by Community Planning partner organisations across Tayside;
• Not including those services that are not specifically targeted at people with drugs and alcohol problems

2. Compile Programme Budget
• Broad patterns expenditure & activity
• Clinically meaningful programme of services
• Raise questions about value for money
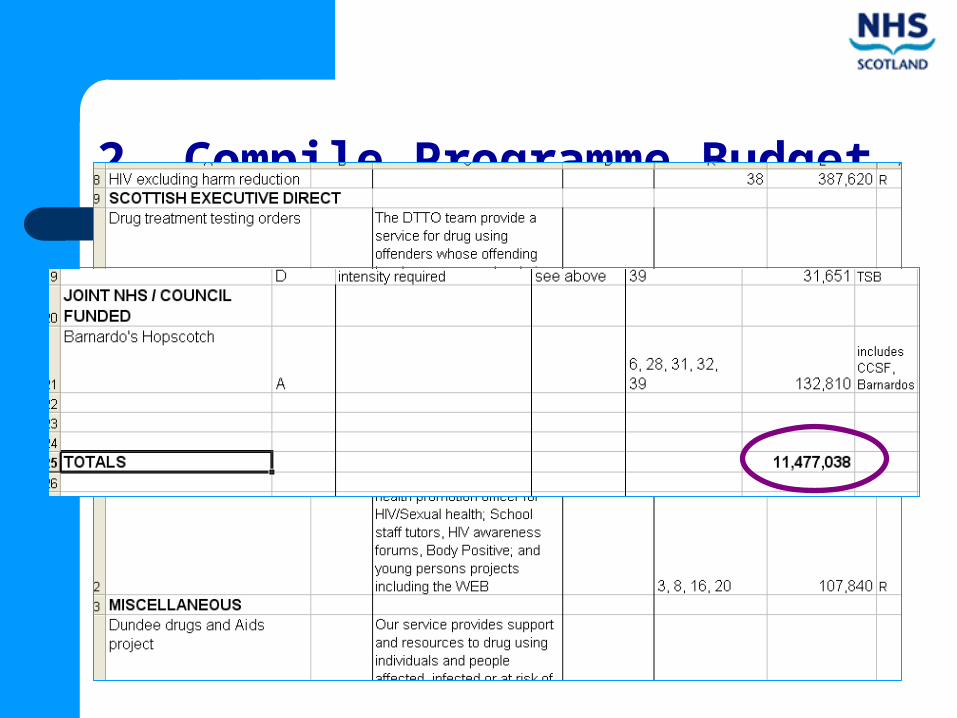
2. Compile Programme Budget
Example 1 – Tayside Drugs & Alcohol

3. Form advisory panel & stakeholder groups
• Responsibility for developing criteria
• Generating options for change
• Assessing marginal benefits

3. Form advisory panel & stakeholder groups
Example – Tayside Drugs & Alcohol
Advisory Panel
CEO P&K Council
3 DAAT Chairs
Trust Medical Director
Mental Health Commissioner
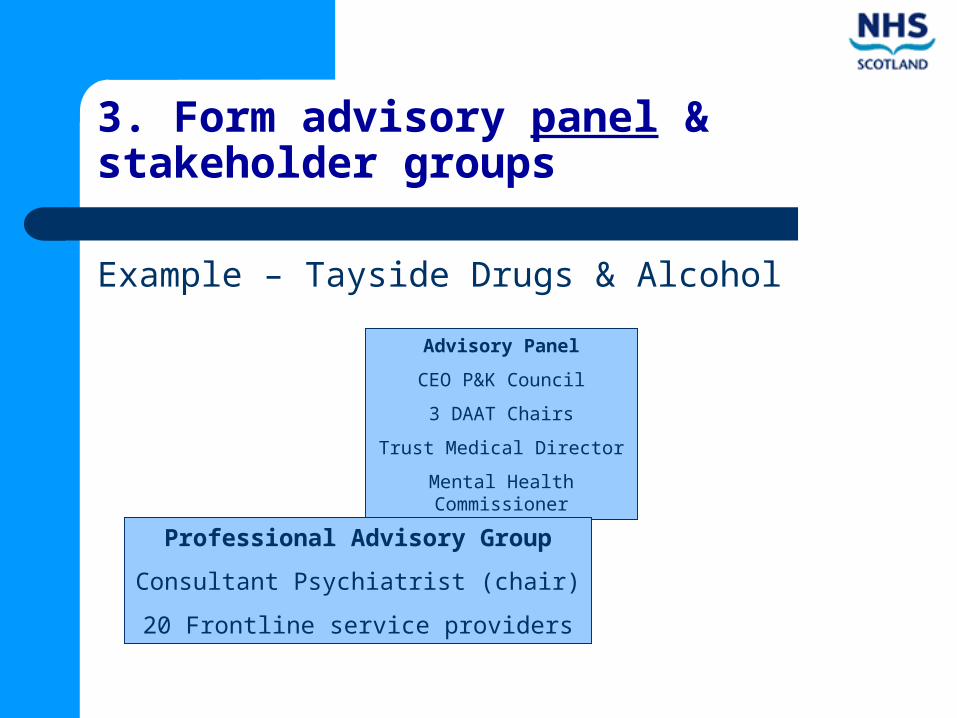
3. Form advisory panel & stakeholder groups
Example – Tayside Drugs & Alcohol
Advisory Panel
CEO P&K Council
3 DAAT Chairs
Trust Medical Director
Mental Health Commissioner
Professional Advisory Group
Consultant Psychiatrist (chair)
20 Frontline service providers

3. Form advisory panel & stakeholder groups
Example – Tayside Drugs & Alcohol
Advisory Panel
CEO P&K Council
3 DAAT Chairs
Trust Medical Director
Mental Health Commissioner
Professional Advisory Group
Consultant Psychiatrist (chair)
20 Frontline service providers
Scottish Drugs Forum
6 Service User Focus Groups

3. Form advisory panel & stakeholder groups
Example – Tayside Drugs & Alcohol
Advisory Panel
CEO P&K Council
3 DAAT Chairs
Trust Medical Director
Mental Health Commissioner
Professional Advisory Group
Consultant Psychiatrist (chair)
20 Frontline service providers
Scottish Drugs Forum
6 Service User Focus Groups
Project Team
Me
Psychiatrist
Nurse
3 DAAT Co-ordinators
Finance manager
Community pharmacist
4. Determine locally relevant decision making criteria
• Criteria to assess benefits gained/lost
• Relative weights for criteria importance

4. Determine locally relevant decision making criteria
• Quality & Length of Life
• Quality of Service
• Feasibility
• Policy & Strategy
Example – Tayside Drugs & Alcohol

4. Determine locally relevant decision making criteria
Example – Tayside Drugs & Alcohol

5. Advisory panel identify the options
• Areas for service growth;
• Areas for resource release through producing the same outcomes with fewer resources;
• Areas for resource release through scaling back or stopping services;
• Areas where growth and resource release occur simultaneously

Example – Tayside Drugs & Alcohol
5. Advisory panel identify the options
• Professional advisory group generated options
• Assessed options against Quality/length of life & Quality of service criteria
• Project team collated evidence

5. Advisory panel identify the options
• 23 Service Investment Candidates
Example 1 – Tayside Drugs & Alcohol

5. Advisory panel identify the options
• 23 Service Investment Candidates
• 31 Service Disinvestment Candidates
Example 1 – Tayside Drugs & Alcohol

6. Panel makes recommendations
Example – Tayside Drugs & Alcohol
Benefit-cost ratio = (weighted benefit x no. client beneficiaries) / cost

Example – Tayside Drugs & Alcohol
7. Validity Checks with additional stakeholders

Lessons from Tayside PBMA Study
It is feasible to apply PBMA in practice Potential to bridge doctor-manager divide Addresses root cause of problem of
managing scarcity – shared appreciation of opportunity cost (balance clinical autonomy & financial responsibility)

Lessons from Tayside
“A Scottish NHS without market competition but
with PBMA, result happiness. A Scottish NHS without a market
and without PBMA, result misery”