session 4 cv boot camp part 1 - ccrn certification and ... 4 cv boot camp part 1.pdfedema •...
TRANSCRIPT

Cardiovascular Boot Camp April 2009
www.cardionursing.com 1
CNEA 2009 1
Cardiovascular
Assessment
Presented By:
Karen Marzlin, BSN, RN, CCRN-CMC
2
Auscultatory Areas

Cardiovascular Boot Camp April 2009
www.cardionursing.com 2
3
The Cardiac Cycle
Systole and Diastole
4
Cardiac Diastole
(Atrial and Ventricular):
Early Passive Filling

Cardiovascular Boot Camp April 2009
www.cardionursing.com 3
5
Atrial Systole & Ventricular Diastole: Late Active Filling
Atrial Kick
6
Beginning Ventricular Systole:Isovolumic Contraction

Cardiovascular Boot Camp April 2009
www.cardionursing.com 4
7
Ventricular Systole:
Ejection
8
FIRST HEART SOUND

Cardiovascular Boot Camp April 2009
www.cardionursing.com 5
9
Basic Heart Sounds
S1
• Closure of the Mitral (M1) valve and the Tricuspid (T1)valve
• Beginning of Ventricular Systole and Atrial Diastole
• Isovolumic contraction
10
Basic Heart Sounds
S1
• Location: Mitral area – at the hearts apex
• Intensity: Directly related to force of contraction
• Duration: Short
• Quality: Dull
• Pitch: High

Cardiovascular Boot Camp April 2009
www.cardionursing.com 6
11
SECOND HEART
SOUND
12
Basic Heart Sounds
S2
• Closure of Aortic (A2) Valve and Pulmonic (P2) Valve
• End of Ventricular Systole Beginning of Ventricular Diastole

Cardiovascular Boot Camp April 2009
www.cardionursing.com 7
13
Basic Heart Sounds
S2• Location: Pulmonic area
• Intensity: Directly related
to closing pressure in
the aorta and pulmonary
artery
• Duration: Shorter than
S1
• Quality: Booming
• Pitch: High
14
Third and Fourth Heart Sounds
S3 and S4
• Ventricular diastolic filling sounds
• Low frequency sounds
• Produced by ventricular filling rather than valve closure
• Normal in children and young adults

Cardiovascular Boot Camp April 2009
www.cardionursing.com 8
15
THIRD HEART SOUND
16
S3
Ventricular Gallop
• Ventricular Gallop
• Early diastole
• Caused by increased diastolic pressure
Cardiovascular Boot Camp April 2009
www.cardionursing.com 9
17
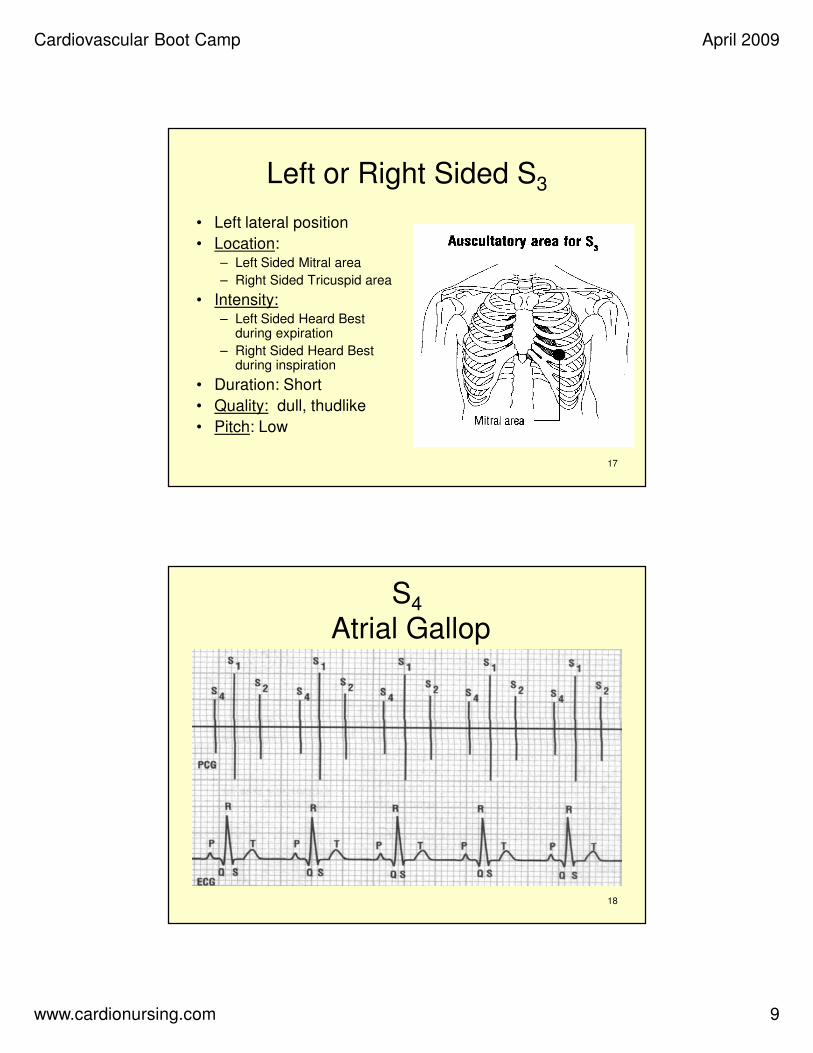
Left or Right Sided S3
• Left lateral position
• Location: – Left Sided Mitral area
– Right Sided Tricuspid area
• Intensity:– Left Sided Heard Best
during expiration
– Right Sided Heard Best during inspiration
• Duration: Short
• Quality: dull, thudlike
• Pitch: Low
18
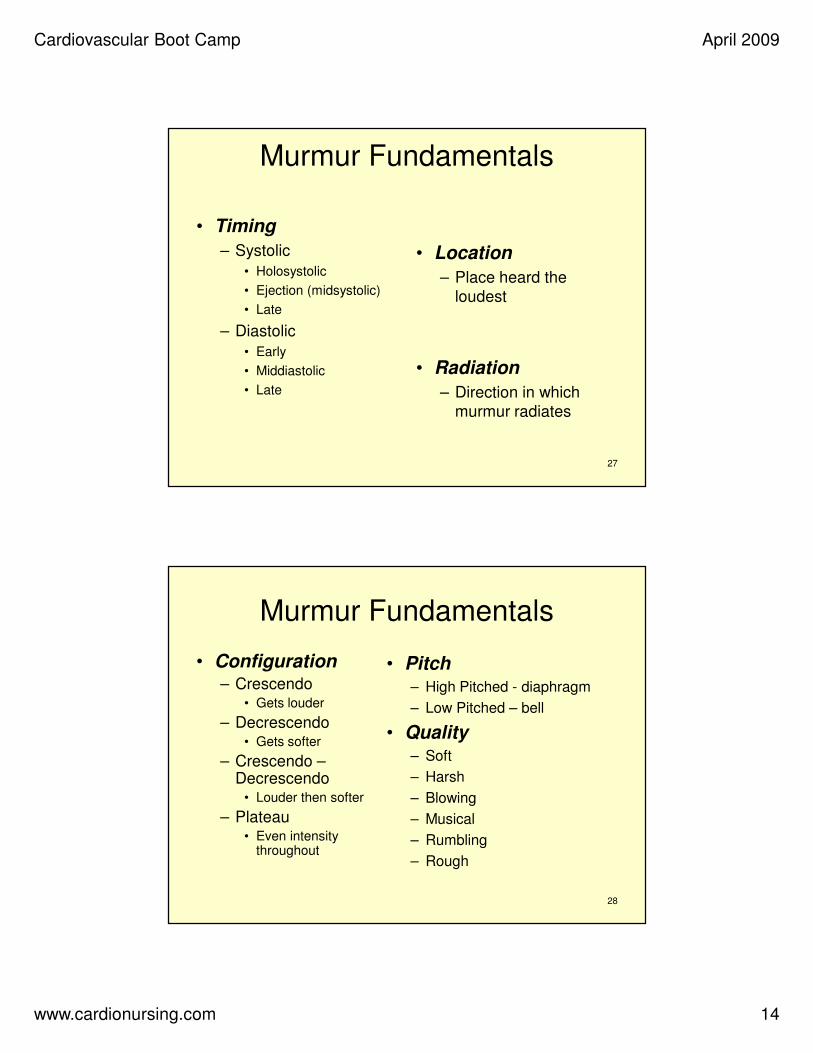
S4
Atrial Gallop

Cardiovascular Boot Camp April 2009
www.cardionursing.com 10
19
S4
Atrial Gallop
• Late diastole
• Caused by atrial contraction and the propulsion of blood into a noncompliant ventricle
20
Left or Right Sided S4
• Left Lateral position
• Location: – Left Sided Mitral Area
– Right Sided Tricuspid area
• Intensity: – Left Sided Louder on
expiration
– Right Sided Louder on inspiration
• Duration: Short
• Quality: Thudlike
• Pitch: Low

Cardiovascular Boot Camp April 2009
www.cardionursing.com 11
21
Summation Gallop
Combination of S3 and S4
22
MURMURS

Cardiovascular Boot Camp April 2009
www.cardionursing.com 12
23
Murmur Fundamentals
Turbulence
• Murmur: If turbulence is intracardiac
• Bruit: If turbulence is extracardiac
24
Murmur Fundamentals
Causes of Turbulence
Forward flow through a stenotic valve
Backward flow through an incompetent
valve

Cardiovascular Boot Camp April 2009
www.cardionursing.com 13
25
Murmur Fundamentals
Causes of Turbulence
• Flow through a septal
defect or an AV fistula
• Flow into a dilated chamber or a portion
of a vessel
26
Murmur Fundamentals
• Stenotic Murmurs
– Valve does not open appropriately
– Heard during the part of the cardiac cycle when the valve is open
• Regurgitant Murmurs
– Valve does not close appropriately
– Heard during the part of the cardiac cycle when the valve is to be closed
Cardiovascular Boot Camp April 2009
www.cardionursing.com 14
27
Murmur Fundamentals
• Timing
– Systolic
• Holosystolic
• Ejection (midsystolic)
• Late
– Diastolic
• Early
• Middiastolic
• Late
• Location
– Place heard the
loudest
• Radiation
– Direction in which
murmur radiates
28
Murmur Fundamentals
• Configuration– Crescendo
• Gets louder
– Decrescendo• Gets softer
– Crescendo –Decrescendo
• Louder then softer
– Plateau• Even intensity
throughout
• Pitch– High Pitched - diaphragm
– Low Pitched – bell
• Quality– Soft
– Harsh
– Blowing
– Musical
– Rumbling
– Rough

Cardiovascular Boot Camp April 2009
www.cardionursing.com 15
29
Systolic Murmurs
• Tricuspid and Mitral Valve Closed
– Tricuspid
Regurgitation
– Mitral Regurgitation
• Pulmonic and Aortic Valve Open
– Pulmonic Stenosis
– Aortic Stenosis
30
Aortic Stenosis
Systolic Ejection Murmur• Timing: Midsystolic
• Location: Best heard
over aortic area
• Radiation: Toward right
side of neck
• Configuration:
Crescendo-decrescendo
• Pitch: Medium to high
• Quality: Harsh

Cardiovascular Boot Camp April 2009
www.cardionursing.com 16
31
Pulmonic StenosisSystolic Ejection Murmur
• Timing: Midsystolic
• Location: Best heard over pulmonic area
• Radiation: Left neck of left shoulder
• Configuration:
Crescendo-decrescendo
• Pitch: Medium
• Quality: Harsh
32
Systolic Murmurs
Mitral Regurgitation• Timing: Holosystolic
• Location: Mitral area
• Radiation: To the left axilla
• Configuration:Plateau
• Pitch: High
• Quality: Blowing, harsh or musical

Cardiovascular Boot Camp April 2009
www.cardionursing.com 17
33
Systolic Murmurs
Tricuspid Regurgitation• Timing: Holosystolic
• Location: Tricuspid area
• Radiation: To the right of
sternum
• Configuration: Plateau
• Pitch: High
• Quality: Scratchy or
blowing
34
Diastolic Murmurs
• Diastolic regurgitant murmurs
– Retrograde flow across an incompetent semilunar valve
• Diastolic filling murmurs
– Forward flow across stenotic or obstructed AV valves
Cardiovascular Boot Camp April 2009
www.cardionursing.com 18
35
Diastolic Murmurs
• Tricuspid and Mitral Valves Open
– Tricuspid Stenosis
– Mitral Stenosis
• Pulmonic and Aortic Valves Close
– Pulmonic
Regurgitation
– Aortic Regurgitation
36
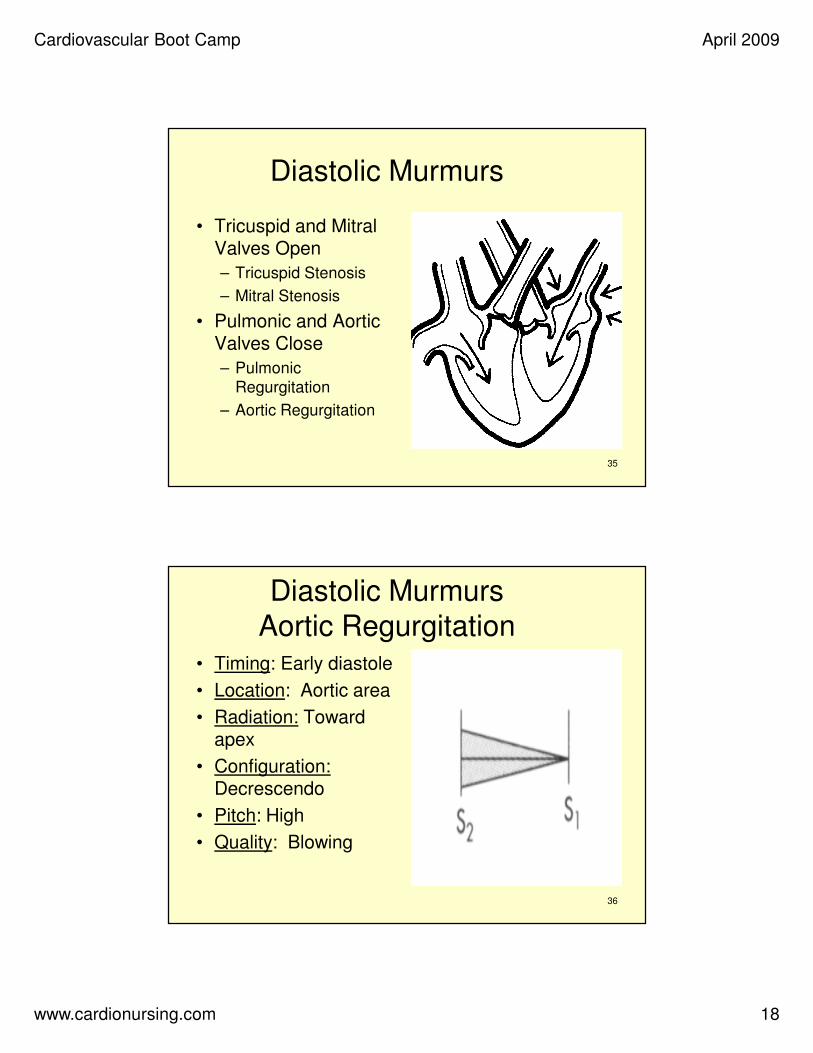
Diastolic Murmurs
Aortic Regurgitation• Timing: Early diastole
• Location: Aortic area
• Radiation: Toward apex
• Configuration:Decrescendo
• Pitch: High
• Quality: Blowing
Cardiovascular Boot Camp April 2009
www.cardionursing.com 19
37
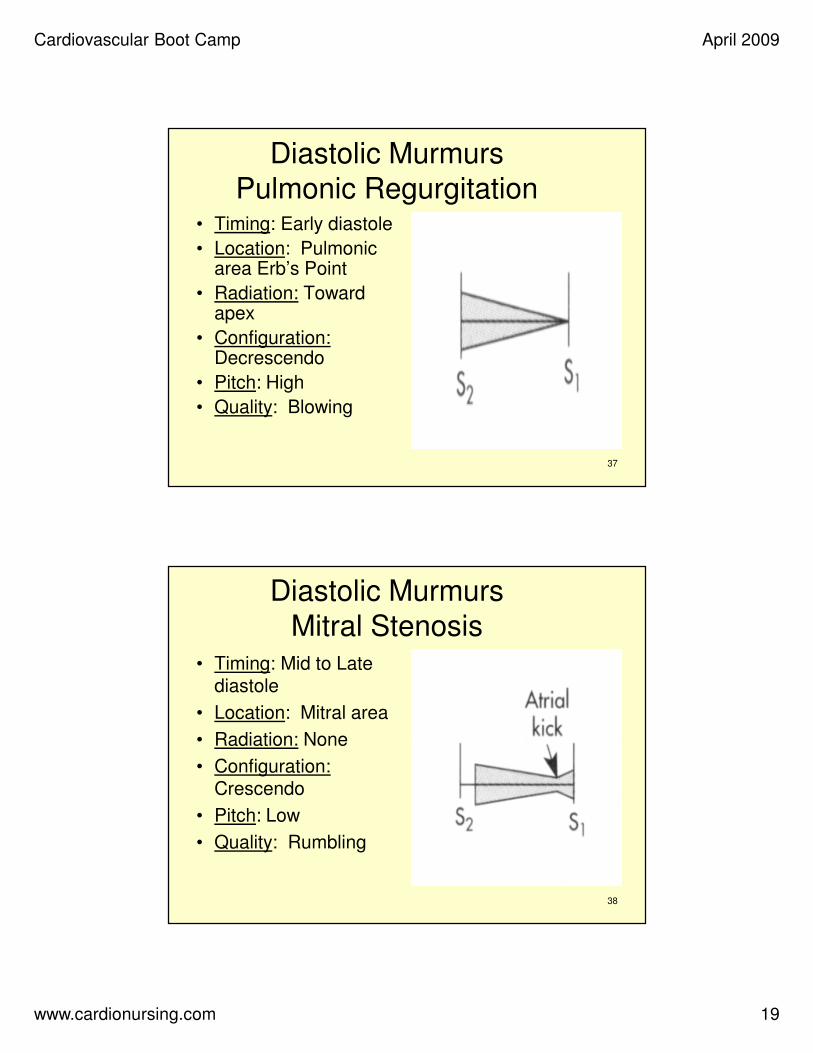
Diastolic Murmurs
Pulmonic Regurgitation• Timing: Early diastole
• Location: Pulmonic area Erb’s Point
• Radiation: Toward apex
• Configuration:Decrescendo
• Pitch: High
• Quality: Blowing
38
Diastolic Murmurs
Mitral Stenosis• Timing: Mid to Late
diastole
• Location: Mitral area
• Radiation: None
• Configuration:Crescendo
• Pitch: Low
• Quality: Rumbling

Cardiovascular Boot Camp April 2009
www.cardionursing.com 20
39
Diastolic Murmur
Tricuspid Stenosis
• Timing: Mid to Late diastole
• Location: Tricuspid area
• Radiation: None
• Configuration:Decrescendo
• Pitch: Low
• Quality: Rumbling
• Increases during inspiration and decreases during expiration
40
Other Sounds
Pericardial Friction Rub
• Timing: Systolic, Early diastolic and late diastolic
• Location: Tricuspid area and Xyphoid area
• Radiation: None
• Configuration: Plateau
• May get louder during inspiration
• Pitch: High
• Quality: Grating, scratching

Cardiovascular Boot Camp April 2009
www.cardionursing.com 21
41
Other SoundsVentricular Septal Defect or
Rupture• Timing: Continuous
• Location: 3-4 LSB
• Radiation: Widely throughout the precordium
• Configuration: Plateau
• Pitch: High
• Quality: Harsh
42
Other Sounds
• Papillary Muscle Rupture
– Same as Mitral Regurgitation

Cardiovascular Boot Camp April 2009
www.cardionursing.com 22
43
REMEMBER:
The most important part of
the stethoscope is the part
between the ear pieces.
44
Other Assessment Tools

Cardiovascular Boot Camp April 2009
www.cardionursing.com 23
45
Blood Pressure
• Definitions:– BP = CO X SVR
– Systolic: Maximum pressure when blood is expelled from the left ventricle
– Diastolic:Measures rate of flow of ejected blood and vessel elasticity
– Pulse Pressure: Difference between systolic and diastolic pressure
46
Cardiac Assessment
• Blood Pressure
– Variation of up to 15mm Hg between arms is
normal
– BP in legs - 10 mm Hg higher than arms
– Narrowed pulse pressure – vasoconstriction
• Innervation of sympathetic nervous system – Hypovolemic shock
– Widened pulse pressure – vasodilation
• Excessive vasodilatory mediator release– Septic shock

Cardiovascular Boot Camp April 2009
www.cardionursing.com 24
47
JVP (Jugular Venous Pressure)
• Reflects volume and pressure in right side
of heart
• Visual inspection
• HOB 30 -45 degree angle
– 45 degree angle will cause venous pulsation to rise 1 to 3 cm above the manubrium
48
Measuring JVD
• Raise HOB until pulsation in internal jugular seen (usually 30 – 45 degrees)
– Use targeted light
– Use centimeter ruler
• Measure distance from angle of Louis (Manubriosternal joint)
to top column of blood
• Draw imaginary horizontal line from column to sternal angle

Cardiovascular Boot Camp April 2009
www.cardionursing.com 25
49
JVD (Jugular Venous
Distension)• Normal JVD level is 3 cm above the
sternal angle
• Sternal angle is 5cm above right atrium
• JVD of 3 cm + 5cm = estimated CVP of 8cm
• Estimated CVP> 8 cm– Increased blood volume
– Usually RV failure• Tricuspid valve regurgitation
• Pulmonary hypertension
50
Tips to Take Away for JVD Assessment
• If unable to accurately assess
– Lie patient flat to visualize and then raise HOB
– If venous congestion is expected may need to sit or stand patient to see top of column
Cardiovascular Boot Camp April 2009
www.cardionursing.com 26
51
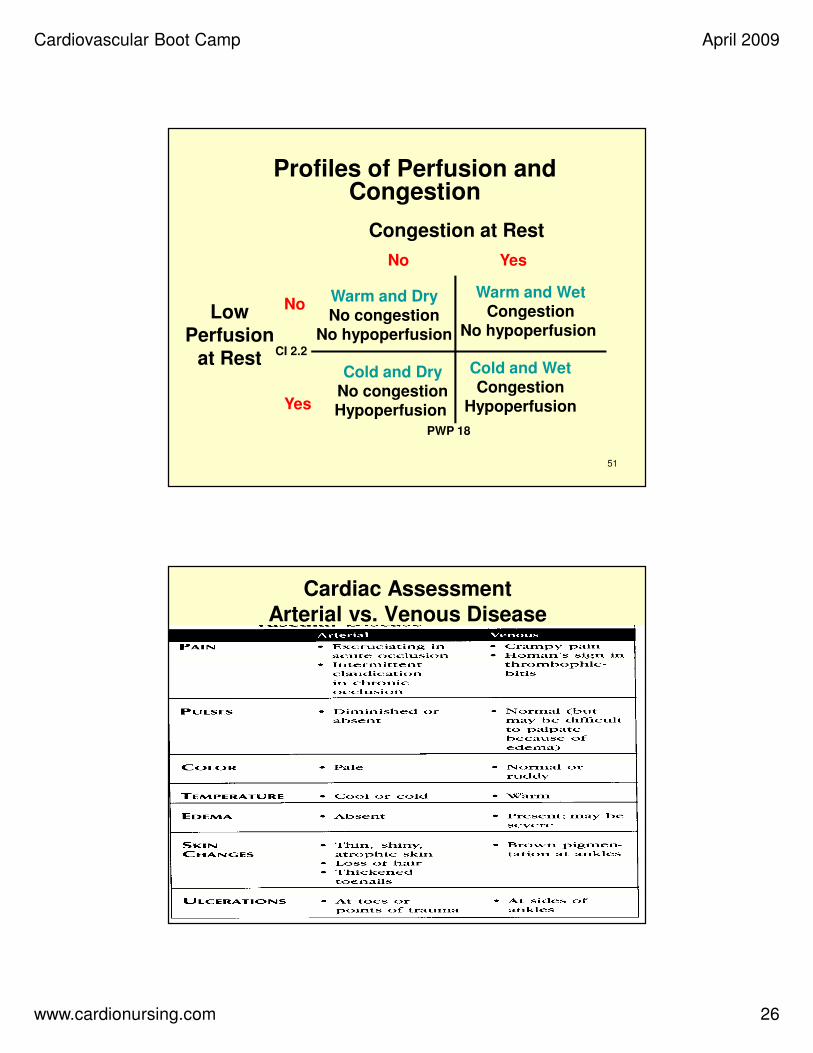
Profiles of Perfusion and Congestion
YesNo
Warm and Dry
No congestion
No hypoperfusion
Warm and Wet
Congestion
No hypoperfusion
Cold and WetCongestion
Hypoperfusion
Cold and DryNo congestionHypoperfusion
Congestion at Rest
Low Perfusion
at Rest
No
Yes
PWP 18
CI 2.2
52
Cardiac Assessment
Arterial vs. Venous Disease

Cardiovascular Boot Camp April 2009
www.cardionursing.com 27
53
Edema
• Evaluated on a 4-point scale.
• 0 = None present.
• 1+ = 0 to 1⁄4 inch Trace.
• 2+ = 1⁄4 to 1⁄2 inch Mild.
• 3+ = 1⁄2 to 1 inch Moderate.
• 4+ = > than 1 inch Severe.
• Described as pitting or non-pitting.
• Anasarca: generalized edema.
54
Pulses
• 4 point scale (0-3)
• 0 = absent
• 1+ = Palpable but thready and weak,
easily obliterated
• 2+ = Normal, easily identified, not easily
obliterated
• 3+ = Full, bounding, cannot obliterate

Cardiovascular Boot Camp April 2009
www.cardionursing.com 28
55
Central Cyanosis
• Occurs when more than 5 grams/dL of hemoglobin is deoxygenated
• Results in a bluish or steel-gray discoloration of the skin and mucous membranes– Bluish or steel-gray discoloration of the lips can be from central
or peripheral cyanosis
– Oral mucosa or the tongue may be better tools for assessment of central cyanosis
• Usually not seen until oxygen saturation drops to between 73% to 78%
• Absence of cyanosis does not exclude hypoxemia
56
Peripheral Cyanosis
• Caused by peripheral vasoconstriction
and decreased local blood flow
• May occur with or without central
cyanosis (i.e., with or without hypoxemia)
Usually observed in the nailbeds of the
hands or feet, the earlobes or nose
• Should improve with warming

Cardiovascular Boot Camp April 2009
www.cardionursing.com 29
57
Pulsus Paradoxus• To measure the pulsus paradoxus, patients are often
placed in a semirecumbent position; respirations should be normal. The blood pressure cuff is inflated to at least 20 mm Hg above the systolic pressure and slowly deflated until the first Korotkoff sounds are heard only during expiration. At this pressure reading, if the cuff is not further deflated and a pulsus paradoxus is present, the first Korotkoff sound is not audible during inspiration. As the cuff is further deflated, the point at which the first Korotkoff sound is audible during both inspiration and expiration is recorded. If the difference between the first and second measurement is greater than 12 mm Hg, an abnormal pulsus paradoxus is present.
(Yarlagadda, Chakri, 2005 Cardiac Tamponade. Retrieved 3-22-06 from www.emedicine.com)
Risk Assessment
58

Cardiovascular Boot Camp April 2009
www.cardionursing.com 30
59
Risk Assessment in UA / NSTEMI
• TIMI Risk Score
– Age > 65
– 3 or > risk factors for CAD
– Prior 50% or > stenosis
– ST deviation on ECG
– 2 or > anginal events in
previous 24 hours
– Use of ASA in prior 7 days
– Elevated cardiac biomarkers
• GRACE
– Older age
– Killip class
– Systolic BP
– Cardiac arrest during
presentation
– Serum creatinine
– Positive initial cardiac
markers
– HR
Stroke Risk Assessment
• Congestive Heart Failure
• Hypertension
• Age > 75
• Diabetes
• Stroke TIA
60

Cardiovascular Boot Camp April 2009
www.cardionursing.com 31
61
Assessment Integration For Cardiac Emergencies
62
Assessment Considerations for Emergencies
• Tamponade
– Beck’s triad
– Pulses Paradoxus
• Pulmonary Embolus
– Right axis deviation
– T wave inversion
– Respiratory Alkalosis
• Acute Aortic Dissection
– Diastolic murmur
– Bilateral BPs
– 4 extremity pulses
– Inferior MI
• Papillary Muscle Rupture
– Holosystolic murmur
– Acute pulmonary edema
• VSD
– Holosysytolic murmur

Cardiovascular Boot Camp April 2009
www.cardionursing.com 32
63
Thanks for Attending Cardiovascular Boot Camp
You may contact us at www.cardionursing.com
64