serum levels of omentin, chemerin and adipsin in patients with biopsy-proven nonalcoholic fatty...
TRANSCRIPT

Scandinavian Journal of Gastroenterology, 2011; 46: 91–97
ORIGINAL ARTICLE
Serum levels of omentin, chemerin and adipsin in patients withbiopsy-proven nonalcoholic fatty liver disease
YUSUF YILMAZ1, OYA YONAL1, RAMAZAN KURT1, YESIM OZEN ALAHDAB1,FATIH EREN2, OSMAN OZDOGAN1, CIGDEM ATAIZI CELIKEL3, NESE IMERYUZ1,CEM KALAYCI1 & EROL AVSAR1
1Department of Gastroenterology, Marmara University School of Medicine, Altunizade, Istanbul, Turkey, 2Institute ofGastroenterology, Marmara University, Maltepe, Istanbul, Turkey, and 3Department of Pathology, Marmara UniversitySchool of Medicine, Altunizade, Istanbul, Turkey
AbstractObjective.The novel adipokines omentin, chemerin, and adipsin are associated with insulin resistance and the components ofthe metabolic syndrome. We assayed circulating levels of these molecules and examined their association with clinical,biochemical, and histological phenotypes in patients with nonalcoholic fatty liver disease (NAFLD).Material andmethods.Serum levels of omentin, chemerin, and adipsin were assayed by enzyme-linked immunosorbent assay in 99 patients withbiopsy-proven NAFLD and 75 control subjects. We analyzed associations between adipokines and the characteristics ofpatients with NAFLD using multivariable linear regression models.Results.Adipsin levels did not differ between patients andcontrols, whereas both omentin and chemerin levels were significantly higher in patients with biopsy-proven NAFLD than incontrols (both p values <0.001). Serum omentin levels were significantly associated with C-reactive protein (r = 0.29, p < 0.01)and the degree of hepatocyte ballooning (r = 0.27, p < 0.01), whereas chemerin showed a modest association with liver fibrosis(r = 0.22, p = 0.04). After stepwise linear regression analysis adjusting for potential confounders, serum omentin levels retainedtheir independent significance as a predictor of hepatocyte ballooning in patients with NAFLD (b = 1.42; t = 2.79, p < 0.01).Conclusions. Our results suggest that serum omentin levels are raised in patients with NAFLD regardless of potentialconfounders and represent an independent predictor of hepatocyte ballooning.
Key Words: Adipokines, enzyme-linked immunosorbent assay, liver fibrosis, nonalcoholic fatty liver disease
Introduction
Nonalcoholic fatty liver disease (NAFLD), a hepaticmanifestation of the metabolic syndrome (MetS) [1],is the most common liver disease in developed coun-tries and a major cause of abnormal liver functiontests in hepatology practice [2]. The term NAFLD isused to describe a wide spectrum of fatty liver changesranging from simple steatosis to nonalcoholic steato-hepatitis (NASH) [3]. Accumulating research sug-gests that NAFLD is independently associated withinsulin resistance [4]. In addition, insulin resistancemay predict the severity of liver damage or fatty
infiltration in patients with NAFLD [5]. These obser-vations indicate that either insulin resistance plays arole in the pathogenesis and progression of liverdamage, or the two phenomena have a commonpathogenic mechanism [6].Adipokines are fat-derived hormones and cyto-
kines that play a central role in insulin homeostasis,as well as immunity, and are fundamental to thepathogenesis of the MetS [7,8]. Numerous reportshave demonstrated altered levels of classic adipo-kines such as leptin, adiponectin, and resistin inpatients with NAFLD [9–11]. The interplay of var-ious adipokines may play a crucial role in the
Correspondence: Yusuf Yilmaz, Department of Gastroenterology, Marmara University School of Medicine, Istanbul 34662, Turkey. Tel: +90 533 4403995.Fax: +90 216 6886681. E-mail: [email protected]
(Received 3 August 2010; accepted 10 August 2010)
ISSN 0036-5521 print/ISSN 1502-7708 online � 2011 Informa HealthcareDOI: 10.3109/00365521.2010.516452
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.

progression from fatty infiltration to inflammationand fibrosis, and the potential usefulness of adipo-kines as noninvasive diagnostic tests in patients withNASH has generated great interest [12]. In addition,the altered concentrations of adipokines in patientswith metabolic liver disease suggest that circu-lating levels of these molecules might serve asuseful biomarkers in the entire histological spectrumof NAFLD [10,11]. Several novel adipokines havebeen recently identified. Omentin is a novel 34-kDaadipokine that is mainly expressed in the vascularfraction of visceral fat depots and is barely detectablein subcutaneous adipose tissue and mature adipo-cytes [13]. This polypeptide hormone increases insu-lin sensitivity in human adipocytes and is closelyassociated with obesity and insulin homeostasis [14].Interestingly, circulating omentin levels have beeninversely associated with obesity and insulin resis-tance [15]. Chemerin is an adipocyte-secreted factorplaying a crucial role in adipocyte differentiation andinsulin signaling [16]. Recently, Kukla et al. [17]have shown that serum chemerin levels are higher inpatients with NASH and positively associated withhepatocyte ballooning degeneration, total choles-terol, and diastolic blood pressure. In addition,Sell et al. [18] reported that chemerin levels areelevated in obese patients with a significant activityscore for NAFLD, portal inflammation, fibrosis, andfibroinflammation. Adipsin, also known as adipocytecomplement factor D, is the rate-limiting enzyme inthe alternative pathway of complement activa-tion [19]. Adipsin, together with other componentsof both the classical and alternative complementcascade, is primarily expressed by adipocytes inhuman subjects and is currently considered an adi-pokine [20]. The high expression of adipsin in vis-ceral adipose tissue suggests that this molecule maycontribute to the metabolic complications associatedwith increased visceral fat mass [21].In the present study, we assayed circulating levels
of omentin, chemerin, and adipsin and examinedtheir association with clinical, biochemical, and his-tological phenotypes in patients with histology-provenNAFLD.
Material and methods
Study participants
This observational case–control study consists of99 patients with NAFLD (50 males and 49 females,mean age, 48 ± 8 years) and 75 healthy subjects(37 males and 38 females, mean age, 48 ± 7 years).The two groups were comparable in age and sex.
Patients with NAFLD were consecutively seen atour hospital-based specialized outpatient clinicsover the past 12 months. All showed ultrasonographicevidence of steatosis grade 1 or higher. Patients withviral hepatitis, hemochromatosis, Wilson’s disease,autoimmune hepatitis, primary biliary cirrhosis,sclerosing cholangitis, biliary obstruction, alpha-1antitrypsin deficiency, ischemic cardiac or cerebro-vascular disease, impaired renal function or malig-nancies were carefully excluded from the presentstudy. Subjects using estrogens, amiodarone, ster-oids, tamoxifen, and lipid lowering agents were noteligible for this study. Patients with daily alcoholintake exceeding 20 g/day or previous abdominalsurgery were also excluded. A total of 75 healthyage- and sex-matched volunteers served as controls.All subjects included in the control group were judgedto be in good health, with normal results on liverfunction tests and confirmed as having normal liver byultrasound. Subjects with a consumption of alcohol>20 g/day or who were taking any medication were notincluded in the control group. All patients and con-trols were of Turkish descent.The Ethics Committee of the Marmara University
School of Medicine approved this study and all par-ticipants provided written informed consent prior toparticipation.
Clinical and biochemical characterization
All subjects underwent physical examination,anthropometric measurements, and biochemicalscreening. Body mass index (BMI) was calculatedfrom measurements of height and weight. Diabetesmellitus was diagnosed according to American Dia-betes Association’s (ADA) criteria [22]. The MetSwas diagnosed using the Third Adult TreatmentPanel (ATP III) criteria [23]. The estimate ofinsulin resistance was calculated using the homeosta-sis model of insulin resistance (HOMA-IR) index,with the following formula: insulin resistance = fastingplasma insulin (in microunits per milliliter) � fastingplasma glucose (in millimoles per liter)/22.5. Bloodpressure was measured using a mercury sphygmoma-nometer in a quiet room after ‡10-min rest. Korotkoff1 and 5 were taken for systolic and diastolic bloodpressures, respectively. Routine blood chemistry anal-yses were performed at the central laboratory ofclinical chemistry of our hospital. Serum high-sensitivity C-reactive protein (hs-CRP) levels weremeasured in duplicate, random order, and in ablinded fashion using a commercially availablemethod (Dade Behring, Marburg, Germany). Theintra- and interassay coefficients of variation for
92 Y. Yilmaz et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.

hs-CRP were 4.6% and 6.1%, respectively, and thelower detection limit was 0.19 mg/dl.
Liver histology
Ultrasonography-guided liver biopsies were per-formed under conscious sedation using a 16-gaugeHepafix needle. All biopsy specimens were placed informalin solution for fixation and embedded in par-affin blocks. Serial sections (sectioned at 4 mm inter-vals) were stained with hematoxylin–eosin, Masson’strichrome. An experienced pathologist blinded toclinical data scored the liver biopsies according tothe National Institute of Diabetes and Digestive andKidney Diseases (NIDDK) NASH Clinical ResearchNetwork scoring system [24]. Steatosis was scoredfrom 0 to 3 with a four grades scoring system fromS0 to S3: S0, no steatosis or <5%; S1, 5–33%; S2,33–66%; S3, >66%. Lobular inflammation wasgraded as follows: stage 0, no foci; stage 1, <2 fociper 200� field; stage 2, 2–4 foci per 200� field; stage3, >4 foci per 200� field. Ballooning degeneration ofliver cells was evaluated as: grade 0, absent; grade 1,few cells; grade 2, many cells. The histological NASHscore was defined as the unweighted sum of the scoresfor steatosis (0–3), lobular inflammation (0–3), andballooning (0–2); thus ranging from 0 to 8. Cases withscores of 0–2 were considered as having simple stea-tosis; on the other hand, cases with scores of 5 orgreater were diagnosed as definitive NASH. Caseswith activity scores of 3 and 4 were considered asborderline NASH [24]. Fibrosis was staged as fol-lows: stage 0, no fibrosis; stage 1, perisinusoidal orperiportal fibrosis with three different patterns: 1A,mild, zone 3, perisinusoidal; 1B, moderate, zone 3,perisinusoidal fibrosis; and 1C portal/periportal fibro-sis; stage 2, perisinusoidal and portal/periportal fibro-sis; stage 3, bridging fibrosis; and stage 4, cirrhosis.
Measurement of serum omentin, chemerin, and adipsin
All blood samples were collected from an antecubitalvein between 8:00 and 9.00 a.m. after an overnightfasting. Samples were centrifuged at 2500g for 10 minand serum aliquots were stored at �80�C until imme-diately before analysis. Serum omentin levels weredetermined using a commercially available enzymeimmunoassay kit (Alexis Biochemicals, San Diego,CA, USA) according to the manufacturer’s protocol.The minimum detection limit was 0.4 ng/ml.Serum chemerin was assayed using a quantitativeenzyme immunoassay kit (Biovendor, Modrice,Czech Republic). The minimum detection limit
was 0.13 ng/ml. Adipsin was quantified with theapelin-36 enzyme-linked immunosorbent assay(R&D Systems, Inc., Minneapolis, MN, USA)according to the manufacturer’s instructions. Theminimal detectable concentration was 0.013 ng/ml.All measurements were performed in duplicate,and the results were averaged. For all assays, theintra- and interassay coefficients of variation were<9% and <12%, respectively. These assays were per-formed by an investigator blinded to the sources of thesamples. Each sample was analyzed in duplicate, andthe mean value of the two measures was used for theanalyses.
Data analysis
The Kolmogorov–Smirnov test was performed in allcontinuous variables to define the presence of nor-mality. Gaussian variables are expressed as mean ±standard deviation (SD), skewed data are reported asmedians and interquartile ranges, and categoricalvariables are expressed as counts. Skewed variableswere logarithmically transformed to improve normal-ity prior to statistical analysis and then back-transformed to their natural units for presentationin the text and tables. The Student’s t-test wasused to evaluate differences between the two studygroups in normally distributed continuous variables.When normality was not confirmed, the Mann–Whitney U test was used. Correlations among thestudy variables were tested by the Spearman’s corre-lation coefficient. Multivariable stepwise linearregression analyses were performed to identify inde-pendent predictors of the severity of histologicalfeatures of NAFLD (i.e. steatosis, lobular inflamma-tion, hepatocye ballooning, and liver fibrosis); thecovariates included in these models were omentin,chemerin, and adipsin; all variables are listedin Table I. All statistical analyses were performedusing SPSS version 11.0 for Windows (SPSS, Inc.,Chicago, IL, USA). A value of p < 0.01 (two-sided)was considered as statistically significant to reduce thelikelihood of type I error [25].
Results
Table I presents the general characteristics of subjectswith and without NAFLD. The two study groups didnot differ in terms of age, sex, systolic and diastolicblood pressure, and high-density lipoprotein choles-terol. Between-group comparison analysis identified anumber of variables to be different in patients withhistology-proven NAFLD compared with controls
Novel adipokines in NAFLD 93
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.
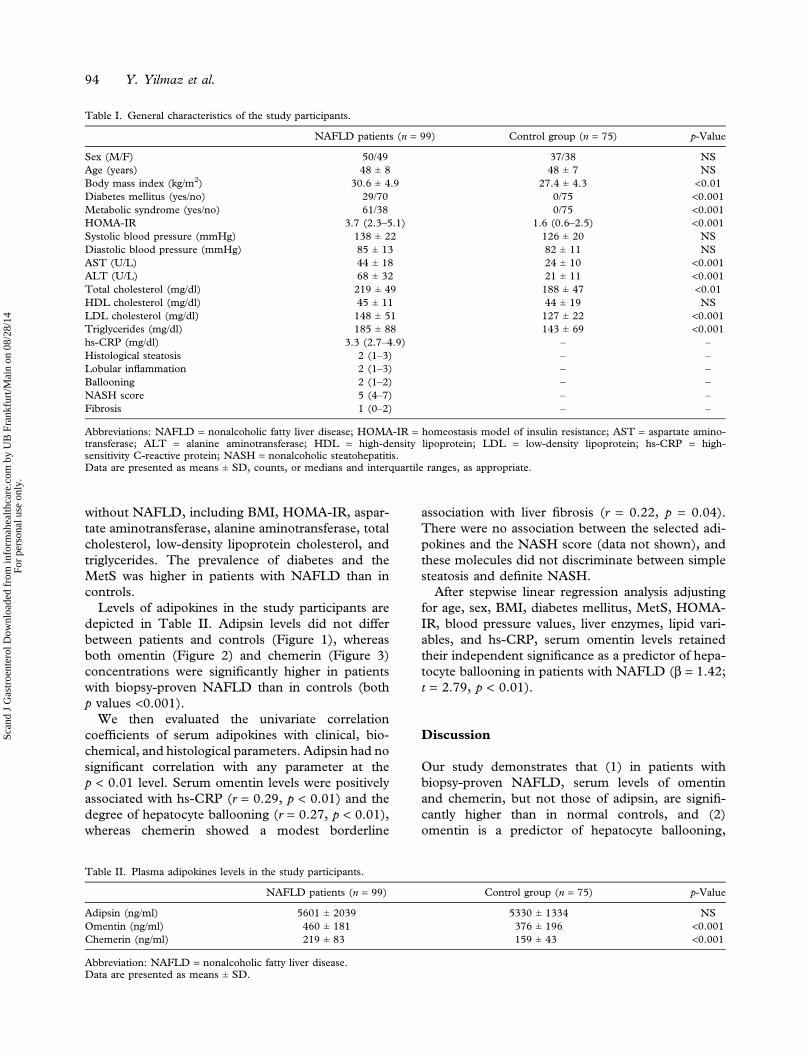
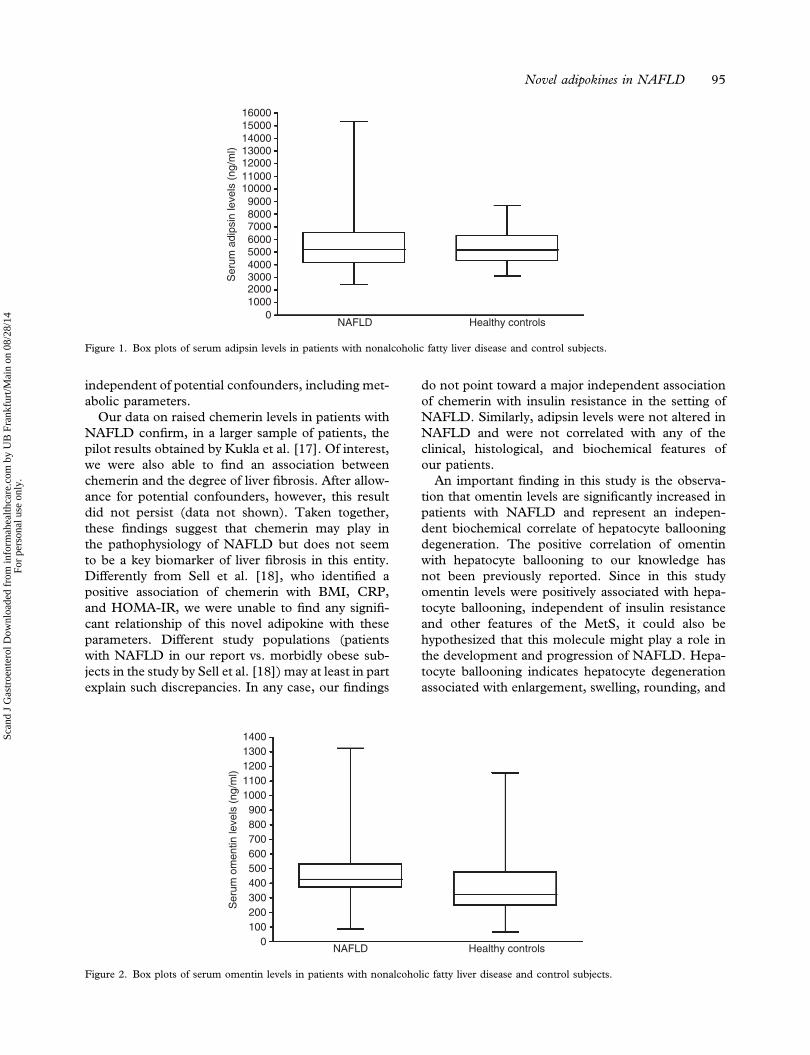
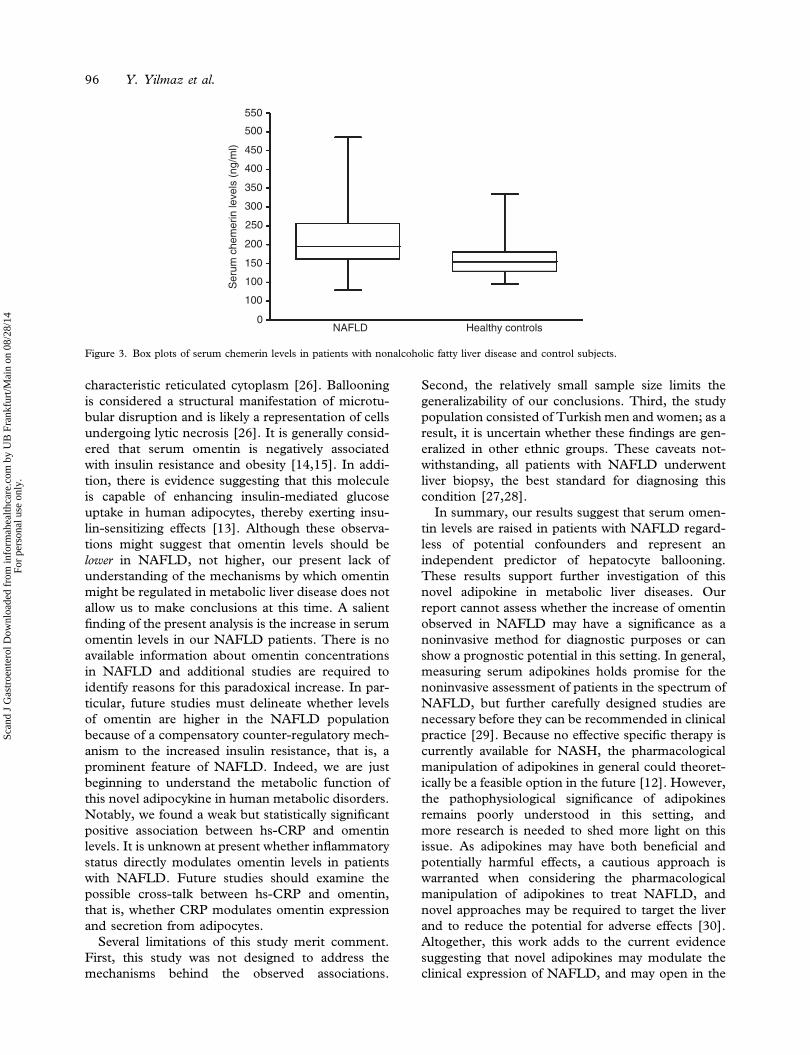
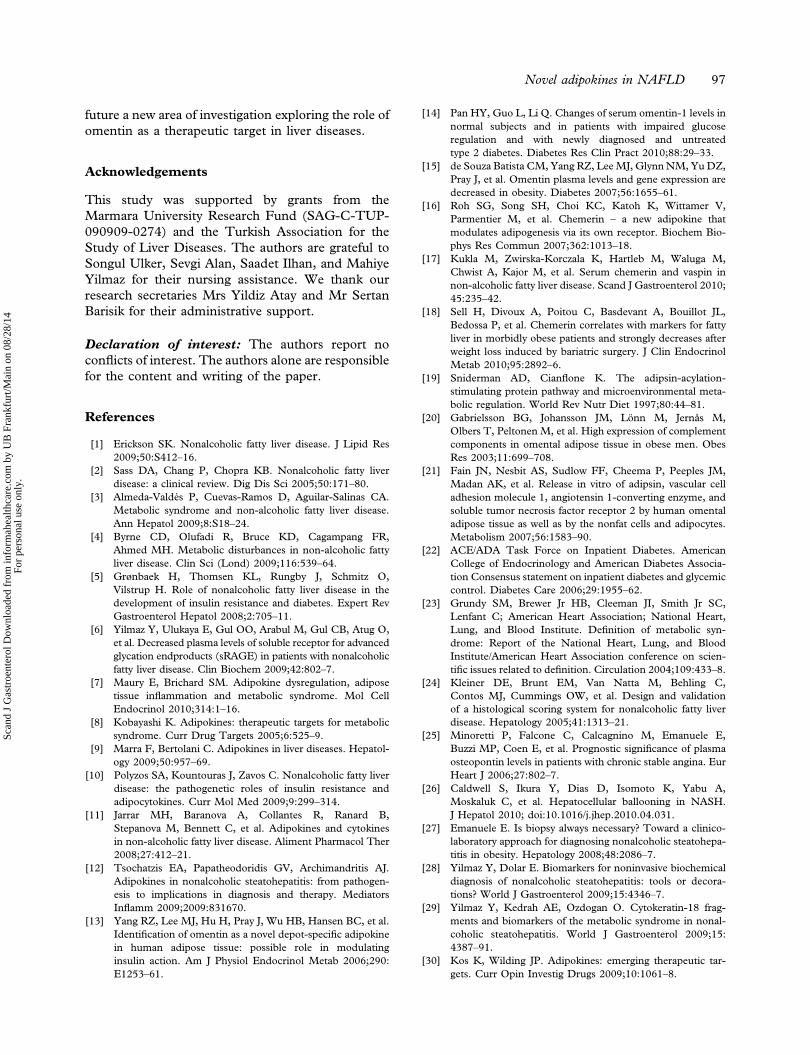
without NAFLD, including BMI, HOMA-IR, aspar-tate aminotransferase, alanine aminotransferase, totalcholesterol, low-density lipoprotein cholesterol, andtriglycerides. The prevalence of diabetes and theMetS was higher in patients with NAFLD than incontrols.Levels of adipokines in the study participants are
depicted in Table II. Adipsin levels did not differbetween patients and controls (Figure 1), whereasboth omentin (Figure 2) and chemerin (Figure 3)concentrations were significantly higher in patientswith biopsy-proven NAFLD than in controls (bothp values <0.001).We then evaluated the univariate correlation
coefficients of serum adipokines with clinical, bio-chemical, and histological parameters. Adipsin had nosignificant correlation with any parameter at thep < 0.01 level. Serum omentin levels were positivelyassociated with hs-CRP (r = 0.29, p < 0.01) and thedegree of hepatocyte ballooning (r = 0.27, p < 0.01),whereas chemerin showed a modest borderline
association with liver fibrosis (r = 0.22, p = 0.04).There were no association between the selected adi-pokines and the NASH score (data not shown), andthese molecules did not discriminate between simplesteatosis and definite NASH.After stepwise linear regression analysis adjusting
for age, sex, BMI, diabetes mellitus, MetS, HOMA-IR, blood pressure values, liver enzymes, lipid vari-ables, and hs-CRP, serum omentin levels retainedtheir independent significance as a predictor of hepa-tocyte ballooning in patients with NAFLD (b = 1.42;t = 2.79, p < 0.01).
Discussion
Our study demonstrates that (1) in patients withbiopsy-proven NAFLD, serum levels of omentinand chemerin, but not those of adipsin, are signifi-cantly higher than in normal controls, and (2)omentin is a predictor of hepatocyte ballooning,
Table I. General characteristics of the study participants.
NAFLD patients (n = 99) Control group (n = 75) p-Value
Sex (M/F) 50/49 37/38 NSAge (years) 48 ± 8 48 ± 7 NSBody mass index (kg/m2) 30.6 ± 4.9 27.4 ± 4.3 <0.01Diabetes mellitus (yes/no) 29/70 0/75 <0.001Metabolic syndrome (yes/no) 61/38 0/75 <0.001HOMA-IR 3.7 (2.3–5.1) 1.6 (0.6–2.5) <0.001Systolic blood pressure (mmHg) 138 ± 22 126 ± 20 NSDiastolic blood pressure (mmHg) 85 ± 13 82 ± 11 NSAST (U/L) 44 ± 18 24 ± 10 <0.001ALT (U/L) 68 ± 32 21 ± 11 <0.001Total cholesterol (mg/dl) 219 ± 49 188 ± 47 <0.01HDL cholesterol (mg/dl) 45 ± 11 44 ± 19 NSLDL cholesterol (mg/dl) 148 ± 51 127 ± 22 <0.001Triglycerides (mg/dl) 185 ± 88 143 ± 69 <0.001hs-CRP (mg/dl) 3.3 (2.7–4.9) – –
Histological steatosis 2 (1–3) – –
Lobular inflammation 2 (1–3) – –
Ballooning 2 (1–2) – –
NASH score 5 (4–7) – –
Fibrosis 1 (0–2) – –
Abbreviations: NAFLD = nonalcoholic fatty liver disease; HOMA-IR = homeostasis model of insulin resistance; AST = aspartate amino-transferase; ALT = alanine aminotransferase; HDL = high-density lipoprotein; LDL = low-density lipoprotein; hs-CRP = high-sensitivity C-reactive protein; NASH = nonalcoholic steatohepatitis.Data are presented as means ± SD, counts, or medians and interquartile ranges, as appropriate.
Table II. Plasma adipokines levels in the study participants.
NAFLD patients (n = 99) Control group (n = 75) p-Value
Adipsin (ng/ml) 5601 ± 2039 5330 ± 1334 NSOmentin (ng/ml) 460 ± 181 376 ± 196 <0.001Chemerin (ng/ml) 219 ± 83 159 ± 43 <0.001
Abbreviation: NAFLD = nonalcoholic fatty liver disease.Data are presented as means ± SD.
94 Y. Yilmaz et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.
independent of potential confounders, including met-abolic parameters.Our data on raised chemerin levels in patients with
NAFLD confirm, in a larger sample of patients, thepilot results obtained by Kukla et al. [17]. Of interest,we were also able to find an association betweenchemerin and the degree of liver fibrosis. After allow-ance for potential confounders, however, this resultdid not persist (data not shown). Taken together,these findings suggest that chemerin may play inthe pathophysiology of NAFLD but does not seemto be a key biomarker of liver fibrosis in this entity.Differently from Sell et al. [18], who identified apositive association of chemerin with BMI, CRP,and HOMA-IR, we were unable to find any signifi-cant relationship of this novel adipokine with theseparameters. Different study populations (patientswith NAFLD in our report vs. morbidly obese sub-jects in the study by Sell et al. [18]) may at least in partexplain such discrepancies. In any case, our findings
do not point toward a major independent associationof chemerin with insulin resistance in the setting ofNAFLD. Similarly, adipsin levels were not altered inNAFLD and were not correlated with any of theclinical, histological, and biochemical features ofour patients.An important finding in this study is the observa-
tion that omentin levels are significantly increased inpatients with NAFLD and represent an indepen-dent biochemical correlate of hepatocyte ballooningdegeneration. The positive correlation of omentinwith hepatocyte ballooning to our knowledge hasnot been previously reported. Since in this studyomentin levels were positively associated with hepa-tocyte ballooning, independent of insulin resistanceand other features of the MetS, it could also behypothesized that this molecule might play a role inthe development and progression of NAFLD. Hepa-tocyte ballooning indicates hepatocyte degenerationassociated with enlargement, swelling, rounding, and
16000150001400013000120001100010000900080007000
Ser
um a
dips
in le
vels
(ng
/ml)
600050004000300020001000
0NAFLD Healthy controls
Figure 1. Box plots of serum adipsin levels in patients with nonalcoholic fatty liver disease and control subjects.
14001300120011001000900800700600
Ser
um o
men
tin le
vels
(ng
/ml)
500400300200100
0NAFLD Healthy controls
Figure 2. Box plots of serum omentin levels in patients with nonalcoholic fatty liver disease and control subjects.
Novel adipokines in NAFLD 95
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.
characteristic reticulated cytoplasm [26]. Ballooningis considered a structural manifestation of microtu-bular disruption and is likely a representation of cellsundergoing lytic necrosis [26]. It is generally consid-ered that serum omentin is negatively associatedwith insulin resistance and obesity [14,15]. In addi-tion, there is evidence suggesting that this moleculeis capable of enhancing insulin-mediated glucoseuptake in human adipocytes, thereby exerting insu-lin-sensitizing effects [13]. Although these observa-tions might suggest that omentin levels should belower in NAFLD, not higher, our present lack ofunderstanding of the mechanisms by which omentinmight be regulated in metabolic liver disease does notallow us to make conclusions at this time. A salientfinding of the present analysis is the increase in serumomentin levels in our NAFLD patients. There is noavailable information about omentin concentrationsin NAFLD and additional studies are required toidentify reasons for this paradoxical increase. In par-ticular, future studies must delineate whether levelsof omentin are higher in the NAFLD populationbecause of a compensatory counter-regulatory mech-anism to the increased insulin resistance, that is, aprominent feature of NAFLD. Indeed, we are justbeginning to understand the metabolic function ofthis novel adipocykine in human metabolic disorders.Notably, we found a weak but statistically significantpositive association between hs-CRP and omentinlevels. It is unknown at present whether inflammatorystatus directly modulates omentin levels in patientswith NAFLD. Future studies should examine thepossible cross-talk between hs-CRP and omentin,that is, whether CRP modulates omentin expressionand secretion from adipocytes.Several limitations of this study merit comment.
First, this study was not designed to address themechanisms behind the observed associations.
Second, the relatively small sample size limits thegeneralizability of our conclusions. Third, the studypopulation consisted of Turkish men and women; as aresult, it is uncertain whether these findings are gen-eralized in other ethnic groups. These caveats not-withstanding, all patients with NAFLD underwentliver biopsy, the best standard for diagnosing thiscondition [27,28].In summary, our results suggest that serum omen-
tin levels are raised in patients with NAFLD regard-less of potential confounders and represent anindependent predictor of hepatocyte ballooning.These results support further investigation of thisnovel adipokine in metabolic liver diseases. Ourreport cannot assess whether the increase of omentinobserved in NAFLD may have a significance as anoninvasive method for diagnostic purposes or canshow a prognostic potential in this setting. In general,measuring serum adipokines holds promise for thenoninvasive assessment of patients in the spectrum ofNAFLD, but further carefully designed studies arenecessary before they can be recommended in clinicalpractice [29]. Because no effective specific therapy iscurrently available for NASH, the pharmacologicalmanipulation of adipokines in general could theoret-ically be a feasible option in the future [12]. However,the pathophysiological significance of adipokinesremains poorly understood in this setting, andmore research is needed to shed more light on thisissue. As adipokines may have both beneficial andpotentially harmful effects, a cautious approach iswarranted when considering the pharmacologicalmanipulation of adipokines to treat NAFLD, andnovel approaches may be required to target the liverand to reduce the potential for adverse effects [30].Altogether, this work adds to the current evidencesuggesting that novel adipokines may modulate theclinical expression of NAFLD, and may open in the
550
500
450
400
350
300
250S
erum
che
mer
in le
vels
(ng
/ml)
200
150
100
100
0NAFLD Healthy controls
Figure 3. Box plots of serum chemerin levels in patients with nonalcoholic fatty liver disease and control subjects.
96 Y. Yilmaz et al.
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.
future a new area of investigation exploring the role ofomentin as a therapeutic target in liver diseases.
Acknowledgements
This study was supported by grants from theMarmara University Research Fund (SAG-C-TUP-090909-0274) and the Turkish Association for theStudy of Liver Diseases. The authors are grateful toSongul Ulker, Sevgi Alan, Saadet Ilhan, and MahiyeYilmaz for their nursing assistance. We thank ourresearch secretaries Mrs Yildiz Atay and Mr SertanBarisik for their administrative support.
Declaration of interest: The authors report noconflicts of interest. The authors alone are responsiblefor the content and writing of the paper.
References
[1] Erickson SK. Nonalcoholic fatty liver disease. J Lipid Res2009;50:S412–16.
[2] Sass DA, Chang P, Chopra KB. Nonalcoholic fatty liverdisease: a clinical review. Dig Dis Sci 2005;50:171–80.
[3] Almeda-Valdés P, Cuevas-Ramos D, Aguilar-Salinas CA.Metabolic syndrome and non-alcoholic fatty liver disease.Ann Hepatol 2009;8:S18–24.
[4] Byrne CD, Olufadi R, Bruce KD, Cagampang FR,Ahmed MH. Metabolic disturbances in non-alcoholic fattyliver disease. Clin Sci (Lond) 2009;116:539–64.
[5] Grønbaek H, Thomsen KL, Rungby J, Schmitz O,Vilstrup H. Role of nonalcoholic fatty liver disease in thedevelopment of insulin resistance and diabetes. Expert RevGastroenterol Hepatol 2008;2:705–11.
[6] Yilmaz Y, Ulukaya E, Gul OO, Arabul M, Gul CB, Atug O,et al. Decreased plasma levels of soluble receptor for advancedglycation endproducts (sRAGE) in patients with nonalcoholicfatty liver disease. Clin Biochem 2009;42:802–7.
[7] Maury E, Brichard SM. Adipokine dysregulation, adiposetissue inflammation and metabolic syndrome. Mol CellEndocrinol 2010;314:1–16.
[8] Kobayashi K. Adipokines: therapeutic targets for metabolicsyndrome. Curr Drug Targets 2005;6:525–9.
[9] Marra F, Bertolani C. Adipokines in liver diseases. Hepatol-ogy 2009;50:957–69.
[10] Polyzos SA, Kountouras J, Zavos C. Nonalcoholic fatty liverdisease: the pathogenetic roles of insulin resistance andadipocytokines. Curr Mol Med 2009;9:299–314.
[11] Jarrar MH, Baranova A, Collantes R, Ranard B,Stepanova M, Bennett C, et al. Adipokines and cytokinesin non-alcoholic fatty liver disease. Aliment Pharmacol Ther2008;27:412–21.
[12] Tsochatzis EA, Papatheodoridis GV, Archimandritis AJ.Adipokines in nonalcoholic steatohepatitis: from pathogen-esis to implications in diagnosis and therapy. MediatorsInflamm 2009;2009:831670.
[13] Yang RZ, Lee MJ, Hu H, Pray J, Wu HB, Hansen BC, et al.Identification of omentin as a novel depot-specific adipokinein human adipose tissue: possible role in modulatinginsulin action. Am J Physiol Endocrinol Metab 2006;290:E1253–61.
[14] Pan HY, Guo L, Li Q. Changes of serum omentin-1 levels innormal subjects and in patients with impaired glucoseregulation and with newly diagnosed and untreatedtype 2 diabetes. Diabetes Res Clin Pract 2010;88:29–33.
[15] de Souza Batista CM, Yang RZ, LeeMJ, GlynnNM, YuDZ,Pray J, et al. Omentin plasma levels and gene expression aredecreased in obesity. Diabetes 2007;56:1655–61.
[16] Roh SG, Song SH, Choi KC, Katoh K, Wittamer V,Parmentier M, et al. Chemerin – a new adipokine thatmodulates adipogenesis via its own receptor. Biochem Bio-phys Res Commun 2007;362:1013–18.
[17] Kukla M, Zwirska-Korczala K, Hartleb M, Waluga M,Chwist A, Kajor M, et al. Serum chemerin and vaspin innon-alcoholic fatty liver disease. Scand J Gastroenterol 2010;45:235–42.
[18] Sell H, Divoux A, Poitou C, Basdevant A, Bouillot JL,Bedossa P, et al. Chemerin correlates with markers for fattyliver in morbidly obese patients and strongly decreases afterweight loss induced by bariatric surgery. J Clin EndocrinolMetab 2010;95:2892–6.
[19] Sniderman AD, Cianflone K. The adipsin-acylation-stimulating protein pathway and microenvironmental meta-bolic regulation. World Rev Nutr Diet 1997;80:44–81.
[20] Gabrielsson BG, Johansson JM, Lönn M, Jernås M,Olbers T, Peltonen M, et al. High expression of complementcomponents in omental adipose tissue in obese men. ObesRes 2003;11:699–708.
[21] Fain JN, Nesbit AS, Sudlow FF, Cheema P, Peeples JM,Madan AK, et al. Release in vitro of adipsin, vascular celladhesion molecule 1, angiotensin 1-converting enzyme, andsoluble tumor necrosis factor receptor 2 by human omentaladipose tissue as well as by the nonfat cells and adipocytes.Metabolism 2007;56:1583–90.
[22] ACE/ADA Task Force on Inpatient Diabetes. AmericanCollege of Endocrinology and American Diabetes Associa-tion Consensus statement on inpatient diabetes and glycemiccontrol. Diabetes Care 2006;29:1955–62.
[23] Grundy SM, Brewer Jr HB, Cleeman JI, Smith Jr SC,Lenfant C; American Heart Association; National Heart,Lung, and Blood Institute. Definition of metabolic syn-drome: Report of the National Heart, Lung, and BloodInstitute/American Heart Association conference on scien-tific issues related to definition. Circulation 2004;109:433–8.
[24] Kleiner DE, Brunt EM, Van Natta M, Behling C,Contos MJ, Cummings OW, et al. Design and validationof a histological scoring system for nonalcoholic fatty liverdisease. Hepatology 2005;41:1313–21.
[25] Minoretti P, Falcone C, Calcagnino M, Emanuele E,Buzzi MP, Coen E, et al. Prognostic significance of plasmaosteopontin levels in patients with chronic stable angina. EurHeart J 2006;27:802–7.
[26] Caldwell S, Ikura Y, Dias D, Isomoto K, Yabu A,Moskaluk C, et al. Hepatocellular ballooning in NASH.J Hepatol 2010; doi:10.1016/j.jhep.2010.04.031.
[27] Emanuele E. Is biopsy always necessary? Toward a clinico-laboratory approach for diagnosing nonalcoholic steatohepa-titis in obesity. Hepatology 2008;48:2086–7.
[28] Yilmaz Y, Dolar E. Biomarkers for noninvasive biochemicaldiagnosis of nonalcoholic steatohepatitis: tools or decora-tions? World J Gastroenterol 2009;15:4346–7.
[29] Yilmaz Y, Kedrah AE, Ozdogan O. Cytokeratin-18 frag-ments and biomarkers of the metabolic syndrome in nonal-coholic steatohepatitis. World J Gastroenterol 2009;15:4387–91.
[30] Kos K, Wilding JP. Adipokines: emerging therapeutic tar-gets. Curr Opin Investig Drugs 2009;10:1061–8.
Novel adipokines in NAFLD 97
Scan
d J
Gas
troe
nter
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B F
rank
furt
/Mai
n on
08/
28/1
4Fo
r pe
rson
al u
se o
nly.