serum adenosine deaminase levels in reactional and non
TRANSCRIPT

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 1/140
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 2/140
AUTHORS P.K NIGAM, P. SRIVASTAVA, P.K. BATRA
DEPARTMENTS OF DERMATOLOGY, STD ANDBIOCHEMISTRY, PT. J.N.M. MEDICAL COLLEGE,RAIPUR.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 3/140
ABSTRACT BACKGROUND AND AIMS: Altered serum adenosine
deaminase (ADA) levels have been recorded in variousdiseases involving lymphocytes and/orlymphoreticular system including leprosy.
The study was planned to evaluate alterations in serum ADA levels, if any , in reactional and non reactional
leprosy.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 4/140
Introduction Adenosine deaminase (ADA), an enzyme of purine metabolism,
in part regulates the lymphocytes metabolism and is alsoimportant for lymphocytic differentiation and growth.
It is present in lymphocytes in high concentration. The level of enzyme in T-lymphocytes varies according to cellulardifferentiation.
Its activity appears to be necessary for an effective immuneresponse as shown by many studies like in combined
immunodeficiency disease, and in typhoid fever. Besides this, increased activity of serum ADA has also been
demonstrated in tubercular pleural effusion, peritonealtuberculosis, AIDS, and cancer patients.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 5/140
Methods Eighty patients of different types of leprosy, clinically
diagnosed, slit smear examined and biopsy confirmed wherever necessary, and 20 normal healthy controlspreferably relatives of the patients, were included inthe study.
They were thoroughly examined to rule out any
associated immunological disease. Five milliliters of venous blood was collected and
serum was separated. ADA estimation was done by themethod as described by Giusti (1974).

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 6/140
Results Eighty patients of leprosy comprised 54 males and 26
females.
The age of the patients ranged from 5 years to 62 years.
The duration of illness ranged from 15 days to 3 years.
There were 12 patients each of tuberculoid (TT),borderline tuberculoid (BT), mid borderline (BB),borderline lepromatous (BL), and lepromatous leprosy
(LL). Besides these, twenty patients were of reactional
leprosy, 10 patients in type 1 and 10 patients in type 2reaction were included.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 7/140
Results The mean serum ADA level in the normal healthy
controls was 10.31 ± 0.58 u/L. The mean serum ADA levels in various types of non-reactional leprosy casesare shown in Table below:

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 8/140
Results Comparison of mean serum adenosine deaminase
levels (u/L) in non-reactional leprosy patients(excluding LL) as a group and leprosy patients in type Ireaction is shown below.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 9/140
Results Comparison of the mean serum adenosine deaminase
levels (u/L) in leprosy patients with type I and type IIreactions is shown below.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 10/140
Results Comparison of the mean serum adenosine deaminase
levels (u/L) in LL leprosy patients (without reaction)and LL leprosy patients in type II reaction is shownbelow.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 11/140
Discussion A number of parameters including ADA activity have been used
to assess cell mediated immune response in different diseases. Low ADA activity has been observed in severe immune
deficiency diseases and raised ADA levels have been reported in
lymphocytic proliferative diseases. There was a significant increase in serum ADA levels in our
multibacillary leprosy patients as compared to paucibacillary leprosy patients.
Paucibacillary patients in reaction showed a further increase in
levels as compared to patients without reaction. Similarly LL patients in type II reaction showed significantly
higher levels as compared to LL patients without reaction.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 12/140
Discussion An increased activity of serum ADA has also been demonstrated
in leprosy patients by other workers as well.
Suri Babu et al in their study of ADA activity in serum and
peripheral blood lymphocytes of leprosy patients also observedthat serum ADA levels were elevated in tuberculoid as well aslepromatous cases as compared to control subjects.
The lymphocyte adenosine deaminase activity also showed asimilar trend.
They suggested that, since the overall activity of the enzyme isnot deficient in leprosy, the cellular immune aberration seen inthe different types of leprosy may be due to abnormalproliferation of different subsets of lymphocytes in response toM. leprae.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 13/140
Discussion Shende et al also observed that ADA levels were
higher in leprosy patients as compared to that incontrols thus correlating with the immunologicalstatus of patients. However, their patients with leprareaction showed decreased ADA levels and highergrade of lepromin test positivity was associated withincreased ADA activity.
Dayal et al also observed that the mean serum andlymphocyte ADA levels in multibacillary leprosy weresignificantly high as compared to the control group.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 14/140
Discussion The present study showed that as one moves from
tuberculoid to lepromatous spectrum mean serum ADA levels increase and are particularly more in the
presence of lepra reactions. This indicates their potential for being used as a
marker of activity of disease in leprosy in general andlepra reactions in particular.
However, the difference between the values of thecontrol group and type of leprosy was statistically significant only for the BL and LL group.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 15/140
Discussion Increase in ADA levels particularly in lymphocytes has been
attributed by various workers to increased lymphocyteproliferation as a result of antigenic stimulation.
This lymphocyte proliferation in vitro can be measured by
lymphocyte transformation test (LTT). Studies have indicated that it gradually increases from LL to BB
spectrum. Dayal et al, in their study indicated that ADA levels in serum can
not be taken as an index of lymphocyte proliferation as
suggested in some reports. Chaudhary et al have also shown that serum ADA levels may not
run exactly parallel with the conventional parameters of cellmediated immunity in leprosy patients.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 16/140
Discussion Lack of any correlation between ADA levels and
LTT(lymphocyte transformation test) along thespectrum of leprosy can be due to many factors.
ADA is also present in monocytes and increasestremendously during their maturation intomacrophages. Lymphocyte ADA level estimation alsoincorporates B-lymphocyte ADA which is not at all
involved in cell mediated immune response. Further studies in this area should assess whether
these raised levels of serum ADA revert back to normalor not once the reaction phase subsides.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 17/140

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 18/140
AUTHORS P. K. Nigam, Prashant Kumar*, N. Pathak**,
S. Mittal***
Departments of Dermatology, *Medicine, and***Pathology, Pt. J.N.M. Medical College &
Assoc. Dr. B.R.A.M. Hospital, Raipur and **Sai
Sahara Pathology Clinic, Raipur . 492001, India.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 19/140
ABSTRACT
Background:
Histopathological evaluation of skin lesions is notfeasible in many leprosy endemic areas.
Fine needle aspiration cytology (FNAC) is a simplertool compared to histopathology for the evaluation of
the cytomorphology of skin lesions.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 20/140
Aims:
To study the cytomorphology of leprosy lesions infine needle aspirates and correlate it with the
histopathology.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 21/140
INTRODUCTION Cytology is a widely accepted diagnostic procedure for
a large variety of malignant and inflammatory lesions.
Skin-slit smears stained for acid-fast bacilli (AFB) have
been conventionally used for the assessment of leprosy
lesions but their use has been restricted to the
evaluation of the bacterial index and morphological
index.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 22/140
Marian Ridley emphasized the interpretation of cellular
exudate in conventionally stained Ziehl-Neelsen smears.
Singh etal studied the cytomorphology of the cellularexudates in fine needle aspirates (FNA) of leprosy lesions
and could sub-classify them on the same position on the
Ridley Jopling(R-J) scale as seen in histology. It was also
observed that FNA smears, in contrast to slit-skin smears, were free of confounding epidermal squamous cells and
therefore better suited for evaluating cell morphology.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 23/140
The current study was undertaken to evaluate theutility of FNA in reactional and non-reactional leprosy
lesions.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 24/140
METHODS Seventy patients attending the skin and leprosy clinic
were studied. Their diagnosis and classification in theR-J scale were based on clinical examination using
standard criteria.
Fine needle aspirations were done on therepresentative lesions followed by a skin biopsy fromthe same site for histopathological examination.
Biopsies were evaluated and classified according to thehistological criteria established by Lucas and Ridley and the World Health Organization.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 25/140
Fine needle aspiration smears were specially evaluatedfor cellularity, morphological details of macrophages,accompanying inflammatory cells and bacterial index.
All smears were air-dried and stained with May-Grunwald-Giemsa (MGG) stain and modified Ziehl-Neelsen’s stain.
Skin tissue for histopathology was obtained in 53patients and stained with H and E stain.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 26/140
Cytological criteria for sub-classification of leprosy were applied as defined by Singh et al.These are asfollows:
Tuberculoid leprosy (including TT and BT)
Cellular smears
Cohesive epithelioid cell granulomas
Numerous lymphocytes not infiltrating thegranuloma
No stainable AFB (BI=0)

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 27/140
Mid-borderline leprosy (BB)
Fair cellular yieldPoorly cohesive granulomas composed of an
admixture of epithelioid cells and macrophages
Few lymphocytes infiltrating the granulomas
BI = 1+ to 2+

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 28/140
Borderline lepromatous leprosy (BL)
Moderate cellularity
Singly dispersed macrophages with ‘negativeimages’; no epithelioid cells
Numerous lymphocytes diffusely admixed with
macrophages
BI = 3+ to 4+

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 29/140
Lepromatous leprosy (LL)
Heavy cellularity
Numerous foamy macrophages in a fatty background with intracellular and extracellular
‘negative images’
Few lymphocytes
BI = 5+ to 6+ (globi)

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 30/140
Reaction
Numerous fragmented AFB (MI< 1) and neutrophils
suggest a Type II reaction in LL (erythema nodosumleprosum).

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 31/140
RESULTS A total of 70 patients (46 males and 24 females) were studied.
Their age ranged from nine years to 64 years (mean 34.5 ± 2.75 years).
The duration of leprosy ranged from one month to three years (mean1.9 ± 0.6 years).
Five patients had indeterminate leprosy (I), 12 patients had tuberculoidleprosy (TT), 19 patients had borderline tuberculoid leprosy(BT), eight
patients had mid-borderline leprosy (BB), 12 patients had borderlinelepromatous leprosy (BL) and 14 patients had lepromatous leprosy(LL).
Of these, 15 patients presented with a lepra reaction (nine with a Type1 lepra reaction and six patients with a Type 2 lepra reaction).

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 32/140
The histopathological study of the tissue confirmed the clinicaldiagnosis in all the 53 patients except in two patients in whomthe histopathological picture was nonspecific.
Patients with tuberculoid leprosy showed moderate to heavily
cellular smears, cohesive epithelioid cell granulomas, numerous
lymphocytes not infiltrating the granulomas and no stainable
AFB.
Skin smears of mid-borderline leprosy patients showed fairly
cellular smears, poorly cohesive epithelioid cell granulomascomposed of an admixture of epithelioid cells and macrophages
and a few lymphocytes infiltrating the granuloma.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 33/140
Borderline leprosy patients were characterized by
moderately cellular smears, singly dispersed macrophages
with ‘negative’images, no epithelioid cells and numerous
lymphocytes diffusely admixed with macrophages.
Lepromatous leprosy patients showed heavy cellularity,
foamy macrophages, fatty background, neutrophils,lymphocytes, collagen and elastin and stainable AFB in all
smears.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 34/140
The smears of patients with reactional leprosy were highly
cellular with foamy macrophages and ‘negative’ images,
neutrophilic infiltrate, degenerating collagen and elastin, a
few lymphocytes and a fatty background.
Among nine patients with a Type 1 lepra reaction (BT, six;BB, two;and BL, one), neuritis was present in six; none of them had a nerve abscess.
All the patients presented with exacerbation of erythemaand inf lammation over existing lesions and appearance of afew new lesions.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 35/140
The cytomorphological features in six of the nineclinically diagnosed patients of type 1 reaction wereconfirmed by FNAC of skin aspirates using the
standard cytological criteria described by Ridley andRadia.
All the remaining three patients showed nonspecificcytological features.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 36/140
All the borderline group patients (BT, BB and BL) hadheavily cellular smears, lymphocytes, neutrophils andedematous background.
However, loose epithelioid cell granulomas and giantcells, collagen, elastin and proliferating fibroblasts
were present in a significantly large number in smearsof borderline leprosy patients with a Type 1 leprareaction.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 37/140
The cytological features of Type 2 lepra reaction werepresent in five of the six patients with ENL.
The histopathological examination of the skin biopsy showed evidence of ENL in all of them except one.
The smears were more heavily cellular withfragmented collagen and elastin and a significant
increase in neutrophils in patients with a Type 2 leprareaction, while foamy macrophages with fatty background were relatively more commonly seen innonreactional lepromatous leprosy patients.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 38/140
DISCUSSION Ridley and Jopling proposed a histological classification of
leprosy reflecting the immunological spectrum of the disease.
It divides leprosy into five clinically and histologically recognizable groups based on the distribution of epithelioid
cells, Langhans giant cells, foam cells, globi, lymphocytes,
plasma cells, fibroblasts, a clear sub-epidermal zone, cellular
cuffing and infiltration of nerves.
The histopathological criteria for sub-classification of leprosy as
defined by Ridley and Jopling have been applied to cytologicalsmears by Singh et al. They could place most of their patients inthe same group as on histopathology.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 39/140
Out of the 53 patients of leprosy in whomhistopathology was done, 41 (77.3%) showedcorrelation of cytomorphological features with clinico-
pathological diagnosis. In the remaining 12 patients (22.1%) there was poor
correlation, possibly because of incorrect siteselection.
Moreover, this number might have been less if aspirates had been taken from multiple sites, as wasobserved by Singh et al.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 40/140
Hence, it may be concluded that there is a fairly goodcorrelation between the clinical, histological and
cytomorphological features of skin aspirates and that it
is possible to classify leprosy along the R-J scale based
on cytological smears.
Thus, in endemic areas, especially where histopathological
services are not available, cytomorphological assessment of leprosy lesions may be advocated as a simple tool for
evaluation of the primary diagnosis and natural course of
the disease.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 41/140

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 42/140
AUTHORS Rameshwar Gutte, Vidya Kharkar, Sunanda
Mahajan, Siddhi Chikhalkar, Uday Khopkar
Department of Dermatology, Seth GS Medical College
and KEM Hospital, Mumbai, India

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 43/140
Abstract Granulomatous mycosis fungoides (GMF) is a rare type
of cutaneous T cell lymphoma.
A 38-year-old married male presented with decreasedsweating all over the body for last 8 years, progressiveredness and scaling over body for 2 years and multiplenoduloulcerative lesions over the body for 1 year.
Cutaneous examination revealed generalized erythemaand scaling with poikilodermatous changes over chestand upper back along with multiple noduloulcerativelesions.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 44/140
Abstract Skin biopsy from a nodular lesion revealed dense
granulomatous infiltrate of atypical lymphocytes withepidermotropism and sparing of appendages.
Diagnosis of GMF was made.
Computed tomographic scan of thorax, abdomen andpelvis revealed axillary and inguinal
lymphadenopathy. Immunohistochemistry revealed leukocyte common
antigen and CD3 positivity suggestive of T cell origin
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 45/140
Abstract Patient was started on CHOP (Cyclophosphamide,
Hydroxydaunorubicin, Oncovin and Prednisolone)
regimen of chemotherapy with marked improvementafter three cycles of chemotherapy.
This case had some clinical resemblance to
lepromatous leprosy.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 46/140
Introduction Granulomatous mycosis fungoides (GMF) is a rare type of cutaneous T cell lymphoma (CTCL).
The first case of this entity described in 1970 had multipleulcerated nodules, many of which healed spontaneously with
atrophic scars and poikiloderma. Heterogenous nature of clinical presentation delays diagnosis
and consequently diagnosis is based mainly on histopathologicalfeatures, immunohistochemistry and gene rearrangementstudies.
This case was reported for its rarity, association withhypohidrosis, granulomatous lymphadenitis and to highlight itsresemblance to lepromatous leprosy.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 47/140
Case Report A 38-year-old married male hailing from Uttar Pradeshpresented with decreased sweating all over the body for last8 years, generalized redness and scaling over the body for 2
years and multiple painful ulcerated lesions over the body
for 1 year. He was apparently alright 25 years back (1984) when he
developed asymptomatic hypopigmented patches overright thigh and face.
Gradually he developed multiple patches all over the body
over a period 10 years. The patient had taken multiple ayurvedic and
homeopathic treatments in past without any improvementbut no anti-leprosy treatment was received

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 48/140
Case Report Later, the lesions started becoming dry and confluent with
dyspigmentation since last 2 years and at the same time hedeveloped multiple painless swellings over neck, axillae
and groins for which he was treated with antituberculoustherapy empirically without improvement.
Since the last 1 year he started getting multiple painfulnoduloulcerative lesions over the body at multiple sites.
He was investigated for leprosy and CTCL. Skin biopsy was suggestive of CTCL and he was referred to
an oncologist for further management.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 49/140
Lymph node biopsy showed diffuse infiltrate of atypicallymphocytes with histiocyte microgranulomas.
Bone marrow aspiration and biopsy showed normal uninvolvedbone marrow.
Hemogram revealed marginally raised erythrocytesedimentation rate (36 mm at the end of 1 hour) and white bloodcell count (10,800 cells/mm 3 ).
Rest of the investigations including liver and kidney functiontests were within normal limits.
His serology was negative for HIV 1 and 2 as well as HBsAg andhepatitis C virus.
Computed tomographic scan of the thorax, abdomen and pelvisrevealed bilateral axillary and inguinal lymphadenopathy

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 50/140
Diagnosis of mycosis fungoides (MF) nodular stage with lymph node involvement was made.
He was referred to them by the oncopathologist torule out leprosy in view of history of hypopigmentedpatches, hypohidrosis and granulomatous infiltrate inhistopathology.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 51/140
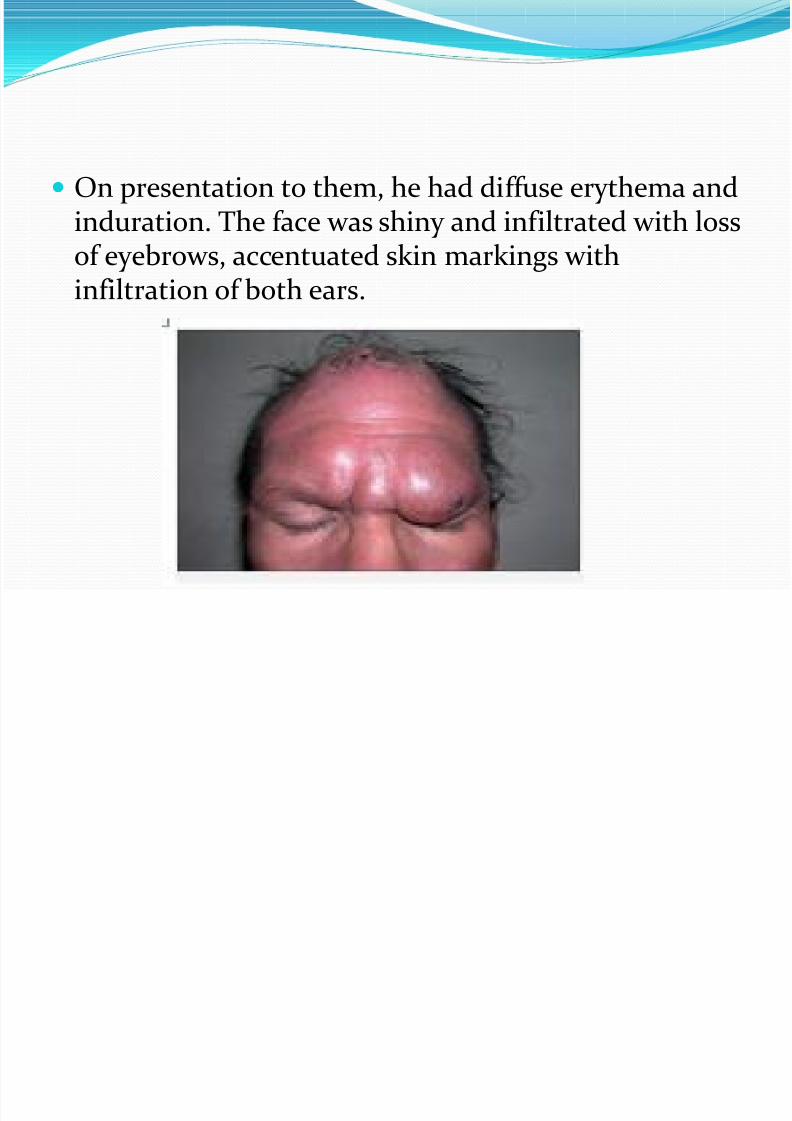
On presentation to them, he had diffuse erythema andinduration. The face was shiny and infiltrated with lossof eyebrows, accentuated skin markings with
infiltration of both ears.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 52/140
He also had poikilodermatous changes all over thebody along with multiple painful indurated nodules of various sizes ranging from 2 to 6 cm. Many of these
were ulcerated.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 53/140
But there were no hypopigmented patches.
There was bilateral axillary and inguinallymphadenopathy.
The lymph nodes were firm, non-tender, mobile andnon-matted measuring 2-3 cm in largest diameter.There was no sensory deficit, and peripheral nerveexamination was also normal.
Rest of the general and systemic examination was within normal limits.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 54/140
They did a repeat skin biopsy from a nodular lesion onforearm.
Histopathology revealed dense infiltrate of lymphocytes
within the dermis extending deep up to subcutaneous fat. The lymphocytes were of large size with hyperchromatic
indented nuclei.
There was marked epidermotropism without spongiosisand some lymphocytes were aligned singly at the basal
layer of the epidermis with characteristic basal tagging of lymphocytes.
Multiple tuberculoid granulomas with Langhans andforeign body type of giant cells were also seen.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 55/140
Special stains for mycobacteria and fungi revealed noorganisms.
Infiltrate spared the nerves and appendages.
The number of sweat units appeared normal but there was granulomatous infiltrate around them.
Slit skin smear was negative for Mycobacterium leprae.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 56/140
Peripheral smear examination revealed no definite atypicallymphocytes.
Immunohistochemistry of skin biopsy was positive for
leukocyte common antigen and CD3 suggesting T cellorigin of lymphoma.
Tumor cells were negative for CD15, CD20, CD23, CD30 andanaplastic lymphoma kinase-1.
Polymerase chain reaction (PCR) for monoclonality of the
malignant cells is more confirmatory but they could not doit due to unaffordability of patient.
PCR for M. leprae was also not done due to unavailability and as Fite-Faraco stain was also negative.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 57/140
Thus, they confirmed the diagnosis of GMF stage IV A2 of EORTC staging of MF.
The patient was started on CHOP(Cyclophosphamide, Hydroxydaunorubicin, Oncovinand Prednisolone) regimen of chemotherapy by theoncologist with good improvement in skin lesions afterthree cycles .
However, erythema and scaling were persistent andno noticeable improvement in hypohidrosis was seen.
The patient is following up with the oncologist.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 58/140
Discussion Granuloma formation in MF is now a well-characterizedfeature and was first reported in 1970.
Because of variable presentation, GMF lacks particular
clinical criteria for diagnosis, making it primarily ahistopathological diagnosis and it should be suspected incases of granulomatous dermatitis with other features of MF.
It can be confused especially with granulomatous slack
skin or leprosy and should be differentiated onhistopathology.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 59/140
Granuloma formation is known to occur in variouslymphomas and other malignancies including solidorgan malignancies and even malignant melanoma
with variable frequency. Hodgkin's disease has the highest frequency of
granuloma formation among the various lymphomas.
It is rarely seen in non-Hodgkin's lymphomasincluding cutaneous lymphomas.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 60/140
In cutaneous lymphomas, two variants, granulomatousslack skin and GMF are especially associated withgranuloma formation.
Though the granuloma is usually sarcoidal, tuberculoid
and granuloma annulare like granulomas are also describedin GMF.
Both GMF and granulomatous slack skin can be mistakenfor some non-neoplastic granulomatous dermatitis onhistology but epidermotropism with atypical lymphocytes
helps to differentiate between the two. Concomitant occurrence of non-neoplastic granulomas
with MF like sarcoidosis and granuloma annulare orinfectious granulomas may also be considered.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 61/140
GMF may also be mistaken for leprosy specially incountries like India where leprosy is endemic.
This leads to delay in diagnosis and treatment. A case of granulomatous slack skin mistaken for leprosy
and treated with dapsone and rifampicin has beendescribed.
Diagnostic dilemma with leprosy is more likely if a patienthas peripheral neuropathy due to GMF itself.
Presence of epidermotropism and atypical lymphoidinfiltrate throughout the dermis without any anatomicalpreference with sparing of appendages and dermal nervesallows differentiation between the two on histopathology.
These findings were present in the above case.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 62/140
Granulomatous lymphadenitis is rare in GMF.
A case of GMF with granulomas in lymph nodeinitially diagnosed as sarcoidosis is reported.
In this case, clinical and histological involvement of lymph nodes with formation of multiple histiocyticmicrogranulomas was observed.
There was no CNS, pulmonary, thyroid or intestinalinvolvement.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 63/140
In view of history of disease starting ashypopigmented patches initially, GMF in this casepresumably evolved from preexisting hypopigmented
MF. To the best of the knowledge, presence of hypohidrosis
with GMF is not reported.
The hypohidrosis in their case could be due to
inflammatory and compressive effect of the densegranulomatous infiltrate onto sweat units.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 64/140
The exact etiology of granulomatous reactions associated withmalignancies in not known.
Some consider it as peculiar hypersensitivity response to malignantcells or some persistent infection while some consider it as protectivephenomenon with good prognosis.
Prognostic significance of granulomas in the setting of malignantdisease is not clear though some may consider it as protective responseof host.
Granuloma does not necessarily mean better prognosis as four patientsof GMF who died of disseminated disease have been reported. ]
A case with spontaneous regression of GMF in HIV positive patient hasalso been described.
Regression was thought to be probably due to cytotoxic effect of HIV on neoplastic cells.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 65/140
In conclusion, the case had many unusual features, viz., presence of hypohidrosis, granulomatous lymphnode involvement.
GMF presumably evolved from hypopigmented MF.
It had clinical resemblance to leprosy due to diffuseinfiltration of face, loss of eyebrows and history of hypopigmented patches.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 66/140

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 67/140
AUTHORS PVS Prasad, PK Kaviarasan
Department of Dermatology Venereology and Leprosy,Rajah Muthiah Medical College & Hospital, AnnamalaiUniversity, Tamil Nadu, India

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 68/140
Abstract Leprosy remains an important problem globally.
Timely detection of new cases and prompt treatment withMDT continue to be the main intervention strategies.
They reviewed the various issues related to classification,treatment, drug resistance and the possible steps toeliminate the disease in the near future.
The need for newer anti leprosy agents has been felt and
various agents like fluroquinolones, macrolides andminocycline have all been tried in various combinationsand duration.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 69/140
Uniform MDT in all leprosy patients might be a logical onetoo.
Drug resistance can be identified by PCR based DNA sequence analysis which saves much time.
Drugs like thalidomide analogues, pentoxifylline, selectivecytokine inhibitory drugs have proved effective incontrolling type-2 reaction in leprosy patients. New drugsfor leprosy reactions are still needed.
Far from being eliminated as a public health problem,
leprosy still causes a considerable long term morbidity inboth developing and developed world.
New treatment and the optimal length of MDT requiresfurther research.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 70/140
Introduction Leprosy is a chronic infectious disease caused
by Mycobacterium leprae ( M. leprae) which mainly affects the skin and peripheral nerves.
The treatment of leprosy has been revolutionizedsince the introduction of multidrug therapy (MDT) in1981, following the recommendation of the WorldHealth Organization (WHO).

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 71/140
The global detection of new cases has declined by 4%during 2007 when compared to 2006.
Although the figures are highly encouraging, the
number of new cases detected annually has remainedquite stable during the last 15 years.
Timely detection of new cases and prompt treatment with MDT continue to be the main interventionstrategies.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 72/140
Although these regimens are generally satisfactory,limitations in terms of persisting activity and latereactions/relapses in paucibacillary (PB) leprosy, along
with the persistence of dead and/or live organisms inmultibacillary (MB) forms of the disease have beenobserved.
This article elaborates the recent trends in the
management of leprosy and future plans to eliminatethis disease.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 73/140
WHO Therapy and Its Impact The need for an internationally accepted classification for
leprosy was recognized long ago.
In 1981, WHO recommended a classification for
operational purpose as pauci- and multi-bacillary (PB andMB).
This was introduced to simplify disease recognition and toensure that all patients were apparently treated with MDT.
Though WHO classification and treatment have becomemuch simpler for health workers, the expertise needed torecognize a wide range of presentations of symptoms andsigns of the disease is gradually vanishing.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 74/140
Initially, WHO incorporated slit skin smears in theclassification and patients with bacterial index (BI) of 2+ were only included in MB category of disease.
In 1988, WHO further modified its recommendationsthat a positive smear at any site was sufficient toinclude in MB category.
Much later the need for skin smear was droppedaltogether so that the current classification includesanyone with six or more skin lesions under MB.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 75/140
There is a chance of under treatment according to thiscriteria. In a study from Philippines, it was concludedthat 38-51% of patients may have the risk of under
treatment if Ridley Jopling's (RJ) classification isincorporated into WHO classification.
Hence, the two classifications should be seen ascomplementary and not as exclusive
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 76/140
However, it may considered that WHO classification may be useful for treatment and RJ classification for predictingthe complications in a given patient.
Another pitfall of WHO classification is that neuriticleprosy is also not included. In India, the proportion of neuritic leprosy cases has been found to be as high as 18%.
It would also be important to consider how newer tests
such as PGL-1, T-cell-based tests and skin tests using newantigens fit into the RJ and WHO classification in future.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 77/140
Issues related to therapy Therapy of leprosy has also been constantly revised. In
the beginning of 1981, WHO recommended to treatMB cases till two consecutive skin smear negative
results were achieved. Subsequently, in 1992, fixed duration therapy (FDT)
was introduced where MB patients were giventreatment for 2 years or 24 pulses in a period of 36
months by which time the dependability of skin smear was removed.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 78/140
Later, in 1995, WHO redefined the therapy with 12 pulses of MDT-MB.
Hence, it was recommended to stop treatment at the end of 12months or if 12 pulses were completed in a period of 18 months.
Skin smear examination was not mandatory. Since 1998, the great majority of MB patients has been treated
with MDT for only 12 months.
However, there is no information about the 5-year relapse rate.
Apparently, determination of the relapse rate after 12-monthMDT is highly relevant, and should be considered as a toppriority for research.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 79/140
In contrast, the duration of PB therapy has notchanged since WHO's first recommendation andremains for 6 months, or six pulses to be completed
within 9 months. As most patients in this group are lepromin-positive,
it was opined that residual organisms which remainafter stoppage of therapy would be tackled by the
immunity of the host.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 80/140
A third category has been introduced as single lesionpaucibacillary leprosy (SLPB), where single dose rifampicin 600mg, ofloxacin 400 mg, and minocycline 100 mg (ROM) therapy
was recommended for cure.
The recommendation was on the basis of a multicentric double-blind field trial conducted in India. This regimen was applied widely in India, Bangladesh, and
Brazil, but patients should be under surveillance for 2 years afteradministration of therapy.
Preliminary results showed only a marginal advantage over the
conventional therapy. Report of the international leprosy association technical forum
recommended this regimen only in those countries where singlelesion leprosy cases are at large.
N d f t

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 81/140
Need for newer agents
The reason for the need of new drugs and regimens are: (1) From the operational point of view, the recommended
duration of treatment, particularly for MB leprosy is stilltoo long.
(2) Two of the components of currently administered drugsfor MB leprosy, i.e., dapsone and clofazimine are only
weakly bactericidal against M. leprae. Hence furthershortening the duration of treatment by this regimenmight result in high relapse rate.
(3) Administration of the daily components, dapsone, andclofazimine cannot be supervised. (4) Patients who cannot tolerate any of the drugs in MDT-
MB need a safer and effective alternative
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 82/140
Over recent years, many important advances havebeen made in developing molecular diagnostics, inidentifying highly effective drugs and designing
multidrug regimens for treatment.
Several effective regimens have been developed, whichare generally satisfactory.
Fl i l

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 83/140
Fluoroquinolones
This group of compounds exerts their antimicrobial effect by inhibiting α subunit of DNA gyrase (an enzyme which is notaffected by any other therapeutic agent in use) and thereby interfering with bacterial DNA replication.
Several f luoroquinolones such as ofloxacin, pefloxacin,sparfloxacin, and moxifloxacin have all been found to beeffective against M. leprae.
Ofloxacin is preferred as the other two drugs need to be given ina very high dose to achieve the same effect as ofloxacin at a doseof 400 mg. It is bactericidal against M. leprae although less so
than a single dose of rifampicin. When given daily for 22 days, itkilled 99% of the viable organisms. Moxifloxacin has been found to be more effective than the other
fluoroquinolones.
M lid

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 84/140
Macrolides
Several members of this group have been evaluated,and clarithromycin appears to be promising.
Clarithromycin is a semi-synthetic macrolide
antibiotic structurally related to erythromycin. Mousefootpad studies showed potent bactericidal activity of this drug, but it is less effective than rifampicin.
At a dose of 500 mg per day, the drug is reported tokill 99% of M. leprae by 58 days.
Mi li

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 85/140
Minocycline
Minocycline is the only tetracycline which exhibitssignificant activity against M. leprae.
It is because the drug is lipophilic which permits it to
penetrate the bacterial cell wall. It is bactericidal against M. leprae but lesser than
rifampicin.
The drug binds reversibly to the 30 S unit of theribosome, thus blocks the binding of aminoacyltransfer RNA to the messenger RNA-ribosomalcomplex and thus inhibits protein synthesis.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 86/140
Combination regimens A highly desirable new regimen is one that would permit allof the components to be administered once monthly undersupervision, which would significantly reduce the risk of emergence of rifampicin-resistant mutants, caused by
irregular administration of the daily dapsone-clofaziminecomponent, and would also simplify the treatment.
ROM is the first fully supervisable, monthly administered
regimen. Its efficacy of monthly doses for treatment of MBand PB leprosy has been tested in field trials in threedifferent countries.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 87/140
Rifapentine, a rifampicin derivative, is another drug which has pharmacokinetic properties far superiorthan rifampicin with significantly higher peak serum
concentrations and much longer serum half-life. Recent findings from mouse experiments indicate that
rifapentine and moxifloxacin are significantly morebactericidal, respectively, than rifampicin andofloxacin, which is far more bactericidal than ROM.
Combination of rifapentine-moxifloxacin-minocycline(PMM) is found to be more superior.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 88/140
Rifampicin 600 mg is also combined with once a monthclarithromycin at a dose of 1000 mg and minocycline 200mg. This regimen has caused significant delay in growthof M. leprae in mice.
Similarly, a combination of daily ofloxacin withminocycline along with monthly rifampicin has also beentried.
Another regimen included usual MDT-MB along with
addition of of loxacin and minocycline once monthly. Intensive short course regimens consisting of daily doses of
rifampicin with ofloxacin for 1 month in MB patients haveproduced high relapse rates
Uniform MDT

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 89/140
Uniform MDT
A common regimen for treatment of PB and MB leprosy is desirable. However, the size of the bacterial populations and the underlying
immunological responses are different in two groups. Hence, a common regimen would appear likely to result in over
treatment of PB patients or under treatment of MB patients. Recently, the WHO technical Advisory Group (TAG) on Elimination of
Leprosy proposed "implementation of a uniform 6-month MB-MDTregimen for all patients."
As there is no proper information on the follow-up of 1 year FDT in MBpatients, there is no justification to test the possibility of furthershortening the duration of MDT for MB patients to 6 months.
Addition of clofazimine in PB regimen in 44 patients has improved theclinical outcome and produced disappearance of lesions and regressionof granuloma.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 90/140
Quadruple regimen In a study at Belgium, MB patients were given weekly supervised doses of rifampicin, ofloxacin, clofazimine,and minocycline for 6 weeks.
Initial results are highly encouraging.
Relapse rate was only 2%. However, long-term follow-up is needed in all these shortened regimens.
A MDT
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 91/140
A-MDT
With MDT, the adherence was only 70-80%. However, to accelerate leprosy elimination process, recently the
WHO leprosy programme and its TAG have changed
dramatically their position on supervised therapy. They concluded that after the first dose of MDT "supervision of
the subsequent monthly component of the MDT regimens is nolonger essential.“
Further, on the basis of this conclusion they recommendedlarge-scale implementation of accompanied multidrug therapy (AMDT), which refers to a policy that patients are provided theentire supply of MDT drugs at the time of diagnosis, whenchoosing someone close to them to accompany them with theirtreatment.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 92/140
The problems which are yet to be solved are: (1) Whether AMDT is to be applied routinely or only in
special situations. (2) Who may be chosen to supervise? (3) How does AMDT help? (4) How to train health workers to supervise AMDT? With
large-scale implementation of AMDT, the quality of treatment is a matter of real concern.
Without a guarantee of quality, quantitative achievementor a declaration of leprosy elimination is meaningless.
Therefore, it is time to replace wishful thinking withevidence-based practice, and discontinue theimplementation of AMDT as a routine in the field.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 93/140
Drug resistance Emergence of rifampicin resistance would create lot of difficulties for an individual patient, and its widespreaddissemination would pose a problem to the community and a threat to leprosy control.
Rifampicin resistance could emerge rapidly in a very fewpatients.
Although rifampicin resistance was not reported in morethan 10 million patients who completed MDT, this could be
due to two reasons. (1) Post-MDT surveillance for relapse has been
discontinued.
(2) Rifampicin susceptibility testing is difficult to carryout.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 94/140
Polymerase chain reaction (PCR)-based DNA sequence analysis of the rpoB gene of M. leprae was infull concordance with those of the susceptibility
testing in mouse footpad system. This approach may lead to the diagnosis of 80%
rifampicin-resistant strains of M. leprae.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 95/140
Recently, there have been reports on multidrugresistance to M. leprae.
Besides resistance to rifampicin, the strains were also
resistant to at least one or more drugs other thandapsone, including ofloxacin and sparfloxacin.
Although the number of multidrug-resistant strains issmall, their occurrence is indeed an alarm bell and
must be closely scrutinized.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 96/140
In a recent study, across three countries it was foundthat from new cases 3% were dapsone-resistant and2% were rifampicin-resistant.
In samples from relapsed patients, 15% were dapsone-resistant and 8% were rifampicin-resistant.
Chemoprophylaxis

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 97/140
Chemoprophylaxis
Recently, because the new case detection rate (NCDR) has notdiminished following implementation of MDT, there has beenrenewed interest in chemoprophylaxis.
Both dapsone and acedapsone were used earlier for this purpose.
Two basic principles are followed in chemoprophylaxis. They are: (1) Rifampicin should be one of the components. (2) The treatment should be administered only in a single dose. Rifampicin alone or ROM therapy has been proposed for this. Both have been found to have an equal efficacy and hence single
dose of rifampicin alone has been proposed. Only one trial report is available on this aspect which shows that
the protective effect was only 35-40%. In this trial, a dose of 1500 mg of rifampicin was administered
and this was not compared with 600 mg of rifampicin.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 98/140
The limitations of chemoprophylaxis are:
(1) If chemoprophylaxis is confined to only householdcontacts, the benefit will range up to 15%.
(2) The effect of chemoprophylaxis may only betransitory and has to be repeated.
Reactions in leprosy

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 99/140
Reactions in leprosy
Reactions in leprosy pose greater problems than thedisease itself.
For type-1 reaction steroids, chloroquine and
cyclosporine are used. Treatment with thalidomide provides an effective
alternative to steroid therapy gives better long-termcontrol and avoids the adverse effects of prolonged
steroid therapy.
The results of cyclosporine varies from the modest tohighly effective.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 100/140
Type-2 reaction has generally declined due to theaddition of clofazimine in MB-MDT.
Treatment of reaction is on the basis of suppression of
inflammation and its consequences. Drugs such as corticosteroids, non-steroidal anti-
inflammatory drugs (NSAIDS), chloroquine,antimonials, pentoxiphylline, and thalidomide are
used in type-2 reaction.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 101/140
Controlled clinical trials have demonstrated thatthalidomide rapidly controls ENL and is superior to aspirinand pentoxifylline.
However, thalidomide is teratogenic when taken in early pregnancy and is unavailable in many leprosy endemiccountries.
Thalidomide analogs, which are chemically similar tothalidomide but appear to lack its side effects are being
pursued. Revimid and actimid are promising in thiscategory.
They are currently in phase I and II trials.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 102/140
Pentoxifylline, a methyl xanthine derivative has beenused in one study but found to be less effective in thecontrol of type-2 reaction.
Though several new drugs are available, steroids andthalidomide are the mainstay in the control of type-2reaction.
Selective cytokine inhibitory drugs (Sel CIDs) arephospho-diesterase type-4 inhibitors with potentTNFα activity but without T-cell co-stimulatory effect.It is currently under investigation.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 103/140
On the basis of earlier studies on the prevention of deformitiesfollowing recommendations were made.
1. Steroids were recommended to treat reactions and nerve functionimpairments (NFIs) of recent onset; the expected recovery rate forNFI is approximately 60%.
2. MB patients and those with existing NFIs would be carefully monitored for new nerve function loss, as they are the groups at thegreatest risk.
3. Assessment of nerve function using standard methods every monthduring MDT is recommended.
4. Research is recommended to identify the optimal steroid regimen, to
develop alternative and more effective for the reactions and recentnerve function loss.5. Further research is recommended on the use of prophylactic
steroids, in prevention of NFI.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 104/140
Major points for future investigation are:
1. Mechanisms of Schwann cell injury in leprosy:TNFα, cytotoxic T-cell, and apoptosis.
2. The definition of tissue markers as indicative of nerve damage: myelin components, ninjurinadhesions, and ECM components.
3. Establishment of therapeutic interventions for nerveregeneration: Matrix metalloproteinases inhibitors,inhibitors of apoptosis, adhesion inhibitors, andmethycobalamine

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 105/140
Role of immunotherapy Besides the presence of a small population of viable
organisms ("persisters') after therapy, the problem of persistence of a large pool of dead bacilli is oftenencountered. Immunomodulators that can stimulate CMI
have been applied to reduce this pool. These agents can be divided into three broad categories.
1. Drugs such as levamisole and zinc.
2. Antigenically related mycobacteria such as BCG, ICRC
bacillus, BCG plus killed M. leprae, Mycobacteriumw ( Mw), and M. vaccae.
3. Other immunomodulators such as transfer factor,recombinant interferon γ(IFN γ), and interleukin-2.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 106/140
Transfer factor-induced transient effects such as lepromin conversion,granuloma formation, and increased influx of lymphocytes locally.
Intralesional administration of IFN γ in leprosy patients inducedaccumulation of lymphocytes and monocytes at the local site of injection.
There was a distinct fall in bacillary index at the local site, with theformation of epithelioid granuloma and occurrence of reversal reactionin some cases.
Enhanced bacterial clearance with IFNγ has been reported.
The administration of interleukin-2 has accelerated bacterialclearance.
However, these effects were seen only at the local site.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 107/140
With regard to vaccine development for leprosy, theexplosion of genomic information from both thepathogen ( M. leprae) and its natural hosts (man andarmadillo) has been revolutionary.
Gene cloning and recombinant protein expressiontools can be used for the subsequent immunologiccharacterization and vaccine efficacy trials of high-priority antigens.
Potent vaccines have the added advantage of producing long-lived immunological memory, whichcan block multiple exposures over host's lifetime.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 108/140
Vaccines may be very useful to take us to the next level diseaseeradication.
The following are ongoing research with future potentials.1. Protein make-up of armadillo-derived M. leprae has been studied
using two-dimensional polyacrylamide gel electrophoresis. There are391 cell-associated proteins. These proteins may encompass activitiesinvolved in virulence or capable of being immunogenic during
various stages of infection.2. Testing for vaccine efficacy in the armadillo would also allow for the
assessment of efficacy across the disease spectrum as the armadillo
manifests similar bacterial growth characteristics andhistopathological features observed in humans infected with M.leprae.
Can We Hope to Eliminate
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 109/140
Can We Hope to Eliminate
Leprosy?
The principles of disease elimination and eradicationhave been clearly described by Dowdle in the Bulletin
of WHO in 1998. Control of disease is defined as the reduction of
disease incidence, prevalence, morbidity, or mortality to a locally acceptable level as a result of deliberate
efforts; continued intervention measures are requiredto maintain the reduction.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 110/140
Elimination of disease is defined as the reduction tozero of the incidence of a specified disease in a definedgeographical area as a result of deliberate efforts;
continued intervention measures are required. Similarly, elimination of infection is defined as a
reduction to zero of the incidence of infection causedby a specific agent in a defined geographical area as a
result of deliberate efforts; continued measures toprevent reestablishment of transmission are required

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 111/140
Eradication is defined as the permanent reduction tozero of the worldwide incidence of infection caused by a specific agent as the result of deliberate efforts;
intervention measures are no longer needed.
Extinction is defined as in which the specific infectiousagent no longer exists in nature or in the laboratory.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 112/140
Milestones in leprosy elimination In leprosy, WHO limited elimination to control
instead of transmission, using prevalence instead of incidence.
Elimination in leprosy was defined as reducing theglobal prevalence to less than 1 per 10,000.
The 44th World Health Assembly in 1991 passed aresolution to "eliminate leprosy as a public health
problem" by the year 2000.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 113/140
In the year 2000, WHO announced the elimination was achieved globally, i.e., a world prevalence of lessthan 600,000 leprosy patients.
In 2005, a strategic plan for the elimination of leprosy was introduced.
By the end of 2005, all but six countries reported aprevalence of less than 1 per 10,000.
The six countries are Brazil, Republic of Congo,Madagascar, Mozambique, Nepal, and Tanzania.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 114/140
For the period 2006-2010, WHO introduced the"Global Strategy for Further Reducing the Leprosy Burden and Sustaining Leprosy Control Activities" to
address the remaining challenges in providing servicesfor leprosy patients under conditions of lowprevalence.
Impact of MDT on trends of

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 115/140
Impact of MDT on trends of
transmission It was assumed that MDT would reduce the transmission of M.
leprae through a reduction of the number of contagiousindividuals in the community, but unfortunately there is noconvincing evidence for this hypothesis.
There were two large-scale studies on trend analysis available tointerpret the impact of MDT globally.
In the first study published by Meima in 1997, the authorconcluded that factors such as case detection and treatment
would reduce leprosy transmission is reasonable, but the reality may be more complicated.
Individuals incubating the disease may already harbor many bacilli, and it is possible that those individuals already transmit M. leprae to others long before the onset of the disease.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 116/140
More interestingly, a general acceleration of downwardtrends in the NCDR after the introduction of MDT hasnot occurred.
In the more recent study, the same author showed no
general decline in case detection at global level up to
2000.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 117/140
There are no suitable tests to detect the subclinicalmycobacterial infections reliably, including M. leprae.
Assessment of results of leprosy control depends on
information about disease and not infection. Disease statistics are expressed in terms of prevalence
and new case detection.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 118/140
Disease prevalence in leprosy is measured by countingall patients receiving MDT at a given time andexpressing this as a ratio using the population as the
denominator (in leprosy, it is per 10,000). Therefore, the figures are linked to the length of
treatment.
As the duration of treatment is reduced from 24 to 12
months, the prevalence also is reduced by 50%.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 119/140
For PB group, there is a chance that patients might bemissed for that year as those patients on roll only onDecember, 31 are taken into account.
Hence, those patients who completed in the first half of the year may not be included into the figures.
Indian scenario

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 120/140
Detection of new cases in leprosy in 2007 and thenumber of new cases detected previously:
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 121/140
In India, it was found that the NCDR dropped by 75%from 559,938 in 2000 to 139,252 in 2006.
The factors which may be responsible are operational
influence and BCG vaccination. Protective efficacies against leprosy ranged from 24%
to 34% in randomized control trials in India.
At the same time, proportion of new cases with WHOgrade-2 disability increased from 1.6% to 2.2%between 2004 and 2007 which is an increase by 38%.This is an alarming situation.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 122/140
Decline in the transmission of incidence (i.e., onset of disease) of leprosy may be related to several factors.
The period during which M. leprae is transmitted, whichcan be reduced by early case detection and chemotherapy.
BCG vaccination, which is not only widely administered asa preventive measure for many against tuberculosis, butalso appears to afford protection against leprosy.
Improvement in socioeconomic conditions such as housingconditions, member of persons per household per room,family size, and nutritional factors.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 123/140
Lessons learnt The assumption that case detection and treatment
would reduce leprosy transmission is reasonable, butthe reality may be more complicated.
Individuals incubating the disease may already harbormany bacilli, and these individuals might havetransmitted M. leprae to others long before the onsetof the disease, given its long incubation period.
Such transmission could be prevented by early casedetection and treatment.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 124/140
Second problem is delay between the onset of diseaseand detection.
Leprosy is a quiescent disease and hence there may be
substantial delay before the patient seeks treatment.The average detection delay exceeded 2 years in a study in Ethiopia.
It is possible that close contacts of a leprosy patientbecome infected rapidly.
Other factors which could limit the impact of controlare carriage of infection in the nose, persistence of M.lepraein the soil and even in animal reservoirs

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 125/140
Global leprosy situation at the beginning of 2008-South-east Asia statistics is given below.
Cure rates % for PB and MB not known.
Leprosy's Global Statistics -

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 126/140
p y
Fallacies Leprosy statistics pose particular problems for
surveillance for several reasons.
There are problems with diagnosis and classification of
the disease in the field even in good programmes.Problems in stigmata and confidentiality, which affect
reporting practices and official data.
Leprosy's Global Statistics -

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 127/140
p y
Fallacies There have been major operational changes in the
recent years in many countries.
There are often delays in reporting from some
countries.Statistics have emphasized only prevalence, which is
difficult to interpret.
Political pressures associated with eliminationinitiative, which appear to have influenced the mannerof reporting statistics.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 128/140
The most striking trend in global leprosy in recent years is thedecline in India, which reported 137,685 new cases in 2007 whencompared to 559,938 in the year 2000.
This implies that India's contribution to the global leprosy
burden has declined from 73% to 54% of the world's newly detected leprosy cases over these years.
It is unclear the extent to which this decline reflects changes inascertainment and criteria for new cases to be counted in India.
It is doubtful whether single lesion cases are being systematically
counted. Without such information, this important trend in India's
statistics remain difficult to interpret.
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 129/140
Relapse statistics are of considerable interest, becauseof their potential relevance to drug resistance.
Three countries provide more than 80% of the world's
total of 2355 reported relapses. India reported no relapses.
It is apparent that vast majority of relapses in the world go unreported with present systems
8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 130/140
Again, cure rates should be substituted with treatmentcompletion rate, which is not available for many countries including India.
Overall, the global prevalence statistics are notcomparable.
Due to these problems, they are of little use inmonitoring global leprosy trends.
WHO has recognized this problem, and the current(2005-2010) Global Strategy urges a concentrationupon new case detection.
Scenario Analysis of Leprosy

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 131/140
Trends Up to 2020 Now a days, the diagnosis and treatment of leprosy are
easy and most endemic countries are striving to fully integrate leprosy services into existing general health
services. This is especially important for those under-served
and marginalized communities mostly at risk fromleprosy, often the poorest of the poor.
Access to information, diagnosis, and treatment withMDT remain the key elements in the strategy toeliminate the disease as a public health problem.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 132/140
Most previously, highly endemic countries have nowreached elimination (defined as a registeredprevalence rate of <1 case/10,000 population).
However, pockets of high-endemicity still remain insome areas of Angola, Brazil, Central African Republic,Democratic Republic of Congo, India, Madagaskar,Mozambique, Nepal, and the United Republic of Tanzania.
These countries remain highly committed toeliminating the disease, and continue to intensify theircontrol activities.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 133/140
The need for an internationally accepted classificationsystem for leprosy was recognized long ago.
Many classifications have been proposed each with its
merits and demerits. It would now be timely to establish agreed clinical and
histological case definitions for classifications together with protocols for patient classification.
New diagnostic tests such as T-cell-based tests shouldfit into the new classification and protocols.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 134/140
MDT-based control appears to reduce transmission.
The pace of reduction is highly uncertain, but in any case slow. BCG may enhance the pace, but its impact is
also uncertain. M. leprae genome can now be explored using in
silico analysis to identify new immuno-dominantgenes which can be used for developing new leprosy
vaccines.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 135/140
The gray areas in leprosy control are the role of closecontact transmission, the speed of transmission, and theextent of contagiousness during the incubation period.
Research addressing these questions is essential to narrow
down the uncertainty regarding the impact of MDT-basedcontrol.
There are newer regimens available to treat leprosy, butrifampicin is still considered as the sheet anchor in thetreatment of leprosy.
Although rifampicin resistance has not yet been reportedto occur in a larger scale, we should be aware of thispossibility in future and evolve alternative strategies.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 136/140
More than 13 million cases were detected and treated with MDT between 1982 and 2002.
Nevertheless, many new cases are still detected yearly
and future projections of the global leprosy burdenindicate that at least 5 million new cases will arisebetween 2000-the year of leprosy "elimination"-and2020.
To attain leprosy elimination in future effectiveintervention is needed to interrupt the transmissionof M. leprae.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 137/140
BCG vaccination does not offer full protection and inthe absence any other specific vaccination against thebacillus, other strategies such as chemoprophylaxis of
subclinically infected people at risk must bedeveloped.
Similarly, the other possibilities such as nonhuman orenvironmental reservoirs of M. leprae need to be
explored.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 138/140
There are considerable numbers of people who arecompelled to live under the threat of deteriorating functiondue to established leprosy-related impairments.
It is predicted that there will be still approximately onemillion cases with WHO grade-2 deformities in the year2020.
With the expertise that is available to intensify research, we continue to anticipate that a more effective treatment will eventually be developed to address the risk of NFI.
Prevention of deformities does not require advancedtechnology but will require advanced thinking.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 139/140
When elimination of the disease is defined as thereduction to zero of the incidence, leprosy is definitely not eliminated.
We need genomic-based technologies to address theunresolved issues of transmission and infection with M. leprae.

8/22/2019 Serum Adenosine Deaminase Levels in Reactional and Non
http://slidepdf.com/reader/full/serum-adenosine-deaminase-levels-in-reactional-and-non 140/140
THANK YOU