serous effusion - bosnianpathology.org effusion pf.pdf · female-ovary, uterus, breast, gi tract,...
TRANSCRIPT
16.06.2016
1
Cytology of Serous Effusions
From basics to challenges
Pınar Fırat, MD, MIAC
Department of Pathology, İstanbul University,
İstanbul Faculty of Medicine, TURKEY
• Objectives – Basic principles in the evaluation of serous effusions
– Differential diagnosis between reactive mesothelial
proliferations, metastatic carcinomas, and malignant
mesotheliomas
– Role of immunohistochemistry for correct
interpretation
– Use of other ancillary tests when needed.
Cytology of Serous Effusions
From basics to challenges
Serous effusion
• Systemic / local disease
• Common
• Frequently reactive
• Any type of tumor may cause malignant
effusion
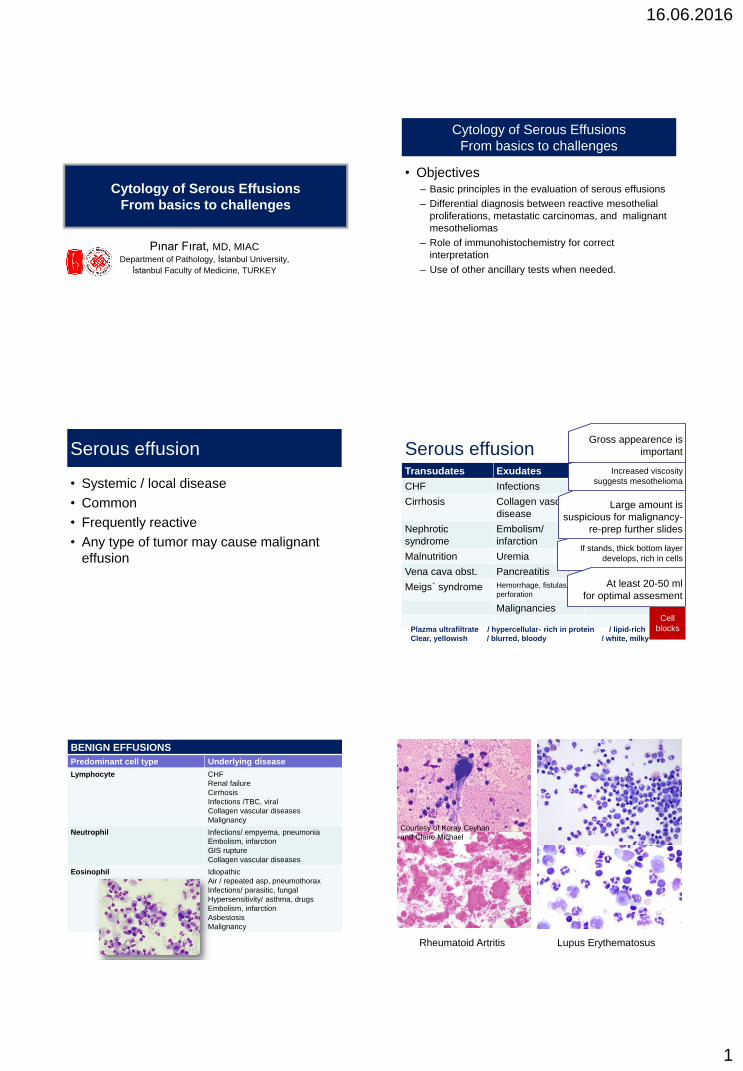
Serous effusion Transudates Exudates Chylous
CHF Infections Trauma
Cirrhosis Collagen vascular
disease
Malignancies
Nephrotic
syndrome
Embolism/
infarction
Malnutrition Uremia
Vena cava obst. Pancreatitis
Meigs` syndrome Hemorrhage, fistulas,
perforation
Malignancies
Plazma ultrafiltrate / hypercellular- rich in protein / lipid-rich
Clear, yellowish / blurred, bloody / white, milky
If stands, thick bottom layer
develops, rich in cells
At least 20-50 ml
for optimal assesment
Large amount is
suspicious for malignancy-
re-prep further slides
Increased viscosity
suggests mesothelioma
Gross appearence is
important
Cell
blocks
BENIGN EFFUSIONS
Predominant cell type Underlying disease
Lymphocyte CHF
Renal failure
Cirrhosis
Infections /TBC, viral
Collagen vascular diseases
Malignancy
Neutrophil Infections/ empyema, pneumonia
Embolism, infarction
GIS rupture
Collagen vascular diseases
Eosinophil Idiopathic
Air / repeated asp, pneumothorax
Infections/ parasitic, fungal
Hypersensitivity/ asthma, drugs
Embolism, infarction
Asbestosis
Malignancy
Courtesy of Koray Ceyhan
and Claire Michael
Rheumatoid Artritis Lupus Erythematosus
16.06.2016
2
Main question is….
• Is it malignant? A malignant effusion may be the manifestation
of a known malignancy
Determines the stage of the disease and the
appropriate therapy
Not always malignant in cancer patients!
Initial presentation of an unknown malignancy
Primary site ?
Sensitive!
Specific!
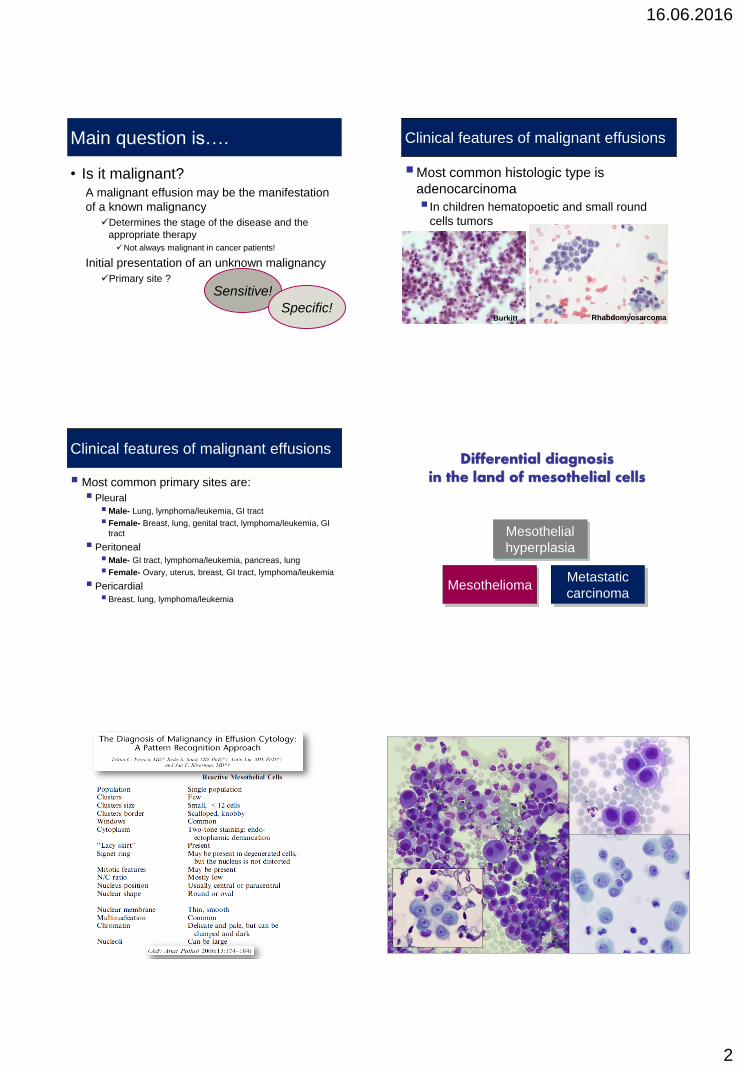
Clinical features of malignant effusions
Most common histologic type is
adenocarcinoma
In children hematopoetic and small round
cells tumors
Rhabdomyosarcoma Burkitt
Clinical features of malignant effusions
Most common primary sites are:
Pleural
Male- Lung, lymphoma/leukemia, GI tract
Female- Breast, lung, genital tract, lymphoma/leukemia, GI
tract
Peritoneal
Male- GI tract, lymphoma/leukemia, pancreas, lung
Female- Ovary, uterus, breast, GI tract, lymphoma/leukemia
Pericardial
Breast, lung, lymphoma/leukemia
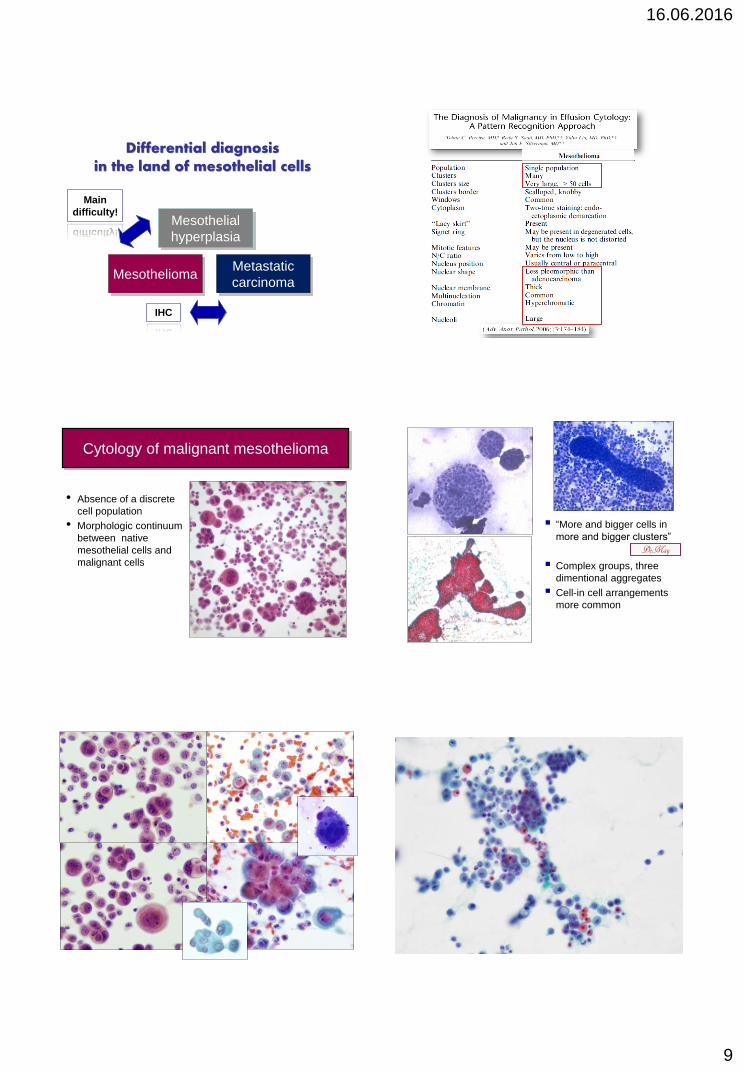
Differential diagnosis in the land of mesothelial cells
Mesothelioma
Mesothelial
hyperplasia
Metastatic
carcinoma
16.06.2016
3
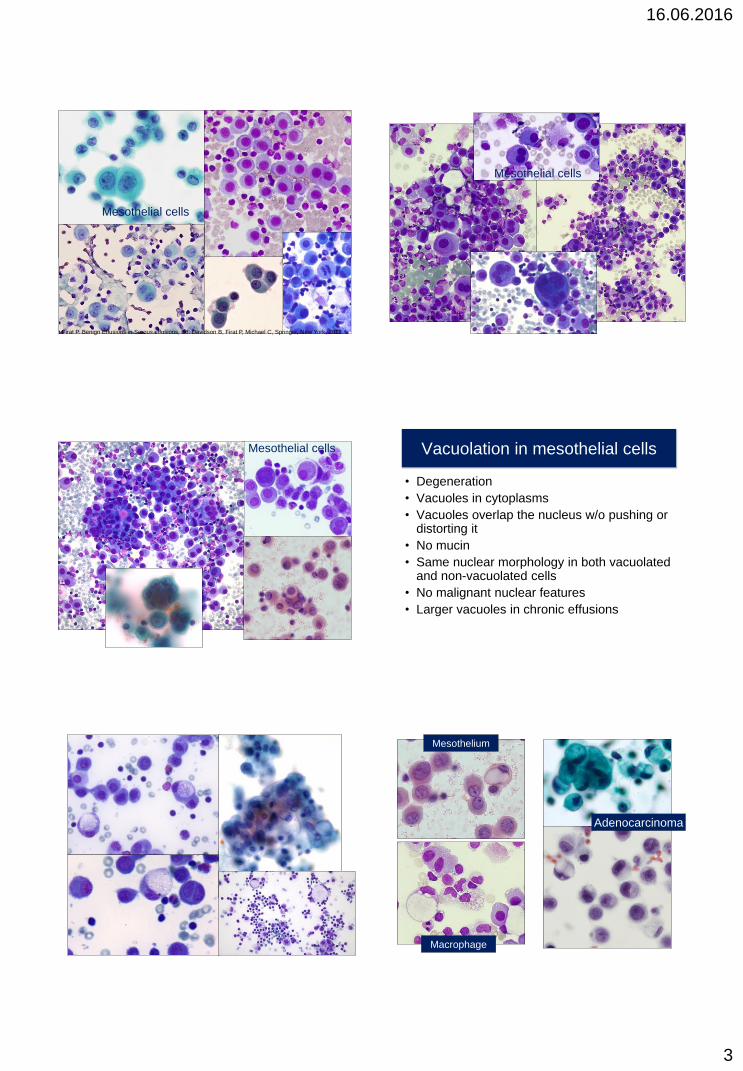
Mesothelial cells
Firat P. Benign Effusions in Serous effusions, Ed. Davidson B, Firat P, Michael C, Springer, New York, 2012
Mesothelial cells
Mesothelial cells Vacuolation in mesothelial cells
• Degeneration
• Vacuoles in cytoplasms
• Vacuoles overlap the nucleus w/o pushing or distorting it
• No mucin
• Same nuclear morphology in both vacuolated and non-vacuolated cells
• No malignant nuclear features
• Larger vacuoles in chronic effusions
Adenocarcinoma
Mesothelium
Macrophage
16.06.2016
4
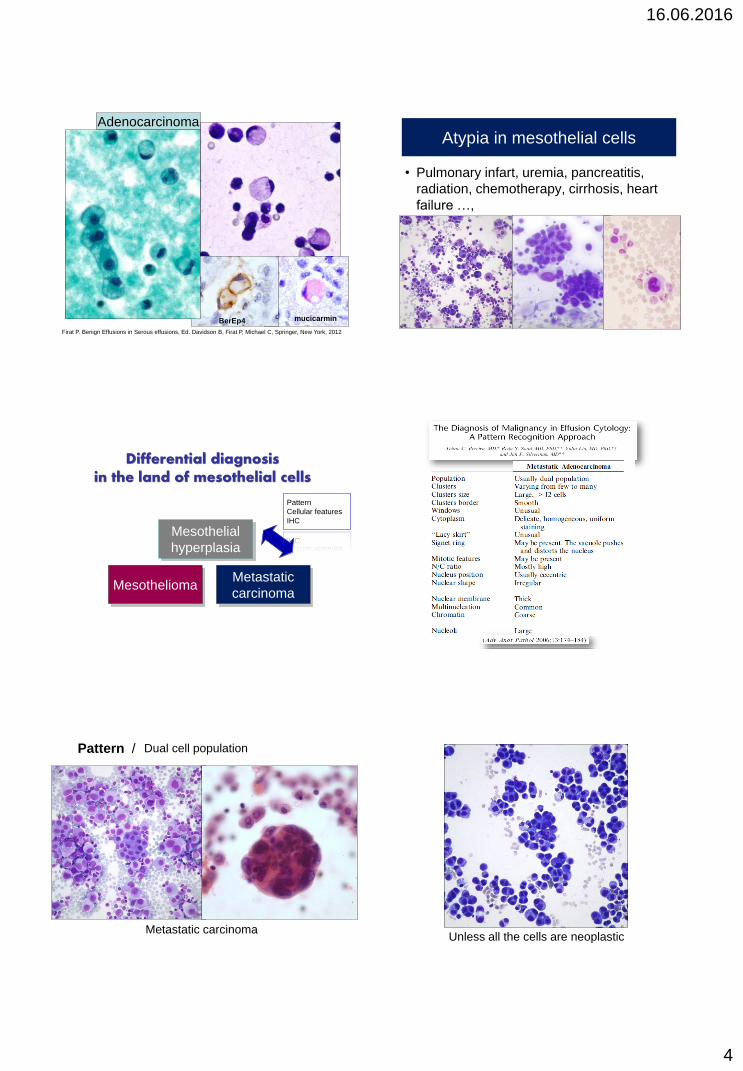
Adenocarcinoma
BerEp4 mucicarmin
Firat P. Benign Effusions in Serous effusions, Ed. Davidson B, Firat P, Michael C, Springer, New York, 2012
Atypia in mesothelial cells
• Pulmonary infart, uremia, pancreatitis,
radiation, chemotherapy, cirrhosis, heart
failure …,
Differential diagnosis in the land of mesothelial cells
Mesothelioma
Mesothelial
hyperplasia
Metastatic
carcinoma
Pattern
Cellular features
IHC
Dual cell population
Metastatic carcinoma
Pattern /
Unless all the cells are neoplastic
16.06.2016
5
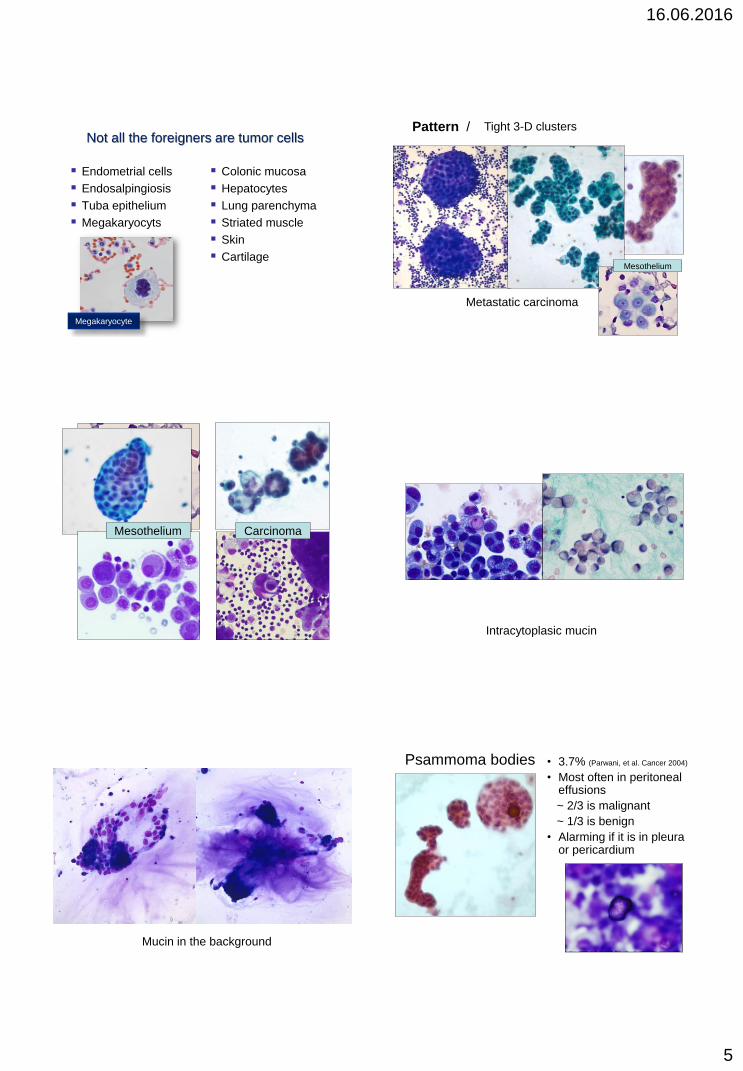
Not all the foreigners are tumor cells
Endometrial cells
Endosalpingiosis
Tuba epithelium
Megakaryocyts
Colonic mucosa
Hepatocytes
Lung parenchyma
Striated muscle
Skin
Cartilage
Megakaryocyte
Tight 3-D clusters Pattern /
Metastatic carcinoma
Mesothelium
Carcinoma Mesothelium
Intracytoplasic mucin
Mucin in the background
Psammoma bodies • 3.7% (Parwani, et al. Cancer 2004)
• Most often in peritoneal effusions
~ 2/3 is malignant
~ 1/3 is benign
• Alarming if it is in pleura or pericardium
16.06.2016
6
Metastatic carcinoma
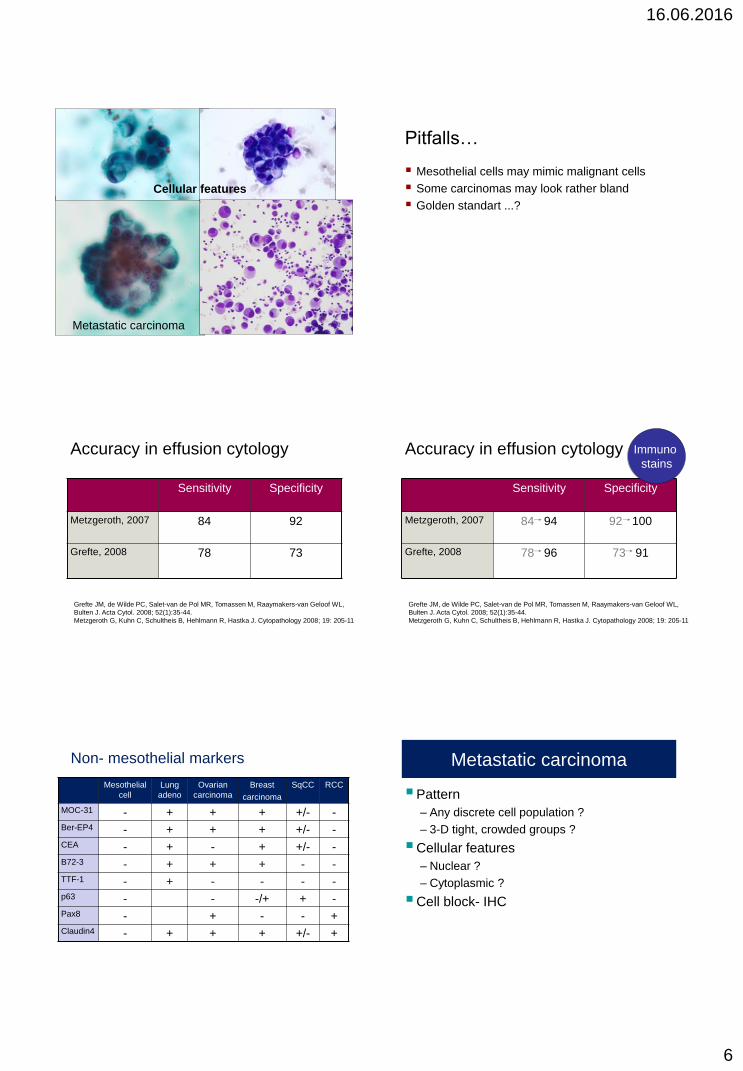
Cellular features
Pitfalls…
Mesothelial cells may mimic malignant cells
Some carcinomas may look rather bland
Golden standart ...?
Accuracy in effusion cytology
Sensitivity Specificity
Metzgeroth, 2007 84 92
Grefte, 2008
78
73
Grefte JM, de Wilde PC, Salet-van de Pol MR, Tomassen M, Raaymakers-van Geloof WL,
Bulten J. Acta Cytol. 2008; 52(1):35-44.
Metzgeroth G, Kuhn C, Schultheis B, Hehlmann R, Hastka J. Cytopathology 2008; 19: 205-11
Accuracy in effusion cytology
Sensitivity Specificity
Metzgeroth, 2007 84 94 92 100
Grefte, 2008
78 96
73 91
Grefte JM, de Wilde PC, Salet-van de Pol MR, Tomassen M, Raaymakers-van Geloof WL,
Bulten J. Acta Cytol. 2008; 52(1):35-44.
Metzgeroth G, Kuhn C, Schultheis B, Hehlmann R, Hastka J. Cytopathology 2008; 19: 205-11
Immuno
stains
Mesothelial
cell
Lung
adeno
Ovarian
carcinoma
Breast
carcinoma
SqCC RCC
MOC-31 - + + + +/- -
Ber-EP4 - + + + +/- -
CEA - + - + +/- -
B72-3 - + + + - -
TTF-1 - + - - - -
p63 - - -/+ + -
Pax8 - + - - +
Claudin4 - + + + +/- +
Non- mesothelial markers Metastatic carcinoma
Pattern
– Any discrete cell population ?
– 3-D tight, crowded groups ?
Cellular features
– Nuclear ?
– Cytoplasmic ?
Cell block- IHC
16.06.2016
7
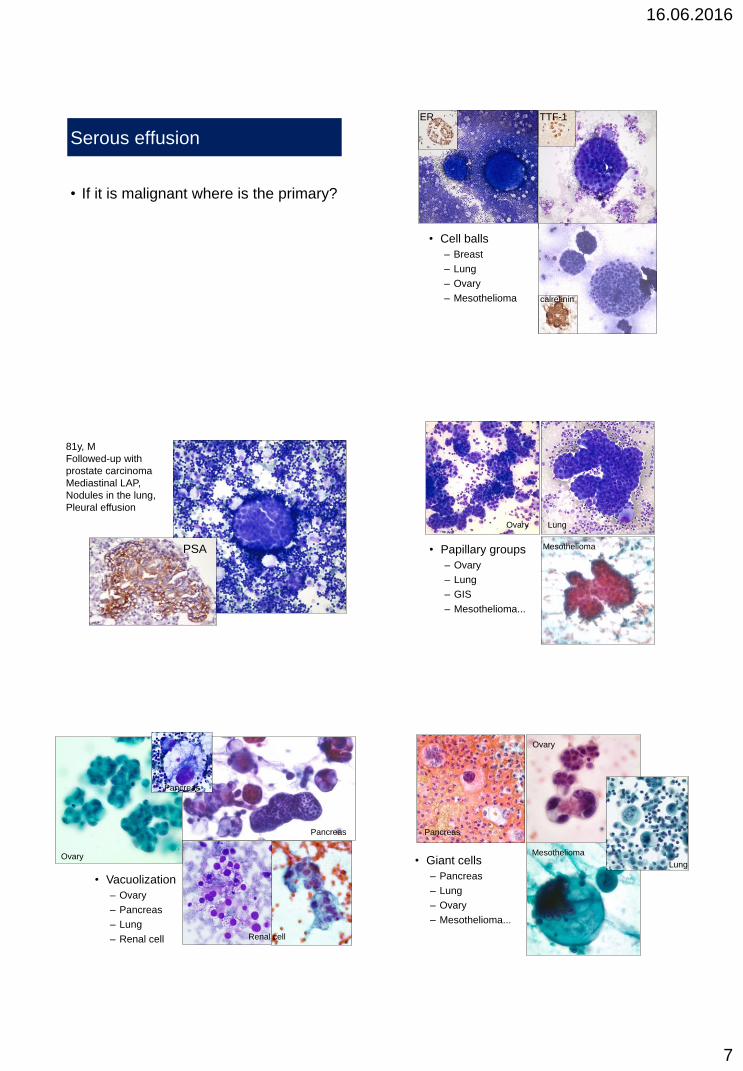
Serous effusion
• If it is malignant where is the primary?
ER TTF-1
• Cell balls
– Breast
– Lung
– Ovary
– Mesothelioma calretinin
PSA
81y, M
Followed-up with
prostate carcinoma
Mediastinal LAP,
Nodules in the lung,
Pleural effusion
• Papillary groups
– Ovary
– Lung
– GIS
– Mesothelioma...
Mesothelioma
Ovary Lung
• Vacuolization
– Ovary
– Pancreas
– Lung
– Renal cell
Pancreas
Ovary
Pancreas
Renal cell
• Giant cells
– Pancreas
– Lung
– Ovary
– Mesothelioma...
Mesothelioma
Ovary
Pancreas
Lung
16.06.2016
8
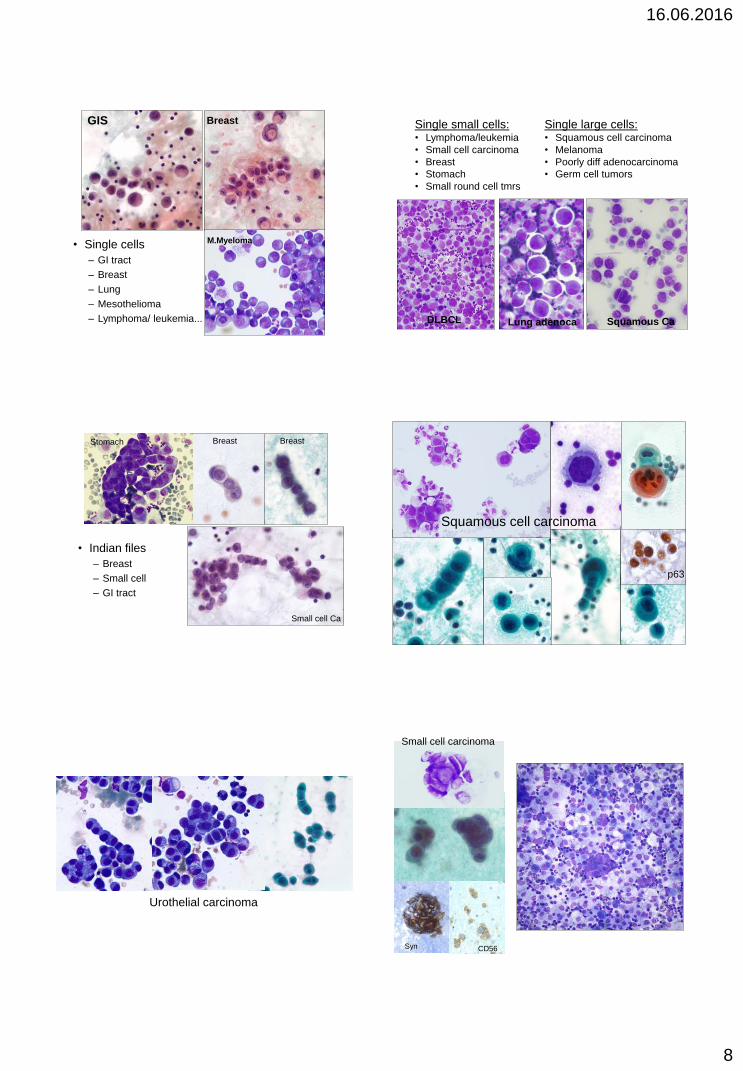
Breast
• Single cells
– GI tract
– Breast
– Lung
– Mesothelioma
– Lymphoma/ leukemia...
M.Myeloma
GIS Single small cells: • Lymphoma/leukemia
• Small cell carcinoma
• Breast
• Stomach
• Small round cell tmrs
Single large cells: • Squamous cell carcinoma
• Melanoma
• Poorly diff adenocarcinoma
• Germ cell tumors
Squamous Ca Lung adenoca DLBCL
• Indian files
– Breast
– Small cell
– GI tract
Breast Breast
Small cell Ca
Stomach
p63
Squamous cell carcinoma
Urothelial carcinoma
CD56 Syn
Small cell carcinoma
16.06.2016
9
Differential diagnosis in the land of mesothelial cells
Mesothelioma
Mesothelial
hyperplasia
Metastatic
carcinoma
IHC
Main
difficulty!
Cytology of malignant mesothelioma
• Absence of a discrete
cell population
• Morphologic continuum
between native
mesothelial cells and
malignant cells
“More and bigger cells in
more and bigger clusters”
Complex groups, three
dimentional aggregates
Cell-in cell arrangements
more common
DeMay
16.06.2016
10
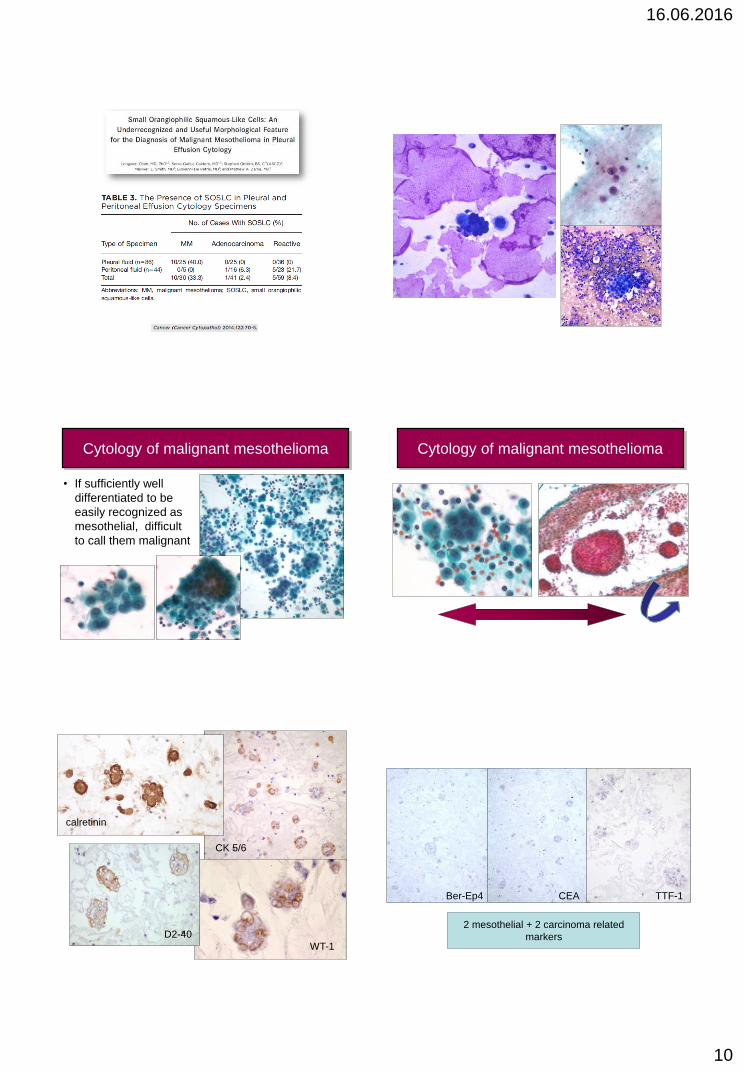
Cytology of malignant mesothelioma
• If sufficiently well
differentiated to be
easily recognized as
mesothelial, difficult
to call them malignant
Cytology of malignant mesothelioma
calretinin
CK 5/6
WT-1
D2-40
Ber-Ep4 CEA TTF-1
2 mesothelial + 2 carcinoma related
markers
16.06.2016
11
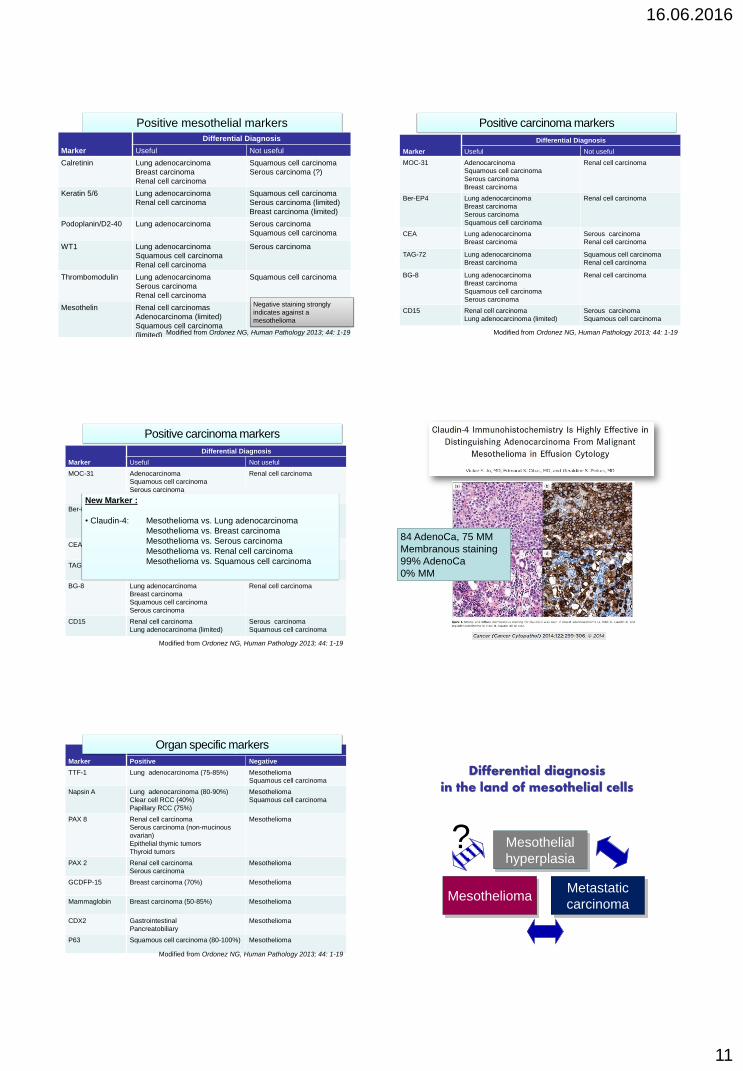
Positive mesothelial markers
Marker
Differential Diagnosis
Useful Not useful
Calretinin Lung adenocarcinoma
Breast carcinoma
Renal cell carcinoma
Squamous cell carcinoma
Serous carcinoma (?)
Keratin 5/6 Lung adenocarcinoma
Renal cell carcinoma
Squamous cell carcinoma
Serous carcinoma (limited)
Breast carcinoma (limited)
Podoplanin/D2-40 Lung adenocarcinoma Serous carcinoma
Squamous cell carcinoma
WT1 Lung adenocarcinoma
Squamous cell carcinoma
Renal cell carcinoma
Serous carcinoma
Thrombomodulin Lung adenocarcinoma
Serous carcinoma
Renal cell carcinoma
Squamous cell carcinoma
Mesothelin Renal cell carcinomas
Adenocarcinoma (limited)
Squamous cell carcinoma
(limited)
Serous carcinoma
Modified from Ordonez NG, Human Pathology 2013; 44: 1-19
Negative staining strongly
indicates against a
mesothelioma
Marker
Differential Diagnosis
Useful Not useful
MOC-31 Adenocarcinoma
Squamous cell carcinoma
Serous carcinoma
Breast carcinoma
Renal cell carcinoma
Ber-EP4 Lung adenocarcinoma
Breast carcinoma
Serous carcinoma
Squamous cell carcinoma
Renal cell carcinoma
CEA Lung adenocarcinoma
Breast carcinoma
Serous carcinoma
Renal cell carcinoma
TAG-72 Lung adenocarcinoma
Breast carcinoma
Squamous cell carcinoma
Renal cell carcinoma
BG-8 Lung adenocarcinoma
Breast carcinoma
Squamous cell carcinoma
Serous carcinoma
Renal cell carcinoma
CD15 Renal cell carcinoma
Lung adenocarcinoma (limited)
Serous carcinoma
Squamous cell carcinoma
Positive carcinoma markers
Modified from Ordonez NG, Human Pathology 2013; 44: 1-19
Marker
Differential Diagnosis
Useful Not useful
MOC-31 Adenocarcinoma
Squamous cell carcinoma
Serous carcinoma
Breast carcinoma
Renal cell carcinoma
Ber-EP4 Lung adenocarcinoma
Breast carcinoma
Serous carcinoma
Squamous cell carcinoma
Renal cell carcinoma
CEA Lung adenocarcinoma
Breast carcinoma
Serous carcinoma
Renal cell carcinoma
TAG-72 Lung adenocarcinoma
Breast carcinoma
Squamous cell carcinoma
Renal cell carcinoma
BG-8 Lung adenocarcinoma
Breast carcinoma
Squamous cell carcinoma
Serous carcinoma
Renal cell carcinoma
CD15 Renal cell carcinoma
Lung adenocarcinoma (limited)
Serous carcinoma
Squamous cell carcinoma
Positive carcinoma markers
Modified from Ordonez NG, Human Pathology 2013; 44: 1-19
New Marker :
• Claudin-4: Mesothelioma vs. Lung adenocarcinoma
Mesothelioma vs. Breast carcinoma
Mesothelioma vs. Serous carcinoma
Mesothelioma vs. Renal cell carcinoma
Mesothelioma vs. Squamous cell carcinoma
84 AdenoCa, 75 MM
Membranous staining
99% AdenoCa
0% MM
Marker
Organ
Positive Negative
TTF-1 Lung adenocarcinoma (75-85%) Mesothelioma
Squamous cell carcinoma
Napsin A Lung adenocarcinoma (80-90%)
Clear cell RCC (40%)
Papillary RCC (75%)
Mesothelioma
Squamous cell carcinoma
PAX 8 Renal cell carcinoma
Serous carcinoma (non-mucinous
ovarian)
Epithelial thymic tumors
Thyroid tumors
Mesothelioma
PAX 2 Renal cell carcinoma
Serous carcinoma
Mesothelioma
GCDFP-15 Breast carcinoma (70%) Mesothelioma
Mammaglobin Breast carcinoma (50-85%) Mesothelioma
CDX2 Gastrointestinal
Pancreatobiliary
Mesothelioma
P63 Squamous cell carcinoma (80-100%) Mesothelioma
Organ specific markers
Modified from Ordonez NG, Human Pathology 2013; 44: 1-19
Differential diagnosis in the land of mesothelial cells
Mesothelioma
Mesothelial
hyperplasia
Metastatic
carcinoma
?
16.06.2016
12
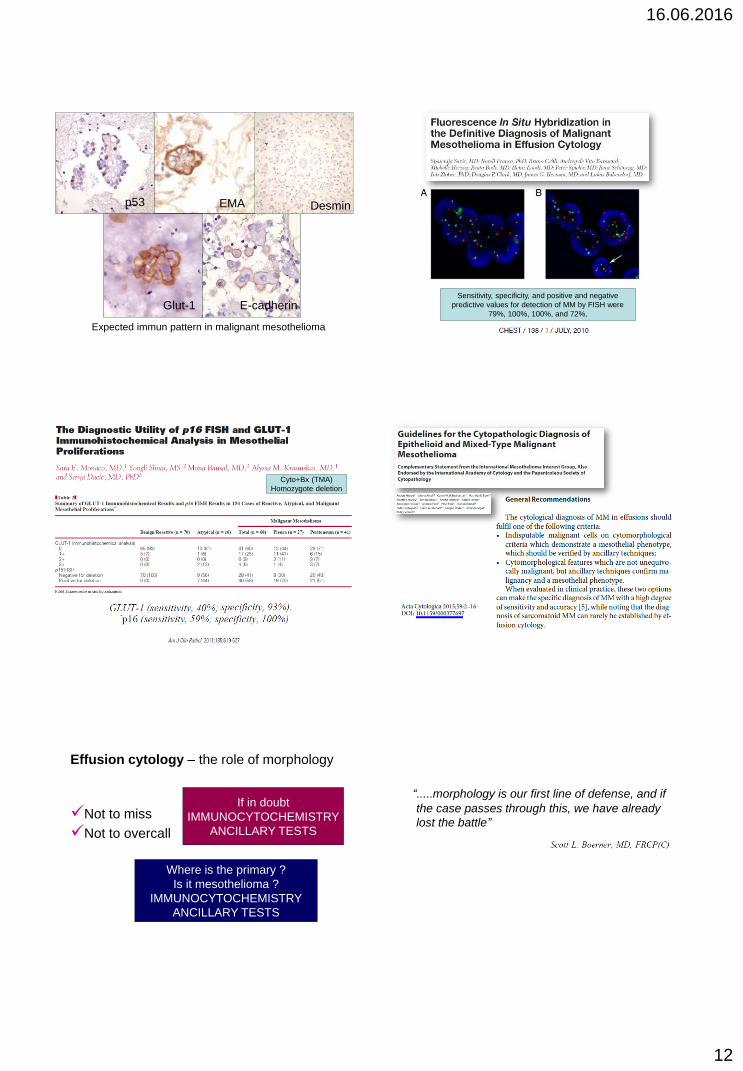
EMA Desmin
Expected immun pattern in malignant mesothelioma
Glut-1
p53
E-cadherin Sensitivity, specificity, and positive and negative
predictive values for detection of MM by FISH were
79%, 100%, 100%, and 72%,
Cyto+Bx (TMA)
Homozygote deletion
Effusion cytology – the role of morphology
Not to miss
Not to overcall
Where is the primary ?
Is it mesothelioma ?
IMMUNOCYTOCHEMISTRY
ANCILLARY TESTS
If in doubt
IMMUNOCYTOCHEMISTRY
ANCILLARY TESTS
“.....morphology is our first line of defense, and if
the case passes through this, we have already
lost the battle”

16.06.2016
13
“.....morphology is our first line of defense, and if
the case passes through this, we have already
lost the battle”
“.....immunocytochemistry adds great value to our
interpretation, and may be the only tool to save
the patient ”
NOT
always