serious paracetamol poisoning results liver transplantation · paracetamol poisoning is the most...
TRANSCRIPT

Gut 1994; 35: 809-814
Serious paracetamol poisoning and the results ofliver transplantation
D J Mutimer, R C S Ayres, J M Neuberger, M H Davies, J Holguin, J A C Buckels,A D Mayer, P McMaster, E Elias
AbstractParacetamol poisoning is the mostcommon cause of fulminant liver failurein the United Kingdom. An accurateassessment of prognosis at the time ofreferral will allow the appropriate appli-cation of liver transplantation in thissetting. The outcome of 92 patientsconsecutively admitted to a specialist liverunit with severe poisoning has beenexamined. In patients who did not have a
transplant, a fatal outcome was seen for26/82 (32%), and was associated with latepresentation, coma grade, prothrombintime prolongation, metabolic acidosis,and renal dysfunction. Cerebral oedema,and sepsis were responsible for mostdeaths. Prognostic criteria defined atKing's College Hospital seemed to predictthe outcome ofpatients who did not have a
transplant managed on the Birminghamliver unit. Seventeen patients were listedfor transplantation, 10 had liver trans-plantation, and seven of 10 survived.Seven were listed but not transplanted,and one of seven survived. Psychologicalrehabilitation of patients who had a
transplant has not proved difficult. Theseresults suggest a role for liver transplanta-tion in the management of selectedpatients with paracetamol poisoning.(Gut 1994; 35: 809-814)
liver Unit, QueenElizabeth Hospital,Edgbaston,BirminghamD J MutimerR C S AyresJM NeubergerM H DaviesJ HolguinJ A C BuckelsA D MayerP McMasterE Elias
Correspondence to:Dr D J Mutimer, Liver Unit,Queen Elizabeth Hospital,Edgbaston, Birmingham B1 52TH.
Accepted for publication11 October 1993
Paracetamol poisoning is the most common
cause of fulminant liver failure in the UnitedKingdom.1 Most patients present early afterparacetamol poisoning,2 and are effectivelytreated with N-acetylcysteine.3 Late presenta-tion is commonly associated with the develop-ment of liver damage, and may be complicatedby significant nephrotoxicity. An analysis ofpatients presenting to King's College Hospital(KCH) liver unit (between 1973 and 1985)4suggested that the prognosis of patients withsevere hepatotoxicity had improved, and thatthis improvement was independent of specifictreatment used by that unit during this period.More recently, 'late' administration ofN-acetylcysteine - that is, a period greater than12 hours elapsed from poisoning to treatment- has been shown to improve the outcome ofpatients with paracetamol induced fulminanthepatic failure.5 6
Fulminant hepatic failure is now a common
indication for liver transplantation,7 andtransplantation may also improve the prog-nosis of selected patients with paracetamolinduced hepatotoxicity.8 The appropriate
application of liver transplantation in thissetting requires an early and accurate assess-ment of prognosis. Factors predicting theoutcome of patients treated at KCH have beendefined.' 9 10 Advanced coma grade, acidosis,severe and sustained coagulopathy, and renaldysfunction are features that identified patientswith a poor prognosis. Potential problems withpsychological rehabilitation should also beanticipated, and will influence the selection ofpatients for transplantation. Many patientshave a history of impulsive and self-destructivebehaviour. The longterm prognosis of suchpatients with respect to both repeatedself-harm and compliance with treatment isuncertain.We have undertaken a retrospective analysis
of patients treated for paracetamol poisoningin the Birmingham Queen Elizabeth Hospitalliver unit. The association of selected clinicalfeatures and laboratory results with patientoutcome were examined. Prognostic criteriadefined at KCH were assessed in non-transplanted patients treated on theBirmingham liver unit.We report the short term results of liver
transplantation for this indication. Successfullongterm rehabilitation of survivors oftransplantation is also described.
Patients and methodsNinety two patients (51 female) with seriousparacetamol toxicity were admitted to theQueen Elizabeth Hospital liver unit between1 September 1990 and 30 March 1992.These patients represent a few of those whosecondition and prognosis had been discussedwith physicians on the unit, and they wereselected for transfer on the basis of the severityof liver dysfunction or associated complica-tions, or both. Transfer to the liver unit wasgenerally recommended (a) if the prothrombintime (measured in seconds) at the time ofreferral was numerically greater than theinterval (measured in hours) from poisoning tothe time of referral, (b) if the prothrombin timewas in excess of 50 seconds, (c) if metabolicacidosis was confirmed at presentation, and(d) for all patients with establishedencephalopathy.
Referring units were generally advised tointubate and ventilate patients with advancedhepatic coma before transfer. Patientsprogressing to grade 3 coma after transfer wereparalysed, seated, intubated, and ventilated.Central venous lines were inserted in allpatients with significant hepatic or renaldysfunction. Pulmonary artery floatation
809
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from

Mutimer, Ayres, Neuberger, Davies, Holguin, Buckels, Mayer, McMaster, Elias
U,
CO4-0
a1)._
5
0
20-25
Age
Figure 1: Age ofpatients at presentation showing bimodal distribution
catheters were inserted if arterial hypotensionpersisted despite adequate blood volumeexpansion, and continuous arteriovenoushaemodialysis (CAVHD) by a peripheral shuntwas established immediately in oliguricpatients. Episodes of raised intracranialpressure were treated by hyperventilation andintravenous mannitol. Thiopentone infusionwas used for patients with refractory intra-cranial hypertension. All patients received H2receptor blockers. Antibiotic prophylaxis was
not routinely used. When sepsis was eitherproved or suspected, antibiotics were startedimmediately after sampling of specimens formicrobiological culture. Treatment withN-acetylcysteine was not started on the liverunit, but in many cases infusion had beencommenced at the referring hospital. In thesecases, the recommended infusion schedule wascompleted on the liver unit.The median age of the 92 referred patients
was 29 years (range 14-74, 51 female) with a
bimodal distribution (Fig 1). Thirteen patientshad a history of previous parasuicide, andfive of multiple previous suicide attempts.Sixteen had serious premorbid psychiatricdisease (including longstanding depression andalcoholism). In 36 cases the paracetamol over-
dose was clearly an impulsive act, precipitatedmost commonly by relationship or financialproblems. In most cases, however, no clearsingle precipitating event could be identified.
Statistical analysis- data are expressed as
median (range). Statistical comparisonbetween groups was made by Wilcoxon ranksum test and x2 test with Yates's correctionwhere appropriate.
Results
CONDITION AT PRESENTATION ANDMANAGEMENT BEFORE REFERRALThe median interval from the time ofpoisoning to presentation for the 92 patientswas 19 hours (range 9-59). The medianinterval from poisoning to presentation in10 patients who subsequently had livertransplantation was 27 hours (17-43), and innon-transplanted patients was 18 hours(9-59). Non-transplanted patients whosubsequently died presented significantly laterthan those who survived to be discharged fromhospital (p=0 01) (Table I).
Seven patients presented early (within 12hours of poisoning), but four of these were nottreated with N-acetylcysteine. The three treatedpatients experienced significant hepatotoxicitybut survived. Two untreated patients sub-sequently died, and two survived. Two offour untreated patients had measured plasmaparacetamol concentrations below the recom-mended treatment threshold (at five and ninehours respectively) and one subsequently died.There was trend towards improved outcome inthose patients treated at presentation withN-acetylcysteine (mortality in treated patients24%, in untreated patients 42%, p= 0- 1).Table I shows the laboratory results at
the time of presentation. Many patients hadestablished liver failure with encephalopathy atthe time of presentation, and prothrombintime prolongation at the time of presentationwas significantly associated with ultimatepatient outcome (p<0 05).
Arterial pH was measured in only 24patients at the time of initial presentation.Four of these 24 patients subsequently hadliver transplantation, and all were severelyacidotic at the time of presentation. Thepresence of acidosis directly influenced theircandidature for transplantation. The progno-sis of the 20 non-transplanted patients is pos-sibly related to arterial pH at presentation(p = 0 1). In this group of 20 patients, an arte-rial pH<7-30 had a predictive value (forsubsequent death) of about 90%.
TABLE I Clinical and laboratory data of 92 consecutive admissions with paracetamol poisoning
Non-transplants
All patients (92) Transplants (10) Alive (56) Dead (26)
Interval (h)OD-presentation 19 (9-59) [48] 27 (17-43) [6] 17 (9-59) [31]* 24 (16-54) [11]* *p= 0-01OD-liver unit 62 (24-107) [53] 53 (26-70) [7] 62 (24-107) [33] 56 (29-91) [13] NS
PresentationPT 52 (14-180) [45] 54 (29-120) [7] 47 (14-101) [23]* 80 (24-180) [15]* *p<0 05pH 7-29 (6 90-7 47) [24] 6-90-7-16 [4] 7-37 (7-12-7-47) [8] 7-26 (6 90-7-46) [12] p=0-1Creatinine 196 (65-517) [21] 156-304 [3] 316 (65-157) [9] 172 (90-379) [9] NS
QE admissionPT 61 (18-180) [87] 71 (48-125) [10] 58 (18-159) [54] 56 (33-180) [23] NSpH 7-47 (7-18-7-58) [32] 7-18-7-38 [3] 7-47 (7-32-7 58) [23] 7-45 (7 38-7-48) [6] p=0-08Creatinine 147 (62-933) [83] 274 (78-446) [10] 115 (62-933) [521* 263 (85-593) [211* *p= 0-001
*For non-transplanted alive v dead; [ ] number of observations; OD=overdose; PT prothrombin time.
810
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from

Serious paracetamol poisoning and the results of liver transplantation
TABLE II Association ofpeak prothrombin time (PT) andpeak serum creatinine with outcome in non-transplantedpatients
Peak PT <50 50-100 100-150 >150Dead 0 7 11 8Alive 9 28 14 5
Peak creatinine (mcmol/l) <150 150-300 >300Dead 0 3 21Alive 25 10 17
Twelve (60%) of these 20 non-transplantedpatients died. The overall mortality of the 82non-transplanted patients was only 32%(26/82), which is significantly less than themortality seen in these 20 patients who hadarterial pH measured at presentation. It isprobable that arterial pH is more likely to bemeasured at the time of presentation in thosepatients with a poorer prognosis.
CONDITION ON TRANSFER AND MANAGEMENTIN THE LIVER UNITThe median interval from presentation (at thereferring centre) until arrival on the liver unitin Birmingham was 36 hours (range 2-71),and from poisoning to arrival was 62 hours(range 24-107).
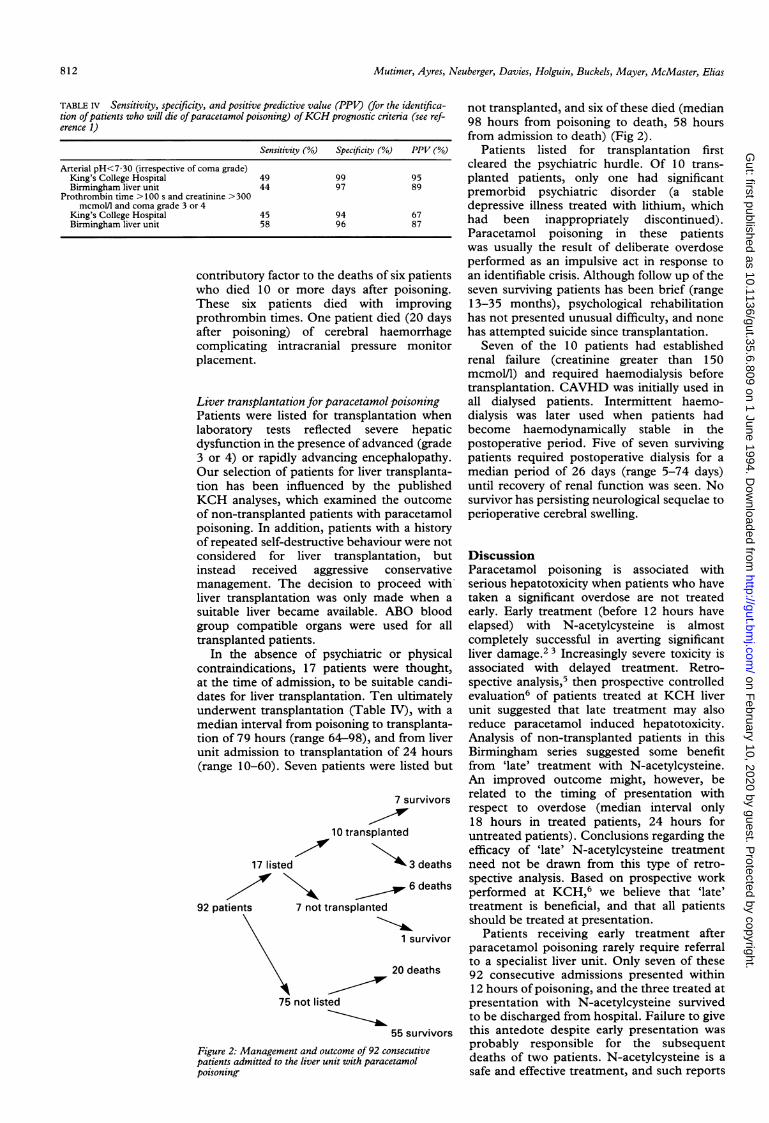
Sixty three (68%) achieved hospitaldischarge, and 29 died. Seventeen patientswere 'listed' for, and 10 of these subsequentlyhad liver transplantation. Seven transplantedpatients survived (median follow up 16months, range 13-35 months on 1 May 1993).Six patients died on the waiting list, and onepatient recovered to be withdrawn from the list(and was eventually discharged). Seventy fivepatients were not listed for transplantation,and 20 died. Nine of these 20 were excludedfrom consideration for liver transplantationbecause of premorbid psychopathology, whichwe considered would prejudice successfulrehabilitation after transplantation. Fivepatients were considered unfit for transplanta-tion at the time of their arrival on the liver unit(aspiration pneumonitis 4, irreversible cerebraloedema 1), two patients had improvingprothrombin times (transplantation feltto be inappropriate), and one patient (74 yearsof age) was too old to be considered forgrafting.
Non-transplanted patientsHepatic coma grade at the time of admissionto the liver unit was significantly associatedwith patient outcome. The mortality of
TABLE III Eight patients had arterialpH measured at both the presenting hospital and onarrival in the liver unit (excluding patients who were ventilated or given bicarbonate)
Patient Presenting Liver unit(age/sex) pH pH Interval Outcome
28/F 7-33 (47) 7-45 (65) 18 Dead/non-transplanted17/M 7-32 (12) 7-46 (62) 50 Alive/non-transplanted43/F 7-35 (38) 7 50 (74) 36 Alive/non-transplanted21/F 7-12 (14) 7-32 (24) 10 Alive/non-transplanted48/M 6-99 (36) 7-18 (42) 6 Dead/transplanted50/F 7-45 (16) 7-42 (54) 38 Dead/non-transplanted27/F 7-44 (NK) 7-48 (NK) 10 Dead/non-transplanted19/F 6-90 (24) 7-21 (26) 2 Alive/transplanted
Hours after overdose shown in parentheses; NK=time of overdose not known.
non-transplanted patients admitted with grade4 coma was in excess of 60% (16/26), and nodeaths were seen in 26 patients who were notencephalopathic at the time of admission.Most patients with severe coagulopathy
were given fresh frozen plasma after presenta-tion, before arrival on the liver unit. Admissionprothrombin time values were not statisticallyassociated with the outcome of the 82non-transplanted patients. Peak prothrombintime (measured at any time between presenta-tion and death or discharge) was stronglyassociated with patient outcome. Stratificationof peak prothrombin time values (Table II)shows this association. No deaths were seenin the group with peak prothrombin time<50 seconds, and 62% mortality (8/13)was associated with peak values greater than150 seconds. Peak prothrombin time >100seconds was associated with 50% mortality.
Arterial pH values affected by the admini-stration ofbicarbonate solutions and by the useof mechanical ventilation have not beenincluded in the following analyses.
Arterial pH values at the time of admissionto the liver unit were significantly higher thanthose recorded at the time of presentation(median 7.47 v 7-29, p=0.02) (Table I).Paired values - that is, at presentation and attime of admission to liver unit - were availablefor eight patients, and pH increased during thisinterval in 7/8 (Table III).At least one arterial pH measurement was
made for 48/82 non-transplanted patients. Anexamination of the first arterial pH measure-ment for each of these patients confirmed thatthe presence of metabolic acidosis was stronglyassociated with outcome - mortality 11/13when pH<7K35. The exact interval frompoisoning to measurement of arterial pH wasknown in only 34 of 82 non-transplantedpatients. Most measurements (21/34) wereperformed at least 48 hours after poisoning.Only four measurements were made within 18hours of poisoning. Two of these four patientssurvived - both were acidotic at presentation,and both were treated with N-acetylcysteine.
Renal dysfunction (reflected by raised serumcreatinine) at the time of admission to the liverunit was strongly associated with subsequentmortality of non-transplanted patients. Peakserum creatinine was also associated withpatient outcome, an association shown bystratification of peak creatinine values (TableII). Fifty per cent mortality was associated withpeak serum creatinine greater than 300mcmol/l, and no mortality was seen whenserum creatinine did not exceed 150 mcmol/l.
Thirty one non-transplanted patientsrequired haemodialysis and 18/31 (58%)subsequently died. The mortality among51 patients who did not require dialysis wasonly 16% (p<0 01).
Cerebral oedema was the predominantcause of death in non-transplanted patients.Sixteen of 20 patients who died within 10 daysof poisoning had cerebral oedema, whichwas refractory to treatment with mannitol,hyperventilation, and thiopentone. Sepsis,most often pulmonary, was an important
811
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from
Mutimer, Ayres, Neuberger, Davies, Holguin, Buckels, M4ayer, McMaster, Elias
TABLE IV Sensitivity, specificity, and positive predictive value (PPV) (for the identifica-tion ofpatients who will die ofparacetamol poisoning) ofKCH prognostic criteria (see ref-erence 1)
Sensitivity (Oo) Specificity (Go) PPV (/0)
Arterial pH<7-30 (irrespective of coma grade)King's College Hospital 49 99 95Birmingham liver unit 44 97 89
Prothrombin time >100 s and creatinine >300mcmol/l and coma grade 3 or 4
King's College Hospital 45 94 67Birmingham liver unit 58 96 87
contributory factor to the deaths ofwho died 10 or more days afterThese six patients died withprothrombin times. One patient diafter poisoning) of cerebral hcomplicating intracranial pressuiplacement.
Liver transplantation for paracetamolPatients were listed for transplantlaboratory tests reflected sevedysfunction in the presence of advai3 or 4) or rapidly advancing encelOur selection of patients for liver 1tion has been influenced by theKCH analyses, which examined tlof non-transplanted patients with rpoisoning. In addition, patients wiof repeated self-destructive behavioconsidered for liver transplantinstead received aggressive cmanagement. The decision to prliver transplantation was only masuitable liver became available. Igroup compatible organs were utransplanted patients.
In the absence of psychiatriccontraindications, 17 patients weat the time of admission, to be suildates for liver transplantation. Telunderwent transplantation (Tablemedian interval from poisoning totion of 79 hours (range 64-98), aniunit admission to transplantation(range 10-60). Seven patients wer
10 transplar
17 listed
92 patients 7 not transplanted
75 not listed
Figure 2: Management and outcome of 92 ccpatients admitted to the liver unit with paracpoisoning-
six patientspoisoning.improving
ed (20 daysaemorrhagere monitor
poisoningtation whenre hepaticnced (gradephalopathy.transplanta-published
he outcome?aracetamolith a historyur were not
not transplanted, and six of these died (median98 hours from poisoning to death, 58 hoursfrom admission to death) (Fig 2).
Patients listed for transplantation firstcleared the psychiatric hurdle. Of 10 trans-planted patients, only one had significantpremorbid psychiatric disorder (a stabledepressive illness treated with lithium, whichhad been inappropriately discontinued).Paracetamol poisoning in these patientswas usually the result of deliberate overdoseperformed as an impulsive act in response toan identifiable crisis. Although follow up of theseven surviving patients has been brief (range13-35 months), psychological rehabilitationhas not presented unusual difficulty, and nonehas attempted suicide since transplantation.
Seven of the 10 patients had establishedrenal failure (creatinine greater than 150mcmol/1) and required haemodialysis beforetransplantation. CAVHD was initially used inall dialysed patients. Intermittent haemo-dialysis was later used when patients hadbecome haemodynamically stable in thepostoperative period. Five of seven survivingpatients required postoperative dialysis for amedian period of 26 days (range 5-74 days)until recovery of renal function was seen. Nosurvivor has persisting neurological sequelae toperioperative cerebral swelling.
:ation, but Discussion-onservative Paracetamol poisoning is associated withroceed with serious hepatotoxicity when patients who haveide when a taken a significant overdose are not treatedABO blood early. Early treatment (before 12 hours haveised for all elapsed) with N-acetylcysteine is almost
completely successful in averting significantor physical liver damage.2 3 Increasingly severe toxicity isre thought, associated with delayed treatment. Retro-table candi- spective analysis,5 then prospective controlledn ultimately evaluation6 of patients treated at KCH liverIV), with a unit suggested that late treatment may alsotransplanta- reduce paracetamol induced hepatotoxicity.d from liver Analysis of non-transplanted patients in thisof 24 hours Birmingham series suggested some benefitre listed but from 'late' treatment with N-acetylcysteine.
An improved outcome might, however, be7 survivors related to the timing of presentation with
respect to overdose (median interval only18 hours in treated patients, 24 hours for
nited untreated patients). Conclusions regarding theefficacy of 'late' N-acetylcysteine treatment
>3 deaths need not be drawn from this type of retro-spective analysis. Based on prospective work
6 deaths performed at KCH,6 we believe that 'late'treatment is beneficial, and that all patientsshould be treated at presentation.
1 survivor Patients receiving early treatment afterparacetamol poisoning rarely require referralto a specialist liver unit. Only seven of these
20 deaths 92 consecutive admissions presented within12 hours of poisoning, and the three treated atpresentation with N-acetylcysteine survivedto be discharged from hospital. Failure to give
55 survivors this antedote despite early presentation was
onsecutive probably responsible for the subsequent-etamol deaths of two patients. N-acetylcysteine is a
safe and effective treatment, and such reports
812
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from

Serious paracetamol poisoning and the results of liver transplantation
would support a policy of 'treatment for all',at least until the development of significanthepatotoxicity has been excluded (invariablypresent within 48 hours of poisoning). Such a
policy would also provide an opportunity forpsychological counselling and intervention.Most cases of poisoning result from
deliberate overdose. Some patients havepremorbid psychiatric disturbance, but in mostcases the overdose is precipitated by relation-ship or financial problems. All potential treat-ment options, including liver transplantation,should be considered for these patients.The mortality seen in patients not under-going liver transplantation was 32% (26/82).Twenty one patients did not develop hepaticencephalopathy. The mortality seen inpatients with fulminant hepatic failure(which by definition requires the presence ofencephalopathy) was 41% (25/61). Themortality seen in patients progressing toadvanced coma (grade 3 or 4) was 61%.Outcome was clearly related to grade ofencephalopathy, both at presentation, and atthe time of admission to the liver unit.O'Grady et al saw a death rate of 66% in a
comparable group of patients with advancedcoma admitted to KCH liver unit during a
12 year period.1In an attempt to define those patients who
might benefit from the application of innova-tive treatment, prognostic factors have beendefined for patients presenting with paraceta-mol poisoning. The severity of coagulopathyas reflected by peak prothrombin time,'prothrombin time rising on day 4,9 and admis-sion factor VIII/V ratio10 were all found to haveprognostic value in patients with hepatic comatreated at KCH after paracetamol overdose.Admission factor V values less than 10% ofnormal also predicted outcome in the same
setting. 10
In patients referred to the Birmingham liverunit, prothrombin times (both presentationand peak values) were significantly higher innon-transplanted patients who subsequentlydied when compared with those who survived(Tables I and II). Liver unit admissionprothrombin time values were frequentlyaffected by the administration of fresh frozenplasma in the referring hospital before transfer,and did not distinguish fatal from non-fatalpoisoning. Despite the enthusiasm of some
liver units for its measurement,10 11 factor V
values are not routinely measured in patientswith fulminant liver failure managed in theBirmingham liver unit.O'Grady et al found that admission (to
the liver unit) arterial pH provides importantprognostic information irrespective of coma
grade. In that retrospective analysis, metabolicacidosis (pH<7-30) had a 95% predictive valuefor subsequent death. We have seen a fatal out-
come for 9/10 patients with an arterialpH<7-30 measured at some time after presen-
tation. Our analysis highlights potentialproblems in the use of arterial pH measure-
ments to predict outcome. We have shown thatarterial pH was more likely to be measured inpatients with a bad outcome. The prognosticvalue of prospectively collected data, withrespect to both sensitivity and predictivevalue, will probably be different. Unfor-tunately, arterial pH measurement lackssensitivity (for prediction of subsequent death),and many patients with admission arterialpH>7-30 will subsequently die. Metabolic aci-dosis seems to be an early and transient phe-nomenon after paracetamol poisoning. TableIII clearly shows the propensity of metabolicacidosis to correct without treatment as illus-trated by the paired measurements.The prognostic value of arterial pH
measurement is dependent on the timingof that measurement with respect to the time ofpoisoning. Because of greater awareness of itsprognostic value, arterial pH will be measuredmore commonly at the time of initial presenta-tion. The extrapolation of the KCH criterion tothis early period is probably not justified. Forexample, arterial pH was recorded within18 hours of admission in only four of 82 non-
transplanted patients in the Birmingham series.Two of these four were acidotic (pH< 7-35) butsurvived. Both were treated at presentation withN-acetylcysteine. The predictive value of earlyarterial pH measurements may be significantlyless than that defined by O'Grady, and may beinfluenced by treatment with N-acetylcysteine.Despite these criticisms, persisting that is, 48hours and severe metabolic acidosis hasimportant prognostic value, and may provide an
opportunity for early listing for livertransplantation (before the onset of hepaticencephalopathy).
O'Grady et al have proposed criteria thatcan be applied to the selection of patientswith paracetamol poisoning for liver transplant-
TABLE V Characteristics of 10 transplanted patients on admission to the liver unit and before liver transplantation (worst values* recorded at either QE or
presenting hospital)
Intervals QE admission Worst value*
OD- QE-Age/sex Outcome presentation OD-QE transplantation Coma PT pH Creatinine Coma PT pH Creatinine
38/F A 34 50 48 1 76* 7-38 319 4 100 7-38 D32/M A 17 68 22 4 102 Vent 134 4 172 Vent 15419/F A 18 65 14 3 95 7-34 114 4 140 7-34 11431/F A NK NK 20 4 66* Vent 446 4 123 Vent D20/F A 24 53 11 4 88* Vent 284 4 160 Vent D29/M A 43 70 20 4 48* Vent 263 4 92 7-35 D19/F A 24 26 43 1 59 7-21 126 3 300 6-90 D29/M D NK NK 35 4 125* Vent 423 4 136 7-08 D47/M D 36 41 27 3 62* 7-18 331 4 > 120 6-99 D23/F D NK NK 60 4 49* Vent 113 4 > 120 7-16 158
D=Haemodialysis commenced before liver transplantation; *fresh frozen plasma given by referring hospital before transfer; vent-patient ventilated; NK=time ofoverdose not known.
813
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from

814 Mutimer, Ayres, Neuberger, Davies, Holguin, Buckels, Mayer, McMaster, Elias
ation.I We have examined the sensitivity andpredictive value of these criteria in forecastingthe outcome of the 82 non-transplantedpatients admitted to the Birmingham liver unit(Table IV). Both KCH criteria are highlypredictive of the outcome of patients managedin the Birmingham liver unit. Seven of 10 trans-planted patients also fulfilled these criteria(Table V).The prospective definition of prognostic
criteria and improved patient selection forliver transplantation remain important chal-lenges for hepatologists. The prospectivecollection of clinical and laboratory data, and atime dependent analysis of these data, mayimprove the sensitivity and predictive value ofpatient selection criteria. Transplanted patients(selection usually based on existing criteria)should be excluded from these analyses, as theirinclusion simply reinforces, and cannotimprove existing prognostic formulas.Most liver transplant units are convinced
that liver transplantation has significantlyimproved the outcome of selected patientswith fulminant hepatic failure. Despite calls fora controlled trial,12 it seems unlikely that livertransplantation will be submitted to controlledevaluation in the management of patientswith life threatening paracetamol toxicity.In the absence of controlled evaluation, thevalidity of patient selection policies is possiblybest reflected by the outcome of those patientswho are 'listed' but not transplanted. Thesepatients may either die, or show signs ofrecovery before the availability of a donororgan. Seventeen patients admitted to theBirmingham liver unit with severe paracetamolpoisoning were listed for transplantation.Seven of 10 transplanted patients survived, butonly one of seven non-transplanted patientssurvived to be discharged from hospital(p<005). Importantly, the interval fromlisting to death in non-transplanted patients(median 58 hours) was not less than theinterval from listing to transplantation (median24 hours).The KCH liver unit criteria were prospec-
tively applied in that centre to the selection ofsuitable transplantation candidates.8 Twentynine of 66 consecutive patients had indicatorsof a poor prognosis. Six of 29 ultimately hadliver transplantation, and 4/6 survived. Twentythree were not given a transplant, and only four(17%) survived.These comparisons indirectly support
selection criteria (for liver transplantation)applied to patients referred to Birmingham andKCH with severe paracetamol poisoning.Some patients are clearly unsuitable for
liver transplantation. Patients with serious
premorbid psychiatric disease should bemanaged conservatively. Successful longtermrehabilitation of the patient with a history ofrepeated self-injury seems unlikely.
Other patients have developed complica-tions that would mitigate against recovery aftertransplantation. Some complications of liverfailure, such as aspiration pneumonitis, arepossibly preventable. Patients with advancedhepatic coma should undergo endotrachealintubation before transfer, and should beaccompanied by a senior anaesthetist. Livertransplantation could not be considered atreatment option for four patients withaspiration pneumonitis. Three of these fouraspirated during transfer from the referringhospital to the liver unit. Experienced liverunits should be consulted early, permittingpatient transfer before the development ofencephalopathy and incipient cerebraloedema.
Liver transplantation is now an importanttreatment option for selected patients withfulminant liver failure secondary to para-cetamol poisoning.
The authors wish to acknowledge the contribution made to thecare of these patients by the junior medical and surgical staff,and by the nursing staff working on the liver unit.
1 O'Grady JG, Alexander GJM, Hayllar KM, Williams R.Early indicators of prognosis in fulminant hepatic failure.Gastroenterology 1989; 97: 439-45.
2 Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH.Efficacy of N-acetylcysteine in the treatment ofacetaminophen overdose. N Engl J7 Med 1988; 319:1557-62.
3 Prescott LF, Illingworth RN, Critchley JAJH, Stewart MJ,Adam RD, Proudfoot AT. Intravenous N-acetylcysteine:the treatment of choice for paracetamol poisoning. BMJ1979; 2:1079-100.
4 O'Grady JG, Gimson AES, O'Brien CJ, Pucknell A,Hughes RD, Williams R. Controlled trials of charcoalhemoperfusion and prognostic factors in fulminanthepatic failure. Gastroenterology 1988; 94: 1228-30.
5 Harrison PM, Keays R, Bray GP, Alexander GJM, WilliamsR. Improved outcome of paracetamol-induced fulminanthepatic failure by late administration of acetylcysteine.Lancet 1990; 335: 1572-3.
6 Keays R, Harrison PM, Wendon JA, Forbes A, Gove C,Alexander GJM, et al. Intravenous acetylcysteine in parac-etamol induced fulminant hepatic failure: a prospectivecontrolled trial. BMJ 1991; 303: 1026-9.
7 Mutimer DJ, Elias E. Liver transplantation for fulminanthepatic failure. In: Boyer J, Ockner R, eds. Progress in liverdiseases. Philadelphia: WB Saunders, 1992; 10: 349-67.
8 O'Grady JG, Wendon J, Tan KC, Potter D, Cottam S,Cohen AT, et al. Liver transplantation after paracetamoloverdose. BMJ 1991; 303: 221-3.
9 Harrison PM, O'Grady JG, Keays RT, Alexander GJM,Williams R. Serial prothrombin time as prognostic indica-tor in paracetamol induced fulminant hepatic failure.BMJ 1990; 301: 964-6.
10 Pereira LMMB, Langley PG, Hayllar KM, Tredger JM,Williams R. Coagulation factor V and VIII/V ratio aspredictors of outcome in paracetamol induced fulminanthepatic failure: relation to other prognostic indicators. Gut1992; 33: 98-102.
11 Samuel D, Bismuth H. Selection criteria and resultsof orthotopic liver transplantation in fulminant andsubfulminant hepatitis. In: Williams R, Hughes RD, eds.Acute liverfailure. Proceedings of the eleventh BSG SK&FIntemational Workshop. 1990: 73-7.
12 Chapman RW, Forman D, Peto R, Smallwood R. Livertransplantation for acute hepatic failure. Lancet 1990;335:32-5.
on February 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.809 on 1 June 1994. D
ownloaded from