serial changes in the biophysical profile in patients undergoing cervical ripening with a controlled...
TRANSCRIPT

The Journal of Maternal-Febl Medicine 8:&11 (1999)
Serial Changes in the Biophysical Profile in Patients Undergoing Cervical Ripening
With a Controlled Release PGE2 Vaginal Pessary Erol Amon,' Kathy Fossick, and Baha Sibai
Department of Obstetrics and Gynecology, St. louis University School of Medicine, St. louis, Missouri
Objective: The purpose of this study was to evaluate the effects of exogenous administration of PGEZ upon the components of the biophysical profile. Methods: The study group included 17 nulliparas at 238 weeks gestation, with a Bishop score of 1 4 , requiring induction of labor. A controlled release vaginal pessary containing 10 mg of PGE2, designed to release hormones at -0.8 mg per hour in vitro, was used for 12 hours of cervical ripening. The BPP was performed by the same sonographer at three intervals: prior to pessary insertion, at 6 hours, and 12 hours. Results: None of these patients had membrane rupture or went into spontaneous labor during the ripening process. All patients subsequently required amniotomy and oxytocin. The proportion of patients scoring 2 points for fetal breathing movements decreased from 59% at baseline to 0% at 12 hours, P < 0.0005, and the proportion of patients with fetal body movements decreased from 100% at baseline to 25% at 12 hours, P < 0.0005. However, the other components of the biophysical profile were not affected. The mean maternal plasma PGE2 metabolite concentrations were 235 pg/ml, 475 pg/inl, and 466 pdml at 0,6 and 12 hours, respectively, P < 0.005. Conclusions: In term patients, vaginal administration of the PGEZ pessary was associated with improved Bishop score over 12 hours and significant increases in maternal plasma PGEM levels at 6 hours and 12 hours. These changes were inversely related to fetal breathing and body movements. J. Matern.-Fetal Med. 1999;8:8-1 I .
1999 Wile)..-Liss, Inc.
Key words: prostaglandin E2; fetal breathing movements; fetal body movements; biophysical profile; cervical ripening
INTRODUCTION The events leading to parturition in the human are still
poorly understood. There is a growing body of medical literature that supports the view that prostaglandins, espe- cially prostaglandin E2 (PGE2) and F2 alpha (PGF2 alpha), play critical roles in the events leading to labor and delivery [l]. The clinical use of various PGE2 formulations for cervical ripening and for labor induction in pregnant women at term has been an acceptable clinical practice [2].
The biophysical profile assessment of fetal well-being consists of five parameters [3]. The relationship of labor to these parameters have recently been evaluated in the human 141. There is an inverse relationship between fetal breathing movements and labor in both preterm animals [5] and preterm humans [6]. In fetal sheep, there is also a strong inverse relationship between fetal breathing movements and PGEZ infusions and fetal plasma PGE2 concentra- tions [7].
The effect of PGEZ on the biophysical profile in the human fetus has not been well characterized. Some clini- cians use the biophysical profile to assess fetal well-being during cervical ripening, when the fetal heart rate monitor cannot provide convincing evidence of well-being. The purpose of this study is to evaluate the effects of the changing hormonal milieu due to exogenously administered PGEZ upon the components of the biophysical profile.
SUBJECTS AND METHODS Twenty-five women who met strict criteria to receive
intravaginal prostaglandin were eligible for this study. The
*Correspondence to: Erol Amon, M.D., St. Louis University School of Medicine, Department of Obstetrics and Gynecology, 6420 Clayton Road, St. Louis, MO 631 17.
Received 10 February 1998; revised 18 June 1998; accepted 20 July 1998
D 1999 Wiley-Liss, Inc.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
BIOPHYSICAL PROFILE AND PGE2 9
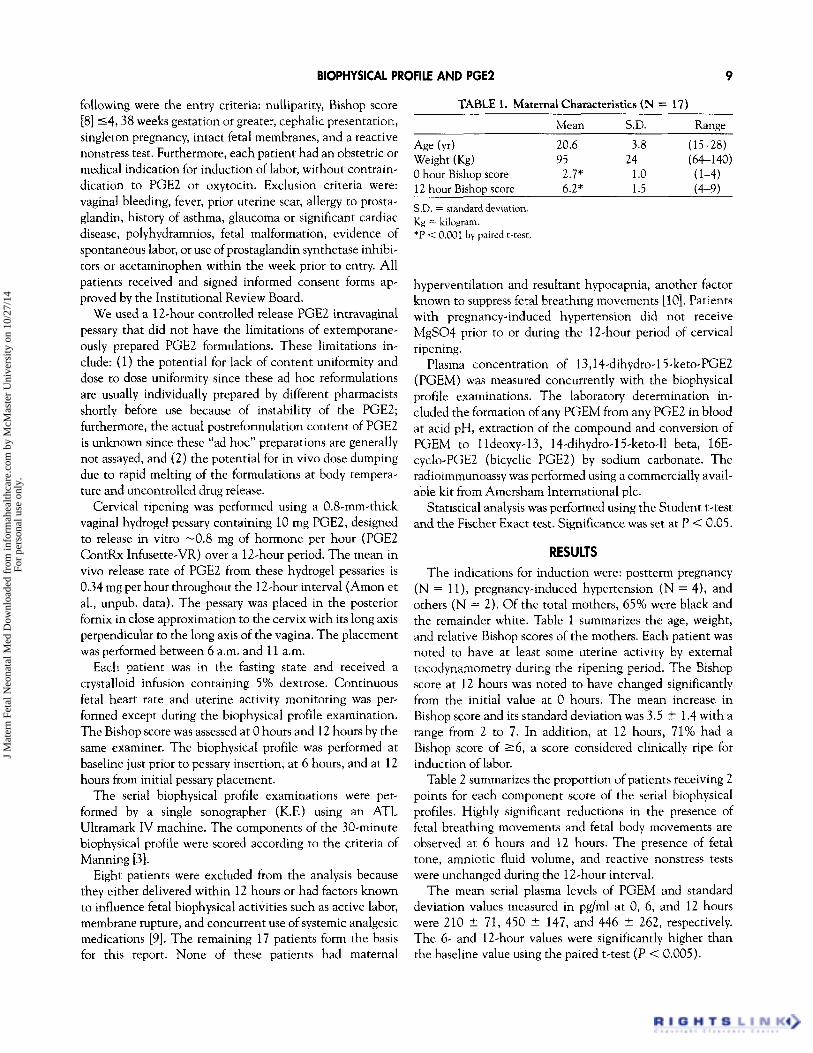
following were the entry criteria: nulliparity, Bishop score [8] 14,38 weeks gestation or greater, cephalic presentation, Mean S.D. Range
20.6 3.8 (15-28) singleton pregnancy, intact fetal membranes, and a reactive
95 24 (64-1 40) nonstress test. Furthermore, each patient had an obstetric or
2.7* 1 .o (1-4) medical indication for induction of labor, without contrain-
6.2* 1.5 (4-9) dication to PGEZ or oxytocin. Exclusion criteria were: vaginal bleeding, fever, prior uterine scar, allergy to prosta- glandin, history of asthma, glaucoma or significant cardiac disease, polyhydramnios, fetal malformation, evidence of
TABLE 1. Maternal Characteristics (N = 17)
Age (v) Weight (Ks)
hour Bishop Score 12 hour Bishop Score
S.D. = standard deviation. K~ = kilogram. *P < 0.001 by paired t-test.
spontaneous labor, or use of prostaglandin synthetase inhibi- tors or acetaminophen within the week prior to entry. All patients received and signed informed consent forms ap- proved by the Institutional Review Board.
We used a 12-hour controlled release PGE2 intravaginal pessary that did not have the limitations of extemporane- ously prepared PGEZ formulations. These limitations in- clude: (1) the potential for lack of content uniformity and dose to dose uniformity since these ad hoc reformulations are usually individually prepared by different pharmacists shortly before use because of instability of the PGE2; furthermore, the actual postreformulation content of PGEZ is unknown since these “ad hoc” preparations are generally not assayed, and (2) the potential for in vivo dose dumping due to rapid melting of the formulations at body tempera- ture and uncontrolled drug release.
Cervical ripening was performed using a 0.8-mm-thick vaginal hydrogel pessary containing 10 mg PGE2, designed to release in vitro -0.8 mg of hormone per hour (PGE2 ContRx Infusette-VR) over a 12-hour period. The mean in vivo release rate of PGEZ from these hydrogel pessaries is 0.34 mg per hour throughout the 12-hour interval (Amon et al., unpub. data). The pessary was placed in the posterior fornix in close approximation to the cervix with its long axis perpendicular to the long axis of the vagina. The placement was performed between 6 a.m. and 11 a.m.
Each patient was in the fasting state and received a crystalloid infusion containing 5% dextrose. Continuous fetal heart rate and uterine activity monitoring was per- formed except during the biophysical profile examination. The Bishop score was assessed at 0 hours and 12 hours by the same examiner. The biophysical profile was performed at baseline just prior to pessary insertion, at 6 hours, and at 12 hours from initial pessary placement.
The serial biophysical profile examinations were per- formed by a single sonographer (K.F.) using an ATL Ultramark IV machine. The components of the 30-minute biophysical profile were scored according to the criteria of Manning [3].
Eight patients were excluded from the analysis because they either delivered within 12 hours or had factors known to influence fetal biophysical activities such as active labor, membrane rupture, and concurrent use of systemic analgesic medications [9]. The remaining 17 patients form the basis for this report. None of these patients had maternal
hyperventilation and resultant hypocapnia, another factor known to suppress fetal breathing movements [lo]. Patients with pregnancy-induced hypertension did not receive MgS04 prior to or during the 12-hour period of cervical ripening.
Plasma concentration of 13,14-dihydro-15-keto-PGE2 (PGEM) was measured concurrently with the biophysical profile examinations. The laboratory determination in- cluded the formation of any PGEM from any PGEZ in blood at acid pH, extraction of the compound and conversion of PGEM to 1 ldeoxy-13, 14-dihydro-15-keto-11 beta, 16E- cyclo-PGE2 (bicyclic PGE2) by sodium carbonate. The radioimmunoassy was performed using a commercially avail- able kit from Amersham International plc.
Statistical analysis was performed using the Student t-test and the Fischer Exact test. Significance was set at P < 0.05.
RESULTS The indications for induction were: postterm pregnancy
(N = l l ) , pregnancy-induced hypertension (N = 4), and others (N = 2). Of the total mothers, 65% were black and the remainder white. Table 1 summarizes the age, weight, and relative Bishop scores of the mothers. Each patient was noted to have at least some uterine activity by external tocodynamometry during the ripening period. The Bishop score at 12 hours was noted to have changed significantly from the initial value at 0 hours. The mean increase in Bishop score and its standard deviation was 3.5 t 1.4 with a range from 2 to 7. In addition, at 12 hours, 71% had a Bishop score of 2 6 , a score considered clinically ripe for induction of labor.
Table 2 summarizes the proportion of patients receiving 2 points for each component score of the serial biophysical profiles. Highly significant reductions in the presence of fetal breathing movements and fetal body movements are observed at 6 hours and 12 hours. The presence of fetal tone, amniotic fluid volume, and reactive nonstress tests were unchanged during the 12-hour interval.
The mean serial plasma levels of PGEM and standard deviation values measured in pg/ml at 0, 6, and 12 hours were 210 Ifr 71, 450 ? 147, and 446 t 262, respectively. The 6- and 12-hour values were significantly higher than the baseline value using the paired t-test (P < 0.005).
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

10 AMON ET AL.
TABLE 2. Biophysical Profile Characteristics (N = 17)”
Breathing Body Amniotic movements movements Tone fluid volume NST
Ohr 59%* loo%* 100% 88% 100% 6 hr 6% 65% 88% 88% 100%
12hr 0%* 24%* 88% 88% 94% ”Percentage of fetuses showing the “presence” of Biophysical Profile components. NST = nonstress test. *P < 0.0005 bv Fisher Exact Test.
The incidence of cesarean section was 29%. The mean birthweight was 3,391 2 440 g (range, 2,5804,360 8). Two infants had Apgar scores at 5 minutes <7. There were no neonatal deaths. One infant had transient tachypnea of the newborn.
In a nonconcurrent, poststudy analysis of a small group of eight women undergoing oxytocin induction of labor at term, we could not find any decrease in fetal biophysical activities during the latent phase.
DISCUSSION This study correlates the use of exogenous PGEZ for
cervical ripening and serial biophysical profile parameters over 12 hours in the human. The hydrogel intravaginal pessary we used has a relatively constant and sustained in vivo release rate for PGE2, 0.34 mg/hr over 12 hours (Amon et al. unpub. data), which allows for a greater degree of prolonged uniformity in exogenous PGEZ exposure to this group of study patients.
Using the PGEZ controlled release pessary, we found an increase in the Bishop score from the baseline to the 12-hour value that was both statistically and clinically significant. Furthermore, the mean PGEM plasma concen- trations were significantly increased at 6 hours and 12 hours from the baseline value. Since no placebo pessaries were tested along with the active pessaries, it is uncertain to what extent the measured concentrations of PGEM represent over basal levels that might be measured in control patients. However, it should be noted that none of our study women were considered to be in active labor.
Fetal breathing movements during the 6- and 12-hour observation periods were almost completely absent. In addition, fetal body movements were significantly dimin- ished at 12 hours. Although we had no concurrent placebo- controlled group, these effects are clearly associated with the PGEZ pessary. Our study design excluded patients with many confounding clinical factors that affect fetal breathing movements and body movements [9,10]. Furthermore, serial evaluations of the same fetus by the same examiner strength- ens our evaluation. Moreover, in a limited set of observa- tions, eight women undergoing the first day of induction of labor with oxytocin alone had no significant decrease in
fetal breathing movements or body movements. Although inconclusive, these added observations suggest a separate effect due to the exogenous PGE2. Unfortunately, other serial changes as in PGE2 plasma concentrations were not assessed. This would have significantly strengthened our study.
Other clinical investigators studied patients in a more advanced phase of labor, after amniotomy, and after epidural placement. Boylan and Lewis [lo] found a significant decrease in the time incidence of fetal breathing move- ments from 36% antenatally to 0.3% during labor. However, in contrast to our work, the mean cervical dilation in labor during the observation period was 4 cm (range 2-9cm). Although 11 of these labors were induced by PGEZ vaginal pessaries, no further analysis of this subgroup was performed. They found no significant decrease in the time incidence of fetal body movements. Richardson and colleagues (1 I] serially studied the time incidence of fetal breathing and body movements during labor in 20 women who underwent induction. In contrast to our study, 15 of these women had labor induced by amniotomy and 17 received epidural anesthesia, indicating an active phase of labor. The mean percent time spent breathing during the observation periods decreased significantly from 25.6% at baseline to 8.3% during latent phase labor and 0.8% during active labor. Sasoon and coworkers [4] studied serial changes in the biophysical profile during labor. In all patients, measure- ments were taken initially during labor, followed at 30 minutes postepidural, indicating active labor, and 30 min- utes postmembrane rupture, whichever came first. They noted a steady decline in both fetal breathing movements and body movements during the intrapartum period.
Animal studies strongly suggest a very tight link between fetal breathing movements and PGE2. In the sheep, the species best studied, there is an inverse relationship between prostaglandin, especially PGE2, and fetal breathing move- ments. A marked increase in the incidence, amplitude, and regularity of fetal breathing movements occurs during infusions into fetal sheep of prostaglandin synthetase (cy- clooxygenase) inhibitors (PGSI), meclofenamate, Indo- methacin, and acetylsalicylic acid [7]. Conversely, PG infusions diminish fetal breathing movements 11 21. Fetal breathing movements were markedly reduced or completely absent during fetal infusions of PGE2. Although there were statistical decreases in fetal breathing movements due to infusions of PGF2 alpha, there were not as marked as in the case of PGEZ [12]. The inverse relationship holds not only with the infused doses of PGE2, but also with fetal plasma levels of PGEZ [7]. It appears that the site of action of PGE2 and PGSI on fetal breathing movements in sheep is in the lower pons or medulla [13]. Furthermore, the link between labor and fetal breathing movements may well be PGE2. During parturition, the fetal plasma concentration of PGEZ increases in the sheep [14]. In the human during parturition,
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

BIOPHYSICAL PROFILE AND PGE2 1 1
there are increases in the concentrations of PGEZ and the F2 alpha in the amniotic fluid and their metabolites in maternal plasma and urine [l]. At birth there is a sudden and dramatic onset of continuous breathing by the new- born. Clearly, there are other factors that are related to the onset of breathing at birth, but it is noted that concentra- tions of PGEZ decrease rapidly to very low levels after continuous ventilation is established [ 151.
Despite differences in study designs, our findings are consistent with published work of both clinical and animal investigators. Our study was substantially different from others in that all observations occurred only during the ripening phase or latent phase of labor. All of our study women ultimately required oxytocin and or amniotomy, after removal of the intravaginal PGE2 pessary, and only after the 12-hour observation period.
In conclusion, in term patients, during exogenous admin- istration of a PGEZ controlled-release vaginal pessary for the purpose of cervical ripening, the unfavorable or low Bishop score is significantly improved over 12 hours, the maternal plasma levels of PGEM are significantly increased at 6 hours and 12 hours, and changes in fetal breathing movements and fetal body movements are inversely related to changes in PGE2 concentrations and changes in the Bishop score.
Since pharmaceutical preparations of PGE2 are now in clinical use, we caution the clinician during his or her interpretation of a diminished biophysical profile score during the process of cervical ripening with PGE2. This is especially of concern during prolonged inductions. There- fore, in the setting of the unfavorable cervix, we urge the clinician primarily to rely on the nonstress test and uterine activity-induced changes in the fetal heart rate monitor as a predictor of fetal well-being.
ACKNOWLEDGMENTS We acknowledge Harrison M. Langrall, M.D., of Con-
trolled Therapeutics Corporation for making this study
possible. We also acknowledge Joan Bristol and John Knowles for measuring the plasma concentration of PGEM. This work was supported in part by Controlled Therapeutics Corporation, Malvern, PA.
1
2
3
4
5
6.
7.
8.
9.
10. 11.
12.
13.
14.
15.
REFERENCES Casey ML, MacDonald PC. The initiation of labor in women: regulation of phospholipid and arachidonic acid metabolism and or prostaglandin production. Semin Perinatol 1986; 10:27@-275. Jacobs MM. Clinical obstetric use of arachidonic acid metabolism and potential adverse effects. Semin Perinatol 1986;10:299-315. Manning FA, Morrison I, Lange IR, Harmon CR, Chamberlain PF. Fetal assessment based on biophysical profile scoring: experience in 12,620 referred high risk pregnancies. I. Perinatal mortality by fre- quency and etiology. Am J Obstet Gynecol 1985;151:343-350, Sassoon DA, Castro LC, Davis JL, Bear M, Hobel CJ. The biophysical profile in labor. Obstet Gynecol 199@;76:36@-365. Patrick J , Challis JRG, Cross J, et al. The relationship between fetal breathing movements and prostaglandin E2 during ACTH-induced labour in sheep. J Dev Physiol 1987;9:287-295. Castle BM, Turnbull AC. The presence or absence of fetal breathing movements predicts the outcome of preterm labour. Lancet 1983;8348: 471-473. Kitterman JA. Arachidonic acid metabolites and control of breathing in the fetus and newborn. Semin Perinatol 1987;11:43-52. Bishop EM. Pelvic scoring for elective inductions. Obstet Gynecol 1964;24:266-268. Boylan P, Lewis PJ. Fetal breathing in labor. Obstet Gynecol 1980;56: 35-38. Boddy K, DawesGS. Fetal breathing. Br Med Bull 1975;31:3-7. Richardson B, Natale R, Patrick J. Human fetal breathing activity during electively induced labor at term. Am J Obstet Gynecol 1979;133:247-255. Kitterman JA, Liggins GC, Fewell JE, Tooley WH. Inhibition of breaching movements in fetal sheep by prostaglandins. J Appl Physiol 1983;54:687-692. Koos BJ. Central stimulation of breathing movements in fetal lambs by prostaglandin synthetase inhibitors. J Physiol 1985;362:455466. Challis JRG, Dilley SR, Robinson JS, et al. Prostaglandins in the circulation of the fetal lamb. Prostaglandins 1976;11:1@41-1049. Clyman RI, Mauray F, Roman C, Rudolph AM, Heymann MA. Circulating prostaglandin E2 concentrations and patent ductus arterio- sus in fetal and neonatal lambs. J Pediat 198@;97:455461.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.