selective renal angiography in wegener's
TRANSCRIPT

Annals ofthe Rheumatic Diseases, 1983, 42, 192-195
Selective renal angiography in Wegener'sgranulomatosisH. M. MOUTSOPOULOS, P. C. AVGERINOS, C. G. TSAMPOULAS, ANDP. A. KATSIOTIS
From the Departments ofMedicine and Radiology, School ofMedicine, University ofloannina, loannina,Greece
SUMMARY Two patients whose illnesses meet the criteria of Wegener's granulomatosis arepresented. Selective renal angiography performed in both revealed multiple arterial aneurysmssimilar to those classically found in polyarteritis nodosa.
In the last 15 years selective angiography, particu-larly of the kidney, has been proposed as a valuablediagnostic and follow-up procedure in polyarteritisno,dosa.'2 The characteristic angiographic appear-ance in polyarteritis nodosa consists of multiple smallaneurysms that are uniform in size, 1 to 5 mm, andassociated with medium and small arteriesexclusively. 1-3
Selective renal angiography has not been usedextensively in Wegener's granulomatosis, andsporadic reports have been negative4 5 with theexception of a single case whose angiographicchanges were similar to those of polyarteritisnodosa.6We present 2 patients with Wegener's
granulomatosis. Selective renal angiography in bothrevealed multiple arterial aneurysms similar to thoseobserved in polyarteritis nodosa.
Case reports
CASE 1A 30-year-old machinist was admitted to our unitwith a month's history of fever, frontal headache,cough, and nasal discharge. On examination he wasfebrile (temperature 39 3°C) and normotensive.Tenderness over frontal and maxillary sinuses wasnoted. Rales were heard on auscultation of his rightlung base. Laboratory investigation showed the fol-lowing abnormal results: haematocrit 38%, totalwhite blood count 9-8 x 109/l (polymorphonuclearcells 72%, lymphocytes 26%, monocytes 2%),erythrocyte sedimentation rate was 1 16 mm/h. UrineAccepted for publication 16 March 1982.Correspondence to Dr H. M. Moutsopoulos, Department ofMedicine, School of Medicine, Ioannina, Greece.
microscopy showed 10 red blood cells per high-power optic field. Sinus x-rays showed diffuseopacification of maxillary and left frontal sinuses. Achest x-ray revealed multiple, well-demarcated,nodular, cavitating lesions in both lung fields (Fig. 1).Biopsy of the nasal mucosa and the right maxillarysinus showed granulomatous necrotising vasculitis,consistent with Wegener's granulomatosis. Thepatient was started on a regimen of prednisone 1mg/kg/day and cyclophosphamide 2 mg/kg/day.
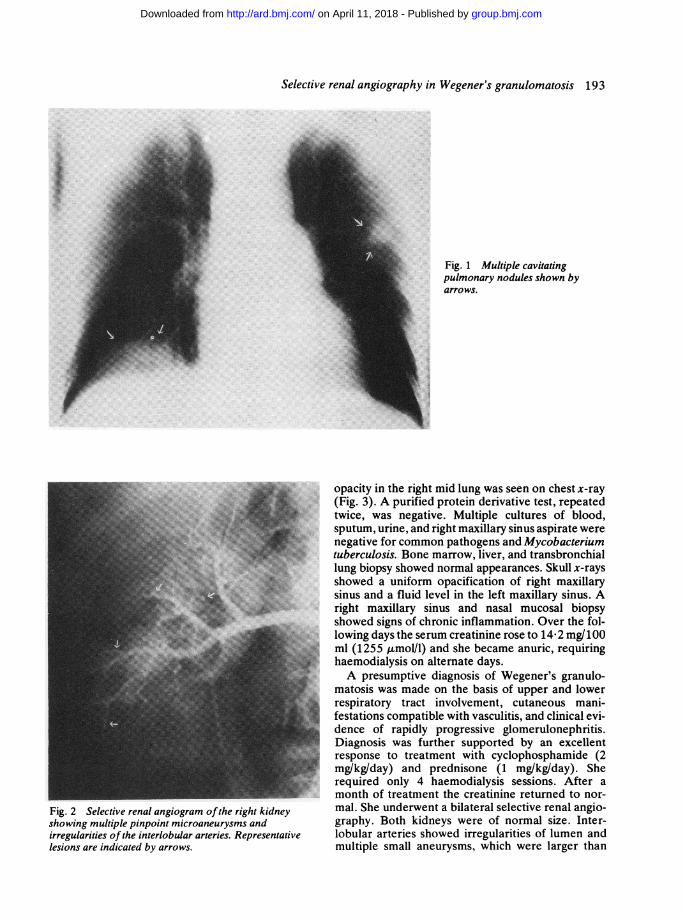
Bilateral selective renal angiography wasperformed 4 months after initiation of treatment.Kidneys were of normal size and shape. Multiplepinpoint microaneurysms and irregularities of theinterlobular arteries were observed in bothkidneys (Fig. 2).CASE 2A 53-year-old housewife was admitted with 20 days'history of fever, arthritis of the right wrist, arthralgiaof both knees, and productive cough with bloodstained sputum. On admission her temperature was38- 8°C, blood pressure 120/80 mmHg, and pulse rate1 20/min. Mucosal ulcerations were noted on the hardpalate, and rales were heard over the right lung base.Numerous ecchymoses and petechiae were observed,mainly over the lower limbs. Laboratory investiga-tions gave the following abnormal results: haematoc-rit 30%, total white blood cell count 14 x 109/l(polymorphonuclear cells 90%, lymphocytes 8%,monocytes 2%). The erythrocyte sedimentation ratewas 140 mm/h. Serum creatinine was 5 6 mg/100 ml(495 ,moI/l). Urine analysis revealed proteinuria of1 . 1 g/l and specific gravity of 1008. Urine microscopyshowed numerous red and white blood cells and redblood cell casts. A large (5 x 3.5 cm) cavitating
192
group.bmj.com on April 11, 2018 - Published by http://ard.bmj.com/Downloaded from
Selective renal angiography in Wegener's granulomatosis 193
Fig. 2 Selective renal angiogram ofthe right kidneyshowing multiple pinpoint microaneurysms andirregularities of the interlobular arteries. Representativelesions are indicated by arrows.
Fig. 1 Multiple cavitatingpulmonary nodules shown byarrows.
opacity in the right mid lung was seen on chest x-ray(Fig. 3). A purified protein derivative test, repeatedtwice, was negative. Multiple cultures of blood,sputum, urine, and right maxillary sinus aspirate werenegative for common pathogens and Mycobacteriumtuberculosis. Bone marrow, liver, and transbronchiallung biopsy showed normal appearances. Skull x-raysshowed a uniform opacification of right maxillarysinus and a fluid level in the left maxillary sinus. Aright maxillary sinus and nasal mucosal biopsyshowed signs of chronic inflammation. Over the fol-lowing days the serum creatinine rose to 14-2 mg/100ml (1255 umolIl) and she became anuric, requiringhaemodialysis on alternate days.A presumptive diagnosis of Wegener's granulo-
matosis was made on the basis of upper and lowerrespiratory tract involvement, cutaneous mani-festations compatible with vasculitis, and clinical evi-dence of rapidly progressive glomerulonephritis.Diagnosis was further supported by an excellentresponse to treatment with cyclophosphamide (2mg/kg/day) and prednisone (1 mg/kg/day). Sherequired only 4 haemodialysis sessions. After amonth of treatment the creatinine returned to nor-mal. She underwent a bilateral selective renal angio-graphy. Both kidneys were of normal size. Inter-lobular arteries showed irregularities of lumen andmultiple small aneurysms, which were larger than
group.bmj.com on April 11, 2018 - Published by http://ard.bmj.com/Downloaded from

194 Moutsopoulos, Avgerinos, Tsampoulas, Katsiotis
Fig. 3 Chext x-ray showing a large (5 x3-5 cm) cavitatingnodule in right mid-lung.
those observed in the previous case. Scalloping of therenal outline due to peripheral wedge-shaped defectswere seen on the parenchymal phase compatible withsmall peripheral cortical infarcts (Fig. 4).
Discussion
The most interesting aspect of these 2 cases, whichmeet the criteria of Wegener's granulomatosis, is thepresence of multiple microaneurysms on selectiverenal angiography. Multiple aneurysms of the smalland medium sized renal arteries demonstrated ante-mortem by angiography was first described inpolyarteritis nodosa in 1965.17 This finding wasconsidered to be pathognomonic of the disease.8Recently it has been shown that similar angiographicfindings occur in other systemic necrotising vas-culitides, such as allergic granulomatosis and overlapsyndromes.9 10 To our knowledge only one case withmultiple bilateral renal aneurysms occurring inassociation with Wegener's granulomatosis has beenreported.6 Other nonvasculitic conditions likemycotic aneurysms, trauma, and tumour invasion'can give a similar angiographic appearance. Theseconditions, however, should seldom be difficult todifferentiate clinically from a necrotising vasculitis.
It is of interest that the angiographic findingsappeared to parallel the severity of glomerularinvolvement. In the first case, in which microscopichaematuria was the only evidence of glomerularinvolvement, angiography showed relatively few pin-point aneurysms. In the second case, however, wherestrong evidence of extensive glomerular damageexisted, the aneurysms were larger, more numerous,and associated with wedge-shaped peripheralinfarcts.The 2 cases suggest that arterial aneurysms may be
a more frequent finding in Wegener's granulomatosisthan previously thought.6 It is also possible, if oneconsiders the presence of arterial aneurysms asenough evidence for the diagnosis of an overlapsyndrome, that these 2 cases represent an overlapsyndrome between Wegener's granulomatosis andpolyarteritis nodosa. Finally, one is faced with thequestion of whether these 2 entities may representdifferent expressions of the same vasculitic processthat leads to multiple aneurysm formation. Systema-tic study by selective renal angiography of such casesmay solve this question.
We thank Dr D. Emmanuel for his suggestions and comments andMs E. Papanikolaou for excellent secretarial assistance.
References
Fig. 4 Selective renal angiogram ofleft kidney showingmultiple microaneurysms and scalloping ofthe renal outline.
1 Fleming R J, Stem L Z. Multiple intraparenchymal renalaneurysms in polyarteritis nodosa. Radiology 1965; 84: 100-3.
group.bmj.com on April 11, 2018 - Published by http://ard.bmj.com/Downloaded from

Selective renal angiography in Wegener's granulomatosis 195
2 Kohn B J, Stulberg H J. Angiographic diagnosis of polyarteritisnodosa. West J Med 1971; 114: 40-2.
3 Evens R G, Dorby C A, Eckert J F. An exercise in radiologic-pathologic correlation. Radiology 1968; 91: 1028-32.
4 Ekelund L. Lindholm T. Angiography in coliagenous disease ofthe kidney. Acta Radiol (Diagn) (Stockh) 1974; 15: 413-22.
5 Lundstrom B, Lindqvist B, Solerbergh H, et al. Nephroangio-graphy in Wegener's granulomatosis. A comparison with panar-teritis nodosa.Acta Radiol (Diagn) (Stockh) 1975; 16: 641-53.
6 Baker S B, Robinson D R. Unusual renal manifestations ofWegener's granulomatosis. Am J Med 1978; 64: 883-9.
7 Bron K M, Strott C A, Shapiro A P. The diagnostic value ofangiographic observations in polyarteritis nodosa. Arch InternMed 1965; 116: 450-3.
8 Essigner A, Bonard M. Panarteritis nodosa, an angiographicentity presentation of two cases. Br J Radiol 1971; 44: 184-7.
9 Fauci A S, Haynes B F, Katz P. The spectrum of vasculitis.Clinical, pathologic, immunologic and therapeutic con-siderations. Ann Intern Med 1978; 89: 660-76.
10 Kohler P F, Claman H N. Systemic vasculitis. In: Franklin E C,ed. Clinical Immunology Update. New York: Churchill-Livingstone, 1981: 293-319.
group.bmj.com on April 11, 2018 - Published by http://ard.bmj.com/Downloaded from

Wegener's granulomatosisSelective renal angiography in
Tsampoulas and P. A. KatsiotisH. M. Moutsopoulos, P. C. Avgerinos, C. G.
doi: 10.1136/ard.42.2.1921983 42: 192-195 Ann Rheum Dis
http://ard.bmj.com/content/42/2/192Updated information and services can be found at:
These include:
serviceEmail alerting
online article. article. Sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 11, 2018 - Published by http://ard.bmj.com/Downloaded from