see psoriasis: look deeper report
DESCRIPTION
ÂTRANSCRIPT
see psoriasis:look deeperRecognising the life impact of psoriasis
2
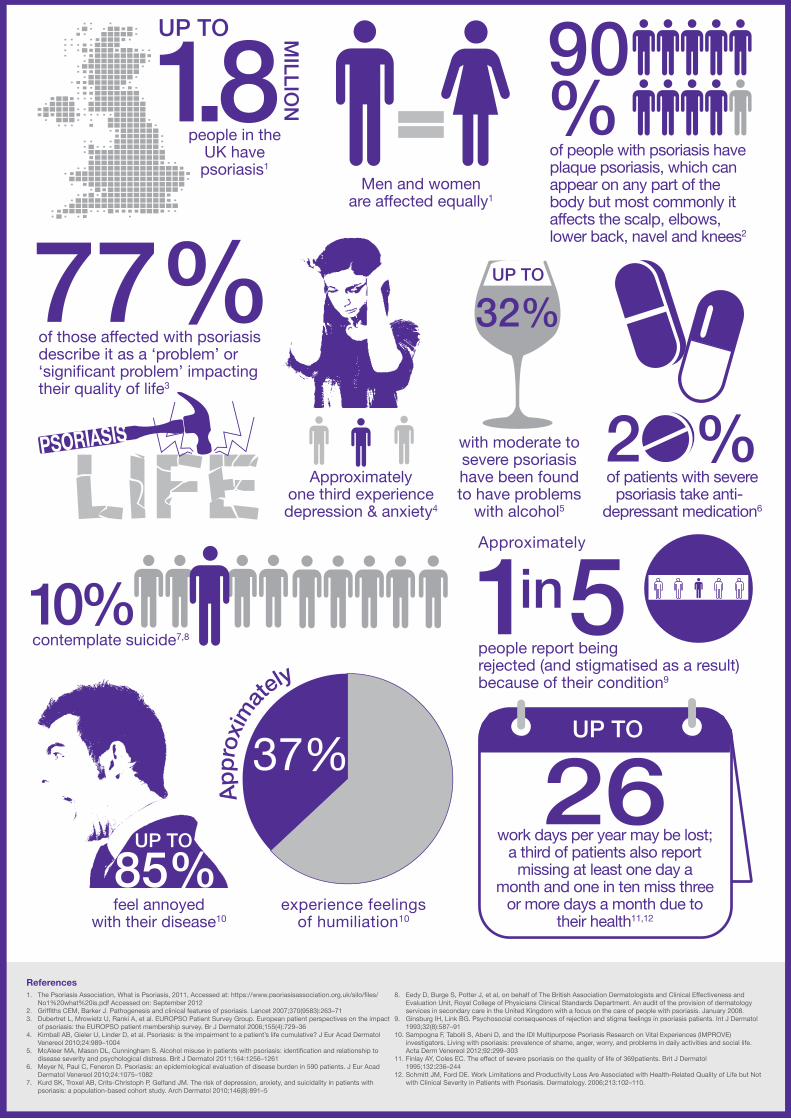
people in theUK havepsoriasis1
Men and womenare affected equally1
of people with psoriasis have plaque psoriasis, which can appear on any part of the body but most commonly it affects the scalp, elbows, lower back, navel and knees2
of those affected with psoriasis describe it as a ‘problem’ or ‘significant problem’ impacting their quality of life3
Approximatelyone third experience depression & anxiety4
with moderate to severe psoriasis have been found to have problems
with alcohol5
contemplate suicide7,8
Approximately
people report beingrejected (and stigmatised as a result) because of their condition9
experience feelingsof humiliation10
App
roxi
mat
ely
work days per year may be lost;a third of patients also report
missing at least one day a month and one in ten miss three
or more days a month due totheir health11,12
feel annoyedwith their disease10
of patients with severe psoriasis take anti-
depressant medication6
1. The Psoriasis Association, What is Psoriasis, 2011, Accessed at: https://www.psoriasisassociation.org.uk/silo/files/No1%20what%20is.pdf Accessed on: September 2012
2. Griffiths CEM, Barker J. Pathogenesis and clinical features of psoriasis. Lancet 2007;370(9583):263–713. Dubertret L, Mrowietz U, Ranki A, et al. EUROPSO Patient Survey Group. European patient perspectives on the impact
of psoriasis: the EUROPSO patient membership survey. Br J Dermatol 2006;155(4):729–364. Kimball AB, Gieler U, Linder D, et al. Psoriasis: is the impairment to a patient’s life cumulative? J Eur Acad Dermatol
Venereol 2010;24:989–10045. McAleer MA, Mason DL, Cunningham S. Alcohol misuse in patients with psoriasis: identification and relationship to
disease severity and psychological distress. Brit J Dermatol 2011;164:1256–12616. Meyer N, Paul C, Feneron D. Psoriasis: an epidemiological evaluation of disease burden in 590 patients. J Eur Acad
Dermatol Venereol 2010;24:1075–10827. Kurd SK, Troxel AB, Crits-Christoph P, Gelfand JM. The risk of depression, anxiety, and suicidality in patients with
psoriasis: a population-based cohort study. Arch Dermatol 2010;146(8):891–5
8. Eedy D, Burge S, Potter J, et al, on behalf of The British Association Dermatologists and Clinical Effectiveness and Evaluation Unit, Royal College of Physicians Clinical Standards Department. An audit of the provision of dermatology services in secondary care in the United Kingdom with a focus on the care of people with psoriasis. January 2008.
9. Ginsburg IH, Link BG. Psychosocial consequences of rejection and stigma feelings in psoriasis patients. Int J Dermatol 1993;32(8):587–91
10. Sampogna F, Tabolli S, Abeni D, and the IDI Multipurpose Psoriasis Research on Vital Experiences (IMPROVE) investigators. Living with psoriasis: prevalence of shame, anger, worry, and problems in daily activities and social life. Acta Derm Venereol 2012;92:299–303
11. Finlay AY, Coles EC. The effect of severe psoriasis on the quality of life of 369patients. Brit J Dermatol 1995;132:236–244
12. Schmitt JM, Ford DE. Work Limitations and Productivity Loss Are Associated with Health-Related Quality of Life but Not with Clinical Severity in Patients with Psoriasis. Dermatology. 2006;213:102–110.
References

3
Anyone living with psoriasis will agree that it is life-changing.
For up to approximately 1.8 million people in the UK who are affected by psoriasis, it is more than just a skin condition.1,2 The multi-faceted nature of psoriasis means the effects go beyond visual signs and symptoms.2 It can impact on emotional and physical wellbeing and in some people it is associated with depression, anxiety and suicidal thoughts, particularly in those affected with more severe psoriasis.3-6
Yet, despite the documented impact on emotional wellbeing, these wider effects often go unrecognised and untreated.5,7
We, the Psoriasis Association and the Mental Health Foundation, have come together to raise awareness of the need for healthcare professionals to look at psoriasis holistically, to consider both the physical symptoms and psychological wellbeing, and ensure people with psoriasis receive the care and support they need. Some people with psoriasis often feel that their GP regards psoriasis as a minor skin complaint and are dismissive of the emotional aspects leaving many to continue unaided on the isolating and emotional journey associated with psoriasis.5,7
This report is part of the See Psoriasis: Look Deeper campaign exploring psoriasis as a complex, progressive condition which has numerous consequences for the individual, their family, and society as a whole.2,3,4,8,9
We call for…
− The full impact of psoriasis to be recognised and treated by multi-disciplinary teams who will look deeper, both literally and metaphorically, to ensure that the treatment people receive addresses all their health needs.
To create change, we need to…
− Prioritise political efforts to ensure that the financial levers and incentives for commissioners are aligned to multi-disciplinary working. Beginning with the National Institute for Health and Clinical Excellence (NICE) guidance on the management of psoriasis, and following through to the guidance issued by the NHS Commissioning Board to the new Clinical Commissioning Groups (CCGs), the NHS must support collaborative working that can respond appropriately to both the physical and psychological needs of people with psoriasis.
At the same time, we are calling on people with psoriasis, and their families and friends, to consider the broader impacts of the condition and be aware of the potential impact on psychological wellbeing and quality of life. We ask them to not suffer in silence, but to ask for help to ensure that they receive appropriate referrals and treatment when they need it most.
Helen McAteer, Chief Executive, Psoriasis Association
Andrew McCulloch, Chief Executive, Mental Health Foundation
Foreword
see psoriasis:look deeper
Together we can work towards improved holistic care for people with psoriasis. We just need to see beyond the skin and look deeper into their needs.
4
Looking beyond the skin
*People with psoriasis submitted postcards for inclusion within the See Psoriasis: Look Deeper campaign describing how their psoriasis makes them feel and express the impact that the condition has on their life. People could choose to stay anonymous if they preferred.
Many people see psoriasis as a condition that only affects the skin and impacts on appearance; they do not realise that the effects can go much deeper and can have a lasting effect for those living with the condition day-to-day.7 As a long-term condition affecting many patients for most of their adult life, its unpredictable nature means its impact varies, so while some people manage for years without a psoriasis flare, others are affected regularly.10
Similarly, the severity of psoriasis can vary enormously; some people have a single, isolated plaque that is barely noticeable, yet others can be affected in many different areas of the body.10 Psoriasis plaques can be itchy or sore, and may cause the skin to crack and bleed.11
Psoriasis is strongly associated with the risk of other health issues, further adding to the difficulty that many patients face. Between 6% and 40% develop psoriatic arthritis – stiffness, pain and swelling of the joints, which may lead to deformity;12-15 whilst the risk of developing conditions such as cardiovascular disease, type 2 diabetes, depression and Crohn’s disease is also increased.2,14,15,16
Psoriasis – The FacTs
>
>
>
It is a chronic inflammatory disease estimated to affect between 1.5% and 3%
of the UK population, which means that up to
1.8 million people are affected1,2,4,13,17
90% of people with psoriasis have plaque
psoriasis which can appear on any part of
the body but most commonly it affects the
scalp, elbows, lower back, navel and knees17
Most people are managed in Primary Care
with topical treatments; however, if these
treatments are not successful, people with
psoriasis may be referred to specialist
dermatology services for UV light therapy,
systemic treatments or biologics10
WHY DID YOU IMPACT INTO MY LIFE? WHERE DO
YOU COME FROM? WHEN I WAS A CHILD WHY DID
PEOPLE THINK I HAD FLEAS? WHY WHEN I COMBED
MY HAIR DI D IT LOOK LIKE A SNOWSTORM? WHY
DID GIRLS SHUN ME LIKE I HAD THE PLAGUE?
WHY WAS I BORN, JUST TO HAVE SUCH A LONELY
EXISTENCE? WHY? WHY? WHY?

5*People with psoriasis submitted postcards for inclusion within the See Psoriasis: Look Deeper campaign describing how their psoriasis makes them feel and express the impact that the condition has on their life. People could choose to stay anonymous if they choose.
Like it or not, we live in a society where appearance matters, so it should come as no surprise that psoriasis impacts on the psychological wellbeing as well as quality of life for those who have to endure it.2,4
Contrary to popular belief, these effects are not always related to or based on how severe the condition may be. For example, someone with physically mild symptoms may have more difficulty coping than others with more severe or extensive symptoms.18 It essentially boils down to how each individual feels they can cope and the support they have to do so.
The relationship between physical health and emotional wellbeing is complex. Those with psoriasis can have low esteem or suffer from depression and anxiety, and if unrecognised, these health issues can prevent people from effectively managing their psoriasis.19 Instead they may develop unhelpful ways of coping such as avoiding being in public, excessively using alcohol and overeating.19 These ways of coping can negatively affect other health conditions associated with psoriasis, such as heart disease or diabetes.19 It is this pain and discomfort of psoriasis along with its emotional impact, which can lead people with psoriasis into a cycle of despair.19
‘I don’t want to be rejected’Because of the obvious visibility of psoriasis, many people experience rejection and stigmatisation,2 which can have a detrimental effect on their self-esteem. Approximately one in five people report being rejected (and stigmatised as a result of their condition).20 This happens most often in public and in communal places such as the gym, swimming pool, at the hairdressers or at work.20
‘Sometimes I don’t want to be around anymore’Worryingly, approximately one third of people living with psoriasis also experience depression and anxiety.2 What is more shocking, however, is that psoriasis is associated with an increased risk of suicidality.3 Up to 1 in 10 people contemplate suicide, highlighting the devastating effects of the disease.2,5,6,19
‘My everyday life and family are affected’A European-wide patient survey found that 77% of those affected with psoriasis describe it as a ‘problem’ or ‘significant problem’ in terms of impacting their quality of life.12 Simple activities such as cleaning the house or doing the laundry, which are taken for granted by many, need to be done more frequently.9 Social lives and relationships can also be restricted, further adding to the psychological pressure.2, 21
It is not just the impact psoriasis has on the individual that needs consideration. Psoriasis also significantly affects family and friends.8,22,23 Around 90% of people with a family member or relative with psoriasis report that their life is adversely impacted – affecting social lives, holiday plans and time with other family members.8,23
Relationships, including sexual relationships, can also be affected, even after symptoms have improved.21
‘Drinking helps to numb the pain’This impact on everyday life and relationships can have serious consequences and lead to excess alcohol use. Up to one third of patients with moderate to severe psoriasis have been found to have problems with alcohol,24 which can be extremely damaging as excess alcohol intake can increase the risk of other associated conditions and lead to excessive mortality from alcohol-related causes in people with psoriasis.24,25
My Psoriasis, My Pain
*People with psoriasis submitted postcards for inclusion within the See Psoriasis: Look Deeper campaign describing how their psoriasis makes them feel and express the impact that the condition has on their life. People could choose to stay anonymous if they preferred.
I’m obese and prefer to stay that way so people see the fat rather than the psoriasis. Lack of interest and care from my GP adds to my low self-esteem. After horrible comments in the swimming pool, I don’t like to swim and with psoriatic and osteoarthritis setting in, lack of exercise adds to the obesity. Externally I smile and try to be jolly; internally I loathe myself and will be glad when life’s over.Anonymous*
I have known you now for over 40 years and
you never fail to surprise me. When you are
good I feel on top of the world and confident,
but when you are bad my confidence plummets
and I find myself in a very dark place feeling
life is not worth living. Lesley*
6 *People with psoriasis submitted postcards for inclusion within the See Psoriasis: Look Deeper campaign describing how their psoriasis makes them feel and express the impact that the condition has on their life. People could choose to stay anonymous if they preferred.
Psoriasis - An emotional battle2,5,6,19,20,21
� Approximately one third experience depression and anxiety2
� Up to 85% of people feel annoyance with their psoriasis21
� 1 in 3 experience feelings of humiliation about their condition21
� 1 in 5 people report being rejected (and stigmatised) as a result of their condition20
� 1 in 10 contemplate suicide2,5,6,19
� A third experience problems with loved ones21
Psoriasis can affect the gaining and retaining of paid work and life-time earning potential2
About one third of patients, who are not working, describe being unable to work due to their psoriasis27
Unemployment is three times more likely for people affected with psoriasis than for those unaffected28
Up to 26 work days per year may be lost;27 a third of patients also report missing at least one day a month and one in ten miss three or more days a month due to their health28
DID yoU KnoW..?
>
>
>
>
Work and economic woesWhen the full implications of psoriasis are considered in terms of economic impact, the figures are shocking. One in five people with psoriasis experience discrimination at work and one in four believes that psoriasis has affected their career choice.9
Severe psoriasis requires people with psoriasis to regularly attend specialist clinics as well as phototherapy sessions, which can take one to two hours each time,9 or in some cases, stay in hospital for an average of 14 days.5 This can lead to difficulties for those in demanding careers which require long hours and close attention. As a result, psoriasis is also associated with lower productivity and reduced income.9 For many, the inability to enjoy a fulfilling career or employment and financial stability can further impact their psychological wellbeing.
There is also the overall impact and economic burden to society, which needs to be considered. The cost of adult mental health services in England is currently around £6.6 billion.26 There is now, more than ever, a need to provide appropriate and effective psychological support to ensure the risk of long-term mental health problems for patients with psoriasis is reduced and further burden on already stretched services is avoided.
You are with me day and night, 24 hours.
Everything I do is affected by you. You make
me feel uncomfortable, untidy and sometimes even
ashamed. You never let me be free of your soreness,
unsightliness, your pain and unpleasantness.Richard*
I lost 2 jobs due to my skin condition, during those years I was only working for about 9 months per year due to inpatient/outpatient treatments for my ‘chronic’ psoriasis. Hospital inpatient could be anything up to 7 weeks at any one time in those days. Time off work became a great burden (financially) on my young wife and young children.
Richard*
7
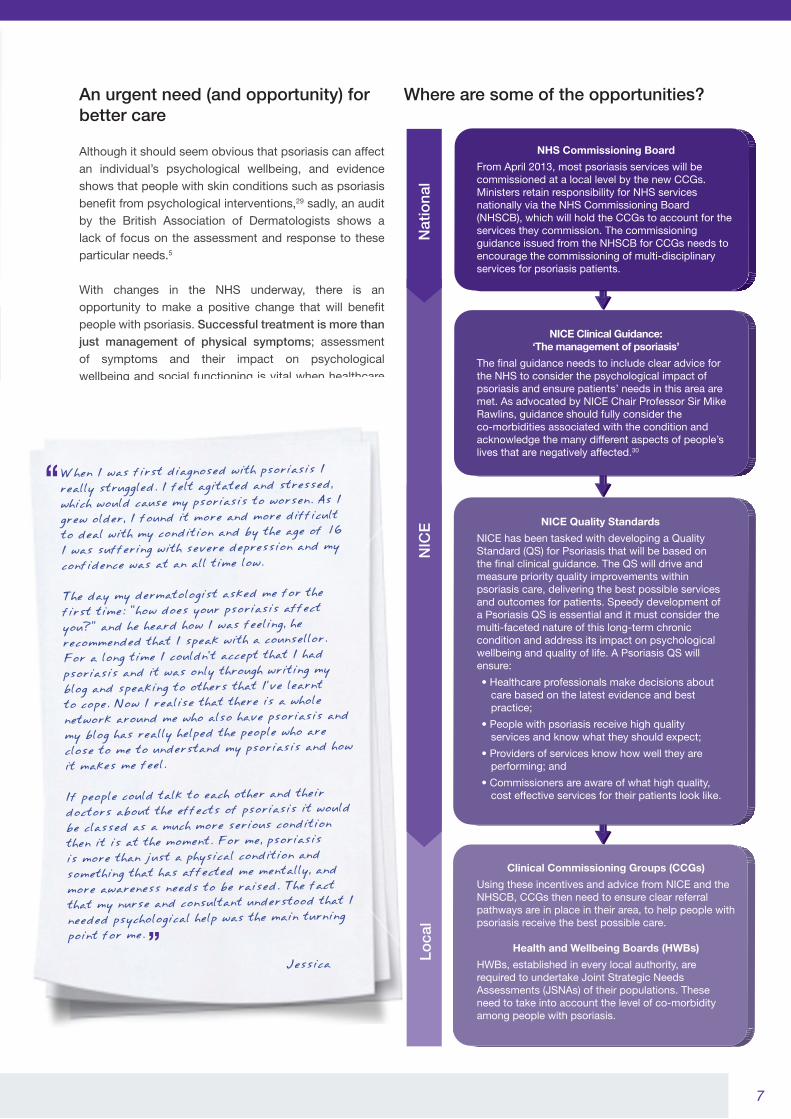
Where are some of the opportunities? An urgent need (and opportunity) for better care
Although it should seem obvious that psoriasis can affect an individual’s psychological wellbeing, and evidence shows that people with skin conditions such as psoriasis benefit from psychological interventions,29 sadly, an audit by the British Association of Dermatologists shows a lack of focus on the assessment and response to these particular needs.5
With changes in the NHS underway, there is an opportunity to make a positive change that will benefit people with psoriasis. Successful treatment is more than just management of physical symptoms; assessment of symptoms and their impact on psychological wellbeing and social functioning is vital when healthcare professionals are considering the range of treatments and options.
When I was first diagnosed with psoriasis I really struggled. I felt agitated and stressed, which would cause my psoriasis to worsen. As I grew older, I found it more and more difficult to deal with my condition and by the age of 16 I was suffering with severe depression and my confidence was at an all time low.
The day my dermatologist asked me for the first time: “how does your psoriasis affect you?” and he heard how I was feeling, he recommended that I speak with a counsellor. For a long time I couldn’t accept that I had psoriasis and it was only through writing my blog and speaking to others that I’ve learnt to cope. Now I realise that there is a whole network around me who also have psoriasis and my blog has really helped the people who are close to me to understand my psoriasis and how it makes me feel.
If people could talk to each other and their doctors about the effects of psoriasis it would be classed as a much more serious condition then it is at the moment. For me, psoriasis is more than just a physical condition and something that has affected me mentally, and more awareness needs to be raised. The fact that my nurse and consultant understood that I needed psychological help was the main turning point for me.
Jessica
Clinical Commissioning Groups (CCGs)
Using these incentives and advice from NICE and the NHSCB, CCGs then need to ensure clear referral pathways are in place in their area, to help people with psoriasis receive the best possible care.
Health and Wellbeing Boards (HWBs)
HWBs, established in every local authority, are required to undertake Joint Strategic Needs Assessments (JSNAs) of their populations. These need to take into account the level of co-morbidity among people with psoriasis.
NICE Quality Standards
NICE has been tasked with developing a Quality Standard (QS) for Psoriasis that will be based on the �nal clinical guidance. The QS will drive and measure priority quality improvements within psoriasis care, delivering the best possible services and outcomes for patients. Speedy development of a Psoriasis QS is essential and it must consider the multi-faceted nature of this long-term chronic condition and address its impact on psychological wellbeing and quality of life. A Psoriasis QS will ensure:
• Healthcare professionals make decisions about care based on the latest evidence and best practice;
• People with psoriasis receive high quality services and know what they should expect;
• Providers of services know how well they are performing; and
• Commissioners are aware of what high quality, cost effective services for their patients look like.
NICE Clinical Guidance: ‘The management of psoriasis’
The �nal guidance needs to include clear advice for the NHS to consider the psychological impact of psoriasis and ensure patients’ needs in this area are met. As advocated by NICE Chair Professor Sir Mike Rawlins, guidance should fully consider the co-morbidities associated with the condition and acknowledge the many different aspects of people’s lives that are negatively affected.30
NHS Commissioning Board
From April 2013, most psoriasis services will be commissioned at a local level by the new CCGs. Ministers retain responsibility for NHS services nationally via the NHS Commissioning Board (NHSCB), which will hold the CCGs to account for the services they commission. The commissioning guidance issued from the NHSCB for CCGs needs to encourage the commissioning of multi-disciplinary services for psoriasis patients.

8
Action at a local level Gold Standard Psoriasis Care
The Royal Free Psoriasis and Psoriatic Arthritis Service based
at the Royal Free Hospital, London, is a patient centred service
comprising of a large multi-disciplinary team with dermatologists,
rheumatologist, biologics nurse, phototherapists, clinical nurse
specialist and psychologist.
It provides an unusually comprehensive approach to the
management of patients with psoriasis and psoriatic arthritis,
presently seeing approximately 80-100 patients a week. The aim
of the service is not only to manage patients medically, but to
address the considerable psychological distress and social impact
of the condition, and it is a gold standard of care for patients with
psoriasis and psoriatic arthritis.
A ‘psycho-dermatology’ service integrating a psychology service
within the established dermatology department at the Royal Free
Hospital provides psychological therapy for patients with skin
conditions. Developed by Consultant Dermatologist, Dr Sandy
McBride, Psychologists Dr Alexandra Mizara and Professor Alex
Clarke, with the help of Dermatrust and an NHS innovation award,
this service provides essential support and therapy for patients
with a wide range of skin conditions enabling them to live the lives
they wish and cope with the considerable impact of disfiguring skin
conditions.
With the new emphasis on devolved decision-making, some local areas are already innovating and providing multi-disciplinary services. MPs and other policy-makers with an interest in supporting this campaign are invited to make enquiries in their local area regarding the existence of a clear referral pathway and the availability of multi-disciplinary services for people with psoriasis.
As powers for the commissioning of services shift to a local level, CCGs have a responsibility to ensure that referral pathways account for the multi-disciplinary challenges presented to those with psoriasis. This can be more easily achieved by taking a holistic view of care and treatment options so that the impact of psoriasis on patients’ overall wellbeing is effectively managed
Sir Paul Beresford, MP, Chair of the All Parliamentary party group on Skin
The See Psoriasis: Look Deeper campaign provides an excellent opportunity to
drive a better understanding of psoriasis and the detrimental impact it can have to a person’s overall
quality of life. The campaign has given patients a voice and encouraged them to describe the impact
that psoriasis has not only to their skin, but their entire lives including their psychological wellbeing.
The evidence base for service provision in the UK is currently poor and there needs to be significant research investment
for us to understand not only the complexities of psoriasis management but the life impact of this chronic, long term
condition. Pioneering work in Manchester, as part of a National Institute for Health Research (NIHR) Programme Grant (the
IMPACT study), has already started this process but this is only one piece of research. We need a sustained approach
which involves research and its implementation in service delivery in order to encourage people to think differently about
psoriasis.
I hope that the See Psoriasis: Look Deeper campaign will encourage people living with psoriasis, their friends
and family as well as healthcare professionals and policy-makers, to look at the disease in a completely new way and be
motivated to make a positive change. I fully support the initiative and I am positive it will contribute to improved, holistic
care for patients with psoriasis.
Professor Chris Griffiths, Professor of Dermatology, The University of Manchester
9
Making a positive change to the lives of people with psoriasis
Endorsements
Together we can work towards improved holistic care for people with psoriasis. We just need to see beyond the skin and look deeper into their needs.
Action is needed to encourage people with psoriasis, together with their families and friends, to actively seek treatment which addresses the effects of this long-term condition on psychological wellbeing and quality of life. When they make that step, they need to be met with professionals who are able to understand and treat all aspects of their condition in a unified system that communicates well and co-ordinates their care.
Although there are many clinical aspects of psoriasis which can be managed with the correct assessment and treatment, a shift in thinking is also needed to improve lives. People with psoriasis deserve the best care; however, they need to feel comfortable in proactively seeking help. We need to create a stigma-free environment and rather than enduring rejection, people with psoriasis should expect to be met with understanding and support to ensure they continue with day-to-day activities and maintain a good quality of life.
We, as the See Psoriasis: Look Deeper Collaboration, call upon…
Policy makers to… � Ensure that the forthcoming NICE clinical guideline on psoriasis
adequately considers the multi-faceted long-term nature of psoriasis and the impact it has on an individual’s psychological wellbeing and quality of life
� Speed up the development of a Psoriasis Quality Standard that contains clear advice to the NHS on the need to consider the psychological wellbeing and quality of life impact of this long-term condition
� Ensure the Commissioning Guidance produced by the NHS Commissioning Board requires CCG to commission services for people with psoriasis that are multi-disciplinary, addressing the long-term impact on psychological wellbeing and quality of life
� Ensure that all local health economies establish clear referral pathways for psoriasis with closely allied multi-disciplinary teams who can address the multi-faceted nature of this long-term condition
People with psoriasis to… � Understand that help is available to address the multi-faceted
long-term nature of psoriasis including the impact it has on their psychological wellbeing and quality of life
� Talk to their healthcare professional about the impact of their psoriasis on their psychological wellbeing and quality of life, and to ask for support and resources when needed
Friends and family of those people with psoriasis to… � Understand that psoriasis can have a significant effect on a person’s
psychological wellbeing and quality of life, and to encourage the person living with psoriasis to talk to their healthcare professional about these effects and ask for help.
This is an important initiative highlighting the deeper impact of living with
psoriasis and the need for a greater understanding of the associated issues.
Clearly much greater support is required including interventions that consider
the psychological health consequences of the condition.
Tony Cassidy, Chair, British Psychological Society Division of Health Psychology
The Primary Care Dermatology Society (PCDS), which represents GPs with
an interest in skin disease, is acutely aware of the need for GP education
(which it provides) emphasising the psychological and social care for people
with psoriasis. It is not enough to merely offer creams without understanding
the needs of patients and their families as well as the options available for
ongoing care. GPs now have a greater role influencing the commissioning
process to make sure their patients receive what they need and deserve.
Dr Stephen Kownacki, Executive Chair PCDS
The See Psoriasis: Look Deeper Campaign is something to which I give my
wholehearted support, personally as a seasoned Consultant Dermatologist, but
also on behalf of the BAD as its current President. It is not widely appreciated
outside of Dermatology how much suffering psoriasis causes – unless you are
a patient, of course. Yet there is so much we CAN do in 2012, with education,
training and marshalling of multidisciplinary resources. This campaign is about
saying ‘Please, let us get on and do it’. I am with you all the way.
Chris Bunker, Consultant Dermatologist and president of the British
Association of Dermatologists
The See Psoriasis: Look Deeper campaign is a brilliant step forward
in helping patients feel supported in their day to day experience of living
with psoriasis. It also challenges carers, health care professionals and the
public to understand that living with psoriasis is very much more than living
with a skin disease. Psoriasis can have a marked impact on an individual’s
confidence, self-belief and mental health. All too often the impact of living
with psoriasis is severely underestimated by the public. See Psoriasis: Look
Deeper addresses that underestimate impact beautifully.
Dr Anthony Bewley, Consultant Dermatologist and lead of the British
Association of Dermatologist’s Psycho-dermatology Working Party
The BDNG fully support the report and the campaign See Psoriasis:
Look Deeper, recognising and looking beyond the physical symptoms of
psoriasis and dealing with the psychological wellbeing of our patients, which
will only lead to better outcomes for patients and their families.
The British Dermatological Nursing Group
Heading up a leading funder of skin disease research I welcome the report
and the wider See Psoriasis: Look Deeper campaign. Over recent years I have
observed how the physical distress caused by skin disease for many people is
mirrored by an often silent but deeper psychological suffering. I hope that this
campaign will help psoriasis sufferers find their voice whilst ensuring research
communities and health service providers listen and take action.
Matthew Patey, Chief Executive of the British Skin Foundation
I warmly welcome the work undertaken by the Collaboration and the
commitment they have shown in producing this valuable report. I hope the
report and accompanying See Psoriasis: Look Deeper campaign will ensure
that the levers within the NHS work to their full potential in order to tackle the
multidisciplinary challenges presented by psoriasis.
Sir Paul Beresford MP, Chair of the All Parliamentary party group on Skin

10
Ack
now
led
gem
ents
The Collaboration
Drs Chris Bundy and Sandy McBride are both members of the British Association of Dermatologists Psycho-dermatology working party led by Dr Anthony Bewley. This multi-professional group aims to identify the service needs and provision for people with skin conditions including psoriasis and improve the training for specialists in Dermatology to better manage psychological and psychiatric aspects of skin conditions including psoriasis.
The Mental Health FoundationThe Mental Health Foundation is the UK’s leading mental health research,
policy and service improvement charity. It is committed to reducing the suffering caused by mental ill health and to help everyone lead mentally healthier lives. It helps people to survive, recover from and prevent mental health problems by carrying out research, developing practical solutions for better mental health services, campaigning to reduce stigma and discrimination and promoting better mental health for us all.
Sandy McBride
Dr Sandy McBride is a Consultant Dermatologist at Royal Free Hampstead NHS Trust. She has an interest in the comprehensive management of patients
with psoriasis and has set up one of the only integrated psychology and dermatology services in the UK. She was awarded an NHS innovation award to develop the service.
Psoriasis Association
Psoriasis Association was founded in 1968 to provide information, advice and support to people with psoriasis and psoriatic arthritis. The organisation aims
to represent the views of patients at a local and national level with an ever-expanding voice, and to remain aware of the issues that really matter to its membership and to people whose lives are affected by psoriasis.
Christine Bundy
Dr Chris Bundy is a senior lecturer in Behavioural Medicine at the University of Manchester. Chris researches what psychological support works best for
people with psoriasis. With the rest of the Manchester team, Chris has developed online resources for people with psoriasis in a study funded by the Psoriasis and Psoriatic Arthropathy Alliance. She designs and delivers training programmes for all dermatology specialist staff to manage psychological aspects of psoriasis.
Professor Chris Griffiths, MD FRCP FMedSci
Professor Chris Griffiths gained a 1st class hons BSc in Anatomy and qualified in Medicine from St Thomas’ Hospital Medical
School, London University. He trained in Dermatology at St Mary’s Hospital, London, and at the University of Michigan, USA, where he was also on Faculty for 4 years. He was appointed to the Foundation Chair in Dermatology at the University of Manchester in 1994 and is an honorary consultant dermatologist at Salford Royal NHS Foundation Trust. Professor Griffiths developed the ‘hub-and-spoke’ model of dermatology services for Greater Manchester, and introduced a multi-disciplinary clinic for severe psoriasis – the Manchester Psoriasis Service – awarded Hospital Doctor Dermatology Team of the Year in 2002. At the University of Manchester he has served variously as: Head of Medicine and Neuroscience; Head of the School of Translational Medicine; Research Dean and; Director of the Manchester Academic Health Science Centre.
Professor Griffiths’ named lectureships include: Sydney Watson Smith (2006); Parkes Weber (2007); Von Zumbusch, Munich (2008) and; Hellerstrom, Stockholm (2010). He is co-founder of the International Psoriasis Council and is its President-Elect. He received the psoriasis lifetime achievement award of the American Skin Association in 2009. The Times of London named him as one of the UK’s Top 200 doctors in 2010 and in 2011 he was appointed as an NIHR Senior Investigator and elected to Fellowship of the Academy of Medical Sciences.
Professor Griffiths has been President of: the British Association of Dermatologists (2004-5); European Dermatology Forum (2010-11) and; British Society for Investigative Dermatology (1997-2000). He serves on the editorial boards of eight scientific journals. He has published 425 Pubmed cited articles in scientific journals, has an H-Index of 73 and is senior editor of Rook’s Textbook of Dermatology. Professor Griffiths has long-standing research interests in all aspects of psoriasis including immunological mechanisms, immunotherapy, pharmacogenomics, and the ‘brain–skin axis’.
11
References
1. What is Psoriasis, 2011, Accessed at: https://www.psoriasisassociation.org.uk/silo/files/No1%20what%20is.pdf Accessed: September 2012
2. Kimball AB, Gieler U, Linder D, et al. Psoriasis: is the impairment to a patient’s life cumulative? J Eur Acad Dermatol Venereol 2010;24:989–1004.
3. Kurd SK, Troxel AB, Crits-Christoph P, Gelfand JM. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol 2010;146(8):891–5.
4. National Institute for Health and Clinical Excellence. Psoriasis: the management of psoriasis. NICE guideline. Draft for consultation, May 2012. http://www.nice.org.uk/nicemedia/live/12344/59182/59182.pdf. Accessed: September 2012
5. Eedy D, Burge S, Potter J, et al, on behalf of The British Association Dermatologists and Clinical Effectiveness and Evaluation Unit, Royal College of Physicians Clinical Standards Department. An audit of the provision of dermatology services in secondary care in the United Kingdom with a focus on the care of people with psoriasis. January 2008.
6. Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Brit J Dermatol 1998;139:846–850.
7. Nelson PA, Chew-Graham CA, Griffiths CE, Cordingley L; The IMPACT Team. Recognition of need in health care consultations: a qualitative study of people with psoriasis. Br J Dermatol 2012; doi: 10.1111/j.1365-2133.2012.11217.x. [Epub ahead of print]
8. Eghlileb AM, Davies EEG, Finlay AY. Psoriasis has a major secondary impact on the lives of family members and partners. Brit J Dermatol 2007;156:1245–1250.
9. Meyer N, Paul C, Feneron D. Psoriasis: an epidemiological evaluation of disease burden in 590 patients. J Eur Acad Dermatol Venereol 2010;24:1075–1082.
10. Patient UK. Psoriasis Fact Sheet. Accessed at: http://www.patient.co.uk/health/Psoriasis.htm on 13 September 2012.
11. NHS Choices. Symptoms of psoriasis. Accessed at: http://www.nhs.uk/Conditions/Psoriasis/Pages/Symptoms.aspx on 13 September 2012.
12. Dubertret L, Mrowietz U, Ranki A, et al. EUROPSO Patient Survey Group. European patient perspectives on the impact of psoriasis: the EUROPSO patient membership survey. Br J Dermatol 2006;155(4):729–36.
13. Ibrahim G, Waxman R, Helliwell PS. The prevalence of psoriatic arthritis in people with psoriasis. Arthritis Care Res 2009;61(10):1373–1378.
14. Kimball AB, Gladman D, Gelfand JM, et al for the National Psoriasis Foundation. National Psoriasis Foundation clinical consensus on psoriasis comorbidities and recommendations for screening. J Am Acad Dermatol 2008;58:1031–42.
15. Menter A, Griffiths CE, Tebbey PW, et al; International Psoriasis Council. Exploring the association between cardiovascular and other disease-related risk factors in the psoriasis population:
the need for increased understanding across the medical community. J Eur Acad Dermatol Venereol 2010;24(12):1371–7.
16. Azfar RS, Seminara NM, Shin DB, et al. Increased Risk of Diabetes Mellitus and Likelihood of Receiving Diabetes Mellitus Treatment in Patients With Psoriasis. Arch Dermatol 2012;18:1–6. doi: 10.1001/archdermatol.2012.1401. [Epub ahead of print].
17. Griffiths CEM, Barker J. Pathogenesis and clinical features of psoriasis. Lancet 2007;370(9583):263–71.
18. Russo PA, Ilchef R, Cooper AJ. Psychiatric morbidity in psoriasis: a review. Australas J Dermatol 2004;45(3):155–9.
19. National Psoriasis Foundation Mental Health Issue Brief January 2012. Accessed at: http://www.psoriasis.org/document.doc?id=350 on 10 September 2012.
20. Ginsburg IH, Link BG. Psychosocial consequences of rejection and stigma feelings in psoriasis patients. Int J Dermatol 1993;32(8):587–91.
21. Sampogna F, Tabolli S, Abeni D, and the IDI Multipurpose Psoriasis Research on Vital Experiences (IMPROVE) investigators. Living with psoriasis: prevalence of shame, anger, worry, and problems in daily activities and social life. Acta Derm Venereol 2012;92:299–303.
22. Basra MK, Finlay AY. The family impact of skin diseases: the Greater Patient concept. Br J Dermatol 2007;156(5):929–37. Epub 2007 Mar 23.
23. Tadros A, Vergou T, Stratigos AJ, et al. Psoriasis: is it the tip of the iceberg for the quality of life of patients and their families? J Eur Acad Dermatol Venereol 2011;25(11):1282–7. Epub 2011 Jan 17.
24. McAleer MA, Mason DL, Cunningham S. Alcohol misuse in patients with psoriasis: identification and relationship to disease severity and psychological distress. Brit J Dermatol 2011;164:1256–1261.
25. Poikolainen K, Karvonen J, Pukkala E. Excess mortality related to alcohol and smoking among hospital-treated patients with psoriasis. Arch Dermatol 1999;35:1490–1493.
26. Mental Health Strategies (MHS) for Department of Health. 2010/11 National Survey of Investment in Adult Mental Health Services. October 2011.
27. Finlay AY, Coles EC. The effect of severe psoriasis on the quality of life of 369 patients. Brit J Dermatol 1995;132:236–-244.
28. Schmitt JM, Ford DE. Work Limitations and Productivity Loss Are Associated with Health-Related Quality of Life but Not with Clinical Severity in Patients with Psoriasis. Dermatology 2006;213:102–110.
29. British Journal of Dermatology: A meta-analysis of the effectiveness of psychological interventions for adults with skin conditions. The Department of Psychology, University of Sheffield. 2009.
30. NHS National Institute for Health and Clinical Excellence, Newsroom.http://www.nice.org.uk/newsroom/news/NICEShouldProduceGuidanceOnMultipleMorbidities.jsp?textonly=true. Accessed October 2012
For more information on psoriasis or the importance of emotional wellbeing and quality of life, please visit the following websites:
Psoriasis Association Mental Health Foundation https://www.psoriasis-association.org.uk/ http://www.mentalhealth.org.uk/
October 2012AXHUD120275o
The initiative is funded by an educational grant from Abbott UK.