screening for hepatocellular carcinoma in chronic carriers of hepatitis b virus: incidence and...
TRANSCRIPT
Screening for Hepatocellular Carcinoma in Chronic Carriers of Hepatitis B Virus: Incidence and Prevalence of Hepatocellular Carcinoma in
a North American Urban Population
MORRIS SHERMAN, KEVORK M. PELTENAN, AND CINDY LEE
Objective: To prospectively determine the prevalence and annual incidence of hepatocellular carcinoma in hepatitis B carriers in a heterogeneous urban North American population and to assess the diagnostic accu- racy of tests used for screening for this cancer. Design: Prospective cohort study of 1,069 chronic carriers of hepatitis B virus using screening with a-fetoprotein alone or in combination with ultrasonography every 6 months. Results: The mean age of the cohort was 39 -t 12 years (? SD), 65% were men, 71% were Asians. At the first screening visit, serum a-fetoprotein was 220 pgl L in 4%. In those subjects who were also screened by ultrasonography during the first visit, 9% were found to have focal lesions. Only 3 subjects were found to have hepatocellular carcinoma at the first screening, giving a prevalence of 281/100,000 chronic carriers of hepatitis B virus. The cohort was followed for 2,340 person-years (mean, 26 months follow-up, with a range from 6 to 60 months). During this period, 11 more subjects, 10 men and 1 woman, were diagnosed to have hepatocellular carcinoma (annual incidence, 470/100,000). In men only, the annual incidence was 657/100,000. During the study, 5 subjects died from hepatocellular carcinoma (annual mortality rate, 214/100,000). Sensitivity and specificity of serum a-fetoprotein >20 pg/L were 64.3% and 91.4%, respectively. For ultrasonography, sensitivity was 78.8% and specificity 93.8%. Conclusions: These data suggest that the incidence and prevalence of hepatocellular car- cinoma in hepatitis B carriers in our area, an urban North American setting, are as high as in countries where hepatitis B is endemic. Current screening tests have significant false-positive and false-negative rates,
Abbreviations: HBV, hepatitis B virus; HCC, hepatocellular carcinoma; AFP, a-fetoprotein; US, ultrasonography; ALT, alanine transaminase; AST aspartate transaminase; CI; confidence interval; HBeAg, hepatitis B e antigen.
From the Division of Gastroenterology, Department of Medicine, The To- ronto Hospital, and the University of Toronto, Toronto, Ontario, Canada.
Received July 28, 1994; accepted April 10, 1995. Supported by a grant from the National Research and Development Pro-
gram of Health and Welfare Canada, and from Schering Canada, Inc., Mon- treal, Canada. K.M.P. is the recipient of Scbering Fellowship in Hepatology at the University of Toronto.
Address reprint requests to: Morris Sherman, MD, PhD, The Toronto Hospi- tal (EN 9-2231, 200 Elizabeth St, Toronto, Ontario, M5G 2C4 Canada.
Copyright 0 1995 by the American Association for the Study of Liver Diseases.
0270-913919512202-0009$3.00/0
raising questions about the cost-benefit of screening for hepatocellular carcinoma in our study population. (HEP- ATOLOGY 199522~432-438.)
Studies from the Far East and sub-Saharan Africa, where hepatitis B virus (HBV) infection is endemic,' have indicated an etiologic role for the virus in the development of hepatocellular carcinoma (HCC).'s3 Most patients with symptomatic HCC have tumors that are not amenable to surgical re~ec t ion .~ ,~ In such patients, survival is limited to a few weeks or months. HCC is estimated to cause between 250,000 and 1 mil- lion deaths annually, ~ o r l d w i d e . ~ , ~
There is an increased interest in the use of screening tests to detect HCC in patients a t a stage before symp- toms develop, because it has been suggested that early disease may respond more favorably to treatment.' Studies from mainland Chinag and Alaska" support the view that screening with serum a-fetoprotein (AFP) is effective in finding small tumors. However, other investigators from Japan" and Taiwan'' have reported that serum AFP increases too late during development of HCC to be an effective screening method. They have suggested that repeated real-time ultrasonography (US) is a more sensitive and specific screening test. However, in Europe, two studies have shown that screening for HCC with US did not result in better survival.13J4
The usefulness, frequency, and cost-effectiveness of screening for HCC may well differ in different geo- graphic areas or among different ethnic populations, because there may be differences in the incidence and growth characteristics of HCC.15 There are also likely major differences in the epidemiology of hepatitis B between endemic and nonendemic areas, particularly with respect to age at which the disease is acquired. In endemic areas, HBV infection is usually acquired in childhood. In North America, where chronic HBV car- rier state occurs in less than 1% of the population and the annual incidence of HCC is below 4 cases per 100,000,16 it is likely that adult acquisition of the infec- tion is a significant factor. I t is unknown whether hepa- titis B carriers in North America have the same risk for HCC as do HBV carriers in endemic regions.17
432
HEPATOLOGY Vol. 22, No. 2, 1995 SHERMAN, PELTEKIAN, AND LEE 433
We have carried out a prospective study of HBV car- riers in the greater Toronto area, using serum AFP and US as the screening tests for HCC. The aims of this study were to determine the following: (1) the demo- graphics of chronic HBV carriers in our area; (2) the prevalence, incidence, and mortality of HCC in this population; and (3) the sensitivity, specificity, positive predictive value, and negative predictive value of AFP and US as screening tests for detection of HCC.
PATIENTS AND METHODS Subjects who tested positively for hepatitis B surface anti-
gen for more than 6 months and who were over the age of 18 years were eligible. Recruitment was by referral from gastro- enterologists and family physicians in the metropolitan To- ronto area. In addition, subjects were recruited through pub- licity about the Liver Cancer Screening Program through newspapers, radio, and television. Therefore, this study was both population-based (i.e., the population of asymptomatic HBV carriers with no evidence of liver disease) and clinic- based (patients with evidence of liver disease).
The study was designed as a feasibility study, predicated on the design of a planned larger randomized controlled study to determine if screening reduced the mortality from HCC. Therefore, after informed consent was obtained, subjects were randomized to be screened a t 6-month intervals with either AFP alone or AFP plus US.
At recruitment, subjects had tests performed for the follow- ing: blood count, prothrombin time, serum albumin, serum alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase, hepatitis B surface antigen, hepatitis B surface antibody, hepatitis B e antigen (HBeAg), hepatitis B e antibody, and AFP. Sera were tested for hepatitis delta, hepatitis C and human immunodeficiency virus only when clinically indicated. All hepatitis B serological tests were de- termined by commercial radio immunoassay kits (Abbott Laboratories, North Chicago, IL). AFP assay (normal value <5 pg&) was also performed by commercial kit (Abbott Labo- ratories). At the 6-month screening visits, ALT, AST, and AFP were repeated.
Patients who were randomized to US had high-resolution real-time US examination of the upper abdomen. Subjects who missed the screening appointments were contacted to determine whether the subject had withdrawn from study or whether an end-point (i.e., diagnosis of HCC or death from HCC or any other cause) had occurred.
Subjects in whom serum AFP was increased or in whom US showed a mass, had additional investigations. All subjects with increased AFP levels had a second AFP test performed 1 month later. In addition, all subjects in whom the AF'P was above 20 pg/L and in whom neither pregnancy nor reactiva- tion of chronic hepatitis was present also had a US examina- tion. Additional investigations were performed at the discre- tion of the attending physician. The diagnosis of HCC was confirmed by histological examination of tissue obtained from liver biopsy or surgical resection, or the combination of diag- nostically increased AFP plus typical features on ultrasonog- raphy or computed tomography.
The study protocol was approved by University of Toronto Review Committee on the Use of Human Subjects.
RESULTS Demographics of Hepatitis B Carriers
Between February 1989 and March 1994, 1,069 chronic hepatitis B carriers were referred to the Liver
0 " <20 20-29 30-39 40-49 50-59 6069 >69
Age group (years)
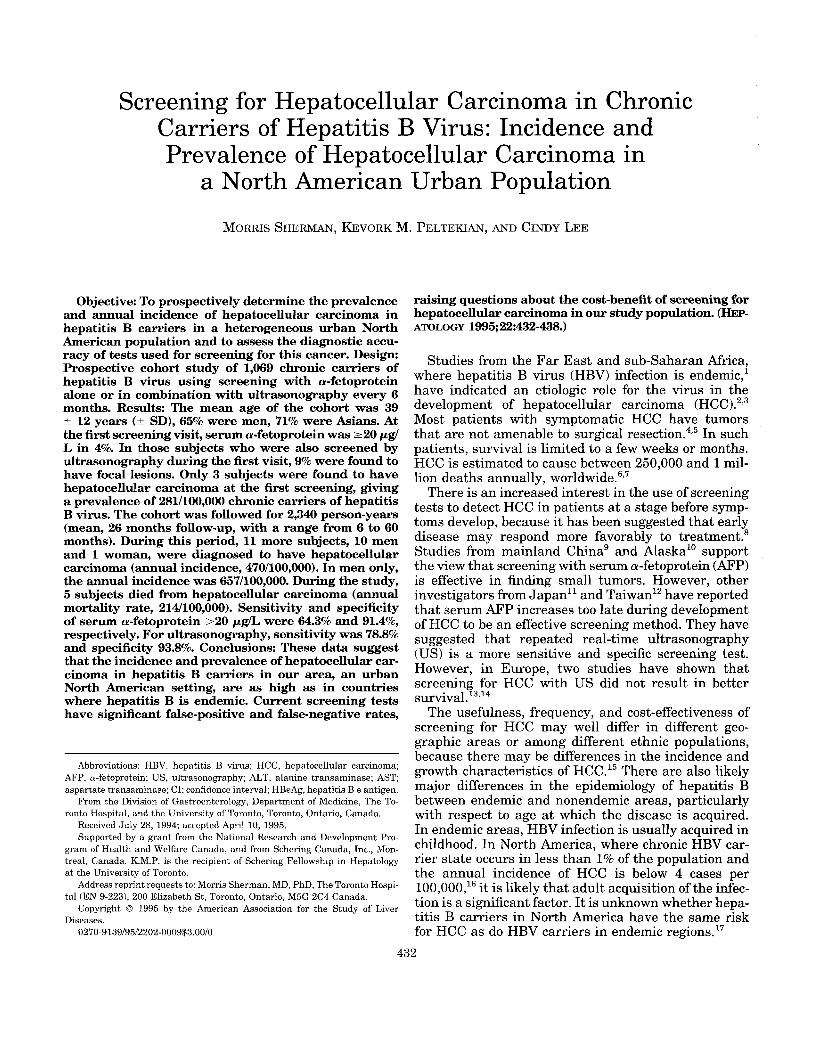
FIG. 1. The distribution of 1,069 subjects enrolled in the Liver Cancer Screening Program by age and gender.
Cancer Screening Program. The mean age of subjects was 39 % 12 years (% SD). Sixty-five percent were men. The distribution of the subjects by age and gender is shown in Fig. 1. Of the 1,037 subjects whose ethnic origin was recorded, 739 (71%) were Asian, 195 (19%) were white of European descent, and 26 (3%) were black. The remaining 77 (7%) were Middle Eastern or Latin American.
HBeAg or hepatitis B e antibody was determined in 1,047 subjects. A total of 243 subjects (23%) were HBeAg-positive, whereas 754 (72%) were HBeAg-nega- tive and hepatitis B e antibody-positive. In addition, 50 subjects (5%) tested negative for both HBeAg and hepatitis B e antibody.
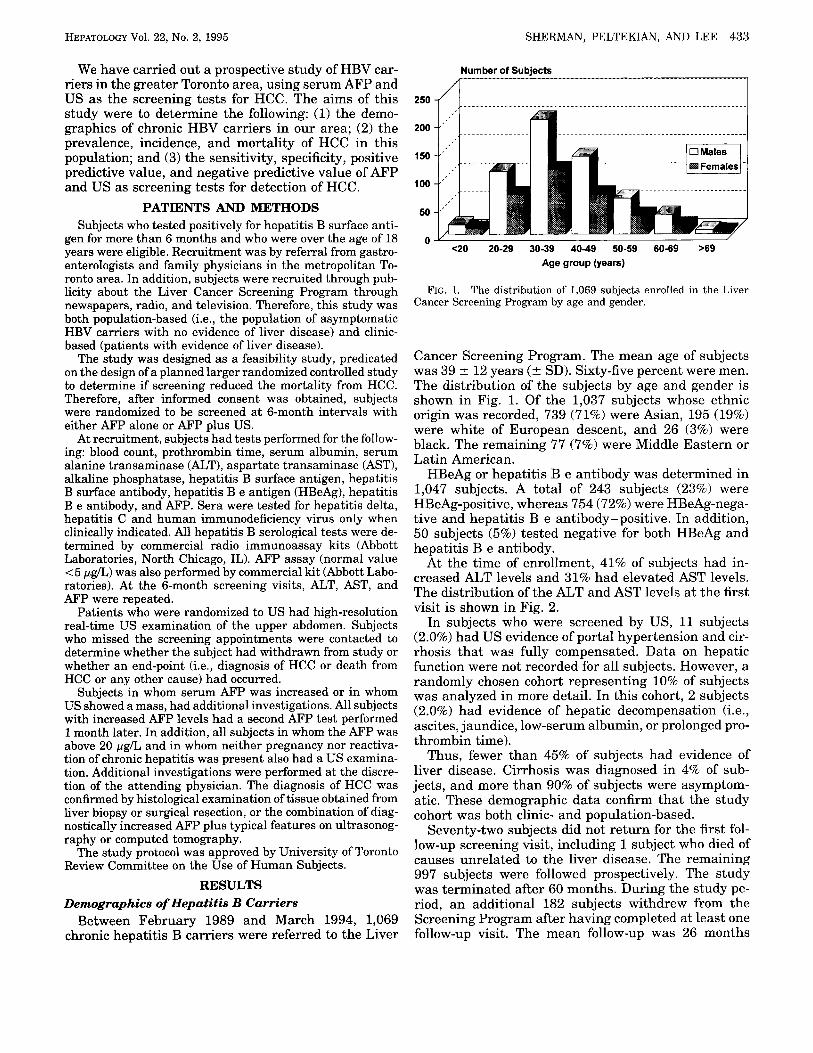
At the time of enrollment, 41% of subjects had in- creased ALT levels and 31% had elevated AST levels. The distribution of the ALT and AST levels at the first visit is shown in Fig. 2.
In subjects who were screened by US, 11 subjects (2.0%) had US evidence of portal hypertension and cir- rhosis that was fully compensated. Data on hepatic function were not recorded for all subjects. However, a randomly chosen cohort representing 10% of subjects was analyzed in more detail. In this cohort, 2 subjects (2.0%) had evidence of hepatic decompensation (i.e., ascites, jaundice, low-serum albumin, or prolonged pro- thrombin time).
Thus, fewer than 45% of subjects had evidence of liver disease. Cirrhosis was diagnosed in 4% of sub- jects, and more than 90% of subjects were asymptom- atic. These demographic data confirm that the study cohort was both clinic- and population-based.
Seventy-two subjects did not return for the first fol- low-up screening visit, including 1 subject who died of causes unrelated to the liver disease. The remaining 997 subjects were followed prospectively. The study was terminated after 60 months. During the study pe- riod, an additional 182 subjects withdrew from the Screening Program after having completed at least one follow-up visit. The mean follow-up was 26 months
434 SHERMAN, PELTEKIAN, AND LEE HEPATOLOGY August 1995
Number of Subjects
1
N - ~ x N 2 - 4 x N 4-10xN >10xN 0 "
N
FIG. 2. Initial serum ALT, AST, and AFP levels in 1,069 chronic HBV carriers enrolled in the Liver Cancer Screening Program. The AFP normal range for this graph is the laboratory normal of 5 pgl L. However, for the purposes of screening, we have used a level of 20 pg/L before considering further investigation.
(range, 6 to 60 months) accounting for 2,340 person- years of observation.
Prevalence and Incidence of HCC
At enrollment, HCC screening tests were truly posi- tive in 3 subjects, giving a prevalence for HCC of 281 per 100,000 (95% confidence interval [CII, 36 to 598/ 100,000) HBV carriers. In this study, we have defined prevalence as tumors detected at entry to the study. We recognize that tumors detected within the first year were likely to have been present at entry, but because they were undetectable at entry, we have elected to treat these as incident tumors. All tumors that oc- curred after enrollment were identified after 12 months of follow-up. In 11 other subjects, 10 male and 1 female,
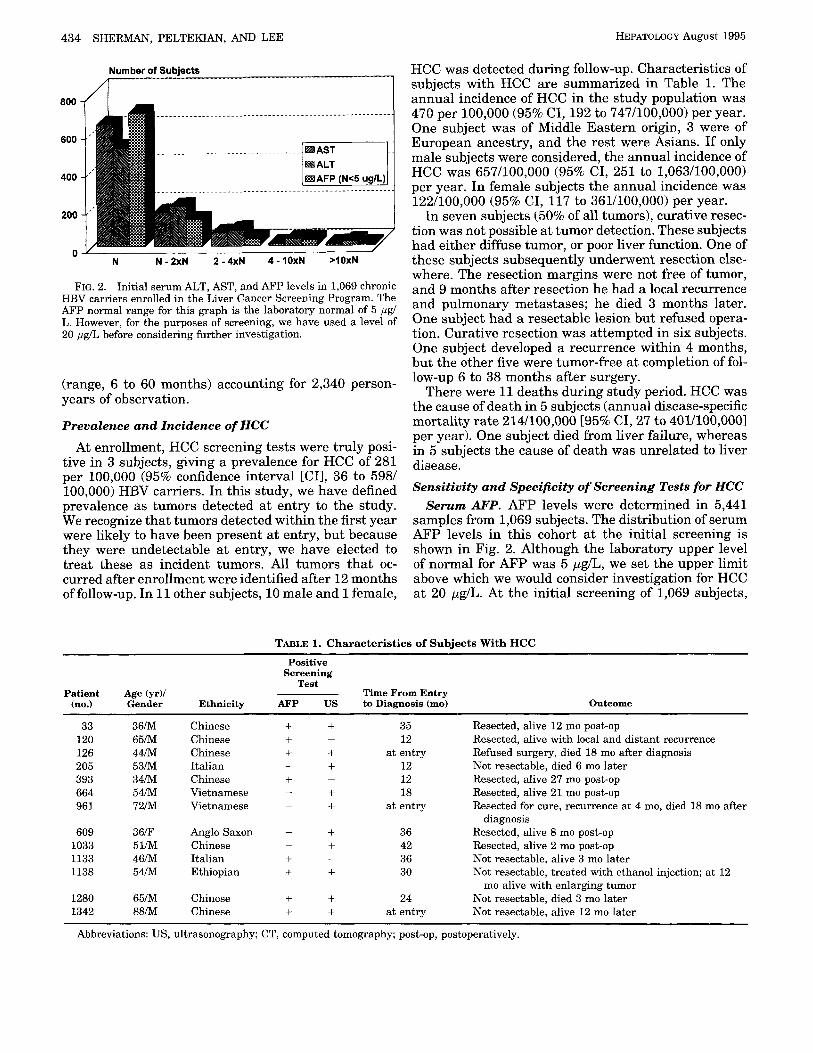
HCC was detected during follow-up. Characteristics of subjects with HCC are summarized in Table 1. The annual incidence of HCC in the study population was 470 per 100,000 (95% CI, 192 to 747/100,000) per year. One subject was of Middle Eastern origin, 3 were of European ancestry, and the rest were Asians. If only male subjects were considered, the annual incidence of HCC was 657/100,000 (95% CI, 251 to 1,063/100,000) per year. In female subjects the annual incidence was 122/100,000 (95% CI, 117 to 361/100,000) per year.
In seven subjects (50% of all tumors), curative resec- tion was not possible at tumor detection. These subjects had either diffuse tumor, or poor liver function. One of these subjects subsequently underwent resection else- where. The resection margins were not free of tumor, and 9 months after resection he had a local recurrence and pulmonary metastases; he died 3 months later. One subject had a resectable lesion but refused opera- tion. Curative resection was attempted in six subjects. One subject developed a recurrence within 4 months, but the other five were tumor-free at completion of fol- low-up 6 to 38 months after surgery.
There were 11 deaths during study period. HCC was the cause of death in 5 subjects (annual disease-specific mortality rate 214/100,000 [95% CI, 27 to 401/100,0001 per year). One subject died from liver failure, whereas in 5 subjects the cause of death was unrelated to liver d' isease. Sensitivity and Specificity of Screening Tests for HCC
Serum AFP. AFP levels were determined in 5,441 samples from 1,069 subjects. The distribution of serum AFP levels in this cohort at the initial screening is shown in Fig. 2. Although the laboratory upper level of normal for AFP was 5 ,ug/L, we set the upper limit above which we would consider investigation for HCC at 20 ,ug/L. At the initial screening of 1,069 subjects,
TABLE 1. Characteristics of Subjects With HCC
Positive Screening
Test Patient Age (yrY Time From Entry
(no.) Gender Ethnicity AFP US to Diagnosis (mo) Outcome
33 120 126 205 393 664 961
609 1033 1133 1138
1280 1342
-
3 6 m 6 5 m 4 4 m 5 3 m 3 4 m 54/M 72/M
36/F 5 1/M 4 6 m 5 4 m
65/M 8 8 m
~~~
Chinese Chinese Chinese Italian Chinese Vietnamese Vietnamese
Anglo Saxon Chinese Italian Ethiopian
Chinese Chinese
+ + + + +
+
-
- - + + +
- -
+ +
-
-
- + + +
+ + + +
35 12
at entry 12 12 18
at entry
36 42 36 30
24 at entry
Resected, alive 12 mo post-op Resected, alive with local and distant recurrence Refused surgery, died 18 mo after diagnosis Not resectable, died 6 mo later Resected, alive 27 mo post-op Resected, alive 21 mo post-op Resected for cure, recurrence at 4 mo, died 18 mo after
Resected, alive 8 mo post-op Resected, alive 2 mo post-op Not resectable, alive 3 mo later Not resectable, treated with ethanol injection; a t 12
mo alive with enlarging tumor Not resectable, died 3 mo later Not resectable, alive 12 mo later
diagnosis
Abbreviations: US, ultrasonography; CT, computed tomography; post-op, postoperatively.
HEPATOLOGY Vol. 22, NO. 2, 1995 SHERMAN, PELTEKIAN, AND LEE 435
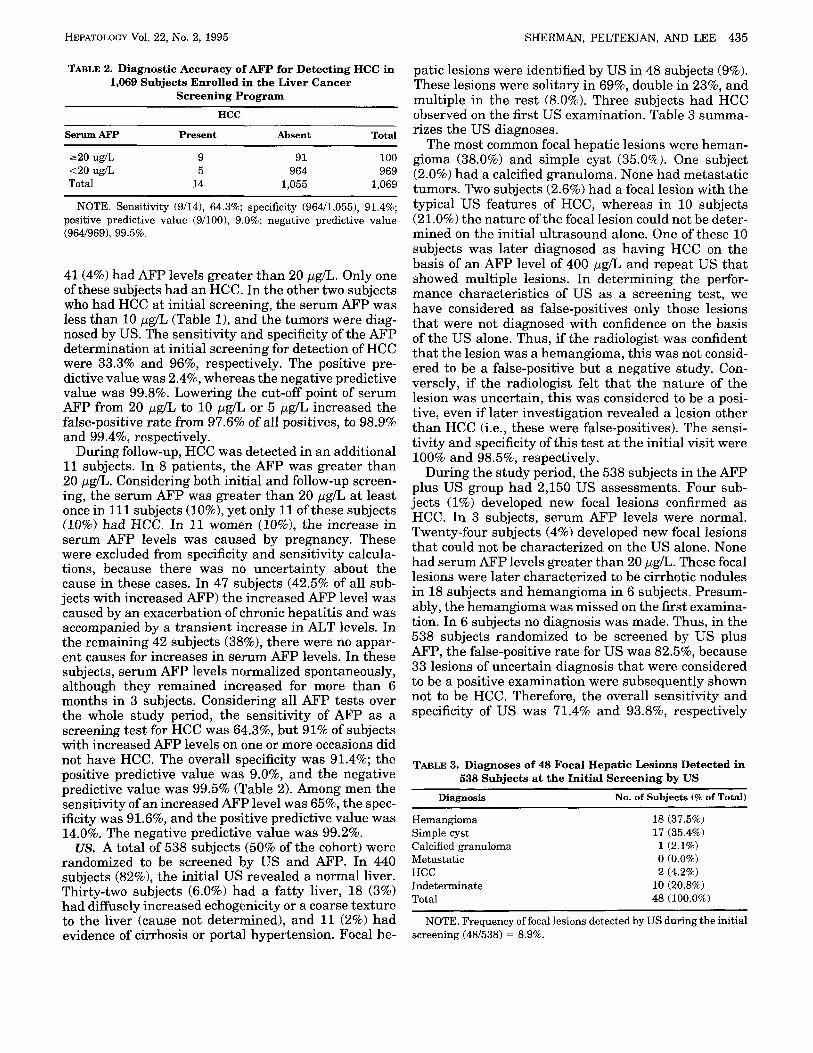
TABLE 2. Diagnostic Accuracy of AFP for Detecting HCC in 1,069 Subjects Enrolled in the Liver Cancer
Screening Program ~~
HCC
Serum AFP Present Absent Total
220 ug/L 9 91 100 <20 ug/L 5 964 969 Total 14 1,055 1,069
NOTE. Sensitivity (9/14), 64.3%; specificity (964/1,055), 91.4%; positive predictive value (9/100), 9.0%; negative predictive value (964/969), 99.5%.
41 (4%) had AFP levels greater than 20 pgL. Only one of these subjects had an HCC. In the other two subjects who had HCC at initial screening, the serum AFP was less than 10 pgL (Table 11, and the tumors were diag- nosed by US. The sensitivity and specificity of the AFP determination at initial screening for detection of HCC were 33.3% and 96%, respectively. The positive pre- dictive value was 2.4%, whereas the negative predictive value was 99.8%. Lowering the cut-off point of serum AFP from 20 yglL to 10 pglL or 5 ygL increased the false-positive rate from 97.6% of all positives, to 98.9% and 99.4%, respectively.
During follow-up, HCC was detected in an additional 11 subjects. In 8 patients, the AFP was greater than 20 ygk. Considering both initial and follow-up screen- ing, the serum AFP was greater than 20 pg/L at least once in 111 subjects (lo%), yet only 11 of these subjects (10%) had HCC. In 11 women (lo%>, the increase in serum AFP levels was caused by pregnancy. These were excluded from specificity and sensitivity calcula- tions, because there was no uncertainty about the cause in these cases. In 47 subjects (42.5% of all sub- jects with increased AFP) the increased AFP level was caused by an exacerbation of chronic hepatitis and was accompanied by a transient increase in ALT levels. In the remaining 42 subjects (38%), there were no appar- ent causes for increases in serum AFP levels. In these subjects, serum AFP levels normalized spontaneously, although they remained increased for more than 6 months in 3 subjects. Considering all AFP tests over the whole study period, the sensitivity of AFP as a screening test for HCC was 64.3%, but 91% of subjects with increased AFP levels on one or more occasions did not have HCC. The overall specificity was 91.4%; the positive predictive value was 9.0%, and the negative predictive value was 99.5% (Table 2). Among men the sensitivity of an increased AFP level was 65%, the spec- ificity was 91.6%, and the positive predictive value was 14.0%. The negative predictive value was 99.2%.
US. A total of 538 subjects (50% of the cohort) were randomized to be screened by US and AFP. In 440 subjects (82%), the initial US revealed a normal liver. Thirty-two subjects (6.0%) had a fatty liver, 18 (3%) had diffusely increased echogenicity or a coarse texture to the liver (cause not determined), and 11 (2%) had evidence of cirrhosis or portal hypertension. Focal he-
patic lesions were identified by US in 48 subjects (9%). These lesions were solitary in 69%, double in 23%, and multiple in the rest (8.0%). Three subjects had HCC observed on the first US examination. Table 3 summa- rizes the US diagnoses.
The most common focal hepatic lesions were heman- gioma (38.0%) and simple cyst (35.0%). One subject (2.0%) had a calcified granuloma. None had metastatic tumors. Two subjects (2.6%) had a focal lesion with the typical US features of HCC, whereas in 10 subjects (21.0%) the nature of the focal Iesion could not be deter- mined on the initial ultrasound alone. One of these 10 subjects was later diagnosed as having HCC on the basis of an AFP level of 400 ygL and repeat US that showed multiple lesions. In determining the perfor- mance characteristics of US as a screening test, we have considered as false-positives only those lesions that were not diagnosed with confidence on the basis of the US alone. Thus, if the radiologist was confident that the lesion was a hemangioma, this was not consid- ered to be a false-positive but a negative study. Con- versely, if the radiologist felt that the nature of the lesion was uncertain, this was considered to be a posi- tive, even if later investigation revealed a lesion other than HCC (i.e., these were false-positives). The sensi- tivity and specificity of this test at the initial visit were 100% and 98.5%, respectively.
During the study period, the 538 subjects in the AFP plus US group had 2,150 US assessments. Four sub- jects (1%) developed new focal lesions confirmed as HCC. In 3 subjects, serum AFP levels were normal. Twenty-four subjects (4%) developed new focal lesions that could not be characterized on the US alone. None had serum AFP levels greater than 20 pgL. These focal lesions were later characterized to be cirrhotic nodules in 18 subjects and hemangioma in 6 subjects. Presum- ably, the hemangioma was missed on the first examina- tion. In 6 subjects no diagnosis was made. Thus, in the 538 subjects randomized to be screened by US plus AFP, the false-positive rate for US was 82.5%, because 33 lesions of uncertain diagnosis that were considered to be a positive examination were subsequently shown not to be HCC. Therefore, the overall sensitivity and specificity of US was 71.4% and 93.8%, respectively
TABLE 3. Diagnoses of 48 Focal Hepatic Lesions Detected in 538 Subjects at the Initial Screening by US
Diagnosis No. of Subjects (% of Total)
Hemangioma Simple cyst Calcified granuloma Metastatic HCC Indeterminate Total
18 (37.5%) 17 (35.4%) 1(2.1%) 0 (0.0%) 2 (4.2%)
10 (20.8%) 48 (100.0%)
NOTE. Frequency of focal lesions detected by US during the initial screening (48/538) = 8.9%.

436 SHERMAN, PELTEKIAN, AND LEE HEPATOLOGY August 1995
TABLE 4. Diagnostic Accuracy of US for HCC in 538 Subjects Randomized to Screening
With AFP and US HCC
us Present Absent Total Suspicious focal lesions 5 33 38 No focal lesions 2 498 500 Total 7 531 538
NOTE. Excludes subjects in the AFP only group who had US because of elevated AFP. The use of US under these circumstances is not true screening. If these US examinations are included the overall sensitivity is 78.6%. Sensitivity (5/7), 71.4%; specificity (498/ 531), 93.8%; positive predictive value (5/33), 15.1%; negative pre- dictive value (498/500), 98.4%.
(Table 4). The positive predictive value of US was 15.1%, and the negative predictive value was 98.4%.
Subjects randomized to screening with AFP alone, whose serum AFP was >20 pg/L during follow-up had US assessment of the upper abdomen if neither reacti- vation of hepatitis nor pregnancy was present. An addi- tional 22 subjects (4%) randomized to screening with AFP alone (n = 531) required US. Focal lesions compat- ible with HCC were identified in 4 subjects. In 3 others with markedly increased and increasing serum AFP levels, US remained negative, but HCC was diagnosed by computed tomography or angiography (Table 1). Thus, in the 11 subjects who developed HCC during follow-up, US was falsely negative in 3, in that the US did not detect HCC at a stage when AFP became increased. Overall, including subjects randomized to US and AFP and those randomized to AFP only, in whom US was done in follow-up of an increased AFP level, US was positive in 11 of 14 subjects with HCC, resulting in an overall sensitivity of 78.6%.
DISCUSSION
Our study has shown that in our urban North Ameri- can population the risk of hepatocellular carcinoma is similar to that reported in studies from countries where hepatitis B is endemic.2,10~1s The study population is representative of the distribution of hepatitis B carri- ers in Toronto (i.e., mainly subjects of Asian descent and, to a lesser extent, subjects of Southern and East- ern European descent). As in other studies, HCC was much more frequent in men than in women and was more frequent in Asians than in subjects of other ethnic backgrounds. The small number of tumors that devel- oped precluded drawing conclusions about differences in incidence in different ethnic groups. The population studied was drawn from the practices of gastroenterolo- gists and family physicians, as well as from the general public, who became aware of the study through adver- tising in the media and by word-of-mouth. It is routine practice for physicians looking after immigrant com- munities in Toronto to test all such patients for HBV. Only 2.4% of subjects had any evidence of cirrhosis, although 40% had increased liver enzymes at recruit-
ment. Thus, the study population is probably represen- tative of the larger population of hepatitis B carriers with respect to presence and severity of liver disease.
There are few prospective studies on the incidence of HCC in an urban North American population. Stud- ies in other countries have reported that the incidence is between 387 to 527/100,000/year.2~'031g~zo In one North American study from the National Institutes of Health, 2 subjects with HCC were found in 166 chronic HBV carriers observed for 8 years." A case-control study in New York showed a relative risk of HCC of 9.7," which is 10-fold less than that reported from Taiwan.' In a prospective study of 1,925 subjects of Asian descent in the Delaware Valley, the incidence was 155/100,000/ year.23 In a smaller (207 subjects) Asian population in California, the incidence was in excess of 3,0001 100,000/year.24 The difference in these two studies is probably because of the high prevalence of cirrhosis in the California study.
In contrast, in a longitudinal study of hepatitis B carriers in Montreal who were believed to be infected in childhood, no HCCs had been detected after 16 years of follow-up.25 It is possible that this cohort was too young to have developed a significant incidence of HCC. The mean age of this cohort was 46 -+ 8 years (? SD). In our study, five subjects with HCC were identified in the cohort of similar age (e.g., 30 to 59 years).
The differences in the incidence of HCC reported by different studies may have several explanations. First, it is not always clear that populations in different stud- ies are comparable. Clinic-based studies would be ex- pected to include a high proportion of patients with established cirrhosis, in whom the incidence of HCC would be expected to be higher. On the other hand, population-based studies would be expected to have a lower proportion of subjects with cirrhosis, so the ex- pected incidence of HCC would also be lower. Another explanation may be that the risk of HCC varies in dif- ferent populations of HBV carriers. In populations in which infection is largely acquired in adulthood (e.g., in North America), the risk of HCC may be lower than in those who acquire the infection in childhood. Alter- natively there may be environmental factors present in Asian countries that are not present in North America, such as cocarcinogens that may be responsible for the higher incidence of HCC in Asian HBV carriers. Ma- toxin is one factor that has been widely held to play a part in the pathogenesis of HCC in Asia.
Screening for HCC is widely believed to be an effec- tive form of secondary prevention. However, the effi- cacy of screening in decreasing the mortality from HCC has never been shown. Screening studies have shown that it is possible to find small lesions that may be r e~ec tab le .~~ , '~ In two studies from Italy, screening de- tected small tumors that were resected if possible. However, the mortality in the resected and unresected groups was ~ i m i 1 a r . l ~ ~ ~ ~ These were clinic-based studies in subjects who were cirrhotic; therefore, the resection rate was lower than has been reported elsewhere,28 and the mortality rate was correspondingly high. However,

HEPATOLOGY Vol. 22, No. 2, 1995 SHERMAN, PELTEKIAN, AND LEE 437
clinic-based populations are not ideal for evaluating the benefits of screening, because the prevalence of cir- rhosis is likely to be high compared with population- based screening. Cirrhosis may preclude resection in a high proportion of subjects and will adversely influence survival. If screening is to be widely applied, the major- ity of subjects who will be screened (i.e., the hepatitis B population at large) will not have cirrhosis or will have only mild cirrhosis. Thus, the incidence of HCC is likely to be lower than in a clinic population. Further- more, the rate of false-positive tests, particularly with ultrasonography, is likely to be higher.
The efficacy of screening cannot be evaluated with the available data in the literature because of method- ological problems, such as lack of control groups, lack of randomization, and the lack of suitable end points. A study to evaluate the efficacy of screening for HCC must include a suitable population (i.e., representative of the larger population of hepatitis B carriers). There should be an unscreened control group. The end point should be disease-specific mortality not tumor detec- tion. No such study has been reported to date.
It is not clear that the studies reported so far can be applied to an urban North American population of noncirrhotic hepatitis B carriers. As discussed pre- viously, the incidence of HCC may be different in those who acquire hepatitis B in childhood than in adult ac- quired disease. In our population, the majority of carri- ers are likely to have acquired their disease in child- hood in their native countries. In the Delaware Valley study referred to earlier,23 the study population was exclusively Asian, and the incidence of HCC was 155/ 100,00O/year. Our study includes a more heterogeneous population, yet we report a higher incidence of HCC. However, the number of subjects with HCC in both studies is small (3 and 14), and one more or one less HCC would make a large difference to the incidence.
We used the standard recommended screening tests, namely US and AFP. Both tests had significant false- positive and false-negative rates. The AFP level was increased for reasons other than HCC far more often than it was increased because of HCC. In most cases, clinical judgment prevented invasive investigations be- ing performed unnecessarily, but additional noninva- sive investigations were required in some cases, with the attendant increase in costs and in patient anxiety. Furthermore, AFP screening missed 5 of the 14 tumors. US missed 3 of 9 lesions that presented with high AFP levels. However, a greater problem was the finding of suspicious masses on US, which required intensive in- vestigation, but turned out not to be HCC.
Our findings highlight that if screening of hepatitis B carriers is to become widespread in North America it will bring with it an increase in the number of unnec- essary investigations performed to confirm false-posi- tive results, with attendant increases in costs and pa- tient and physician anxiety.
The sample size in this study was too small to allow estimation of which method of screening was more ef- fective. Indeed, such a study may require upwards of
10,000 subjects. The question is an important one, be- cause there are millions of hepatitis B carriers at risk for HCC, and to screen such large numbers will be very expensive. Although hepatitis B vaccination will eventually eliminate hepatitis B as a cause for HCC, it will be at least a generation before the prevalence of this disease decreases significantly.
Although the number of tumors detected in our study is small and may not be representative of tumors found on screening in general, more than 50% of tumors de- tected by screening were not resectable. Furthermore, one subject developed a recurrence after surgery, cast- ing further doubt on the value of screening.
There may be a difference in resectability when HCC is discovered within the first year of screening (preva- lent tumors) compared with those discovered after the first year (incident tumors). It is possible the prevalent tumors are more advanced at detection, resulting in a lower likelihood of cure. In our study, there may have been a difference in the resectability rate in prevalent or incident tumors (1/3 resectable vs. 5/11 respectively), but the numbers are too small to draw any conclusions.
The data from this study bring into question the value of screening HBV carriers for HCC and should dampen the enthusiasm with which screening is being performed. However, this study is not definitive, in that the sample size and period of follow-up are insufficient to allow any estimation of whether screening alters disease-specific mortality, the gold standard of cancer screening. Rather, we hope that these results provide the stimulus for the development of a properly con- trolled trial to answer this important question.
Screening hepatitis B carriers in North America may or may not be an effective way of decreasing the mortal- ity from the disease, but until the completion of a ran- domized, controlled study any screening is performed more in hope of benefit than with certainty.
Acknowledgment: We are indebted to Drs J. E. Heathcote, L. M. Blendis, S. V. Feinman, and G. A. Levy and all other physicians from the greater Toronto area who referred subjects to the Liver Cancer Screen- ing Program.
1.
2.
3.
4.
5.
6.
REFERENCES
Szmuness W. Hepatocellular carcinoma and the hepatitis B vi- rus: evidence for a causal association. Prog Med Virol 1978; 24:40-69. Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carci- noma and hepatitis B virus: a prospective study of 22,707 men in Taiwan. Lancet 1981;2:1129-1133. Steiner PE. Cancer of the liver and cirrhosis in trans-Saharan Africa and the United States of America. Cancer 1960; 13:1085- 1145. Maraj R, Kew MC, Hyslop FLJ. Resectability rate of hepatocellu- lar carcinoma in rural southern Africans. Br J Surg 1988; 75:335- 338. Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hase- gawa H, Nakajima Y, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment: study of 850 patients. Cancer 1985;56:918-928. Zhou XD, Tang ZY, Yu YQ, Yang BH, Lin ZY, Lu J Z , Lin ZY, et al. Long-term survivors after resection for primary liver cancer:

438 SHERMAN, PELTEKIAN, AND LEE HEPATOLOGY August 1995
clinical analysis of 19 patients surviving more than ten years. Cancer 1989; 63:2201-2206.
7. London WT. Primary hepatocellular carcinoma-etiology, pathogenesis, and prevention. Hum Pathol 1981; 12:1085-1097.
8. Tang ZY, Yu YG, Zhou XD, Yang BH, Ma ZC, Lin ZY. Subclinical hepatocellular carcinoma: an analysis of 391 patients. J Surg Oncol 1993;3(suppl):55-58.
9. Tang ZY, Yang BH, Tang CL, Yu YQ, Lin ZY, Weng HZ. Evalua- tion of population screening for hepatocellular carcinoma. Chin Med J-Peking 1980;93:795-799.
10. Heyward WL, Lanier AP, McMahon BJ, Fitzgerald MA, Kil- kenny S, Paprocki TR. Early detection of primary hepatocellular carcinoma: screening for primary hepatocellular carcinoma among persons infected with hepatitis B virus. JAMA 1985;
11. Liver Cancer Study Group of Japan. Primary liver cancer in Japan: clinicopathologic features and results of surgical treat- ment. Ann Surg 1990;211:277-287.
12. Hsu HC, Wu TT, Wu MZ, Sheu JC, Lee CS, Chain DS. Tumor invasiveness and prognosis in resected hepatocellular carci- noma: clinical and pathogenetic implications. Cancer 1988;
13. Cottone M, Virdone R, Fusco G, Orlando A, Turri M, Caltagirone M, Maringhini A, et al. Asymptomatic hepatocellular carcinoma in Child's A cirrhosis: a comparison of natural history and surgi- cal treatment. Gastroenterology 1989;96:1566-1571.
14. Colombo M, de Franchis R, del Ninno E, Sangiovanni A, de Fazio C, Tommasini M, Donato MF, et al. Hepatocellular carcinoma in Italian patients with cirrhosis. N Engl J Med 1991;325:675- 680.
15. McMahon BJ, London T. Workshop on screening for hepatocellu- lar carcinoma [commentary]. J Nat Cancer Instit 1991;83:916- 919.
16. Sandler DP, Sandler RS, Horney LF. Primary liver cancer mor- tality in the United States. J Chronic Dis 1983;36:227-236.
17. Di Bisceglie AM, Order SE, Klein JL, Waggoner JG, Sjogren MH, Kuo G, Houghton M, et al. The role of chronic viral hepatitis in hepatocellular carcinoma in the United States. Am J Gas- troenterol 1991;86:335-338.
18. Obata H, Hayashi N, Motoike Y. A prospective study on the
254:3052-3054.
6112095-2099.
development of hepatocellular carcinoma from liver cirrhosis with persistent hepatitis B virus infection. Int J Cancer
19. Beasley RP. Hepatitis B virus: the major etiology of hepatocellu- lar carcinoma. In: Fortner JG, Rhoads JE, eds. Accomplishments in cancer research, 1987. Philadelphia: Lippincott, 1988:80-106.
20. McMahon BJ, Alberts SR, Wainwright RB, Bulkow L, Lanier AP. Hepatitis B-related sequelae: prospective study in 1400 hepatitis B surface antigen-positive Alaska native carriers. Arch Intern Med 1990; 150:1051-1054.
21. Di Bisceglie AM, Hoofnagle JH. Elevations in serum alpha-feto- protein levels in patients with chronic hepatitis B. Cancer
22. Prince AM, Alcabes P. The risk of development of hepatocellular carcinoma in hepatitis B virus carriers in New York a prelimi- nary estimate using death-records matching. HEPATOLOGY
23. London WT, Atleson J , Eto T, Fine M, Hwang C. Early detection of hepatocellular carcinoma among Asians living in the United States. In: Tabor E, Di Bisceglie AM, Purcell RH, eds. Etiology, pathology, and treatment of hepatocellular carcinoma in North America. Houston: Gulf Publishing, 1991:243-254.
24. Tong MJ, Schwindt RR, Lo G-H, Co RL. Chronic hepatitis and hepatocellular carcinoma in Asian Americans. In: Tabor E, Di Bisceglie AM, Purcell RH, eds. Etiology, pathology, and treat- ment of hepatocellular carcinoma in North America. Houston: Gulf Publishing, 1991:15-24.
25. Villeneuve JP, Desrochers M, Infante-Rivard C, Willems B, Ray- mond G, Bourcier M, Cote J , et al. A long-term follow-up of healthy hepatitis B virus surface antigen carriers in Montreal. Gastroenterology 1994; 106: 1000-1005.
26. Shinagawa T, Ohto M, Kimura K, Stunetomi S, Morita M, Saisho H, et al. Diagnosis and clinical features of small hepatocellular carcinoma with emphasis on utility of real-time ultrasonogra- phy. Gastroenterology 1984; 86:495-502.
27. Chen D-S, Sung J-L, Sheu J-C, Lai M-Y, How S-W, Hsu H-C, et al. Serum alpha-fetoprotein in the early stage of human hepato- cellular carcinoma. Gastroenterology 1984; 86:1404-1409.
28. Okuda K. Primary liver cancer: quadrennial review lecture. Di- gestive Diseases and Sciences 1986;31:1333-1463.
1979;24:741-747.
1989;64:2117-2120.
1982; ~ ( s u P P ~ ) : 15s-20s.