scottish polypharmacy programme: synthesis of case ... - ific
TRANSCRIPT

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Scottish Polypharmacy Programme:
Synthesis of case studies, PESTEL and SWOT
Alpana Mair Martin Wilson
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
The evolution of polypharmacy in Scotland
A history lesson

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
1980s
Early papers encouraging move from pharmacists as dispensers to pharmacists practice and involvement in prescribing and review
Nuffield Committee of Inquiry Pharmacy. A Report to the National Foundation 1986
The way forward for hospital pharmaceutical services 1988 HC88(54) London and 1988 (GEN) 32 in Scotland
1980s
Prescribing GP and consultant led. Much variability.
Lower prescribing rates
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
1990s
• Moves to highlight potential positive impact of Pharmacy profession to future healthcare
Strategy for the Future of Pharmacy RPSGB 1995
Clinical pharmacy in the hospital pharmaceutical service: a framework for Practice Scottish Office 1996
From compliance to concordance, achieving shared goals in medicines taking RPS (1997).
Clinical pharmacy practice in primary care: a framework for the provision of community-based NHS Pharmaceutical Services Scottish Office 1999
1990s
• Rise of evidenced based medicine• Cochrane Data Base
• SIGN 1993
• NICE 1999
• Profusion of RCTs driving prescribing
• Primary and Secondary Prevention

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
2000s
• 2001 Health and social care act amended to allow non medical prescribers inc Pharmacy
• 2007 regulations allow Pharmacist Prescribers
2000s
• Standardisation of prescribing around evidenced based medicine
• QOF 2004
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
2010 +
• Increase in Pharmacist Prescribers
• Prescription for Excellence 2013• Pharmacist integration to
primary care
2010 +
• 2010 to 2012• Local areas develop
polypharmacy guidelines• Highland, Tayside
• Lothian Poly reviews and ACP
• 2012 1st Edition National Guideline
• 2014/15 Polypharmacyintroduced to QOF
• 2015 2nd Edition• Most downloaded doc on
SIGN website.
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
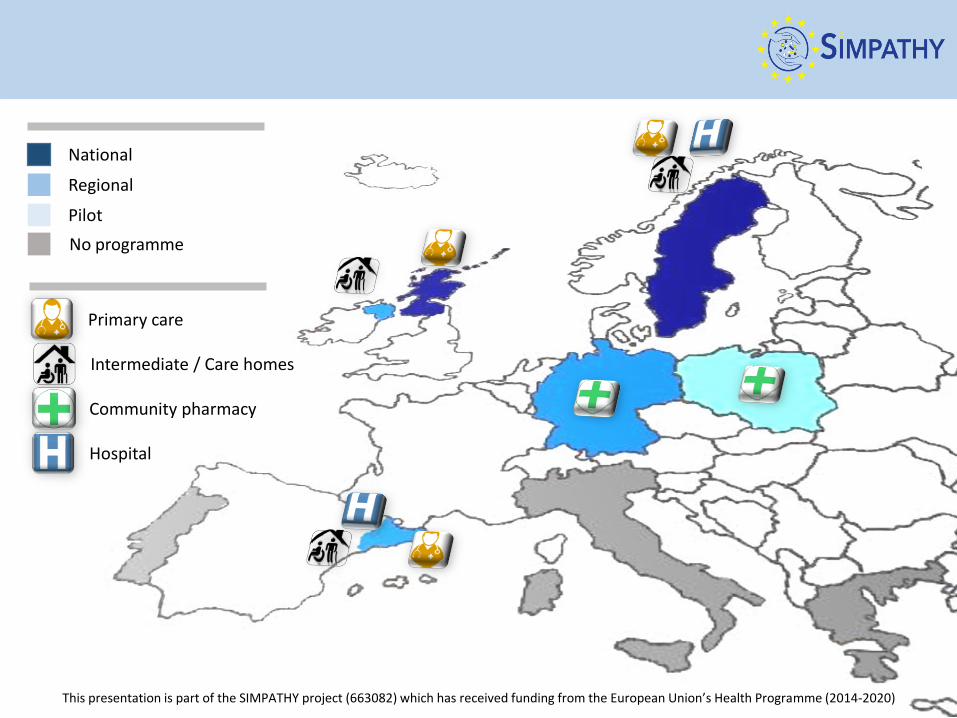
Hospital
Intermediate / Care homes
Primary care
Community pharmacy
National
Regional
Pilot
No programme

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Key Concepts - Clinical
•Development and reinforcement of structure to drug review / prescribing
•Adult specific goals•Opened the box on ‘Bang for Buck’ on guideline medications•Focus on drug safety.

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Game changing concepts
If guideline says Prescribe X drug it is GUIDANCE not INSTRUCTION and not prescribing may well be acceptable (and often desirable) in a range of situations
One size does not fit all.....

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Why did you jump off a cliff?
Because the Guideline told me to.

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Designed to encourage multidisciplinary practice
• Aim of improving working between• Community Pharmacy• [Prescribing support pharmacists]• Hospital Pharmacy• GP• Hospital Consultants
• Getting these links to work well main way to make progress.

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
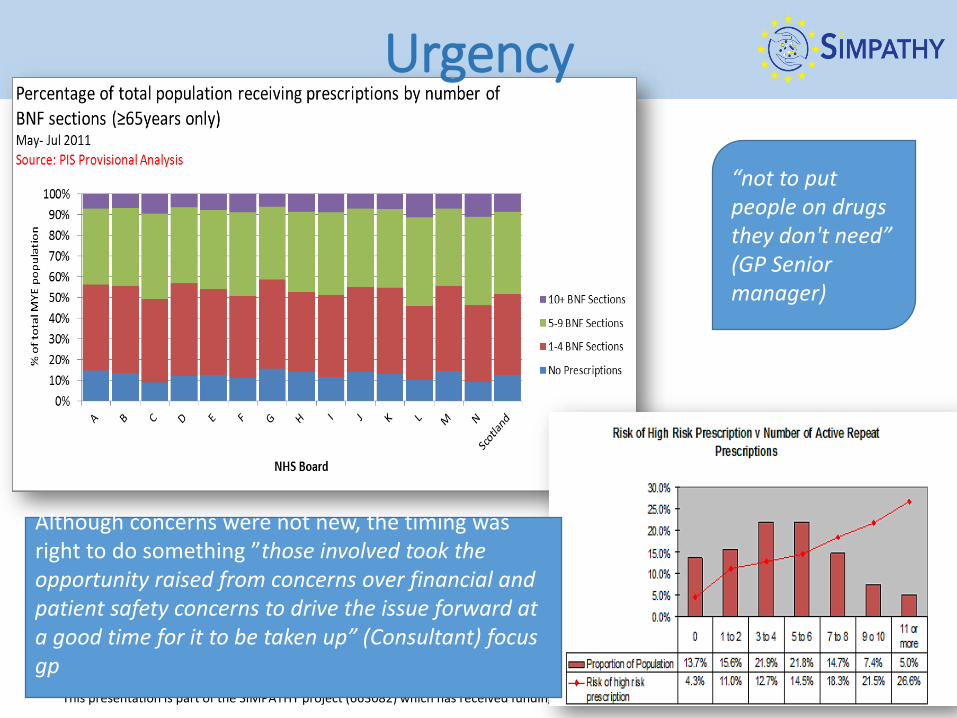
Urgency
“not to put people on drugs they don't need” (GP Senior manager)
Although concerns were not new, the timing was right to do something ”those involved took the opportunity raised from concerns over financial and patient safety concerns to drive the issue forward at a good time for it to be taken up” (Consultant) focus gp
This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Build powerful coalition: Enlist a Volunteer Army & Remove barriersPolypharmacy national Programme: guidance : consensus 7 steps
GP contract and commitment to practice based pharmacists £16.2M(Scot) + £31M in England

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Domain Steps Process
Aims 1. What matters to the patient
Review diagnoses and identify therapeutic objectives with respect to: Identify objectives of drug therapy Management of existing health problems Prevention of future health problems
Need
2. Identify essential drug therapy
Identify essential drugs (not to be stopped without specialist advice) Drugs that have essential replacement functions (e.g.
thyroxine) Drugs to prevent rapid symptomatic decline (e.g. drugs
for Parkinson’s disease, heart failure)
3. Does the patient take unnecessary drug therapy?
Identify and review the (continued) need for drugs with temporary indications with higher than usual maintenance doses with limited benefit in general for the indication they
are used for with limited benefit in the patient under review (see
Drug efficacy & applicability (NNT) table)
Effectiveness 4.
Are therapeutic objectives being achieved?
Identify the need for adding/intensifying drug therapy in order to achieve therapeutic objectives to achieve symptom control to achieve biochemical/clinical targets to prevent disease progression/exacerbation
Safety 5.
Does the patient have ADR or is at risk of ADRs? Does the patient know what to do if they’re ill?
Identify patient safety risks by checking for drug-disease interactions drug-drug interactions (see ADR table) robustness of monitoring mechanisms for high-risk
drugs drug-drug and drug-disease interactions risk of accidental overdosing
Identify adverse drug effects by checking for specific symptoms/laboratory markers (e.g.
hypokalaemia) cumulative adverse drug effects (see ADR table) drugs that may be used to treat ADRs caused by other
drugs Sick Day rule cards
Cost-effectiveness 6.
Is drug therapy cost-effective?
Identify unnecessarily costly drug therapy by
Consider more cost-effective alternatives (but balance against effectiveness, safety, convenience)
Patient centeredness 7.
Is the patient willing and able to take drug therapy as intended?
Identify risks to patient non-adherence by considering
Is the medicine in a form that the patient can take?
Is the dosing schedule convenient?
Is the patient able to take medicines as intended?
Might the patient benefit from the Chronic Medication Service (CMS)?
Is the patient’s pharmacist informed of changes to regimen?
Ensure drug therapy changes are tailored to patient preferences by
Discuss with the patient/carer/welfare proxy therapeutic objectives and treatment priorities
Decide with the patient/carer/welfare proxies what medicines have an effect of sufficient magnitude to consider continuation or discontinuation
Identify objectives-“What Matters to you?”
“Realistic medicine”

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
VISION:prescribe well:avoidharm
IMS Report “ Advancing responsible use of medicines” & WHO, World Bank Global data set across 186 countries: 4% of total avoidable costs due to polypharmacy.Total of ).3% global health expenditure could be saved = $18bn
For patients receiving 5 meds-30.1%; 47% with 10 or more in 12 months- increases with increase in no
“you need a few visionary leaders who can understand the strategic context in which they're working to come up good ideas and then you need to take it through whatever part of the system it needs to go through, the healthcare provider management group takes the decision” (Board, GP Senior manager)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Risk Stratification :Polypharmacy Guideline 2015.
Prior to the launch of the national guidance, the NHS Lothian pharmacy service was “already engaged with a number of practices in a service level agreement”“Lothian had prescribing advisors in strategic positions who could allocate a very small resource to needy practices who had prescribing medicines management, medicines optimisation issues”
Volunteer Army

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Enable by removing barriers-Practice models:
Link with anticipatory care plans
Different models tested in different boards
Barriers were removed to enable action in terms of contractual arrangements. Polypharmacy was linked with other contractual services“we've linked the polypharmacy work in people's minds, whenever possible, with anticipatory care planning and anticipatory care planning for general practice was also born in Highland and these two things happened together” (GP Senior manager)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Generate short term wins & sustain: Economic Case

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
What has been successful?
Growth in prescribing in % terms.
Items dispensed
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
2010 2011 2012 2013 2014
Scotland
England
Wales
N Ire

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Outcome Duration NNT Annualised NNT
Any Diabetesrelated end point
10 years 20 200
Diabetes related death
10 years 91 910
Microvascularcomplication
10 years 36 360
Aiming blood sugar < 6 v < 15[achieved 7% v 8 %]

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Sustain Acceleration

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)
Institutionalising change- Creating Adaptive Practice models:
GP contract link with care pathway for
Anticipatory care plans

This presentation is part of the SIMPATHY project (663082) which has received funding from the European Union’s Health Programme (2014-2020)The SIMPATHY project has received funding from the European Union’s Health Programme (2014-2020)
www.simpathy.eu
https://twitter.com/simpathyproject