scoliosis and lung function in spinal muscular atrophy
TRANSCRIPT
Eur Spine J (1995) 4:268-273 Eurgpean Spmelournal
�9 Springer-Verlag 1995
Scoliosis and lung function in spinal muscular atrophy
D. Robinson, C. S. B. Galasko, C. Delaney, J. B. Williamson, and J. L. Barrie
Department of Orthopaedic Surgery, University of Manchester, Royal Manchester Children's Hospital, Manchester, UK
Summary. The notes and radiographs of 43 patients with a confirmed diagnosis of spinal muscular atrophy were re- viewed. A significant inverse linear relationship between the severity of scoliosis and the percentage of predicted vital capacity and peak flow was found. The patients who stood had a significantly better lung function than patients who were confined to a wheelchair, and their scoliosis de- teriorated significantly more slowly. Sixteen patients un- derwent surgical spinal stabilisation, 4 with Harrington in- strumentation and 12 with segmental spinal instrumenta- tion, at an average age of 12 years and 11 months. The average curve correction achieved was 40%. The decline in lung function seen pre-operatively was not only re- versed, but a significant improvement was found at final follow-up.
Key words: Spinal muscular atrophy - Scoliosis - Lung function - Standing regimen - Harrington instrumenta- tion - Segmental spinal instrumentation
The aims of this study were to investigate the relationship between scoliosis and lung function in patients with spinal muscle atrophy (SMA), and analyse the effects of stand- ing and of spinal surgery on their progression. SMA is an autosomal recessive neuromuscular disorder. Through de- generation of the anterior horn ceils it causes weakness which is more marked proximally than distally and affects the lower limbs more than the upper limbs. It forms a con- tinuum of disease severity, although there is a single gene coding for all degrees of severity, which has been accu- rately mapped on chromosome 5 [4, 12, 16]. There are several classifications, but the one found to be the best guide to prognosis is based on the patient's maximal un- aided functional ability [6]. Three clinical subtypes have
Received: 3 January 1995 Revised: 21 April 1995 Accepted: 15 May 1995
Paper read at the ESDS meeting, Birmingham, 1994, and selected for full publication. Correspondence to: C. S. B. Galasko, Department of Orthopaedic Surgery, Clinical Sciences Building, Hope Hospital, Eccles Old Road, Salford, Manchester M6 8HD, UK
been recognised: in the severe group patients never achieve the ability to sit unsupported; in the intermediate group they do achieve the ability to sit but never to stand; in the mild group the patients achieve the ability to stand or walk independently [7].
The most serious orthopaedic problem encountered is that of scoliosis [24], which usually occurs in all but the most minimally involved [2]. Riddick et al. [22] stated that once a curve appeared, progression without treatment was almost certain.
Hardy and Curtis [13] in 1973 were the first to men- tion spinal fusion for the treatment of scoliosis in SMA, but this involved considerable risk. Post-operative respira- tory complications are common. Aprin et al. [1] reported that 10 out of 22 patients developed atelectasis and pneu- monitis, 4 requiring intubation for 5 days. There is some suggestion that spinal fusion can decrease the patient's overall function and in particular that it can result in loss of walking ability [24]. This probably occurs because some patients require trunk movement to walk.
Prolonged post-operative immobilisation can lead to disuse atrophy [9]. A lower complication rate has been re- ported in patients treated with Luque rather than Harring- ton instrumentation [3], but concern has been expressed that in patients with a potential for long-term survival, Luque instrumentation failure may occur eventually if there is inadequate spinal arthrodesis. There have been few studies of spinal surgery in SMA that have reported the effect on lung function, but those that have suggest that overall there is a continued fall in the post-operative values [1, 3, 17, 21, 22].
Scoliosis occurs relatively early in patients with SMA. Our treatment programme has been to brace children who have a curve of more than 15-20 ~ until they are old enough for surgery. We have also encouraged standing in these patients using some form of orthosis. I f it is not pos- sible to control the scoliosis, an early fusion is carried out, the youngest patient in our series being 6 years 9 months.
Patients and methods
A retrospective case-note and radiographic review was carried out on 43 patients who presented with SMA at the Royal Manchester Children's Hospital. The diagnosis was made, in all patients, on
269
neurological examination that demonstrated the typical weakness, tremors, areflexia and normal sensation [19]. The diagnosis was confirmed with EMG and muscle biopsy. The classification of each case into one of three categories was done according to the patient's greatest functional achievement without orthotic inter- vention. There were 21 boys and 22 girls, of whom 39 (91%) were found to have spinal deformity. The scoliotic curve pattern was thoracic in 17, thoraco-lumbar in 13, lumbar in 8 and double in 1. The curve was convex to the right in 18 and to the left in 20.
The disease was classified as severe in 6 patients, as interme- diate in 12 and as mild in 25. The median age when scoliosis was first noted in the "severe" patients was 1 year 6 months (range 2 months - 3 years 11 months); in the "intermediate" patients it was 2 years 1 month (range 6 months - 7 years 4 months) and in the "mild" patients it was 8 years 1 month (range 1 month - 16 years 11 months). The median angle when bracing began was 27 ~ de- grees (range 12-34 ~ in the severe group, 28 ~ (range 8-45 ~ in the intermediate group and 40 ~ (range 5-73 ~ ) in the mild group.
As part of the routine, each patient had an AP radiograph taken of the spine when they were first seen in the clinic. If the patient was able to sit or stand, an erect film was taken. Thereafter, radi- ographs were taken at 6-monthly intervals. The severity of the sco- liosis was measured from the radiographs using the Cobb method [5]. The patients' vital capacity (PFT 2 Plus Vitalograph) and peak flow (Wright peak flow meter) were also recorded on these occa- sions. Predicted normal values were based on armspan, as this is the most accurate method in scoliotic patients [14].
Patients with the mild form who were no longer independently mobile were offered a standing regimen. Those who accepted were encouraged to stand for a minimum of 2 h per day. All the patients with the intermediate form were offered a standing regimen. The progression of scoliosis and lung function were compared in each category of SMA between those patients who accepted the stand- ing regimen and those who refused. There was no difference in terms of the severity of the disease, the scoliosis or lung function in each category of SMA between those who accepted and those who refused the standing regimen.
If the patient and their family accepted surgery, the patient was admitted to hospital for respiratory and cardiac assessment. The fi- nal decision about fitness for surgery was made by the anaesthetist [18]. Three patients had surgery refused due to either poor lung function or previous complications while under general anaesthetic.
The overall relationship between scoliosis and lung function was investigated by plotting the percentage of predicted vital ca- pacity and peak flow against the Cobb angle. Thirty-nine patients had scoliosis at last follow-up and of these 33 had lung function tests with a corresponding radiograph. The number of measure- ments per patient varied from 1 to 12, taken over a maximum pe- riod of 9 years 8 months. Post-operative values were not included. The results were analysed by a linear regression analysis.
Results
There was no difference in the progression of scoliosis in patients with the mild form of SMA between those who were still independent ly mobi le and those who stood in orthoses. The scoliosis deteriorated more rapidly in those confined to a wheelchair, but the difference did not reach statistical significance.
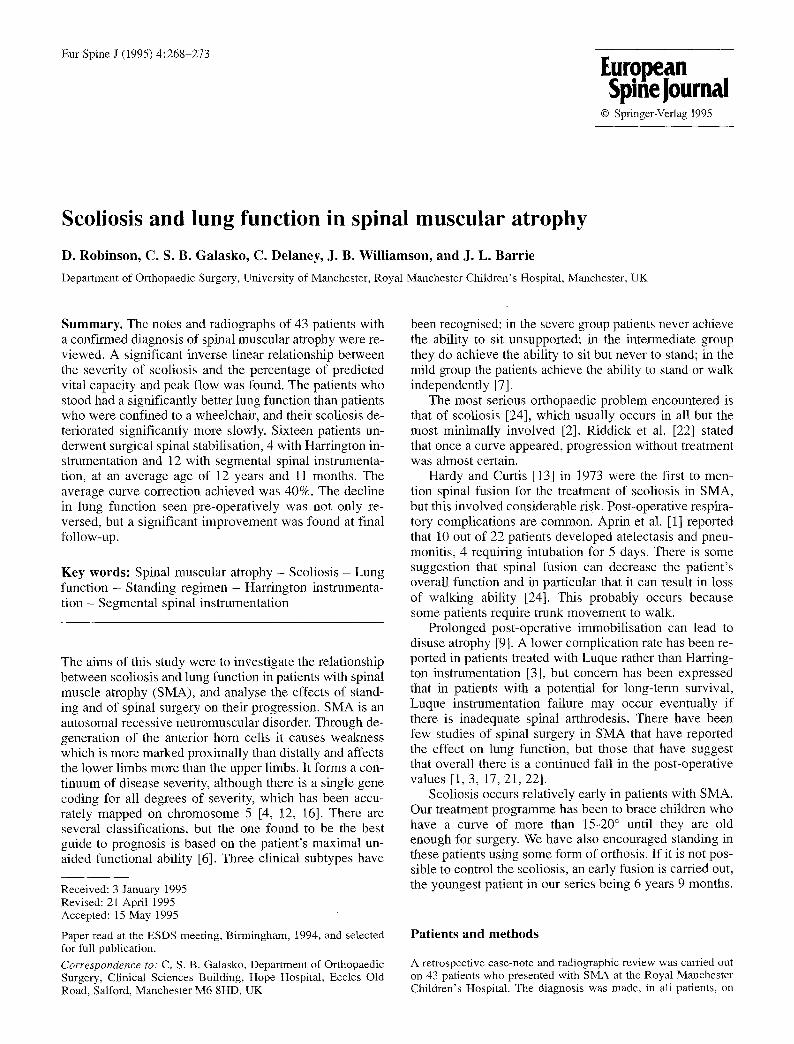
In patients with the intermediate form of SMA, the scoliosis deteriorated almost twice as fast in the patients who were whee lcha i r -bound than in those who stood (Fig. 1). This difference was statistically significant.
All patients with mi ld SMA showed an annual in- crease in vital capacity. There was no significant differ- ence between the patients who were independent ly mobi le and those who stood. The vital capacity increased at about
14.
12.
1 0 '
S c l i o s i s
i n c r e a s e / y r 8 �9
(degrees )
6 -
) M i l d I n t e r m e d i a t e
Fig. 1. The effect of standing on scoliosis (measured in degrees us- ing the Cobb method) in patients with mild and intermediate forms of spinal muscle atrophy (SMA). The figures shown are the annual increase in scoliosis in degrees per annum. �9 Mobile; [] able to stand in orthoses; [] wheelchair-bound; *P < 0.05
400 �9
V i ta l c a p a c i t y
i n c r e a s e / d e c r e a s e
p e r y r (ml)
300 ,
200 .
100 �9
O. m m
.1 oo Mi ld I n t e r m e d i a t e
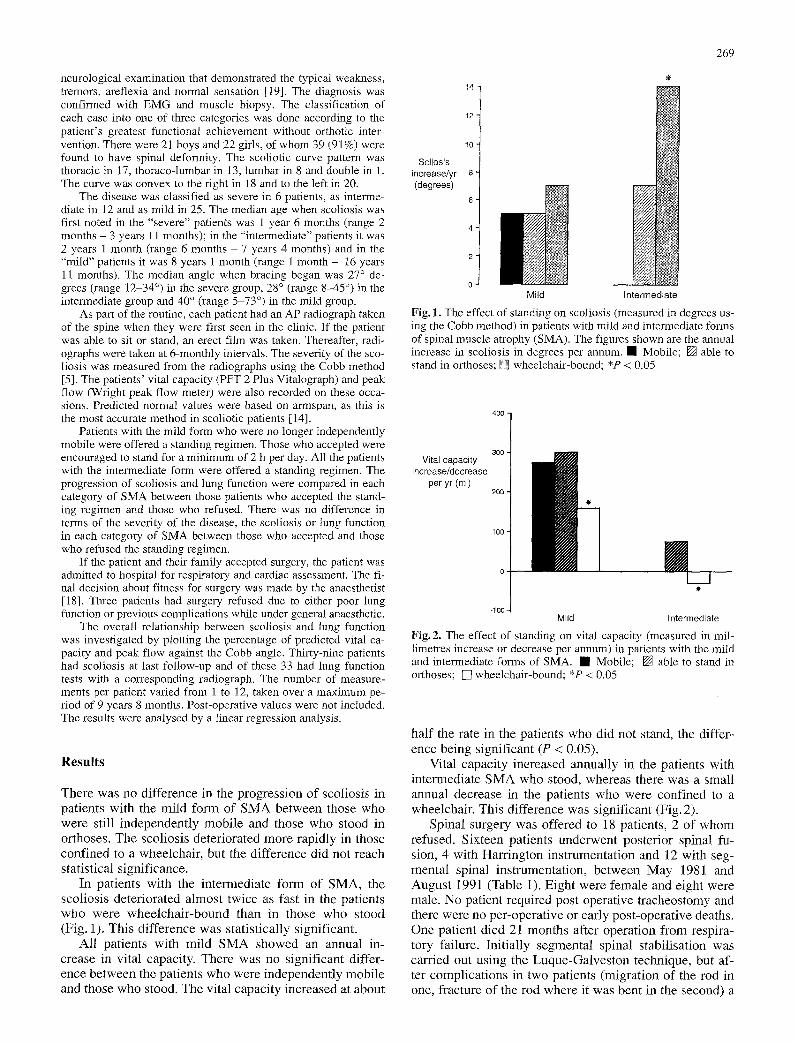
Fig. 2. The effect of standing on vital capacity (measured in mil- limetres increase or decrease per annum) in patients with the mild and intermediate forms of SMA. �9 Mobile; [] able to stand in orthoses; []wheelchair-bound; *P < 0.05
half the rate in the patients who did not stand, the differ- ence being significant (P < 0.05).
Vital capacity increased annual ly in the patients with intermediate SMA who stood, whereas there was a small annual decrease in the patients who were confined to a wheelchair. This difference was significant (Fig. 2).
Spinal surgery was offered to 18 patients, 2 of whom refused. Sixteen patients underwent posterior spinal fu- sion, 4 with Harrington instrumentat ion and 12 with seg- mental spinal instrumentat ion, between May 1981 and August 1991 (Table 1). Eight were female and eight were male. No patient required post-operative tracheostomy and there were no per-operative or early post-operative deaths. One patient died 21 months after operation from respira- tory failure. Init ial ly segmental spinal stabilisation was carried out using the Luque-Galves ton technique, but af- ter complicat ions in two patients (migration of the rod in one, fracture of the rod where it was bent in the second) a
270
Table 1. Data on patients, scoliosis and surgery
Patient Age at Type of Type of Scoliosis (~ Loss of correction (~ (in order surgery curve surgery of surgery) (years Pre- Post- Correction 1 year Final Follow-up
+ months) operative operative (%) follow-up (months)
1 12 + 7 T HRI 114 80 30 7 14 54 2 19 + 5 L HRI 96 92 4 14 16 60 3 14 + 5 L HRI 92 46 50 26 16 114 4 16 + 3 T/L SSI 98 46 53 22 30 114 5 10 + 7 T SSI 126 78 38 a _ Died 21 months
after operation 6 16 + 10 L SSI 33 7 79 23 23 54 7 19 + 9 T HRI 54 48 11 6 8 30 8 12 + 6 T/L SSI 58 44 24 12 16 72 9 12 + 8 T SSI 132 58 56 - 8 42
10 14 + 11 L SSI 80 58 28 -1 -8 54 11 10 + 2 T SSI 98 55 44 23 15 24 12 8 + 0 T SS1 84 60 29 2 2 18 13 12 + 3 L SSI 90 50 44 2 2 18 14 20 + 0 T/L SSI 60 26 57 4 - 12 15 6 + 9 T/L SSI 85 28 67 - - - 16 9 + 10 T/L SSI 93 70 25 -
T, Thoracic; L, Lumbar; T/L, Thoraco-lumbar; HRI, Harrington rod instrumentation; SSI, Segmental spinal instrumentation Data omission due to radiographs not being available for analysis as these times
single "U"-shaped rod was used [10]. The rod was t r immed to length and applied to the spine, after suitable moulding, with the closed end fixed to the sacrum. The rods were fixed from T3 or T4. Both a lumbar lordosis and a dorsal kyphosis were moulded into the rod. Some correction of the scoliosis was obtained when the patient was placed prone on the table and further correction was achieved during the wiring. A facet joint excision and fu- sion was carried out at each level. Spinal cord function was tested intra-operatively with Stagnara 's wake-up test [25] up to 1986 and thereafter with spinal cord monitoring [26]. Although these patients are weak, they have normal sensation and bladder control.
The average Cobb angle when surgery was offered was 71 ~ (range 32-112~ while the average angle when surgery was carried out was 87 ~ (range 33-126~ The av- erage age at operation was 12 years 11 months (range 6 years 9 months to 20 years). The patients were usually ad- mitted 2 days prior to surgery. Following operation, they were kept in the intensive care unit for 24 -72 h.
The median blood loss at operation was 2665 ml (range 800-5520 ml). There was no specific reason why one patient lost in excess of 5 1 blood, but this did not af- fect the patient 's post-operative progress.
The median post-operative hospital stay for patients undergoing Harrington instrumentation was 35 days (range 25-56 days), while for those with segmental spinal stabilisation it was 16 days (range 8-63 days).
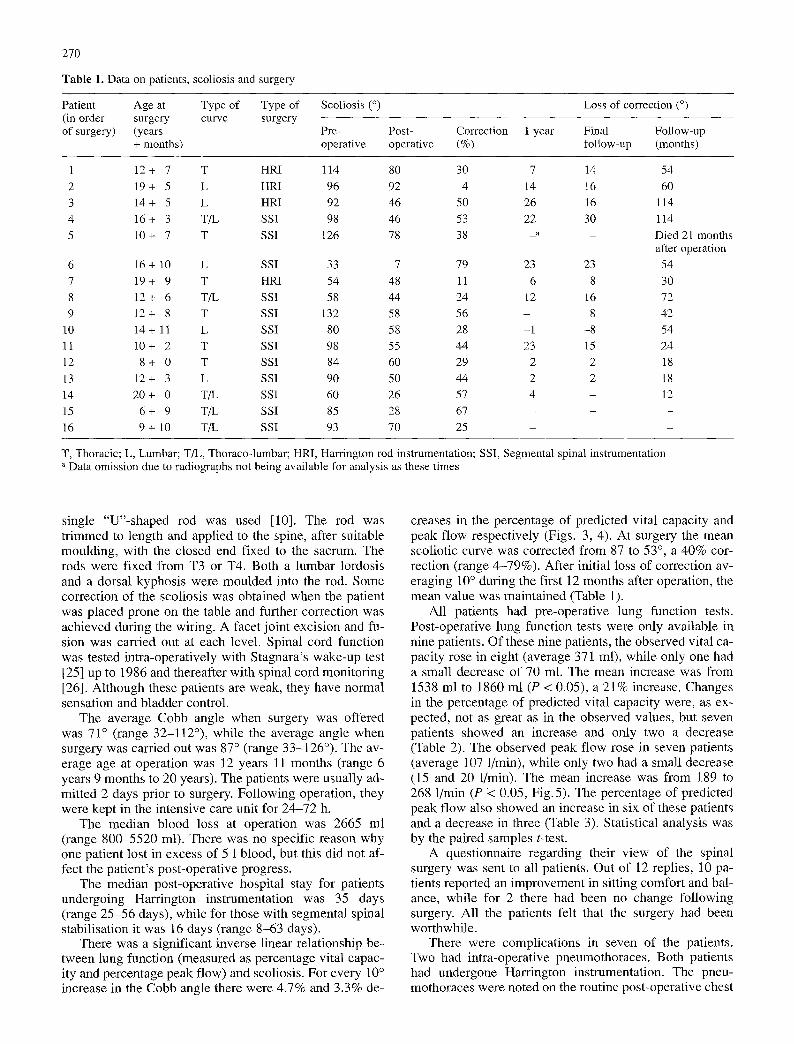
There was a significant inverse linear relationship be- tween lung function (measured as percentage vital capac- ity and percentage peak flow) and scoliosis. For every 10 ~ increase in the Cobb angle there were 4.7% and 3.3% de-
creases in the percentage of predicted vital capacity and peak flow respectively (Figs. 3, 4). At surgery the mean scoliotic curve was corrected from 87 to 53 ~ a 40% cor- rection (range 4-79%). After initial loss of correction av- eraging 10 ~ during the first 12 months after operation, the mean value was maintained (Table 1).
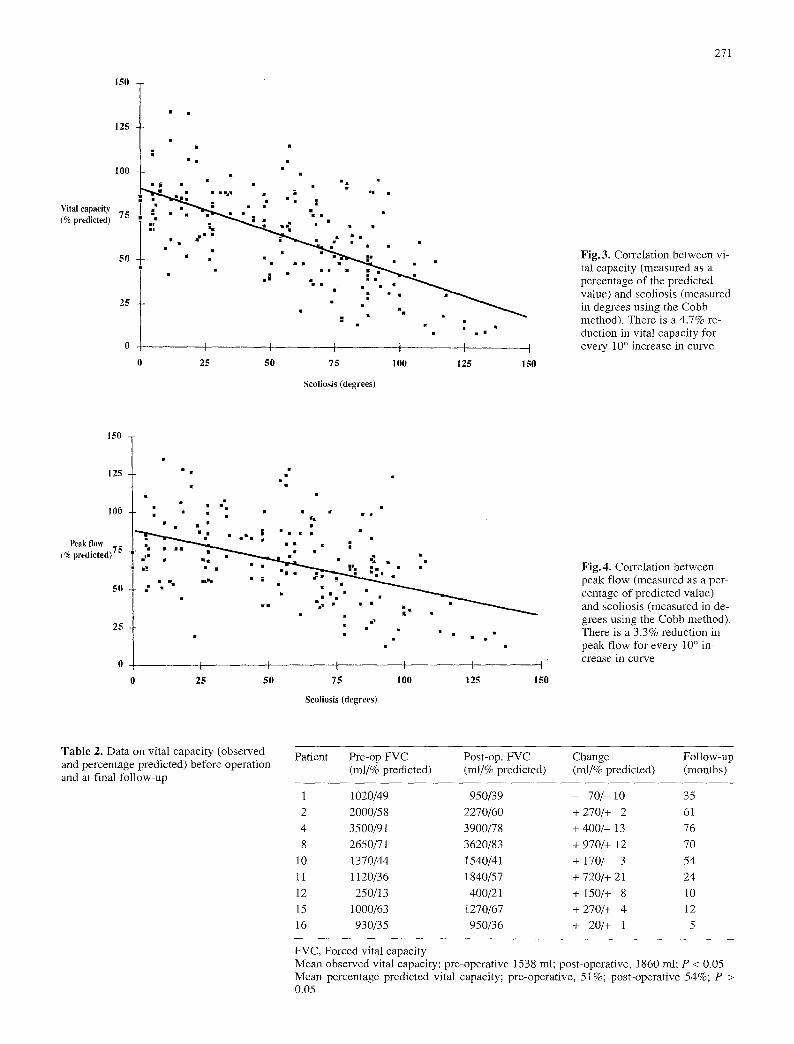
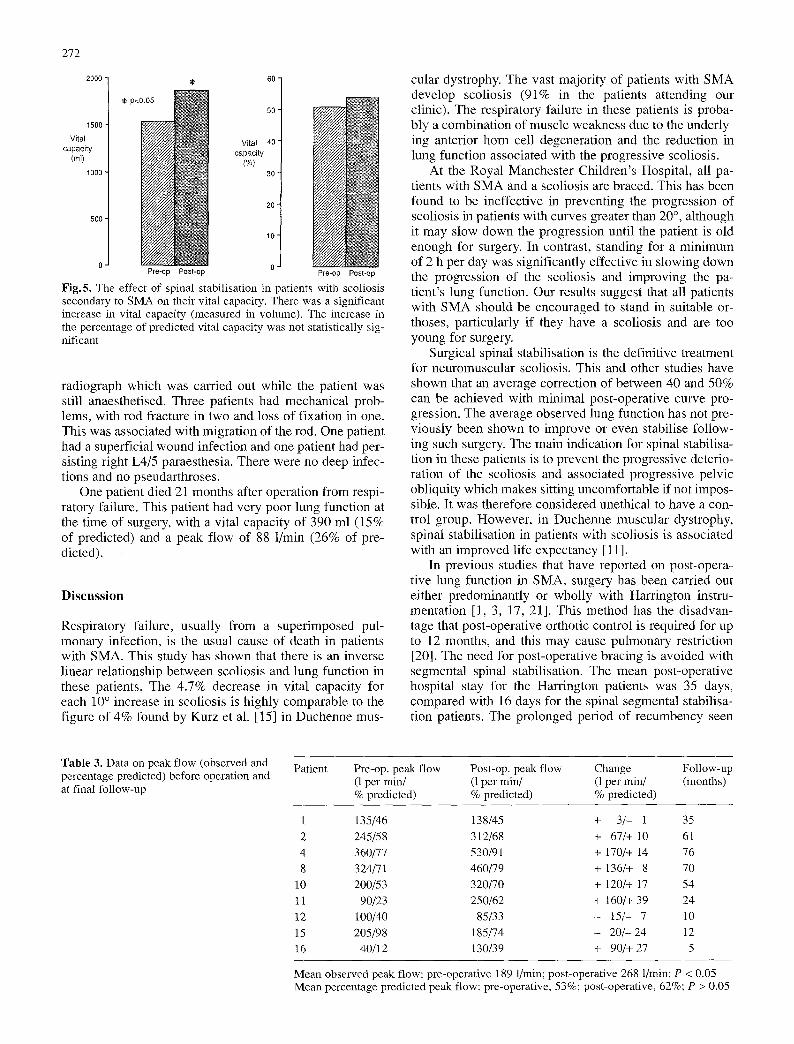
All patients had pre-operative lung function tests. Post-operative lung function tests were only available in nine patients. Of these nine patients, the observed vital ca- pacity rose in eight (average 371 ml), while only one had a small decrease of 70 ml. The mean increase was from 1538 ml to 1860 ml (P < 0.05), a 21% increase. Changes in the percentage of predicted vital capacity were, as ex- pected, not as great as in the observed values, but seven patients showed an increase and only two a decrease (Table 2). The observed peak flow rose in seven patients (average 107 1/min), while only two had a small decrease (15 and 20 1/min). The mean increase was from 189 to 268 1/min (P < 0.05, Fig.5). The percentage of predicted peak flow also showed an increase in six of these patients and a decrease in three (Table 3). Statistical analysis was by the paired samples t-test.
A questionnaire regarding their view of the spinal surgery was sent to all patients. Out of 12 replies, 10 pa- tients reported an improvement in sitting comfort and bal- ance, while for 2 there had been no change following surgery. All the patients felt that the surgery had been worthwhile.
There were complications in seven of the patients. Two had intra-operative pneumothoraces. Both patients had undergone Harrington instrumentation. The pneu- mothoraces were noted on the routine post-operative chest
150
125
I00
Vital capacity (% predicted) 75
50
25
�9 � 9 �9
u
I I | t 1 I
0 25 50 75 100 125 150
Scoliosis (degrees)
271
Fig. 3. Correlation between vi- tal capacity (measured as a percentage of the predicted value) and scoliosis (measured in degrees using the Cobb method). There is a 4.7% re- duction in vital capacity for every 10 ~ increase in curve
150
125
100
Peak flow _~; (% predicted) 7"
50
25
m
�9 �9 �9 �9 � 9
N
t l I i ~ I I
25 50 75 I00 125 150
Scoliosis (degrees)
Fig. 4. Correlation between peak flow (measured as a per- centage of predicted value) and scoliosis (measured in de- grees using the Cobb method). There is a 3.3% reduction in peak flow for every 10 ~ in- crease in curve
Table 2. Data on vital capacity (observed and percentage predicted) before operation and at final follow-up
Patient Pre-op FVC Post-op. FVC Change Follow-up (ml/% predicted) (ml/% predicted) (ml/% predicted) (months)
1 1020/49 950/39 - 70 / - 10 35
2 2000/58 2270/60 + 270/+ 2 61
4 3500/91 3900/78 + 400/ - 13 76
8 2650/71 3620/83 + 970/+ 12 70
10 1370/44 1540/41 + 170/- 3 54
11 1120/36 1840/57 + 720/+ 21 24
12 250/13 400/21 + 150/+ 8 10
15 1000/63 1270/67 + 270/+ 4 12
16 930/35 950/36 + 20/+ 1 5
FVC, Forced vital capacity Mean observed vital capacity: pre-operative 1538 ml; post-operative, 1860 ml; P < 0.05 Mean percentage predicted vital capacity; pre-operative, 51%; post-operative 54%; P > 0.05
272
2000
1500
Vital capacity
(rnl) 1000
500
p.d
60-
50-
VJtaJ 40 capacity
(%) 3 0
20"
10"
Pre-~p Post-op 0 Pre-op Post-op
Fig.5. The effect of spinal stabilisation in patients with scoliosis secondary to SMA on their vital capacity. There was a significant increase in vital capacity (measured in volume). The increase in the percentage of predicted vital capacity was not statistically sig- nificant
radiograph which was carried out while the patient was still anaesthetised. Three patients had mechanical prob- lems, with rod fracture in two and loss of fixation in one. This was associated with migration of the rod. One patient had a superficial wound infection and one patient had per- sisting right L4/5 paraesthesia. There were no deep infec- tions and no pseudarthroses.
One patient died 21 months after operation from respi- ratory failure. This patient had very poor lung function at the time of surgery, with a vital capacity of 390 ml (15% of predicted) and a peak flow of 88 1/min (26% of pre- dicted).
Discussion
Respiratory failure, usually from a superimposed pul- monary infection, is the usual cause of death in patients with SMA. This study has shown that there is an inverse linear relationship between scoliosis and lung function in these patients. The 4.7% decrease in vital capacity for each 10 ~ increase in scoliosis is highly comparable to the figure of 4% found by Kurz et al. [15] in Duchenne mus-
cular dystrophy. The vast majority of patients with SMA develop scoliosis (91% in the patients attending our clinic). The respiratory failure in these patients is proba- bly a combination of muscle weakness due to the underly- ing anterior horn cell degeneration and the reduction in lung function associated with the progressive scoliosis.
At the Royal Manchester Children's Hospital, all pa- tients with SMA and a scoliosis are braced. This has been found to be ineffective in preventing the progression of scoliosis in patients with curves greater than 20 ~ although it may slow down the progression until the patient is old enough for surgery. In contrast, standing for a minimum of 2 h per day was significantly effective in slowing down the progression of the scoliosis and improving the pa- tient's lung function. Our results suggest that all patients with SMA should be encouraged to stand in suitable or- thoses, particularly if they have a scoliosis and are too young for surgery.
Surgical spinal stabilisation is the definitive treatment for neuromuscular scoliosis. This and other studies have shown that an average correction of between 40 and 50% can be achieved with minimal post-operative curve pro- gression. The average observed lung function has not pre- viously been shown to improve or even stabilise follow- ing such surgery. The main indication for spinal stabilisa- tion in these patients is to prevent the progressive deterio- ration of the scoliosis and associated progressive pelvic obliquity which makes sitting uncomfortable if not impos- sible. It was therefore considered unethical to have a con- trol group. However, in Duchenne muscular dystrophy, spinal stabilisation in patients with scoliosis is associated with an improved life expectancy [11].
In previous studies that have reported on post-opera- tive lung function in SMA, surgery has been carried out either predominantly or wholly with Harrington instru- mentation [1, 3, 17, 21]. This method has the disadvan- tage that post-operative orthotic control is required for up to 12 months, and this may cause pulmonary restriction [20]. The need for post-operative bracing is avoided with segmental spinal stabilisation. The mean post-operative hospital stay for the Harrington patients was 35 days, compared with 16 days for the spinal segmental stabilisa- tion patients. The prolonged period of recumbency seen
Table 3. Data on peak flow (observed and percentage predicted) before operation and at final follow-up
Patient Pre-op. peak flow Post-op. peak flow Change Follow-up (1 per min/ (1 per min/ (1 per rain/ (months) % predicted) % predicted) % predicted)
1 135/46 138/45 + 3/- 1 35 2 245/58 312/68 + 67/+ 10 61 4 360/77 530/91 + 170/+ 14 76 8 324/71 460/79 + 136/+ 8 70
10 200/53 320/70 + 120/+ 17 54 11 90/23 250/62 + 160/+ 39 24 12 100/40 85/33 - 15/- 7 10 15 205/98 185/74 - 20/- 24 12 16 40/12 130/39 + 90/+ 27 5
Mean observed peak flow: pre-operative 189 1/min; post-operative 268 l/rain; P < 0.05 Mean percentage predicted peak flow: pre-operative, 53%; post-operative, 62%; P > 0.05

273
with the Harr ing ton ins t rumenta t ion may pred ispose pa- tients to many problems, inc luding respira tory infect ion and increas ing musc le a t rophy and respi ra tory musc le weakness . Pu lmonary compl ica t ions have been frequent ly repor ted in these pat ients in the ear ly pos t -opera t ive pe- r iod [1, 8, 21, 22].
The results o f our s tudy show that spinal s tabi l isat ion provides severa l benefi ts in patients with scol iosis sec- ondary to SMA. First , there is often a large reduct ion in the sever i ty o f the curve, which is usual ly maintained. The progress ive pe lv ic obliquity, which can make si t t ing un- comfor tab le i f not imposs ib le for pat ients who are largely conf ined to wheelchairs , is halted. This was conf i rmed by the v iews of the patients , in that 10 of the 12 contacted felt that there had been an improvemen t in their sit t ing com- fort. The other ma jo r benefi t shown by this s tudy was that spinal s tabi l isat ion can a l low an improvemen t in lung function, as opposed to the cont inued deter iorat ion associ- ated with progress ive scoliosis . This is par t icular ly impor- tant as most o f these pat ients eventua l ly die f rom respira- tory fai lure and it is l ikely, therefore, that the improve- ment in lung function will increase their l ife expectancy.
The surgical approach that we now adopt is to stabil ise the spine f rom T3 or T4 to the sacrum, using an open rec- tangle. The c losed end is wired to the sacrum and the open ends are t r immed to size. The rod is f ixed to both laminae at each level with sublaminar wires, and facet jo int fu- sions are carr ied out at each level , inc luding L5/S 1. We advise such surgery to whee lcha i r -bound patients aged 10 years or more whose curves are in excess o f 25 ~ , p rovid- ing they are fit enough for surgery. Younger chi ldren are encouraged to stand and their curves are braced ei ther un- til they are old enough for surgery or serial radiographs show that the curve is p rogress ing rapid ly despi te the bracing. The diff icul ty arises in pat ients who are still mo- bi le but require trunk m o v e m e n t for walking. In these pa- tients, we would only advise surgery if the curve was pro- gressive, had reached 40 ~ plus, and the pat ient and fami ly rea l ised that independent ambula t ion may be lost fo l low- ing spinal s tabi l isat ion. The extent of the fusion may need to be mod i f i ed in the mobi le group.
References
1. Aprin H, Bowen JR, MacEwen GD, Hall J (1982) Spine fusion in patients with spinal muscular atrophy. J Bone Joint Surg [Am] 64: 1179-1187
2. Benady SG (1978) Spinal muscular atrophy in childhood. A re- view of 50 cases. Dev Med Child Neurol 20:746-757
3. Brown JC, Zeller JL, Swank SM,' Furmnasa PT, Warath SL (1989) Surgical and functional results of spine fusion in spinal muscular atrophy. Spine 14:763-770
4. Brzustowicz LM, Lehner T, Castillo LH (1990) Genetic map- ping of chronic childhood-onset spinal muscular atrophy to chromosome 5q 11.2-13.3. Nature 344:540-541
5. Cobb JR (1948) Outline for the study of scoliosis, instructional course lectures. Am Acad Orthop Surg 5:261-275
6. Dubowitz V (1974) Benign infantile spinal muscular atrophies. Dev Med Child Neurol 16:672-675
7. Dubowitz V (1978) Muscle disorders in childhood. Saunders, Philadelphia
8. Evans GA, Drennan JC, Russman BS (1981) Functional classi- fication and orthopaedic management of spinal muscular atro- phy. J Bone Joint Surg [Br] 63:516-522
9. Furumasu J, Swank SM, Brown JC, Gilgoff I, Warath S, Zeller J (1989) Functional activities in spinal muscular atrophy pa- tients after spinal fusion. Spine 14 : 771-775
10. Galasko CSB, Delaney C, Morris P (1992) Spinal stabilisation in Duchenne muscular dystrophy. J Bone Joint Surg [Br] 74: 210-214
11. Galasko CSB, Williamson JB, Delaney CM (1995) Lung func- tion in Duchenne muscular dystrophy. Eur Spine J 4: 263-267
12. Gilliam TC, Brzustowicz LM, Castilla LH (1990) Genetic ho- mogeneity between acute and chronic forms of spinal muscular atrophy. Nature 345 : 823-825
13. Hardy JH, Curtis BH (1971) Neuromuscular scoliosis. J Bone Joint Surg [Am] 53 : 1021-1022
14. Hepper NGG, Black LF, Fowler WB (1965) The relationships of lung volume to height and arm span in normal subjects and in patients with spinal deformity. Am Rev Respir Dis 91:356- 362
15. Kurz TL, Mubarak SJ, Schultz P, Park SM, Leach J (1983) Correlation of scoliosis and pulmonary function in Duchenne muscular dystrophy. J Pediatr Orthop 3 : 347-353
16. Melki J, Abdelhak S, Sheth O (1990) Gene for chronic proxi- mal spinal muscular atrophies maps to chromosome 5q. Nature 344 : 767-768
17. Merlini L, Granata C, Bonfiglioli S, Marini ML, Cervellati S, Savini R (1989) Scoliosis in spinal muscular atrophy: natural history and management. Dev Med Child Neurol 31:501-508
18. Morris P, Galasko CSB (1987) Anaesthesia for spinal stabili- sation in children and adolescents with neuromuscular disease. In: Galasko CSB, Noble J (eds) Current trends in orthopaedic surgery. Manchester University Press, Manchester, pp 203- 220
19. Namba T, Aberfield DC, Grob D (1970) Chronic proximal spinal muscular atrophy. J Neurol Sci 11:401-423
20. Noble-Jamieson CM, Heckmatt JZ, Dubowitz V, Silverman M (1986) Effects of posture and spinal bracing on respiratory function in neuromuscular disease. Arch Dis Child 61:178- 181
21. Piasecki JO, Mahinpour S, Levine DB (1986) Long term fol- low-up of spinal fusion in spinal muscular atrophy. Clin Or- thop 207 : 44-54
22. Riddick MF, Winter RB, Lutter LD (1982) Spinal deformities in patients with spinal muscular atrophy. A review of 36 pa- tients. Spine 7:476-483
23. Rodillo E, Marini ML, Heckmatt JZ, Dubowitz V (1989) Sco- liosis in spinal muscular atrophy: review of 63 cases. J Child Neurol 4 : 118-123
24. Schwentker EP, Gibson DA (1976) The orthopaedic aspects of spinal muscular atrophy. J Bone Joint Surg [Am] 58 : 32-37
25. Vanzelle C, Stagnara P, Jouvinroux P (1973) Functional mon- itoring of the spinal cord during spinal surgery. Clin Orthop 93 : 173
26. Williamson JB, Galasko CSB (1992) Spinal cord monitoring during operative correction of neuromuscular scoliosis. J Bone Joint Surg [Br] 74:870-873