schulz exhibit 2
TRANSCRIPT

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 1/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 2/90
Name:----
2nd BiennialSchizophrenia Treatment:Bridging Science to Clinical Care
April 6-7, 2006
Hyatt RegencyRegency Ballroom1300 Nicollet Mall
Minneapolis, Minnesota
This Continuing Medical Education conference is presented by:
International Congress on Schizophrenia Research;
Department of PsychiatryUniversity of Minnesota;
&
Office of Continuing Medical EducationUniversity of Minnesota
The Office of Continuing Medical Education at the University of Minnesota is committed to providing
the highest quality educational programs for physicians and other health care providers. Our goal is to
improve the health of the public through provision of local, regional, national and international educational
programs and to share the excellence and innovation of the University of Minnesota Medical School. Our
educational courses are designed to promote a lifetime of outstanding professional practice.
For information on CME offerings through the University of Minnesota, contact:
Office of Continuing Medical Education
University of Minnesota
Phone: 612-626-7600 or 800-776-8636
E-mail: [email protected]
www.cme.umn.edu
CME Medical SchoolUNIVERSITY OF MINNESOTA
Continuing Medical Education

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 3/90
Abstract
PI/geNu.
1
10
14
21
29
,AG-ENDA
2 ' 1 1 1 B ien nia! S ch iZ f!Pliren ia T reatm en t: B rid gin g S den ce to C lln ica! C are
Thursda! f ' . t J p r i ( 6, .2006
7:00 a.m. Registration and Continental Breakfast
8:15 Introduction
S . C ha rle s S ch ulz a nd C aro l A . T amm in ga
CAnE & CAFE: Treatment Implications from Multicentered Trials
Chair: Stephen Olson
/1-,\( 8:30) Do CATIE Results Impact Pharmacologic\_,_,,~'
Treatment of Schizophrenia? .
9:15 The First Steps - CAFE Results .
10:00 Break
10:30 What Does All This Mean? ..
11:15 Panel Discussion
12:00 p.m. Lunch
Schizophrenia I Bipolar Continuum
Chair: Carol A. Tamminga
1:30 Human Brain Imaging: Clinical Uses in Psychiatry ..
2:15 Are There Overlapping Genes and Endophenotypes? ..
3:00 Break
3:30 Treatment Implications Across the Diagnostic Continuum:
The Role of Antlpsychotics ..
4:15 Panel Discussion
5 : 0 0 Adjourn
-1-
John G . Csernansky
S te ph en CO ls on
Peter F . Buckley
C aro l A . T amm in ga
Irving l Gottesma.n
a nd D an ie l R . H an so n
Ph ilip G . J anic ak

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 4/90
Page 2 of 2
. - A b s t r a c tP ag e N o.
38
43
49
AJENDA, con t .
2 1 1 1 iB ien nia! S ch izo yliren ia T rea tm en t: B titfgin g S den c« to C lln icaf C a re
Frir!a! f l L j J r i f T, 20Q6
7:30 a .m. Registration and Continental Breakfast
Early Stages of Schizophrenia: The Prodrome and First Episode
Chair: Tonya White
8:30 The Biological Underpinning of First Episode Schizophrenia Robert B. Zipursky
9:15 Research in Childhood and Adolescent Onset Psychosis... Tonya White
10:00 Break
10:30 Antipsychotics in Teens .,................................................. S. Charles Schulz
11: 15 Panel Discussion
12:00 Course Adjourns
T lian f !fo ufir atten din g tliis co urse. W e li'!J 'e it wa s e du ca tio n af a nd i'! fo n na tiv e.
_TL

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 5/90
COURSEFKULTY
S cliiz oy lir en ia T r ea tm e n t: B r id g in g Sdenc« to C /ln ic a! C a re
Peter F. Buckley, MD, C ha irm an an d P ro fe sso r, D ep artm ent o f P sych ia try a nd H ea lth B eh avio r,
M e dic al C olle ge o f G eo rg ia , G eo rg ia
John G. Csernansky, MD, G re go ry B . C ou ch P ro fe ss or o f P sy ch ia try , Wa sh in gto n U niv ers ity S ch oo l o f M e dic in e,
Missouri
Irving I. Gottesman, PhD, Hon FRCPsych,B ern ste in P ro fe ss or in A du lt P sy ch ia try , S en io r F ello w in P sy ch olo gy ,
U niv ers ity o f M in ne so ta Me dic al S ch oo l, M in ne so ta
Daniel R. Hanson, MD, PhD, Ass is ta nt P ro fe ss or , V et er an s A ffa ir s Medic al Ce nt er , M in ne ap olis , M in ne so ta
Philip G. Janicak, MD, P ro fe ss or o f P sy ch ia tr y, Ru sh Un iv er sity Medic al Ce nt er ; Medic al D ir ec to r, P sy ch ia tr y C lin ic al
Resea rch Cen te r, I ll in o is
Stephen C. Olson, MD, D ire cto r o f S ch iz op hre nia P ro gram a nd A ss oc ia te P ro fe ss or o f P sy ch ia try , University of
M in ne so ta ; A tte nd in g P sy ch ia tris t, U niv ers ity o f M in ne so ta Me dic al C en te r, M in ne so ta
S. Charles Schulz, MD, P ro fe ss or a nd H ea d, D ep artm en t o f P sy ch ia try , U niv ers ity o f M in ne so ta Me dic al S ch oo l,
Minnesota
Carol A. Tamminga, MD, P ro fe ss or o f P sy ch ia try , U niv ers ity o f T ex as , S ou th we ste rn Me dic al C en te r, T ex as
Tonya White, MDj A ss is ta nt P ro fe ss or o f P sy ch ia try , U niv ers ity o f M in ne so ta Me dic al S ch oo l, M in ne so ta
Robert B. Zipursky, MD, FRCP(C), P ro fe ss or a nd Tap sc ott C h air in S ch iz op hr en ia S tu die s; V ic e-Ch air , R e se ar ch ,
D ep artm e nt o f P sy ch ia try , U niv ers ity o f T oro nto ; C lin ic al D ire cto r, S ch iz op hre nia P ro gram , C en tre fo r A dd ic tio n a nd
M ental H ea lth , T oron to , O nta rio, C an ada

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 6/90
EDUCAT IONAL OBJECI'lVES
The overall goal of the Second Schizophrenia Treatment: Bridging Science to Clinical Care is to review and discuss
psychopharmacology, the schizophrenia/bipolar continuum, and the prodrome and early stages of schizophrenia.
Fo{ fow in !J t li is c 0' !l cr cnce, jJ ar ti cj pan ts s li ou fr l b e a 6 f e to :
• Analyze and discuss the recent multicentered trials reporting comparisons of atypical antipsychotic medications in
patients with schizophrenia who have had the illness for some time (CATIE) and those at the outset of the illness
(CAFE).
• Describe the latest studies that have explored the relationship of schizophrenia to bipolar disorder - from a vantage
point of the underlying biology to the new pharmacological options for treatment.
• Identify the recent advances in the study of first episode schizophrenia and its prodrome. Attention will focus on
assessment and intervention.
CREDIT STATEMENTS
American Medical Association/PRA
The University of Minnesota designates this educational activity for a maximum of 9.0 AMA PRA Category 1 Credits™.
Physicians should only claim credit commensurate with the extent of their participation in the activity.
The University of Minnesota is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide
continuinq medical education for physicians.
Minnesota Board of Psychology
This activity has been approved by the Minnesota Board of Psychology (Board Log #0604-7520) for 4/6=7; 4/7=3;
Total 10 continuing education hours.
Minnesota Board of Social Work
This activity has been reviewed and is acceptable for up to 9.0 prescribed credits by the Minnesota Board of Social Work.
Minnesota Board of Nursing
This activity has been designed to meet the Minnesota Board of Nursing continuinq education requirements. However, the nurse
is responsible for determining whether this activity meets the requirements for acceptable continuing education.
If you intend to claim fewer than the maximum number of hours for this activity,
please sign your name and number of hours on the sheet at the registration desk before you leave.
-IV-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 7/90
F .A C lJ LT Y ADDENDUM
CO'!ftlct ifIn te r e st I '! f onna tion
T he Univ ers ity o f M in ne so ta O ffic e o f C on tin uin g Me dic al E du ca tio n h as a c on flic t o f in te re st p olic y th at re qu ire s c ou rs e
fa cu lty to d is clo se w he th er o r n ot th ey h av e fin an cia l in te re sts o r a ffilia tio ns w ith o rg an iz atio ns w ith ad ire ct a nd s ub sta ntia l in te re st in th e s ub je ct ma tte r o f th eir p re senta tio ns .
T he fo llo win g in fo rm atio n w as re ce iv ed from c ou rs e fa cu lty fo r
Schizophrenia Treatment: Bridging Science to Clinical Care ,
It is n ot a ss um ed th at th es e fin an cia l in te re sts o r a ffilia tio ns w ill h av e a n a dv ers e im pa ct o n fa cu lty p re se nta tio ns .T he y s im ply a re n ote d h ere to fu lly in fo rm c ou rs e p artic ip an ts .
Peter F. Buckley, MD: Consul tant : Abb ott, A lamo Pha rm ac eu tic als , A stra Ze ne ca , B ris to l-M ye rs S qu ib b, E li L illy ,
J an ss en P ha rm ac eu tic a, M e rc k, P fiz er; G ra nt/R e se arc h S up po rt (P rin cip al In ve stig ato r o r w o rk in g d ire ctly fo r
c ompsny /c ompeny's a gen t): Astr aZ eneca, B ris to l-Myer s Squib b, E li L illy , J an ss en Pharmaceutic a, P fiz er , S o lv ay ;
Honorar ia : Abb ott, A lamo Pha rm ac eu tic als , A stra Ze ne ca , B ris to l-M ye rs S qu ib b, E li L illy , J an ss en P ha rm ac eu tic a,
Pfizer
John G. Csernansky, MD: Consul tant : El i L il ly , Sanofi -Aven ti s; Sp ea ke rs B ure au : Janssen , B r is to l-Mye rs Squ ibb ;G ra nt/R e se arc h S up po rt (P rin cip al In ve stig ato r o r w ork in g d ire ctly fo r c omp en y/c omp en y's a ge nt): Pfizer;Honorar ia : Janssen, Bristo l-Myers Squibb .
Irving I. Gottesman, PhD, Hon FRCPsych: in dic ate d no fin an cia l in te re sts o r a ffilia tio ns
Daniel R . Hanson, MD, PhD: in dic ate d no fin an cia l in te re sts o r a ffilia tio ns
Philip G. Janicak, MD: Consul tant : B ris to l-Mye rs Squib b, J an ss en , P fiz er , S h ire ; Sp ea ke rs B ure au : Abbott,
B ris to l-Myers Squib b, A str aZ eneca, J an ss en , P fiz er , S h ir e; G ra nt/R e se arc h S up po rt (P rin cip al In ve stig ato r o r w ork in g
d ire ctly fo r c omp an y/c omp an y's a ge nt): B ris to l-Myer s Squib b, A str aZ eneca, So lv ay , J an ss en , Neuro ne tic s;
Honorar ia : A bb ott, B ris tol-M ye rs S qu ib b, A stra Ze ne ca , Ja ns se n, P fiz er, S hire . I d o in te nd to d isc us s o ff
la be l/in ve stig ativ e u se (s ) o f th e fo llo win g c ommerc ia l p ro du ct(s )/d ev ic e(s ): A ntip sy ch otic s fo r m oo d d is ord ers ;
a ntic onv ulsa nts a nd lith iu m fo r p sy ch otic d iso rd ers ; d evice -b ase d th era pie s fo r m oo d a nd p sy ch otic d is ord ers .
Stephen C. Olson, MD: Consul tant : As traZene ca , B ris to l-Myer s Squib b, P fiz er ; Sp ea ke rs B ure au : El i L i ll y,
B ris to l-Myers Squib b, J an ss en ; G ra nt/R e se arc h S up po rt (P rin cip al In ve stig ato r o r w o rk in g d ire ctly fo r
c omp sn y/c orn pe ny s a ge nt): A straZeneca, E li L illy, S olvay, M erck, P fizer. I do intend to discuss off
la be l/in ve stig ative u se (s) o f th e fo llo win g comm ercia l p ro du ct(s)/d evic e(s): T re atm en t o f p sy ch osis p ro drome w ith
ant i psychot ics.
S. Charles Schulz, MD: Consul tant : El i L il ly , As traZeneca ; Speake r's Bu reau: El i L i ll y, As traZeneca ;
G ra nt/R e se arc h S up po rt (P rin C ip al In ve stig ato r o r w o rk in g d ire ctly fo r c omp en y/c omp sn y's a ge nt): Abbo tt, E li L illy ;
Honorar ia : A stra Ze ne ca . I d o in te nd to d is cu ss o ff-la be l/in ve stig ative u se (s) o f th e fo llo win g c omme rcia l
p ro du ct(s )/d ev ic e(s ): o la nz ap en e, ris pe rid on e, q ue tia pin e, z ip ra sid on e, a rip ira zo le in te en ag ers .
Carol A. Tamminga, MD: Consul tant : A ve ra (d ru g d eve lo pm en t); N eu ro ge n (d ru g d eve lo pm en t); A ca dia (d ru gd eve lo pm en t); In tra ce llu la r T he ra pie s (d ru g d eve lo pm en t); N up ath e (d ru g d ev elo pm en t); P atte rso n, B elk na p,
Webb & T yle r (fo r Jo hn so n & Johnson on a legal case); O rganon (ad hoc consultant); Abbott (ad hoc
consultant); Spe ak ers B ure au : AstraZeneca; G ra nt/R e se arc h S up po rt (P rin cip al In ve stig ato r o r w ork in g d ire ctly fo r
c ompsn y/c ompeny's a gen t): Natio na l In stitu te o f M e nta l H ea lth (N IMH ), S ta nle y Me dic al R es ea rc h In stitu te ;
Honorar ia : Univ ers ity o f C olo ra do Me dic al S ch oo l, U niv ers ity o f A rk an sa s fo r M e dic al SC ie nc es , U niv ers ity o f T ex as
M ed ic al B ra nch , U niv ers ity o f P en nsy lva nia S ch ool o f M ed ic in e, In stitute o f L ivin g/H artfo rd H osp ital, B eth Isra el
D ea co ne ss Me dic al C en te r/H arv ard , L un db ec k USA , In c., W rig ht S ta te U niv ers ity , Y ale U niv ers ity , C orn ell U niv ers ity ,
J ou rn al o f C lin ic al P s yc hia tr y; Fu ll -t ime /par t- time Emp loyee : Americ an J ou rn al o f P sy ch ia try
Tonya White, MD: in dic ate d no fin an cia l in te re sts o r a ffilia tio ns
Robert B. Zipursky, MD, FRCP(C): Honorar ia : El i L i ll y
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 8/90
KKNOWLEDGMENT
S tg;yo rt Jo r tlie zuiBienniai S cfriz oy fire nia T rea tme nt c o'! ier en ce
has 6 een_p roPitfedftom tliifo {! ow in !f c om j Ja nie s:
. . Gold Level
AstraZeneca
Br is to l-Mye rs Squ ibb
E li L illy a nd C ompa ny
Janssen Pha rmaceu tica
Exhibitor Level ' .
E li L illy a nd C ompa ny
Forest Pharmaceutica ls
We g ra te fu lly a ck nowle dg e th eir s up po rt
S eve ral of th e compa nies ha ve e ducatio na l d isp la ys at this con fere nce w hich a tte nd ee s m ay visit
to le arn m ore ab ou t p rod uct lin es or info rm ation rela ted to S ch izop hre nia T re atm ent.
-VI-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 9/90
Do CATIE Results ImpactPharmacologic Treatment of
Schizophrenia?
John G. Csernansky, M.D.
Washington University School of Medicine
t ? - : CATIE
CATIE Trial Organization
Sponsor:National Institute of Mental Health
Contract Organization:University of North Carolina
Collaborating Universities:Duke University. Yale University. Columbia University
Contract Research Organization:Quintiles Incorporated
Sites:
57 schizophrenia trial sites
I~ (;A'l'TE
CATIE Schizophrenia Trial DesignPhaso1- Phase2 Phase3
DoubI~Ind. nadOI'll
tna,,"-"tnslgnment.
o t.A.NZ.APlNE
PartlclpantswhodlaeontllWt P.tir~pc1t1·Whod~
PM"'I<t!.2.2H.Ilthft'ttnI ~.2m22it0tl.td~c :laupiM or thezlp ,..tI daM ~I ~"g ~~tbel
fVldomlutJon~thwly1i .~';;=~~ E H A z m EDECAHOATE
oQ1.AHZAP~E
. .~~
QUE'TlAPINE
RtsPERlOONE
ZJPRAS ICOHE
dZlPRASJOOHS
~ OlNaAPJHE.QUETlAP INE or
ruSl 'ERlDOHE
o fUSPEfUDONE
PERPHENAZJNE
"1"IWG lA:~withTt)rN"'211100notgotr.mdortUod'loporpllon;u:ine:pI'Ia$&tB:p;utir;;ip.3nl3wMJd
patphona:rino'rilbe~ndon'i;tod'lo;matypical(~.QI.IfIIi;1pine,Of~lbafon:IoligibililylO'~2.
ATI E Stroup TS et a t Sch izophr Buf l .2003;29:15-31
-1-
Primary Questions Addressed
by CATIE Schizophrenia Trial
• How do the second generation anti psychotics
compare with a representat ive f irst generat ion
antipsychotic?
What is the comparative effectiveness of the
second generat ion antipsychotic drugs?
• Are the second generation antipsychotics cost·,
effective?
f): CATIE S tro up TS e t at Schizophr Bull. 2003;29:15-31.
CATIE Schizophrenia Trial: Overview
Participants
1460 people with schizophrenia
• Trial duration
Subjects participate for 18 months
• Design
Pragmatic trial that is a hybrid of efficacy
and effect iveness trial designs
t ? - : CATIF. s tro up TS e t e t Sch izophr Buf l .2003;29:15·31.
CATIE Phase 1:
Double-Blinded and Randomized
Olanzapina7.5-30 mgJday
Perphenazine8 -3 2 mg Jd ay
QueUapine201}-S00 mgJday
Risperidone1.5-6 mgJday
Ziprasidone
'P- . -",-on-s-w-;th-TO-n-o-I-as-s;-gn-.-d-IO-P-.rp-C-h.-naz-;n- ' . '4 0- 1 60 mg /d ay '
~Z lp ra s id one added a f te r 40% sample en ro l le d
TIE Str oup TS et aI Sch izophr Bu l / ..2003;29;15-31

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 10/90
Primary Outcome Measure:
All-Cause Treatment Discontinuation
Efficacy Tolerability
~All-Cause
Discontinuation
~Clinician Input Patient Input
-7:.CATIE
Primary Treatment Comparisons
Primary Phase 1 Treatment Comparisons
Secon@ySIOfl2B
Eac h ,&JypiQIvs.. Po~HodlborvMultiple~MfUS\I\'IQni
" " ' ~ I
Power for Pairwise Comparisons
of Discontinuation Rate
• 85% power to identify a 12% difference betweentwo atypicals (olanzapine, quetiapine, risperidone)
• 76% power to identify a 12% difference between
perphenazine and an atypical (olanzapine,quetiapine, risperidone)
• 58% power to identify a 12% difference betweenziprasidone and another antipsychotic medication
• Power is based on actual count of 1460randomized patients
l ? : : f ~ATIE 11
-2-
Hypotheses for Primary Outcome:
All-cause Discontinuation1. There are overall differences among antipsychoticmedications (olanzapine, quetiapine, rispendone,and perphenazine)
2a. There are differences between second generationantipsychotic medications (olanzapine, quetiapine,and risperidone)
2b. There are differences between the first generationantipsychotic (perphenazine) and secondgeneration antipsychotic medications (olanzapine,quetiapine, and risperidone)
3. There are differences between ziprasidone andthe other antipsychotic medications (olanzapine,quetiapine, risperidone, and perphenazine)
-7:CATIE
Primary Treatment Comparisons(Ziprasidone is excluded from all primary comparisons)
1. Overall treatment differences in Phase 1?
Inc luding perphenaz ine, exc luding TD pat ients
If yes (pSO.()5), proceed t() 2I \. and28: .
2a.Overali atypical differences in Phase 1/1A?
Exc luding perphenaz ine, inc luding TD pat ients
I f yes (p:sD.05), proceed to pairwise atypica l comparisons
3 comparisons, each eva luated at p :sD..05
2b.Pairwise atypical vs perphenazine differences in Phase 1?
Excluding TD patients
3 Pairwise comparisons Hochberg Adjus tment: smalles t p-vaiueeva luated at 0 .0513=0 ..0167
-7 :CATIE
CATIE Schizophrenia Trial:
Phase I Results
1 7 - : CATIE Uebe rma n JA e t at. NElM. 2005;353:'209-1223.
10

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 11/90
Demographic & Clinical Characteristics
Assessment I n = ; : . ~ 1DomoaraohicsA e mean SO 40.6 11.1
Gender1080174%Male
Race
0 While 874 (60%)
0 Black IAf r ican-Amer ican 513 (35%)
0 A ll o t he r ra ce QfOUPS 7'{5%
Soan ish /Hispan ic! La t ino e thn ic itv 17012%
Education (veats 12. 1 2 .3
Marital Status
0 Married 167 (11%)
0 Previousty Married 42529%)
0 Never Married 86~59%
Unemp lo e d 1217 85%
Exacerbat ion InPast 3 Mon lhs 402 2B%
PANSS Tot al S co re 3 0· 21 0 75. 7 1 7. 6
C finiclan Rated CGI Sever it y Score ( 1~7) 40 (O.9)CG- s o f 4 = • moderateJ ~r
Phase I Randomization and TreatmentOLZ DUET RISP PER" ZPR p;.vaJue
""336 n=337 0=341 ""'-'261 n=185
jotent-to-ueat patients 330 3 2 . 333 257 183
Average modal dose (mg) 20.1 543.' 3.s 20.B 112.8
Patients teaching malilTllll dose '''' ,,% 40% '0% 48% <0.001
Time to Discontinuation for Any Reason
OvenlI~·O.OO4'
0.'
0 .e -
o.
01P<O.OOlloro£ilnmpino V$ quatlapine
P:::O.0Q2ror~vs~
-Q.,dll","" -ZlF1olido'". . . . .-ct.
1 ~ 1 . " " . . . . ZPR
tnool:SO) t"-nl, ,. . . '" (n-tll)
21°1&,('1'.) 2&.l(!2%1 2~(74'!fo1 tll2{~"L1 I . c S I 7 1M i o )
01P.:,~.5) 1
., 5. ' as16.9,1211 1 '.0 ,6 .1 1 I • .5. 6.3 1 p.1 .S, .,
. . g : ~ t . J e rs'"
0."0.002' 0.021 O.02e
?c:CATIE
Demographic & Clinical Characteristics
Psvch ia tl ic H is to rv
Age of First Treatment for Any Behavioral or 240 (B.9)
Emotional Problem
Basel ine Ant ipsv chot ic Med ic at ions
O lanzap lne Alane . 322 (22'(0)
Que tiap ine A lone 95 (7'(0)
Risperidone Alone 275 (19%)
Combinations with 0,0, or R 125 (9'(0)
A ll O th er s ( no l O,a,R) 229 (16%)
None 414 28%,
B asenne Med ical D iagnoses
Diabetes Type I o r " 154 11%
I jy p~ rl i idemia 204 14%
Hvoertension 289 20%
Obese 8MI >=30 611 42%
13 14
Overall Rates of Discontinuation by
Reason in ITT Population
(n=1432)
Reason for'Discontinuation n %
All-cause 1061 74.1
Lack of eff icacy 340 23.7
tntolerablnty 213 14.9
Patient's Decision 428 29.9
(No te : admin is tr at iv e is induded in a ll -c ause , bul no! in any o f the o ther categor ies)
ATIE15 16
Time to Discontinuation for Lack of Efficacy
!. ~ o.. .Gr.)D~"'O.ool '' - - _i
0.& -ce-
-.j
~ 0.'a
.i0.'
J P<O.OOllar(l~V5Q\IC\i;lpine.~andpe~
0 ~. .1, 15 .r~lo~forUadtofErr~!mo)
-OtiIn1:l~ . . . . . . . . . Dpr.dcf<1".
. " '. . . . . . . . Rbp"1dono.
ou: QUIIT RJSp PER ZPR
(0-130, !notl2:9) (n"3ll1 ,='" In·,11l1
Ois<::ominuad .a { 15%J 92f2S"4) ; , ( 27%) 65(Z5%) «f2 .%)
1K;pbn-t.4eief25Ih'%UIe{1TOS 6.0 '.0 • . . 6•I I I S ' . 4 C l J 118 .0 ,-1 , . , 5 .11 .0) foI·4,9.0I '4.5,9.1\ f J.2.f2.11
tHa:.o!rdr.l tb:s l~ - 0.4' 0 .. 0.47 0.59<O.(XW .. 0.001' <0.001' 0.026
~ CATIE 1.17
-3-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 12/90
Time to Discontinuation Owing to
!
, -Patient Decision
"-_Ovot; ; lfp-¥i:It..oe:: ;O.O:W
~ 0.'
f~.
E 0.'
!0.'. .• 0>
}0 3 '. 9 2 , I,
TIlT1I:!IOOi$.CO!1bnl).llho!\o..-ngIOPalionrsO&m.ion{rro)
-.,...,.. . . . . . _ . Q ! .I I It b pi . .. . _ . D _,- Rl'~M
OLZ OUEr IUSP PE R ZPR(nIKlJO) (n-l29l ,,,,,W) (n·:lS1) (n.1!l)
Oiso;l:nIitwed 78f2_".) 109(33%) 101130%) n<""" 6J{3A%)
I Kapbn-Mltior 2 . 5 1 t 1 %tile (rRJs) '".,"
.. ,3.'
( 95%cq [ B . O . 1 7 · 1 t J Il.l,7.(J] (l.1,8.61 (H.B.II 1 3 . . 0 . 6 . 1 1
I Ha:I:: lIrd~Iic)$'orOtal1t3p1ne - 0.56 0.ti7 or n 0.63<0.001' 0.008' 0.036 0.018
~ rA'l'IF. 19
CATIESchi:z:ophrenia Trial:
Phase II Results
CATIE Phase II: Treatment
Comparisons
23
- 4 -
PANSS Total Score
Interaction of t im e • treatment inditates s ign if i cant var i at i on in t re at me n t e R ee ls o ve r l im e
h n pr ov em e ru w a s Inftiany g r eal e sl w i th o i an z api n e but i ts a d va n ta g e d im in is ha d a v er t ime.
The number 01 p a ti en ts d e cl in e s o ve r a s se ss m en t l im e s. L ea s t - sc u ar e m e en e st im a te s a re f ro m a
rn i xet i model . which assumes t ha t data a re m is si ng a t r a nd om . v et oe s a t t at er l im e p oi nt s a re based on
the cuservec data f or c :o n ti rw in g p a ti en ts a s w e ll a s e st im a te d data f o r d i s c or l li n ued pa ti e nt s
~'CATIE
CATIE Phase II: Preference Pathways(for people who discontinue Phase 1)
Olanzapine, Quetiapine, orRisperidone-one of these
not taken in Phase 1
I Randomization withinchosen pathways
ATIE S lr O Up T S et at. Schizophr BUll. 2003;29:15-31.
CATIE Phase II: Treatment Comparisons
Same Strategy for liT and liE
1.0verall treatment difference?
3 d f. test
If yes (pgj.OS). proceed to 2A and 26:
za, Pairwise test treatment vs. atypical (0. a. R)differences?
3 Pai rw ise cornpar tsons Hochberg Adjus tmen t sma ll es t p -value
evaluated at 0.OS13=0..0167
2b. Atypical differences (o.o, R)?
2d. f. t es t
I f yes (pgj.05). proceed to pai rwise atypical comparisons
3 comparisons, each evaluated at p~105
~ CATIE
20
22
24

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 13/90
Phase liT: Baseline DemographicsTotal
(n=444)
Demographics
Ace at chase 2 baseline. mean SD 40.8 11.0
Gender
Male 308 (69%)
Race
o While 291 (66%)
0 Black IAfrican-American 132(30%)
o All a lher race orouos 20(4%)
SaanishlHisoanici Latino elhnicilv 56 13%
Educalion (veers 12.1 2 .3
ATIE
Time to Discontinuation for Any Reason
08'. . . . . . ,.
Overall P-value=O 004·
0,6
04
-02
oL-----~----~----~----~--o 4 6 12 16
TIme 1. 0 Q is c: on ti nu a Uo n f or A n y C a us e ( m o)
--OIBr1Z3plne
Oueliapine
Risperidone
• Z ipras1dOl " l! !
~ CATIE
Time to Discontinuation for Lack of Efficacy
tt
"--, Ovor . lJIP . . . . .akJu"G.D44·
ae ..."-~----
I
"-.
OA . ~"" " .... -
'2
.. , . . tz
" "T""",m~bLado.ofElraocy!.,..,)
-""",""", - -Ouetbp;,.,. , . . . .. . . .OLZ RISP QUET ZP R
n=fiG n=69 n=<;3 n=135
tsconunued 1 3';' 826% 35% 42 1%
i(aplan-MeJer 25%ilo 9.1 8.3 4.2
"~1hn(3.5.-J (29.1301 (3.0.5.9) 12.4.5.8J
Hazard Ratios for 082 050 0.49
Ofanzapine10~'s.i;541
10.28.0.96} (O.27.0.8910.038 O . Q 1 B
p\ CP TIE 29
25
27
Phase liT: Reason for Discontinuation
from Phase I
0,039
OLI RlSP QUET ZPR TotalIn0:101l) (n=1tJ.4) (11=95) fn=131J (n.:.UC) p-vawe
Inadequate Thetapeutic Elfed 54 I SO"!.) 39 ( 38%) 37 f 39~.) 54 ( 39%) 18414"".) 0221
Unao: :eplab loSideEffec ts 29(27'Y.) 46 (<<%) 39( 41%) 54 (3 9%) T58(3 8%1
OLZpairwiset~ 0.008 0.032
TIE
Time to Discontinuation for Any Reason
Overall P-value=0004'
aun=6G
44 67%
RISP
n=G9
4464%
cuar,. .,
53 84%
Z J > R
nl::'135
104 %K ap la n- Mei er Med ia n
(mas)
95%CI
.3
135.97]7.0
[41.10.0J
•. 0
(31,04BI
Z8
{2A.4.4]
Hazard Ratios (or
Olanzapine
0.65
1°.43.0.97J
0.034'
1.02
10.67,1 .551
0.939
0.S1
10.43.0.87J
0.006'
Hazard Rat io s f or
Risperidone0.54
1043,0.951
0.027"
O . S O
10.42.0.'5,0.005'
Haz:ard Rat io s f or
Queliapine
0.94
10~;d ;31 '
TIE
Time to Discontinuation Due to Patient's Decision
0.'
c. S
• . .
"
TIE
0.048
ae
2'
30

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 14/90
Time to Discontinuation Due to Intolerability
0.6
0.'
02
4 a 12 16rmo '0 ~!ion Owing 10 1n1ol1lf2bility l m o J
I OLI I RlSP I(n=S61 ( n=69)
QUET I ZPR I(n=63) (n=135)
Discontinued 13(20%) 7(10%) 11 1m, , ) 19 (14%)
Phase liE: Baseline Characteristics
Assessment Tota l
0=99
39.7 10.4e mean SO
~:~~~~ ,.- -.--,--'--"-- . ".. _ 80 81%
Race
o Whi t ec Black IAfr ican-Amer ican
c All o th e r r a ce c rc u es
6 3 ( 64 % .)
33(33%)
33%
S p an is h /H is p an ic / L a ti no e t hn ic it y 14114 '10)
Edu ca ti on e ar s 12.6 2.0Married 99%
lJnemployed 64 (86%)
Time to pis,continuation for Any Cause
I 0.e ) "
J 0.6- " l~ ~---------,
J 1 5 tI 17 15
T""tI~iQtMy~!IRIJ
_ =N-..t5) Ouft;a,*,,(N<I!~!
~ O f ~fJ ~ :N f n 11 f I . G
I=:m~1 , 2 . r ' ~ fl2.~
0.57 0.39 0,42
HaurtfRilt0kwCbupl'lcl 1O~~;'61 to I~!~ec] (1l*~I~~6'1
aes 0.73
H&utd R l l t i o J IooOantDpi'oa 1 O ' : ' : ii , ' :; ' 1 I C t f ; J , . ti T l
'"H&DnlFbliolllooO\lortDpiw f O - : ~
t;k CATIE
33
35
-6-
~~eIlT:Most P'r,r' '1matic Side Effects
r>.du RlSP OUEr ZPR' P,.,;;lut
(nort08) 1n:1(4) (n..-ss) In"137)
D!scontinuedDuelo 19" ""19%
""0,478
SideElleds(Total)
WeighVMctaboli(; 8% ' ' I . I " " . " "0.004
Extr .1pyr . ;1midaJ ,' . ""J ,% " . om
" " " ' ' ' ' ' ' 0% ", " , 1% 0.797
0""' 8% 8% '''I ''''' 0.591
\J
ATIE
Demographic & Clinical Characteristics:Reason for Discontinuation from Phase I
"-"- ."- " : ~ " - - " ."-~""_.""-" ""-- .. "- ..
Assessment ClOZ aLI aUET RISP Tom l p-vaiue
" " " . n=19 0"'15 n=16 0=99
I n adequa te T he rapeu ti c 4.4(90%) 16(84%) 12(80%) 13(61%) 85(86%) 0.712Err"",
U n ac ce p ta b le S id e 3(6%) o (O"k ) 1(7%) 1 {6%} 5 (5%) 0773Elfects
Patient Decision 24% :3 16% 213% 1 S% 8 B% 0.290Adminlslr.l!ive 00% 00% o 0 '10 16% 11% NT
Time to Discontinuation for Lack of Efficacy
,~:'\"L __
o-r;a p-'r. lhro" 0.010"
1 , , " 15T~lD~b'l-'O.glEIFgq>(mG)
~fN""$l ~("",.,-~!N.'n ~ 'N'=")
CLOZ OU QUET
",,",5 n=17 1'1"14
NlJITIbor 6iscontinul'ld 5 11% 635% 6 .3%
f ? ; : "CATIE
HalOIttIFQtioslorClot;Ipine 0.2" 0.16
10.01,0.78\ 10.04.0.5410.019" O.()(),C"
0 .16(0.05.0.50410.003'
HazartlFQliosfor~ 0_66
1 0 2 D . 2 . . 2 2 J0"505
0."{O,21.2.231
0.5181.03
{O.3:1, l .2S!0.957
32
34

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 15/90
Relapse Versus Discontinuation as
Outcome Measures100
90
~ 8070
:i s60. .
.c50e
c. 40. .30>
~ 20
" 10U)
R.isperidone
- Haloperidol
100 200 300 400 500 600 700 800
Time In··study (days)
Mean time to relapse 452 (rlsper idone] vs 391 (haloper idol) days· p < .001
7 :: CATIE C sem an sk y J G e t a I . NEJM. 2002;346:1f5.22.
Conclusions
• In Phase I.only olanzapine had an outcome that wassuperior to the other antipsychotic treatments
In Phase liT. both olanzapine and risperidone had superioroutcomes as compared to other antipsychotic treatments
In Phase liE. clozapine was superior to other treatments
Discontinuation was a common outcome across alltreatments - lack of efficacy and patient decision weremore common than poor tolerability
Judgments about relative effectiveness of differentantipsychotics are dependent~ tcome measure
ATIE
Relapse Versus Discontinuation as
Outcome Measures
Rol.llp:H
In: IdequOlllr
. . . . . . . . .Po o rcomplia~
A d " " " ".... nts
Chou tocUseonUnue. . . . . . .
foUow-up
All oU...r
10 15 20
Pationts roportJng (~.)
44.1" '_ of nspertdcne- and S2.7·A. of hatcpertdct-treated s u b Joc t s d i s con t in u od
t he : s tudy for roasons unrelated t o re lapse (not s lgn ff i can t Jydi f f e ren t ,
p : : ' .CATIE Csemansky JG et aI. NEJM. 2002;346:16-22.
25
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 16/90
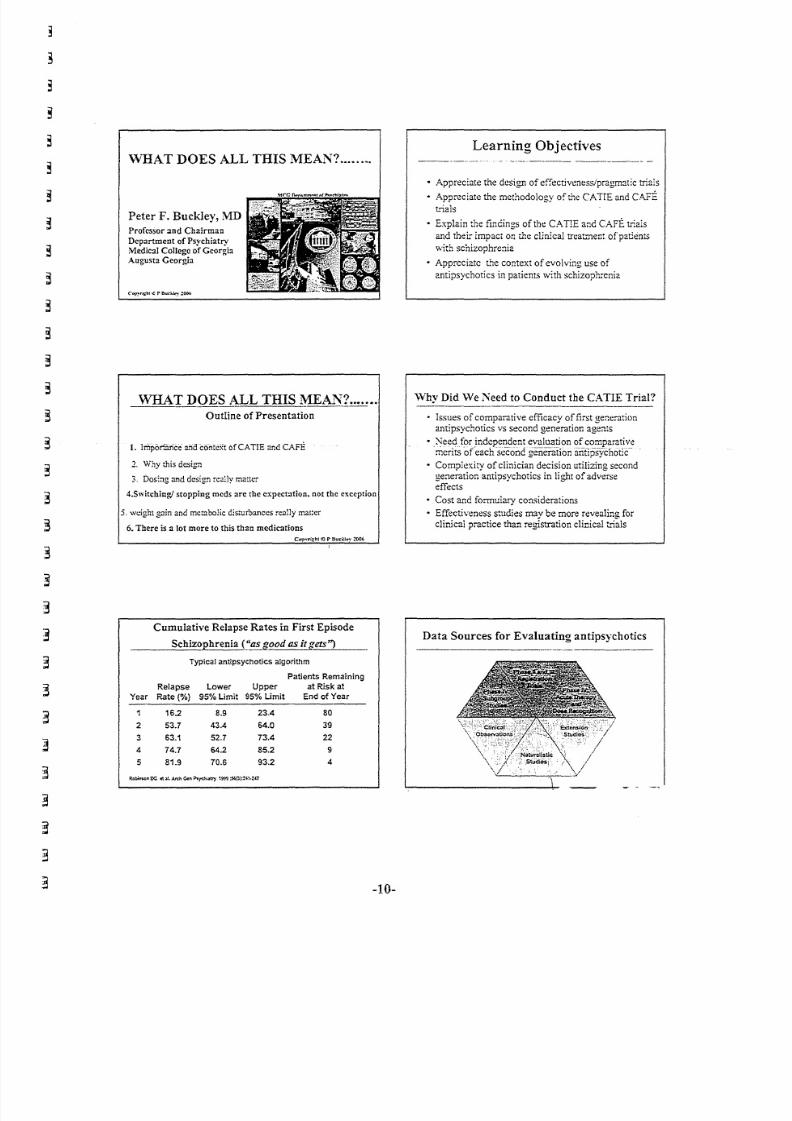
\VHAT DOES ALL THIS MEAN? .
Peter F. Buckley, MD
Professor and Chairman
Department of Psychiatry
Medical College of Georgia
Augusta Georgia
WHAT DOES ALL THIS ~AJ.,\1= ..Outline of Presentation
1. lrriporiarice andcontext 6fCATIE and CAfE
2, Why this design
s. Dosing and design really matter
4.Switcning/ stopping mcds are the expectation, not the exception
5 "w e i g ht g a in a n d m e t ab o li c d is tu r ba n ce s r ea ll y m a t te r
6. There is :1 lot more to this than medicationsC o~ vr i: :: bl ~ r8u l :' ; 'I ( > 'o ' 2006
Cumulative Relapse Rates in First Episode
Schiz~hrenia (~'!zsggod as ! ! . % c ; : : e t s = -· ' _ t _ ' ) _
Typical antipsyc:hotics algorithm
Patients Remaining
Relapse Lower Upper at Risk at
Year Rate(%) 95% Limit 95% Limit End of Year
16.2 8.9 23,4 80
2 53.7 43.4 64.0 39
3 63,1 52.7 73.4 22
4 74.7 64.2 85.2 9
5 81.9 70.6 93.2 4
-10-
Learning Objectives
• Appreciate the design of effectiveness/pragmatic trials
• Appreciate the methodology of the CAIIE and CAFE
trials
• Explain the findings of the CAIIE and CAFE trials
and their impact on th e clinical treatment ofpatients
with SChizophrenia
• Appreciate the context of evolving use of
antipsychotics in patients with schizophrenia
Why Did We Need to Conduct the CATIE Trial?
• Issues of comparative efficacy of first generationantipsychotics vs second generation agents
·NeedforindcEcrl_~ent evaluation of comparativemerits of each second generationantipsychot£
• Complexity of clinician decision utilizing secondgeneration antipsychotics in light of adverseeffects
• Cost and formulary considerations
• Effectiveness studies may be more revealing for
clinical practice than registration clinical b;ls
Data Sources for Evaluating antipsychotics

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 17/90
Pros and Cons of Registration Clinical Trials_ .._-------_._._ ... _ ..---- ----..------Pro
• FDA registration
• Placebo-controlled
Double-blind
Strict criteria
• Prove efficacy
• Detect adverse events
Co n
• No optimal patient
representation
Short-term duration
Most other meds not
allowed
• Limited dosinginformation -
~b.:lSti.1:n C$, Cl:a:OI"W.Sucll.loyPF,,20~:11::~lQ.
Factors Contributing to Antipsychotic
_ _ _ . _. . E J f ~ ~ 1 i y .e _ I J _ e .~ s '_ _ _ _
Compared to ri~r:!done at a dose of 4_I!!g/day-_.theequivalent dose of quetiapilze is ..•
p _ B : - - - -
SOOm~ j . . ( . , . . y
A!x)vc 800m:
bJ~ = = = = = - = - = =JO :::D JO sc
% ot respondents (N=2S6)
Buckley. oJ C!i:: Psyc.~oph:;)rm200S
-11-
/
Eff e ct iv e n e ss
Efficacy
Effectiveness = +
Tolerability
Dosing With First-Generation Antipsychotics
"In general clinical practice, the dosage of
an antipsychotic drug used in the treatment
of patients with schizophrenia is determined
at best on a pragmatic 'trial-and-error'
basis some doctors prefer high doses
and others prefer low doses; what dosecomparison studies there are do not offermuch of a guide in the usual patient:'
.V;ln v".~<:!1 T. C ' : _ : . . S a o rv : (\ 'l :i c- P 4 \l f \. \ ! . .. e vd ~ In': t eal l f ' l l ."Ol !· ·kC"OuJ.i lnt$c!\~".Uph.mli.;I';r.t 'CIt!\. .0: I\,..;."'>! a. 5 . : .h . .!r.SC ,;0.:\ li,.- ,\'n..n"'f1'1!r-,"~""'''''''"w I'wi,""' ('fwnll:1,""j,,-,J/uHI woJ T I' nJ I . .. . , ,,, ,) A ~ ro"Ctl,;llr;c,l'I'l:!"~"" 1',"Xl
Dosing of Second-Generation Antipsychotics
During Maintenance Therapy: Art or Science·?
• Dosing of second-generation antipsychotic
medications in the maintenance treatment of
schizophrenia is currently "more art than science"
• Study information on long-term use of second-generation antipsychotics is now emerging to inform
dosing decisions
There is a conspicuous absence of fixed-dose studies
• The dosing profiles differ between second-
generation agents

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 18/90
Reasons to Switch Antipsychotic Medication
Persistent symptoms
- Positive
- Negative
- Cognitive
- Affective
Side effects
- Extrapyramidal symptoms (EPS)
- Subjective dysphoria
- Weight gain
- Metabol ic
- Sexual dysfunction
- Sedat ion or insomnia
- Anticholinergic
We are not yet measuring health consistently enough
Frequency of B:z.seJineAssessrnent for Weight andMetabolic
Parameters Prior to Iniciat:ing Treatment with a SG.,A.
p.~.n. '& ..m'~~••!5~~~~:!iiiiiiir--r-~lH.lght .. blJdy W.li1h~
w.I•••, ~ u m " ~ · ~ ~ ' g l : DBlood p..... u...
F•• tlng btood gluco ••
F•• tlng lipid prom.
W ~ ro M ~
Evidenced-Based Practices in
Mental Health
Prac t ice Level o f E v id en ce Extent of
Imp l emen ta t iDn
concerted TMAP lmptementatinn, Med MAP var-iable
medlcatlcn APAfPORT/exPf:n consensus
management guidelines
muUisystemacic randomized control trial:s limited
family therapy demonstration projects 'partbl fidelity'
assertive randomized conlroltriab variable
commonity demonstration projects
treatment
ADA Consensus on Antipsychotic Drugs and
Obesity and Diabetes: Monitoring Protocol
Stan 1 2 w ks12
wks wks mos. mos. yrs.
Per sona l / fami ly Hx X X
Weight (EMI) X X X X X
Wais l circumference X X
B l o o d p r es s ur e X X X
Fa st i n g g l uco s e X X X
F a st in g l ip id p ro f il e X X X
Dbbtlts cere. 27:596-601. 2004
Advocacy, Recovery, And The Challenges of
Consumerism For Schizophrenia
« ..... One o[tlt~_t;Q!!§e_qu_e!1£~s_oL11t()te
effective treatments is that aspersons
improve, they will have an increasing
ability to express their views and
identify what they see as barriers totheir recovery. »
Frese, 1998
Schizophrenia PORT
Adherence rates generally <50%
• Correct maintenance dose of antipsychotic: 29%
• Adjunctive antidepressant: 46%
• Adherence lower for psychosocial treatments than for
pharmacotherapies
• Family psycho education: 10%
• Vocational rehabi litat ion: 22%
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 19/90
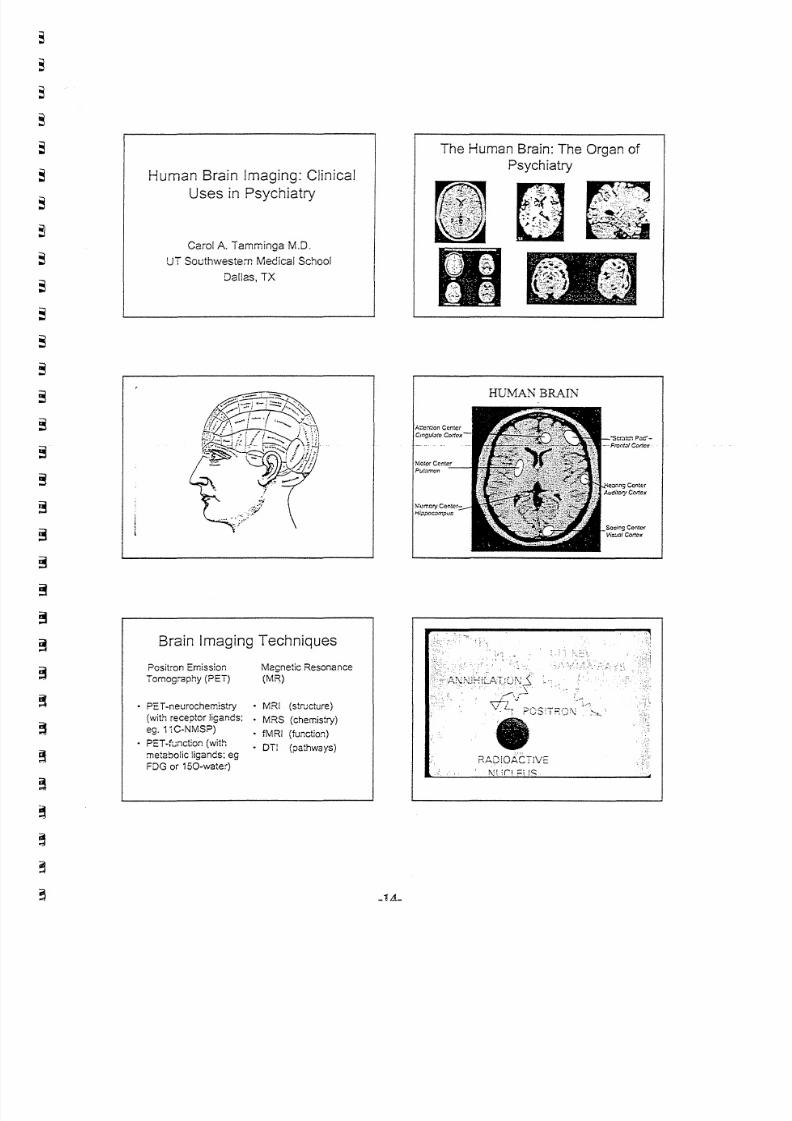
Human Brain lmaging: ClinicalUses in Psychiatry
Carol A. Tamminga M.D.
UT Southwestern Medical School
Dallas, TX
Brain Imaging Techniques
Positron EmissionTomography (PET)
Magnetic Resonance(MR)
• PET-neurochemistry • MRI (structure)(with receptor l igands; • MRS (chemistry)
ego1,C-NMSP) • fMRI (function)
• PET-function (with • Dil (pathways)metabolic ligands; egFDG or 150-water)
The Human Brain: The Organ of
Psychiatry
H U M AN B RA IN
:::':,:
RAO!OACTiVE
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 20/90
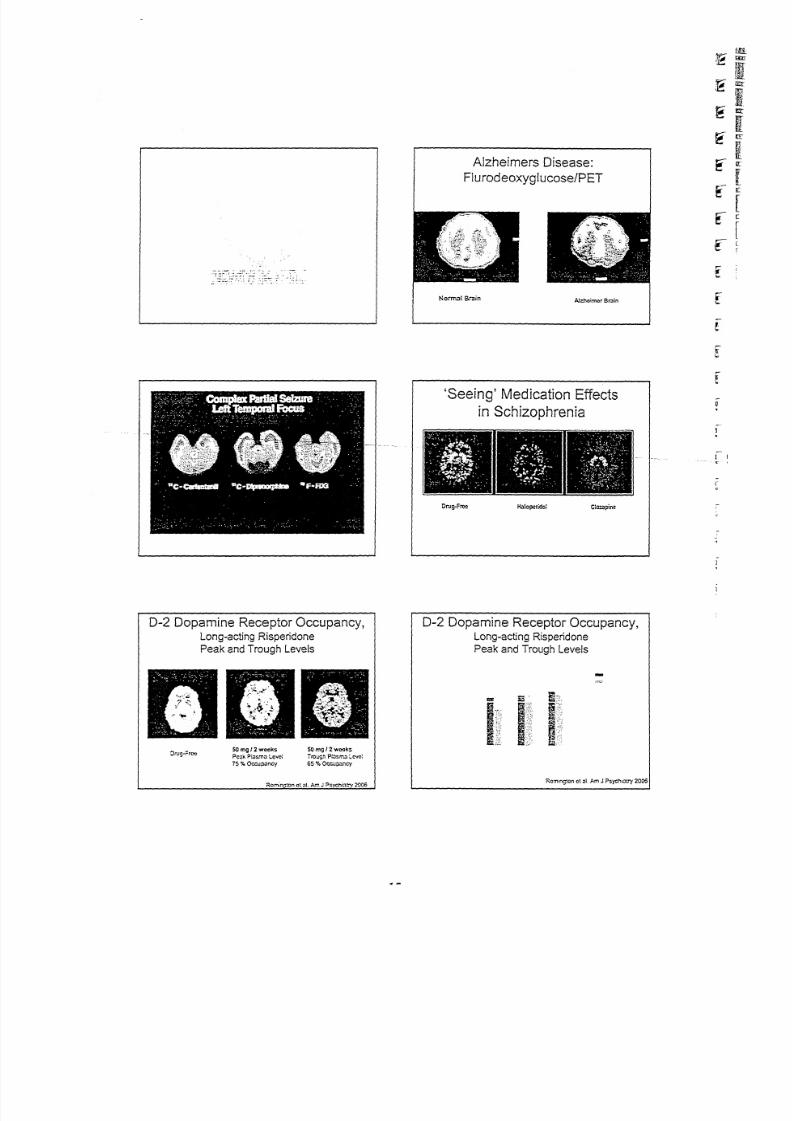
D-2 Dopamine Receptor Occupancy,Long-acting Risperidone
Peak and Trough Levels
so mg 12 weexsP C . : J k Ptasma :"el(c~
75 % Occupancy
50 ",g f 2 wook:
Tro;.;gn p : n S l " : " ' . . t I Level
65%Oec:.:;>ancy
Rcminc:~o:'lat ~I. A . - - r . J ?sVCf ' l i : lt rv 2006
Alzheimers Disease:
Flurodeoxyglucose/PET
A.l.;:hoimorBr.:IinNo rm~16r . l i n
'Seeing' Medication Effects
in Schizophrenia
O r u g . F I ' C < > Haloperido l C i C C J p i n e
0-2 Dopamine Receptor Occupancy,Long-acting Risperidone
Peak and Trough levels
I
" " 1 5 . . .~ . . . I m ~ : ;
I I JRC:T1ing!on c t a t. Am J ? s yc h e: .' )' 2 0 06

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 21/90
PHARMACO-IMAGING
Pharmacokinetics, Detection and Likeability:
DA T Occunancv of r~-Methvnhenidate
versus OROS-Methvphenidate
Spencer, Biederman, Ciccone, et a l.
SponSOiCU by 7'v1c7'c ilPharmaceut ica ls
Average::SEM d-MPH Concentration-Time Profi les:
4() rno !R-MPH :iQ mg OROS MPH
c0' _._._" -----v-." c:
::. c'!":.o- ,...- ~ t::
'j tc, •• ~ " ). ........ ",,.v,:,"
ccupancy- lime ro lies:
90 mg OROS-MPH
S pe nc er . e t a t, A M J ?svch .2C06
-16-
Rate of Drug Uptake Into the Brain
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - ~iv cocaine ivM?H ora! MPH
i..1m~(tfA"
~ ~ 'A 1.:
; " ; A r ;$ ' 0_
! . " . . ~
~_ ,. ., ... w. ""' .... "t ~;;" _ .' ... _ ....
l'_l_i n.-(_I
. '• ,Rapid
'.
• • • j Slow 1
"_ '~)f " * " , . - . • " . . . " ' Qoo
n.-I_I
1----------------,----------• Cocaine ( iv) and meL~y lphe~idate ( iv ) produce a ·high·bet me thy lphenidate (oral ) does no t
• The slow brain uptake of orai methy.phenicate per rn :: se f fec ti ve t rea tmen t w . t. l- : ou t a ' "h igh"
Volkow..: ~:.A l ' c h Cell P = o y c l J 1 ! 1 ' 9 5 : 5:' J N f l f J f ' O , $ . C / 2 O Q 1 ,
Average:l :SEM d·MPH Concentration-Time Profi les:
4Q mg iR-MPH 9Qm g OROS MPH
--

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 22/90
Listening Task in Schizophrenia
Normal Bra in
Schizophren ia Bra in
A modern MRI scanner.
-17-
OAT Occupancy vs._Detection
:R·~1?H
c o rrel auon . . 0 J!-
o
"
o oC) 0 0
% OccupancySccncor. t!: : 1 : . A . \ A J ?svch.2006
Decision-Making in Schizophrenia
Normal Bra in
Schizophren ia Brain
LAUTERBURG AND MANSFIELD:NOBEL PRIZE IN MEOICINE. 2003. MAGNETIC RESONANCE IMAGING
o OROS·\1r;~C~: J. ll on - OJ) )

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 23/90
Making an MR Signal
Contrast and contrast-to-noise in MR
images.'. \: ;r~:
Memory for a New Picture
~ ~ ! " " ' /
: : 1sceeaeuee: S0rm. .31 minu:; Sehi::ophroni:a
Overview
Images of Brain Activation
MovingFinger
Rest Motor Cortical
Activation
CLINICAL APPLICATIONS:
Functional Brain Imaging
• Alzheimer's disease (reduce parietal and
frontal neuronal activity).
• Epilepsy (interictal reduction in neuronal
activity and ictal excitation).
• Brain tumors (metabolically active=fast
growing; metabolically inactive=benign),
• Receptor occcupancy in drug developmentfor DA, 5HT, opioid drugs for CNS activity.
-18-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 24/90
NORMAL HUMAN: SEX DIFFERENCE PROGRESS IN NEUROIMAGING
1890 2005

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 25/90
SCHIZOPHRENINBIPOLAR
CONTINUUM
ARE THERE OVERLAPPING GENES &ENDOPHENOTYPES ?
II. Gottesman & D.R HansonUniversity of Minnesota Med. School
Historical Roots of Dilemma
All in all it may be concluded that there is no strong1- , empirical evidence invalidatinglhe dichotomy along-
Kraepelinian lines if only the existence of someadditional nosological entities is taken into
consideration. But this is, of course, not a proof,only a suggestion that the dichotomy is still, in
general, a valid hypothesis. (1990/1994)
Erik Slrt)mgren (1909-1993)
His v iew after d iscussin9 Gries inger's (1845) Einheitspsychose andUrs te in (1912 ), C r. C loninger (1994 ) & Crow (1994 ),
0degaard Revisited
Table ij" O i ~ gn o ni c u i lt r iu u ti o n 0 1 NO~ 9 i~ n inJu patient] ;nd ( n f ir p s ydu :ni e r e l a ti v es t
f't1tt1'lU9'e0lj!JYthot;enlninl;
No"o l di" 11 lOl.n!nMring:
PlIlb,ndd..,.,OIlI P'JYdlcric
fd.:i'ft~ Sdll.laplll~"Q; Rucu., . Allfal"
PtythOlu IIfycham
_._--,Smit09!trtnQ.Jtntfd,lK1
'"78. 7.l
'"Sdljlllllhrtn4,d~ldlltd na ,,.1 5 ' : ; ' IlJ
Sd!i.lOPIlf"lt>U,l\Qcltffd
hehIlGlllretht_C'tt.l
'" " . '" ",RUC: IW tP1 l ' ch01<I
" ". H ..5 Z . . . .
AlYpial~ftl<:1inplrdloul
" ca s ,8 1 iss
Mttlic-drprenin'plythlml . ,ra.t 10.6 '0 2
-- British Concepts
--- New York Concept of Schizophrenia
Z u bi n. K r ame r.WHO,Cooper
'60s
From Farmer et al, 1987
DSM-lli Categories and MZ/DZ Concordance
Ratio in the Maudsley Twin Series
Reanalysis
MZ/DZ Concordance Ratio8,
" 1 1 1 1 1 1 1OSM-III Categories

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 26/90
Multifactorial Model
( a.....-.w.bUl~ I, , , , t . ,.2L, ...:u. , . .. ..L. ,.IIl. ., . .IIL,
5p00c:itk.-u.cJW>iI~
f .. L 1+21.! .. 3L! ..... L! ... aL I .eL I
~ ... ...uc.I~
I +L !.2L'.aL' .....b'.aL, ...IIL'c;;;..--.I ..... uJ lI..blllq
• _ L I _ 2'L I _ llL t - . . L ! - Ill.. I - aL I
"-""-1 -1.. t_2L,_IILI_41..,_at.t_lJLt. ._ -
Gottesman, Shields. Hanson 1982
F in al D ia gn os es (R DC ) o f T arg ets a nd
S ib lin gs , B oth S amp le s (K im lin g 2 0 05 )
HRSz HRA f f Ne--."
S ch iz O ji li re n li He fa te d - -
P sy ch o si s ( SR P )- - Z O - u , rr % ) ' 5- (4.2%) -1- (M%)-_
A ff e ct iv e P s yc hot ic s13 (9.1%) 8 (6]%) 2 (0.8%)
(S M, SP , M 1DP )
B i po l ar D i so r de r6 (4.2%) 10 (8.3%) 9 (3.9%)
-NonPsyc:notic
A f fe c ti ve D i so r de r46 (32.4%) 48 (40.1%) 74 (32.1%)
-NonPsyc:notic
Anxi e ty D is o rde rs &19 (13.4%) 19 (15.8%) S5 (24.0%)
S ub st an ce A b us e
N o A xis I D is or de r 38 (26.8%) 30 (25.0%) 89 (38.7%)
--.·."""TttU"1::l..rx:u.r:,~
--- -'''1.'or(l.!-~
Fltll-f""'"\IOl.,1I·ll_! -:;V''''1«.,U.J-w..,IW'.-~
:!1:~'=~~r:~:i!--. . "UI_~t..-I.'
Prediction of SRP: (%) Sensitivityand False Positives
Erlenmeyer·Kimling et al, 2000
HRSz HRAff
False FalseMeasure Sensitivi ty Positive Sensitivity Positive
~Attenti!lll 58.3 17.9 0. .0 0/-Verbal Memory 83.3 28.4 25 ..0 11.3
Gross Motor Skill 75.0 26.9 50.0 5.7
All 3 Together 50.0 10.4 0.0 00
- - - - - - - - -HRSz = Highrisk tor ~phlllniaHRA f l = H i g h r i sk for affedive diso rders
NC = No rma l t . on ' II l 3r i son S \ l bi e c ts ( a n se n s i t iv i ty & false positives r ol es . . 0 % )
.ccncress-wneuer.aracct,
Convergencebetweenpooled linkage results of schizophrenia
and genes relatedto glial growth or synaptic strength
1 2 3! ~ ~,? 8~ ~ ! O ~1 12_
ht j · r ; : - ~ ~ : r ~ ; r t ·r ; u , r r! ' r ~: ~';' :.~t ; ~ ,- = ~ ~ I tU
PI I L . ~ - : u• . _ . .: lNX' 1-. . !! ., : ~- - r - - s., ru:u..i II f" '· "" '- _ _ ~~ -. I r - u.. ~p-J Pt"",c:i!!' -~ •.. - .-- ... - m '
~ WtSI~ ~I!: D - ~ I r Q U n I ~ ~~~._.::- -'-";;..n--~ !!". ;: ..,~!.!~~ :::- ~ l.M'U~UC U
U ,,1-U
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 27/90
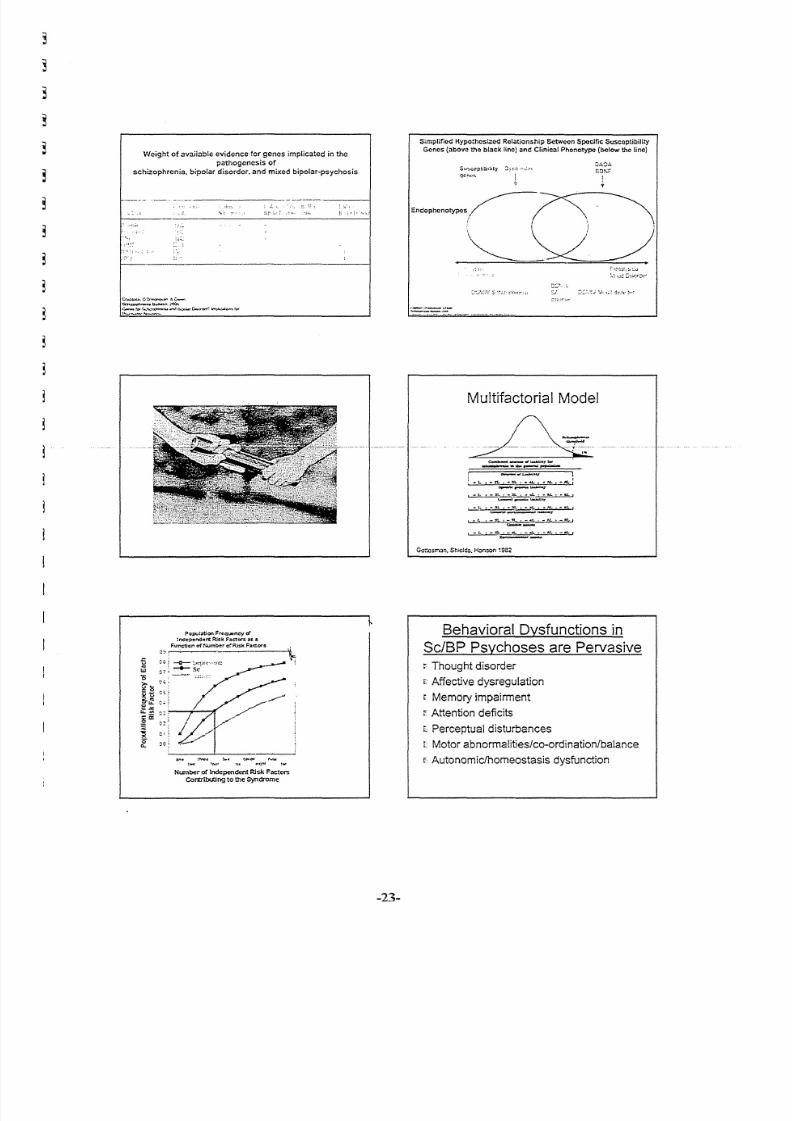
Weight o f avai lable ev idonce for genes impl ica ted in the
pathogenesis of
schizophrenia. bipolar disorder. and mixed bipolar-psychosis
Simplified Hypoth!>si::od Relationship 6ctwoon Specific Suscoptibil ity
Genes (above :.~eblack lino) and Clinical Phonotype (below the line)
S:J~"cptib,:,ty _'~:;:;"_;,\",
qc~(,~.
EnCOP!1cnoty;>csi~~
" '...... )'. );
~~
'_.'''_~l_---,,,.--,..~,' ..•.'.'.'"" --.~.-,.~"--,., - - .. .~.. - . , -
Cr;":'Jo.Xj,.C'o.~"",'l.C-::c.N.U;tph ..... l l ..u.t>n , .;'OOI'
~t : ' : , : ' : . . ~ ; , ; , . ~ . . . . . . . .1 0 . : : 0 ' . . . . .. c-.~\Y1'~ ~~~~
o ~;
'5 on
'"IIJ :;7
'0
h' = " - ~
~~
,g
1 ! ! " "Co :
u, . . c::
~ii:
c ~;e
~ : :: i ~
0- c ce,
Number or Inc!ependerlt RIsk Factor.;
Contributing to the Syndrome
Multifactorial Model
: "L t-::JL,.:" .. , • .u.,.IIl,.,-lILl~,-- ,\M.WJ. . . ,.
I_I .-n.t~.-N..'-""!
Gottesman, Sh i el d s, H a n son ~9S2
-23-
Behavioral Dysfunctions in
Sc/BP Psychoses are Pervasive
Thought disorder
E Affective dysregulation
Memory impairment
Attention deficits
t Perceptual disturbances
c Motor abnormalities/co-ordination/balance
f Autonomic/homeostasis dysfunction

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 28/90
"If we come to examine the smallest
ramifications of the cerebral arteries in
microscopical sections of the brains oflunatics, I believe it is exceptional to f ind
-----t} le-vessels---~a--- perfectly----healthy-- -1-
state ... the innermost coat of the artery
may show a variable amount of
proliferation, by which the calibre is much
diminished ... "
Brain Changes in Sc/BP
Psychoses
~ Diminished brain tissue (?maller brains.larger ventricles)
: Abnormalities of hippocampus/disruption
of pyramidal cell layer
r Variable and non-specific findings
: Gliosis is debated
,
1j
1j
0, s . s . Kc~~!M.D~R .& W l ' o J f l1 r J . ) tD ..~ti-t:~rm\!L~tD..F..A . . . F~"-.r.J!i.M.D..
K . £ . A ; ;" < : . M . D . . ,~JU . S c h m , J " ~ \ . D .
Brain Changes in Sc/BP
Psychoses
.- For many patients, no obvious8Onormality
r Imaging studies variably show decreased
metabolic activity in frontal lobes, temporal
lobes, various other regions
s Alterations in cerebral blood blow
"' would suggest, therefore, that the., .degeneration of the nerve-cells is
possibly often a secondary result of the
want of proper nourishment of the cell,-due--to-the cuttmg off Of rl:LeJJ:1 Qo d$t!:ppk _
by - di~~L_.Qr occluded _arteries.
Beadles, JMentsCiencA
~
-24-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 29/90
In"!,' t •• ,~I"(). . . . . '.;, . . . - . . .
, ". ...:
": /. -
. - /_"''''''''\IH'";''''''!I'''
t'l.....·,l·.••('."H."
Realities We May Encounter
~ There are no "Schizophrenia" or "Bipolar" genes
t'- The genetic factors for SelBe are o . o t . 1 o the
brai~
IT The genetic factors in Sc/BP are not "abnormal"
r Biological & environmental factors may be
common in well & i ll (nul li fy null Ho design)
'---------------.---- -!
-25-
-;0 1~ 2
c;
i
.
2
iil
~ ~'.,Ii'
~:.~.!:
2219 20 21 x- ~ " ,5 -r s 17 'j3
,'" - . ,L,
• x ~ •- J..::; " ..
I~ .• I : . I
I - . ,.~..I
~. I
r... .. . ~ 7
Hansen & Go::csrn::m 2005
" '. "· .· . .. .. "" . .. I .: ~ . .. . ~ . . 'I . .. .. .. .. .. . t...·."(_,,~_...:"",'..,..., ....,,..
~2CC5 O,R,
Hanson &I.L
Go:tcs."nan
" /)
Reality: Psychotic symptoms in____ disease can be Sc-like or
BP-like
E Huntington
LWilson
t Demyelinating
r Inflammatory eNS/vascular
L Parkinson
s: Paraneoplastic
r Seizure
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 30/90
Conclusion
r There must be at least some overlap inbiological and environmental factors in the
development of both Sc and BP given:
- Causal/contributing factors are very common
- Neurobiology does not separate affect fromthought (e.g. basal ganglia disease)
( A multitude of common environmental
agents may playa role in the...----developmentofpsychoses-but-the speclflc-> ---
nature of the 'trauma' may have little
relevance---it is the body's response,
shaped by genetic factors, that determine
whether the reaction is curative or
damaging
Implications
When the facts change, I change
ny mind. And what do you do,
.•.?
John Maynard Keynes [1883-1946]
British economist & monetary exper
-26-
Implications
f Reformulating our concepts regarding
- Pathophysiology-g lia, vascular supply, & neurons
- Imaging technology
- Psychopharmacology
I Treatment--e.g. anti-inflammatory agents
I Prevention- immunization, prophylactic anti-
infectives, anti-inflammatory agents, prenatalnutrition, etc.
What next?
( To define the areas of overlap and
uniqueness, we should discourage
researchthatstudiesschizop hrenia .and,
bipolar illness separately1-- .

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 31/90
Disclosure Information
2nd Biennial Schizophrenia Treatment 2006Phillip G. Janicak, M.D.
I have the following financial relationships to disclose:• Consultant for: Bristol Myers Squibb(BMS); Janssen; Pfizer; Shire
• Speaker Bureau for: Abbot; BMSiAstre-zenece: Janssen; Pfizer;Shire
• Grant/Research support from: BMS; Astra-Zeneca; Solvay;Janssen; Neuronetlcs
• Honorar ia from: As a speaker for the above companies
I will discuss the following off label use and/orinvestigational usein my presentation:• Antipsychotics for mood disorders• Anticonvulsants and lithium for psychotic disorders• Device-based therapies for mood and psychotic disorders
Objectives
o To review the interplay of psychotic
and mood symptoms across the.cHagriostiC contim.ium---
o To focus on the role of antipsychoticsfor both schizophrenia and mood
disorders
o To review relevant safety and
tolerability issues
Schizophrenia and Related
Psychotic Disorders: Core Sym
Affective natteningAlogia
Avotltton
AnhedoniaSodal inattentiveness
-scnnetcerten First Rank Symptoms
Treatment Implications Across
the Diagnostic Continuum: TheRole of Antipsychotics
Phillip G. Janicak, M.D.
Professor of Psychiatry
Rush University Medical Center
Chicago,IL
International Congress on Schizophrenia Research
April 6, 2006
Antipsychotics: Indications
o Schizophrenia
o Schizoaffective disorder
-~ O~Bipolar-disordef---
o Major depression
-29-
o Psychosisdue to other medical disordero Developmental disability (psychosis/aggression)
o Tourette's disorder
n - , ~
; tchizoaffective Disorder: CoreSymptoms
o Presence of a ful l mood syndrome plusconcurrent prominent delusions orhallucinations
o Presence of psychotic symptoms for at
least 2 weeks without prominent moodsymptoms
o Mood symptoms are present during asubstant ia l proportion of an episode
o Subtypes:
• Bipol¥,.manic,depressed,ormixedtype• Depr~ive type
- - - - - - - - - - - - - - - - - - - - - - - - - - - -
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 32/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 33/90
First Episode: Schizophrenia
Proportion of Remission
·0. . .·•!~
c·S 10
· 12f. . 26
39
· 52Ej::
Chlorpromazine
Clozapine
P=.033·
60 6020 40
% Patients With Remitted Symptoms
-8'1 GE E logistic regression for eeceetec measvres, cxmtrol led tor gender, duntjon, and weeks of
t re atment , T he fe w as a ls o I I ! > Ig ni fi ca .n t g en du e ff ec t (pc.Ol60, ....I th m al e CD feml li e o dd s ! '; ,t Ic 01remission bSing 1.89' I but no tIonJrignt intmCllgn with drug
uecerrran JA er II. Heurops'ftnophllmlllcololl'l 2003;28:995-'1003
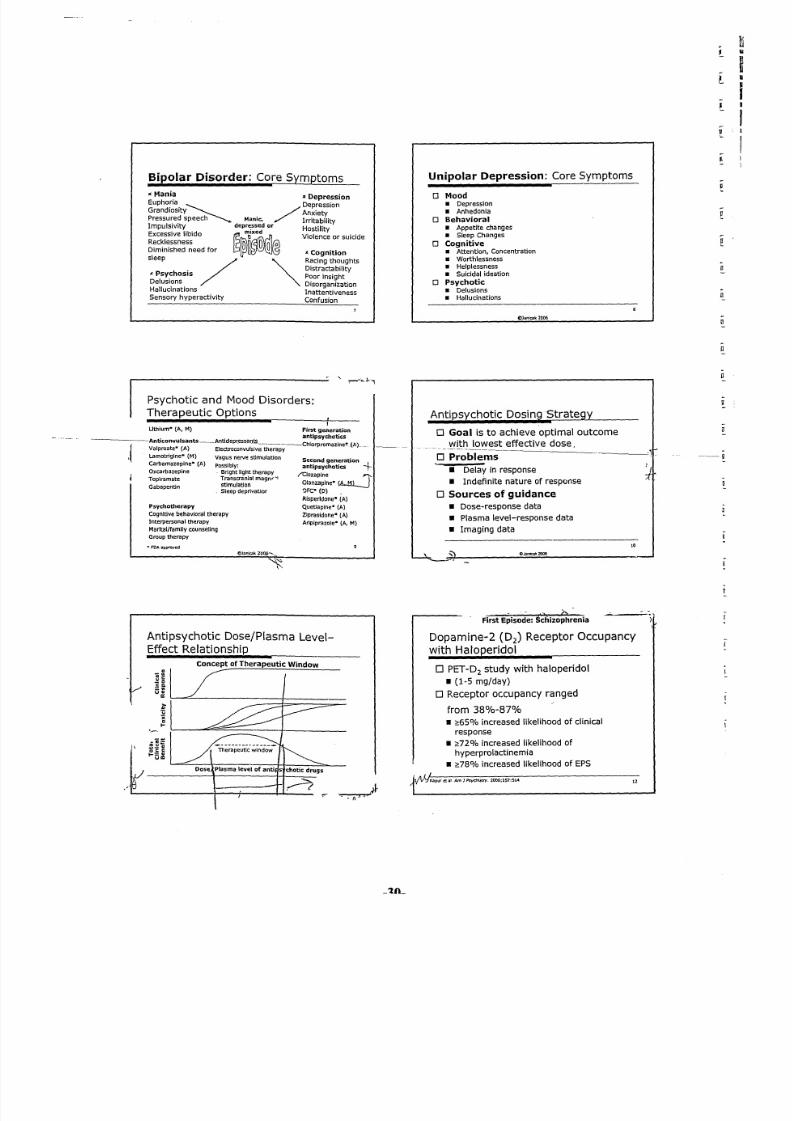
Acute Treatment: Schizophrenia
Risperidone vs Haloperidol:
PANSSTotal and Factor Scores (LOCF Analysis)
Fadors
UncontrolledDiso rganized Hosti li ty Anx iety lThough t E xd tem~l Dep resSIon
TotalPAHSS
~---~·--O
J-2
e-4
3 -6
Ul -6e- -to0
~ -12
~ -14
U wiG
-16
-20
S Risper idone 6 mg/d (n=255)
Haloperidol 20mg/d (n=85)
lOCF . . last Observation carried forward.·P<O,Ol risperidOntllShalooertdol' '1'$:0.05
Marder er"I,.J ClJ"Psychiatry. 1997;58:538
Acute Treatment: Schizophrenia
Clozapine Response Rates
Treatment-Refractory Schizophrenia
Duration Responders
N (wk) ("10)
Kane, 1988 126 6 30
Meltzer, 1990 51 26 61
Pickar, 1992 21 16 38
Conley, 199? 25 52 60
Breier,19~:'~ 30 52 60
Marder, 1995 54 29 54
Buchanan, 1998 61 ,';2 49
Rosenheck, 1999 205 52 60
"
100
IJ
rs
-31-
First Episode: Schizophrenia
First Principal Component
Neurocognitive Improvement
0.4
0.32*OlZ
• HAL
1: .0.3.'"E 1 iOJ:
0.2> ue cc.~E •_:I:
0.1
Composite
Keefe RSEet "I, Am) P$yd'I.iarry 2004;161:965-995, Data provided courtesy orDr ]A Ueberrnan 14
Acute Treatment: Schizophrenia
Schizophrenia Symptom Improvement:
PANSS Total Score
Baseline Study week
Analysis by last: observation camed fu rward ( lOCF ) a nd I nd ud ed s dl lU lp tv -e n\ c a nd s ct ti zo .aReat ve
patient$.
·Statlstically significant P<D.OSforIIrtplprarole, rtsperidone vs placebo (trt1ll4),Sahli AR.er ill Blo/ PsychlJtTy .. 2001;2{suppl 1):3055
______~~.v~.~·~I~_f~b~'~'~(~A-~~
Maintenance Treatment: Schizophrenia
Long-Acting Antipsychotics:
Potential Advantages
o Maybenefit treatment-refractory patientson oral preparations
o Mayimprove adherence
o Bioavailability approaches 100%
o Lower and more predictable plasma druglevels with clinically equivalent doses of oralpreparations
o Longer duration of action
o Possiblyfewer side effects, especiallywithhaloperidol decanoate; risperidonemicrospheres
18
\ tI Ja ni Ca k 2 00 6
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 34/90
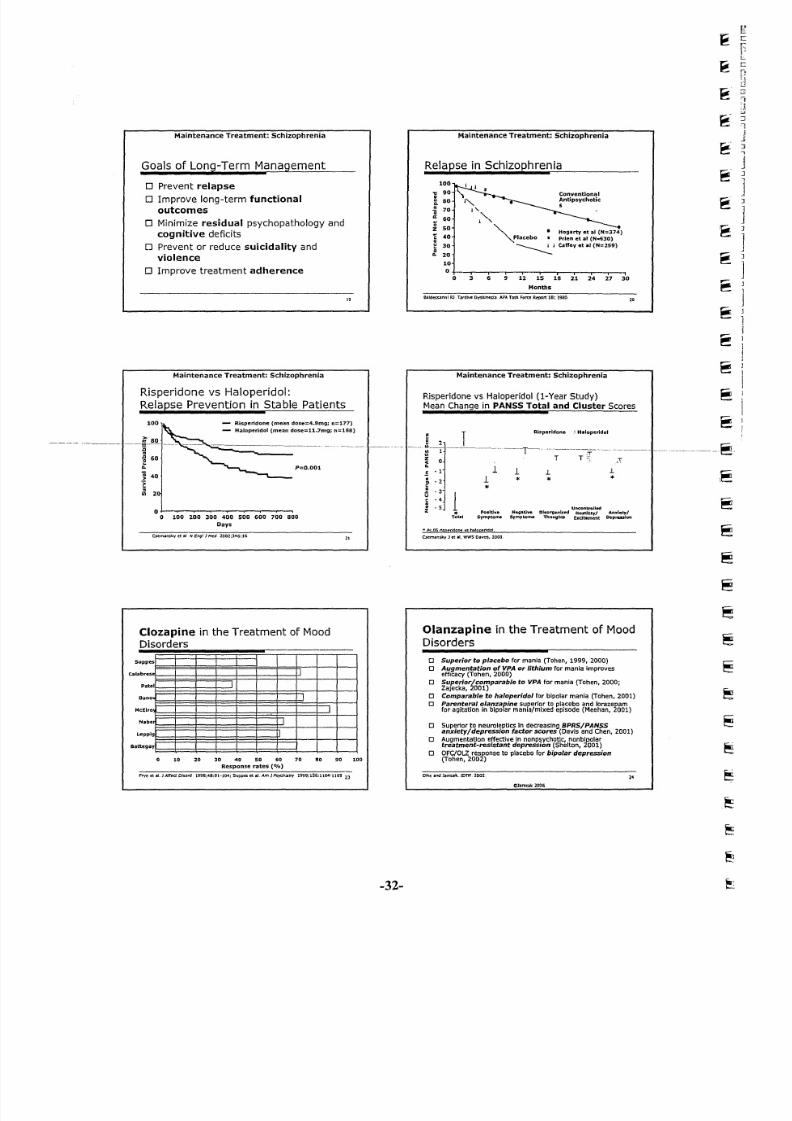
Maintenance Treatment: Schizophrenia
Goals of Long-Term Management
o Prevent relapse
o Improve long-term functional
outcomes
o Minimize residual psychopathology and
cognitive deficits
o Prevent or reduce suicidality and
violence
o Improve treatment adherence
Maintenance Treatment: Schizophrenia
Risperidone vs Haloperidol:
Relapse Prevention in Stable Patients
100 - Ri sp er idone (mean dose: :4.9mgi n: :177)
- Ha lop erid ol (mea n dos e=11.7mg; n=188)
P=0.001
o ~o 100 200 300 400 500 600 700 800
Days
Csemansky et a t N E ro gl J />led 2002;346:16
Clozapine in the Treatment of MoodDisorders
30 40 50 60 70
Response rates (O/o)
8010 20
Frye er at, J Affea Oisort l. 1998:48:91·104: Suppes et er. Am) Psycttioltry 1999;156:1164'1169 23
19
21
90 100
-32-
Maintenance Treatment: Schizophrenia
Relapse in Schizophrenia
100
" 90
~ SO0-m70. .
" 60l;
SOZ~40c
~ 30
•0. 2010
0
0
ConventionalAntipsychotic
•' "I'" -I '-
•Hogarty et a l (N=374)
Placebo Prien et al (N-630)
~,J CaffeV et iII l (N=2S9)
_'r--.--'~ -r---,---.,3 6 9 U ~ U II ~ D ~
Months
B al de ss ar in l F U. T ar di ve D ys kJ ne sJ a A PA T as k F of 'c e Report 16; 1 9$ 0
Maintenance Treatment: Schizophrenia
Risperidone vs Haloperidol ( I-Year Study)Mean Change in PANSS Total and Cluster Scores
~ JRis:peridone H<lloperidol
-- -__. "L.
" IT\In
Tz . _ " 1 _ ' : "<. .1 1.5 ·1 .L .l
!1 * * *·2
*·3
1" ·4e.. ·5 Uncontrolled:t
*Positive HCI1JaUni otsofljanb:ed HostlUty/ Amdety/
Tolal SymPWmI Symptoms Thoughts Exdt.ment ~pre:ulon
• ~OS r ta!~ridone V$ ha1 o eendo t .Csemansj, ;y J e r " , WW S naves . 2000
Olanzapine in the Treatment of Mood
Disorders
o Superior to placebo for mania (Tehan, 1999, 2000)o Augmentat ion o f VPA or lithium for mania improves
efficacy (Tohen, 2000)o Superior/comparable to VPAfor mania (Tohen, 2000;
Zajecka, 2001)o Comparable to haloperidol for bipolar mania (Tohen, 2001)
o ra~r:~f:~~~~a~~~fa~~:~Fai~~~~~~~ig~~(~~~~~n~e~8Bho Superior to neuroleptlcs In decreasing BPRS/PANSS
anxiety/depression factor scores (Davis and Chen, 2001)
o :~ja~:~~.:'~~~~ed~p=~~~(~~elrg~,bTo"Jt)
o gro1;'~~2b'W:!,)onseto placebo for bipolar depression
Olke and lanlak., r oT N, 2 00 2
Cllantcak 2006
2 .
~-~
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 35/90
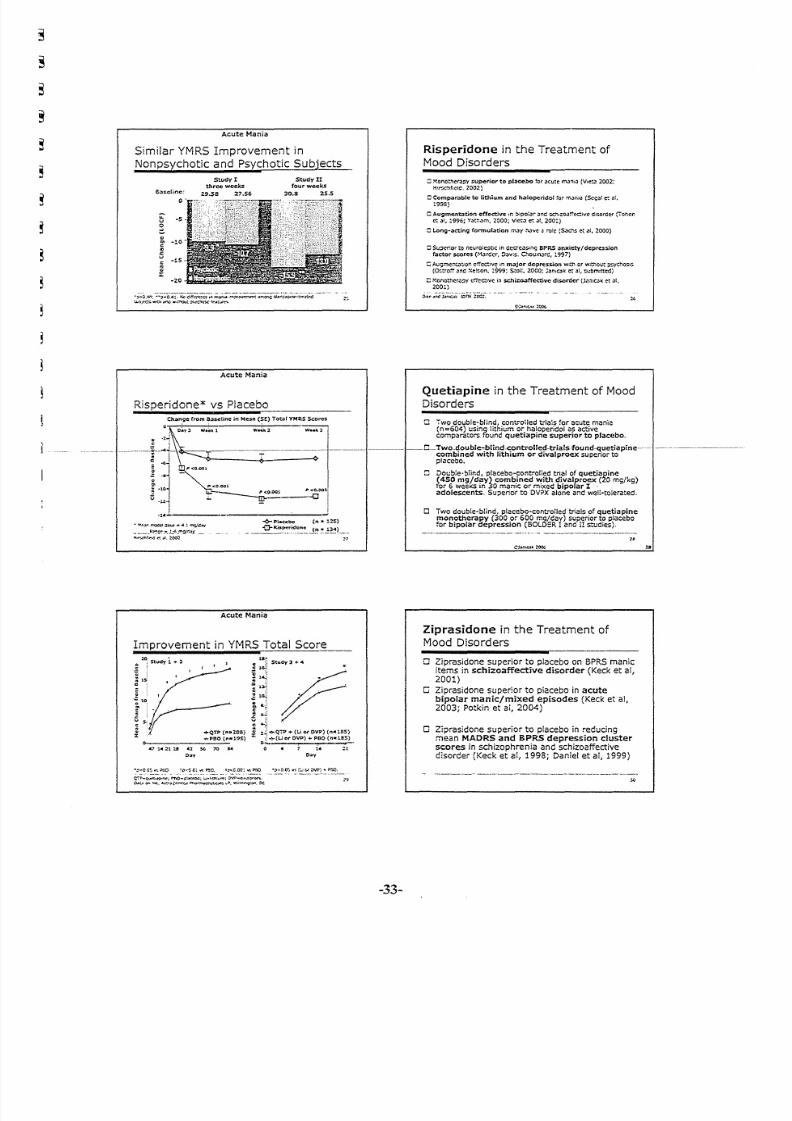
Acute Mania
Similar YMRS Improvement in
Nonpsychotic and Psychotic Subjects _
Study Ithree weeks
29.58 27.56
Study IIfour weeks
30.8 25.5aasenee:
. . . . -5v
~Q
'" -10
~J:u
-IS
~z
Acute Mania
Risperidone* vs Placebo
• ! ' o !" , , , , '. 1 T 'QC.e :t ~IXC .. "-,~ ~r;Jt!tt.,
__._.}t~~~.,-~,J:..~.." ' . '. ; I _( "~ ' I. _ _ ,
M,.-••C1\t.'!;(! eo : ~t :!oo:!
Acute Mania
Improvement in YMRSTotal Score,. .
e l Stu<ty: . .. . l
.:: :
c; :: ; rs. ."
I t O l ~ ' " "';; ~2 .. ....QTP <"_lQ8)
:c 0.- ....,.PBO(n_195)
.714::1 13 41 ~ 70 ...
0 .,
CI~1Study 3 ...<4
e 1~'
:l~
i: J~...j
~~4-~
: :~ +QTP + ru Of' OV?) (n.:'B5)
:r : o.::(LJ orOVP) +PBO (n-18S)
o 14::1
Doy
- e-c c o: .-s euo ~p.:~ 0;. vo; ~C. '::"C.OC: ~!"nO ·~·'O,Oo:."o;::...; c.I' OW) .. Pt:O.-" - _., - - _ , ,- ..- .. . _ .._ .. ,.." . . -_
C':'"P-~o.t:I.~; rt\O-~!.Io:~; ~""UI:"'<T!; 0Vf' ..c. .1!"~,
~:.> 1 ; 1 < \ '<If:, ...~~.....~"'~ Ph4"""KNt.u..'!; .,fi', Wi!,... c ; r . O I " I . or;
Risperidone in the Treatment of
Mood Disorders
::;Monotr.<:r.JPYsuperier to pteeebe for acute t':'l.1~iJ (Vu:!:~2002:H\r-_.c,:',Cld,2002)
:: CompOlmble to lithium Zlnd h31operidol :o~-n...U:"')(Scg;,t e: lll.1995)
C Augment4J tion effec tive rn !>ipo!a:- ;Jnd:-;C'h:o.lr,'ed:ivcdisorder (Toncnct .)!, :'996; Yath.)r."I, 2000; Vict,) et 031,200:,
c : LonO~3ctjn~ fOMnubtion m.:ty :'\J:VC a -e'c {~c.."'~ et aI, 2000)
:::scceeer to ncufo:c:ltiC in C::CC"C')::;. i !" l9 BPR$ 3nxiety/depresslon
f:J:ctor scores (MJ:fC:cr, O;'V!$. C~Ol:Ir\Jrc:, 1997)
: : A c . :Gmc ! 1 t .a : ;o ~ e ! :c : c. :i v < ; i:'l m.oJ:jor depN: ss io n W :: l' 1 o r W)thOl.!t ~chQ!;.l:;
( O: :; :ro :" :' " ne : N e! :: on . : '9 99 ; s ee n. 2 000; ; ;: sn tQ k c t at, :;'l.ibmittc::d)
C Monothcr,,::>yerrecave in s.chj:z:~ff~ve di$Order (J.."In:C.)i(e t " I.200~)
r-t Two double..blind, controlled trials ~oracute mania(n=604) ~si"g iithium or haloperidol asactivecomparators found quetiapine superior to placebo.
I~·_····_~~·· C_Two_double.blind-controlled-trials·found-<luetiapine-·~· ---'~-'---'--~~--combined wi th li th ium or divalproex super ior toplacebo.
Dot.:bie-blind,placebo-controlied trial of quetiapine(450 mg!day) combined with divalproex (20mg/kg)tor 6 weexs in ~Omanic or mixed bipolar I .adolescents, Su~erior to DVPXalone andwelt-tolerated,
-33-
Quetiapine in the Treatment of Mood
Disorders
CJ Two double-blind, plecebo-contrctted trials of quetiapinemonotherapy (300 or 600 mq/dav) superior to placebo
for bipolar depression (BOLO:R !and I!studies),
Ziprasidone in the Treatment of
Mood Disorders
o Ziprasidone superior to placebo on 6PRS manicitems in schizoaffective disorder (Keck et ai,2001)
o Ziprasidone superior to placebo in acutebipolar manic/mixed episodes (Keck et al,2003; Potkin et ai, 2004)
o Ziprasidone superior to placebo in redudngmean MAORS and BPRS depression clusterscores in schizophrenia and schizoaffectivedisorder (Keck et ai, 1998; Daniel et al, 1999)
:.

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 36/90
-.- PI .ceb o (n=122 ; Mean 8 ,.el1ne, 2'.7) 0 Convincing monotherapy evidence for
o -0-Ariplpr.owle (n=123, Me.n 8ase l lner 2B.2) efficacy in acute treatment of mania; onset
'e--L-j\"\"--'-·,·-·--------:---··,·, ._I .__...-=~o~f-a-ct-io-n~w_:it-h-in""'":2-:-4-d-a~Y~s--__:__:"::---c~
~~ 0 Strong evidence for or augmentation or
g > ; combination in maniame
~~ ·6 0 Future studies need to focus on subtype
: III ·7 * response patterns::E -8
-9 • e.g., mixed, rapid cycling, substance-10 J_~~ __ ~ ~________ abuse comorbidity
Acute Mania
Ziprasidone vs Placebo:
Mean Change from Baseline in MRS" 14 21
·2
· ·4
'"c -s·""e -a··:t '10
-12
-14Placebo (n:::66)
-a- Ziprasldone ("=131)
(80-160 mg/dav)
p<O.Ol.
p<O.DDl vs placebo,
ICed.et')l Am} Psych/arty 2003
·P<O,OI v5plecebo,t..OCf Inaly!>ls:
KeeXeti\l" Am)PsydJJ.)rry 2003
Acute Mania
Aripiprazole vs Placebo: Mean
Change from Baseline in YMRS
Day4 Week1 Day10 Week 2. Week 3
Acute Bipolar Depression
Olanzapine-Fluoxetine Combination(OFC)
• P lacebo (n : :: 355)
.6. Olanupine (n:::: 351)
o Qlaru:apine-nuoxetine combination
(n:::: a2)
.P< .05'1$ placebo.
Tonen MFJr. et II An:h Get'!Psych/dtry" 2003;60:1079"1088. Erntum In:Arttl Gert PSyct lio lt ry 3S2004;6:176
Jl
JJ
t*
-34-
Acute Mania
Arieiprazole
AripiprazoleDuration Mean
Study (wk) Comparator Dose (mg) Response11 3 Placebo 28 40%/19%"
2 3 Placebo 15,30 41«¥o,4solo/38%-
Placebo 28 510f0/31%"
4 12 Haloperidol 22 500f0/28%'
IKetk, er ill. Am J Psydll",try. lOOJ;HHl:1651.
Data on file. Bristol·Hyers SQuibb Company and Otsuka Americ:DFhlrm<aceutlcal. lrn;; 2003
Summary
SGAs in Acute Bipolar Manic/Mixed
Episodes
Acute Bipolar Depression
Mood Stabilizer Plus Risperidone
and/or Paroxetine
f8III
Q
:E. .::: 8
6
. . Risper idonC! (n; :: 10)
,o.'Pilroxetine (n ....lQ)
- e - - Risperidone + p.;lto'ICetinti (n = 10)
0123456789101112
Week
Sheltcn R. Stahl S J ClIftPsydIIatry 2004;65:1115--1719
32
J'

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 37/90
Bipolar Maintanence
The Role of SGAs
o Studies of maintenance ant ipsychotic therapy in
bipolar disorder are sparse
• Only studies to date are for olanzapine andaripiprazole
• Some lonqer-terrn acute trials (eg, 12 weeks)
provide indirect data (quetiapine, aripiprazole)
o Role of SGAs in bipolar maintenance is st il l being
refined
• Long-term tolerability is a critical factorsince pat ients wi ll not take drugs they cannot
tolerate
Strakowsk i SM, eea t El tf J Op Pharmllcofner 20DJ:~(5l:751~760
Adverse Effects
Adverse Effects
H.aloper ldof Cblaplne Risper idone Olart t.apine OUetiapine Zlprasidone Aripiprazol~ ,
Objectives
EPS· 0/. 0/' 0/'
We i gh t g a in 0/.
AIltichol ioergic 0/' +/++ 0/' 0/'
HemalDlOgical
Cardiovascular
Endocrinological 0/. ",. ",. 0/.
SedatiOn ./ -0A! a p pr o pr ia t e d o se s ; o e ncoe: • "'mild; -=mode ra! .e : : + +- + '" Substantial
Adapted f rom Masand PSee if H .Jndoaok o f P : ;y eh i. 6t ry I n Priml Jry c "r r. 1996
o To review the interplay of psychotic
and mood symptoms across the----I--.----dia~gn-o·stic-continuum----··--·------·- --- ..-._--.---
o To focus on the role of antipsychoticsfor both schizophrenia and mood
disorders
o To review relevant safety andtolerability issues
CJaric:lk2000
-36-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 38/90
The Biological Underpinning ofFirst Episode Schizophrenia
Robert Zipursky. MO.FRCPCProfossor of Psychi:>try
Tapscot t Cha ir in Schizophren ia Studies
University of Toronto
The Dopamine Hypothes isof Schizophrenia
• Drugs that block dopamine O2receptors resolve psychosis
Relat ionship Between Base line Dopamine Levels
and the Decrease in Posit ive Symptoms Measured
After 6 Weeks of Ant ipsychot ic Treatment
0
SOI 0.5r'= 0.58. P = 0.001
~ !!X l I
" "40,
0
~j
30 !~ 00
~ 20 0 00<:
0 00
101
0 0
I , 0
0:: o~~-----·-o~ -60 -s o -40 -30 -20 -10 0
C h .. .1 n go i n P o si !l vo S y m pt om s
Fol low ing 6 Wool u o f An:Ij)~yc:hOtie TroJtmGnt {.":')
B iology and Illn ess Ou tcome
• What is the nature of the disease weare treating?
+ Is schizophrenia a neurodevelopmentalor a neurodegenerative disease?
• How does our understanding of biologyinform our expectations about clinicaloutcomes?
.. .
Haloperidol and D 2 Occupancy
How Quickly Do Antipsychotics Work?
! Immediate onset ,
~;]I
I
Time (weeks)
k : o < : : O. K.l:wr S, AIenovWt ':'.~--ky RJl kr:It Con P: : yr ;h imry . :ZOCZ;( ;O:~ZU!.-~Z::
-38-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 39/90
I~~~~" '- - - - - - - - - - - -. .- - I ~ ~ ~ ~ . = - - - - ~ - - - · - - - - i . ~. .- . -
~ .. . . . . _ . . .. .
Perc en t Im pro vemen t Over T ime(Core Psycho ti c Symptoms)*
WC'Ckso! Treatment
.p < C ~ . PV~ I. OC~ ~~(e:;cn: the m..'ldl C~t.'d 0: ~me_Ef':'Of ! : m r - : . tt'prC"~: SE,
MCOr.I::I1 /.If:J'lGoI7nP:;yctu;ay :::lC:.GC:~:'Z~~~
Gra y Ma tte r Volume Defic itsin Sch izophren ia
+ When are thei_evident?-"------
+ Do the deficits increase over time?
+ Is outcome a function of the magnitudeand distribution of gray matter deficits?
+ Is the course of illness determined byongoing loss of gray matter volume?
B ra in A bn ormalitie s a nd Outcome
F :f !" '. J:' C 1. C o ro na l S ec ti on . .. . of t he B ra in . .~ o f:! P ati en t W i:. .. "Schizophrenia Wi3 1
Poor Outcome, !lPatient W~:'hGood Outceme. and :lHC':l l thy Comparison Sl:ojec.
Staa l et al, Am J P s yc h ", :r y 1 5 S :1 1 4 0 .1 1 4 2, Ju l y 2 0 01
-39-
BPRS "Psy cho sis " F a cto r Shows Imp ro vemen t
W ith in 2 H ours W ith A nti~chotics _: : P t4cebo
. , . .. ~rtd¢'
.Ot.l1naplnc
2Ho\J~ 24 Hour:.
.p~; 05 'IS ~"lce:>o
I<.;J;)I.:t'S C:.1~ Am J P=~. ZQO!.:,c.::~:!~!).oIe,
,1 -1
l :~~-~-:. .. .. ._ . . - .. .
Gray Matter Volumes Change with Age

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 40/90
t-yr Change in B ra in Volumes
, " ,
1", i
.t . ! T 1 ·I· I,• ~ -'-
,:,::- i, ,~ ri - a I
!'
Cabn . W,d r:1 (1001) ~rch G t 1 I Ps.vcAi f l l ty .59.IOOloIOIO
If the bra in a bnormalities fou nd in
.- __ schizophrenla.are. notprogressiv.e,---then why are the long-term cou rse
and outcom e so poor?
Berkson 's Fa llacy
~ . - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - ~
. .. t h ose who have o ther d isab iliti es th at a re notcausa ll y connected to the condi tion being inves tiga teda re more lik el y to ente r t he fo rmal tr ea tmen t s ys tem
.. . th ese e tio lo gicall y unrel ate d condi tio ns may have apernic io us i nflu en ce on the cou rse o f t he il ln ess.
P . C o h en . J C o he n. A rc h G e ne ra l P s yc 11 ia tt y 1 98 4; 41 :1 1 71 1 -1 1 82
Whole Brain
Volumo
(co,
- -_tIIIcIb_
pelleU
'~I
Z i p u r sk y e t ;1 1 , S c h iz o p h r en i a R e s ea r c h 2 0 04 ; 71 : 5 15 . 5 1 6
The Clinic ian's I llusionP . C o he n, J. Cohen, Arch Gene ra l Psych i a try 1984;41 ;1118- 1182
--
. .. t he a tt ribu tion o f the cha racter is ti c and cou rse o f those_..p_atLellis__w_ho_are_currentlyJllJoJruu:mfire.pop_ulatiQocontracting the i llness.
... t he c lin ic ia n's sample is b ia sed towa rd cases o f l ongd ura tio n s inc e the prob ab ility tha t a c as e w ill ap pe ar in ap reva lence sample is p ropo rt iona l to i ts durat ion.
Time to Remission in F irs t Episode Sch izophren ia
Lieberman J, et al AIr:h Gen Psych i a tt y . 1993;511(5):369-376.
-40 -

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 41/90-41-
R ecovery from psychotic illness:a 15- and 2 5-year internati?~al fo llow -up study
G .Ha rr is on c t 0 1 ; ,
B r it is h ~ou " 'o l o ! P s y ch i o tr y ( 2 00 1 ) . 1 7S .5 0 s. .S ~7
+ 14 inc idence coho r. .s /4p reva lencecoho r ts (N = 1633)
+ % t im e p sy ch ot ic in f ir st 2 y rs b es t p re dic to r o f o ut com e
+ - 5 0% o f t ho se w i th s chi zophr en ia r at ed a s " re cove red "
• - 4 0% h ad n ot b ee n p sy ch otic in p as t 2 y ea rs
• 5 6- 74%we re wo rk in g f or m o st o f t h e p as t 2 y ea rs
Wha t det ermines t he ou tcome f rom sch izoph ren ia?
"~ /: ~ : t ~____j
Pa tien ts No t Expe riencing Psycho ticS ymp tom ~xace rb atio n o r Rela ps e
1.0~
~-'-'
o s J ~~~ 0.61
~
~Ok
I'0~ . : : : i
I
O . 2 JI
0.00 12 24 3S 4S 60 72
Week
Reemct'!; lcr:C7of iJ"ychotlc :ym;:rto:r.s :amon; so c l irJc ; l: !Y :: :J!:) lcpatents wi:'''! recent-onset
G~:;,~~:.~e~~::;~r.t;;~,~ c e ; ~ s : r . ~ m . ~ : i~~I protocol
Why do so m any patients do poorly?
+ Premorbid deficits
• l imited access to needed interventions
• Non-adherence with resulting relapses
• Downhill spiral due to stigma, poverty.homelessness, unemployment
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 42/90
Research in Childhood and
Adolescent Onset Psychosis
Tonya In, i/e, M.D., Assistant Pro fe ssor
Division o/Child and Adolescent Psychiatry
Unt'versitv Afflliations:
Departmen t o f Ped ia tric s, Insti tu te o f Child Development , Cen te r for
Neurohehavioral Development, 'Center for Magnetic Resonance Research, Center
for Excel lence in Children' s Men ta l Heo .l th
Communin, Affiliations:
Board Member: Minneso ta Assoc ia tion for Children' s Men ta l Hea lth,
Educational Network of Minnesota
The Team
PlnlcipznlJ- Th:anky.u~
- hri cto tJ
- 5ib~"p
- H=hhy"o~R,ef(lTahsoorm
CQJrmIUtI;,y Hd U.iocn.i,y Mftll~lllnllli
l 'TOfeuJo~
- .AMd41l1~~1f
- Yo"rbh)'l:lot:nuCIiU;
~ UorMO~IC_
- HooI"fJftIr~DtplI ini loItI:
Rtse2n:h Auilbnll
- ....~Civirrgne:s
- Ab en Fo a.
- W m~ Le-m
Cndu"r/Medial SIudnlU
• D oIU y, aH c! r l . . . . . ~"hhbl
- 1 .i: IL .ia
- k c . .. .. C an pb dI
~dtnu~ I C aI i cC . Ik 1 I. M .D .
Voluntnn
MI~Sd<tnidl
~ f bint -~ 'r ;c r
'mdoaora! Rntlrcli Auocialc- M . nu f .l K n> d i. M .O .
- A )' So C'T Il l" I Un Fi Ut -, M .O
FltullyCoUaboralll"~l~d:in.f'bD
McmiaLac:Qm.PII.D
AfWa .....jum.M.D
.IoR:"udG.M.O~I'II.D
Sa>a~.I'II.D.
I'rkfMib.M.D
J~IwIJCIl$ I! I , .MD
TimS)WS.,M.D.
Mrnlon I Sponwn~ KdYmO.Unt .M.D .
~ 5 .. C I w I c : s SduU.. M.D.
- Q<#" l a.A.Nr l I -I I cI. f ' II . .O_ INCiouarnm,l'!t. .D.
FundlntSllu~
Ctf tl cr (o rN~bm . .. i onIDn-o~
NAflSAD
N I M H
MQluIII Incu~Na .ros. :i c" 't ~ IMINDI
M i nl > C. W M e di Q l F o ul !d .1 h ca
Schizophrenia - The etiologic puzzle
ra re .
M al es ha ve ea rl ie r a ge o f o nse t
B o th g en et ic a nd e nv ir on m en ta l
c om po ne nt s i nv ol ve d
D iv er se a rr ay o f b ot h c og ni ti ve
a nd c li ni ca l s ym p to m s
D rug s o f a bu se c an m im ic
s ym p to m s o f s ch iz op hr en ia
I mp ro ve me nt o f p os it iv e
symptoms wi th typ ic a l
neu ro lep t ics
Im pro vem en t o f sy mpt om s an d
c og ni ti on w it h a ty pi ca l
neu ro lep t ics
Phases of Schizophrenia
Pre-l lIness
Subtle Neurocognit ive
& Social Defici t s
• M ot or f un ct io n
• A t t e nt i cn
Symptoms o f
Schizopbrenia
• H a l l u c in a t io n s• W o r k in g memory
• D ef ic it s i n s oc ia l
cognit ion
• D e l u si o n s
• D i so rg an iz ed t ho ug hl
• D is or ga ni ze d s pe ec h
• N e g at i ve SymPtoM
Relationship between the Onset of Psychosis and a
History of Cognitive Decline and Social Withdrawal
A T im e u e e Approadl
r A t!"l------------:~-t > J ""-=='"
/!V I
15 14 13 12 11 to 9 8 7 8 5 " 3
Y8~ 8.b-oOmetofMod.~ Psychnis
2 1 Il~rclp~1

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 43/90
Genetic Factors
i' L• 1 ;. .. " ,, -, _. ,
'? ;~I'''''_'''!'O_", ~
i~~
_._-::
Hcr..ar. Brain Deve'oprnen;
.M
(;""'='<~."""""' ' ' I'o ' ' ' \I':\~:.l' M.t.(~~'1:\t..::."t t"...
I"'~'t'( ... ,!,-,,'"'''' ~1""t:Z::\~..pC;',,-, .\~;,l,r'{.;.it>
-44-
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 44/90
,
Adolescent minus adul t
statisrical parametr ic map
o f gr;lY m : : : u c ! ' reductions
(Zvscorc =,,5),
;-,~
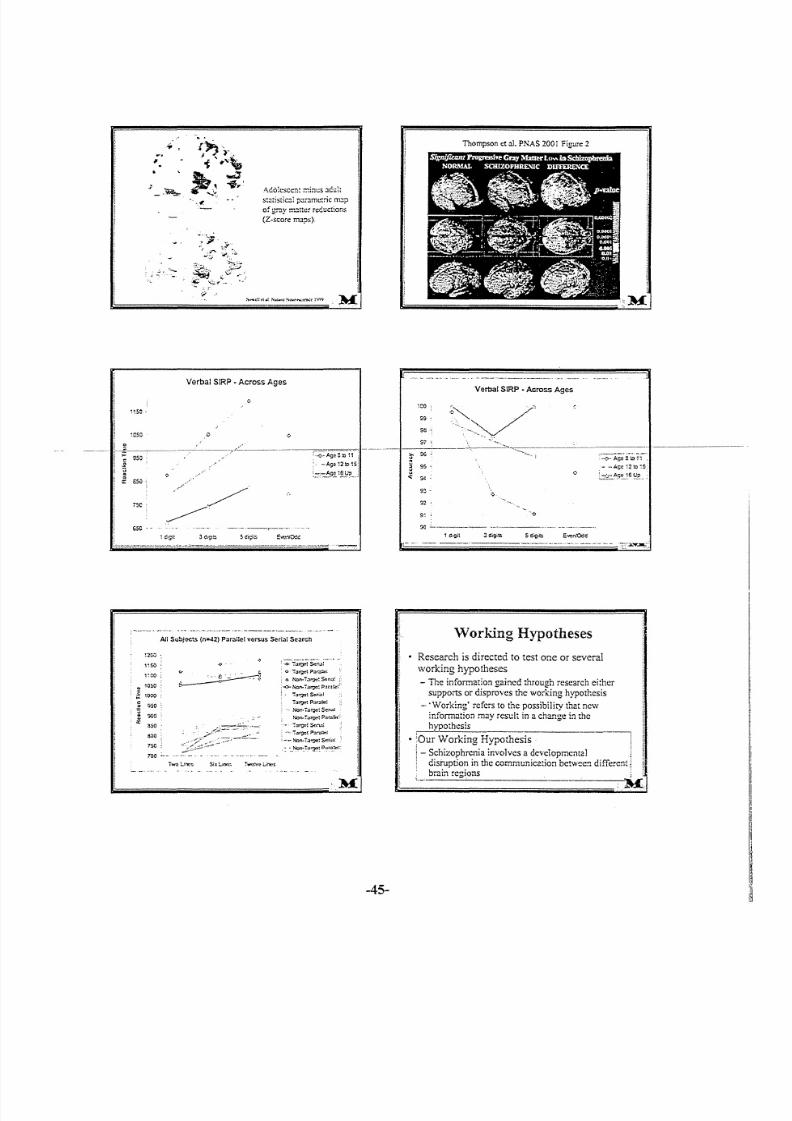
Verbal SIR? • Across Ages
~ ~5 0 ..
750
65C . -
All Subj~.s ( n = -42 ) PO l r ."Ue I versus Seri~: So: trch
;200'
1,50 ;
1":00
10S0
:000
-0- i . :l r o e t S d n ,, :
O''l'.:s*tj).::Ir.l~'
. 0 Non--i . lr: : lQ: S t l n . ' l :
,..o-No,n.i<u?o: ?~t;I!lc::'
. " ra t? O! $ (!riO !;
i ' : I ' ! " O M Pnr.lGo:
Non-'ta roe ! ~rl;lj
Non- f ' ll"gf!t Parn::tl,
_- ;.::u',;:t~:~n,;t!
: ""''':'olf?Ct ?.:.ro~;
: -~ . N on - T.::.~! Seriol;
: ~_ ,N< ln:T! I, ? : ,:_Pp~ .~ ?c : :
~50
\ l O O
800
7S0
7 00 ; ,_ ._
T ho m ps on c t : 1 1 . P NA S 200 iF ig ur e 2
----
Verbal SIRP • Across Ages
'co
99
58
$i'
il' 95
~ 95
. ; ; :9<
90
n
9;
so, .ccn
-0-- Ag e e:o r-:
- - Age ,2:0 ~5
L:!~::.~9!:,,~e Y . P . , _
Working Hypotheses
• Research is directed to test one or severalworking hypotheses
- The information gained through research ei ther
supports or disproves the working hypothesis
- .Working' refers to the possibility that newinformation m ay r esu lt in a ch an ge in th e
hypothesis
• 'Our Working Hypothesis
: - Schizophrenia involves a developmental
. disrupt ion in the communicat ion between di fferent]
bra in regions.--~=------,----...c....---M
-45-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 45/90
Testing the Hypothesis: How?
• If there is a problem with the connectivity
between brain regions. how do you measure that
in living people'?
- Diffusion Tensor I rr '& l lg ing
- F un ctio na l M ag ne tic Resonance l rnaging
- Elcctroenccpholography
- Magnctocnccphalography
B r o li n I n 1: 1 : :i n ;: : in Childhood :InC Adolescent Pxychiarric Disorders
h~~i':f·www .:nacrn!J.or. :hnfo_rc!\ot . :! ."c~:l! . .t icio;:s. · \\hilC._hr. .t :r.J:s{).uc::;.ht . .. !~
blue= inferior/superior (into 0:-
ou t of plane).
. '
Gyrification
-46-
: t ,I';
: t J [ 1t
o
..&.T.....

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 46/90
Alterations in Patterns of Gyrification in
Development and Schizophrenia
//
~!di' _-;
\ 1 0 0" : ', , 11 , . . . .t, : . . , . .: . .. . . ~. . .. .. . !.........._·.....r..... ,t h ~ "; . - ~ " -..,i' " · " . . . 1 <>1 ";1 . .' . . . . . 1 01. . , 't.., ..I~';'..tv ".,.~ : >. I t1'>< ~, .. . . ' . . . . ~~ . .
--i
M
-47-
~~I»."' ........."'...._
......_ ..u..
- = - = : : : = - : . =
The Team
"an",ip,llnl.-Th."",:,",.,,:!'aI_.
" " ' " ' "r~.h"~".----.~rnT.h ..... rff'o
~~1 .... _.~" .... : . 1 0
'II~""I:~~y........, . ,. ) I< I o o . . . . ( ~ ·
I'.JV.(~(·:....;.
.......1··"1'~•..,_.. ... _
kn"."fh -,"-,.unn.
.....t"I0~
. ,: . .. . 1 '. .. .
WiI\o._
G,...Ju~""'Ift!l{~~.....m.t ..
1:'~U.""'f:"''''''' ''':
"'.....~n~••,:._~IIr. tuIIY(:O)oIt.boo"J. t . .I"
(_ ~..,,&; ..... f't.:l
' "' - t_~j", !.1
"' .-..lo4l)
;._,r....:..~v,!.'. r'..:'.. .,.,~ ~:)
~I,(i "n
~-"",~,",)r_h~M~
.:..;.... 0.).._:'<10
,,('\u ""t:."":lI I o oo I . . .. . , . , i"!I!)
~vno!I.l:s..u"'"1....... i.H~~, .......!:)o-,.~~,_..._ " ' A i f : v . r >
" ' " " , , e l t " "'U-. ....~~
;-:.-,....~
M o - oo . . :;r_......:~ '_.!)...",·_~"\t:";"Il
~ ....~ ..~,r, ;...

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 47/90
Antipsychotics in Teens
International Congress on Schizophrenia Research
Schizophrenia Treatment: Bridging Science to
Clinical Care
S. Charles Schulz, M.D.
Professor and Head
Department of Psychiatry
University of Minnesota Medical School
Disclosure Information2nd Biennial Schizophrenia Treatment 2006
S. Charles Schulz, M.D.
I h av e t he f o ll o wi ng f in an ci al r el at io n sh ip s t o d is cl o se :- C o ns ul ta nt f o r E l i L il ly , A st ra Z en ec a
- S pe ak er 's B u re au f o r E li L il ly , A st ra Z en eC 2
- G r an V Re se an :b S u pp or t f ro m A b bo tt , E li L il ly , A st ra Z en ec a
- S to ck ho ld er in N on e
- H o no r ar ia f ro m A st ra Z eo ec a
- E mplo ye e o f N o ne
I w il l d is cu ss t he f ol lo w in g o ff l ab el u se a nd /o ri nv e st ig a ti o na l u s e i n my p r es en t at io n : An t ip sy ch o t icm edica tio ns, a s n one a re a pp ro ve d f or u se in p atie ntsu nder 1 8
• To describe diagnostic and epidemiologiccharacteristics of schizophrenia when it occurs in • Psychotic symptoms of p eople who developteenagers schizophrenia frequently begin during teenage
___ .1__._" To sample neuropsychiatric studies of adoles.c~llts._.__ .I I._._ ...) 'ears - maybe as many as40%of cases in lJI.J!kL--.I ....------··--·with schizophrenia that illustrate a similar (Loranger, 1984)pathophysiology compared to adult subjects • The diagnosis of schizophrenia is generally stable
• To review studies of pharmacological treatment in in the first episode after 6 months from indexadolescent schizophrenic patients interview (Carlson, 1994)
• To conclude with a synthesis of the use of • Outcome may be poorer in earlier onsetantipsychotic medication approaches to schizophrenia; however, large scale studies haveadolescents with schizophrenia. not been performed (Ropcke, 2005)
Objectives
Early-onset Schizophrenia: A IS-Year Follow-up
Rdpcke. B and Eggers , C: Eu r Ch i ld Adolesc. P s yc h ia tr y 2 0 05
In tr od uc tio n: T he o bje ct iv e o f t he s tu dy w as t o a sse sso u tc ome i n a do l es ce nt s w it h s ch iz o ph re ni a 1 5 y ea rs a ft eri n it i al t r e atmen t
M et ho ds : G l ob al sy mp to m s a nd G l ob al A sse ss me nt o f
S o ci al F un ct io n w e re t he m a in m e as ur es
R esu lts: O f th e 55 su bje cts, 8 5% w ere fo und a nd 71 %in te rv ie we d. F ul l r em iss io n w as o bse rv ed in 8 % , m o de ra teo utco me in 56% , and po or o utco me in 36% . S ev ere o rv er y se ve re im pa ir me nt ( G AS F ) w as n ot ed f or 5 1 % .D ia gn osis w as st ab le o v er t im e f or 7 0% o f t he sa m pl e.
Conc lus ions : In t hi s s am p le t he re w e re m a ny s im i la ri ti es t oa du lt s ch iz o ph re ni a a nd s om e d if fe re nc es f ro m YEOS ,
-49-
Diagnosis and Epidemiology of Schizophrenia
When ItOccurs in Adolescents
Brain Imaging Studies Reveal Morphometric
Differences Between Adolescent
Schizophrenia Patients and Controls
• MR1 studies reveal differences in ventricular and
cortical areas (Rapoport, 1997; Friedman, 1999;
Kumra, 2000)
• Imaging studies suggest possibility of
"progression" of imaging measures during
adolescence (Rapoport, 1999), but not in all
studies (James, 1999)
• Functional imaging studies also show differences
between patients and controls (Jacobsen, 1997)
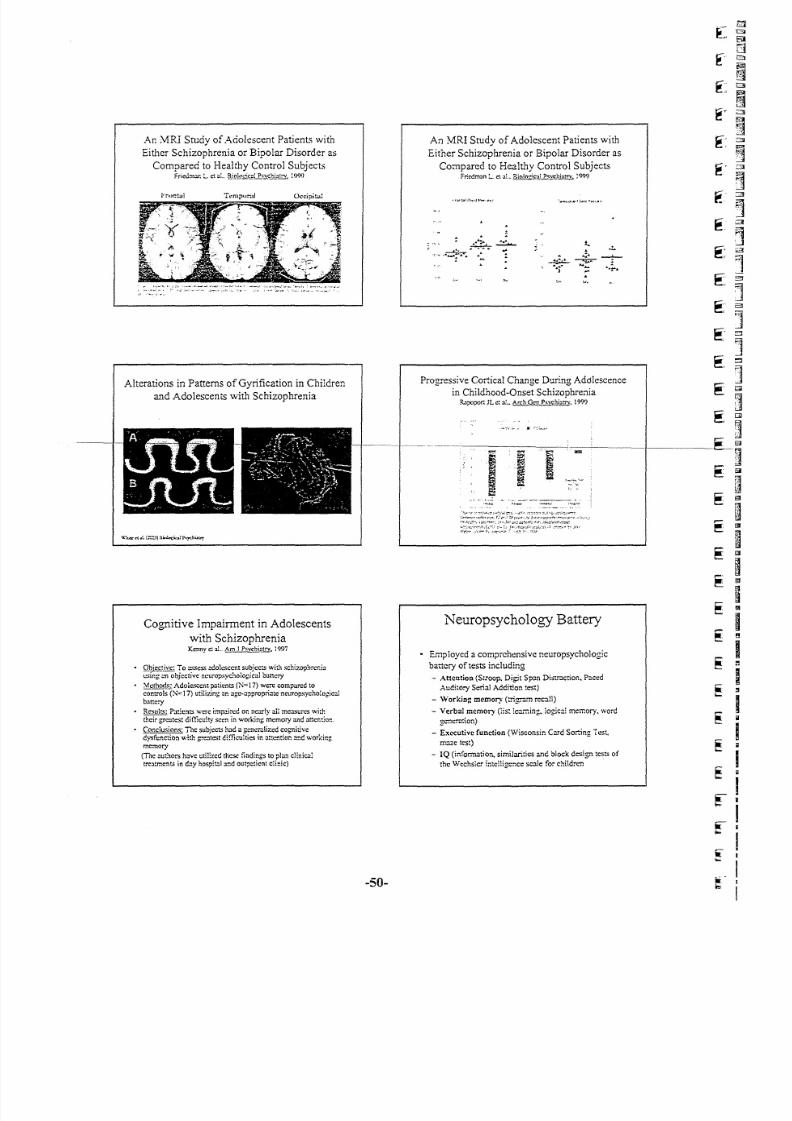
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 48/90
An MRl Study of Adolescent Patients with
Either Schizophrenia or Bipolar Disorder as
Compared to Healthy Control Subject,
F r i C \ .l : n ;t r . L ct c!.. B _ i £ l J . 0 : :i ~ ! P ~ ' . ! !. c . 1 i. : .1 ! ! Y .: ' ) ( } ( '
Alterations in Patterns of Gyrification in Children
and Adolescents with Schizophrenia
Cognitive Impairment in Adolescents
with SchizophreniaKenny ct al.. Am.l P~}:c..hl~!r.Y.1997
Q l J l r ; _ C J 1 V C : To assess adolescent subjects wi~h schizophrenicl ! S i n g en objective neuropsychological battery
~-;; Adole sc ent patie nts (N~ 17)were compa re d 10controls (N~~17)utilizing en age-appropriate neuropsychological
battery
R~lJlf$: P a th : :l ts w e r e impaired o n n e ar ly all measures v...i:h
th eir g re ate st d iffic uh y se en in working memory a.,d attention.
C o nc lu sio ns : T he subjects h : Jd a generelized cogni tive
dysfunction with g r ea te s t d i f f ic u l t ie s i n a !! C !1 :: o n z n d. w o rk i ng .
memo r y
(The authors have t.•tilized t he se f in di ng s t o p la n clinicaltreatments in day hcspital !t.~dcutpcticnt cl inic)
-50-
An MRI Study of Adolescent Patients with
Either Schizophrenia or Bipolar Disorder as
Compared to Healthy Control SubjectsF riedm an :._ tlal., RiQ!o ~·;~~ .?Lf2;; .~..r .J:!!!: .y~: QQ< )
Progressive Cortical Change During Adolescence
in Childhood-Onset SchizophreniaRapopo r t JL c: al.• 8!:£h.Q_~~Qj:1;"'. 1999
Neuropsychology Battery
• Employed a comprehensive neuropsychologic
battery of tests including
- Atten tion (St roop. Digi t Span Dist ract ion, Paced
Auditory Seria l Addition test)
- Working memory (trigram recall)
- Verba l memory (lis; l earning, logic al memory. word
g c " . .neration)
- Exe cutive func tion (Wisconsin Card Sorting Test,
maze test)
- IQ (informati on. similarities a nd block design tests of
the Wechsler intelligence scale for children

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 49/90
WORKING ME:'>IORY
"V('ch~cr Tower o r London BRrEF Workin:,:
Workin;: ;\tem. Test :\1cmory Sc",1('
Figuro 1_EXJmplc of !i"..::lbloworxi~ memory c c r l e i : : : : . in
a do le sc en t p C) ~ ic n~ with sc.'11zophrcniorS?<!CO.r.Jrr.eo~cmlo i ' . s
Antipsychotics in Teens
Schizophrenia Treatment: Bridging Science
to Clinical Care
Neuropsychiatric Measures
• Studies illustrate the similarity of adolescent
to adult forms of the illness and point to the
need for engaging treatment
• The neuropsychological tests also illustrate
the pathophysiology of the illness and may
be carefully used in treatment planning
-51-
Neurocognitive functioning and clinical status
during the first year of treatment in
adolescent-onset psychosis.Wozn~k_'; r:t, W!"Jto. ;,J . Jensen ••L . 61oc:k. . E . . Guim; )r .}C! ;. A . Loi ::cn , w,. So
Sc:.'utz. S C (2006c Fcbr.:ary).
Overview
• Males ::md1crr~lc~. 3SCSi2 - ,7• S chi zo p hr cni fO t r. " l. S c ." ' I. : ;o ;:m ro nt ; l_ & SChlZoOlH'Cct!VC
• Exc l~ : ;i o :, :s : iQ < 7 0 . n cu ro lo gi c: :1 d ls -o re c r o r i nj ur y" c o ne it io n 3 ~CC " J: 1g or ai n.
POD, oeO. suestaocc ceosc• W ' .. :J jo r it yo f p .: lt ie n ts w e re o n a ty pi co l o :m u ps yc ", ot ic m e ci cn e s
• E nro l:cC , n = 3 0; T we lv e m o nt !' : f o! :o w . .u p, n = ~C
M:lin finding:!; wore:
h C og ni tiv c d ofi cits o f o b ov t , S O w er e e vid en t a t b as elin e i n m a rr y ~ or n. Jln s
. . A ! !. ~ouSh symp tom! ; ! lu c " '. . .. :. a t( . oCo ve r 1 0i lo w. .y p o ne , g on er al ly . i mp ro ve d ~ y o ne
yC3~wi!.~ t . " 'Oat rnc r. : . , cogni tivc func tioning wa s Quite sbblco
• T he re w as n o s :. ;b s: an ti al c V. .c !o :" '. eoo t e : cC : !' ~ nCY .imt> ro vcmc :\ ! i n mos : O:"COS
o ! cogn i ti ve ! u :" IC "j o nin 9o
Prt:!.CnUJc 0. : me $J'cr.nutlltlir.:or W o rk :; ho p o n S ch i: op hf 'C fl iu R C :; l' Jl Jf Ch , D :w o :: .
SwrlZI) I'1:, r , (J,
P RO CES SJ :- 1G S PEED
W<'dnJC'rPrO(~, SlroopColor COWAl"f luctJ(y
Spc:1:'d fl ldcx Naminc
Figure 2. Examplo o!s t. :J b :C d e f ic it s i n p ro c es s in g s pe e d I n
adole scen t ~ t icn ts w i t. ~ se .~ l ;: !O i 'h ron ia~s ;: >o c: r tom condi ti o ns
{b::lSCli r:o :md 12 mont: l (tT..l shO'Nn)
Duration of Psychosis and Outcome
in First-Episode Schizophrenia
• Severity of'first-episode patients was followed for
three years to examine the impact of length of
illness on outcome
• Duration of psychotic symptoms was related to
time of remission (p=0.03) and level of remission
(1'=0.0])" Prodrome was also related to level of
remission ( ; r O c O O O } ) .
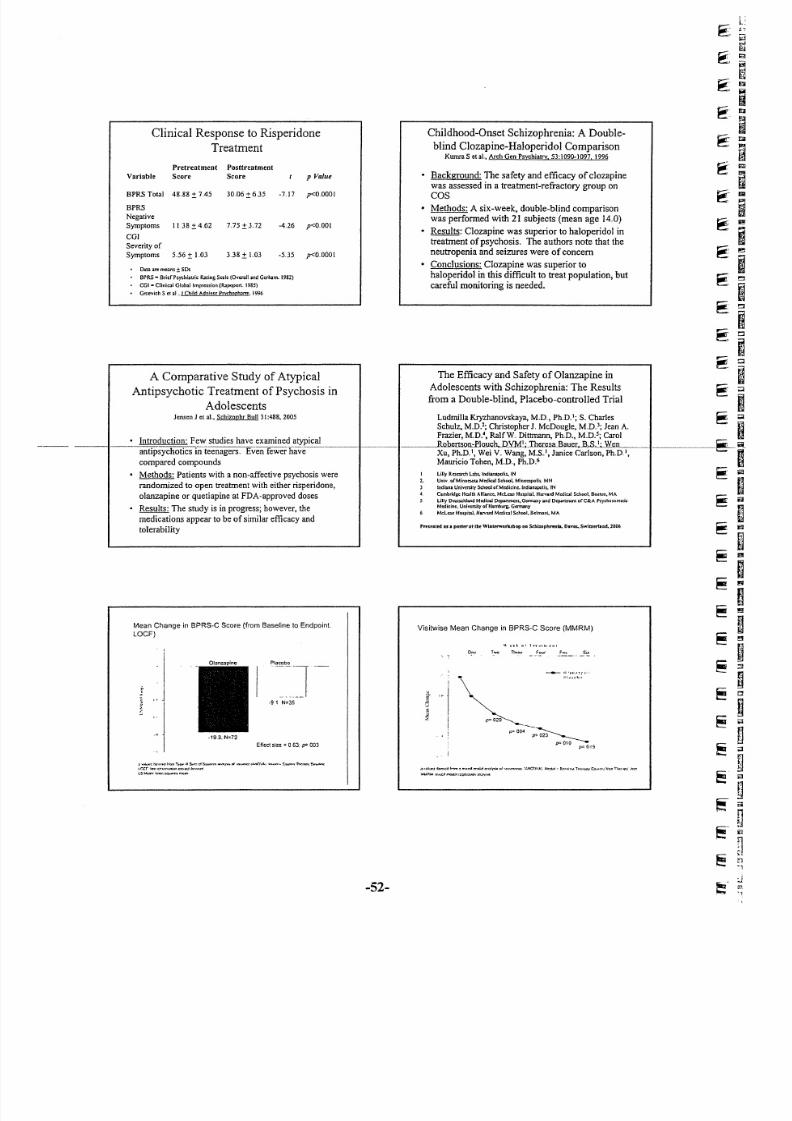
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 50/90
C linica l R espo nse to R isperido ne
Trea tmen t
Pretreatment Postt reatment
Variable Score Score p Value
BPRS Total 48,88 ± 745 30.06 ± 6.35 -7J7 p<MOOI
BPRS
Negative
Symptoms 1138 ± 4..62 V5±3,72 -4.26 p<O,OOI
COl
Severity of
Symptoms 556 ± L03 338 ± L03 -5..35 p<0.0001
[hw;uemeans;tSDs
BrRS" Bri c: rp sy th ia tr ic Rat ing S ca le [Over af and Gcrbam. 1982)
CGI" Clinic:J! Glohallmpress ion [Rapoport, 1985)
G rcev ieh S e t al , J Child Adolesc Psvchoph:mn, 1996
Childhood-Onset Schizophrenia: A Double-
blind Clozapine-Haloperidol ComparisonKumra Set at, Arch Goo Psychiatry 53:1090-1097, 1996
B ac kg ro un d: T he sa fe ty a nd e ff ic ac y o f c lo za pin ew as a sse sse d in a t re at m en t-re fra ct ory g ro up o n
COS
• M et ho ds: A six -w ee k, d ou bl e-b lin d c om p ariso nw as pe rfo rm ed w ith 21 su bje cts (m ea n a ge 1 4,0)
R esu lt s: C lo za pin e w as su pe rio r t o h al op erid ol intre atm ent o f psycho sis. T he a utho rs no te tha t the
n eu tro pe nia a nd se iz ure s w ere o f c on ce rn
• C onclu sio ns: C lo za pine w as su pe rio r to
h al op erid ol in t his d if fic ul t t o t re at p op ul at io n, b utc ar ef ul m o n it o ri ng i s n ee de d.
A Com para tiv e S tudy o f A typica l T he E ff icacy and Safe ty o f O lanzapine in
A ntipsycho tic T rea tm ent o f P sycho sis inA do le sce nts w ith S chizo phre nia : T he R esu lts
Adolescen tsfro m a D ouble-b lind, P lacebo -co ntro lled T ria l
Je nse n J et at, Schizophr Bull 31:488, 2005 Ludmi l laK ryzhanovskaya ,M.D . ,Ph ,D . I ;S . Char lesSchu lz ,M .D .2 ;Clu i s topher r, McDoug l e ,M .D . ) ; J e anA .
· I nt ro d u ct io n : F ew s tu d ie s h a ve e x am in e d a t yp ic a lF r a zi e r,M .D . ', Ra l fW . D i t tmann,Ph .D .,M .D . 5 ;Ca ro lRQb.er tson:Elo_u(;h,j ) .YM~;J1Jl: r_esa_Bau,et,J l,S.~;W ~ I 1__ _
antipsychotics in - t een age r s, E v en f ewe r h av e- -- -- -· Xu , P h .D .I, W e i v . .W ang ,M .S .I , J a ni c eCa r l son , P h .D .I ,c omp ar ed c omp o un ds Mau r ic i oToh en ,M .D . , P h .D . '
·Me t ho d s: P a t ie n ts w i th a n o n- af fe c ti v e p sy ch o si s w e re I Lil ly R e se n n: h 1 . .c l l~ I n di a na p ol is ., I N
r an dom i z ed t o o p e n t re a tm e n t w i th e it he r r is pe ri do n e ,2- U n iv , o r M in n es o ta M e di ca l S c ho o l. , M in n c: tp O li ~ . M N
J I nd ia nf l U n iv e rs it y S ch oo l o r M e di ci ne . l nd ia na po li s. . T N
o l a nz a pi ne o r q u et ia p in e a t FDA - ap pr o v ed d o se s, C ll tt lb r id g e H e al th A l li an c e, M c Le an H a s: pi ~ ~ H l I J " V a r o M c rJ ic al S c ho o l, B o st o n, M A
s l.illy D e ut sc hl an d M e di ca ! D e pa nm a u. G=y a nd D tp .l lr tm en l o f C & A Psydloromalic
· R e su lt s: T h e s tu dy i s i n p ro g re ss ; h owe v er , t he M e di ci ne , U n iv e rs it y o ( H am b ur g. G e rm a ny
• M cL C 2I l H o sp it aL H a rv ar d M ed ic al S ch oo l. B el mc ru , M A
me di ca ti on s a pp ea r t o b e o f s im i la r e ff ic ac y a nd
tolerabi li ty Prc'U'Oled U. pester-at Ibe Wiluuworlubop all Scbizophrmls. DIVOt. .Swlturlud. 2006
Mean Change in BPRS-C Score (from Baseline 10Endpoint
LOCF)
i
,. J · 91 N=35
E f fe ct s iz e = 0 6 3; p= 003
, t _ _ ~'IM! r " , , , , T~IM"" 5 ." ,, :: 1 ~" '" _ . .." " 01 ',,,,,,,",,,,,,,r.tK!'JJ., ''''''''~ ~"~ . ' " ' ie.W' ' ' ' 'Incr 1:n '~~""" ;n ; ." ,c. , ,ICI ' I In<wu"l5 I.letn,I.._1 '''''.If?1.mU'n
Visitwise Mean Change in BPRS-C Score (MMRM)
_O"'"'~r'''I' I~~~""
-.. . . . . . . . . , _p=004 -~
IF 023 '__..___
p=010 -..p= ors
,>..:I~:IlmIId!""" ~t n : > " " I I Y . l < k t " " I . ' I ' , . . . . . . Co! · .o.=~"a,' :;. .IICrJI.'''':. M e tI e< ' n., .~!"", lim:. !», CD.~~'[V<:, !ll:"",op,. 11::11
lootl.mu. ""u;rlrncodo."1'~~~'r~
-52-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 51/90
Mean Changes in Secondary Efficacy Measures (from Baselineto Endpoint, LOCF)
Efficacy MeasureOlanz..apinc Placebo
(n=721 (n=35)PANSS·
Total" ·213 -8.6
Pcs luve ' -65 ·27
Negative~ ·38 ·18
CG1-S . " ·05
CGt·I~· 27 38
OAS
Tolal ., 0 ·01
Verbal Aggression ·05 ·02
Physical Aggress ion Toward-03 -02
Objects
Physica l Aggress ion Towards Sel l 01 01
Physical Aggress ion Toward Others ·0.2 01
005
002
08,
004
< 001
OS,
163
256
053
.019
Antipsychotics in Teens
Schizophrenia Treatment: Bridging Science
to Clinical CareMedication Treatment
Studies are beginning to emerge about medication
treatment in adolescent schizophrenia patients, but isstill amazingly thin considering the magnitude of the
problem
Comparison studies that may inform management arejust now being reported
Questions sti ll to be addressed include: I) What is the
best dosing strategy? 2) Are side-effects different in
teenagers? 3) What is a reasonable algorithm to
manage treatment resistance?
Family Issues in Programmatic Treatment of
Adolescent Schizophrenia Schizophrenia
• Confusion in early attempts to help• As more patients are treated in an ambulatory
setting, a multidisciplinary team approach is
useful-_...
• Shock and denial during early treatment ..··Proven psych-o'soci1l1itl1erventiCfrfs-to-forestall
relapse include
- Family psychoeducation
• Concern about medication and side effects - Social Skills Training Program
• Proven psychosocial programs that improve
• Special needs in psychoeducation andoutcomes and further reduce symptoms
- Cognitive Rehabilitationsupport
._ Cognitive Behavior Therapy
TrP« II! S",.,ol s.""" ....""~, ...., ...1eo-.;,:",nc..c I..NC~VI.r: IAo:It.1. C,M'J:tt n""JIITtLonw.Of
~ .1 ' : 0 ' > 1 - 1 )Q~'M:; WII!\t:cll'. b 'n !. .t . .. ~ " ,, :" :! J: .ooc ln : ~~u", . .
. " ' ' ' '' ' '~1.:nr l~ '' ' ' ''
-53-

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 52/90
AstraZeneca
Resu lts Upda te
David Brennan
August 3rd, 2005
Overview of 1H Resulis
US Market Update
Seroquel®
Crestor®
Nexium®
Future
;/';
2 ,AE~traZt:::neca(2
1

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 53/90
AstraZeneca
S econd Q u arter and H alf Y earResults
In order to utilize the 'Sat e Harbor' prov isions ct the United States Private
Securit ies Lit igation Ref onn / let ct1995, AstraZena:;a is providing the
f allowing cautionary steternert. This presentation contains forward-looking
statements with respect to thef inancial condit ion, resul ts o f operations and
businesses o f AstraZeneca By their nature, forward-looking statemerts and
f orecasts irv oive risk and uncertainty because they relate to e-; ents and
depend on circumstances that will occur in the future. There are a number o f
fectors that could cause ectual results and developrnerts to differ materialty
f rom that expressed or implied by thesef orward-Iooking statements. These
f octo IS include, among other things, the loss or expiration o f patents,
marketing exclusivity or trade manes: exchange ratef luctuations; the risk that
R&D will not yield new products that achieve commercial success; the impact
of competition; price cortrcls and prce reductions; taxation risks; the risk ctsubstartial product liabil ity claims; the impsct o f any failure by third parties to
supply materials or services; the risk ct delay to new product launches; the
difficutties o f obtaining and maintaining gov ernmental approv as for products;
and the risk o f erwironmentalliabilities.
2

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 54/90
2005 2004 Actua l CER
___jm_-~ $m growth growth
Sales 6,132 5,288 +16% +13%
Opera ting pro fit 1,718 1,052 +63% +53%
EPS $0.75 $0.48 +55% +400/0
2005 2004 Actua l CER$m $m growth growth
Sales 11,875 10,362 +15% +12%
Operating profit 3,171 2,104 +51% +44%
EPS $1.38 $0.95 +45% +37%
Dividends $0.38 $0.295 +29%
Share repurchase $1,182m $968m
I'
6 AstraZenec.;{.2
3

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 55/90
Actualgrowth
+15%
CERgrowth
+12%Sales
2005
$m
11,875
2004
$m
10,362
-----,--,-----'"----,-~-- .. --~--~-,--North America 5,731 5,016 +'14% +13%
Europe 4,362 3,803 +15% +8'/0
Japan 736 666 +11% +9%
Rest of World 1,046 877 + 1 g o lo +'15%,.
i),
7 l\straZenec.:{";?
i/O:;
8 ,AstraZe:neca'_Z
4
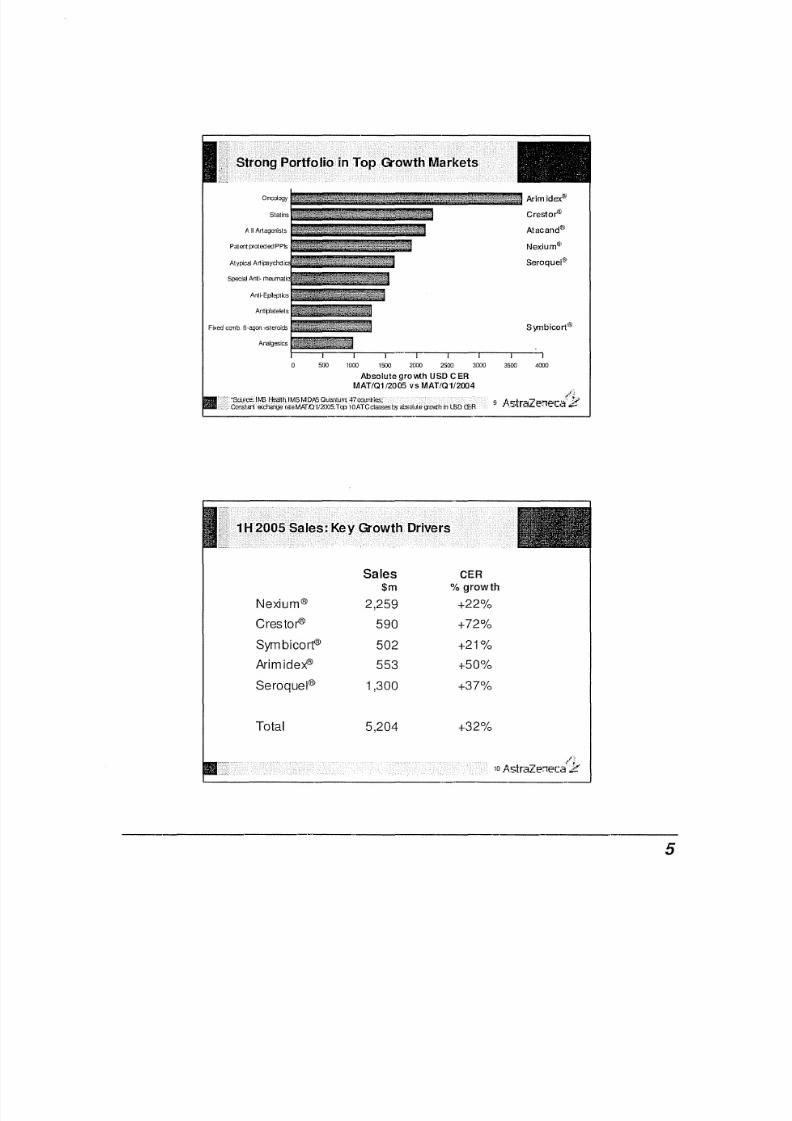
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 56/90
o n c ~ o I : o g yIIIF'--Arimid
ex
Qi1Statins Crestot'"'
Atacand"
P at en t p ro te de d P P S Nexium®
Seroquel'fl1
F ix ed c on b B -a go n + st er oi ds Symbicort®
Analgesics
o 500 1000 1500 2000 2500 3000 3500 4000
Absolute gro v.th USD C ER
MAT/01 /2005 vs MAT/01/2004
Sales CER
$m % growth
Nexium® 2,259 +22%
Crestor" 590 +72%
Symbicort® 502 +21%
Arirnidex" 553 +50%
Seroquel® 1,300 +37%
Total 5,204 +32%
I~
10 AstraZeTlec.:{2
5

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 57/90
Launch ofCrestor®
:; ;20%
'"> -(;
" 15%a,
~.c;
" § :Ie 10%C J
f-
~5%
------
------------,--,~-----------------------------
" ,~PnIQseClli·· .
Expiry
-- Total Sales - M I l . T Growth - R&D/ SG&A - M I l . T Growth
'S t rong ea rn ings growth : +37% CER
'M a r gin : 2 6.7% o f s ale s; f - ~
12 , . o , s t r a Z e i f l e c , : : : t J r
6

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 58/90
AstraZeneca
Results Update
David Brennan
August 3rd, 2005
AstraZeneca
US Business Update
Tony Zook
August 3rd, 2005
7

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 59/90
2004 US Pharma Mcrket Exceeded $2358
$250Market Value +7%
4.0
3.8
$200_ _ _ _ - - -
3.6
~$ ~pre,aiPIIO"' 3.4 ~
$150 +4% 3.2 ' I i . -
~ B ~3.0 Cl e :
ID TRx 0 :: \9 .
O J $100 2.8 !
2.6e
$50Dollar market growth for
2.4
2005 forecasted to be2.2
7.5% to 8.5%$0 2.0
2000 2001 2002 2003 2004 2005
Com petition for Share of Voice greater than ever
Medicare Prescription Benefit: $270 billion over 10 years
Renewed emphasis on safety
Challenges with approvals timing
Clinical trials expense
Increasing managed care influence on patients/co-pays
Pharma reputation crisis
OTCs and generics playing a greater role
,t)'
16 /lstraZeneca .2
------------------------, ..~--8

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 60/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 61/90
CustomerIn fo r ma t i on
AZPhmrnceuti:al
Sales Speciaists
·1 1 miilioo detaHSffnonth
-650,000 calls/month
• I nt eg r a t ed sales
r ep or t s up p or ti n g
Operations,P e rf or m a ne e &
Communicat ions
• S tr at eg ic T ar ge ti ng P la n• Co ll ab o ra ti o n & Pre-Call
P I an ni n g t oo l s
a AZ ranks 6th in sales force size but 5th in
total sales
37% increase in Sales per Rep
AZ was ranked 1st or 2rd for all activities
with GEs
AZ improved with Cardiologists, moving
from 6th to 3rd in rating rank for
Traditional Details and Samples,
remained at 3rdfor Meetings and
Events, and improved from 511 to 3rdforDisease-State Management Programs
2004 2002
Detail
AZ Effe ctivenes s
O""'all < I 5
Anesth esiology 6 7
Cardiology 3 ii
GE 1 1
GPIFPlOO 5 6
GS i 5 5
1M 4 -stoeu,ology - . .Oncology 2 6
Pediatrics 10 7
Psychiatry 6 -7
Pulmonology 7 4
10

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 62/90
Pfizer Pfizer
GSK GSK2
Merck3 Sancf i .Aventis
4 Sanoti-Avents
hJovartis PfizerForest
l?
21 r,,"straZe.'1en:/k
11

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 63/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 64/90
Market
~ US Sales Grov.th Share Cap SBili
Total Mar l<et"""$24"3' ~% -roo%
Pfizer$30 -2% 12% $205
2 GSK $19 2% 8% $136
3J&J $16 3% 7% $193
4 Merck $15 0% 6% $68
5 $12 15~ti 5° 1 $68AstraZ ene ca '0
6 Novartis$11 9% 5% $111
7 Sanoti-Avantls $11 13% 4% $114
8
Arrqsn
$11 26% 4% $75
9 BMS $9 -10% 4% $49
10 W)-€th $8 6% 3% $60
lr
25 l 'l,straZel1ec.::{ ..I2 '
5.6% 176%
+3.7 $2.3827.0% 25%
$379M31.6% +8.4 41%
28.5% +2.3 $4.18 12%
$1.3828.5% +1.3 15%
13

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 65/90
Nexium'": 1H sales $2,259m, up 22%
US sales$1,514m, up 18%
Other markets $745m, up 28%
Crestor": 1H sales $590m, up 72%
US sales $338m, up 83%
Other markets $252m, up 57%
Sercquel": 1H sales $1 ,300m, up 37%
US sales $933m, up 34%
Other markets $367m, up 44%
Tamox ifen con tin ues to dec lin e80%
70% -------_________ Strong volume growth60% _____ - - _50% ~amOxifen47.2%
40%
Arlmldex" 31.6%
~~~~
2 0 " / . , ' " " t 1 T . . 'e-,1".t.-t:£r"-at"'-a; I I< ' --
~ -~--,--'--..-10% ---
1-------
30%
0%
~ MM M
C 0 0 0- c
;~
c." 0<
M
ogo
o
l:o
.,-;It. A r i mi c e x Aromasin _,_ F em ara ._. ..- - NolvadexlT amoxf fen ,.28 ,Jl.straZeneca',E
14

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 66/90
40%
30Cl/o
@
J 'lif)
K
20%~~I-
10%
Atenolol = 34.4%
1 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - , - - - -
-4- Topro ~XL
-- Propanolol
M3top rolo I Tenormin _. Atenolo I
Coreg -- Innopran X L ,_ An Others
Drive key brand growth
Foster deeper customer relationships
Continued focus on execution and marketing excellence
Continuation of cost containment initiatives and rigorousevaluation of investment decisions
;1.';
30 ..-"straZerrec.:{E
15

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 67/90
Tony Zook
August 3rd, 2005
AstraZeneca
US Business Update
Johan Hoegstedt
August 3rd, 2005
AstraZeneca
16
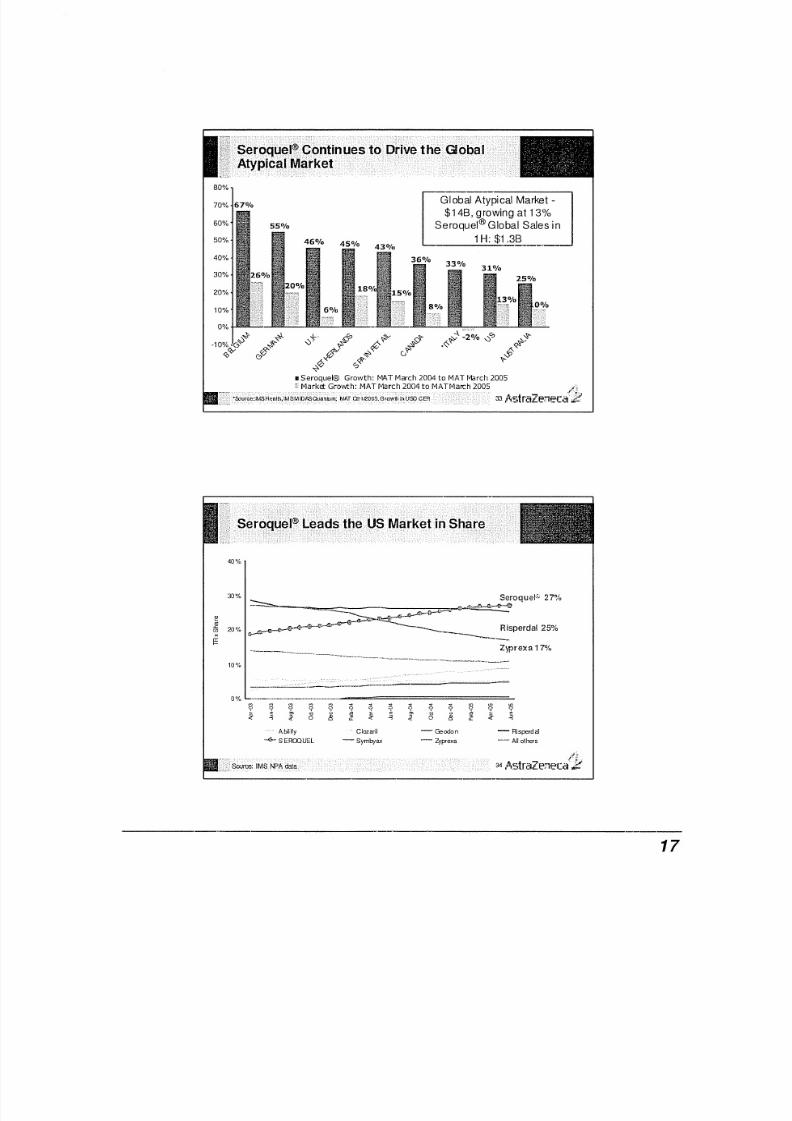
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 68/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 69/90
6.0% -e-vro Actual
3.5%
5.3%
il!
\\ 2 %, ~ ~ %
5.3%
/ - s :4.10
Market growth opportunities:
·PCP education on diagnosingBipolar Mania
·Increasing patient corrplianceon prescriptions
5.5%
5.0%
4.5%
4.0%
3.0% +---r---,.--...----r---.---.----...---..---,.---.--.---,----.
Jan Feb Mar Apr May Jun Jul ALg Sep Oct Nov Dec
2004 = 82%i-I
35 l'l,straZe:teca'~k
35%
30%
25%
> 20%0(/)
~ 15%
10%
5%
0%
~SEFOalEL
_" Z YP REX A'Z YD to
-GEODON
--- SY MB YAX -- R ts PE RD ALIM ·T AB tC ON STA
CLOZARIL - AB IUFY
- ALLOTHEA
/~'c36 ,l\straZenecaZ
18
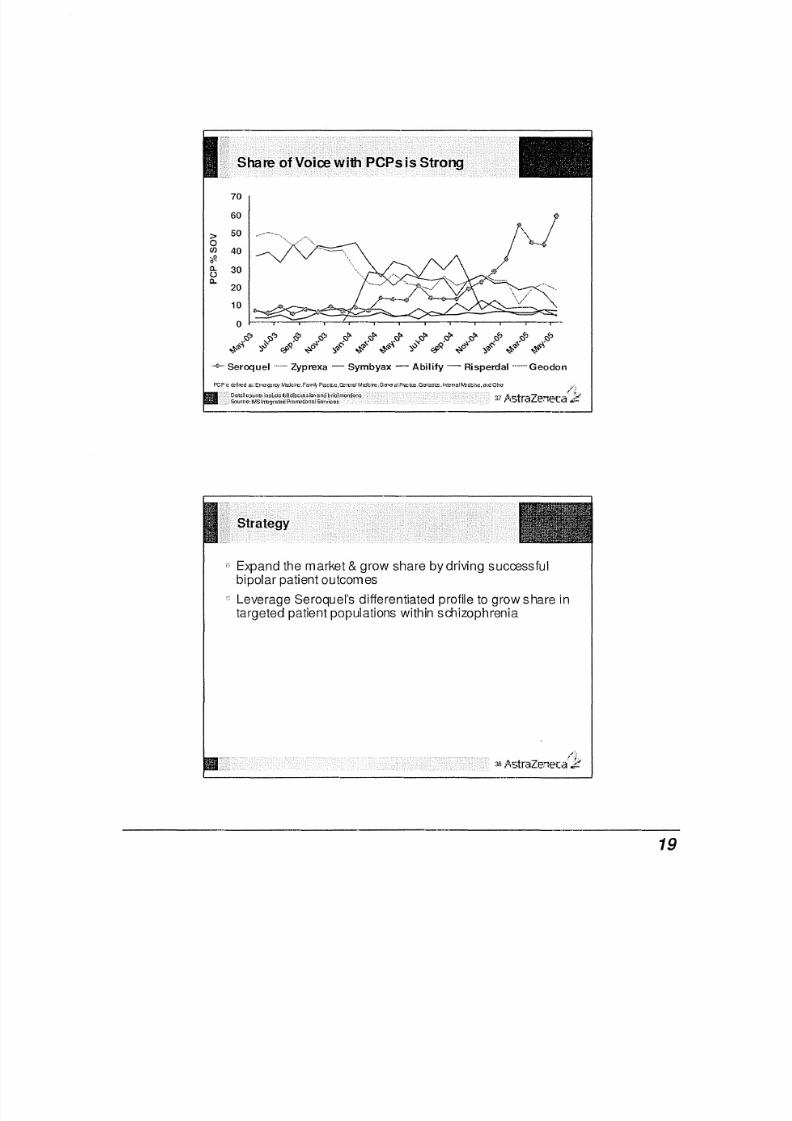
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 70/90
70
60
.;J> 500C/) 40~0
a. 30Ua. ~.-20
10
0
.+..Seroquel Zyprexa - Symbyax - Ability - Risperdal Geodon
pcp is cafmd e s : E rn O 'g :l n: y M o :I ci re . F ami ~' Placito, ( ?a mr a! M wc ir e, G mc ra ! P nc tc e. Ge la uc s , lntena! ~.-bdche,md one
Expand the market & grow share by driving successfulbipolar patient outcomes
Leverage Seroquel's differentiated profile to grow share intargeted patient populations within sdlizophrenia
"";
38 , A s t r a Z e l 1 E ' c . : : r / . 1 ?
19

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 71/90
CAFE: Results presented at the 8th World Congress of Biological
Psychiatry (WCBP) in Vienna, Austria
QUAI=tIZ; ..Re suits presented in May at American Psychiatric
Association convention (APA)
BOLDER: Results presented in May at American Psychiatric
Association convention (APA) and Bolder I study published in JulyAmerican Journal of Psychiatry
Bolder II studyin bipolar depression has finishedrecrui1ment
US submission around year end
Sustained Release for schizophrenia - on track for 1H 06global submission
Other brand enhancing LCM opportunities
/-'{
40 AstraZenecaZ
20

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 72/90
Large and Grow ing Class Best in Class Profile
LCM
AstraZeneca
Johan Hoegstedt
August 3rd, 2005
21
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 73/90
AstraZeneca
Adele Gulfo
August 3rd, 2005
Statin Market Overview
Crestor" Performance & Strategic Positioning
Recent Events/Efforts
22

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 74/90
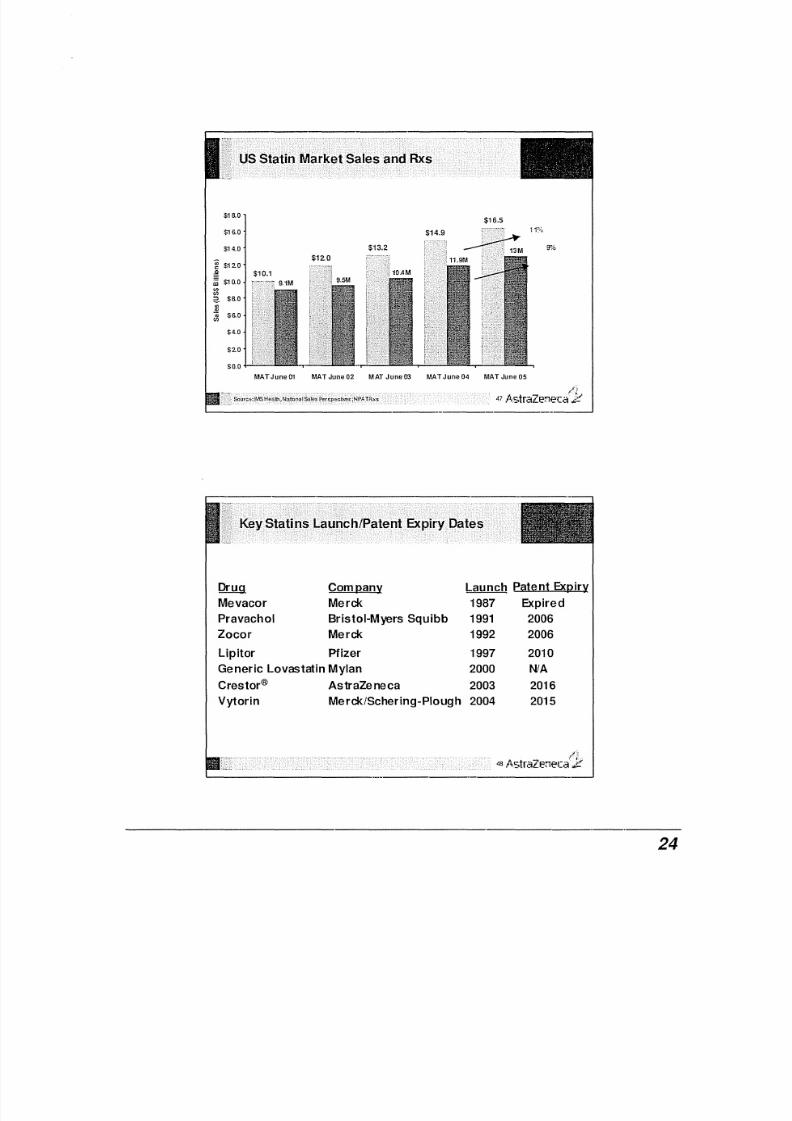
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 75/90
$16.0$16.5
$16.0
$14.0 fp,~
~ $120
a~ $10.0
'"en:: ? $6.0
s
' "$6.0
en
$4.0
$20
$0.0
MATJune01 MAT June02 MATJune03 MATJune04 MAT June05
/1
47 ,.'I,straZel1eca l:i
Drug Company Launch P5:!l~nt ExRiry
Mevacor Merck 1987 Expired
Pravachol Bristol-Myers Squibb 1991 2006
Zocor Merck 1992 2006
Lipitor Pfizer 1997 2010
Generic Lovastatin Mylan 2000 NlA
Crestor® AstraZeneca 2003 2016
Vytorin Merck/Schering-Plough 2004 2015
2 4

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 76/90
60,0%
40,0%
e<1 l.<:C/) 3O,!)'%.xa:z
20,0%
10,.0%
6,2%
0.0%'__ "M"_'", ..._" ..,~ ..__ . . . .------
M0
M M
~ ~ -e ~q q
~q q q q
~ ~ ~ ~ ~ ~ ~s 0 0 :;; s :; : :; : s :; : : ; ; : ; : 0 0 0 : ; ; : ;: ~ : ; ; : ; : s'" '" '" '" '" '"~ ~ ~ § S li ~ !1 ~ s s s :; ; ~ ~ § S li ~ :; :;; s
- Crestor .- Lipitor - Lovastatin -" •. Pr ava:;hoi - Zooor - Vytorin
;t i
49 A s t r a Z r ; :n e c . ; {1 ?
FD A Re~cts PC P e t it i o n
9%VloniSt'f'llrteHeOf~
B% -..- ~x Share
7%
Q)
~ 6%
s:
~ 5%
oI ii 4%
W
~ 3%
C re sb ' 2 00 0
. . . . . .,--.._..~M M M M . . . . ~
~. . . .~~ . . . . . . . . . . . . . . . .
:i l s :; ; s :i l : ; : s : i l : i l s s :i i:;; 2 i S li S li ~ :; :;; s s :i s :;; a- , f , : "
50 . A s t r a Z r : : n e c a " k
---------------------_._--------------
25
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 77/90
Label Update
Labeling rev isiors are a normal cccur rerce
3 minor changes to the prescribing informat ion
FDA Petition response
Renal prof ile can parable to other other marketed stat ins
Muscle toxici ty can parable to other marketed stat ins
Greater LDL-C effk:acy at lower doses increases the risk- benefit o f
Crestor"
3rd party
NLA review
Other independent safety reviews & real world effectiveness studies
51 .AstraZeneca
Hones t and s tra ightfo rwa rd tona lity
R isk inform ation as prom inent a s thebenefits
Educa tiona l condition in format ion
/~
52 .AstraZeneca ;;;f
26

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 78/90
9 Studies
Completed
15 Studies
Ongoing
>46,000
Patients
45
Countries
Statin market offers tremendous opportunity
Crestor" has experienced setbacks and weathered storms
The weight of evidence will continue to show a favorablebenefit-risk profile for Crestor"
Our commitment to Crestor? is undiminished
j';~
54 , ' '\straZcon€'ca'p
27

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 79/90
Adele Gulfo,
VP Primary Care
August 3rd, 2005
AstraZeneca
Linda Palczuk
Executive DirectorAugust 3rd, 2005
ASTraZeneca
US Nexiurrr'Update
28

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 80/90
Strong performance in 1H
us Sales up 18% to $1,514 million
US: positive share gains across all metrics
YTD June Total Rx + 13%'
YTD June Extended UnITs + 16%'
Nexium® passes Prevacid for #1 TRx spot*
NSAID opportunity
PPls represent $13 billion in sales**
~'~J
S7 AstraZem:ca',.B'
.i 30% ---------...-.
(f)
.~§
~ 20% _~-----------
~ ._.-~w
i{ 3 ! . 10%
40%
~ ~ ~ - - - ~ - - - - - - - - - - - - - - - - - - - - - - - - - --e -o
o
~o
~o
I~o
I-- Oneprazole
._ .- Z eg er id
- Prevacd Family_ ." Acipb e x
Prilosec
4t". Ne x u m
_ . . .. _ . P r ot o n ix F am ll y
!_'::
58 ,AstraZeneca{l?
29

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 81/90
40.0%
a :"-~ 30.0%
i' 5]Ili;
'" 20.0%
Nexium® = 28.54%
co
_-_~
_-.1It" __ G I II ;-~
Prell acid Family = 28.46%~ ----_._._._. _ _ •._ - _ . f
+ O . o s
%
+67
%
§~m
c: 10 .0~/"
'"'"
0.0%
~
2 ? 9-c ra
a. u rom mif) Cl
'"
a
a.mif)
, t ¥ _
59 ,'I,straZe:neca'.Je
:~E-' :::rRx:urut-l; t,i ies:==
::::::::==:::O.6t.05:=::.3:2::6'2t:::::===:40'/~
,,,~~,~,- . . . . ""'''- . . . .-,,.,"''----
~ ~ § ~ il ~ ~ ~ ~ ij I ~ ~ ~ ~ j ~ 5 ~ s; :8~~ ~ e 1 5
~ ~ ~;; ; 6 " is 5 ~ ~ ~
;; ~ ~ ~ S • ~0 s"s s s
" " " "-9-Nexium@ Omep r azo le P rev ac id F am il y
~ Pro ton ix Fami ly - Zeger t J
30 '10
20X
-"'--~~-lQ'/"
.. . _ ." " - • • • . _ . lO r .
" ' I .
~ ~ ~ ~ ~ ~Il ~ ~ to ~ ~E s s ~ ~ s
Aci""ex
Prilosec
t~
60 ,l\straZe;neca',k'
30

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 82/90
0303 0403 0104 0204 0304 0404 0105 0205
'.ll!1..Al;.t 'i lIl.A.cJ.
46%c:f'! l.eo
50%PPI ex-Ornep 11 ..2% 8.7
40% Nexium® 19.4% 15JP/o
30%
< t- 20%.c:
i 10%0
c !i 0%:::J
w -10%><
[f -20%
-30%··33%
·35%-40% ·40% -40%
-50%PPI 1I0meprazoie IIPPI ex-omep II Nexium
/';
61 , A < ; : 4 r a Z e n e c . : : h 8 '
40%
35%
30%
e25%
. ..c:
20%(J)
' < t -15%
10%
5%
0%,"
~ < $ ;> ~ < $ ;> < s > " > rfi' ~ \>
! ' : - 'V , , 0 . , " " , " " , . " " ~ " , , < s >
',j::i . . . . cf' < ! 'V '< ~ ....~< .
-1J- NEXIUM'IV ,,--- PRILOSEC
-PREVACIDFAMILY -ACIPHEX
,,_ .• ZE GER ID
- PROTONIXAV
- OMEPRAZOLE
J'
62 AstraZeneca'?
31

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 83/90

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 84/90
Nexium®I.V. approved March 31st
3rd I.V. entrant
Current Market Environment
Highly cornpetitve prcinq on LV.formulation
Contractuallirk between LV. and oralformulations
Nexium® IV/Hospital Strategy
Superior clinical prd ile of Nexiurr® LV.
Priced crmpettv ey
Capture spillov er benef it in retail segnent
(!
65 ,AstraZe!l€c.:t 2'
AstraZeneca
Linda Palczuk
August 3rd, 2005
33

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 85/90
AstraZeneca
The Road Ahead
Sustainable long-term growth enabled by:
Driving unique in-line brand opportunities
Improving operational effidency
Bring differentiated, superior products to market
Disciplined cost management and focus on productivity
Corporate reputation that speaks to identity
Enable a high performance culture
~;l
68 ,l\straZI:'::1eca'if
34

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 86/90
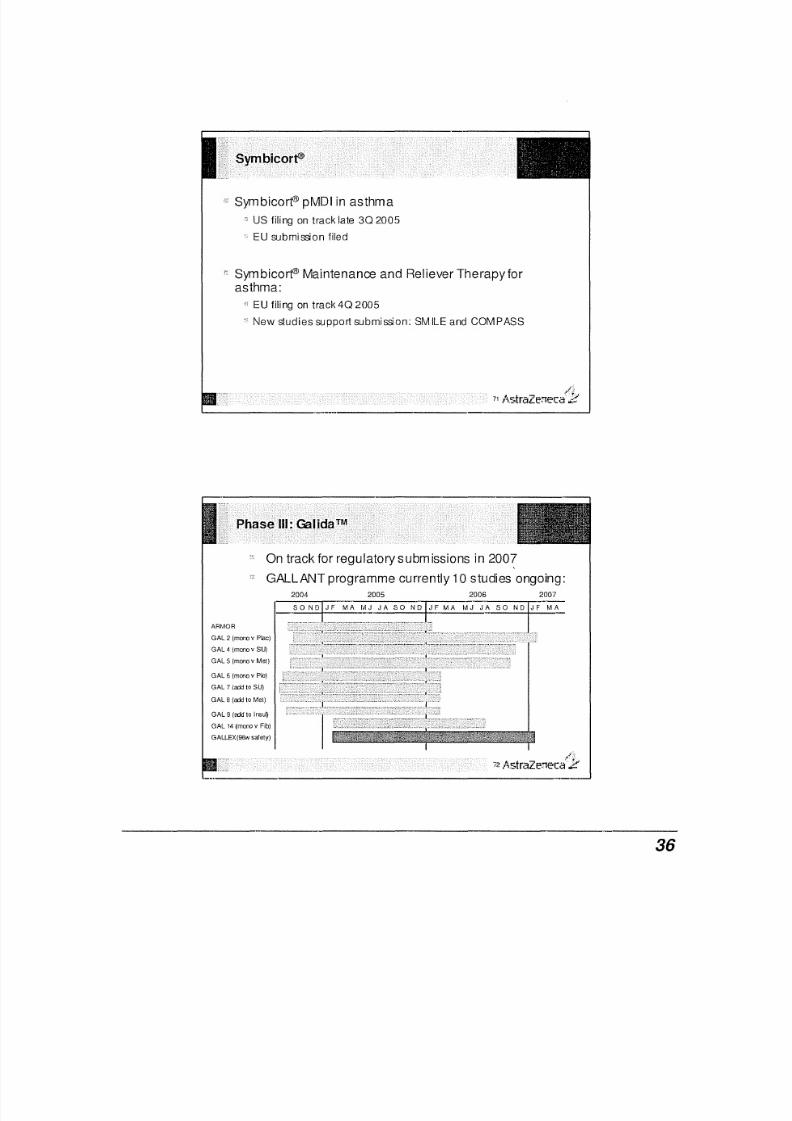
8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 87/90
Symbicorf" pMDI in asthma
us filing on track late 302005
EU submission filed
Sym blcort" Maintenance and Reliever Therapy forasthma:
EU filing on track 402005
New studies support submission: SMILE and COMPASS
On track for regulatory subm issions in 2007
GALLANT programme currently 10 studies ongoing:
2005 2006 20072004
ARMOR
GAL 2 (mono v Pac)
GAL 4 (monov SU)
GAL 5 (mono v Mel)
36

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 88/90
SAINT I first ever positive NeuroprotectantTrial
Significant reduction in disabil ity measured by
Modified Rankin Scale
Effect present
across 6 hour time window
across stroke severities
irrespecttve of r t-PA use
Neurological recovery end point not signif icant onpre-specified analysis
Excellent safety profil e - similar to placebo
~(~
73 AstraZenecaE
Inhibitor of VEGF and EGF signalling
Enters phase II I
Phase II data in NSCLC shows unprecedented anti-tumouractivity
" As monotherapy and in cornbinafion with chemolherapy
Thyroid cancer trials
Activity seen in RET mutated hereditary medullary thyroid cancer
All patients had at least 50% reduction in a key biomarker
(caldtonin)Completion of phase II meeting with FDA
/'~.;74 ,AstraZenec(iI,;;:
37

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 89/90
Pre-clinical Phase I
Phase "
Accelerated dlv elopment
New !l'edical EntitiesPhase tansition since Jan-05Line extensions
/_1
75 AstraZel1eCa'2
Biopharmaceuticals
AZD8593 for haemostasis
Monoclonal antibodies
Abgenix, CaT and AZD31 02
Development and discovery partnerships
Humanised antibodies for oncology, inflammatory andneurosdence disease areas
;I:
76 ,AstraZen€cat'2
38

8/7/2019 Schulz Exhibit 2
http://slidepdf.com/reader/full/schulz-exhibit-2 90/90