school nurse interventions to promote healthy...
TRANSCRIPT

health.mo.gov
School NurseInterventions toPromote HealthyWeight
Resource Guide
BACKGROUNDASSESSMENT AND REFFERALSWORKING WITH FAMILIESRESOURCES
Missouri Department of Health and Senior Services

School Nurse Interventions for Childhood Obesity 2
Acknowledgments
Adapted from Childhood Obesity: School Nurse Toolkit Developed by Rebecca Cartmill, MSN, RN
University of Missouri School of Nursing Capstone Project April 2014
School Nurse Toolkit: Student Overweight/Obesity
Iowa Department of Public Health Bureau of Nutrition and Health Promotion Nutrition and Physical Activity Program
Fall 2011
This resource manual was reviewed and revised based on valuable input from the following Missouri school nurses: Debra Cook, RN, Kennett School District
Katherine Park, MSN, RN, Parkway School District Barbara Brommelhorst, MSN, RN, Wentzville School District
Dianne Herndon, RN, Retired Patti Kamp, RN, Meadow Heights School District
Priscilla Dickerson, RN, Mt Vernon School District Pat Sturges, BSN, RN, Sedalia School District
Further input and recommendations were received from Ellen Barnidge, PhD, MPH, Saint Louis University and
Constance Brooks, PhD, PMHCNS-BC, PHCNS-BC, Retired University of Missouri–Columbia. Reviewers and Advisors: Stacey White MSN, RN, and her sons Dallas White, Jack White and Austin White
June 2015 Missouri Department of Health and Senior Services
Bureau of Community Health and Wellness health.mo.gov/schoolhealth
AN EQUAL OPPORTUNITY/AFFIRMATIVE ACTION EMPLOYER
Services provided on a nondiscriminatory basis.

School Nurse Interventions for Childhood Obesity 3
TABLE OF CONTENTS
INTRODUCTION 4 SECTION 1: BACKGROUND 5 Childhood Obesity Facts 5 Health Effects of Childhood Obesity 5
Definitions of Overweight and Obesity 6 Risk Factors 6 Prevention 7 SECTION 2: ASSESSMENT AND REFERRAL 8 Assessment 8
Protocols to Assure Privacy 8 Nurse/Student Conference 9 Referral 10 Opportunities for Prevention SECTION 3: WORKING WITH STUDENTS AND FAMILIES 12 Motivational Interviewing 12 Self-Reflection 12
Motivational Interviewing Principles 13 Signs of Readiness and Key Questions 16 Motivational Interviewing Algorithms 17
Types of Interviews 19 Sample Dialogue of a Brief Negotiation for Weight Management 21 Measuring Progress 23 SECTION 4: RESOURCES 24 Example BMI Percentile Chart for Boys 2-20 Years of Age 24 Example BMI Percentile Chart for Girls 2-20 Years of Age 25 Example of Plotting BMI on Percentile Chart 26 Screening Tool Blood Pressure Values Requiring Further Evaluation 27
Healthy Lifestyle Questionnaire 28 Sample Lifestyle Questions 29 Example of Weight Management Intervention Plan 30 Pediatric Weight Management Tips for Getting Started 32 Promoting Healthy Eating for Children and Adolescents 33 Promoting Physical Activity in Children and Adolescents 34 Sample Individualized Health Plan (IHP) 35
Internet Resources for School Nurses Addressing Overweight and Obesity 37
REFERENCES 42
School Nurse Interventions for Childhood Obesity 4
INTRODUCTION According to the World Health Organization (WHO, 2012), childhood obesity is one of the most significant health problems of the 21st century. The dramatic rise of childhood obesity and the serious health consequences associated with it cannot be overemphasized. Healthy People 2020 has identified nutrition and weight status as topic areas of concern and developed specific goals aimed at reducing the number of children and adolescents who are obese (U.S. Department of Health and Human Services [USDHHS], 2011). The Healthy People documents, issued in ten-year increments, are considered to be blueprints for addressing the nation’s health. The documents identify the most pressing health concerns for the coming decade and identify strategies to address them. Many are problems that can be addressed through early interventions in school settings. More than 95 percent of our children are enrolled in schools and are spending up to 13 years of their lives there. Schools and school nurses are in a key position to address this issue and advocate for children and adolescents who are, or are at risk, of becoming obese. This resource kit will:
Identify tools for assessment of the child and the school environment. Provide resources for the school nurse to educate and advocate for students who are
overweight or obese. Identify resources to promote healthy diet and physical activity habits in all children.
The school nurse can use this guide as a resource when looking for ways to assist students, who are overweight or obese, and their parents. School staff can be educated regarding their role in promoting healthy eating habits and increasing the level of physical activity in the school setting.

School Nurse Interventions for Childhood Obesity 5
SECTION 1: BACKGROUND
CHILDHOOD OBESITY FACTS Obesity is now the number one health concern among parents in the United States; it is more concerning to them than smoking or drug abuse.1 More than 12 million American children and adolescents (16.9 percent) are obese; and more than 23 million are either obese or overweight (31.8 percent).2 Overall, childhood obesity rates have tripled in the past 30 years. Based on 2011-2012 national data; 8.4 percent of 2-5 year olds, 17.7 percent of 6-11 year olds and 20.5 percent of 12-19 year olds were obese. While the national statistics are staggering, Missouri rates are equally alarming with 28 percent of 10-17 year olds being overweight or obese.3 Furthermore, the most at-risk for disease and disparity, Missouri’s low income 2-5 year olds, have a 12.9 percent rate of obesity.4 Research studies have consistently demonstrated that youth who are overweight or obese have substantially higher odds of remaining obese in adulthood. This sets up a potential lifetime of disease, diminished quality of life and disability; therefore, reversing this trend with effective obesity prevention strategies and evidence-based treatment services is critical to the health of our children. HEALTH EFFECTS OF CHILDHOOD OBESITY Childhood obesity has both immediate and long-term effects on health and well-being.
Immediate health effects include higher likelihood of having:
High blood pressure and high cholesterol, which are risk factors for cardiovascular disease. Seventy percent of obese youth had at least one risk factor for cardiovascular disease.
Pre-diabetes or a high risk for development of diabetes. Bone and joint problems. Breathing problems such as asthma and sleep apnea. Fatty liver disease, gallstones and gastro-esophageal reflux. Social and psychological problems.
Long-term health effects include:
More severe obesity as an adult if overweight as a child. Higher likelihood of having adult health problems such as heart disease, type 2
diabetes, stroke and osteoarthritis. Higher risk of being diagnosed with cancer, such as multiple myeloma and Hodgkin’s
lymphoma. Source: http://www.cdc.gov/obesity/childhood/basics.html

School Nurse Interventions for Childhood Obesity 6
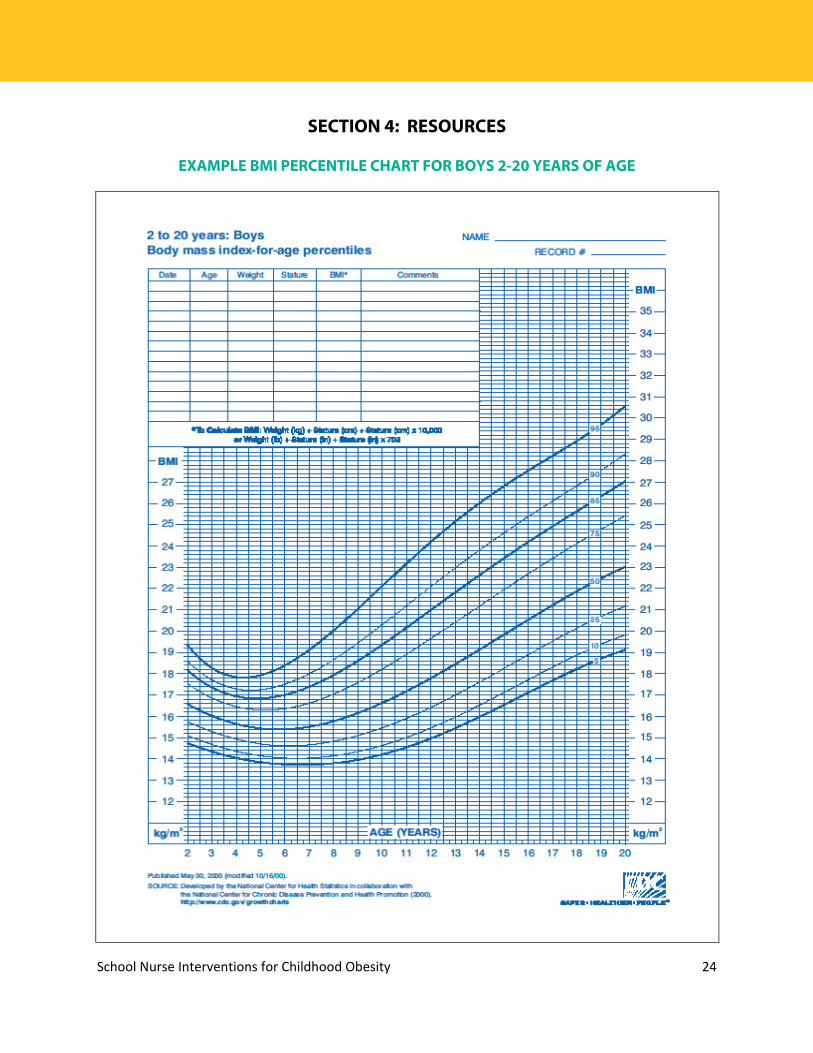
DEFINITION OF OVERWEIGHT AND OBESITY Body mass index (BMI) is a measure used to determine childhood overweight and obesity. It is calculated using a child's weight and height. BMI does not measure body fat directly, but it is a reasonable indicator of body fatness for most children and teens. A child's weight status is determined using an age- and sex-specific percentile for BMI rather than the BMI categories used for adults, because children's body composition varies as they age and varies between boys and girls. Centers for Disease Control and Prevention (CDC) Growth Charts are used to determine the corresponding BMI for age and sex percentile. For children and adolescents (2-19 years of age):
Overweight is defined as a BMI at or above the 85th percentile and lower than the 95th percentile for children of the same age and sex.
Obesity is defined as a BMI at or above the 95th percentile for children of the same age and sex.
Samples of the growth charts are included in the resource section. RISK FACTORS Childhood obesity is the result of eating too many calories and not getting enough physical activity. Many factors contribute to overweight/obesity; however, environmental factors and societal norms have made it difficult for most Missourians to practice behaviors that support a healthy weight. This section lists some of the potential factors that influence weight.
Childhood Lifestyle Factors o Not breastfed as an infant or weaned early on in the first year of life. o High intake of sugary drinks and other energy dense foods. o Low fruit and vegetable consumption. o More time spent on sedentary activities such as watching television, playing
video games and using interactive hand-held devices.
Family Influences and Parental Modeling o Children with two obese parents are 10 times more likely to become overweight
than children with no obese parents. o Prenatal environment, e.g. mother had gestational diabetes during pregnancy. o No/limited parental role modeling of a healthy diet and physically active lifestyle. o Lack of limits for screen time. o Lack of parenting behaviors that support a healthy weight, such as assuring
adequate sleep. o Frequent meals eaten out where portions are often “super-sized.”

School Nurse Interventions for Childhood Obesity 7
Community Influences o Poor access to affordable healthy foods, especially fruits and vegetables. o School and child care environments that do not support healthy eating and
physical activity. o Limited access to parks or sidewalks for walking, bike riding, and other active
play. o Unsafe neighborhoods that limit opportunity for outdoor physical activity. o Targeted marketing of foods high in sugar, fat and salt. o Increased portion sizes of less healthy foods and beverages.
PREVENTION The easiest way to manage obesity is to prevent it from happening in the first place. It is important for all children to hear prevention messages and experience environments that support healthy behaviors. Dietary and physical activity behaviors are influenced by medical care providers, faith-based institutions, government agencies, the media; and food, beverage and entertainment industries. However, schools play a particularly critical role by establishing a safe and supportive environment with policies and practices that support healthy behaviors and opportunities to learn about and practice healthy eating and physical activity. Source: Centers for Disease Control and Prevention (CDC), 2014
School Nurse Interventions for Childhood Obesity 8
SECTION 2: ASSESSMENT AND REFERRAL
There should be an assessment of weight status for every child entering the school system. The data may come from on-site measurement or reported from a health care provider. The BMI should be tracked using the appropriate body mass index-for-age and sex growth charts which can be found at: http://www.cdc.gov/growthcharts/charts.htm#Set1. Sample growth charts are also included on page 24 in the resource section. Students’ growth screening results are part of the health record and, should only be discussed with the student, their parent/guardian and health care providers with parent permission. The American Academy of Pediatrics recommends a yearly BMI screening for children 2 years of age and older, in conjunction with, a yearly physical exam with their private provider. They do not recommend these screenings at school due to limited resources to address the issue. If students are weighed and measured at school, the school nurse must have the time and resources to track and follow up on students whose BMI falls outside the norms for age and sex. PROTOCALS TO ASSURE PRIVACY The school nurse and other personnel engaged in assessing student weight must recognize the sensitive nature of the assessment, both to the student and his/her parent. Parents/guardians should be given prior notification of the assessment and the opportunity to decline the assessment. The notification should describe the purpose of the assessment (i.e., for surveillance [collecting aggregate data to demonstrate a problem] or for assessing individual health status). It should also assure parents/guardians that the assessment will be done in a private setting and that the data collected will be handled in a confidential manner. See sample parent letter in Growth Screening Guidelines, Missouri DHSS, 2005 at the link below. When assessing BMI, the screener must ensure:
Equipment has been properly maintained and calibrated. Adequate time is allowed for the screening. The assessment is done in a private setting. Confidentiality is assured in terms of sight and sound. Students are weighed and measured facing away from the scales to reduce anxiety. A standard procedure* is followed, with each student being weighed and measured
twice to ensure accuracy. Results are written down before the student steps away from the measuring device to
reduce errors in transcription. Recording measurements incorrectly is a common error that occurs in assessment of height and weight. Recording the information on paper ensures no one else hears the measurement.
*Procedure outlined in Growth Screening Guidelines, Missouri Department of Health and Senior Services, 2005, http://health.mo.gov/living/families/schoolhealth/pdf/GuidelinesForGrowth.pdf

School Nurse Interventions for Childhood Obesity 9
Following the assessment of height and weight, the nurse should calculate the student’s BMI using one of a variety of tools available (e.g., http://nccd.cdc.gov/dnpabmi/Calculator.aspx). The BMI and BMI percentile for age and sex should be recorded in the health record. BMI is only a screening tool, not a diagnostic tool. A child may have a high BMI for age and gender, but to determine if overweight is a problem, other assessments need to be performed. These assessments may include skin-fold thickness measurement, diet and physical activity evaluation, and family history. NURSE/STUDENT CONFERENCE Some students may wish to discuss their screening results with the school nurse. This discussion should be done in a space that respects the student’s privacy. As part of the assessment, the student’s nutritional status, eating habits and physical activity patterns should be routinely evaluated; along with identifying risk factors for overweight/obesity within the family. It is important to ask open-ended questions. The section on motivational interviewing may be helpful in structuring this discussion. A question to open the discussion might be:
“How do you feel about us discussing your physical activity, television watching and eating habits today?”
Next, follow up with more focused questions addressing both physical activity and eating habits. Some questions to consider include:
Physical Activity Questions • How many hours of television do you watch each day? • How many hours do you spend playing video games each day? • How often do you play outside? Is it safe to do so? • How often does your family do something active together? What might that
include? • How often does your parent play actively with you?
Nutrition Questions
• What does your family eat in a typical day? • Do you have breakfast? What do you usually eat for breakfast? • When eating at home, does your family routinely eat while watching the
television? • How often does your family eat out each week? • How often are fruits and vegetables served as part of your meals? • What do you eat for snacks? • How many sodas or sugary drinks do you drink each day?
See page 28 in the resource section for a simple, lifestyle questionnaire.

School Nurse Interventions for Childhood Obesity 10
REFERRAL With a baseline BMI, the nurse can determine if the child’s weight status is changing. A change in percentile may signal a developing problem and may warrant a referral to a health care provider for a medical evaluation that may include laboratory tests to identify any co-morbid conditions. The following students are candidates for a medical referral:
Student with a BMI >85 percent, with at least one of the following factors–family history of overweight/obesity, elevated blood pressure for age, or a large increase in BMI.
Student with a BMI >95 percent. Student with a rapid increase in BMI.
OPPORTUNITIES FOR PREVENTION It is helpful to structure the screening environment to communicate preventive care messages that focus on habits that support a healthy weight. This may include: Waiting Area
Display posters with positive nutrition and physical activity messages that reinforce the messages given during the assessment and private consultation. Posters are most effective when placed in areas where screening results will not be shared and placed at eye level of the intended reader.
Display materials that address a variety of different health topics and referral resources. Materials might include:
o Recipes for healthy foods. o A list of programs for overweight children. o Handouts focused on healthy eating and physical activity. o Tip sheets for families wanting to be more involved in their child’s diet and
activity choices. o A list of community sports and physical activity programs.
Consider having chairs without arms that can support a child, adolescent or family member of larger size or heavier weight.
School Nurse’s Office Every visit to the school nurse is an opportunity to convey health messages. Consider:
Creating themed rooms if multiple rooms are available. For example make a “healthy eating room” and a “physical activity room” with appropriate materials displayed in each.
Having handouts for students on key preventive health topics to provide at the end of each visit and to send home to share with parents.
Having armless chairs for students/parents who are a larger size or heavier weight.
School Nurse Interventions for Childhood Obesity 11
General School Environment The school environment should reflect the preventive health messages being provided during assessments and school nurse counseling visits. Some of these opportunities include:
Modeling of healthy weight, healthy eating and physical activity by all school staff. Avoiding the use of food as a reward. Stocking vending machines with water, 100% fruit juices and other healthy snacks. Demonstrating a personal commitment to maintaining a healthy weight. Take time to
walk at school or wear a pedometer in the office; meet students for a weekly walk as part of a “Walk with Your School Nurse” program.
Encouraging physical activity in the classroom and during recess. See page 24 in the resource section for information on materials and websites for programs related to healthy eating, physical activity and staff wellness.

School Nurse Interventions for Childhood Obesity 12
SECTION 3: WORKING WITH STUDENTS AND FAMILIES
This section provides different resources and tools for working on behavior change with families. MOTIVATIONAL INTERVIEWING Overweight and obesity are difficult and sensitive topics to address, especially with children. Parents often become defensive when family nutrition and physical activity patterns are discussed as these patterns may apply to the whole family. Parents may feel their parenting skills are being judged or criticized. Living conditions, unsafe neighborhoods and a lack of resources are often beyond a parent’s control. Discussing such a sensitive topic requires a non-judgmental, non-threatening approach and a willingness to take it a step at a time until the student and parent are willing to participate in the discussion. Motivational interviewing is one tool to address this issue. The section on motivational interviewing will provide further information about how to use this technique when talking with parents and students. It is important to maintain sensitivity regarding overweight/obesity. Terms to consider:
Instead of Consider Obesity Overweight Ideal weight Healthier weight Personal improvement Family progress Focus on weight Focus on lifestyle Diets of “bad foods” Healthier food choices Exercise Physical activity
SELF-REFLECTION The authors of Motivational Interviewing: Helping People Change, Miller and Rollnick, 2013, emphasize compassion for clients and families to assure that healthcare providers actively promote the welfare of others and make the needs of others a priority. An exercise that can help move one to a compassionate viewpoint is to engage in self-reflection and reflection on what life might be like for others (personal communication, August 14, 2014, Brooks, C.W.). A quick moment of reflection can help to shift the mindset to add a component of compassion to the encounter. School nurses can do this by asking these questions:
What are my first thoughts when I see someone who is overweight? What, if any, judgments do I make about people who are overweight? If I were an overweight child, how would I feel when I woke up in the morning to get
ready for school? What fears would I have about going to school? What am I (as the child) thinking about myself? Imagine you are the parent–what goes through your mind if you put yourself in the
parent’s place? How do you feel about your child’s weight? Do you know how your child thinks/feels about his/her weight?

School Nurse Interventions for Childhood Obesity 13
MOTIVATIONAL INTERVIEWING PRINCIPLES Motivational interviewing provides a foundation for assisting individuals with developing the rationale for making a lifestyle change. This resource provides basic information for communicating using motivational interviewing. Motivational interviewing is an “empathic, person-centered counseling approach that prepares people for change by helping them resolve ambivalence, enhance intrinsic motivation and build confidence to change.” (Kraybill and Morrison, 2007) Open questions, affirmation, reflective listening and summary reflections (OARS) are the basic interaction techniques and skills that are used “early and often” in the motivational interviewing approach. The table below provides an explanation and gives examples for each step of the motivational interviewing process.
OARS Explanation Examples Open Questions
Open questions invite others to “tell their story” in their own words without leading them in a specific direction. Open questions should be used often in conversation, but not exclusively. When asking open questions, you must be willing to listen to the person’s response. Open questions are the opposite of closed questions. Closed questions typically elicit a limited response such as “yes” or “no.” The following example contrasts open vs. closed questions. Note how the topic is the same, but the response will be very different: Did you have a good relationship
with your parents? What can you tell me about your
relationship with your parents?
Examples of open questions: How can I help you with ___? Help me understand ___? How would you like things to be
different? What are the good things about ___ and
what are the bad things about it? When would you be most likely to___? What do you think you will lose if you
give up ___? What have you tried before to make a
change? What do you want to do next?
Affirmations Affirmations are statements and gestures that recognize client strengths and acknowledge behaviors that lead in the direction of positive change, no matter how big or small. Affirmations build confidence in one’s ability to change. To be effective, affirmations must be genuine and congruent.
Examples of affirming responses: I appreciate that you are willing to meet
with me today. You are clearly a very resourceful
person. You handled yourself really well in that
situation. That’s a good suggestion. If I were in your shoes, I don’t know if
I could have managed nearly so well. I’ve enjoyed talking with you today.
School Nurse Interventions for Childhood Obesity 14
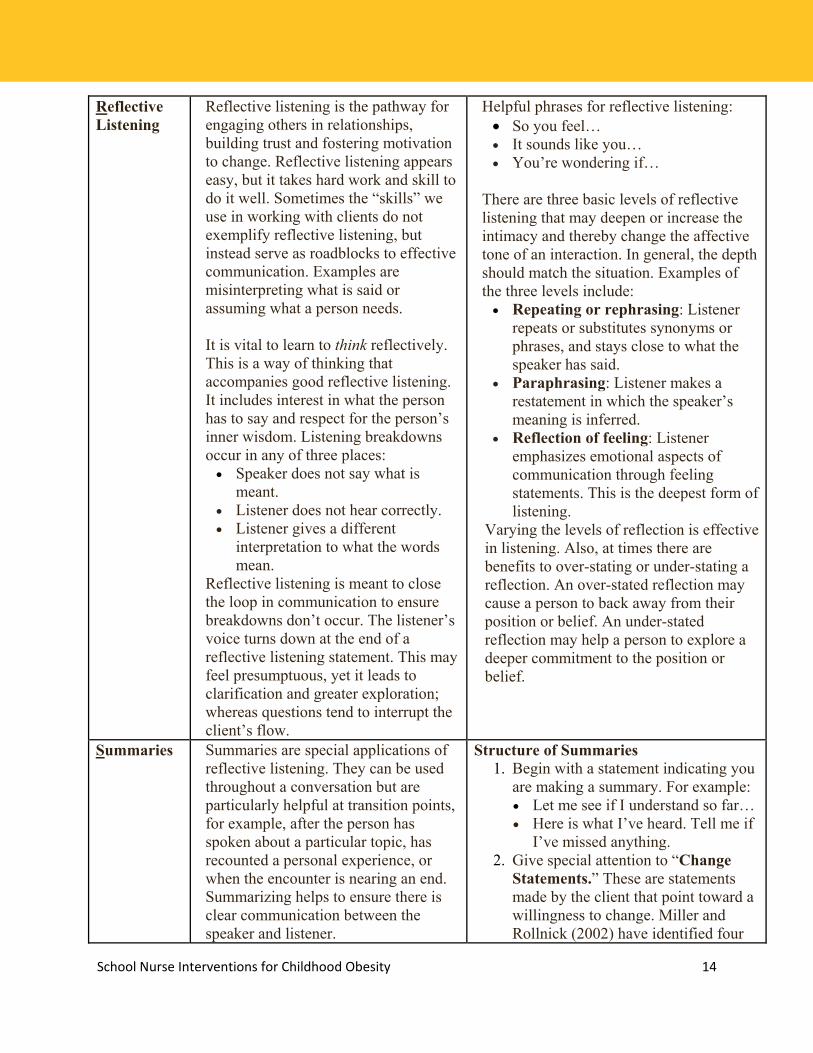
Reflective Listening
Reflective listening is the pathway for engaging others in relationships, building trust and fostering motivation to change. Reflective listening appears easy, but it takes hard work and skill to do it well. Sometimes the “skills” we use in working with clients do not exemplify reflective listening, but instead serve as roadblocks to effective communication. Examples are misinterpreting what is said or assuming what a person needs. It is vital to learn to think reflectively. This is a way of thinking that accompanies good reflective listening. It includes interest in what the person has to say and respect for the person’s inner wisdom. Listening breakdowns occur in any of three places: Speaker does not say what is
meant. Listener does not hear correctly. Listener gives a different
interpretation to what the words mean.
Reflective listening is meant to close the loop in communication to ensure breakdowns don’t occur. The listener’s voice turns down at the end of a reflective listening statement. This may feel presumptuous, yet it leads to clarification and greater exploration; whereas questions tend to interrupt the client’s flow.
Helpful phrases for reflective listening: So you feel… It sounds like you… You’re wondering if…
There are three basic levels of reflective listening that may deepen or increase the intimacy and thereby change the affective tone of an interaction. In general, the depth should match the situation. Examples of the three levels include: Repeating or rephrasing: Listener
repeats or substitutes synonyms or phrases, and stays close to what the speaker has said.
Paraphrasing: Listener makes a restatement in which the speaker’s meaning is inferred.
Reflection of feeling: Listener emphasizes emotional aspects of communication through feeling statements. This is the deepest form of listening.
Varying the levels of reflection is effective in listening. Also, at times there are benefits to over-stating or under-stating a reflection. An over-stated reflection may cause a person to back away from their position or belief. An under-stated reflection may help a person to explore a deeper commitment to the position or belief.
Summaries
Summaries are special applications of reflective listening. They can be used throughout a conversation but are particularly helpful at transition points, for example, after the person has spoken about a particular topic, has recounted a personal experience, or when the encounter is nearing an end. Summarizing helps to ensure there is clear communication between the speaker and listener.
Structure of Summaries 1. Begin with a statement indicating you
are making a summary. For example: Let me see if I understand so far… Here is what I’ve heard. Tell me if
I’ve missed anything. 2. Give special attention to “Change
Statements.” These are statements made by the client that point toward a willingness to change. Miller and Rollnick (2002) have identified four

School Nurse Interventions for Childhood Obesity 15
Summaries cont.
Also, it can provide a stepping stone toward change.
types of change statements, all of which overlap significantly: Problem recognition: “My use
has gotten a little out of hand at times.”
Concern: “If I don’t stop, something bad is going to happen.”
Intent to change: “I’m going to do something; I’m just not sure what it is yet.”
Optimism: “I know I can get a handle on this problem.”
3. If the person expresses ambivalence, it is useful to include both sides in the summary statement. For example: “On the one hand…, on the other hand…”
4. It can be useful to include information in summary statements from other sources (e.g., your own clinical knowledge, research, courts or family).
5. Be concise. 6. End with an invitation. For example:
Did I miss anything? If that’s accurate, what other points
are there to consider? Anything you want to add or
correct? 7. The client’s response to your
summary statement may lead naturally to planning for or taking concrete steps toward the change goal.
Source: Adapted from handouts by David Rosengren and from Miller & Rollnick, Motivational Interviewing, 2nd Edition. 2002. Motivational Interviewing: Open Questions, Affirmation, Reflective Listening, and Summary Reflections (OARS). Retrieved from: http://homeless.samhsa.gov/Resource/Print.aspx?id=32840&g=printtopic&t=427

School Nurse Interventions for Childhood Obesity 16
SIGNS OF READINESS AND KEY QUESTIONS Determining a student’s readiness for change is essential for success. Discussing changes when a student is not ready often leads to resistance, denial of problems or frustration that may hamper future efforts. The following tool provides a basis for starting a discussion with students and parents. Ask the child how ready he/she is to make a change, on a scale of 1 to 10, with 0 being not interested, and 10 being very ready to try to change. Using the questions below; probe for further information about readiness.
0-3 Not ready Key Question Raise awareness Would you be interested in knowing more about reaching a
healthy weight? Elicit change talk How can I help? Advise and encourage What might need to be different for you to consider a
change in the future? 4-6 Unsure Key Question
Evaluate ambivalence Where does that leave you now? Elicit change talk What do you see as your next steps?
What are you thinking/feeling at this point? Build readiness Where does this fit in your future?
7-10 Ready for Change Key Question Strengthen commitment Why is this important to you now? Elicit change talk What are your ideas for making this work? Facilitate action planning What might get in the way? How might you work around
these barriers? How might you reward yourself along the way?
It helps to have a visual aid like this scale for the student to look at while considering his level of readiness:
0 1 2 3 4 5 6 7 8 9 10

School Nurse Interventions for Childhood Obesity 17
MOTIVATIONAL INTERVIEWING ALGORITHMS
MOTIVATIONAL INTERVIEWING FOR THE PRE-CONTEMPLATION STAGE OF CHANGE
Pros
What are the positive things about ...?
What do you think is the up side of ...?
Cons
What are the negative things about…?
Assess readiness for change
How ready are you to ...?
Ask “might” questions.
Do you think you might consider…?
Establish a time frame: When might you want to begin…?
Let it go for now. Be available and prepared to repeat the process.
Explore the pros and cons of current behavior to raise student awareness.
If student is ready for change… If student is not ready for change…
School Nurse Interventions for Childhood Obesity 18
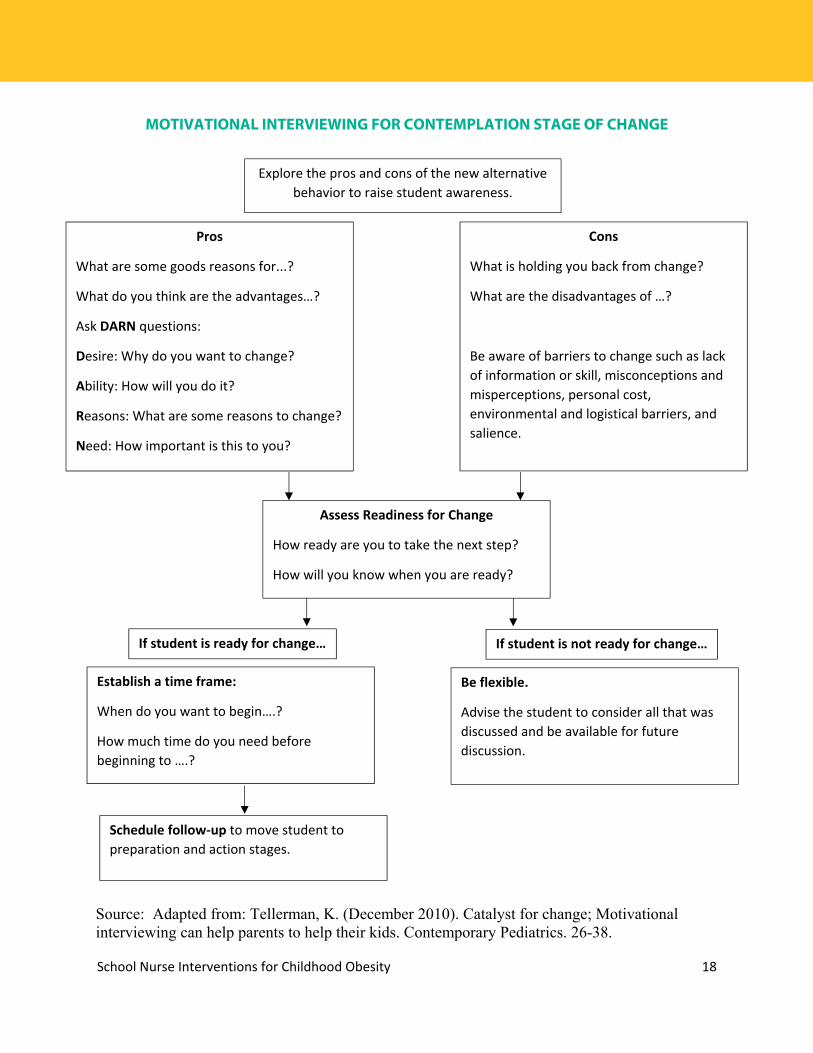
MOTIVATIONAL INTERVIEWING FOR CONTEMPLATION STAGE OF CHANGE
Source: Adapted from: Tellerman, K. (December 2010). Catalyst for change; Motivational interviewing can help parents to help their kids. Contemporary Pediatrics. 26-38.
Pros
What are some goods reasons for...?
What do you think are the advantages…?
Ask DARN questions:
Desire: Why do you want to change?
Ability: How will you do it?
Reasons: What are some reasons to change?
Need: How important is this to you?
Explore the pros and cons of the new alternative behavior to raise student awareness.
Cons
What is holding you back from change?
What are the disadvantages of …?
Be aware of barriers to change such as lack of information or skill, misconceptions and misperceptions, personal cost, environmental and logistical barriers, and salience.
Assess Readiness for Change
How ready are you to take the next step?
How will you know when you are ready?
If student is ready for change…
Establish a time frame:
When do you want to begin….?
How much time do you need before beginning to ….?
Schedule follow-up to move student to preparation and action stages.
Be flexible.
Advise the student to consider all that was discussed and be available for future discussion.
If student is not ready for change…
School Nurse Interventions for Childhood Obesity 19
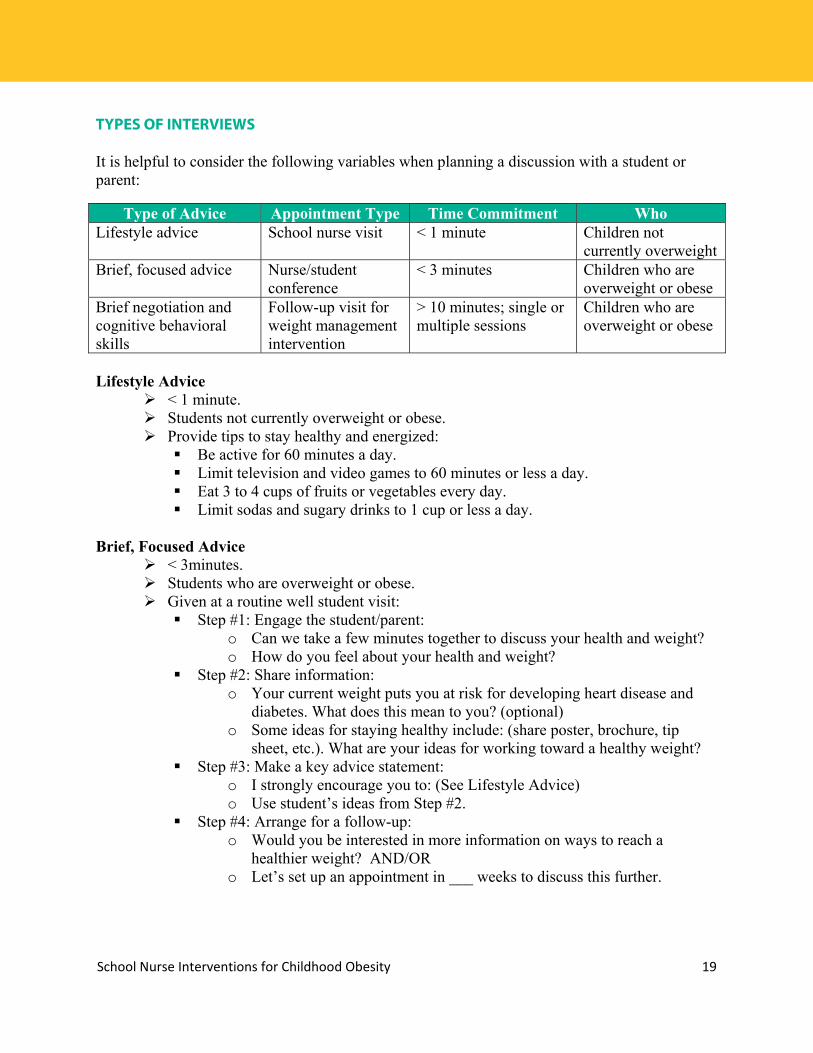
TYPES OF INTERVIEWS It is helpful to consider the following variables when planning a discussion with a student or parent:
Lifestyle Advice
< 1 minute. Students not currently overweight or obese. Provide tips to stay healthy and energized:
Be active for 60 minutes a day. Limit television and video games to 60 minutes or less a day. Eat 3 to 4 cups of fruits or vegetables every day. Limit sodas and sugary drinks to 1 cup or less a day.
Brief, Focused Advice
< 3minutes. Students who are overweight or obese. Given at a routine well student visit:
Step #1: Engage the student/parent: o Can we take a few minutes together to discuss your health and weight? o How do you feel about your health and weight?
Step #2: Share information: o Your current weight puts you at risk for developing heart disease and
diabetes. What does this mean to you? (optional) o Some ideas for staying healthy include: (share poster, brochure, tip
sheet, etc.). What are your ideas for working toward a healthy weight? Step #3: Make a key advice statement:
o I strongly encourage you to: (See Lifestyle Advice) o Use student’s ideas from Step #2.
Step #4: Arrange for a follow-up: o Would you be interested in more information on ways to reach a
healthier weight? AND/OR o Let’s set up an appointment in ___ weeks to discuss this further.
Type of Advice Appointment Type Time Commitment Who Lifestyle advice School nurse visit < 1 minute Children not
currently overweight Brief, focused advice Nurse/student
conference < 3 minutes Children who are
overweight or obese Brief negotiation and cognitive behavioral skills
Follow-up visit for weight management intervention
> 10 minutes; single or multiple sessions
Children who are overweight or obese

School Nurse Interventions for Childhood Obesity 20
Brief Negotiation and Cognitive Behavioral Skills
>10 minutes–single or multiple sessions Follow-up visit for weight management intervention with students who are
overweight or obese: Step #1: Open the encounter–ask permission.
o Would you be willing to spend a few minutes discussing your weight? o Are you interested in discussing ways to stay healthy and energized?
Step #2: Ask an open-ended question, listen and summarize: o What do you think/how do you feel about your weight? o What have you tried so far to work toward a healthier weight? o Share BMI/weight status/risk factors (optional):
Your current weight puts you at risk for developing heart disease and diabetes. Ask for student’s interpretation: What do you make of this?
o Add your own interpretation or advice as needed AFTER eliciting the student/parent response.
Step #3: Negotiate the agenda: o There are a number of ways to achieve a healthy weight. These include:
Physical activity. Eat more fruits and vegetables (goal is to eat 3 to 4 cups a day). Cut back on television and video games. Cut down on sodas and juice.
o Would you like to discuss any of these further today? Perhaps you have another idea that was not mentioned?
Step #4: Assess readiness: o On a scale from 0 to 10, how ready are you to consider (option chosen
above): Straight question: Why a 5? Backward question: Why a 5 and not a 3? Forward question: What would it take to move you from 5 to 7?
Step #5: Explore ambivalence: o Ask a pair of questions to help the student explore the pros and cons of
the issue: What are the things you like about _____? What are the things you
don’t like about ____? What are the advantages of keeping things the same? What are the
advantages of making a change? Step #6: Summarize ambivalence:
o Use these statements to check your understanding of the discussion thus far: Let me see if I understand what you have told me so far…. Begin with reasons for maintaining the status quo and end with
reasons for making a change. Did I get it all? or Did I get it right?

School Nurse Interventions for Childhood Obesity 21
Step #7: Close the encounter:
o Summarize: Our time is almost up. Let’s take a look at what you’ve worked through today…
o Show appreciation/acknowledge willingness to discuss change: Thank you for being willing to discuss your weight.
o Offer advice; emphasize choice and express confidence: I strongly encourage you to be more physically active. The choice to increase your activity, of course, is entirely yours. I am confident that if you decide to be more active, you can do it.
o Confirm next steps and arrange for follow up: Are you able to come back in a couple of weeks so we can continue to work together?
SAMPLE DIALOGUE OF A BRIEF NEGOTIATION FOR WEIGHT MANAGEMENT Before the student enters the nurse’s office, note the student’s age, gender, BMI and percentile, weight status, blood pressure and pulse (if this has been assessed).
Name Charles
Gender Male
Age 10 years
Ethnicity Hispanic
Height 55 inches
Weight 100 lbs.
BMI 23.2 (95th percentile for age and gender)
B/P Pulse Not available
School Nurse: Good morning! I see you are in for your annual school nurse visit. Do you have any concerns about your health? Charles: No, my mom made me come in. School Nurse: Can we take a few minutes together to talk about your health and weight? Charles: I guess so. School Nurse: Your mom is concerned about your weight and thought we might talk about it. How do you feel about your weight? Charles: I know I am bigger than most kids. School Nurse: Have you tried to do anything to get to a healthier weight? Charles: Not really, I just eat what all my friends eat.

School Nurse Interventions for Childhood Obesity 22
School Nurse: Your family has a history of diabetes. Did you know that your current weight makes you more likely to develop diseases like diabetes? Charles: No. My grandpa always complains about his diabetes. School Nurse: Diabetes is not easy to live with. I can understand why he complains. Let’s see what we can do to help you be healthier. There are some things; like eating more fruits and vegetables, cutting back on the number of sodas (sugary drinks) you drink, being more physically active and watching less television/spending less time sitting during free time. Do you want to talk about any of these, or do you have some ideas? Charles: Would riding my bike to school count as physical activity? School Nurse: It sure would. On a scale from 1 to 10, how ready do you think you are to start riding your bike to school? 10 would be the most ready and 1 the least ready (use visual aid). Charles: Probably a 5. School Nurse: Why a 5? Charles: Well, I don’t have anyone to ride with, and there are a couple of busy streets. School Nurse: I see how that would make it scary or unsafe. What sounds good about riding your bike to school? Charles: Riding my bike is pretty fun. And I wouldn’t have to wait in traffic in the car and be late for school. School Nurse: So the busy streets and having no one to ride with may make this change difficult, but you like to ride your bike and you wouldn’t be late for school if you rode your bike. Did I get it right? Charles: Yeah. School Nurse: What do you think your next step is? Charles: I guess I’ll try riding my bike to school one day next week. Maybe I’ll find someone to ride with. School Nurse: Great! I think you are making a very healthy choice for yourself. Thank you for being so willing to discuss this with me. When you come back next month for your flu shot, I want to see how you are doing with your idea to be more physically active.

School Nurse Interventions for Childhood Obesity 23
MEASURING PROGRESS Measuring the progress of weight loss or management can be a frustrating and confusing task. While the ultimate goal may be weight loss or a decrease in BMI percentile, there are other important ways to measure success that should not be ignored. Included below are some ways to track success in weight management efforts.
Knowledge: Gains in knowledge about healthful eating and physical activity practices indicate progress. Knowledge can be measured by asking students the same questions at the start and end of a session or starting a session by asking about knowledge shared in previous visits.
Behavior: Positive changes in eating and physical activity behaviors indicate
progress. It may take some time for changes in behavior to affect weight. For example, increasing daily physical activity by 30 minutes may not result in a decrease of BMI right away, but this should still be considered a success. Use motivational interviewing concepts to assess changes in behavior.
Attitude: A change of attitude can also be a sign of progress. Weight management
can be stressful and overwhelming, especially at the start of a program. If a student’s attitude slowly goes from being closed-off and negative to open and cheerful when discussing weight management, this should be noted as a success. Measuring attitude is subjective. Acknowledging positive attitude changes and exploring these changes with the student, is one way to learn more about the student’s intentions.
Attendance: A willingness to show up for discussions about weight management can
be a sign of success. Arranging for a student/parent to meet with you to talk about weight management may be a difficult task. Remember that every minute spent talking with a student about weight management is an opportunity to evoke change. Do not give up if progress is slow.
Positive changes in eating and physical activity behaviors indicate progress.
School Nurse Interventions for Childhood Obesity 24
SECTION 4: RESOURCES
EXAMPLE BMI PERCENTILE CHART FOR BOYS 2-20 YEARS OF AGE

School Nurse Interventions for Childhood Obesity 25
EXAMPLE BMI PERCENTILE CHART FOR GIRLS 2-20 YEARS OF AGE

School Nurse Interventions for Childhood Obesity 26
EXAMPLES OF PLOTTING BMI ON PERCENTILE CHART
School Nurse Interventions for Childhood Obesity 27
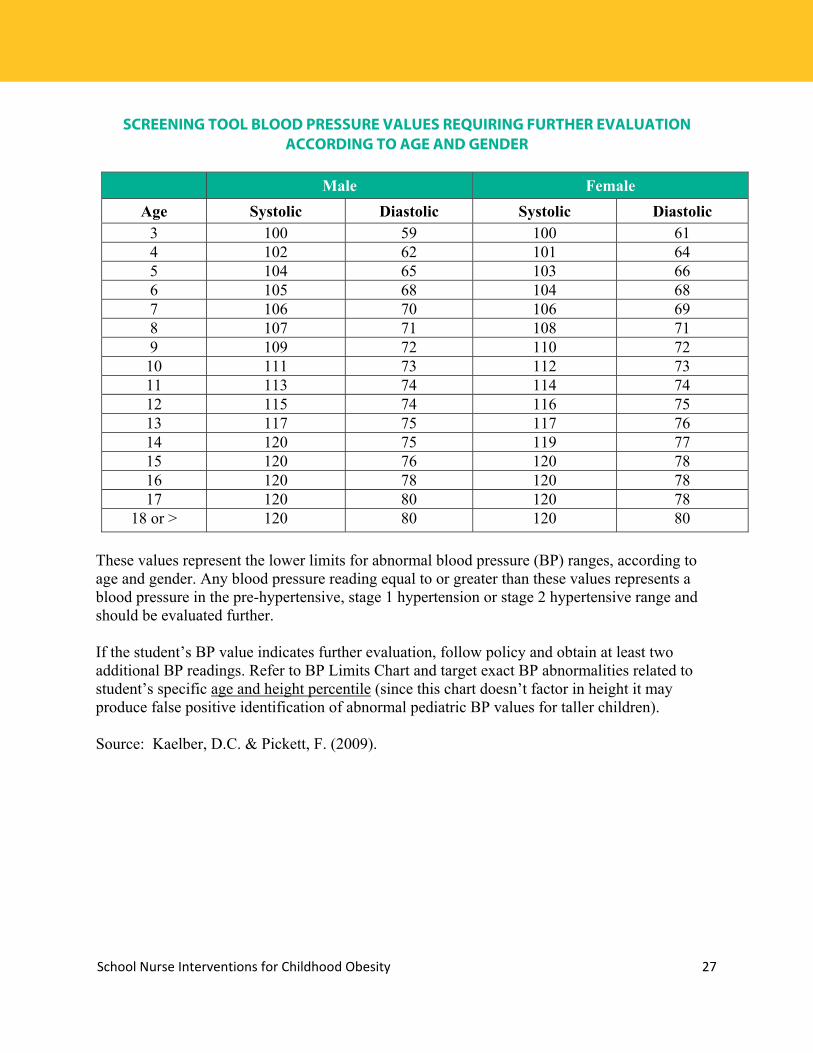
SCREENING TOOL BLOOD PRESSURE VALUES REQUIRING FURTHER EVALUATION
ACCORDING TO AGE AND GENDER
Male Female
Age Systolic Diastolic Systolic Diastolic 3 100 59 100 61 4 102 62 101 64 5 104 65 103 66 6 105 68 104 68 7 106 70 106 69 8 107 71 108 71 9 109 72 110 72 10 111 73 112 73 11 113 74 114 74 12 115 74 116 75 13 117 75 117 76 14 120 75 119 77 15 120 76 120 78 16 120 78 120 78 17 120 80 120 78
18 or > 120 80 120 80
These values represent the lower limits for abnormal blood pressure (BP) ranges, according to age and gender. Any blood pressure reading equal to or greater than these values represents a blood pressure in the pre-hypertensive, stage 1 hypertension or stage 2 hypertensive range and should be evaluated further. If the student’s BP value indicates further evaluation, follow policy and obtain at least two additional BP readings. Refer to BP Limits Chart and target exact BP abnormalities related to student’s specific age and height percentile (since this chart doesn’t factor in height it may produce false positive identification of abnormal pediatric BP values for taller children). Source: Kaelber, D.C. & Pickett, F. (2009).

School Nurse Interventions for Childhood Obesity 28
HEALTHY LIFESTYLE QUESTIONNAIRE

School Nurse Interventions for Childhood Obesity 29
SAMPLE LIFESTYLE QUESTIONS
Samples of Quick and Easy Lifestyle Questions
Ask simple questions that students can understand and answer. If you only have a few minutes, pick one question/topic to explore. Remember, even if you do not get a straight-forward answer, use the time to have an
open discussion about the topic. Don’t just ask–use motivational interviewing!
Dietary Habits
How often do you eat fast food or other meals outside of the home? o Meals eaten outside of the home are more likely to be high in calories, fat and
sugar. How many times per day do you drink sugary drinks (fruit drinks, Gatorade,
lemonade, soda, etc.)? How much do you drink (what size is the cup/container)? o Many times students are not aware of the sugar in the beverages they are
drinking. Drinks such as iced tea or sports drinks are commonly seen as healthy when they are often full of sugar.
How often do you eat breakfast? o Skipping breakfast may lead to over eating later in the day.
How much meat/fruit/vegetables/candy do you typically have at a time? o Use portion sizes students will understand. For example, instead of using
ounces to explain proper protein servings, use a deck of cards or the palm of your hand.
How often do you eat fruits and/or vegetables? How many meals and snacks do you have daily?
o Skipping meals and frequent snacking may lead to increased consumption of energy dense foods.
Physical Activity Do you participate in physical education class? How often?
o For some students, this may be their main source of physical activity. What other types of physical activity do you do?
o Total physical activity through physical education class, free play, time spent outside, organized sports, clubs or community recreation programs should be at least 60 minutes per day. Students that are not used to being active should set smaller goals and work up to 60 minutes.
How many hours per day do you spend watching television, playing video games or using the computer (screen time)?
o Should be less than 2 hours of screen time per day. Where is your television located? Do you have a television in your room?
o Removing televisions from bedrooms may help to decrease screen time and increase hours of sleep.
School Nurse Interventions for Childhood Obesity 30
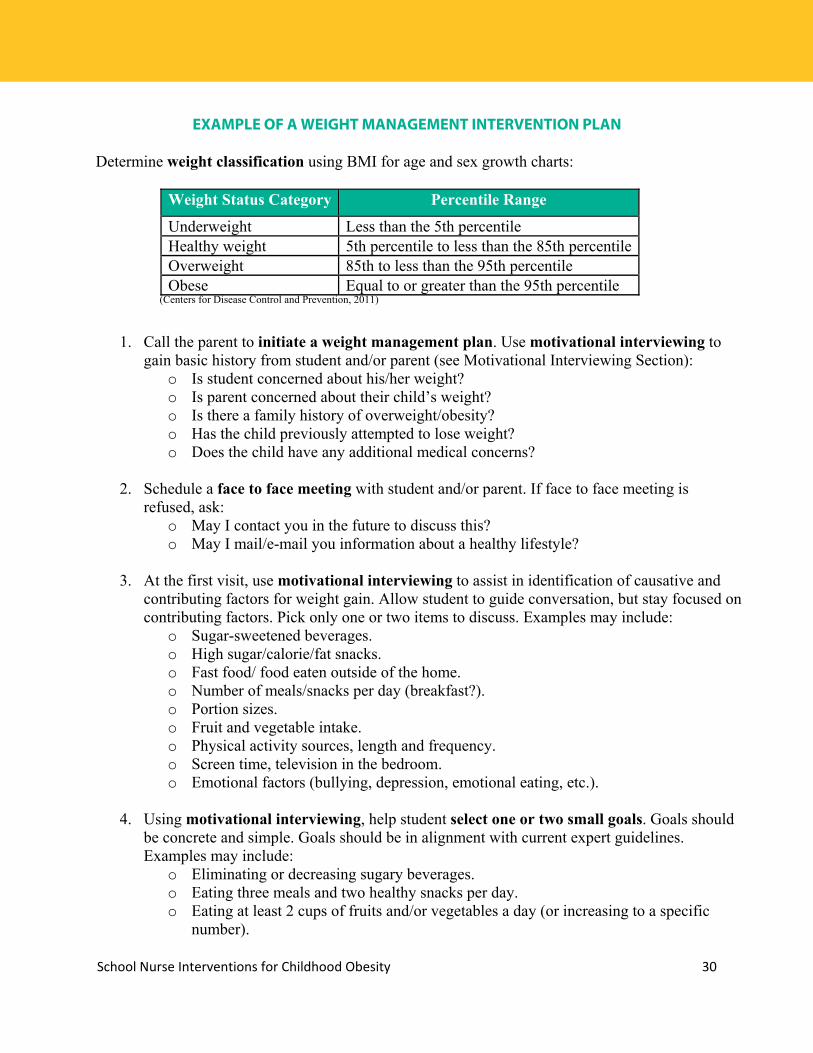
EXAMPLE OF A WEIGHT MANAGEMENT INTERVENTION PLAN
Determine weight classification using BMI for age and sex growth charts:
Weight Status Category Percentile Range
Underweight Less than the 5th percentile Healthy weight 5th percentile to less than the 85th percentile Overweight 85th to less than the 95th percentile Obese Equal to or greater than the 95th percentile
(Centers for Disease Control and Prevention, 2011)
1. Call the parent to initiate a weight management plan. Use motivational interviewing to gain basic history from student and/or parent (see Motivational Interviewing Section):
o Is student concerned about his/her weight? o Is parent concerned about their child’s weight? o Is there a family history of overweight/obesity? o Has the child previously attempted to lose weight? o Does the child have any additional medical concerns?
2. Schedule a face to face meeting with student and/or parent. If face to face meeting is
refused, ask: o May I contact you in the future to discuss this? o May I mail/e-mail you information about a healthy lifestyle?
3. At the first visit, use motivational interviewing to assist in identification of causative and
contributing factors for weight gain. Allow student to guide conversation, but stay focused on contributing factors. Pick only one or two items to discuss. Examples may include:
o Sugar-sweetened beverages. o High sugar/calorie/fat snacks. o Fast food/ food eaten outside of the home. o Number of meals/snacks per day (breakfast?). o Portion sizes. o Fruit and vegetable intake. o Physical activity sources, length and frequency. o Screen time, television in the bedroom. o Emotional factors (bullying, depression, emotional eating, etc.).
4. Using motivational interviewing, help student select one or two small goals. Goals should
be concrete and simple. Goals should be in alignment with current expert guidelines. Examples may include:
o Eliminating or decreasing sugary beverages. o Eating three meals and two healthy snacks per day. o Eating at least 2 cups of fruits and/or vegetables a day (or increasing to a specific
number).

School Nurse Interventions for Childhood Obesity 31
o Drinking four glasses of water daily. o Getting at least 60 minutes of physical activity per day (or increasing to another
specific amount). o Decreasing screen time to less than two hours per day.
5. Praise student for committing to making healthy changes. 6. Schedule a follow- up appointment:
o Determine a schedule for subsequent visits (weekly, bi-weekly, monthly, etc.). o Determine a schedule for height/weight/BMI check (bi-weekly, monthly, etc.). o Determine the role of family or other school staff in reaching goals.
7. At the next visit, check height/weight/BMI (if in accordance with agreed upon schedule) and use motivational interviewing to review progress toward meeting previously set goal. Discuss successes and challenges.
8. Repeat, starting at step 5. 9. Additional interventions:
o Contact primary care provider with parent’s written permission to discuss. recommendations and care plan.
o Collaborate with appropriate school staff/faculty to create a comprehensive plan. o Refer to a registered dietitian nutritionist and/or support group, as needed. o Refer to a counselor/social worker, as needed. o Refer to community resources, as needed.
Source: Centers for Disease Control and Prevention. (2011). About BMI for Children and Teens. Retrieved from: http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html
Contact primary care provider with parent’s written permission to discuss recommendations and care plan.

School Nurse Interventions for Childhood Obesity 32
PEDIATRIC WEIGHT MANAGEMENT TIPS FOR GETTING STARTED
Be supportive
o Do not forget that students may be dealing with teasing and bullying from peers or family members. Overweight students may struggle with body image issues. Be positive and supportive to help students build the confidence and self-esteem necessary to make positive lifestyle changes.
Be realistic o Focus on small specific goals. This will make the large task of weight loss seem
more manageable. Think about it: Would you get better results from asking a student to clean your office or asking a student to file papers and dust your desk? The more specific you can be, the more likely you are to see positive results.
Keep the conversation open o Ask students how they feel, without passing judgment. Let them know they are in
a safe place to talk about feelings and emotions related to weight and health. Encourage students to speak openly. Listening to how a student feels can be just as powerful as giving advice.
Normalize the issue o Talk about weight as a health concern. This keeps it in the same context as other
health issues such as asthma or allergies. Talking about weight, just as you would any other health issue, may help de-stigmatize obesity and help students talk about it more openly.
o When discussing overweight or obesity, the intention is not to focus on the cosmetic implications of excess body weight, but to focus on health risks and conditions as a consequence of overweight and obesity in childhood.
Do not be afraid to talk about weight o Often times, our own experiences or biases make us uncomfortable when talking
about weight. Don’t let this get in the way of meaningful conversations. Source: Strategies to Overcome and Prevent (STOP) Obesity Alliance. (2012).

School Nurse Interventions for Childhood Obesity 33
PROMOTING HEALTHY EATING FOR CHILDREN AND ADOLESCENTS
There are several ways to encourage healthy eating for children and adolescents. Promoting simple, family-centered messages may be the most effective way to help students make changes. The following tips may help students and families improve dietary habits. Find more tips at www.choosemyplate.gov.
Fruits and Vegetables: o Add fruit to hot or cold cereal. o Add vegetables, such as shredded carrots to foods you already love like tacos or
spaghetti. o Make a fruit smoothie for breakfast—blend up fruit (fresh or frozen) with yogurt
or ice. o Buy the fruits and/or vegetables that are on sale—this makes healthy eating
inexpensive and it encourages trying new things. o Eat at least one fruit or vegetable with each meal.
Beverages:
o Know what drinks are sugar-sweetened—soda, flavored milk, canned/bottled iced tea, sports drinks, fruit drinks, Kool-Aid and lemonade are all sugary drinks.
o Limit intake of 100% fruit juice to 8 to 12 ounces per day. o Start out by replacing one sugary drink with water; after a few days, replace
another serving with water. Do this until you are not drinking any sugared drinks. o Craving carbonation? Try plain sparkling water and add a lemon for flavor. o Add fresh fruit or sliced vegetables to water to give it an extra kick. Lemons,
cucumbers, limes, oranges, watermelon and berries are tasty. o Buy a reusable water bottle and fill it up at every drinking fountain.
Portion Control:
o When eating out: Avoid ordering items that are labeled as jumbo, super-sized, giant, family-
size or value-meals. These items are guaranteed to be more than one serving.
Split a meal with a friend. This will help to control portions and save money.
o Portion out a single serving of food using a bowl or plate rather than eating foods out of the package.
o Use a smaller plate or bowl for meals or snacks. o Know what typical portion sizes look like. Practice measuring portions until
comfortable with estimating portions.
Source: Barlow, S.E. & the Expert Committee. (2007). .

School Nurse Interventions for Childhood Obesity 34
PROMOTING PHYSICAL ACTIVITY IN CHILDREN AND ADOLESCENTS
According to several expert organizations, the optimal amount of physical activity for children and adolescents is at least 60 minutes of moderate to vigorous physical activity every day of the week. While this may seem like a difficult goal to reach, there are many ways to promote this behavior and help students form healthy physical activity habits.
Promote increased physical activity by reducing sedentary time. Encourage less than 2 hours of media/screen time daily: o Suggest students meet friends at the park or playground to talk/walk/play instead
of talking on the phone, chatting on the computer or texting. o Recommend active videogames that require physical activity.
Encourage parents/guardians to actively work to reduce sedentary time in the home:
o Remind parents to not use screen/media time as a reward or punishment. This only makes screen time seem even more important to children and adolescents.
o Encourage parents to make ALL bedrooms television-free. o Suggest parents set (and enforce) screen time limits. o Reinforce the importance of leading by example. o Promote physical activity as a fun way to be healthy.
Encourage physical activities that are fun and enjoyable for children and adolescents:
o Fun activities might include joining an afterschool sport group, walking around the school track with friends, dancing, active videogames, going to the playground, playing outside with younger siblings and indoor activities such as bowling or roller blading.
o Don’t forget about less traditional ways to be active: community service, marching band or joining organizations that serve youth.
o Encourage students to try something new: yoga, Pilates, kick-boxing, karate or Zumba!
Promote parental involvement in physical activity:
o Suggest a family activity night, instead of family movie night. o Recommend nightly post-dinner walks. o Is there an activity or sport that parents are passionate about? Have them teach
their child how to do this. Source: American Heart Association. (2012). (Daniels, S.R. & Expert Panel, 2011)

School Nurse Interventions for Childhood Obesity 35
SAMPLE INDIVIDUALIZED HEALTH PLAN (IHP)
Student _____________________________________________ Grade___________________ Teacher/Staff Contact ___________________________________________________________ IHP written by _________________________________________________________________ Date of IHP _________________________ Review Date(s) ____________________________ Assessment Data Nursing
Diagnosis Student’s Goals
Nursing Interventions
Outcomes (evaluation)
Male, 12 years of age BMI 22 BMI percentile for age/sex 90th percentile History of using electronic devices for long periods after school, often at home without supervision and lives in an unsafe neighborhood.
Imbalanced nutrition: consuming more than body requires related to lack of knowledge of recommended nutritional intake for age/level of activity. Sedentary lifestyle related to lack of opportunities for safe outdoor space for physical activity.
Learn ways to improve daily diet through better food choices at school and at home. Increase amount of physical activity by keeping chart and increasing walking time by 5 minutes per day until walking >30 minutes daily; will walk before class each morning on playground.
Education Provide student with information about ways to improve diet. Work with teacher on incorporating nutrition into lesson plans. Work with parent regarding ways to improve family’s diet. Education/Support Meet bi-weekly with student to review chart and provide information about ways to increase activity level. Discuss with parent ways to increase family’s activity level.
Indicator: Makes good food choices. Never 1 Rarely 2 Sometimes 3 Often 4 Consistently 5
Indicator: Adheres to activity plan. Never 1 Rarely 2 Sometimes 3 Often 4 Consistently 5

School Nurse Interventions for Childhood Obesity 36
Family history of high blood pressure, high cholesterol and overweight/obesity.
Lack of knowledge related to risk factors for cardiovascular disease and diabetes and prevention of chronic disease.
Learn risk factors and preventive measures and discuss with family the need to change diet and lifestyle.
Education/Support Provide student and parent with written information and resources for lifestyle changes for family environment.
Indicator: Verbalizes positive attitude toward lifestyle changes. Never 1 Rarely 2 Sometimes 3 Often 4 Consistently 5
School Nurse Interventions for Childhood Obesity 37
INTERNET RESOURCES FOR SCHOOL NURSES ADDRESSING OVERWEIGHT AND OBESITY
Many of the resources listed can be used to develop handouts for parents and students, or for general meetings to discuss nutrition and physical activity, and their relationship to child overweight and obesity.
MISSOURI RESOURCES
Missouri Coordinated School Health Coalition (MCSHC) The MCSHC uses the Centers for Disease Control and Prevention’s (CDC) coordinated school health model to assist schools in their wellness initiatives by providing information about resources and organizations. http://www.healthykidsmo.org Missouri Department of Health and Senior Services
Missouri Team Nutrition Missouri Team Nutrition implements programs that assist Missouri pre-school and school-age children in making healthy, nutritious choices that result in improved health status. http://health.mo.gov/living/wellness/nutrition/teamnutrition/index.php School Health http://health.mo.gov/living/families/schoolhealth/index.php Health Care Provider Tool kit for Physical Activity and Nutrition A tool kit to help providers effectively screen, assess and treat youth with weight issues. The tool kit resources summarize recommendations from the scientific literature and expert work groups related to child and adolescent obesity. http://health.mo.gov/living/healthcondiseases/obesity/childtoolkit.php
Missouri Council for Activity and Nutrition (MOCAN) http://extension.missouri.edu/mocan Local Health Departments Local public health agencies located throughout Missouri work to improve the health of Missourians. These agencies address a wide range of public health issues, from assessing the health risks of environmental problems to providing emergency services during natural disasters. Local public health agencies protect food safety by inspecting restaurants and grocery stores. They work to control communicable diseases, such as flu and tuberculosis, and to alleviate chronic conditions, including heart disease, diabetes and stroke. http://health.mo.gov/living/lpha/lphas.php Missouri Farm to School http://mofarmtoschool.missouri.edu
School Nurse Interventions for Childhood Obesity 38
Get Set Mo Link to calendar of running/walking events in Missouri http://www.getsetusa.com/missouri/running-calendar.php Governor’s 100 Missouri Miles Challenge http://100missourimiles.com
SCHOOL BASED ASSESSMENT TOOLS School Health Index The School Health Index (SHI) is an online assessment tool developed by the CDC. The tool evaluates health practices and policies in the school and then assists in developing a plan for improvement. www.cdc.gov/healthyyouth/shi Curriculum Analysis Tools The CDC developed curriculum analysis tools to help school districts conduct a clear, complete and consistent analysis of health education and physical education curriculum based on national standards.
Health Education Curriculum Analysis Tool (HECAT) www.cdc.gov/healthyyouth/hecat/ Physical Education Curriculum Analysis Tool (PECAT)
www.cdc.gov/healthyyouth/pecat/ WellSAT (through the Rudd Center for Food Policy and Obesity at Yale University) WellSAT 2.0 is an online tool to assess the quality of school districts’ written wellness policy, and provides personalized guidance and resources for making improvements, based on the assessment. http://www.wellsat.org/default.aspx Healthy School Report Card Creating a Healthy School: The Health School Report Card (2010) is a tool for School Health Advisory Councils to use for creating a holistic healthy school environment utilizing the concepts outlined in the Whole School, Whole Community, Whole Child model. http://www.ascd.org/publications/books/110140/chapters/The-Purpose-of-the-Healthy-School-Report-Card.aspx
CENTERS FOR DISEASE CONTROL AND PREVENTION (CDC) RESOURCES Weight Assessment Tools http://www.cdc.gov/obesity/childhood/basics.html Nutrition, Physical Activity and Obesity Resources http://www.cdc.gov/healthyyouth/npao/index.htm
School Nurse Interventions for Childhood Obesity 39
Coordinated School Health Resources (including Whole School, Whole Community, Whole Child Model) www.cdc.gov/healthyyouth/cshp Comprehensive School Physical Activity Program (CSPAP) http://www.cdc.gov/healthyyouth/physicalactivity/cspap.htm The Association between School-Based Physical Activity, Including Physical Education, and Academic Performance http://www.cdc.gov/healthyyouth/health_and_academics/pdf/pa-pe_paper.pdf
HEALTHY SCHOOL ENVIRONMENT RESOURCES What Works for Health, Robert Wood Johnson Foundation What Works for Health provides communities with information to help select and implement evidence-informed policies, programs and system changes that will improve the variety of factors known to affect health. http://www.countyhealthrankings.org/roadmaps/what-works-for-health School Wellness Policy Resources http://healthymeals.nal.usda.gov/school-wellness-resources Robert Wood Foundation http://www.rwjf.org/en/about-rwjf/program-areas/childhood-obesity/strategy.html Alliance for a Healthier Generation https://www.healthiergeneration.org
GENERAL INFORMATION RESOURCES National Initiative for Children’s Health Care Quality http://obesity.nichq.org American Academy of Pediatrics The motivational video, "Change Talk: Childhood Obesity,” is an interactive, training simulation to help pediatricians and other health professionals learn motivational interviewing techniques to counsel families on childhood obesity. In the training simulation, participants engage in a conversation with a mother and her son, using motivational interviewing skills to facilitate family behavioral change. www.aap.org/obesity
Academy of Nutrition and Dietetics http://www.eatright.org
School Nurse Interventions for Childhood Obesity 40
Kids Eat Right http://www.eatright.org/kids U.S. Dietary Guidelines http://www.health.gov/dietaryguidelines Community Commons www.communitycommons.org Community Commons is an interactive mapping, networking and learning utility for the broad-based healthy, sustainable and livable communities’ movement. Community Commons provides many different data sets to assess specific state and county health disparities. The following types of data can be obtained:
Percentage of uninsured population Percentage of population which is obese Percentage of people who are physically inactive Percentage of population who live in food deserts or who have limited food access Percentage of soda expenditures Percentage of population who live within 1/2 mile of a park
RESOURCES FOR CREATING EDUCATIONAL MATERIALS
USDA's Core Nutrition Messages Use these resources in educational tools, activities and interventions to help low-income audiences put the recommendations of the Dietary Guidelines for Americans into practice. http://www.fns.usda.gov/core-nutrition/core-nutrition-messages The National PTA http://www.pta.org/programs/content.cfm?ItemNumber=3132 Kids Health www.kidshealth.org Bulletin Boards in a SNAP http://healthymeals.nal.usda.gov/state-resources/bulletin-boards-snap PE Central Bulletin Boards http://www.pecentral.org/bulletinboard/BulletinBoardSearchresults.asp Fruits and Veggies-More Matters http://www.fruitsandveggiesmorematters.org Fit MD http://fit.webmd.com/about-fit

School Nurse Interventions for Childhood Obesity 41
Sleep Soundly http://extension.missouri.edu/p/GH6116 RESOURCES TO PROMOTE HEALTHY EATING AND PHYSICAL ACTIVITY FOR ALL CHILDREN
Action for Healthy Kids http://www.actionforhealthykids.org/index.php 12345 Fit-Tastic http://www.12345fit-tastic.org MyPlate http://www.choosemyplate.gov Midwest Dairy Council http://www.midwestdairy.com The Wellness Impact: Enhancing Academic Success through Healthy School Environments A brief report by the National Dairy Council showing the benefits of healthy eating and exercise. http://www.nationaldairycouncil.org/ChildNutrition/Documents/Wellness%20Impact%20Student%20Brief%20FINAL%203_3_13.pdf WE CAN! National Heart Lung and Blood Institute Offers ways to enhance children’s activity and nutrition and lists local WE CAN programs. http://www.nhlbi.nih.gov/health/educational/wecan Shape Up America The purpose of Shape Up America! is to educate the public on the importance of the achievement and maintenance of a healthy body weight through the adoption of increased physical activity and healthy eating. www.shapeup.org Presidential Youth Fitness Program http://www.pyfp.org/about/index.shtml Spark http://www.sparkpe.org Let’s Move Active Schools http://www.letsmoveschools.org Girls on the Run http://www.girlsontherun.org
Empower Me at School https://www.healthiergeneration.org/take_action/empower_young_people/engage_youth Fuel Up to Play 60 https://www.fueluptoplay60.com USDA/Team Nutrition http://www.fns.usda.gov/team-nutrition

School Nurse Interventions for Childhood Obesity 42
REFERENCES
1. C.S. Mott. Children’s Hospital National Poll on Children’s Health. (2014). Available at: http://mottnpch.org/reports-surveys/school-violence-gun-related-injuries-top-10-child-health-concerns-us. Accessed on September 1, 2014. 2. Ogden C, Carroll M, Kit B, Flegal K. (2014). Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 2011-2012. JAMA, 300(8)806-814. 3. Kaufman FR. (2002). Type 2 Diabetes in Children and Young Adults: A “New Epidemic”. Clinical Diabetes. 20(4): 217-18. 4. Le J, Zhang, D, Menees S, Chen J, Raghuveer G. (2010). "Vascular age" is advanced in children with atherosclerosis promoting risk factors. Cir Cardiov Imaging; 3(1): 8-14. Barlow SE and the Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007; 120 Supplement December 2007:S164-S192.

School Nurse Interventions for Childhood Obesity 43

School Nurse Interventions for Childhood Obesity 44