sbar - · pdf filesbar a communication technique deb wolski clinical educator cardiac program...
TRANSCRIPT

SBAR A
Communication
Technique Deb Wolski
Clinical Educator
Cardiac Program
March 2008/rev.July 2011

2012/12/21 1 2012/12/21 1
Objectives
• To understand the reason for using this tool
• To ensure the right information is conveyed in
the right way to get the results needed
• To understand the components of SBAR
• To demonstrate the use of this form
2012/12/21 2
SBAR A structured communication tool
used between health team members
to effectively communicate about a
patient
2012/12/21 2

2012/12/21 3 2012/12/21 3
• Endorsed by Safer Healthcare Now
and the Institute for Healthcare
Improvement (IHI)
• Quick to learn, easy to remember
and use
2012/12/21 4
Consists of Four Components:
1. Situation
2. Background
3. Assessment
4. Recommendation
2012/12/21 4

2012/12/21 5
S Situation
Describe the situation
WHAT IS GOING ON NOW ?
2012/12/21 5

2012/12/21 6
B Background
Deliver a concise history
2012/12/21 6

2012/12/21 7
A Assessment
Describe your findings
2012/12/21 7

2012/12/21 8
R Recommendations
What needs to happen?
WHAT WOULD YOU SUGGEST HAPPEN ?
2012/12/21 8

2012/12/21 9
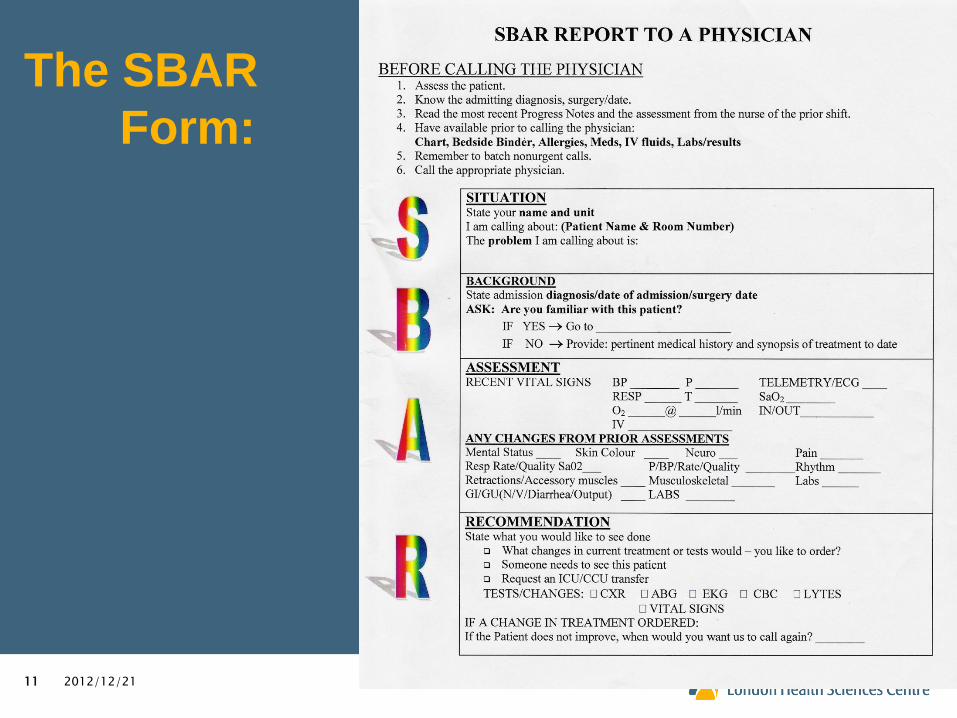
SBAR REPORT TO A
PHYSICIAN
• BEFORE CALLING THE PHYSICIAN
First: Batch calls; ask if anyone else needs to speak to
the resident
1. Assess the patient
2. Review the chart for the appropriate physician
to call
2012/12/21 9

2012/12/21 10 2012/12/21 10
3. Know the admitting diagnosis, date of surgery
or procedure
4. Read the most recent Progress Notes and the
assessment by the nurse from the prior shift.
5. Have available when speaking with the physician:
Chart
Allergies
Meds
IV fluids
Labs & Results
2012/12/21 11
The SBAR
Form:
2012/12/21 11

2012/12/21 12
S
SITUATION
State your name and unit
„I am calling about‟: (Patient Name & Room Number)
„The problem I am calling about is‟:
2012/12/21 12

2012/12/21 13
B
BACKGROUND
State the admission diagnosis and date of admission
State the pertinent medical history
Provide a Brief Synopsis of the treatment to date
2012/12/21 13
2012/12/21 14
A
ASSESSMENT
Provide the following information:
Most recent vital signs: BP Pulse
Respirations (rate and quality)
Retractions / use of accessory muscles
on or not on Oxygen
Temperature if abnormal
2012/12/21 14
2012/12/21 15 2012/12/21 15
Changes from prior assessments, such as:
- VS - Rhythm - Skin Color
- Pain - Mental Status
- Wound drainage - Neuro status
- Musculoskeletal (joint deformity, weakness)
- GI/GU (Nausea /Vomiting/Diarrhea/Urine
Output)

2012/12/21 16
R RECOMMENDATION
Do you think we should:
(State what you would like to see done)
Transfer the patient to ICU or PICU ?
Come to see the patient at this time ?
Talk to the patient and/or family about the code status ?
Ask for a consultant to see the patient now ?
Other suggestion ?
2012/12/21 16

2012/12/21 17
RECOMMENDATION
Are any tests needed ?
Do you need any tests like
CXR ABG EKG CBC
Others?
If a change in treatment is ordered, then ask:
How often do you want vital signs ? _________________________________
If the patient does not improve, when
would you want us to call again?
2012/12/21 17

2012/12/21 18
Example
S – Situation
• “Hi, it‟s Jane Smith, RN, from 6IP calling about Mrs.
Green, a patient of Dr. Heart‟s, in Rm A6202C.
She is complaining of being short of breath at rest
and is using her accessory muscles to breath. Her
oxygen saturation levels are in the low 80‟s on 5L
NP.”
2012/12/21 18
2012/12/21 19
B – Background
• “Are you familiar with this patient?”
• If yes, continue to assessment.
• If no, give pertinent medical history and
synopsis of treatment to date.
• “Mrs. Green was admitted with ACS on Sept. 8th.
She had a CABG x 3 and AVR (mechanical) replacement on Sept. 9th. She has IDDM
and a history of CRF.”
2012/12/21 19

2012/12/21 20
A – Assessment
• Coarse crackles in mid and lower lobes bilaterally
• BP 172/80, P 100, RR 42 & regular, oxygen sat levels of 80-83% on 5L NP with HOB in high fowlers
• RT assessing & has her sats at 90% on 75% face mask
• Clammy & pale; lips and nail beds are cyanosed
• Restless and anxious, although still alert and orientated
2012/12/21 20

2012/12/21 21
Assessment cont’d
• u/o borderline, +ve fluid balance of 2000cc for the previous 12hrs
• continues to have +ve balance of 400cc thus far on this shift
• IV is 5%DW and .9% NaCl at 50cc/hr
• Lasix 40mg IV on days and diuresed 800cc
• Creat. 243, urea 20.3, HB 82, Na 127, K+4.8, INR 2.5
• EKG - sinus tachycardia with frequent PVC‟s.
2012/12/21 21

2012/12/21 22
R = Recommendation
• “I‟m really concerned about Mrs. Smith. I think you need to come and assess her ASAP or transfer her to ICU before a pre arrest happens.”
• “I will be right in.”
• “Is there anything you would like me to do? Any labs, meds or a CXR in the meantime?”
• “Yes, do a STAT portable CXR, STAT lytes, CBC, Mg, Ca, Phos. And give her Lasix 80mg IV now.”
• “Thank You – in the meantime, I‟m calling CCOT to see the patient too.”
2012/12/21 22

2012/12/21 23
References
• Institute for Healthcare Improvement:
Kaiser Permanente of Colorado,
SBAR Technique for Communication: A
situational briefing model; www.ihi.org
• Lyer, Patricia, Med League Support Services,
Inc., :
Articles: Medical Errors – SBAR;
www.medleague.com
2012/12/21 23

2012/12/21 24
References cont’d
2012/12/21 24
• Cardiac Program, London Health Sciences Centre,
Creating a Healthy Workplace through
Employee Engagement: Implementation of the
SBAR Communication Tool;
powerpoint presentation; June 6-8,2007

2012/12/21 25
Thank you for your attention.
2012/12/21 25
Questions?