savvy caregiver advanced course trainer manual caregiver advanced trainer...program. participants...
TRANSCRIPT
Savvy Caregiver Advanced Course Trainer Manual
Ann O’Sullivan, OTR/L, LSW, FAOTA Kate Cole Fallon, MS, LCPC, NCC
Ken Hepburn, PhD Linda Samia, RN, PhD, CNL
December 2013
The project is sponsored by the Maine Office of Aging and Disability Services (OADS), Department of Health and Human Services, with funding from the
US Administration on Community Living

Savvy Caregiver Advanced Trainer Manual – December 2013
1
Savvy Caregiver Advanced Trainer Manual Table of Contents
Introduction, Fidelity and Core Elements …………………………….…………………………… 1
Maintaining Fidelity to the Program …………………………………………………….. 4 How Does a Savvy 1 Trainer Become a Savvy 2 Trainer? ………….……….….. 6
Handouts / Resources for Each Session ……………………………………………………………. 7 Session One ……………………………………………………………………………………………………… 9 Review of Models from Savvy 1…..……………………………………………………….. 12 Need-Driven Behavior Model ……………………………………………………………… 16 The Environment of Behavior ……………………………………………………………… 21 Savvy Concepts …………………………………………………………………………………… 25 The Problem Solving Process …………………………………………………………….… 26 The Impact of Caregiving on the Caregiver …………………………………………. 32 Try It Out ……………………………………………………………………………………………. 35 Session Two …………………………………………………………………………………………………… 36 How Did It Go? …………………………………………………………………………………… 36 Who’s on My Caregiving Team? ………………………………………………………….. 37 Strengthening the Care Team …………………………………………………………….. 41 Guiding Behavior in Activities of Daily Living ………………………………………. 46 Try It Out ……………………………………………………………………………………………. 49 Session Three ………………………………………………………………………………………………… 52 How Did It Go? …………………………………………………………………………………… 52 Caregiving Challenges ………………………………………………………………………… 54 Resources ………………………………………………………………………………………….. 61 Guiding Behavior in ADLs …………………………………………………………………… 62 Try It Out …………………………………………………………………………………….…….. 67 Session Four ………………………………………………………………………………………………….. 68 How Did It Go? …………………………………………………………………………………… 68 Guiding ADLs ……………………………………………………………………………………… 69 The Care Team …………………………………………………………………………………... 74 Challenges and Self-Care ………………………………………………………………….… 75 Program Re-Cap ……………………………………………………………………………….… 77 Maine Statewide Collaboration and Resources ……………………………………………… 85
Savvy Caregiver Advanced Trainer Manual – December 2013
1
Introduction, Fidelity and Core Elements Welcome to Savvy Caregiver Advanced! As a trainer for the original Savvy Caregiver program, you already know what a powerful impact that curriculum can have on family caregivers of people with dementia. We hope this manual will help guide and inform you as you add the Savvy Caregiver Advanced program (which we will be referring to as “Savvy 2”) to the training that you offer. The Savvy 2 program is an outgrowth of Maine’s success with the Savvy Caregiver (Savvy 1) program. Participants are caregivers who completed the Savvy 1 program at least 5 months previously, where the person with dementia continues to live in the community. Savvy 2 focuses on the challenges that are likely to be faced over time as dementia progresses. Like Savvy 1, Savvy 2 is a psychoeducational program. This means that it provides information and emphasizes skills and caregiver self-efficacy. Sessions incorporate practice and group reinforcement, meaning that people try things out and then get feedback. The course is experiential, and participants apply what they learn in class to their own situations. Classes are highly interactive, requiring active engagement in learning and practice and reinforcement of newly learned information / skills, and include debriefing and coaching as new skills are acquired. This form of training has been shown to be very effective. In fact, findings from Pinquart and Sorensen’s (2006) meta-analysis of caregiver interventions suggest that psychoeducational training had the broadest effect on caregiver outcomes. While both Savvy 1 and 2 can help caregivers of people with dementia, they are just two of the many caregiver resources that are available in the community. Trainers should be prepared to guide caregivers towards others supports and resources that may be helpful. It is also important that participants understand that Savvy 2, like Savvy 1, is not a support group, but is a training program. Caregivers often comment on their post-class evaluations that they want more time to share and discuss their situations with each other. Trainers can help them identify existing support groups to join or encourage them to form their own groups ongoing to meet this need. Virtual support groups are also an option for caregivers who prefer this means of connectivity. Where did the Savvy Caregiver Advanced program come from? When Maine began compiling feedback from caregivers who took Savvy 1, a number of responses indicated that caregivers would like additional training to address future needs, which led us to consider what might be helpful. A number of available interventions address caregiver symptoms of depression, stress and anxiety and are helpful in teaching skills that are adaptable. However, these tended to be focused on a specific point in the progression of care, and there seemed to be a need for responding to the ongoing training needs of caregivers.

Savvy Caregiver Advanced Trainer Manual – December 2013
2
To learn more, the evaluation team added a question about ongoing learning needs and preferences to the five-month follow-up surveys for Savvy 1. Nearly half of the respondents reported that their role had changed due to increased demands, and 78% requested additional caregiver training. Half of those individuals offered input on future content. Maine applied for, and was awarded, a second Administration on Aging (AoA, which is now under the umbrella of the Administration for Community Living, or ACL) grant in 2010, with a major goal being the development and refinement of an advanced Savvy Caregiver course, as well as the creation of replication materials (trainer and participant manuals and train-the-trainer program). How Was the Content Developed? While the initial information on the 5-month surveys confirmed that a need existed, more information was needed to refine the framework and content of the program. The University of Southern Maine (USM) researcher analyzed the feedback on surveys to inform focus groups, which were then held in all 5 AAA regions of the state, with 26 caregivers participating (Samia, 2012). Analysis of the focus group discussions showed that caregivers enjoyed the interactive problem-solving of the group related to preparing for the future, shaping the troubling behavior of the care recipient, reshaping the resource team, and caring for themselves. It supported the need for advanced training as caregivers move through the trajectory of caring for persons with dementia.
Identified themes included the following learning needs:
Knowledge and skills to manage new needs / problems (maintain mastery) o Dealing with more challenging and troubling behaviors o Applying the tools acquired in Savvy 1 to a changing situation o Enhancing skills to assess care recipient unmet needs (the meaning of behavior) and to
fit activities and expectations to the person’s ability as dementia progresses o Strengthening skills to achieve contented involvement as dementia continues o Paying attention to the effect of the caregiver on care recipient behavior
Strategies for late stage physical care and activities of daily living (ADLs) o Coping with increasing dependency o Managing resistance o Shifting from reacting to / correcting behavior to assessing the situation and using
nonverbal communication in order to prevent discomfort and troubling behavior
Tools and ideas for planning for the future and facing tough decisions
Strategies for enhancing communication with others o Examining and reshaping the care team o Navigating the formal resource system
Reinforcement of caregiver self-care o Creating awareness of the future loss of their caregiving self o Needing reinforcement of strategies
Savvy Caregiver Advanced Trainer Manual – December 2013
3
The learning needs identified in surveys and focus groups were then translated to an initial curriculum developed by Dr. Ken Hepburn, who developed the original Savvy Caregiver program. Southern Maine Agency on Aging (SMAA) and USM collaborated with him on creating materials and translating the curriculum to trainer notes. Dr. Hepburn came to Maine, offered a training to potential trainers, and got feedback. This was incorporated into the curriculum and SMAA delivered a pilot series to selected Savvy 1 alumni. The program was refined based on that group’s and trainers’ feedback, and the new version was piloted statewide, and then offered in all regions of the state. The resulting caregiver training structure has much in common with Savvy 1. It is also framed as a clinical training with all the elements of a psychoeducational program. The same eligibility requirements (family caregiver of a person with dementia who lives in the community) apply, with the addition of having completed a Savvy 1 course at least 5 months previously. The Savvy 2 series has four sessions, which are 2 hours each, and 6 – 10 caregivers take the class together. Savvy 2 addresses ADLs, caregiver self-care, future planning, and preparing for the challenges ahead. As with Savvy 1, caregivers are exposed to multiple models and strategies but the expectation is that caregivers will gravitate to the ones that best fit their situation and needs. The basic elements include:
A review of the strategies and models learned in Savvy 1
Introduction of additional models as frameworks for considering function and behavior o These models include
The Problem-Solving Process (Nursing Process Model) (Yura & Walsh, 1983) The Need-Driven Behavior Model (Need-Driven Dementia-Compromised
Behavior Model) (Algase, 1996) The Environment of Behavior model
In each session, the class walks through a different ADL, using the models. The curriculum is written using bathing, having a meal, dressing and toileting, although the trainer can incorporate a different activity if it is more relevant to the group.
Participants consider their caregiving teams, including evaluating who is helpful and who is not, considering who to bring in (formal and informal resources), and problem-solving how to ask for and receive help.
There is a strong focus on identifying and considering future challenges, including health care decision-making and options for end of life care. The types of grief that are often experienced by people assisting someone with dementia are considered, and coping strategies are suggested.
The importance of caregiver self-care, both in the present and in the future, is reinforced.
As with Savvy 1, participants are given suggestions about trying out strategies, and report back to the group for discussion and feedback.
As of August 31, 2013, 140 caregivers in Maine had participated in Savvy 2. Of these, 94% attended 3 or more sessions. Participants were overwhelmingly positive in their evaluation of

Savvy Caregiver Advanced Trainer Manual – December 2013
4
the SCP-2 training, with 94.3% strongly agreeing or agreeing that the training was relevant to their situation, 97.2% strongly agreeing or agreeing that the strategies suggested to them in the program were useful to them, and 97.2% strongly agreeing or agreeing that they would recommend the program to other caregivers. Caregivers complete pre- and post-surveys to measure the effectiveness of the program. The measures and tools are the same as those used in Savvy 1, and include:
Caregiver symptoms of depression: Center for Epidemiologic Studies Depression Scale (CES-D)
Caregiver mood: Bradburn Affect Scale
Caregiver competence (Pearlin, et al)
Personal control beliefs: Mastery (Pearlin, et al)
Personal gain (Pearlin, et al)
Self-efficacy (Steffin et al, Revised Scale for Caregiving Self-Efficacy) Results suggest statistically significant improvement in caregivers’ sense of personal gain derived from their caregiving situation, improved negative mood, enhanced sense of self-efficacy in their ability to respond to disruptive behavior and fewer depressive symptoms. Development of Trainer and Participant Manuals One of the AoA grant goals has been to develop tools to make the program replicable in other areas of the country. To help meet this goal, Kate Fallon and Ann O’Sullivan, master trainers at Southern Maine Agency on Aging (SMAA), contracted with the State of Maine to develop the train-the-trainer workshop for associate trainers, and the participant and trainer manuals. The draft manuals were reviewed by Drs. Ken Hepburn and Linda Samia. Participant manual drafts were then reviewed by several SMAA Savvy 2 alumni, and their feedback incorporated. Manuals and accompanying feedback forms were given to participants in four Savvy 2 classes in different parts of the state, leading to the final version. The trainer manual was given to Maine’s Savvy 2 master trainers for review and comment. The draft manual was given to associate trainees to read prior to the training workshop, and their feedback was also incorporated into this final version. Use of this trainer manual in the development of each trainer’s notes is an important way to ensure fidelity to the Savvy 2 program. Maintaining Fidelity to the Program When delivering the Savvy Caregiver Advanced program, it is critical that trainers maintain fidelity to the curriculum and to the core elements that make the program effective. Introducing new elements or leaving out program components may still provide a quality program, but it will not be the Savvy Caregiver Advanced program and should not be identified as such.

Savvy Caregiver Advanced Trainer Manual – December 2013
5
While individual trainers may use their own words and examples to teach the material, the program should be consistent with the training curriculum no matter who is teaching it. Under the AoA grant, specific mechanisms have been in place to monitor fidelity throughout the State of Maine. When the grant is completed, formal infrastructure may not be available for this. However, each agency delivering the program can consider how to monitor fidelity internally. This might include a trainer debriefing after each series, continued use of the fidelity tool, use of enhanced end-of-series evaluations, or other strategies to insure against program “creep”. Care must be taken to make sure new trainers receive standardized training, understand the curriculum, and have the knowledge and support needed to maintain fidelity to it. The term “core elements” refers to those program components that are key in delivering the program as written. Some are related to the structure of the course and some are related to content. Core elements of the Savvy Caregiver Advanced content include:
Developing understanding of advanced behavior guidance models and techniques to help caregivers as their person’s dementia progresses
Learning about several additional models for assessing their person’s behavior and developing more effective strategies for day-to-day care
Building awareness of resources available to help caregivers with advance care planning, end of life decision making, finding appropriate assistance and respite
Continuing to focus on self-care with an emphasis on redefining the care team
Following through on class material by participating in “Try It Out” activities between classes and reporting back on how things went
Following up on activities tried at home, with feedback from the trainer and the group on effectiveness and opportunities for improvement
Understanding the concept of “being comfortable” as an extension of contented involvement, which is introduced and applied to later stage dementia
Being introduced to the concept of self-advocacy when considering the emotional impact of caregiving (using the Feelings Quadrant)
Core elements of program delivery include:
The program is delivered in 4 two-hour sessions (total of 8 hours)
Classes have 6 – 12 participants
Each participant receives a participant manual and handouts o A list of all the handouts appears at the end of this section
Content for each session follows the trainer manual
Approved Savvy 2 slides are used for each session without additions or deletions
Each session is interactive with coaching
Classes are taught by a trainer who has completed the requirements as a Savvy 2 associate, master, or lead trainer
The Fidelity Checklist developed under the AoA grant can be used to help monitor fidelity. (See the Savvy 2 Policy and Procedure manual for information about this.) Agencies should continue

Savvy Caregiver Advanced Trainer Manual – December 2013
6
to use the end-of-series evaluation form, perhaps with some added specific questions, to ensure fidelity. Debriefing, group discussions, and/or collaboration across agencies may help trainers stay true to the curriculum. Refresher / development training might also be offered. How does a Savvy 1 trainer become a Savvy 2 trainer? Savvy Caregiver Advanced trainers start out as Savvy Caregiver trainers. The process for becoming a Savvy 2 associate trainer (AT) in Maine is similar to the process for becoming a Savvy 1 trainer. The first step is to observe a series being taught, to become familiar with the content and the types of discussion that arise from the group. Trainers can then read the trainer manual and take a Savvy 2 AT training session. After that, they co-teach a series, and then teach on one their own. The Savvy 2 Policy and Procedure manual explains this process in more detail. This trainer manual was developed to assist trainers in learning the Savvy 2 material. In the following sections, each session of the course is explained, with the applicable slides appearing in the text. It is important to read the material thoroughly prior to using it, but then to develop your own trainer notes, that are consistent with the curriculum but reflect your own style for delivery. The intent is not that the information in the manual be read aloud to the class. When developing your notes, consider that some participants may have low levels of literacy and / or health literacy, and use plain language to share the content. After teaching the course, go back to your training notes and reflect on what worked well and what could be improved, and revise your notes (while maintaining fidelity to the program) for next time. The Savvy Caregiver Advanced program has gotten strong positive feedback from experienced caregivers. Thank you for your part in supporting them as they take care of their person.
References
Algase, D, Beck, C, Kolanowski, A, Whall, A, Berent, S, Richards, K, Beattie, E. (1996) Need-driven dementia-compromised behavior: An alternative view of disruptive behavior. American Journal of Alzheimer’s Disease and Other Dementias. 11, 10-19.
Pinquart, M, & Sorensen, S (2006). Helping caregivers of persons with dementia: Which interventions work and how large are their effects? International Psychogeriatrics, 18, 577-595.
Samia, LW, Hepburn, KW & Nichols, L (2012) “Flying by the seat of our pants”: What dementia family caregivers want in an advanced savvy caregiver program. Research in Nursing & Health. 35, 598-609.
Yura, H & Walsh, MB (1983). The Nursing Process: Assessment, Planning, Implementing, Evaluating (3rd ed.). New York, NY: Appleton Century – Croft.

Savvy Caregiver Advanced Trainer Manual – December 2013
7
Handouts / Resources for Each Session
Training sites have electronic copies of the handouts developed for the program. Files and updates are available from the Office of Aging and Disability Services (OADS). Sources are included below for those that may be downloaded / ordered. Session 1:
Demographic data collection tools (if used)
Slide handouts
Caregiving challenges (immediate --> long term)
Behavior Log
Safety at Home for People with Dementia
Try It Out
Paper and pencils for floor plan Session 2:
Slide handouts
Guiding a Task
My Caregiving Team
Paper and pencils for care mapping Session 3:
Slide handout
Ongoing Loss: Ideas that May Help
Internet Resources / Free Internet Tools for Caregiver Communication (print back-to-back)
OOVL Decision-Making Tool
Legal and Financial Planning for People with Alzheimer’s Disease (NIA) http://www.nia.nih.gov/alzheimers/publication/legal-and-financial-planning-people-alzheimers-disease-fact-sheet
Connections books (available from OADS and AAAs)
Maine Hospice Council flyer about hospice (available from OADS)
Alzheimer’s Disease: Care and Support at the End of Life booklet (Dr. Laurel Coleman) (OADS) http://www.maine.gov/dhhs/oads/aging/alz/alzheimer/endoflife_web.pdf
End of Life: Helping with Comfort and Care booklet (NIA) http://www.nia.nih.gov/health/publication/end-life-helping-comfort-and-care
Agency on Aging resources: o Agency flyer o Information on living options, LTC assessments o Local resource information

Savvy Caregiver Advanced Trainer Manual – December 2013
8
Also useful, but optional:
Hospitalization Happens (NIA) http://www.nia.nih.gov/alzheimers/publication/hospitalization-happens
Pain in Dementia (AGS Foundation for Health in Aging) http://www.geriatricpain.org/Content/Education/Patient/Documents/Pain%20in%20Dementia.pdf
Session 4:
Slides handout
Class evaluation form
Certificates
Savvy Caregiver Advanced Trainer Manual – December 2013
9
Session One
Materials needed:
Extra pre-survey forms
Demographics data collection tools, if used
2012 replacement pages to update Savvy 1 manual (if applicable)
Flip chart, with pages prepared as indicated in notes
Slide handouts
Plain paper and colored pencils
Behavior Log handout
Safety at Home for People with Dementia handout
Caregiving Challenges handout
Try It Out sheet
Savvy Caregiver Advanced participant manual
o A NOTE ABOUT THE PARTICIPANT MANUAL: The Savvy 1 participant manual was
designed to generally correspond to the content of each session sequentially. In Savvy
2, some topics, such as guiding activities of daily living, are addressed in multiple
sessions. In an effort to make the participant manual most useful as an ongoing
resource, it is organized by topic, rather than by session. This will enable caregivers to
easily locate the information they need when they refer to it in the future.
o This trainer manual includes references to the relevant pages in the participant
manual, so that trainers can point them out in class.
Appendix materials for participant manual
o The participant manual includes an appendix of supporting resource materials with
links to their sources. Each trainer/agency is responsible for printing these out, and
including them in the participant manual materials.
Your group will be comprised of seasoned Savvy participants. Assure them this series will
operate in a very similar fashion. Encourage people to be comfortable and practice good self-
care.
All are strongly encouraged to attend all four sessions but if they can’t, share protocol for
cancellation and for bad weather.
As with Savvy 1, session one is information dense. Participation is most welcome but we once
again want to be sure we are all starting in the same place. Sessions 2 - 4 are much more
interactive.
As always, trainers will be the “time witches” to be sure we stay on task and finish on time.

Savvy Caregiver Advanced Trainer Manual – December 2013
10
Remind them that they will have opportunity to practice at home and emphasize the
importance of the Try It Out activities (this might prompt them early on in the session to think
about which strategies they want to try at home as they are being reviewed / introduced).
Overview Slide (20 minutes, including introductions)
It is helpful to offer some explanation about how and why the Savvy Caregiver advanced class
(Savvy 2) was developed. As mentioned in the Introduction section, it became clear through post-
surveys that caregivers had found Savvy 1 to be very effective but they were looking for
something further. The investigator from USM invited Savvy 1 graduates to focus groups
statewide and the feedback received formed the foundation of Savvy 2.
Highlights from the focus group results:
The state-wide focus groups identified three main themes which guide the program.
This advanced training will introduce participants to material that is new to them. It will tie in
with material from Savvy 1 and it will depend on their knowledge of the Savvy material.
The three areas identified in the slide will be emphasized across the four sessions of the
program.
The three areas and their goals are:
o Behavior: Participants will be able to guide and structure the day-to-day behavior of
persons in more advanced stages of their cognitive loss.
o Resources: Participants will be able to analyze their need for help in caregiving and
will acquire skills and information to help them better meet those needs.
o Challenges: Caregivers will continue to appreciate the potential emotional impact of
caregiving, be able to use techniques to find positives in their caregiving, recognize the
kinds of challenges they may face, and obtain information about ways to face and
resources that might help them to face these challenges.
Savvy Caregiver Advanced Trainer Manual – December 2013
11
Dr. Ken Hepburn, who developed the original Savvy Caregiver series, built the framework for the
training. The researcher at USM and Master Trainers at SMAA worked with Ken to create a series
that was piloted to a select group of Savvy 1 graduates willing to offer constructive feedback in
order to then rework the material. At that point the program was piloted state-wide and has
been offered ongoing since.
The overarching aim of this first session is to offer additional frameworks for caregivers to draw
from in order to better and more efficiently guide and shape behavior. The review of previous
Savvy models is an opportunity to bring everyone onto the same page again, and to highlight how
all these models work together. The overview of the Problem Solving Process is where all the
pieces start to really fit together. Finally, participants will have the chance to consider the
challenges they are facing and how important self-care still is. This opens the door to finding
resources and asking for help, which we will explore in later sessions.
As far as focusing on addressing behavioral issues, Teri’s ABC model is a straightforward way to
think about behavior in general, and it serves as a very good way to perform the first step of the
Problem Solving Process, namely to assess behavior. Other Savvy 1 principles – Fit, the Anchors
of Contented Involvement, and the impact of confusion – are useful in planning and
implementing a behavior guiding or re-establishing strategy, and for then evaluating the
effectiveness of that strategy. In the current program we want participants to develop keener
skills of behavioral assessment and analysis, so we will reintroduce the guiding principles of the
original Savvy.
Introductions
Your name
Who are you providing care for?
About how much of each day do you spend
caregiving?
Introductions
This exercise begins the formation of a group, so it is important to foster respectful listening
and interaction, without letting the process take on a support group dynamic. The main point
of this portion is to establish the broad outlines of the caregiving that is currently going on.
Remind people gently that time is limited and use simplified Introduction slide (above). Guide
them to just answer the questions as there will be time for more exchange a bit later.
If it helps to move things along – and also to keep things in memory – you could use a flip
chart in this activity.

Savvy Caregiver Advanced Trainer Manual – December 2013
12
Review of Models of Behavior
from the
Savvy Caregiver Program
Review of Models from Savvy Caregiver (10-15 minutes)
Found in participant manual pages 3 – 8 and Savvy 1 manual
The introduction slide leads to 10 slides from original Savvy.
We will be referring back to many of these themes as the series progresses.
With each slide, remind participants about the key or central concept and where relevant, the
teaching exercise from the original Savvy program. Some participation might be helpful to
see how people are using the concepts.
The facilitator’s task, from group to group, will be to reinforce the strategies participants are
using and encourage them to tap back into all of them ongoing.
This portion should serve to remind participants about the key ideas and to establish
language shorthand terms for ideas that you will want to use in subsequent parts of the
program. It offers a “refresher” for the language of Savvy.
Be mindful of time. This review is brief. Be sure to leave enough time for new information
that follows. Keep explanations simple.
Slides to review:
o Contented Involvement/over and under stimulation. As we begin to address issues
involved in later stage care, we introduce the concept of “being comfortable” as part
of contented involvement. In more advanced dementia, comfort will be a more
appropriate measure of how things are going, and will be a reasonable goal of care.

Savvy Caregiver Advanced Trainer Manual – December 2013
13
o Confusion is always a possibility. Here we see all the elements of thought affected by
dementia. Remind participants of the driving in snow exercise from Savvy 1.
o Confusion Discomfort Behavior
o ABC Model (Linda Teri). All behavior has meaning.
Savvy Caregiver Advanced Trainer Manual – December 2013
14
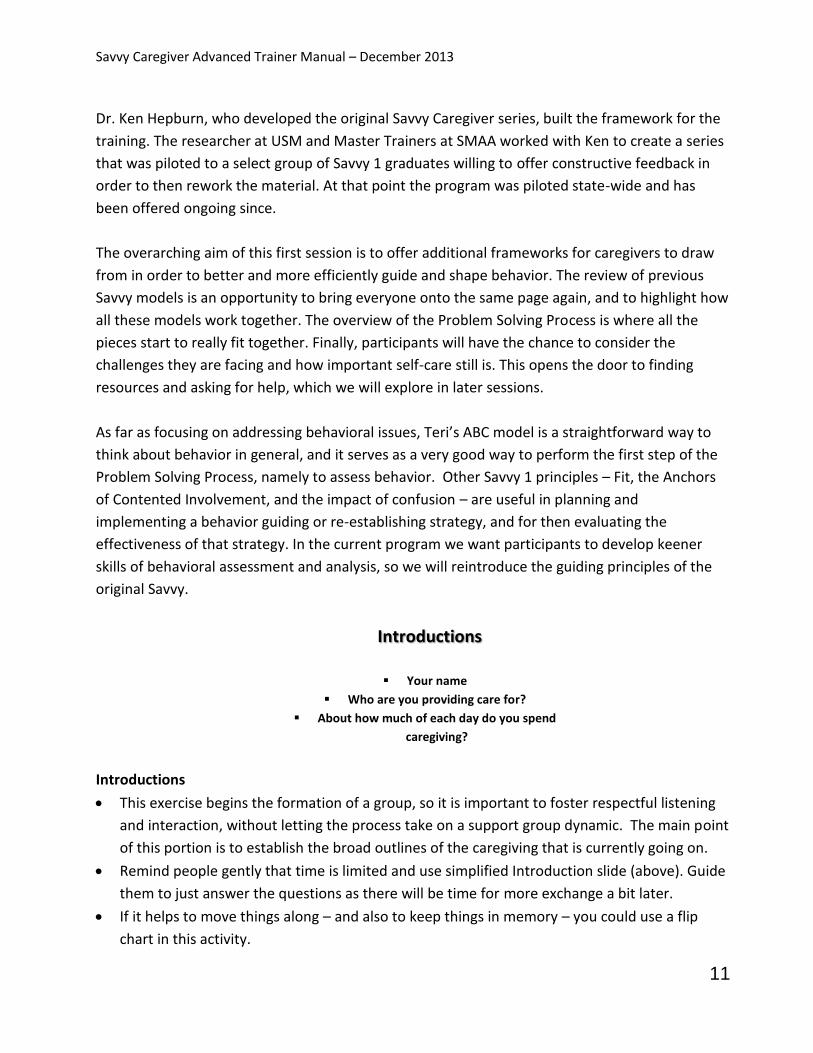
o Person-Others-Surroundings. The key here is that the person with dementia is
gradually less in control of their own behavior.
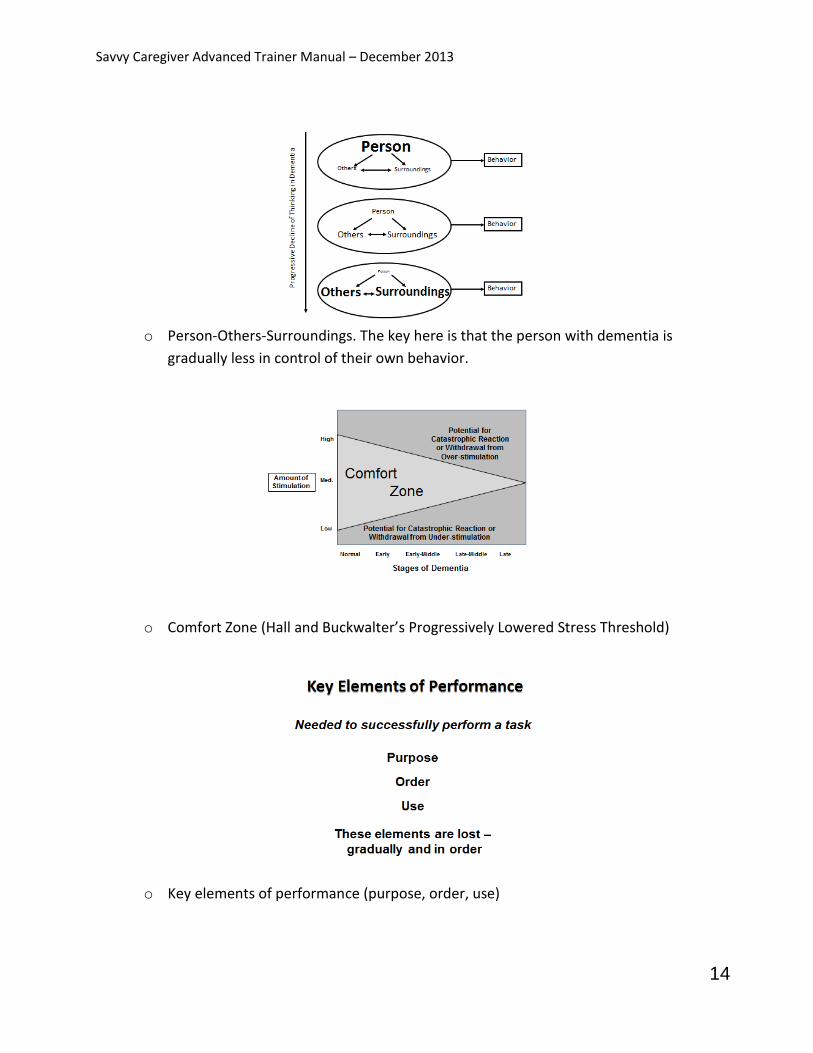
o Comfort Zone (Hall and Buckwalter’s Progressively Lowered Stress Threshold)
o Key elements of performance (purpose, order, use)
Savvy Caregiver Advanced Trainer Manual – December 2013
15
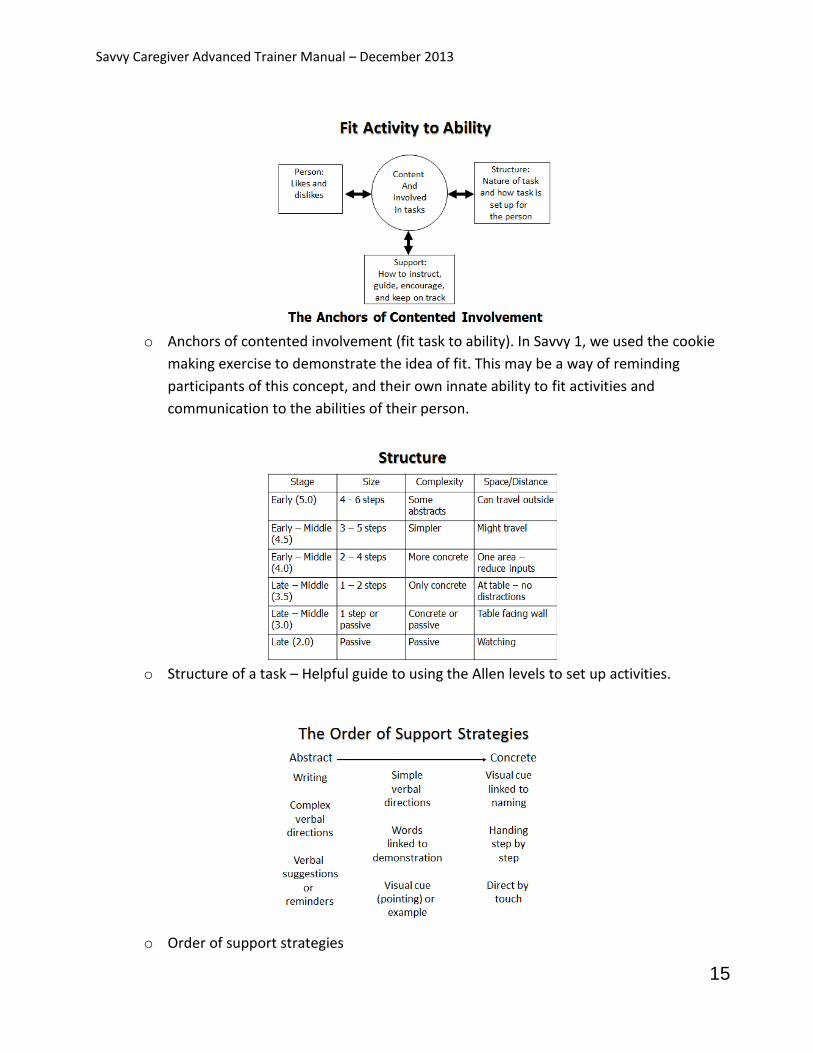
o Anchors of contented involvement (fit task to ability). In Savvy 1, we used the cookie
making exercise to demonstrate the idea of fit. This may be a way of reminding
participants of this concept, and their own innate ability to fit activities and
communication to the abilities of their person.
o Structure of a task – Helpful guide to using the Allen levels to set up activities.
o Order of support strategies

Savvy Caregiver Advanced Trainer Manual – December 2013
16
Mention that we will be building on their understanding of all of these concepts in a way that
will connect and enhance them.
Remind participants that all these models are covered in the Savvy 1 caregiver manual.
Reviewing the information in this manual occasionally, if they aren’t already, may be very
helpful.
Transition: Introducing Models of Behavior
Need-Driven Behavior
The quick review of the Savvy 1 material is over, and now you begin to move into the new
material that is being introduced in the Savvy 2 program. The majority of the new material
focuses on conceptual models that provide ways of understanding and guiding behavior.
There is no expectation that everyone will always utilize every model. People will likely find one
or two that resonate with them and default to them. Be sure participants understand that this is
fine. They are encouraged to take what works for them, and leave what doesn’t. Emphasize that
models are simply frameworks for understanding the person and developing strategies. If
participants use them as part of their clinical outlook, they will become automatic over time.
All of the behavior models in the Savvy Caregiver programs provide ways for the caregiver to
conduct an assessment, to formulate a strategy, to evaluate the strategy, and then to re-assess
and reformulate, if needed, based on this evaluation. What is important is that caregivers leave
the program with confidence in and a sense of competence with some process that 1) takes all of
these elements into account and 2) appreciates that the process is cyclic and on-going. It is not
necessary that they know the names of the models, and we are not advocating one model over
any others.
Need Driven Behavior Model
Found in participant manual pages 9-11
We are now presenting new information. Remind participants that these new models are only to
reinforce what they already know, and to offer them another way of identifying what is
influencing behavior and designing strategies. By the end of session one, we will have a thorough
overview of how to observe and analyze behavior in order to plan for more successful strategies.

Savvy Caregiver Advanced Trainer Manual – December 2013
17
Need Driven Behavior Model (Overview) (15-20 minutes)
Background information: This addresses the core theme of behavior guidance and structuring, as
mentioned in the focus groups.
This model (pioneered by Dr. Donna Algase) is based on the idea that the unexpected and often
troubling behaviors in which persons with dementia engage represent attempts at
communication. The disease progressively erodes a person’s ability to identify a negative
stimulus and, eventually, even to recognize that there is such a stimulus. It also erodes a person’s
capacity to effectively communicate when something is bothering them or what it is. So behavior
can be seen as the expression of an unstated need.
The needs-based model and the ABC model share many attributes. However, the way one model
speaks about behavior may be more appealing to some people than the way the other model
speaks of it, so this is a way to be sure people leave the program as equipped as possible.
This model recognizes that some things (Background Factors) that might contribute to behavior
are things over which the caregiver has no control. It also recognizes that as dementing diseases
progress, their progression has increasing influence on behavior. This is very consistent with
everything participants have learned in Savvy 1. Finally it recognizes that these background
factors have bearing on the current factors in the situation over which the caregiver does have a
degree of control. Both background factors and current factors (discussed in more detail below)
influence behavior – and behavior is a form of communication.
It is important to point out that, while the model appears focused on what might be called
troubling behaviors, it is more general in nature and can be used to structure and guide any
activity as part of the Problem Solving Process, which we will cover later in this session. This is
one more approach to looking at any puzzling behavior and seeing the meaning behind it.
Savvy Caregiver Advanced Trainer Manual – December 2013
18
Unexpected Behaviors
Physical
Verbal
Emotional
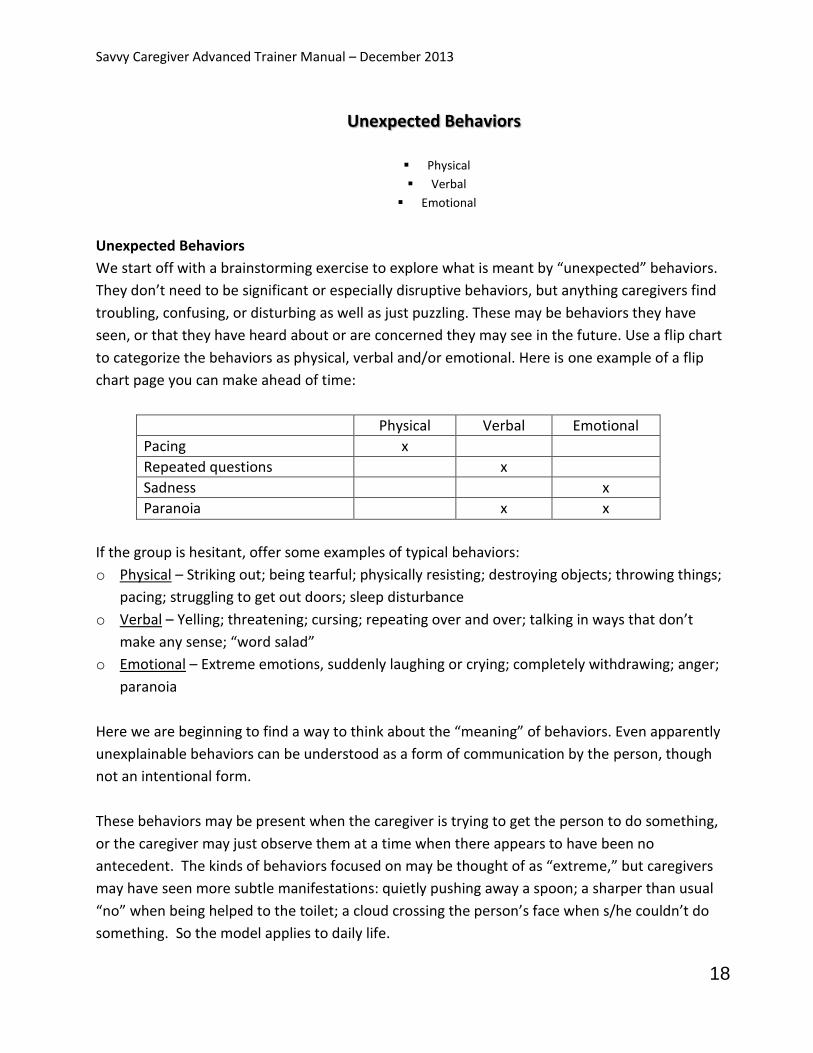
Unexpected Behaviors
We start off with a brainstorming exercise to explore what is meant by “unexpected” behaviors.
They don’t need to be significant or especially disruptive behaviors, but anything caregivers find
troubling, confusing, or disturbing as well as just puzzling. These may be behaviors they have
seen, or that they have heard about or are concerned they may see in the future. Use a flip chart
to categorize the behaviors as physical, verbal and/or emotional. Here is one example of a flip
chart page you can make ahead of time:
Physical Verbal Emotional
Pacing x
Repeated questions x
Sadness x
Paranoia x x
If the group is hesitant, offer some examples of typical behaviors:
o Physical – Striking out; being tearful; physically resisting; destroying objects; throwing things;
pacing; struggling to get out doors; sleep disturbance
o Verbal – Yelling; threatening; cursing; repeating over and over; talking in ways that don’t
make any sense; “word salad”
o Emotional – Extreme emotions, suddenly laughing or crying; completely withdrawing; anger;
paranoia
Here we are beginning to find a way to think about the “meaning” of behaviors. Even apparently
unexplainable behaviors can be understood as a form of communication by the person, though
not an intentional form.
These behaviors may be present when the caregiver is trying to get the person to do something,
or the caregiver may just observe them at a time when there appears to have been no
antecedent. The kinds of behaviors focused on may be thought of as “extreme,” but caregivers
may have seen more subtle manifestations: quietly pushing away a spoon; a sharper than usual
“no” when being helped to the toilet; a cloud crossing the person’s face when s/he couldn’t do
something. So the model applies to daily life.
Savvy Caregiver Advanced Trainer Manual – December 2013
19
Background Factors
There are background factors that may affect behavior and may also have an influence on current
factors, contributing to the kinds of behaviors that caregivers find troubling or difficult. These all
can be taken into account in the assessment of behavior.
Go through each of the background factors, asking participants if they have examples that offer
specifics of the broad concept of background factors. If none are forthcoming, have some
examples of each to offer in order to make the concept clearer.
Dementia stage: Savvy participants likely appreciate the impact of the declining powers
associated with dementia progression. The increased possibility of confusion, the progression to
another stage of the illness and the corresponding decreased capacity to perform daily tasks
increases the likelihood that any request to engage in a task may bring on an unexpected
behavior.
Health problems: As dementia progresses, people become less aware of their own discomfort
and less able to report that something “feels wrong.” Sensory losses (hearing, vision) can also
progress. A person’s underlying health issues may affect their ability to participate in an activity.
For instance, a person with dementia might resist going upstairs for a shower because the
arthritis in his/her knee becomes painful while climbing stairs
Personality: Research suggests that people who were “difficult” and had non-agreeable
personalities earlier in their lives may be more likely to be difficult and disagreeable as their
dementia progresses. A person with a strong sense of privacy may be uncomfortable being
assisted with bathing or toileting.
Neurological problems: Pain and other coexisting diseases like Parkinson’s need to be
considered.
Life history: Troubling events from the past along with previous patterns of difficult behavior
may be influencing behavior in the present. Encourage participants to revisit personal history to
consider otherwise unexplainable behavior. Note that past trauma may become a trigger.

Savvy Caregiver Advanced Trainer Manual – December 2013
20
These factors cannot be changed but caregiver awareness about them may guide strategies for
dealing with them.
Current Life Factors
These are factors that may impact behavior which caregivers can assess and, once understood,
may be addressed to improve behavior. Encourage participants to direct their energy toward
things they have the power to change.
Bodily needs: Consider this first as it becomes more and more difficult for people with dementia
to identify and report discomfort. Consider hunger, thirst, fatigue, dehydration. Might there be a
reaction to medications, pain, constipation, or change in diet? Do they need to use the
bathroom? Consider also infections, sore throat, urinary tract infection (UTI), etc. In addition, a
background factor like arthritis may create a current factor of pain. As in the example above, pain
may be creating an unexpected behavior of resistance to bathing.
Emotional needs: Again, behavior is a form of communication. Consider all the feeling states
likely to be experienced in someone with dementia, like fear, isolation, sadness, frustration. And
then consider that they are unable to recognize or communicate this. Studies have shown that
comfort items can help to create calm. This may include stuffed animals or dolls, a soft throw,
prayer beads, or even a purse. Also note that a background factor like incontinence may create a
current factor like embarrassment.
Physical environment: Consider how the environment is impacting behavior (person-others-
surroundings). Might it be too stimulating, or not stimulating enough? Is there too much clutter,
or noise? Is it too hot, or cold, or bright?
Interpersonal environment: How might the person be reading the caregiver? It is very likely that
people at advanced stages of the disease have strong emotional radar. They can read or pick up
on what those who are helping them are feeling. So, if a caregiver is feeling frustrated or hurried
or impatient, the person may well get this message and react to it. Everyone feels like this at
some point. Assure participants there is no need to beat themselves up over this, just be sure to
account for it as a factor.

Savvy Caregiver Advanced Trainer Manual – December 2013
21
One additional note: emphasize that sudden changes may signal serious physical problems that
the person cannot report on. These can include broken bones, serious infections, or even heart
attacks.
NOTE: The slide showing the Need-Driven model is repeated here to illustrate how the pieces fit
together.
The Environment of Behavior – Intro slide (15-20 minutes)
Found in participant manual pages 11-14
This section is meant to sensitize participants to the effect of both the home and the social
environment on the person, especially as dementia progresses. Although there is an emphasis on
structure in the anchors of contented involvement, here we look at the broader environment, the
living space of the person and caregiver. The object of the exercise will be to identify if there are
elements of the home environment or activities within it that need to be modified in order to
promote greater calm and foster contented involvement.
The program now shifts to directly consider the impact of the environment on behavior. Point out
that the environment has been a factor all along, though not explicitly. When Savvy speaks of
structure (as in structure and support), it addresses not only the set-up of a task or activity but
Savvy Caregiver Advanced Trainer Manual – December 2013
22
the specific location or environment of that activity. The environment can also provide
antecedent stimuli for unexpected behaviors (in the ABC model).
As the person’s own capacity for directing behavior decreases, the power of the surroundings to
shape behavior increases (person-others-surroundings). The physical environment is included in
the current life factors of the Need-Driven model, but now we look at the environment more
thoroughly.
We will consider safety issues as well, but it’s more than a scan of the area. It is a serious effort to
incorporate place and space into the models of behavior guidance we cover in both Savvy 1 and
2. The environment has to be examined in terms of the potential threats it harbors as well as in
terms of the safeguards that are built into it that assure the safety of the individual.
Now that we have considered background and current factors as antecedents to behavior, we will
also look at how the environment can stimulate and respond to behavior. Remind participants
too about the “person-others-surroundings” model and how environment becomes a significant
factor.
Where Care Occurs
Think about where care takes place
What happens where?
Unused spaces?
Spaces for transitions?
Where Care Occurs
Have blank paper and colored pencils available
The purpose of this exercise is to bring awareness to the patterns of use in the environment.
Encourage people to work on this throughout the exercise. Outlining the living space on paper is
helpful though not essential. Invite them to draw a floor plan or even make a list of spaces. The
key is to get people to think about the space they are in regularly, and to incorporate that space
into the way they think about behavior guidance.
Guide participants to consider the space of their daily lives. Offer a couple of minutes for them to
make notes. Talk them through thinking about their spaces, being sure to include their home,
useable outdoor spaces (patios, screened porches, gardens), basements, attics, garages and cars.
Be sure they consider any space where they and/or their person go on a regular basis.
Savvy Caregiver Advanced Trainer Manual – December 2013
23
Then move on to transition spaces: walkways, hallways, and stairs. How does their person react
to these spaces? Are they neutral or do they create either positive or negative reactions?
Once they have a sense of all the spaces they use, ask them to make note of where activities of
daily living (ADLs) take place. What about other activities? Be sure to explain that ADLs are
eating, dressing, bathing, toileting and transferring. Although we focus our discussions largely on
ADLs in this series, the models apply to any activity.
Are there spots that their person is drawn to? Are there places where activities typically go very
well? What about places where activities are particularly challenging? Give them a few moments
to ponder all these options and to make some drawings or notes. They are being asked to think
about things from a new perspective.
Trouble Spots and Comfort Spots
Open the subject up for discussion. Ask if anyone noticed any patterns. Did anyone observe any
places where there is a pattern of cooperation, or resistance? Are there certain places where
their person likes to be?
Where do there tend to be behavior difficulties? Are there any surprises? Encourage discussion
about successes. Remind them that comfort spots can be important antecedents to behavior
guidance and shaping, and these may be places to try out activities that tend to be more difficult.
Environmental Factors
Accommodation
Simplicity
Focus
Reinforcement

Savvy Caregiver Advanced Trainer Manual – December 2013
24
Environmental Factors
As participants begin to take control of the environment in order to guide and shape behavior,
there are some basic helpful strategies they can use:
Accommodate: Consider sensory losses, both in the environment and in the approach to care.
Light and sound impact how one experiences an activity, as does room temperature. Consider
how vision or hearing losses affect the person’s ability to understand and attend to activities.
Simplify: Reduce distractions, which have a greater impact as dementia progresses. The
demands of a “busy” environment can compete with a caregiver’s efforts to guide the person
through a task or activity.
Focus: Even when a task is simplified, sitting facing a window will create a challenge to
attention. A narrower view of the environment will promote greater engagement.
Reinforce: Elements in the environment can be used deliberately to promote engagement in
a task or activity. Smells of cooking to increase appetite; running water to support bathing or
toileting; clothes laid out to encourage dressing.
Putting it All Together
Optimize spaces for behavior
Avoid trouble spots
Change environments
Putting it All Together
Here you can pull the threads of the exercise together. This may be done as a group discussion or
as a guided overview. Go with what works best for each group.
Participants may have identified a challenging space, or you can focus on the bathroom and the
activity of washing up.
Spaces for activities can be optimized as caregivers become more flexible in terms of thinking
about where activities can take place:
Is this the place where this task usually occurs?
Is this a comfort spot or a trouble spot for the person?
Has the place been set up to make it easy to do the task?
Is there is anything about getting to the place that may produce discomfort in the individual?
Are there effective stimuli in the environment?
Is the transitional space in any way producing agitation or serving as a distraction?
Do they have to go past unused spaces to get to the place and, if so, do these spaces have any
“meaning” for the person that may agitate or distract?
Savvy Caregiver Advanced Trainer Manual – December 2013
25
Once in the space, are there distractions (unnecessary noises, mirror, etc.)?
How is lighting and temperature?
If this is a trouble spot, can the task be done elsewhere?
Let participants know that scanning (and, where appropriate, making changes in) the
environment of care will be part of the “Try it Out” home exercise this coming week.
Safety
During task performance
Within the general environment
General safety concerns
Safety
Safety was mentioned in the original Savvy series, but now safety issues are likely more
significant. It is more important than ever to scour the environment for safety hazards (clutter,
inadequate lighting, sharp or hot items...) and to remove them; this then becomes the new
environment within which behavior is guided.
The environment should minimize the risk of wandering. If the person paces, is there a safe and
accessible place for that, both indoors and out? Would the caregiver be alerted if an exit door
was opened? If there are stairs in the house and there is uncertainty about the person’s ability to
navigate them safely, are they adequately blocked?
What are acceptable and unacceptable risks and what resources can the caregiver access to make
decisions about these risks? Give out Home Safety handout. Encourage participants to look into
Safe Return, GPS technology, and to notify local emergency personnel that their person has
dementia.
Savvy Concepts
As a trainer, it is useful to consider how all the various models fit together. Savvy Caregiver
teaches caregivers about many models of behavior. In Savvy 1, models form a framework to think
about behavior and structure activities. In Savvy 2, we have the opportunity to start with the
basic Savvy models, add to them and then pull all the threads together into a tapestry of behavior
guidance.
The ABC model was covered in Savvy 1 but it is central in Savvy 2. Many of the models we use
support the ABC model. The heart of the ABC model is the antecedent, which is something to
address in order to support behavior, as well as something to reflect on when things go off track.
Savvy Caregiver Advanced Trainer Manual – December 2013
26
As you teach Savvy 2, and especially as you walk through the Problem Solving Process in each
session, continue to use the ABC model as an anchor for the other models.
Consider how all the models we reference provide a way to evaluate antecedents:
Background factors
Current factors
Comfort spots/trouble spots – the environment of behavior
The Anchors of Contented Involvement (likes / dislikes; skills)
Person-Others-Surroundings
Structure and support strategies
The caregiver him/herself
The Assessment step of the Problem Solving Process offers an opportunity to consider all these
pieces which need to be considered to some extent in order to determine the meaning behind
behavior and to select strategies for responding. Although caregivers are not expected to walk
through all these models each time, our goal is to familiarize them with all of them in order to
offer as many helpful tools as possible.
Along with raising their awareness of the many factors that act as antecedents, encourage
caregivers to focus on the elements they have the most power to change: Current factors,
structure and support strategies, the environment, and their own approach to a task can all be
adjusted to guide behavior.
Problem Solving Process (overview) (20 minutes)
Found in caregiver manual pages 16-20
As a framework to pull all these models together, we will use the Problem Solving Process, a basic
model used by nurses and other healthcare professionals. This is a cyclical framework in which an
assessment-based plan is put into action and then reviewed, providing more information about
the situation. This information contributes to the next assessment and a revised plan – and so

Savvy Caregiver Advanced Trainer Manual – December 2013
27
on. This is the final new strategy we will be incorporating but it is the one that allows us to pull
all the other pieces together. Be sure to mention where models enhance each other as you walk
through this process model. For example, thinking about Background Factors (from the Need-
Driven Model) that might contribute to an unexpected behavior is a form of assessment; so too is
thinking about “trouble spots,” as is done in the environmental model.
Unexpected and troubling behaviors, as well as contented involvement, occur within the context
of activities that include set up, assistance, communication, guidance, and reinforcement. It’s up
to the caregiver to guide behavior and to maintain / re-establish contented involvement on an
ongoing basis. We are considering behavior from many angles because it is seldom a single event.
It’s up to the caregiver to maintain or alter the context to guide behavior. All the models offer
frameworks for looking at the root of behavior and adjusting for it.
Problem Solving Process
This model is just another component of the caregiver’s toolbox. The intent, in providing them
with instruction in the model, is for participants to keep it in mind as a way of approaching
caregiving situations in general. Again, they only need to utilize a model if it resonates for them
and if they find it useful.
Here we more fully describe the pattern of the Problem Solving Process model. This framework
may be used to design caregiving strategies. Start with an overview of the process model step by
step:
Assess: Examine the situation. Determine what is happening. Consider what might have
produced the situation. Be very specific. Adopt a clinical outlook; step back.
Plan: Make a plan of action, based on the assessment including what they know about their
person and what they think is going on in the situation.
Implement: Follow the plan of action as carefully as possible, and make note of how things
go. Be flexible here. Make notes.

Savvy Caregiver Advanced Trainer Manual – December 2013
28
Evaluate: How did it go? If successful, try to understand why it worked and repeat this. If
there are problems, or it just didn’t work, examine what happened. When did it break down?
Was there some trigger? Some point of resistance? If so, what? Use all these observations
in the “Assess” and Plan” portions of the next cycle of the Problem-Solving Process.
Now, walk through each step in the process using the example of developing a strategy for
getting dressed. This will help clarify how the process works. We will focus each week on one
activity of daily living (ADL). Remind them again what ADL stands for and what they are.
Step 1: Assess
Assessment involves standing back and producing as detailed a description as possible of what
has happened in prior dressing activities, especially those that became challenging and those that
went smoothly. This means moving past a caregiver’s own reaction to the situation and moving
past putting a label or a motive on it and looking as carefully and dispassionately as possible at
the action itself. “What happened?” rather than “why did it happen?”
For example, if a participant cites a challenging experience when the person would not get
dressed, it is not enough to leave it at: “She just refused; she was being stubborn.” This labels the
behavior. From the perspective of assessment, the fact that the person would not participate in a
task associated with dressing is just the beginning. What, exactly, was the task? Was it to follow
an instruction to get dressed? Was it to cooperate at all with dressing? Was it that the task was
begun but stopped in the middle? When the task started, what happened? What did the person
do? Just exactly what did happen? Once the “exactly” part is established, the next question is
what was happening just before the task started to go awry? Did the person already seem out of
sorts or uncomfortable? Or was there an “external antecedent,”? How did the caregiver approach
the person? How was the caregiver feeling? Was the person engaged in something else and
initiating this task was an interruption? Was something else going on in the environment?
Savvy Caregiver Advanced Trainer Manual – December 2013
29
Was the design of the task itself a problematic antecedent? Was it too demanding, given where
the person is in the disease or how they were feeling at the time?
Is this an essential task? If it is not, might it be eliminated? Or might the task be structured so
the person can be successfully engaged in just part of the task?
Encourage participants to consider: antecedents and behaviors based on ABC; background and
current factors; person-others-surroundings; progressively lowered stress threshold.
An important point to make regarding a person’s behavior in all tasks and activities is that disease
progression is always a factor that needs to be considered. Has the disease progressed so that a
task or activity that used to fit the person’s abilities no longer does? Participants may need to
revisit the Allen levels and where they think their person currently fits. Again, refer back to the
original Savvy Caregiver manual for this information, and encourage participants to go back to the
overview of the Allen levels each time their person’s abilities seem to change.
Step 2: Plan
Now participants can prepare for how they want things to go as they plan the dressing activity.
First they need to address any issues that arose as part of the assessment step. Be sure internal
antecedents are addressed prior to beginning the task (hunger, thirst, fatigue, pain).
Then they need to think about how well the task fits the person in terms of their current
dementia stage. Should the task be simplified? Should different kinds of set up and support be
tried? Is the task being done in the right place? Are there things about the environment possibly
interfering? And can these be changed?
As participants consider their strategy, it is relevant to ask whether the task design respects the
person’s remaining abilities to act independently – or whether it represents an infringement on
existing capacities (where too much is being taken away). Are there any safety concerns? Are
there overlearned or familiar behaviors you can tap into for success?
Savvy Caregiver Advanced Trainer Manual – December 2013
30
As an external antecedent, is the caregiver clear about how much time this task is likely to take?
Not understanding this can lead to impatience, a signal the person will almost certainly pick up.
Just what will the caregiver say and/or do to initiate the task? If there is a verbal cue, will it “fit”
the person’s ability to understand it? What kind of visual cue might work well?
Step 3: Implement
The implementation step entails carrying out the plan – but being ready to alter it, in mid-course,
if need be. This is not an exercise in rigidity. If the plan starts to break down in places, encourage
participants to make changes that seem to fit the moment. As caregivers they are likely familiar
with needing to be flexible.
What is important is for them to have an idea, going in, about what kind of behavior they are
seeking. What are the caregiver’s expectations about how the task will go and what the person
will be like as they go through and complete the task? What do they most want to accomplish?
Caregivers will need to be very observant about what is working and what is not working, and
what alternatives are tried and how they work. At the same time, if alternatives are tried, how
does the person seem to be responding to them? It is very possible that setting a plan in motion
is just a way for the caregiver and the person to work out a better plan.
A good outcome is achieving some level of cooperation and participation, and some evidence
that the task is proceeding comfortably, without agitation or resistance.
Savvy Caregiver Advanced Trainer Manual – December 2013
31
Step 4: Evaluate
This final step provides the information needed to start the assessment process again. This is the
“How did it go?” and “What did I learn?” step.
If the plan went well, encourage participants to reflect on the implementation process in order to
examine more closely their own actions, behaviors, and emotional tone and the person’s
responses and specific behaviors. This helps to develop a better sense of what worked.
If things didn’t go exactly as planned, how did the person behave? What did they seem to be
communicating? What did that behavior mean? Is it possible to match previously mentioned, or
perhaps previously unnoticed, antecedents to difficulties that cropped up in implementation?
Remind them again of the ABC model and to look back to what happened just before things went
off course.
If the caregiver had to make adjustments during implementation, what were they and how did
they work? What seemed to work; what seemed not to work? Were they able to monitor their
own behavior while improvising? And how did their person react? Any and all information
gathered feeds back into the next step of assessment again. The cycle begins anew with
everything learned from this process.
If, as a trainer, you would like to read additional tips specific to dressing, information is available
from NIA at
http://www.nia.nih.gov/sites/default/files/sites/default/files/alzheimers_caregiving_tips_groomi
ng_and_dressing_0.pdf and from the Alzheimer’s Association at
http://www.alz.org/care/alzheimers-dementia-dressing.asp#dressing
Savvy Caregiver Advanced Trainer Manual – December 2013
32
The Impact of
Caregiving on the
Caregiver
The Impact of Caregiving on the Caregiver (25 minutes)
Found in participant manual pages 33-35
This is a final group exercise to help participants start to see the toll their current caregiving is
taking on them.
Caregiving Challenges
What is the most difficult challenge you face
right now in taking care of your person?
Caregiving Challenges
Pass around the Caregiving Challenges worksheet. Ask them to work on the first question, listing
what are the greatest challenges they are facing in their caregiving at this point. Give them 2-3
minutes to make some notes. Mention that they will be invited to continue to work on this
handout throughout the 4 weeks.
Prepare a FLIP CHART page beforehand where you can list challenges. Add three columns on the
right to list the three core themes of the program: difficult behavior; resources; practical and
emotional challenges. Hold on to this flip chart page. Display it each week so people may add to
it. This list will be used again in session 4. Similar exercises take place in subsequent sessions,
looking at longer term challenges. The following is one way to design your flip chart, with
examples:
CHALLENGE
BEHAVIORAL
RESOURCES
PRACTICAL OR EMOTIONAL CHALLENGES
Caregiver needs a break x x
Person says inappropriate things x x
Person refusing to shower x x
Ask participants to share some of their challenges. Encourage them to add more to the master list
as they continue to think about this, or if they hear someone else say one that resonates for
Savvy Caregiver Advanced Trainer Manual – December 2013
33
them. Put all responses on the flip chart and check off which category best describes it. Some will
fit into more than one, which is fine. The important thing is to acknowledge how many of these
challenges fit into the themes of the program. Typically, they all will. If a challenge arises that is
not addressed in the program, offer a resource or an individual conversation outside of class time
to discuss this.
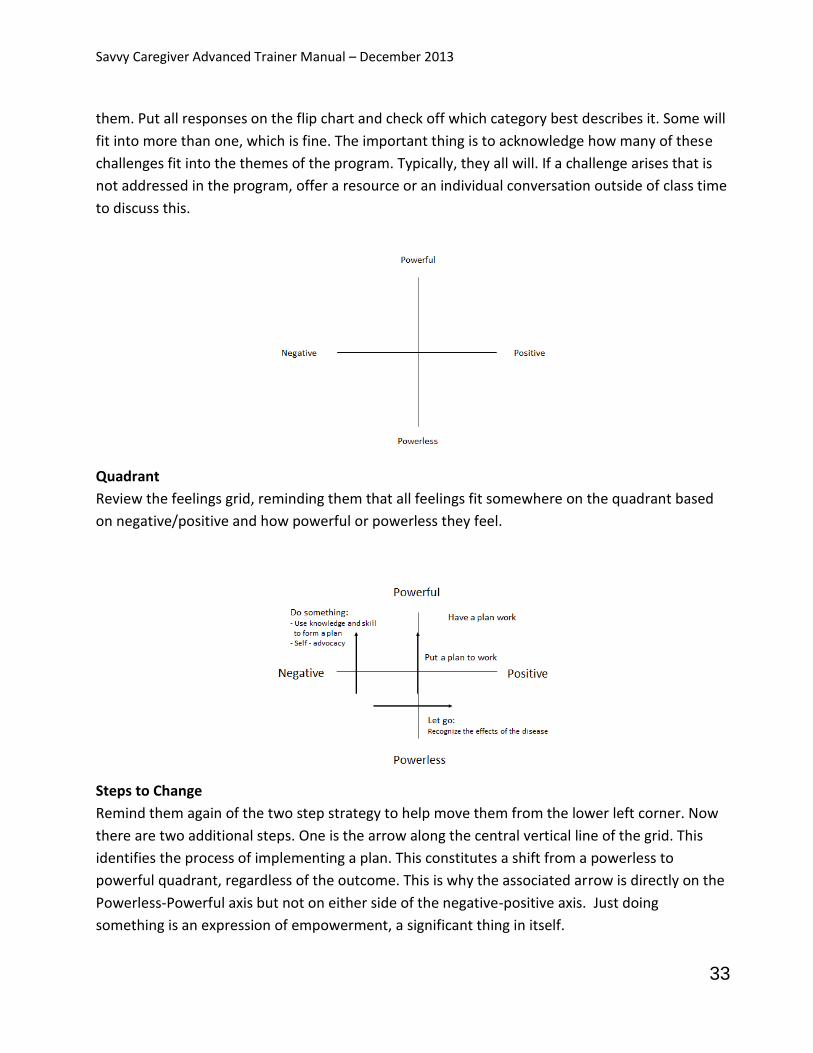
Quadrant
Review the feelings grid, reminding them that all feelings fit somewhere on the quadrant based
on negative/positive and how powerful or powerless they feel.
Steps to Change
Remind them again of the two step strategy to help move them from the lower left corner. Now
there are two additional steps. One is the arrow along the central vertical line of the grid. This
identifies the process of implementing a plan. This constitutes a shift from a powerless to
powerful quadrant, regardless of the outcome. This is why the associated arrow is directly on the
Powerless-Powerful axis but not on either side of the negative-positive axis. Just doing
something is an expression of empowerment, a significant thing in itself.

Savvy Caregiver Advanced Trainer Manual – December 2013
34
The second difference is the addition of the notion of Self-Advocacy to the slide. This, too,
represents a shift in the direction of being empowered, so it constitutes an upward movement on
the grid. Advocating for oneself goes beyond asking for help. It means recognizing one’s abilities
and limits, and communicating one’s own needs in order to get the support that caregiving
requires. This empowers caregivers to get their needs met and avoid burnout, an important part
of self-care.
More Grid
Now we go back to the list of challenges generated by the participants. Work your way down the
list, and ask participants how those challenges make them feel, and where on the quadrant those
would land. You may use yellow post-it notes to place them, write them in or just do this verbally.
Chances are many will end up in the bottom left corner.
Point out that these challenges DO impact how caregivers feel. The good news is, participating in
training is form of empowerment, and will help move them on the grid.
The planning strategy just covered, and the “Try it Out” exercise will also create a more powerful,
positive feeling. The more participants learn about creating a better fit with their person, the
more success they will have, and the more positive and powerful feelings they will experience.
This creates the self-efficacy we are striving for.
Savvy Caregiver Advanced Trainer Manual – December 2013
35
Try It Out (5 minutes)
Trying the strategies discussed at home will encourage confidence.
Subsequent sessions will start with follow up on what participants tried, how it went and
what they learned (just like Savvy 1).
Continue with the “challenge” exercise: Are there additional current problems?
Use the Savvy tools, the ABC model, the Need Driven Model and the problem solving process,
and include a full scan of the environment:
o Assess one caregiving challenge in the area of the person’s behavior
o Develop and try out a plan to guide and structure the person’s behavior in this
challenging area
Savvy Caregiver Advanced Trainer Manual – December 2013
36
Session 2
Materials needed:
Flip chart
Plain paper, colored pencils
Slide handouts
My Caregiving Team worksheet
Guiding a Task worksheet
This session continues the program’s focus on the three main themes of behavior guidance,
strengthening resources for caregiving, and preparing for and dealing with the practical and
emotional challenges in the present and future.
We continue the focus on behavior guidance and re-establishment of calm through the “How Did
it Go?” session and an exercise that uses the problem solving process to walk through managing
an ADL.
How did it go? (30 minutes)
This part of the session is meant to reinforce and develop caregiving self-efficacy. In this case,
what is being reinforced is competence in making practical use of various models taught last
session and previously in the original Savvy Caregiver. Sharing of both successful and not so
successful efforts to put strategies into action builds self-efficacy. This is your first chance to
check in with caregivers to be sure they understand the models introduced in session one, and to
discuss how they are utilizing them. If something is unclear, offer a brief review. If anyone is
willing to offer a description of their attempts, see if you can break their story down into steps we
have discussed: background and current factors; scan of the environment and the role of the
environment on behavior; ABC model; structure and support; assess-plan-implement-evaluate.

Savvy Caregiver Advanced Trainer Manual – December 2013
37
Remind them they aren’t expected to utilize each model every time they strategize. Guide the
discussion to encourage them to consider all aspects of their process.
Be sure to post the list of current challenges from week one. Ask if anyone would like to add to
this list after having some time to think about it.
Session 2 Overview: This session will introduce the notion of a “care team,” and gets participants
started on a process of mapping out what their team looks like. The care team exercise helps
participants to consider where members of their team are helpful and where they need
additional or different support. We will refer back to the OOVL model to guide participants in
decisions about their care team. We will also examine another ADL (preparing / sharing a meal)
using the problem solving process and other models.
Who’s on My
Caregiving Team?
Who’s on My Caregiving Team? (20 minutes)
Found in caregiver manual pages 27-30
This segment introduces participants to the third key theme of the workshop: the care team, the
informal and formal resources that can help with their caregiving. This segment starts with a
guided imagery exercise. A detailed description follows. It includes ONE way to take the results of
the guided image and put them down on paper, to create a “picture” the care team. What is
important is that participants start to consider and engage with the question of the kind of help
they need and are getting, and how to improve that situation. It is not important that they use
the device we give them to do so.

Savvy Caregiver Advanced Trainer Manual – December 2013
38
The purpose of the map exercise is to give participants a way to think about and create some kind
of representation of their team of support. As part of the overall problem-solving approach of
the program, participants need to develop a realistic assessment of how their family-friend-
service system is or isn’t working for them. Over the course of the program, we’ll be asking them
to take some action to make the resource map more aligned with their current reality and more
supportive of what they have committed to doing.
The exercise begins with a guided image that aims to help participants to name the people and
organizations that are currently in their caregiving network. Begin by asking them to paint a
picture of their caregiving world in their mind. You may have them imagine themselves as artists,
drawing or painting their caregiving worlds. You may want to hand out plain paper and colored
pencils ahead of time and invite participants to jot down their thoughts after the guided image
exercise.
Suggest that participants get comfortable in their seats and they might want to close their eyes.
Then talk them through the following exercise, encouraging them to really imagine and envision
their caregiving world:
Think about you and the person with dementia; think about the connection between you, the
linkage you feel both in terms of your relationship and in terms of the work and tasks you do
to take care of him/her.
Now, think about a large space, maybe a big flip chart or a drawing tablet. And, thinking about
the connection between you and the person, put the two of you in the middle of that space.
Imagine writing or drawing the two of you in a way that shows the strength and closeness of
the connection and the kind of importance that connection represents in comparison to all of
the other connections in your life right now.
If it is helpful to think more three dimensionally, start by thinking about yourself with your
person standing in a big room, adjacent to each other. How close are you?
Now, think about other people who are close to you (friends, relatives, neighbors, etc.) and
groups (faith community, club, doctor, etc.) in your life, or your person’s, and who are helpful
in caregiving. Who else is close to you or the person? Are there others who are involved in a
big way right now? Imagine drawing anyone like this into your picture, putting them in
relation to you and your person. How close would you put them? How big would you
represent them? As you’re doing this, think about what help these people or groups provide.
If you are picturing yourself in a room, where are these helpers? Are they next to you? Or
across the room? Or out in the hall? How might you express this on paper?
Savvy Caregiver Advanced Trainer Manual – December 2013
39
Are there other people or groups who are helpfully involved with you or the person,
somewhat importantly but maybe not as intensely as the first group? How would you write
or draw them in on your picture? Think about what help they provide.
Are there other groups or people who play small, helpful roles? How would you draw them in
your picture? How close; how big? Think, too, about what help they provide.
Now think whether there are people or groups who are in the picture of your caregiving life
but who are not only not helping but who actually make demands on you and drain your
energies? Who are they? Are they distant or close? What kinds of demands do they make
on you?
How might you draw these people in your picture? Where might they be in the room with
you? Are they next to you pulling on your arm? Out in the hall calling to you?
Next, think about people or groups who could provide more caregiving help. You may have
already drawn them in, but you know they could do more. How might you draw these people
or groups in your picture? What more do you think they could do?
Open this up for discussion, reminding people to go ahead and draw some ideas. How are people
“seeing” this? What images did they create? Ask them about their helpers, and about those who
are not helping. Did anyone include professional helpers? Doctors’ offices? Are they able to
identify areas where they would like the care team to be different?
Be sure participants understand that this is a work in progress. It is a way to visualize a larger
circle of help around them. Over the next 2 sessions we will look more at what resources are
available and how to access them. This information will help create a care team map that
addresses future care needs as they look ahead. Let them know we will continue to revisit this
map in later sessions.
Sample Drawings
Walk through the sample maps, detailing how this example demonstrates who is close, who is
helping, who is draining, and where changes can be made. Emphasize this is just one possible
approach to creating a caregiving team map. Theirs may look very different, but it is intended to
be a way of describing the instrumental and emotional world in which they are carrying out their
caregiving.

Savvy Caregiver Advanced Trainer Manual – December 2013
40
In the example above, the major relationship is between the caregiver and care recipient. The
daughter is an important part of the picture and is close to the dyad. A nephew is also an
important part of the picture, but more distant. Others – like the brother, church, neighbors, etc.
– are part of the picture, but not as important and not as close as the daughter. Point out that the
both the size and placement of each person on this “map” offers information about their
relationship to the caregiver / care recipient dyad.
Here the strength and direction of energy for all the care team members are portrayed. The
daughter and brother are portrayed as being the strongest supporter, and the nephew is seen as
a big drag. Note that the old friends and church both help (a little) but also make demands.

Savvy Caregiver Advanced Trainer Manual – December 2013
41
As a result of thinking about how to improve the care team, a new element has entered the
picture above - formal services. Also, a decision has been made to reduce the drag from the
nephew and from the church, indicated by a change in arrow size and/or direction. More help is
being sought from the doctor and neighbors, and a choice has been made to be less involved with
old friends. Participants can use their drawing to reflect changes as they occur, or to help them
define what kinds of changes in their care team they need to make in order to better meet their
needs.
Strengthening the
Care Team
Through Decision Making
and Communication
Strengthening the Care Team (25 minutes)
This opens up the process for discussion. Guide participants through a review of who they see as
their supports, and who they see as being a drain. Ask if anyone would like to offer an example of
where they would most like to make an adjustment. Once people acknowledge that they have
something they would like to change, move on to the following exercises that demonstrate
options regarding how to do that.
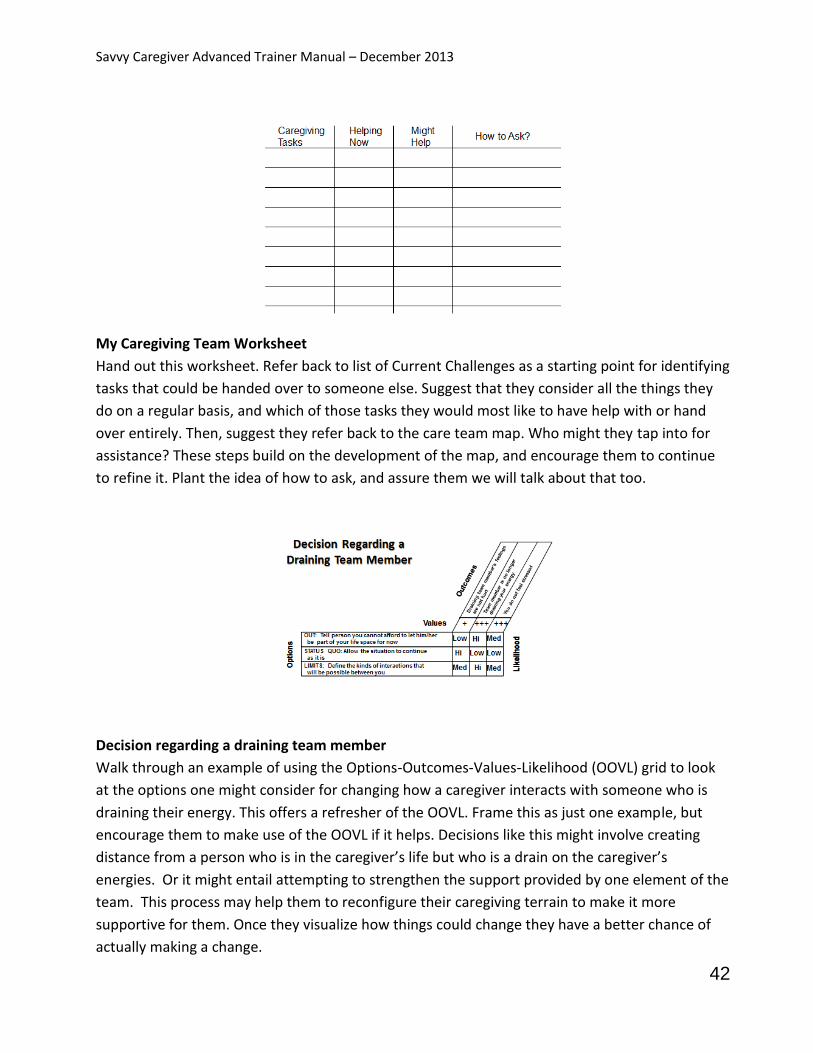
Savvy Caregiver Advanced Trainer Manual – December 2013
42
My Caregiving Team Worksheet
Hand out this worksheet. Refer back to list of Current Challenges as a starting point for identifying
tasks that could be handed over to someone else. Suggest that they consider all the things they
do on a regular basis, and which of those tasks they would most like to have help with or hand
over entirely. Then, suggest they refer back to the care team map. Who might they tap into for
assistance? These steps build on the development of the map, and encourage them to continue
to refine it. Plant the idea of how to ask, and assure them we will talk about that too.
Decision regarding a draining team member
Walk through an example of using the Options-Outcomes-Values-Likelihood (OOVL) grid to look
at the options one might consider for changing how a caregiver interacts with someone who is
draining their energy. This offers a refresher of the OOVL. Frame this as just one example, but
encourage them to make use of the OOVL if it helps. Decisions like this might involve creating
distance from a person who is in the caregiver’s life but who is a drain on the caregiver’s
energies. Or it might entail attempting to strengthen the support provided by one element of the
team. This process may help them to reconfigure their caregiving terrain to make it more
supportive for them. Once they visualize how things could change they have a better chance of
actually making a change.

Savvy Caregiver Advanced Trainer Manual – December 2013
43
If there is time, you can use a prepared OOVL on a flip chart to have participants walk through
either a real situation or a theoretical example.
Decision regarding community obligations
Most caregivers at this point in their caregiving career have little time or freedom to participate
in extracurricular activities. Someone in the group may have an example of having already limited
their community obligations. Ask if anyone in the group would like to use a situation they have
experienced, or walk through the one given. Again, this is just an example of one scenario.
Communication
to Strengthen the
Care Team
Communication to Strengthen the Care Team
So far we have looked at the people and resources that are in the caregiver’s environment of
care. We have started to consider tasks they might want some help with and we have looked at
how to make adjustments to the care team to better support the caregiver. Now it’s time to
consider how to set up a helper for success and how to ask.
We will be building on these key points to build the helper’s self-efficacy and increase the
likelihood things will go well and they will want to help again: choose the right task; provide
detailed instructions; set them up with appropriate expectations and goals; and offer strategies
to defuse agitation. The question is how to communicate this information. The following slides
from Savvy may create a basic framework for this.

Savvy Caregiver Advanced Trainer Manual – December 2013
44
Progressive Decline
One approach here is to ask participants if they would like to summarize what is meant by this
slide. Be sure they capture the idea that their person is less able to guide their own behavior, so it
is incumbent upon the helper to take control of guiding behavior. What the caregiver does and
how the environment is structured will be the driving force behind their person’s behavior.
Anchors of Contented Involvement
Again, if you ask, someone may be willing to explain this graphic. Otherwise summarize how to
create contented involvement: tap into things the person likes; set it up in a way that will
encourage success; and provide appropriate support, cues and reminders. This is good fit.
Remind them how much they know, and how important it is for helpers to have some sense of
this. An outline offered to a helper regarding what works and what doesn’t work regarding fit,
structure and support is more likely to lead to a successful experience for everyone.
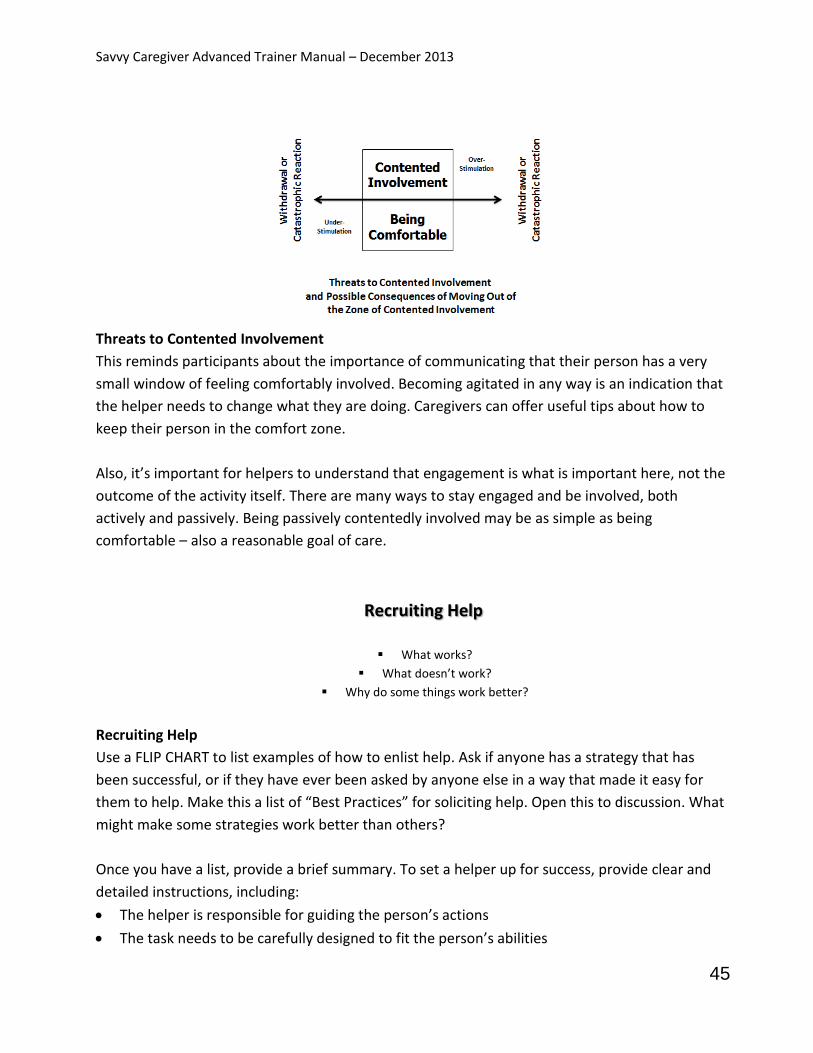
Savvy Caregiver Advanced Trainer Manual – December 2013
45
Threats to Contented Involvement
This reminds participants about the importance of communicating that their person has a very
small window of feeling comfortably involved. Becoming agitated in any way is an indication that
the helper needs to change what they are doing. Caregivers can offer useful tips about how to
keep their person in the comfort zone.
Also, it’s important for helpers to understand that engagement is what is important here, not the
outcome of the activity itself. There are many ways to stay engaged and be involved, both
actively and passively. Being passively contentedly involved may be as simple as being
comfortable – also a reasonable goal of care.
Recruiting Help
What works?
What doesn’t work?
Why do some things work better?
Recruiting Help
Use a FLIP CHART to list examples of how to enlist help. Ask if anyone has a strategy that has
been successful, or if they have ever been asked by anyone else in a way that made it easy for
them to help. Make this a list of “Best Practices” for soliciting help. Open this to discussion. What
might make some strategies work better than others?
Once you have a list, provide a brief summary. To set a helper up for success, provide clear and
detailed instructions, including:
The helper is responsible for guiding the person’s actions
The task needs to be carefully designed to fit the person’s abilities
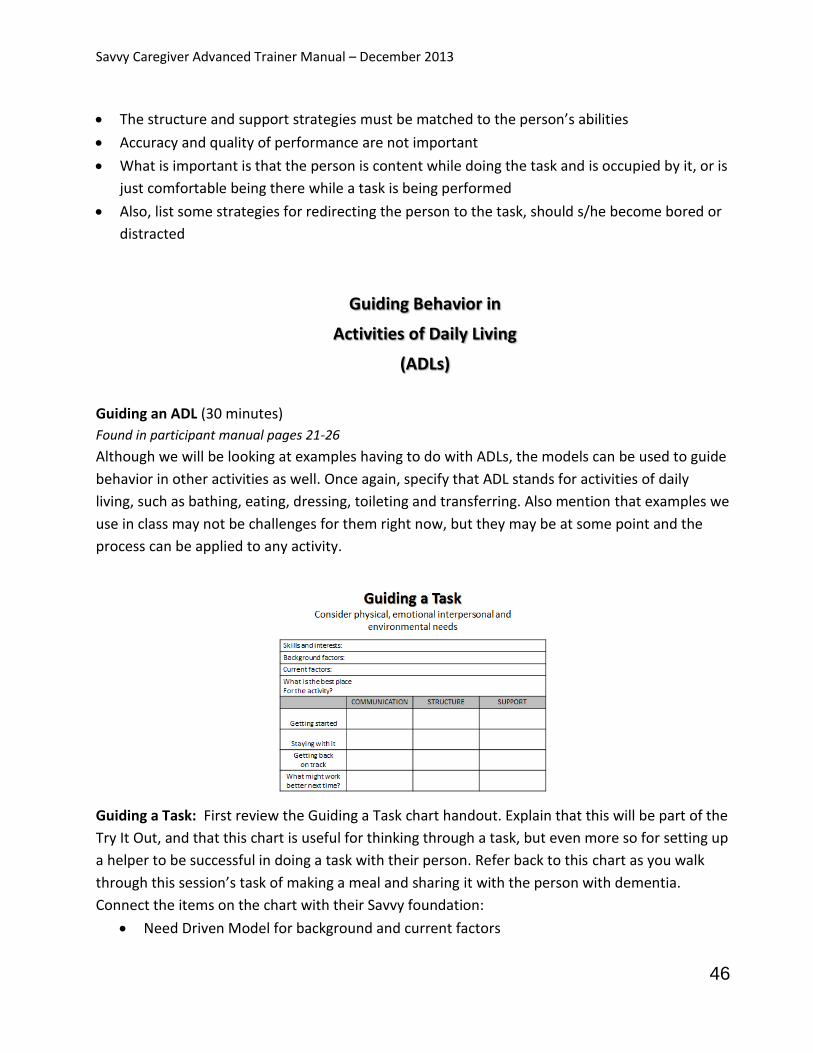
Savvy Caregiver Advanced Trainer Manual – December 2013
46
The structure and support strategies must be matched to the person’s abilities
Accuracy and quality of performance are not important
What is important is that the person is content while doing the task and is occupied by it, or is
just comfortable being there while a task is being performed
Also, list some strategies for redirecting the person to the task, should s/he become bored or
distracted
Guiding Behavior in
Activities of Daily Living
(ADLs)
Guiding an ADL (30 minutes)
Found in participant manual pages 21-26
Although we will be looking at examples having to do with ADLs, the models can be used to guide
behavior in other activities as well. Once again, specify that ADL stands for activities of daily
living, such as bathing, eating, dressing, toileting and transferring. Also mention that examples we
use in class may not be challenges for them right now, but they may be at some point and the
process can be applied to any activity.
Guiding a Task: First review the Guiding a Task chart handout. Explain that this will be part of the
Try It Out, and that this chart is useful for thinking through a task, but even more so for setting up
a helper to be successful in doing a task with their person. Refer back to this chart as you walk
through this session’s task of making a meal and sharing it with the person with dementia.
Connect the items on the chart with their Savvy foundation:
Need Driven Model for background and current factors

Savvy Caregiver Advanced Trainer Manual – December 2013
47
The Environment of Behavior
Anchors of Contented Involvement for skills and interests
Structure and Support handouts for communication and problem solving strategies
Review the next slide to sum up the potential uses for all the models within the framework of the
Problem Solving Process, and then come back to this chart to walk through guiding the task.
Guiding an ADL / Problem Solving Process
This is a group exercise. Use the Problem Solving Process to ask the group to plan out strategies
for guiding the person through one activity of daily living. Today we will focus on making a meal
with the person and sharing it. If this is not appropriate given the people in the group, focus on
keeping someone engaged while making a meal, or simply sharing a meal with the person. This
part of the session requires some flexibility and thinking on one’s feet. Touch on the Need Driven
Model to identify and solve potential problems and link this to the ABC model of behavior. Both
focus on antecedents to behavior.
Ask participants if they can describe something they see as a troubling or disturbing behavior for
this scenario. It is important to get them to narrow down from a broad or vague interpretation of
what happened (“he wouldn’t eat” or “she yells”) to the more precise and specific description of
what happened (“I put down his plate and he got up and walked away;” or “She fussed when I
said it was time to eat, but then she yelled at me when I told her to come to the table.”).
Next, have them either state the actual antecedents or imagine them, including possible
environmental antecedents. In addition to looking at the specific antecedents, ask participants to
think about the behavior in terms of the possible needs the behavior may have been expressing.
Then as they go through the Plan and Implement steps of the process, they should be able to
Savvy Caregiver Advanced Trainer Manual – December 2013
48
state what they will be looking for to determine if the selected strategy is getting them where
they want to go.
ASSESS
Start with a stage somewhere in the middle of the group if possible and establish that as the
target for the planning involved in this exercise.
Establish clear goals: a peaceful meal, no confusion or agitation, pleasant for both.
Walk through with the group, following the outline on the chart. Caregivers may use this
chart to plan a task as part of this week’s “Try It Out”.
The chart handout may be used to provide helpful information to a helper.
Imagine some skills and interests that the care recipient may have that will be useful for the
helper to know.
Consider the Need-Driven Model. What background factors may play a role in this task? Include
likes and dislikes; mobility and sensory issues; rituals and habit. What are the current factors?
Focus on stage of dementia first. Also consider appropriate setup and guidance, and the daily
routine involved.
PLAN
Begin to work through all steps in the chart handout. Use the rows to create structure and
support for the help that will be provided.
ABC model factors:
Establish what antecedents need to be in place in order to get started and support behavior
o Comfortable seat, toileting done
This also takes into account the environment and its influences
o Remember the environment as an antecedent
o Comfort, discomfort; also comfort items may help
o Chaos, distractions, loud music / conversation in background
What kind of communication will work well with the person (verbal, visual, tactile, some
combination) to get the person started? Be sure they indicate how directive they need to be
(support).
How should the meal be set up? And where should it be?
Savvy Caregiver Advanced Trainer Manual – December 2013
49
What kind of cues work to get the person started in helping with meal preparation and / or
getting the person to eat a meal?
IMPLEMENT
Once the meal has begun:
o What special structuring or cuing may help?
o Once their person has begun eating, does one form of communication work better
than others?
o How much assistance is needed?
o Cutting, feeding, clean up?
What happens if their person becomes distracted? What communication, structure, and support
strategies work? What tips or tricks can the caregiver share?
EVALUATE
The last row of the chart provides the caregiver with a way to get feedback from the helper on
how things went, and it is set up in a way that lets the caregiver and helper brainstorm about
how to make the event even better next time. Again, the goal is for this person to want to come
back, so what is needed to make it work even better? Review the Problem Solving Process model
again to demonstrate how the process flows into a new cycle starting with Plan.
If, as a trainer, you would like to read specific tips for eating and meal preparation, information is
available from NIA at
http://www.nia.nih.gov/sites/default/files/sites/default/files/alzheimers_caregiving_tips_daily_a
ctivities_0.pdf, and
http://www.nia.nih.gov/sites/default/files/sites/default/files/alzheimers_caregiving_tips_healthy
_eating.pdf, and from the Alzheimer’s Association at http://www.alz.org/care/alzheimers-food-
eating.asp.
Try It Out (10 minutes)
There are 4 main areas to focus on: Behavior Guidance; Strengthening the Care Team;
Preparation for the Future; and Self-Care
Be sure everyone has structure and support strategy handouts from Savvy Caregiver 1,
session 5; bring extras just in case they don’t.
Savvy Caregiver Advanced Trainer Manual – December 2013
50
Behavior Guidance
Try out ADL behavior guidance based on the models.
Continue to focus on behaviors.
Identify a persistent behavioral challenge not associated with ADLs and develop a plan to re-
establish calm.
Identify any pattern of distraction from tasks or activities; conduct close analysis of distraction
antecedents; formulate and test behavior re-establishment strategies.
Strengthen the Care Team
Make and implement communication strategies and/or key decision choices about at least
one part of the team in an effort to improve the situation.
Are there resource needs not met by the current team?
Identify a person or organization you will ask for help.
Work out a plan for asking for help and do so.
Savvy Caregiver Advanced Trainer Manual – December 2013
51
Preparation for the future
Consider long-term challenges and identify key decisions that will need to be made. We will
discuss this next session.
Self care
Identify one caregiving area associated with emotional distress and deliberately make a move
to shift this into something more satisfying.
Before ending class, you may want to take the opportunity to forewarn people that the next
session will include talking about some difficult subjects: grief, loss, later stage care and end of
life. These topics are tough to explore but our goal, as always, is to help inform and empower the
caregivers. This minimizes the chances that they will feel unprepared later, when they may have
to make hard choices.

Savvy Caregiver Advanced Trainer Manual – December 2013
52
Session Three
Materials needed:
Two flip chart pages for future challenges (see suggested format below)
Slide handout
Ongoing Loss: Ideas that May Help handout
Internet Resources / Free Internet Tools for Caregiver Communication handout
OOVL Decision-Making Tool handout
Legal and Financial Planning for People with Alzheimer’s Disease (NIA)
Connections books
Maine Hospice Council flyer about hospice
Alzheimer’s Disease: Care and Support at the End of Life booklet (Dr. Laurel Coleman)
End of Life: Helping with Comfort and Care booklet (NIA)
Agency on Aging resources: o Agency flyer o Information on living options, LTC assessments o Local resources
Also useful, but optional: o Hospitalization Happens (NIA) o Pain in Dementia (AGS Foundation for Health in Aging)
Folder or sleeve to hold handouts
How Did It Go?
ADL behavior guidance
Care team strengthening
Work on caregiver self-care
How Did It Go? (30 minutes)
Open up discussion with how participants are using the models and strategies taught and
discussed in the first two sessions. Are all the models making sense? What parts are they using?
Ask about trying things out and be sure to help them identify if they are applying the models
where they may not realize it. The point is to draw participants’ attention to being intentional in
using these tools and to learn to assess what happens when they do. Becoming familiar and
feeling comfortable with the models is part of the caregiver self-efficacy development process.
Hearing themselves and others describe successes builds this.

Savvy Caregiver Advanced Trainer Manual – December 2013
53
Ask the group about any efforts to identify resources for help with caregiving, and efforts to then
ask for that help. Participants have much to learn from one another about successfully asking for
and obtaining support. What are the reactions to the caregiving team map exercise? Did people
think more about their team? Did they add any informal or formal resources to the list? Have
they thought more about who is helping and who is not? Did they think about situations in which
improved communication might promote additional help? What changes has anyone made?
Some groups respond more readily to the care team map exercise than others. Ask for feedback,
and if there is confusion, clarify where needed. The exercise is intended to help caregivers
consider all the people who may be available to them both now, and when they need more help
later. Be prepared to offer suggestions to groups that are having difficulty “seeing” this, as well as
to participants who insist there is no one who can help them. The exercise is not meant to create
more stress, or lead anyone to feel pressured to make drastic changes immediately. Remind them
of formal vs. informal resources, and assure them that they will leave this session with more
information about formal resources.
Has anyone identified additional caregiving challenges? What have they done to work on
addressing the feelings associated with caregiving and the challenges ahead? As we continue to
ponder the challenges of caregiving, what are they doing to enhance their own well-being? What
steps are they taking to recognize their feelings, and to move themselves to a more powerful and
positive place on the feelings grid? Acknowledge and congratulate them on any examples of self-
care.
Session 3 Overview
In this session we will be looking at some of the longer term challenges caregivers are likely to
face, and considering some of the factors around later stage care, including sharing some
information about formal resources. As you may have alerted them last week, mention again that
today’s topics may create some discomfort. This exercise of looking at loss and what the future
may hold is all part of self-care. Later, we will work on guiding the ADL of bathing.
Savvy Caregiver Advanced Trainer Manual – December 2013
54
Caregiving Challenges
What is the most difficult challenge you
expect to face in taking care of your
person in the next 6 – 12 months?
Identifying Future Challenges (60 minutes)
Found in participant manual pages 34-35
The main portion of this session focuses on the near and long term challenges in caregiving,
including considering what kinds of decisions will need to be made in later stage care. It may be
helpful to prepare participants up front by pointing out that some of what will be discussed may
be uncomfortable for them. Be clear that talking about later stage care, and the associated
emotions, is not intended to upset them. The goal is to offer participants strategies and
information so they are prepared and better able to deal with these issues, rather than feeling
blind-sided by them. Also suggest someone they may contact outside of class in case anyone
requires more support around these issues. This may be the trainer or someone else.
The start of this exercise is an opportunity to remind participants that dementia is a terminal
illness. Medical providers may not have emphasized this point, and some caregivers may have
had trouble comprehending this earlier on. Gently but clearly emphasize that, unless something
else takes him/her first, dementia will end their person’s life. The further along the journey of
dementia, the more the focus is on their person being comfortable. We will talk more later in this
session about hospice and palliative care. Here you can gently introduce the idea that later stage
care will be about comfort and end of life.
Exercise: Use a flip chart and once again prepare columns displaying the core concepts of the
program: behavioral issues, resources, and emotional/practical challenges. Entitle this one “6-12
month challenges”.
6-12 MONTH CHALLENGES
BEHAVIORAL
RESOURCES
PRACTICAL OR
EMOTIONAL
CHALLENGES
Caregiver will need more break time x x
Person may become incontinent x
Person could start to wander x x x
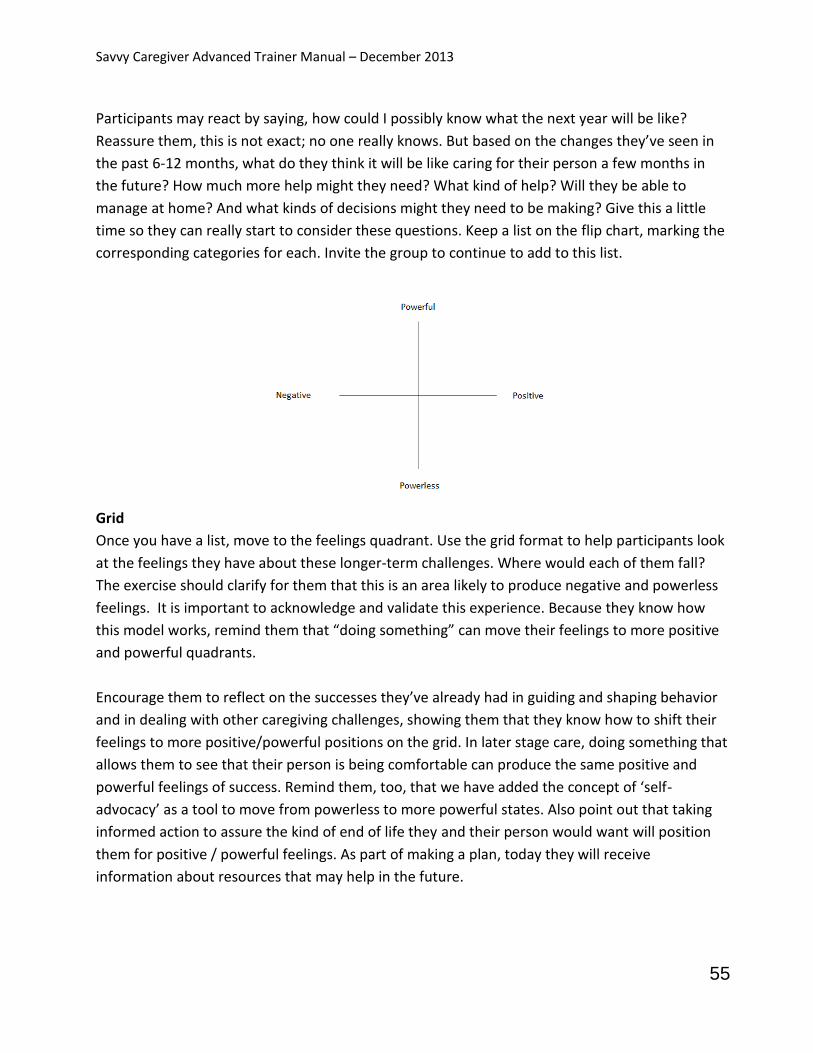
Savvy Caregiver Advanced Trainer Manual – December 2013
55
Participants may react by saying, how could I possibly know what the next year will be like?
Reassure them, this is not exact; no one really knows. But based on the changes they’ve seen in
the past 6-12 months, what do they think it will be like caring for their person a few months in
the future? How much more help might they need? What kind of help? Will they be able to
manage at home? And what kinds of decisions might they need to be making? Give this a little
time so they can really start to consider these questions. Keep a list on the flip chart, marking the
corresponding categories for each. Invite the group to continue to add to this list.
Grid
Once you have a list, move to the feelings quadrant. Use the grid format to help participants look
at the feelings they have about these longer-term challenges. Where would each of them fall?
The exercise should clarify for them that this is an area likely to produce negative and powerless
feelings. It is important to acknowledge and validate this experience. Because they know how
this model works, remind them that “doing something” can move their feelings to more positive
and powerful quadrants.
Encourage them to reflect on the successes they’ve already had in guiding and shaping behavior
and in dealing with other caregiving challenges, showing them that they know how to shift their
feelings to more positive/powerful positions on the grid. In later stage care, doing something that
allows them to see that their person is being comfortable can produce the same positive and
powerful feelings of success. Remind them, too, that we have added the concept of ‘self-
advocacy’ as a tool to move from powerless to more powerful states. Also point out that taking
informed action to assure the kind of end of life they and their person would want will position
them for positive / powerful feelings. As part of making a plan, today they will receive
information about resources that may help in the future.
Savvy Caregiver Advanced Trainer Manual – December 2013
56
Loss and Grief
Found in participant manual pages 35-37
Here is another spot where the group will be confronted with a difficult topic. Take it slow and
check in from time to time to see how they are doing.
You will offer participants language and categories for a number of feelings that are all under the general heading of grief and loss. Focus on the extent to which participants are already dealing with these feelings. Remind them that these emotions are an important part of their experience. Once again, this isn’t to upset them, but to give them an opportunity to acknowledge and consider their feelings in order to identify support and resources for the future. We will also touch on the notion of “reestablishing” their lives after this career of caregiving has been completed. This is a difficult topic for many. Our purpose in introducing the topic of “reestablishment” is simply to introduce another element of being savvy: that a time will come when life again changes for you dramatically. Some forethought is prudent. Follow the bullet points on the slide to define the different types of grief. There is some overlap in these so take the time to make distinctions. Often caregivers will experience much validation in this.
Ongoing loss: This refers to the series of “little losses” in dementia that happen over time for
both the person with dementia and the caregiver. Although each loss on its own may not
seem big, the cumulative effect is significant.
Anticipatory Grief: Anticipatory grief occurs when a loss is imminent, whether someone is
actively dying or has received a diagnosis that indicates end of life is approaching. It may
create a sense of mourning that lingers throughout the journey of dementia, or it may be
experienced when the end of life is near. Others aren’t able to see this kind of grief, so it is
experienced in isolation.
Ambiguous sense of loss: The loss felt when the person is still physically present, but in all
other ways has changed and often feels absent. Others don’t see this type of grief either.
Savvy Caregiver Advanced Trainer Manual – December 2013
57
Disenfranchised grief: Because others don’t see the ambiguous kind of loss experienced by
caregivers, they can’t be supported or validated. This kind of loss is not socially recognized,
leaving caregivers feeling disenfranchised.
Be sure to make the clear connection between other people not being able to recognize their grief experience and therefore not being supportive. Here is where the self-advocacy piece comes back into play for them. Their sense of loss and grief will remain unacknowledged until they communicate what they are feeling to their caregiving team. Otherwise it remains invisible to others. It may be helpful to suggest that dementia presents a gift of time: time to reconnect, to say what needs to be said, to find closure. It may also be a time to record the person’s memories while they are still somewhat intact. And it’s a chance to deliberately slow down. The extra time it takes for people with dementia to perform tasks often causes frustration for caregivers, but encourage them to make use of this to slow life down in ways that nurture them whenever possible. The grief they experience while caregiving does not diminish the grief they will experience when their person dies. However, there will be a new level of loss and grief after death. They will lose their person, but they may also lose their daily routine, their sense of purpose, and their focus. They may feel they have too much time on their hands. They will also likely feel relieved, and it is crucial that they understand that this is normal and not a reason to feel guilty. Give participants a chance to discuss how all this feels, and what they expect. Touch upon the importance of considering what their lives will look like after caregiving. What will be the new “normal”? Creating some purpose outside of caregiving will help them make the transition later. When discussing the extra challenges created on special occasions (holidays, birthdays, anniversaries) be sure to remind them about role flexibility as discussed in session six of Savvy 1. Families with more role flexibility are more resilient. Remind them, too, that after their person dies there will be new challenges on special occasions, and to not be too surprised at how they may react on those days. It is one more opportunity for good self-care. Throughout this journey, one critical piece of self-care is support. Remind participants to help their care team understand how they are feeling so they can feel validated and supported. Encourage them to seek out support through family, friends, community and support groups.
Savvy Caregiver Advanced Trainer Manual – December 2013
58
Future Challenges Here is where you will use the third and final flip chart with categories, to list 12 months+ challenges. This exercise adds to the other lists of anticipated challenges that the participants began and have continued to develop and refine. Be sure to keep previous “Challenges” flip charts posted for comparison, and to continue to add to those if other thoughts arise.
12+ MONTH CHALLENGES
BEHAVIORAL
RESOURCES
PRACTICAL OR EMOTIONAL CHALLENGES
How will I know it’s time to move him? x x
What will keep her content? x x
Will I be able to keep doing this? x x
The focus of this exercise is: what do they expect to happen as the person’s life comes toward its end? What are the concerns about safety? What kinds of help will they need? How will they maintain self-care? Ask them to think about what their person was like 12 months ago. How different are they now? Then, can they project that level of change into the future and imagine how different it will be? This is the time to ask them to imagine if they will realistically be able to continue to manage their person’s care at home, without extra help?
Later Stage Choices
Care choices Comfort choices Location choices
Later Stage Choices Found in participant manual pages 30-32
Guide the group through some of the choices they may potentially have to make.
Savvy Caregiver Advanced Trainer Manual – December 2013
59
Encourage caregivers to consider initiating conversations with their person’s health care
provider (doctor, nurse practitioner) about choices and wishes with an emphasis on including
their person in conversations and decisions as long as possible. In order to be an effective self-
advocate, the caregiver needs to be a full member of the health care team early on.
Care choices involve thinking about what will be acceptable in terms of diagnostic work-ups,
treatment for other issues, procedures. Which symptoms demand diagnosis? Which
diagnoses demand treatment? Have them consider things from colds to flu to pneumonia to
cancer. What will be appropriate as dementia progresses? Questions to guide them might
include:
o What are the short and long term goals of care?
o What outcome might they reasonably expect?
o How would any choice impact what gives life meaning for the person?
o What is most consistent with their goals?
Comfort choices involve considering the tradeoffs between treatment and comfort. They may
be faced with choices down the road for their person regarding feeding tubes, ventilators,
antibiotics. Persons with dementia may develop infections, get the flu or pneumonia. Should
this happen, caregivers face a decision: treat the condition – and prolong the person’s life or
not – with the possibility that the condition will end the person’s life. More and more, medical
providers are recognizing that comfort can be a more realistic and humane care strategy than
continuing to engage in what may be futile efforts to cure. This approach is palliative care,
which seeks to balance the discomfort that might be involved with treating life-threatening
conditions against a broader concern for keeping a person at ease while the natural processes
of an incurable condition take their course. Have they weighed the risks and benefits of
treatments? Have they thought about how hospice care could support later stage care?
Location choices address where their person would receive the most comprehensive care,
and have their safety and well-being managed in a way that does not drain the caregiver. As
demands increase, how to meet these demands must include consideration of where to best
meet them.
It is critical to remind participants that they are their person’s advocate. They have the right to ask all the questions they need to in order to feel equipped to make the best choices possible. There are certain steps caregivers need to take to be able to be an effective advocate for their person, steps that will allow them to work collaboratively with medical and legal systems. The first step is to obtain Power of Attorney for Health Care which allows caregivers to make decisions about the person’s care. Under some circumstances, they may need to become the person’s guardian and/or conservator. This may vary by state. Ideally, the person should already have a written Advance Directive for health care. At some point, a person with dementia will no longer be considered legally competent to sign such documents. It’s important for caregivers to
Savvy Caregiver Advanced Trainer Manual – December 2013
60
understand that they can use their in depth knowledge of their person to make some very good guesses about the care their person would most want, based on their values and what gives their lives meaning.
Later Stage Decision Making Here is one more chance to open up the discussion to major decisions caregivers will face. Possible areas to include: getting more help; when to choose hospitalization; moving the person to long term care; when to call hospice. Ask them to consider who will be involved in these choices. Have them think about their care team map. Who is likely to want to be involved? Has the person with dementia completed an advance directive? Is there a power of attorney for healthcare? Where might family conflicts present a problem? Briefly define different options: living options (nursing facility (NF), residential care), and care options (Do Not Resuscitate orders (DNR); palliative / hospice care; respite). Be sure they are aware that many facilities have lengthy waiting lists. Don’t wait until they need to make a change. Add names to waiting lists early. If they aren’t ready, they can always say, “no thanks”. Finally, go back to the feelings grid and remind them that thinking about all of this information takes an emotional toll. This is part of ongoing loss. Encourage them to practice good self-care.
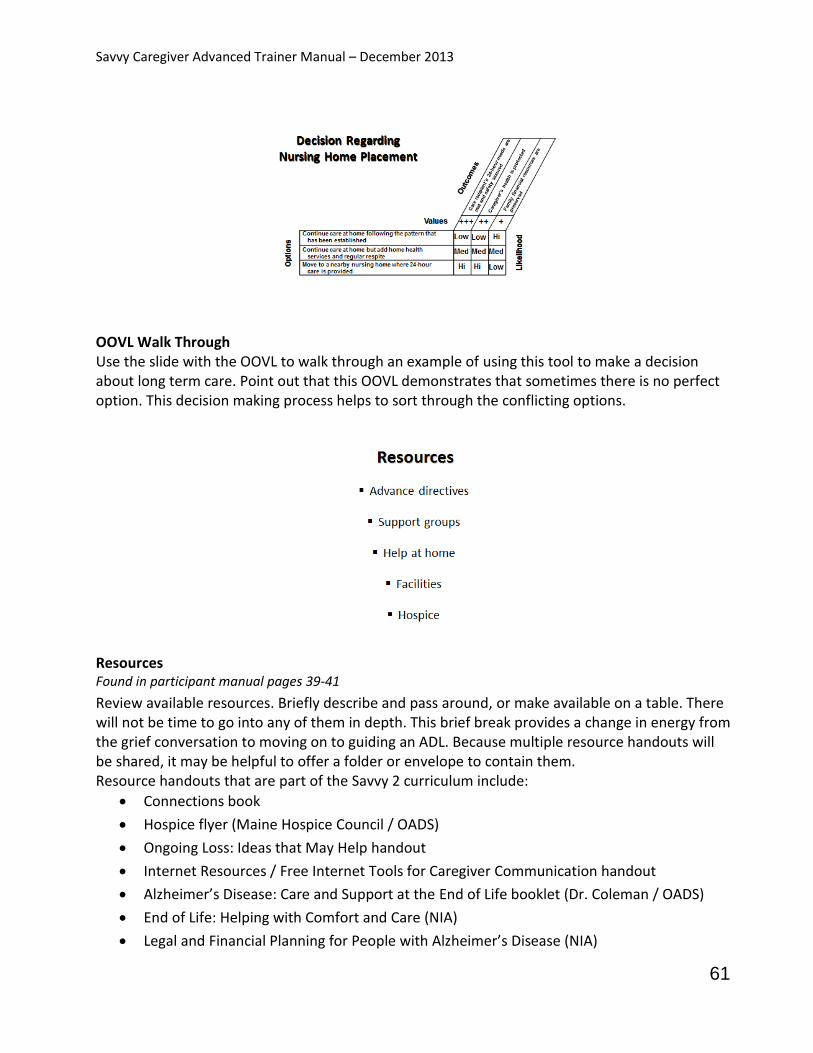
Savvy Caregiver Advanced Trainer Manual – December 2013
61
OOVL Walk Through Use the slide with the OOVL to walk through an example of using this tool to make a decision about long term care. Point out that this OOVL demonstrates that sometimes there is no perfect option. This decision making process helps to sort through the conflicting options.
Resources Found in participant manual pages 39-41
Review available resources. Briefly describe and pass around, or make available on a table. There will not be time to go into any of them in depth. This brief break provides a change in energy from the grief conversation to moving on to guiding an ADL. Because multiple resource handouts will be shared, it may be helpful to offer a folder or envelope to contain them. Resource handouts that are part of the Savvy 2 curriculum include:
Connections book
Hospice flyer (Maine Hospice Council / OADS)
Ongoing Loss: Ideas that May Help handout
Internet Resources / Free Internet Tools for Caregiver Communication handout
Alzheimer’s Disease: Care and Support at the End of Life booklet (Dr. Coleman / OADS)
End of Life: Helping with Comfort and Care (NIA)
Legal and Financial Planning for People with Alzheimer’s Disease (NIA)
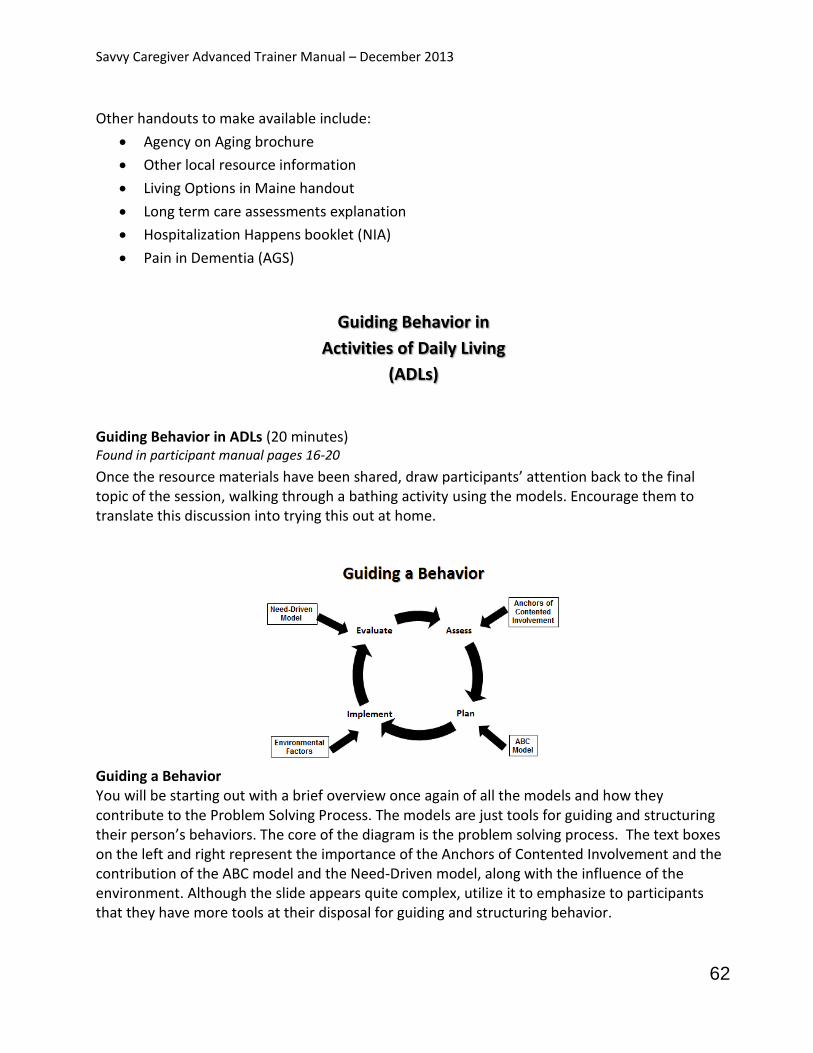
Savvy Caregiver Advanced Trainer Manual – December 2013
62
Other handouts to make available include:
Agency on Aging brochure
Other local resource information
Living Options in Maine handout
Long term care assessments explanation
Hospitalization Happens booklet (NIA)
Pain in Dementia (AGS)
Guiding Behavior in
Activities of Daily Living
(ADLs)
Guiding Behavior in ADLs (20 minutes) Found in participant manual pages 16-20
Once the resource materials have been shared, draw participants’ attention back to the final topic of the session, walking through a bathing activity using the models. Encourage them to translate this discussion into trying this out at home.
Guiding a Behavior You will be starting out with a brief overview once again of all the models and how they contribute to the Problem Solving Process. The models are just tools for guiding and structuring their person’s behaviors. The core of the diagram is the problem solving process. The text boxes on the left and right represent the importance of the Anchors of Contented Involvement and the contribution of the ABC model and the Need-Driven model, along with the influence of the environment. Although the slide appears quite complex, utilize it to emphasize to participants that they have more tools at their disposal for guiding and structuring behavior.
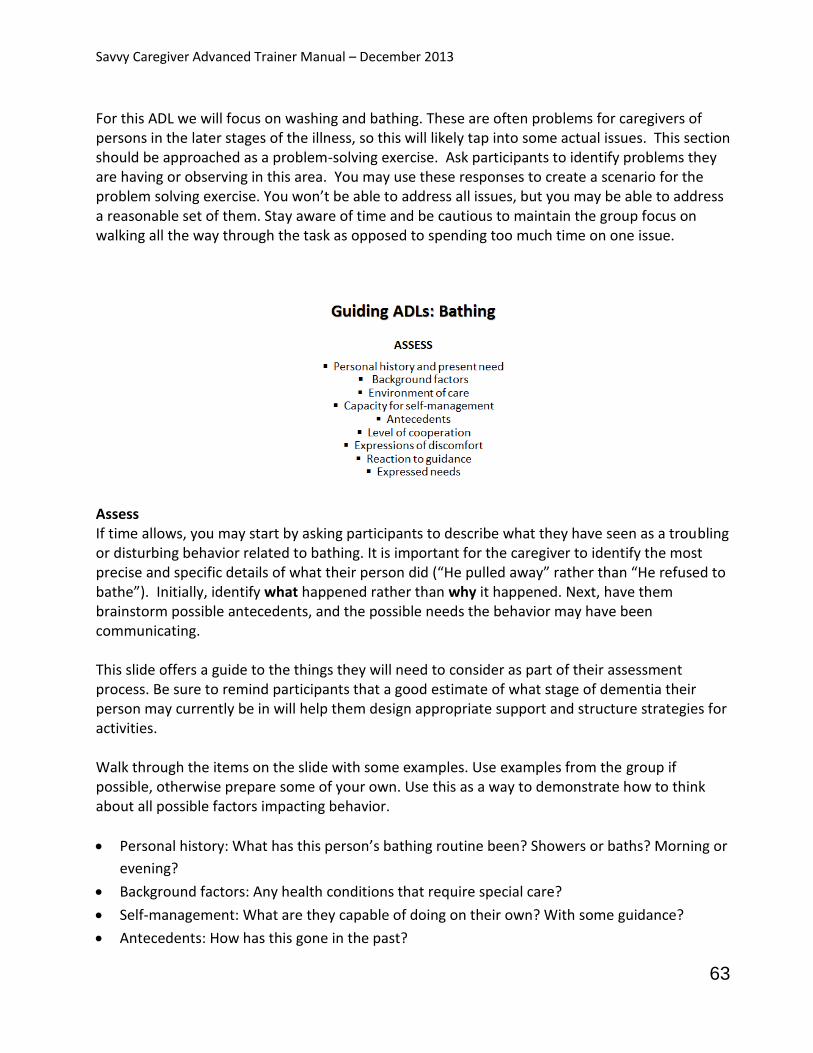
Savvy Caregiver Advanced Trainer Manual – December 2013
63
For this ADL we will focus on washing and bathing. These are often problems for caregivers of persons in the later stages of the illness, so this will likely tap into some actual issues. This section should be approached as a problem-solving exercise. Ask participants to identify problems they are having or observing in this area. You may use these responses to create a scenario for the problem solving exercise. You won’t be able to address all issues, but you may be able to address a reasonable set of them. Stay aware of time and be cautious to maintain the group focus on walking all the way through the task as opposed to spending too much time on one issue.
Assess If time allows, you may start by asking participants to describe what they have seen as a troubling or disturbing behavior related to bathing. It is important for the caregiver to identify the most precise and specific details of what their person did (“He pulled away” rather than “He refused to bathe”). Initially, identify what happened rather than why it happened. Next, have them brainstorm possible antecedents, and the possible needs the behavior may have been communicating. This slide offers a guide to the things they will need to consider as part of their assessment process. Be sure to remind participants that a good estimate of what stage of dementia their person may currently be in will help them design appropriate support and structure strategies for activities. Walk through the items on the slide with some examples. Use examples from the group if possible, otherwise prepare some of your own. Use this as a way to demonstrate how to think about all possible factors impacting behavior.
Personal history: What has this person’s bathing routine been? Showers or baths? Morning or
evening?
Background factors: Any health conditions that require special care?
Self-management: What are they capable of doing on their own? With some guidance?
Antecedents: How has this gone in the past?

Savvy Caregiver Advanced Trainer Manual – December 2013
64
Cooperation: How much do they do? Is there any resistance?
Comfort and discomfort: How do they express these? How can the caregiver distinguish their
person’s experience, i.e. are they afraid or are they cold?
Reactions: How do they respond to different types of guidance?
Expressed needs: Is the caregiver able to sense this? Is there any comfort or pleasure? Fear or
pain?
Environment of care: Must the activity occur in this place? Are there more comforting
options?
Plan Keeping in mind that even bathing is an opportunity for contented involvement / being comfortable, start with considering what part the person is capable of playing in the task. How much participation may the caregiver reasonably expect? Also, they need to watch for signals from their person: are they ready? Feeling resistant or agitated? Are there parts of the activity that the person enjoys? Walk through the items on the slide to guide the discussion. Offer suggestions for making the task more successful.
The right moment: Do this when it works for them best (when they are rested and relaxed)
whenever possible.
Location: Where is the best place to do this activity?
Modesty and intimacy: Only uncover areas being washed; try to have the person wash their
own sensitive areas. Also, ask the caregiver to consider their own comfort level with this
activity. How can they work through their own discomfort? Is this time to enlist some help?
Strategies and equipment: How do they start? What is the routine? Sponge baths are ok too.
Bath seat? Flexible shower hose? Keep the person from getting chilled. Strive to make the
experience pleasurable for the person. It should be pleasurable for the caregiver as well. It

Savvy Caregiver Advanced Trainer Manual – December 2013
65
can be a gentle moment and if it goes well for the person, the caregiver can take pride in its
accomplishment.
Physical comfort: Older skin is more fragile and sensitive. Consider water temperature and
cleansing materials.
Next steps: Be ready for drying and dressing.
Implement The planning phase includes some consideration of goals and expectations. Remind participants
that these must be adjusted accordingly as dementia progresses. Preventing skin breakdown is
likely to remain a goal throughout the course of dementia, but standards of cleanliness, personal
hygiene and dress may loosen over time. Safety and comfort are always important goals as well
and they may take on more importance than appearance over time. Remind participants to
maintain awareness of the aim of the bathing task.
This is an opportunity to deliberately create antecedents to set up a successful experience. What
cues will they be using and how will they communicate? What’s the emotional message? At this
point the caregiver has considered initiating the plan, guiding the person to the location where
the activity is to take place, the removal of clothing, cleaning and drying the person, the replacing
of briefs and clothing, and guiding the person back to the place where the next activity is to take
place. This step is the “try it and see how it goes”. Encourage them to keep track of their efforts
and how each step goes. If the situation calls for it, they may need to make adjustments during
the task. Remind them to keep track of any changes they make to the plan as well. All this
information is important for the evaluation step.

Savvy Caregiver Advanced Trainer Manual – December 2013
66
Evaluate
Overall, were the goals reached? If not, what fell short? This is the caregivers’ opportunity to
review each step of the task.
Were there parts of the process in which the person was cooperative and comfortable? What
were the antecedents of these parts? What approaches were used? Overall, did the activity seem
to fit the person’s abilities? Encourage them to make note of what went well so they can identify
what made it go well (antecedents and strategies) and then reproduce this in other activities.
If there were parts during which the person was uncomfortable or uncooperative, what did the
caregiver do to restore calm? Were there any unexpected events? If any difficulties were
encountered, in terms of the person’s behavior, what might have been their meaning? What
might they have been communicating?
What are the main things learned from evaluating the task that will go into the next assessment
phase to alter the plan?
If, as a trainer, you would like to read more specific tips about bathing, information is available
from NIA at
http://www.nia.nih.gov/sites/default/files/sites/default/files/alzheimers_caregiving_tips_bathing
_0.pdf and from the Alzheimer’s Association at http://www.alz.org/care/alzheimers-dementia-
bathing.asp.

Savvy Caregiver Advanced Trainer Manual – December 2013
67
Try It Out (5 minutes)
Continue to encourage participants to tap into all the models reviewed as part of the problem
solving process to approach an activity or ADL. This will be the final opportunity to try things and
return to class with feedback. Remind them that the models are all tools for them to use as they
deem best in their own situation. They are not expected to use them all, but trying something
new may lead to insights.
Remind them to continue to address their caregiving map, available resources and self-care.
Savvy Caregiver Advanced Trainer Manual – December 2013
68
Session Four
Materials needed:
All three “Challenges” flip chart lists
Slide handout
Class evaluations
Certificates
How Did It Go?
Preparing for the expected and the unexpected
Using the models to guide challenging
behaviors
How Did It Go? (30 minutes)
This is the final time to check in with participants regarding all the key themes of the program.
Starting with the topics from the last session, start with some open ended questions about later
stage care. How has their thinking changed about end of life care? What steps have they taken to
identify resources to help? What adjustments are they considering making to their care team,
and who have they asked for help? What plans have they started to make based on last week’s
talk about later stage decision making and finding resources?
Also ask about how it went this week with behavior guidance. With the models as a framework,
see if participants made attempts to guide an activity or defuse an unexpected behavior.
Reinforce any descriptions of efforts, pointing out where different models were utilized and
where lessons were learned. Ask about what worked and what didn’t, and how they will make
adjustments next time. What have they noticed regarding the impact of the environment on
behavior? Draw participants’ attention to being intentional in using the Savvy Caregiver tools and
to assessing what happens when they do. Build their self-confidence and self-efficacy by
emphasizing any new learning they are demonstrating and any positive changes they are making.

Savvy Caregiver Advanced Trainer Manual – December 2013
69
Session 4
Guiding behavior
Strengthening the care team
Self-care
Wrap-up
Session 4 Overview
Offer a brief overview of the topics to be covered in this session.
Guiding ADLs
Guiding ADLs (30 minutes)
Found in participant manual pages 16-20
This topic slide is just an introduction. In this session you will be using the Problem Solving
Process to walk through assisting with toileting. Depending on the group, this may or may not be
an activity that people are helping with at this point. It is up to each trainer to determine if there
is a different ADL activity that the group would find more beneficial to problem-solve. In most
cases, toileting is a task that everyone will eventually need to cope with, and because of its
challenging nature, addressing it at this time may be especially helpful for future planning. Some
of the suggestions you will be incorporating can be helpful in preventing future problems, so the
group may wish to approach this activity with that in mind.
If you choose to address a different activity, be prepared to work around the discussion notes as
they are focused on toileting.

Savvy Caregiver Advanced Trainer Manual – December 2013
70
Problem Solving Process
Remind participants of the process model and how all the other models feed into it. You may
want to refer back to this slide during the guiding an ADL discussion.
Assess
This ADL activity is likely to be a sensitive topic. By this stage of the disease, it is probably the case
that many care recipients are having at least occasional incontinence.
In the first portion of the exercise, ask people to consider where they are with this task. The
exercise begins with brainstorming about what they all see when they try to help their person
with various components of toileting. For some, they may only need to remind or cue their
person to go and use the bathroom. Naturally, most will have unique and individual experiences,
but you can ask them to estimate at what stage of the disease their person is and to describe
briefly (and perhaps for just one or two participants) how they structure and support the activity.
Remind them that a key part of the assessment is to describe what they see - what actually
happens, before considering what it means. The points on the slide may help to focus this
description. For those who are not yet dealing with toileting issues, suggest they consider their
concerns and how they anticipate both they and their person may react. This will stimulate their
thinking.
The assessment should provide information about the kinds of cooperation and reactions the
caregiver can anticipate in implementing the plan. Review each item on the slide. Ask for
suggestions from the group about how to consider each item. Be ready to offer examples to help
clarify.
Fit: Consider person’s stage, and caregiver’s expectations.
Self-management: Determine what the person is able to do for themselves. Watch for cues.

Savvy Caregiver Advanced Trainer Manual – December 2013
71
Cooperation: The person with dementia is communicating something through their level of
cooperation or resistance. Notice their responses.
Comfort and discomfort: How do participants typically recognize discomfort in their person?
How are these sensations expressed? Mention the fragility of older skin and the importance
of using appropriate cleansing products and methods.
Reactions: What kinds of reactions have people seen, and how do they interpret them? Refer
back to personal history as a possible background factor.
Environment: Remind participants about the environment of behavior. Consider all the ways
the environment might impact this task: room colors, contrast; location of task. Space and
place, i.e. where is the room, what do you walk through to get there. Lighting, temperature
and sound are all factors. What about alternatives like a commode?
Timing: A regular schedule is helpful. Consider how this task works at different times of the
day.
Self-assess: This is an activity that creates great discomfort for many people. Encourage the
group to be sure about their own feelings regarding this, and how they express them. If it
remains uncomfortable, what could they do to “normalize” it? Is this, in fact, something that
they need to get some help with? And are the cues they use with their person working?
Plan
Managing the daily cycle of elimination and urination seems to be the activity most associated
with caregivers reaching some kind of limit. Incontinence is the factor most frequently identified
by caregivers as the reason they consider and then choose to move the person to a long term
care facility. The physical components of incontinence care are unpleasant. The emotional
components of providing this care for a spouse or parent can be difficult. So this is a behavioral
management topic that is or soon will be of considerable concern for participants. It is important
to validate this concern for caregivers, and reassure them that walking through this problem
solving process may give them insight and information to help manage this task.
Savvy Caregiver Advanced Trainer Manual – December 2013
72
The plan needs to specify goals of care. A fundamental part of the plan involves being very clear
about what part, if any, the person can play in this task. Do they give cues about when they need
to go? If so, what are these cues and do they occur at particular times of the day? Does the
person have any times when they reliably need to use the toilet? Can they be counted on for
active help? Passive cooperation? Resistance? Be sure caregivers also anticipate how their
person will respond to being helped.
Some strategies to consider include
Control of fluid intake, while minimizing the chances of dehydration
Maintaining a schedule, with a specific routine for getting to and from the bathroom
Running water to encourage flow
Use of commodes and/or urinals
Introduction of adult briefs, including the routine of getting these on and off
Plan for taking care of skin
Plan for maintaining cleanliness of the home environment
There are a number of steps to the toileting process and each one needs to be mapped out in the
plan. The assessment should provide information about the kinds of cooperation and reactions
the caregiver can anticipate in implementing the plan. In addition to specifying the approaches,
the plan should indicate how the caregiver will initiate the activity; the kind of setting or
surrounding that will be most conducive to success; how communication will take place; and
what kinds of help and direction the caregiver will be providing throughout the process. When
using adult briefs, this task may take place in areas other than in the bathroom.
Part of the plan also includes how the caregiver will approach the unpleasantness of the task.
Caregivers must consider their feelings and possible responses during such an intimate activity.
They need to play a role, and preparing for how they will do this will help them to manage the
challenges involved. Remind them that they may choose to alter their plan of care if this activity
is one they would prefer not to perform. Now is the time to consider what their alternatives are.
Savvy Caregiver Advanced Trainer Manual – December 2013
73
Implement
This part of the exercise will demonstrate whether the goals of care were appropriate. At some
point in the disease process, reducing or reversing incontinence is not an appropriate goal.
Managing voiding and elimination so as to maximize the person’s comfort is an important goal.
Caregiver well-being is a reasonable goal as well. If the goals were not clearly outlined in the
planning phase, adjustments will need to be made during implementation.
Things to keep in mind as part of implementation:
What are the antecedents to support the activity?
What cues will the caregiver use? How will they communicate with their person?
Caregivers need to keep track of each step from initiating the activity to completing it and
moving on to the next activity.
Monitor any change made to the plan during implementation.
Keep track of what worked, what didn’t, their person’s reactions and how they
themselves felt and reacted throughout.

Savvy Caregiver Advanced Trainer Manual – December 2013
74
Evaluate
This is the part of the process where the caregiver looks back and reviews all aspects of the
activity in order to determine what worked and what could be done differently next time.
Although they will not be going into this kind of detail every time, for the purpose of the exercise
and walking through the process, encourage them to break the task down into every component
to consider how it went. If any of the participants have a real life example they are willing to
share, this may be very helpful.
Were goals reached? If not, what fell short?
How did their person respond in each part of the activity? Did this vary?
For parts that went well, what were the antecedents? Note these approaches.
What about for the parts that did not go as well? How did they restore calm?
What was the role of the environment?
What about the caregiver? How did they manage their feelings and reactions?
Finally, what were they able to learn that will help them alter the plan for next time?
The services of an occupational or physical therapist or a home health nurse could be highly
valuable at this time. Because the caregiver is so well informed, an in-home session could be an
extremely productive consultation, providing advice on techniques, products, and other
strategies for toileting.
If, as a trainer, you would like to read specific tips related to toileting and continence, information
is available from NIA at
http://www.nia.nih.gov/sites/default/files/sites/default/files/alzheimers_caregiving_tips_inconti
nence_0.pdf, and from the Alzheimer’s Association at http://www.alz.org/care/alzheimers-
dementia-incontinence.asp.
The final ADL walk through is now complete. Check to see if there are any lingering questions or
concerns before moving on to the program review.
The Care Team
The Care Team (20 minutes)
The focus will now shift to a final review of the Care Team: what they have learned about who is
on their team, how they would like it to shift, and what steps are needed to enable the team to
be more supportive.
Savvy Caregiver Advanced Trainer Manual – December 2013
75
Strengthening the Care Team
Found in participant manual pages 27-30
Ask participants to share what steps they have taken to strengthen their informal care team, or
options they are considering to help reshape their care team picture so it better addresses their
needs. What strategies have people tried? Remind participants of the activities in which they can
engage to strengthen their care team. They might ask for more help, remove someone or some
organization from the team or renegotiate relationships to make them less draining. Ask what
else they have considered or tried.
What else might they have done? Consider sharing information with team members or
identifying new resources. Do they have any new ideas for how to ask for help?
Challenges and Self-Care (15 minutes)
Found in participant manual pages 33-37
Be sure you have posted the three lists of “Challenges” that caregivers have been working on
each week. Here is an opportunity to consider how those challenges feel, which challenges they
may have addressed during the series, and which they will feel better prepared to address

Savvy Caregiver Advanced Trainer Manual – December 2013
76
through changes in their care team. Their feelings about the challenges they listed may change as
they alter their care team and feel more empowered through their own self-advocacy.
Grid
Use the feelings quadrant to evaluate shifts in caregivers’ emotional state now that they’ve gone
through the series and created more strategies for getting support. Start with the current
challenges list.
Considering the immediate challenges identified in the first session, how have participants’
feelings changed? What have they done to address any of these challenges?
Considering the challenges listed for the short and long term, how are participants feeling? Have
they garnered better understanding of these challenges? Inquire about their feelings relative to
decision making regarding their care team, and end of life care specifically. Use the quadrant to
plot some of these feelings to see if they have shifted on the grid. Accentuate any actions they
have taken which created more positive or powerful movement for them.
Remember that they have also spent time focusing on all they have lost and will continue to lose.
These feelings may be more tender after discussing later stage care. If feelings of despair or
defeat emerge, it may be possible to work with them within the context of accepting that the
care they are providing is the very best they can do and that their person’s needs may reach a
point where they exceed any caregiver’s capacity. This is a form of acceptance, and it can pave
the way for them to appreciate all their good work.
Improving the care team is an action caregivers can take to help them move to a more positive
and powerful state. Reinforce this. Encourage them to get more and better help from informal
resources and identify and access formal resources.

Savvy Caregiver Advanced Trainer Manual – December 2013
77
Program Re-Cap
Behavior guidance
Emotional and practical challenges
Care team / Resources
Program Re-Cap (20 minutes)
This re-cap is structured to match the three main topics of the program, as listed on the above
slide. Here you can pull together the threads of all the themes of the program.
Behavior Guidance
This begins the main part of the recap. We start with a final opportunity to review the models
and address questions about them. The five slides that follow are the main slides used to
illustrate the behavior guidance strategies taught in the original Savvy program and also referred
to throughout Savvy 2.
Problem Solving Process
Found in participant manual pages 16-20

Savvy Caregiver Advanced Trainer Manual – December 2013
78
This is the framework we have offered each week to help participants design caregiving
strategies. This model will be quite familiar by now. This is a cyclic model. Each cycle provides
information to help design the next cycle. Remind participants that this is just a framework. It is
intended to help them think about all aspects of an activity, without the expectation that anyone
will go through all these steps for every activity. They are welcome to use the parts of the process
that resonate for them, and return to this framework to address activities that are especially
challenging for them.
Assess: Examine the situation. Determine what is happening. Consider what might have
produced the situation.
Plan: Make a plan of action, based on the assessment of what you think is going on in the
situation.
Implement: Follow the plan of action as carefully as possible, and make note of how things go.
Evaluate: If successful, repeat. If there are problems, or if it just doesn’t work, note observations
from the implementation phase of the plan. Then, start again with the assessment step using this
information.
Fit Activity to Ability
In Savvy 1, we referred to this image as the Anchors of Contented Involvement. This illustrates
the point that, in almost any activity there is a process of continuous and often repeated
assessment that goes on. In this process, we use what we know about a person to adjust tasks
and activities as needed. Caregivers use what they know to select appropriate tasks (Person); to
adjust the kind of task they offer, and the way it is set up (Structure); and to determine what type
of help they give in order to get and keep the person going in the task (Support). At the same
time, using their powers of observation, they continually readjust their strategies based on how
their person is reacting to the task.
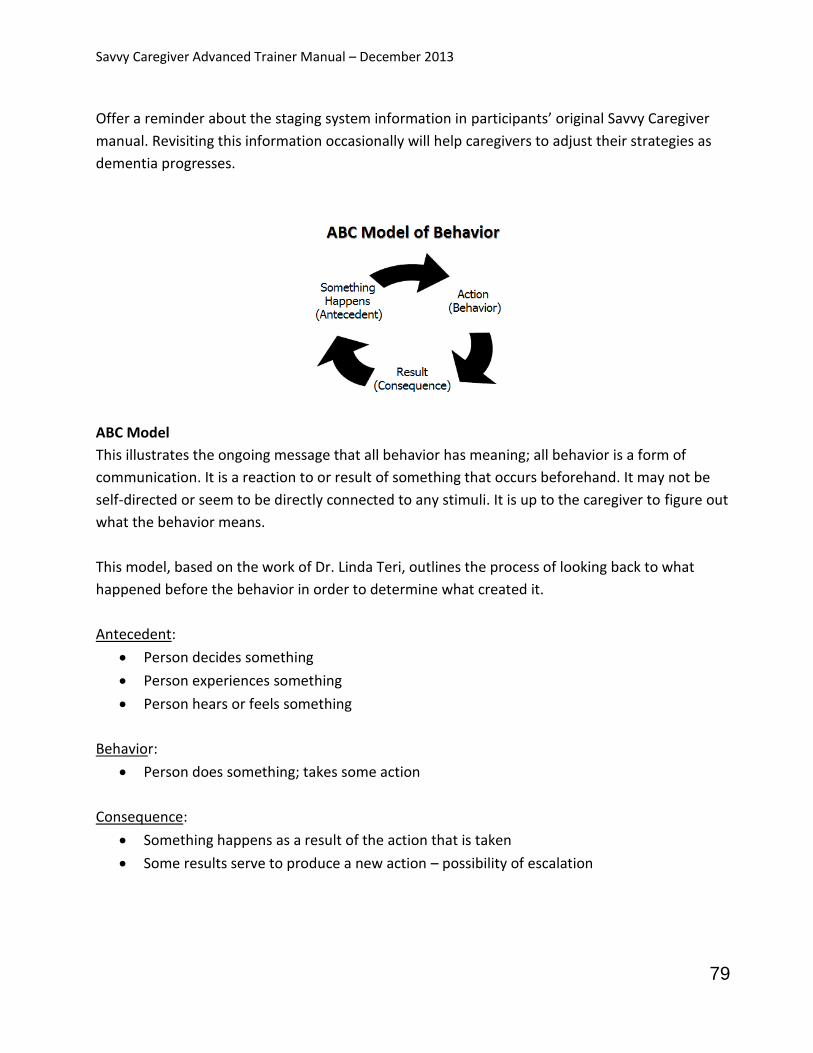
Savvy Caregiver Advanced Trainer Manual – December 2013
79
Offer a reminder about the staging system information in participants’ original Savvy Caregiver
manual. Revisiting this information occasionally will help caregivers to adjust their strategies as
dementia progresses.
ABC Model
This illustrates the ongoing message that all behavior has meaning; all behavior is a form of
communication. It is a reaction to or result of something that occurs beforehand. It may not be
self-directed or seem to be directly connected to any stimuli. It is up to the caregiver to figure out
what the behavior means.
This model, based on the work of Dr. Linda Teri, outlines the process of looking back to what
happened before the behavior in order to determine what created it.
Antecedent:
Person decides something
Person experiences something
Person hears or feels something
Behavior:
Person does something; takes some action
Consequence:
Something happens as a result of the action that is taken
Some results serve to produce a new action – possibility of escalation

Savvy Caregiver Advanced Trainer Manual – December 2013
80
The Environment of Behavior
Found in participant manual pages 11-14
Always consider the impact the surrounding environment has on behavior as part of assessment
and planning. The environment may be considered an antecedent in the ABC model.
Environment can stimulate or respond to behavior.
Encourage caregivers to always think about where care takes place. Sometimes people get stuck
assuming care must take place in certain designated spaces. If there are places where their
person is more cooperative (comfort spots), caregivers may choose to make creative changes in
where activities take place.
Wherever possible, caregivers will have more success when they can accommodate, simplify the
surroundings, make it easier for their person to focus, and reinforce contented involvement. Also,
they can watch for patterns in their environment to track which places tend to be comfort spots
and which tend to be trouble spots.
It is always important to consider safety issues as well and address them as they arise. Enhancing
home safely is vital, and how to do this may need to be revisited as things change.

Savvy Caregiver Advanced Trainer Manual – December 2013
81
Need-Driven Behavior Model
Found in participant manual pages 9-11
This is one more model that provides a way to think about behavior. Within the framework of the
Problem Solving Process, this model is especially helpful during the ‘assess’ and ‘evaluate’ steps.
Unexpected behaviors may be anything that is puzzling or surprising for the caregiver. This is one
more way to think about the meaning behind the behavior.
Background Factors: There are some things over which the caregiver has no control which
contribute to behavior. Dementia is progressive, and this progression itself also has an increasing
influence on behavior. These background factors may also affect current factors.
Current Factors: These are things that impact their person’s behavior which the caregiver may in
fact have some control over. Attending to these will minimize disruptive behaviors.
It is important to point out that, while the model appears focused on what might be called
troubling behaviors, it is more general in nature and may be quite helpful when the caregiver is
thinking about structuring and guiding any activity.
Savvy Caregiver Advanced Trainer Manual – December 2013
82
Emotional and Practical Challenges
Found in participant manual pages 34-37
This is an introduction slide to the next section. You just reviewed the challenges earlier in the
session. Now once again the emphasis is on the importance of keeping the emotional impact of
caregiving in mind and what steps to take to strengthen the caregiving situation in whatever ways
possible.
Caregiving Challenges
Immediate
6 – 12 months
12 months and beyond
Caregiving Challenges
To continue the emphasis on addressing the three major themes of the program, remind
participants once again about the challenges they have stated they are or expect they will be
facing. Congratulate them on identifying and speaking up about these challenges. Many are
taking steps to address them already. Everyone has now considered how they may best prepare
for addressing more in the future.
Looking Ahead
Loss and grieving
Later stage choices
Later stage decision making
Looking Ahead
This slide revisits the discussion topics from week three. All of these involve decision making for
the caregivers, and having a sense of what their person would want. They all also strongly impact
how the caregivers are feeling. Are there any lingering thoughts or questions about these at this
point?
Taking the time to consider these issues and all the options involved produces feelings. This is to
be expected. Taking action to address these feelings will help to move them to more positive and
powerful parts of the feeling quadrant.
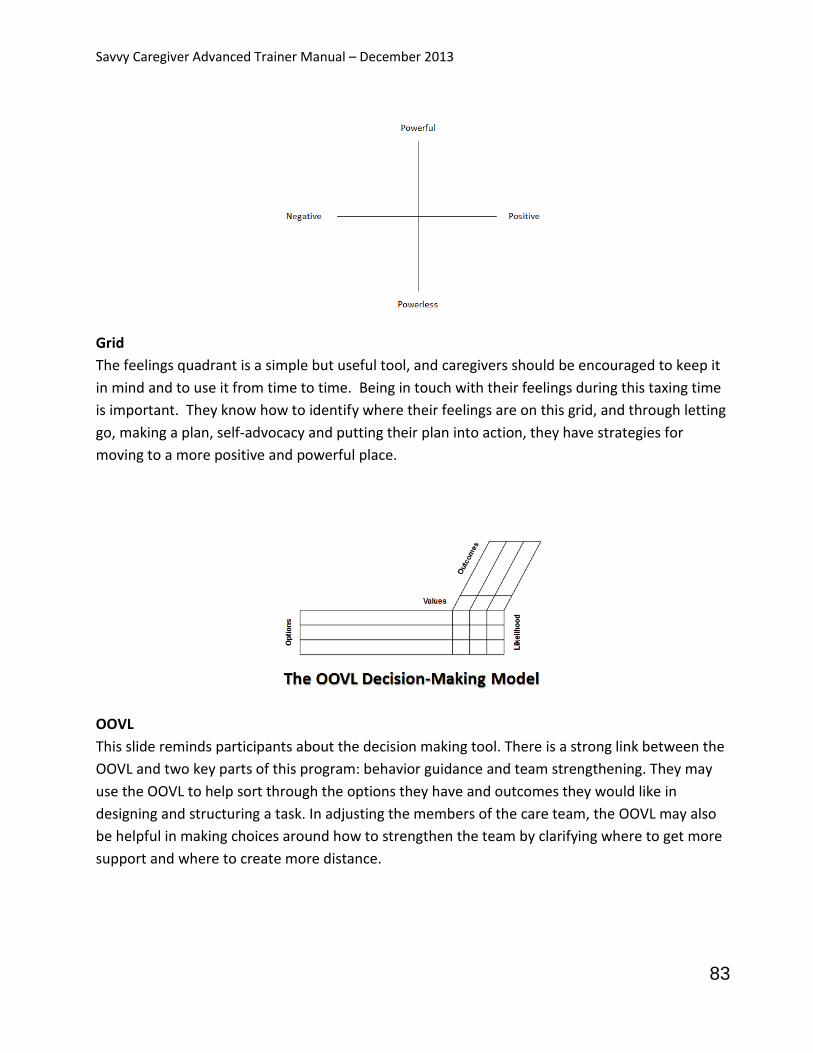
Savvy Caregiver Advanced Trainer Manual – December 2013
83
Grid
The feelings quadrant is a simple but useful tool, and caregivers should be encouraged to keep it
in mind and to use it from time to time. Being in touch with their feelings during this taxing time
is important. They know how to identify where their feelings are on this grid, and through letting
go, making a plan, self-advocacy and putting their plan into action, they have strategies for
moving to a more positive and powerful place.
OOVL
This slide reminds participants about the decision making tool. There is a strong link between the
OOVL and two key parts of this program: behavior guidance and team strengthening. They may
use the OOVL to help sort through the options they have and outcomes they would like in
designing and structuring a task. In adjusting the members of the care team, the OOVL may also
be helpful in making choices around how to strengthen the team by clarifying where to get more
support and where to create more distance.
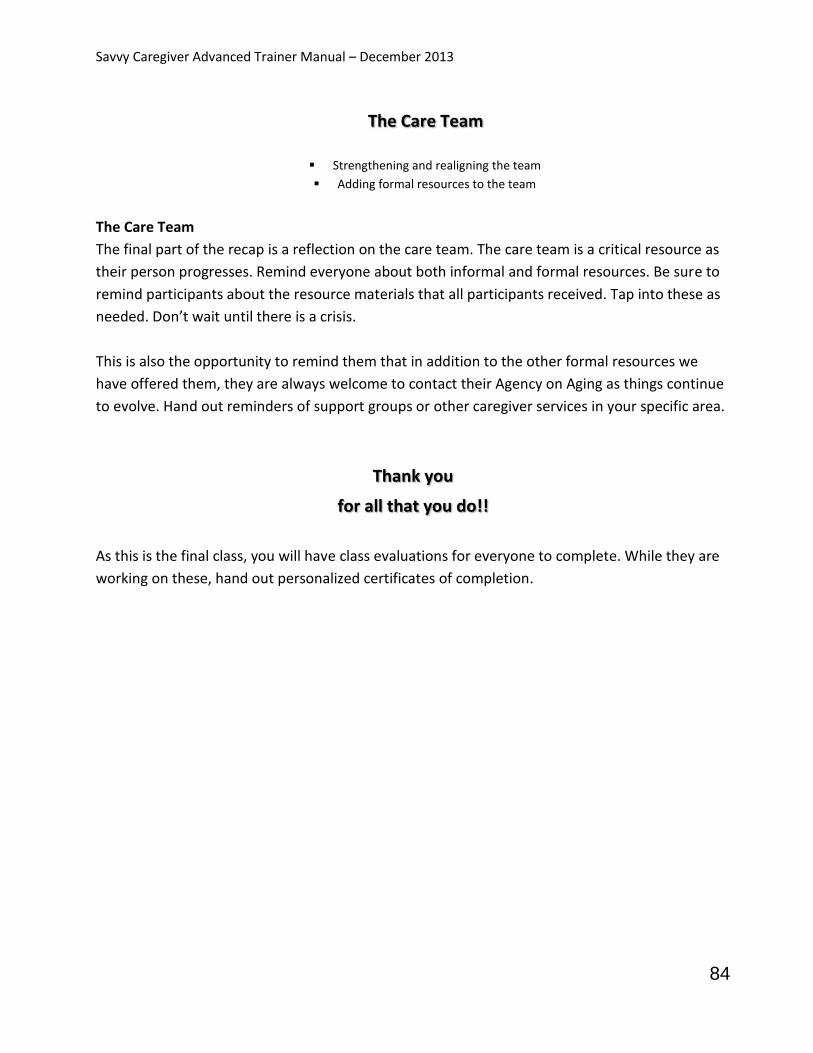
Savvy Caregiver Advanced Trainer Manual – December 2013
84
The Care Team
Strengthening and realigning the team
Adding formal resources to the team
The Care Team
The final part of the recap is a reflection on the care team. The care team is a critical resource as
their person progresses. Remind everyone about both informal and formal resources. Be sure to
remind participants about the resource materials that all participants received. Tap into these as
needed. Don’t wait until there is a crisis.
This is also the opportunity to remind them that in addition to the other formal resources we
have offered them, they are always welcome to contact their Agency on Aging as things continue
to evolve. Hand out reminders of support groups or other caregiver services in your specific area.
Thank you
for all that you do!!
As this is the final class, you will have class evaluations for everyone to complete. While they are
working on these, hand out personalized certificates of completion.

Savvy Caregiver Advanced Trainer Manual – December 2013
85
Maine Statewide Collaboration and Resources The State of Maine is offering Savvy 2 classes under a one year no cost extension to the Administration on Aging ADSSP grant, which runs through August 31, 2014. Only the series’ funded by that ADSSP grant will require the current USM pre-surveys to be sent to participants. Other grants, such as the Dementia-Capable Systems grant through the Maine Office of Aging and Disability Services (OADS), will have separate requirements for data gathering and reporting. Savvy 2 will also be offered through each AAA’s Family Caregiver Support Program (FCSP), as part of meeting the Agency on Aging funding requirements through their state level contracts (Rider A Performance Objectives). Agencies may also identify other funding sources to continue to offer Savvy 2. These might include sponsorships, other grants, tuition, donations, or other ways that the agency develops to sustain the program. Plans for continued sharing of ideas and lessons learned, related to teaching the course, monitoring and maintaining fidelity, and keeping trainers up-to-date, will be discussed and formulated during this grant extension period. During the Administration for Community Living (ACL) grant extension period, the resource people for Savvy 2 associate and master trainers in Maine are: Christine Merchant, Grants Manager Office of Aging and Disability Services 207-287-7134 [email protected]
Contract / grant requirements Training opportunities Funding Fidelity
Kathryn G. Pears, MPPM Dementia Care Strategies, Inc. 207-468-0705 [email protected]
Program fidelity
Training content
Dementia-specific information
Manual revisions / DVDs

Savvy Caregiver Advanced Trainer Manual – December 2013
86
Linda Samia, RN, PhD, CNL Assistant Professor, School of Nursing University of Southern Maine 207-780-4437 [email protected]
Program evaluation
Core program elements and fidelity
Publication(s) After the grant extension period, it is anticipated that statewide collaboration on this program, including information-sharing, identification of funding opportunities, and ongoing skill development, will continue. When the post-grant structure becomes clearer, all associate and master trainers will receive updated information, which can then be incorporated into their trainer manuals for future reference. As trainers, and authors of this manual, we want to recognize all the effort we know has gone into your becoming a Savvy 2 trainer and teaching the course. The research has already shown us how important this program has been for participants. Thank you for your time, energy, and commitment.