salubris is a latin word which means healthy, in good ... is a latin word which means healthy, in...
TRANSCRIPT

WHAT ARE THE COMMON TYPES OF CHILDHOOD CANCERS
AN NCCS QUARTERLY PUBLICATION April – June 2013
Issue No. 25 • MICA (P) 061/10/2010
Salubris is a Latin word which means healthy, in good condition (body) and wholesome.
...HELPING R EADERS TO ACHIEVE GOOD HEALTH

I n Singapore, leukaemia or blood cancer is the most common childhood cancers. It makes up to almost 4 in 10 (40.8%) of all childhood cancers according to the Cancer Registry data up to 1997. By itself, cancer in children is very rare. According to the Singapore Children Cancer Registry, there are
1,103 cases registered in Singapore from 1997 to 2005, which averages to about 120 cases per year. The incidence of childhood cancer is about 137.5 per million per year in Singapore. Half of these cases occur in children below 5 years of age.
The next most common childhood cancers are brain and spinal neoplasms (17.4%), and lymphoma (9.5%). There is an increasing trend of incidence observed in most childhood cancers except for Non-Hodgkin’s lymphoma (NHL), renal tumours and malignant bone tumours.
The survival for all cancers was markedly improved from 30-35% in the period 1968-77 to 55-60% in the period 1988-97. The survival rates especially for patients with leukaemia, NHL and renal tumours, has improved by more than 20% over the three decades. The survival rate of childhood cancer patients has markedly improved in Singapore because of better treatment regimens and outcomes. These results are in line with world-wide trends. Despite increasing incidences of cancer, the treatments have also improved, resulting in better survival outcomes.
Big scientific groups like POG (Paediatric Oncological Group) trials have incrementally resulted in better drug combinations, safer regimens for resource-poor countries and better tolerated side effects.
LEUKAEMIA
Some common symptoms for kids with leukaemia is tiredness and bleeding spots.The diagnosis is usually made with a blood test and a bone marrow biopsy for confirming the presence of malignant blast cells. Further tests are done to confirm the diagnosis. The treatment usually consists of systemic chemotherapy and consolidation radiotherapy in the higher risk patients. There is a move towards giving less radiotherapy to the brain and spinal cord in some of these kids because of the concern towards long term side effects of radiation.
BRAIN CANCER
The next group of patients with brain cancer often present with giddiness, vomiting, unsteadiness. A brain scan usually clinches the diagnosis. Depending on the type of cells, the patient will often require combination treatment with surgery, chemotherapy and radiotherapy. The remission rates are excellent in early stages before spinal metastasis. Similarly there is a concern for the long term side effects of radiation, but unlike leukaemia, radiation is still an integral part of the treatment process in childhood brain cancers. In some centres outside Singapore, there is the availability of the proton teletherapy machines, which are by far, the current state of the art treatment for paediatric brain cancers. The National Cancer Centre Singapore is actively engaging in fund-raising with the hope of building a proton centre facility for this purpose. Proton therapy relies on a physics phenomenon called the Bragg peak which results in a very sharp dose drop off unlike normal photons which continue to have an exit dose. What results are a very precise dosage and the ability to reduce the dose to the surrounding normal organs.
WILMS TUMOUR, RHABDOMYOSARCOMA AND EWINGS SARCOMAS
The last group childhood cancers consist of solid organ tumours, which are rare cancers like Wilms tumour, rhabdomyosarcoma and ewings sarcomas. The child can present with a mass which can be painful or painless. Some kids are very sick while some are still well and behave normally. The diagnosis is made with a panel of tests and imaging and with general clinical acumen of a paediatrician with a sceptical eye to suspect cancer. All these patients generally also require some form of surgery to remove the tumour, and consolidation chemotherapy and radiation to prevent systemic and local relapse. Treatment can last a few months and involve multiple hospital visits to different specialities.
The effect on the child, who is emotionally affected, as well as the parents and family, cannot be neglected in the holistic treatment of these patients. The younger ones develop a phobia of doctors, needles and therapists and need gentle coaxing. At least one of the parent needs to take time off from work or from caring for the other kids to bring the sick child to the hospitals for treatment. The emotional toll and financial burden on the family can be devastating. But there are also charitable organisations in Singapore like Children Cancer Foundation, Make a Wish Foundation as well as Viva Foundation which make it a part of their mission to either help financially, offer comfort or develop new novel cures.
It has been said that it takes a village to care for a child with cancer. We have dedicated teams of specialist doctors, nurses and therapists to help the patient and the family bear the burden of their disease with more ease. In some cases, patients with fever while undergoing chemotherapy have expedited admission to the dedicated cancer ward without a need to go through the accident and emergency departments of the paediatric hospitals. There is also an emergency number they can call to ask for advice.
REFERENCES: Singapore Childhood Cancer Registry 1997 – 2005, http://www.nrdo.gov.sg/uploadedFiles/NRDO/Publications/Spore%20Childhood%20Cancer.Registry%20Report.pdf
PAEDIATRIC CANCERS IN SINGAPOREBY DR FRANCIS CHIN Senior Consultant Department of Radiation Oncology
It is always very emotional and shocking when a loved one falls sick with cancer. And more so when it happens to young kids as it extracts a tremendous psychological toll on the parents and the siblings. It is always unexpected to see children who were previously healthy and happy suddenly grow sick and tired from cancer.
2 3SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

THE LITTLE HERO The will to survive can sometimes help one to overcome even the most difficult challenges. Indeed, 12-year-old Muhammad Khidir bin Yusri is one fine example of bravery and true perseverance as he shares his story with CHARISSA ENG.
M uhammad Khidir enjoys school and sports very much. He is playful, active and a good-natured 12-year-old. He took a keen interest in floorball and joined his school’s team. Khidir would look forward eagerly to each training session and
scoring for the team would make his day.
Then, one day in July 2011, an uneasiness gripped Khidir. He felt weak and tired. The doctor advised him to cease all strenuous physical activity. Soon, several worrying symptoms emerged. He experienced severe headaches, loss of appetite and lethargy. After each meal, he would vomit. These phenomena affected his studies and his grades declined. More than that, he would wet his bed nightly, causing him to suffer from low self-esteem. His parents were very worried and brought him to the doctor again.
The doctor could not identify the problem but prescribed medicine to relieve his symptoms. Thinking that perhaps Khidir was feeling depressed as he could not take part in floorball, they took him for a holiday in Malaysia during the December school holidays. Instead of being all excited and enthusiastic as he normally would, Khidir slept throughout the holiday. He went back to the doctor and was referred to KK Women’s and Children’s Hospital for a more comprehensive checkup. A CT scan showed he had a brain tumour.
His mother, Mdm Rosnani bte Arshad, a Community Management Executive, recounted, “We couldn’t take the news when we heard it. I blamed myself for not taking his word seriously. We thought he was just upset. We would never have imagined it to be a brain tumour. I was at a loss.”
Muhammad Khidir bin Yusri with his parents, Mr Yusri bin Ariffin and Mdm Rosnani bte Arshad.
Given his critical condition, Khidir had to undergo an immediate operation to remove the tumour. His parents explained his condition to him and the need for an immediate surgery. Khidir took the news calmly and did not shed a single tear. His family, including an elder sister and a younger sister, on the other hand, was anxious and perturbed as they camped overnight outside the operating theatre and waited.
After surgery, his eyesight and movements were affected because his tumour was resting on a major nerve in the brain. He was unable to focus his eyes and had to undergo physiotherapy to co-ordinate his movements.
To continue with his recovery, he had to undergo cycles of chemotherapy and radiotherapy as part of the treatment.
Mdm Rosnani added, “After the first chemotherapy session, Khidir developed a high fever. He was very quiet, very pale and shivering. We rushed him straight to the hospital. I really thought that he wasn’t going to make it that night.”
Fortunately, Khidir’s condition stabilised and he was discharged from the hospital. By the second chemotherapy session, he was able to better cope with the side effects. Despite the complicated prescriptions, Khidir took personal responsibility. He took his medicine promptly and also loaded himself with sufficient water, knowing that keeping himself hydrated was crucial for his health.
Despite his optimism and determination to lead a normal life as soon as possible, reality was not in his favour. Khidir had to skip school for half a year.
He was due for his Primary School Leaving Examination (PSLE) in October. The odds were stacking up against him.
His family wanted him to sit for the PSLE in the following year. Khidir refused. He wanted to take the examination together with his peers. As he was unable to attend school, his cousin coached him on his schoolwork. His teachers visited him at home and brought him the homework given out in class. The principal was also very concerned about his condition. Throughout, Khidir has to balance his treatment sessions, the unpleasant side effects, coping with his school work, and the pressure to do well for the national examination.
After his final radiation treatment, he returned to school and was briefly worried about another challenge – hair loss. He had a bald patch on his head. Fortunately, his classmates welcomed him gleefully and supported him with their friendship. Khidir was delighted. He stayed back for extra classes to catch up with his lessons. For his diligence and will power, he was recognised with the Character Development Award by his school.
When the PSLE results were released, Khidir was elated to find that his efforts had paid off. He passed his examination. Like most of his mates, he is continuing with his studies in a secondary school this year. His wish for the New Year is obvious. “I hope to slowly go back to sports, especially floorball!”
4 5SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

NCCS SETS UP THE INTEGRATED TRANSLATIONAL ONCOLOGY NETWORK The National Cancer Centre Singapore (NCCS) has joined Bayer Healthcare and five other research institutions in Singapore to set up the Integrated Translational Oncology Network. With greater collaborations fostered by the Network, it is expected that more will be done to fight the growing cancer burden in Asia Pacific. CHARISSA ENG reports.
T he Asian disease biology is different when compared to other regions in the world. Certain diseases like gastric
and liver cancer are more prevalent among Asians than in others, for example. To address this difference, collaborators set up the Network to fight the cancers prevalent in Asia by enhancing research and development (R&D) collaborations.
In working closer together, researchers hope to better understand the Asian disease biology to develop new specific therapeutics. The implication is that research ideas can get translated to the clinic faster.
On a macro level, the Network hopes to affirm Singapore’s position as a Centre for strategic partnerships, and also where R&D capabilities are deepened to further our standing as a premium biomedical hub for the region.
Currently, cancer is fast emerging as one of the most significant health problems worldwide. In Singapore, according to the Singapore Cancer Registry, the incidence (number and rates) of cancer for the period 2006-2010 has increased compared to the incidence reported for the period 2005-2009 though the composition and order of top ranked cancers have remained the same. There is, therefore, a pressing need for scientific breakthroughs to diagnose and treat cancer early and effectively.
As part of the collaboration, NCCS is currently working on a few projects.
Prof Huynh The Hung, Principal Investigator of the Laboratory of Molecular Endocrinology at NCCS, is working on profiling selected Bayer compounds and compound combinations. He is also doing efficacy profiling in specific patient-derived models from liver and gastric cancers, and correlation analysis with the molecular and genetic characteristics. Prof Huynh is, in other words, trying to get as close as possible to the human situation, using an animal’s body.
Prof Huynh said, “Through this collaboration, researchers and clinicians in Singapore are able to gain access to Bayer’s experimental pipeline drugs. As efficacy, toxicity and indications of novel drugs are largely unknown, researchers on both sides stand to benefit mutually from the results of the collaboration. New knowledge gained may possibly unveil previously undiscovered cancer aberrant biological pathways.”
“The information gathered from such studies may be directly used to justify and support human clinical trials. This would shorten the time required for each compound demonstrating significant efficacy and/or survival advantage to enter clinical trials. This would also benefit patients directly and significantly reduce associated cost and time normally required for new drugs to enter clinical settings.”
NCCS SHOWS IMPROVEMENT IN OVERALL PATIENT SATISFACTION SURVEY
The Patient Satisfaction Survey (PSS) is an annual exercise conducted by the Ministry of Health (MOH) on a nationwide basis for all public healthcare institutions. Its aim is to provide an indication of how patients rate the overall services provided by the institutions in various areas.
T o improve, one must first understand his/her weaknesses in order to right the wrongs. Hence, the PSS offers healthcare institutions the data to analyse their patients’ feedback and understand
how to improve their services.
In its determination to improve on its previous scores, the National Cancer Centre Singapore (NCCS) saw its staff putting in every effort to shore up the weak links. The NCCS has always taken patients’ feedback seriously, and is thus pleased that its collective effort has paid off.
Overall satisfaction scores recorded a 12.1% increase from 2011 to reach 77.4% in 2012. This is one of the significant improvements in scores for NCCS.
Apart from overall satisfaction, patients were also polled in three other areas, namely overall experience, willingness to recommend and value for money.
In terms of overall experience, patients were asked if the institution has met the patients’ expectations. NCCS obtained a 15.5% increase in scores from 67.7% in 2011 to 83.2% in 2012.
When patients were asked if they would recommend NCCS to a friend or relative who had the same medical condition, 85.6% of the patients surveyed in NCCS said they will do so. This is a rise from 74.2% in 2011.
In evaluation of overall value for money, patients were asked to rate the charges levied by an institution. NCCS ranked among the top as the best value for money among the various institutions at 55.3% though this is a 9.2% decline in score.
One of the metrics used for the survey was how expectations and actual satisfaction measure up to each other. This metric was used to assess the perception towards the knowledge and skill executed, care and concern, and clarity of explanation given by doctors, nurses and allied health professionals. It was also used to assess the perception towards care-coordination, facilities and waiting time. It is hoped that by zooming into each individual area, the problematic areas can be sieved out for improvements to be made.
NCCS doctors were exemplary in this area and were able to measure up to patients’ satisfaction in the three areas of knowledge and skill, care and concern, and clear explanation. According to the indices, the doctors’ scores in these areas have obtained an Excellent Class classification in 2012, an improvement from the previous year. The facilities at NCCS were also perceived to be adequate and patients were largely satisfied with the cleanliness, maintenance and the ease of finding one’s way.
All in all, NCCS has done well for PSS 2012. The waiting time for doctors remains to be the biggest challenge for the Centre and NCCS will do its best to look into more measures to improve in this area.
BY CHARISSA ENG
Another doctor, Dr Daniel Tan, Consultant at the Department of Medical Oncology, is currently involved in the pharmacodynamic and pharmacokinetic study of Regorafenib in biopsy-amenable colorectal cancer patients to evaluate tumour bio-markers, anti-tumour activity and safety. He is also leading multiple translational early phase trials in NCCS that involve molecular screening of individual tumours to improve delivery of personalised cancer therapy.
Dr Tan said, “It is always important to find out the tolerability of a drug and in what dosage to ensure that the compound is safe in humans. Every step of this is crucial. We have to understand a particular drug in the laboratory, like its molecular characteristics, and then we can apply it in clinical settings. The design of the latest trial protocol leverages a lot on the different partners so it is crucial that we work fast and we work well together so that more projects can be achieved in shorter periods of time.”
The Network is supported and facilitated by the Economic Development Board (EDB). The parties in the network can look forward to sharing their strategic vision and jointly develop and evaluate novel treatment options for Asian prevalent cancers in collaborative projects and trials. Joint activities, such as annual meetings, workshops or lectures will also be organised, enabling further collaborations with other leading centres in Asia Pacific.
The other partners in the collaboration are the Cancer Science Institute of Singapore, Duke-NUS Medical School, National University Cancer Institute, Singapore, Singapore General Hospital and A*STAR’s Singapore Bioimaging Consortium. It is anticipated that the network will provide cancer patients in the region with greater accessibility to cutting-edge therapies.
6 7SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

M utant p53 is also found in the germ-line in some Li-Fraumeni syndrome patients who are highly
susceptible to cancers, suggesting that mutant p53 may exhibit dominant-negative (DN) activities or that reduced p53 activity may be sufficient to drive carcinogenesis. Although a large body of in vitro work using overexpressed mutant p53 has demonstrated mutant p53’s ability to bind and inhibit wild-type when both co-exist (DN effect), with the initial generation of knock-in mice and cells expressing mutant p53 indicating that DN activity is displayed in some cell types such as embryonic stem cells, breast and lung epithelium, detailed characterisation of mutant p53’s DN activity in multiple tissues after p53 activation and in the context of concomitant tumorigenesis has not been performed, and its significance is not well understood.
As tumours generally retain the wild-type allele in mutant p53 expressing cells in the early phases during which chemotherapy and radiotherapies may be given, the impact of mutant p53’s DN effect can be expected to impact on treatment and survival outcomes.
Extending their study, the researchers investigated the possibility of mutant p53 acquiring Gain-of-Function to drive carcinogenesis. The team compared mouse strains with R172H mutations vis-à-vis R246S and showed that GOF was found only in the former. This showed that GOF of mutated p53 is specifically dependent on mutation-type but is not exhibited across all kinds of genetic mutations, indicating that mutation found in human cancers can behave differently. More investigation is required to determine the possibility of targeting mutant p53 without affecting wild-type p53 in human cells to test the efficacy on cancer therapeutic response.
BY VERONICA LEE
THE ROLE OF DOMINANT-NEGATIVE OR GAIN-OF FUNCTION PROPERTIES OF MUTANT P53
It is known that mutations in p53 occurs in over 50% of human cancers and during the course of tumourigenesis, the mutant allele co-exists with the wild-type allele in the cell for a period of time until the wild-type allele is lost due to loss of heterozygozity which leaves behind only the mutant allele in some cancers. This observation suggests that complete loss of wild-type p53 further promotes tumourigenesis and cells expressing only mutant p53 may have advantages through acquired gain-of-functions. This is supported by the previous analysis of two strains of knock-in mice expressing hot-spot mutants R172H and R270H, which revealed that mutants of p53 were capable of inhibiting p63/73 function to prevent the proliferation with apoptosis. This led to elevated enthusiasm – that all p53 mutants generally exhibit gain-of-functions (GOF) that could be amenable to therapeutic targeting.
To address the role of DN and GOF, Prof Kanaga Sabapathy, Principal Investigator in the Laboratory of Carcinogenesis and Head of the Division of Cellular and Molecular Research, NCCS and his team carried out studies using genetically-engineered knock-in mice strains expressing varying levels of mutant p53. The results showed that DN effect is observed after acute p53 activation by a variety of chemotherapeutic drugs and irradiation which led to reduction in cell death and impact on cancer treatment.
H igh on its agenda was the discussion of state-of-art diagnostic and therapeutic management of soft tissue sarcoma and osteosarcoma. Despite the somber nature of the topic, the atmosphere was a light-hearted one as participants delved into
the unknown to get solutions to their concerns.
Participants shared their knowledge when they were presented with challenging real-life sarcoma cases and given the opportunity to vote for the best course of diagnostic/therapeutic option via an interactive audience response system. Thereafter, the expert panel engaged them in thought-provoking debates on the best course of action guided by the latest scientific literature. They were also treated to presentations by experts from the various sub-specialties within sarcoma.
This event is the brainchild of a group of enthusiastic and passionate sarcoma doctors from across Singapore in the fields of Surgical Oncology, Orthopedics Surgery, Medical Oncology, Radiation Oncology, Pediatric Oncology, Radiology and Pathology. It was supported by the Department of Medical Oncology and Post-Graduate Education Unit of NCCS in an effort to engage and educate the larger medical community.
Dr Quek who is a member of the Singapore Sarcoma Consortium, believes the symposium would be of great benefit to the medical community as it serves as a platform for discussion, exchange of information and expertise for a challenging disease such as sarcoma. He hopes that through these regular education and research meetings, medical professionals would be updated on all the latest aspects related to the field of sarcoma, translating to better care for our patients.
This 1st Singapore Sarcoma Consortium Education and Research Meeting 2013, was organised by the NCCS at its Peter and Mary Fu Auditorium.
INAUGURAL SARCOMA SYMPOSIUM: EXPERTS SHARE KNOWLEDGE Timely Updates on a Challenging Disease
BY AMAL LUQMAN Executive Department of Medical Oncology
Over 100 participants gained new insights about the management of sarcomas through an interactive and buoyant session of mutual learning between sarcoma experts and members of the scientific community held on 2 March.
In his opening speech, organising chairperson and Senior Consultant from NCCS’s Department of Medical Oncology, Dr Richard Quek, reinforced the complexity and heterogeneity of sarcomas and underlined the need for greater integration of care within a multi-disciplinary team.
Dr Richard Quek, NCCS, chairing the session
Dr Aung Lele, KKWCH, Dr Mark Edward Puhaindran, NUH, Dr Sathiyamoorthy Selvarajan, SGH
8 9SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

GAINING A SENSE OF CONTROL AND MASTERY
Art expression can also enhance one’s sense of mastery and control (Council, 2003). In Figure 5 below, it shows a drawing of cancer by the same 9 year old girl. She imagined her cancer to be three big tumours joining together. The outline was in brown as she thinks that brown is the colour of the tumour. However, she had symbolically coloured them over with her favourite colours, giving her a sense of control.
AIDS IN UNDERSTANDING CANCER AND ITS TREATMENT
Children are often confused when cancer happens in the family. Besides coping with the uncertainties, they also have to make sense of the many medical terms and jargons. Figure 6 shows the drawing of a 12 year old boy whose mother is receiving chemotherapy for breast cancer. He described his own feelings and experience of coping with his mother’s cancer as living in a dark gloomy world with many questions and uncertainties. The session not only allowed him the freedom to express his feelings of living with uncertainties but also gave him an opportunity to ask questions that he has on his mind. Figure 7 is his drawing of the war between cancer and chemotherapy.
HEALING THROUGH ART THERAPYBY SARYNA ONG Principal Medical Social Worker/ Art Therapist Department of Psychosocial Oncology
The diagnosis of life-threatening illnesses like cancer can place profound stress on the patients and their families. As a Medical Social Worker and Art Therapist in the National Cancer Centre Singapore, I have worked with many young children; some of them are young children with cancer and others are young children whose parents are diagnosed with cancer. Whether they are young cancer patients or young children coping with parental cancer, a diagnosis of cancer in the family poses many challenges to the emotional and psychological well-being of a child.
BUILDING SELF ESTEEM
Engaging in art can be a powerful vehicle for building self-esteem and sense of well-being. ‘My Mini Flower Gardens’ (Fig. 4) was painted by a 9 year old girl with sarcoma. She had started art therapy before the start of her radiotherapy. Towards the end of the radiotherapy sessions to the head and neck region, she was unable to speak due to side effects of treatment. However, she was still enthusiastic to come for her art therapy session right after her treatment. Without prompting, she painted on the disposable plastic plate usually given to her as a paint palette. Though she was unable to speak in this session, she could still communicate through her painting. Her painting depicted the plants she kept at home and how she will talk to them to help them grow well. Each flower in the painting represented a family member whom she loves. Though limited by speech, enabling art expression and creativity is limitless. Art therapy can also be a way to discover the patient’s strength and aid in building the self-esteem.
C ancer and its treatment often rob the child and family of their normal routine and their sense of security and safety as they deal with uncertainties. For young children with cancer, the challenges of adjusting to treatment and isolation from peers,
school and even home, can be a trying period. For children coping with parental cancer, the separation from a parent through hospitalisation, viewing body image changes and physical care of the ill parent are some possible sources of psychosocial distress.
Unlike adults who have the verbal skills to express themselves or find means to seek help, children are less able to do so. This is when the benefits of bringing art therapy to children can make a difference to their coping with cancer.
ART AS A VISUAL LANGUAGE FOR CHILDREN
Art is the language of children. For children who may not have a fully developed vocabulary to express their emotions and experiences, art expression is a natural language for them to express themselves. It helps children to get in touch with feelings that cannot be easily expressed in words (Malchiodi, 2007). The process of art making often also prompts children to speak more than they would in a solely verbal therapy (Gross & Haynes, 1998). In addition, the artwork serves as a ‘container’ for powerful feelings and aids in the communication between the child and art therapist (Waller, 2006).
Below are some drawings of children depicting how they feel about their parents having cancer:
Fig 1. Drawing
from a 6 year
old girl
Fig 2. Drawing
from a 7 year
old boy
Fig 3. Drawing
from a 12 year old girl
FROM A FOREIGN WORLD TO A FAMILIAR WORLD
Navigating the medical world and being surrounded with the hospital’s sight, smell, sound, and pace, can be very alien to most children. Art therapy forms a bridge between the foreign world of medicine and a familiar world of play using art materials. A visit to the art therapist is a respite for children from taking medicine, blood tests, investigations and more in the hospital. The creative process itself can be relaxing and empowering. Under the guidance of a skillful art therapist, the child can respond to their illness or their parent’s illness in meaningful ways and find emotional support and healing.
Art therapy in a medical setting offers a safe place for patients and families to express powerful emotions associated with cancer diagnosis and cancer journey. It offers potential for tapping into their inner resources and empowering them to cope better with the illness.
REFERENCES:
Councill, T. (2003). Medical Art Therapy with Children. In Malchiodi, C. A. (Ed). Handbook of art therapy. New York: Guilford Press.
Gross, J., & Haynes, H. (1998). Drawing facilitates children’s verbal reports of emotionally laden events. Journal of Experimental Psychology, 4(2), 163-179.
Malchiodi, C. A. (2007). The Art Therapy Sourcebook (2nd Ed.) New York: McGraw Hill.
Waller, D. (2006). Art Therapy for Children: How it Leads to Change. Clinical Child Psychology and Psychiatry, 11(2), 271-282.
For more information on the Art Therapy Programmes offered by NCCS, please visit: http://www.nccs.com.sg/PatientSupportProgramme/ChildrenArtTherapy
WHAT IS ART THERAPY? • A form of psychotherapy that uses art and visual
materials to assist communication with a patient through the images created.
• No prior experience or skill in art is required as the focus is on the art process rather than the aesthetic merit of the artwork.
• Suitable for people of all ages.
• Used in a variety of settings such as medical and mental institutions, schools, prisons, nursing homes, hospices and family service centres for people experiencing developmental, medical, educational, and psychological distress.
• Art therapists are mental health professionals trained in the use of art as well as psychological and therapeutic approaches. They hold a Master’s Degree in the field.
Fig 4. ’My mini flower garden’ Fig 6. Dark gloomy world by 12 year old boy Fig 7. War between cancer and chemotherapy
Fig 5. Drawing of cancer
10 11SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

产生控制和征服感
艺术表达也能加强一个人的控制和征服感 (Councill, 2003年)。图5是同一名9岁女童所画的癌症。她想象自己的癌症是三个结合在一起的大肿瘤。她用褐色画出肿瘤的轮廓,因为她认为肿瘤是褐色的。不过,她象征性地把它们填上她最喜欢的颜色,让她从中产生一种控制癌症的感觉。
促进对癌症及其治疗的了解
当家里有人罹患癌症,孩童往往会感到困惑。除了面对不确定性,他们还必须理解许多医学名词和术语。图6是一名12岁男童的画作,他的母亲罹患乳癌,正在接受化疗。面对母亲患癌的事实,他形容自己犹如活在一个充满疑问和不明确的黑暗世界里。艺术治疗不仅让他自由地表达活在不确定性当中的感受,而且给予他一个提出心中疑问的机会。图7是他描绘癌症与化疗之间的战争。
通过艺术治疗 走出心灵创伤SARYNA ONG
新加坡国立癌症中心 心理社会肿瘤科部门 首席医疗社工/艺术治疗师
确诊患上癌症等危及生命的疾病后,患者及其家属都可能面对巨大的压力。身为新加坡国立癌症中心医疗社工兼艺术治疗师,我曾与许多年幼孩童接触。他们有的是癌症患者,有的是父母患有癌症。无论是他们自己或父母患上癌症,孩童在情感和心理上都面对着许多挑战。
建立自信
进行艺术创作,是建立自信和健康的强大工具。“我的小花园”(图4)是一名患肉瘤的9岁女童所绘。她在进行放射治疗之前,就开始接受艺术治疗。在头部和颈部的放射治疗即将结束时,她因治疗副作用而无法说话。不过,她仍然在放射治疗后,兴致勃勃地进行艺术治疗。她自主在一个通常用作调色板的一次性塑料盘上作画。虽然她无法在治疗中开口说话,但她仍然能通过画作来沟通。她的画描绘了她在家里种的植物,以及她如何跟这些植物说话,帮助它们更好地成长。画中的每一朵花,代表着她所爱的家人。虽然语言能力受限,但艺术表达和创意是无限的。艺术治疗也能用来发掘病患的长处,帮助他们建立自信。
癌症及其治疗往往会影响小孩及家人的日常作息,他们也会因为面对不确定性的状况而失去安全感。对罹癌的年幼孩童而言,适应治疗,以及和朋友、学校, 甚至家人隔离,是一段相当艰难的时期。对父母患有癌症的孩童而言,父母因住院治疗而分开、看到父母的身体变化,以及照顾父母,都可能对孩童造成心理困扰。
与成人不同的是,孩童无法通过言语表达情绪或寻求帮助。因此,艺术治疗能够帮助他们更好地面对癌症。
艺术是孩童的视觉语言
艺术是孩童的语言。对还没掌握足够词汇量来表达情绪和经验的孩童而言,艺术是他们自我表达的天然语言。它能帮助孩童进入言语所难以表达的感觉 (Malchiodi, 2007年)。与纯粹的语言治疗相比,艺术创作过程往往能引导孩童表达得更多 (Gross & Haynes, 1998年)。此外,艺术作品也是一个装载强烈情感的“容器”,能促进孩童与艺术治疗师之间的沟通 (Waller, 2006年)。
以下是一些孩童的画作,描绘了他们对父母罹患癌症的感受:
图1: 一名6岁女
童的画作
图2: 一名7岁男
童的画作
图3: 一名12岁女
童的画作
参考书目
Councill, T. (2003). Medical Art Therapy with Children. In Malchiodi, C. A. (Ed). Handbook of art therapy. New York: Guilford Press.
Gross, J., & Haynes, H. (1998). Drawing facilitates children’s verbal reports of emotionally laden events. Journal of Experimental Psychology, 4(2), 163-179.
Malchiodi, C. A. (2007). The Art Therapy Sourcebook (2nd Ed.) New York: McGraw Hill.
Waller, D. (2006). Art Therapy for Children: How it Leads to Change. Clinical Child Psychology and Psychiatry, 11(2), 271-282.
想知道更多关于新加坡国立癌症中心艺术治疗的项目,请游览: http://www.nccs.com.sg/PatientSupportProgramme/ChildrenArtTherapy
何谓艺术治疗?
• 一种通过使用艺术和视觉材料画出图像,促进与病患沟通的心理治疗。
• 无需经验或艺术才能,因为治疗的重点在于艺术的创造过程,而不是艺术作品的美感。
• 适合各年龄层的人。
• 适用于医院及精神病院、学校、监狱、养老院、疗养院和家庭服务中心等,为面对成长、医疗、教育和心理问题的人提供援助。
• 艺术治疗师是受过训练的心理健康专业人士。他们拥有相关领域的硕士学位,懂得如何运用艺术、心理学和各种疗法。
从陌生到熟悉的世界
对多数孩童而言,走入医疗环境,以及被医院的景象、味道、声音和节奏围绕着,是非常陌生的。艺术治疗可在陌生的医疗世界和熟悉的游戏般绘画世界之间搭建一座桥梁。接受艺术治疗,可让孩童在医院除了吃药、验血和检验之余,给自己一个舒缓的机会。创作过程本身能赋予力量和让人感到放松。在经验丰富的艺术治疗师指导下,孩童能以有意义的方式面对自己或父母的疾病,以及获得情绪上的支持和治疗。
在医疗环境中接受艺术治疗,能让病患及其家人放心抒发他们在确诊患癌和抗癌过程中所经历的强烈情感。艺术治疗为他们提供一个从内在寻找力量的管道,让他们更好地面对疾病。
图4: 我的小花园 图6: 12岁男童笔下的黑暗世界 图7: 癌症和化疗之间的战争
图5: 癌症
12 13SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

A CHARITY OF CHOICEBY FLORA YONG Manager, Community Partnership, Division of Community Outreach and Philanthropy
ONE DOES NOT NEED TO BE RICH TO GIVE TO CHARITY.
In fact, in the National Volunteer and Philanthropy Centre’s Individual Giving Survey 2010 supplement, it was reported that those who earn less than $1,000 a month donated a higher percentage of their personal annual income compared to other income groups.
W hen you get a cold call requesting for donations to the needy, do proceed with caution. There is a chance that the money you are giving is to an organisation that is not a charity, or to a charity but spends most of
what it collects to pay third party fundraisers. There are plenty of bogus charities out there, as well as legitimate ones. Thus, it is good to do some research before donating to make sure your hard-earned money is put to good use.
A legitimate charity should have a working phone number and mailing address. Do take a few minutes to call up the charity before making your decision to donate. Make sure you are speaking to a live person on the phone and not some recorded message. It would be good if you can ask questions about the charity’s purpose, examples of how they have made a difference, and their short-term and long-term goals.
The charity you intend to support should be upfront about how donated money is spent. Find out what percentage of your dollar goes towards the actual charitable services versus the amount spent on costs like administration or for fundraising. Do keep in mind, however, that if a charity is young and less established, it may use more of your dollar for start-up expenses as they do not have a base of loyal donors.
Q: HOW DID YOU SPEND YOUR WEEKEND?
MIA: We set up a table and we set up the signs. We baked cookies and we made lemonade. A lot of people came to our lemonade stand.
JACKSON: Eating cookies.
Q: DO YOU KNOW WHAT THE ACTIVITY WAS FOR?
MIA: Because we were giving money to help fight cancer.
A WEEKEND OF GOODNESSNO PLANS FOR THE KIDS THIS WEEKEND? HERE’S SOME INSPIRATION.
ADELINE TEO interviews Ms Gillian Pearl (a working mum) and her two young children (Mia, 5 and Jackson, 3), who had a meaningful weekend (in January) – running a lemonade stand and raising money for the cancer cause. In a short span of a few hours, the kids raised a whopping $641 to be shared between the NCC Research Fund and the Mount Sinai Hospital Montreal palliative care unit.
Kids’ Fundraiser for NCCS, Mia and Jackson lemonade stand.
Q: WERE YOU TIRED?
MIA: No.
Q: DID YOU ENJOY IT? WHAT DID YOU LEARN?
MIA: Yes. I learned that giving away money is good and that kids should give away more money more often.
Q: WOULD YOU LIKE TO DO IT AGAIN?
MIA: Yes!
Q: FOR MUM – WHAT WAS YOUR MOTIVATION AND PURPOSE/GOAL(S) FOR THIS ACTIVITY?
GILLIAN: I was raised in a very philanthropic home and want to pass on the same traditions to my kids. I hope to teach them the importance of helping others and contributing to the communities in which they live.
Q: DID YOU ACHIEVE YOUR GOAL(S)? WHAT WERE YOUR THOUGHTS AND FEELINGS AT THE END OF THE DAY?
GILLIAN: Yes, we did. I was very proud of the kids. I think they understood what the activity was all about and had a lot of fun doing it, too. They are excited to do it again and I think running a lemonade stand as a fundraising activity is a great way for kids to get involved in helping others through their own efforts.
Q: HOW LONG DID IT LAST?
MIA: Four hours – ummm – don’t know.
Q: HOW DID YOU FEEL WHEN YOU FIRST STARTED DOING IT?
MIA: Excited!
Q: HOW DID YOU FEEL AT THE END OF THE ACTIVITY?
MIA: Happy to give the money away.
It is also wise to check that the charity has in place a privacy policy to ensure that your name and personal details are not handed to another organisation for other purposes.
Once you have decided on a charity, how much should you give? There is no fixed amount to what you wish to give. Do consider getting into the charitable habit by making small regular donations throughout the year with GIRO deductions. Regular giving is the most cost-effective way to support a charity. Donors who donate to a charity with an institute of public character (IPC) status will be accorded 2.5 times tax deduction based on the donation amount.
There are also other ways to give without using money from your own pocket. For example, if you are celebrating your birthday, your wedding anniversary or getting married, you may wish to consider suggesting to your guests to make a donation to your favourite charity in your name, rather than buying gifts.
Supporting local charities is great! Nothing can substitute the direct involvement with a local charitable group. It is the essence of the Singapore community coming together to help those who are in need.
REFERENCES:
National Volunteer & Philanthropy Centre Individual Giving Survey 2010 http://www.nvpc.org.sg/knowledge/researchpublications.aspx
Individual Giving Survey 2010 (Supplement) http://www.nvpc.org.sg/knowledge/researchpublications.aspx
14 15SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013

OUTREACH – PUBLIC FORUMS & CANCERWISE WORKSHOPS
Event Date, Time, Venue Registration
CancerWise Workshop – Basics Of Cancer Part 1
TOPICS:
• What is Cancer?
• What causes Cancer?
• Risk, Signs & Symptoms
• Prevention & Screening
• Types of Cancer Screening
• What are Cancer Tumour Markers?
13 April 2013, Saturday
Session will be conducted in English & Mandarin at different venues
Registration : 1pm Workshop : 1.30pm to 4.00pm
MANDARIN SESSION Function Room, Level 4
ENGLISH SESSION Peter & Mary Fu Auditorium, Level 4
National Cancer Centre Singapore 11 Hospital Drive Singapore 169610
Free Admission
Strictly No Admission for children below 12 years old. Registration is a MUST as seats are limited.
REGISTRATION IS BY PHONE ONLY
Please call: 6236 9447 / 6236 9432 / 6225 5655
Monday to Friday: 8.30am to 5.30pm
Bilingual Public Forum – Reducing Cancer Risk For Women
TOPICS:
• Common Gynaecological Problems
• Contraceptive Pills & Hormone Replacements Therapy – Are there health risks?
• Myths & Misconceptions
• Cancers of the Female Reproductive System: Cervix, Ovary and Uterus
• Risk Factors, Signs & Symptoms
• Early Detection & Prevention
11 May 2013, Saturday
MANDARIN SESSIONTime: 9.15am to 10.30am (Registration: 9am to 9.15am)
ENGLISH SESSIONTime: 11.15am to 12.30pm (Registration: 11am to 11.15am)
Health Promotion Board Auditorium, Level 7 3 Second Hospital Avenue Singapore 168937
Free Admission
Strictly No Admission for children below 12 years old. Registration is a MUST as seats are limited.
REGISTRATION IS BY PHONE ONLY
Please call: 6236 9447 / 6236 9432 / 6225 5655
Monday to Friday: 8.30am to 5.30pm
CancerWise Workshop – Coping With Fear Of Recurrence
TOPICS:
• Understanding Fear and Cancer Recurrence
• Tips in Coping with Fear and Cancer Recurrence
• Building Resilience and Positive Thinking
15 June 2013, Saturday
Session will be conducted in English.
Registration : 1pm Workshop : 1.30pm to 4.00pm
Function Room, Level 4 National Cancer Centre Singapore 11 Hospital Drive Singapore 169610
Free Admission
Strictly No Admission for children below 12 years old. Registration is a MUST as seats are limited.
REGISTRATION IS BY PHONE ONLY
Please call: 6236 9447 / 6236 9432 / 6225 5655
Monday to Friday: 8.30am to 5.30pm
The information is correct At Press time. NCCS reserves the right to change programmes or speaker without prior notice.
SEMINARS / FORUMS / TUMOUR BOARDS / SMC-CME ACTIVITIES FOR MEDICAL PROFESSIONALS
APRIL 2013Date Time Event Information CME Pt Registration Contact
1, 8, 15, 22, 29 3, 10, 17, 24 3, 10, 17, 24 5, 12, 19, 26
5.00pm 4.30pm 5.00pm 5.00pm
NCCS Tumour Board Meetings:
Head & Neck Tumour Board Meeting Sarcoma Tumour Board Meeting General Surgery Tumour Board Meeting Breast Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1
1
1
1
V Kalai / Lim Shufen
64368294 / 6436 8283 [email protected] / [email protected]
1, 8, 15, 22, 29 1.00pm Gynae-Oncology Tumour Board Meeting
@ NCCS Level 1, Clinic A, Discussion Room
1 Lim Shufen / V Kalai
64368283 / 8294 [email protected] / nsokal @nccs.com.sg
1, 8, 15, 22, 29 1.00pm Hepatobiliary Conference
@ NCCS Level 4, Lecture Hall
1 Lim Shufen / V Kalai
6436 8283 / 8294 [email protected] / [email protected]
2, 9, 16, 23, 30 5.15pm Weekly Combined Clinical & Radiology Reviews
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Rachel Tan
6436 8165 / 6436 8172 [email protected] / [email protected]
4, 11, 18, 25 12.00pm Lung Tumour Board Combine SGH-NCCS Meeting
@ SGH Blk 2 Level 1, Radiology Conference Room
4, 18 5.00pm NCC-SGH Joint Lymphoma Workgroup Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
19 1.00pm Journal Club
Topic: To be advised Speaker:
@NCCS level 1, Mammo Suite Discussion Room
1 Phua Chay Sin
6436 8043 [email protected]
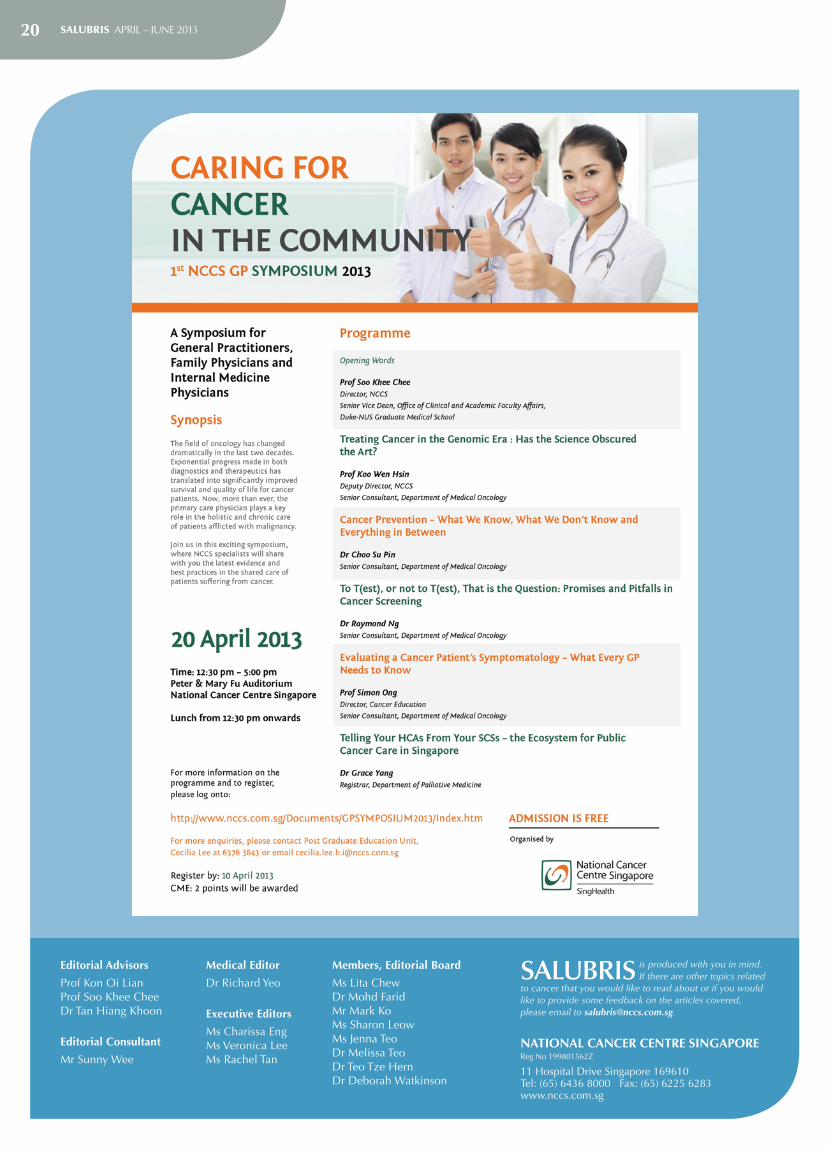
20 12.30pm to 5.00pm
Caring For Cancer in the Community
1st NCCS GP SYMPOSIUM 2013
@ Peter & Mary Fu Auditorium, NCCS Level 4
(Registration / Lunch 12.30pm – 1.30pm)
2 Post Graduate Education Unit
6376 3643 / 6236 9425 / 6236 9423 [email protected]
25 7.30am Endocrine and Rare Tumour Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
25 5.00pm NCC Neuro Onco Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Ang Hui Lan
6436 8165 / 6436 8174 [email protected] / [email protected]
26 1.00pm Teaching Session
Topic: To be advised Speaker:
@NCCS level 1, Mammo Suite Discussion Room
1 Phua Chay Sin
6436 8043 [email protected]
16 17SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013
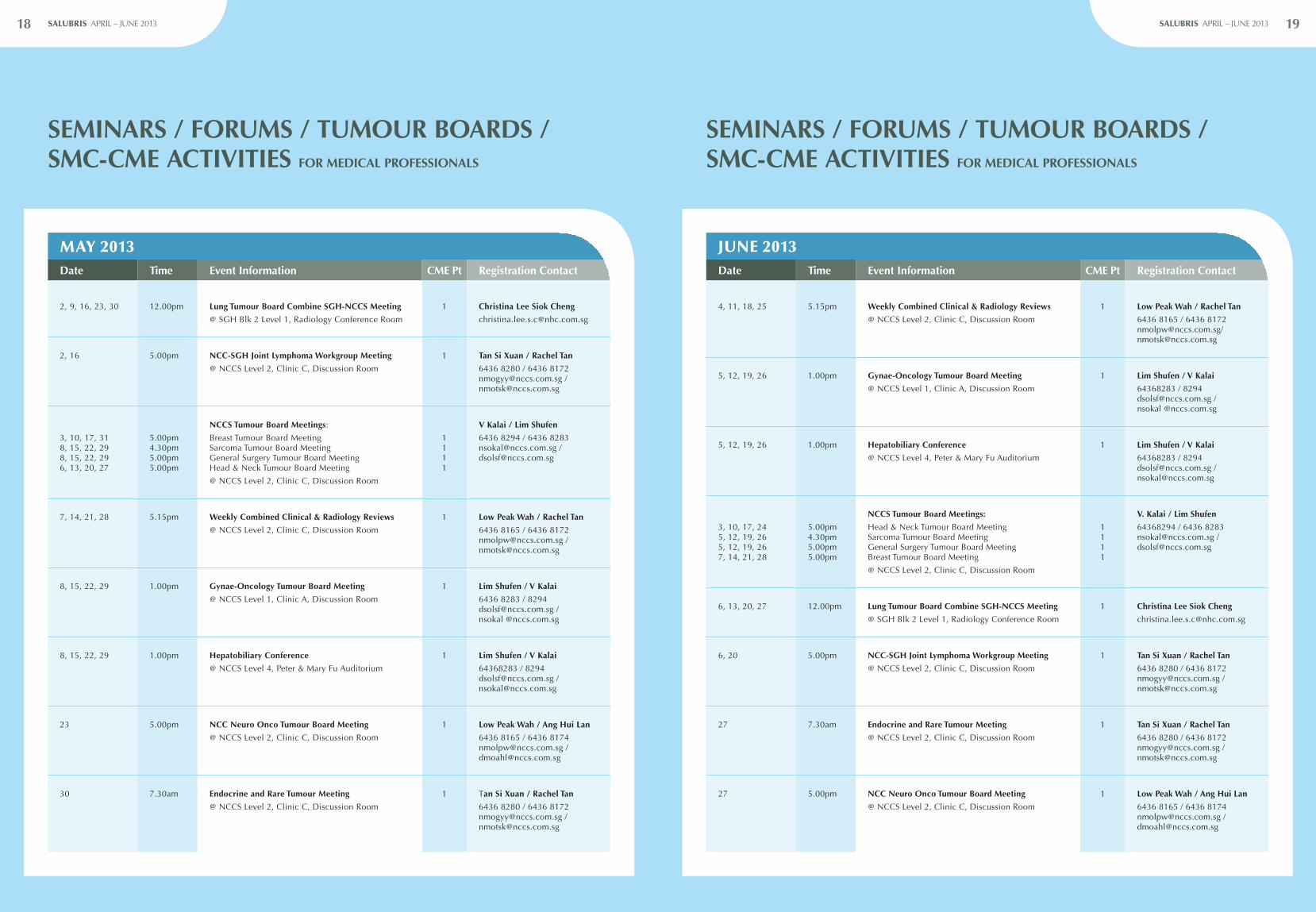
SEMINARS / FORUMS / TUMOUR BOARDS / SMC-CME ACTIVITIES FOR MEDICAL PROFESSIONALS
SEMINARS / FORUMS / TUMOUR BOARDS / SMC-CME ACTIVITIES FOR MEDICAL PROFESSIONALS
MAY 2013Date Time Event Information CME Pt Registration Contact
2, 9, 16, 23, 30 12.00pm Lung Tumour Board Combine SGH-NCCS Meeting
@ SGH Blk 2 Level 1, Radiology Conference Room
1 Christina Lee Siok Cheng
2, 16 5.00pm NCC-SGH Joint Lymphoma Workgroup Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
3, 10, 17, 31 8, 15, 22, 29 8, 15, 22, 29 6, 13, 20, 27
5.00pm 4.30pm 5.00pm 5.00pm
NCCS Tumour Board Meetings:
Breast Tumour Board Meeting Sarcoma Tumour Board Meeting General Surgery Tumour Board Meeting Head & Neck Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 1 1 1
V Kalai / Lim Shufen
6436 8294 / 6436 8283 [email protected] / [email protected]
7, 14, 21, 28 5.15pm Weekly Combined Clinical & Radiology Reviews
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Rachel Tan
6436 8165 / 6436 8172 [email protected] / [email protected]
8, 15, 22, 29 1.00pm Gynae-Oncology Tumour Board Meeting
@ NCCS Level 1, Clinic A, Discussion Room
1 Lim Shufen / V Kalai
6436 8283 / 8294 [email protected] / nsokal @nccs.com.sg
8, 15, 22, 29 1.00pm Hepatobiliary Conference
@ NCCS Level 4, Peter & Mary Fu Auditorium
1 Lim Shufen / V Kalai
64368283 / 8294 [email protected] / [email protected]
23 5.00pm NCC Neuro Onco Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Ang Hui Lan
6436 8165 / 6436 8174 [email protected] / [email protected]
30 7.30am Endocrine and Rare Tumour Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
JUNE 2013Date Time Event Information CME Pt Registration Contact
4, 11, 18, 25 5.15pm Weekly Combined Clinical & Radiology Reviews
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Rachel Tan
6436 8165 / 6436 8172 [email protected]/ [email protected]
5, 12, 19, 26 1.00pm Gynae-Oncology Tumour Board Meeting
@ NCCS Level 1, Clinic A, Discussion Room
1 Lim Shufen / V Kalai
64368283 / 8294 [email protected] / nsokal @nccs.com.sg
5, 12, 19, 26 1.00pm Hepatobiliary Conference
@ NCCS Level 4, Peter & Mary Fu Auditorium
1 Lim Shufen / V Kalai
64368283 / 8294 [email protected] / [email protected]
3, 10, 17, 24 5, 12, 19, 26 5, 12, 19, 26 7, 14, 21, 28
5.00pm 4.30pm 5.00pm 5.00pm
NCCS Tumour Board Meetings:
Head & Neck Tumour Board Meeting Sarcoma Tumour Board Meeting General Surgery Tumour Board Meeting Breast Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 1 1 1
V. Kalai / Lim Shufen
64368294 / 6436 8283 [email protected] / [email protected]
6, 13, 20, 27 12.00pm Lung Tumour Board Combine SGH-NCCS Meeting
@ SGH Blk 2 Level 1, Radiology Conference Room
1 Christina Lee Siok Cheng
6, 20 5.00pm NCC-SGH Joint Lymphoma Workgroup Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
27 7.30am Endocrine and Rare Tumour Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Tan Si Xuan / Rachel Tan
6436 8280 / 6436 8172 [email protected] / [email protected]
27 5.00pm NCC Neuro Onco Tumour Board Meeting
@ NCCS Level 2, Clinic C, Discussion Room
1 Low Peak Wah / Ang Hui Lan
6436 8165 / 6436 8174 [email protected] / [email protected]
18 19SALUBRIS APRIL – JUNE 2013 SALUBRIS APRIL – JUNE 2013
20 SALUBRIS APRIL – JUNE 2013
SALUBRIS is produced with you in mind. If there are other topics related
to cancer that you would like to read about or if you would like to provide some feedback on the articles covered, please email to [email protected].
NATIONAL CANCER CENTRE SINGAPOREReg No 199801562Z
11 Hospital Drive Singapore 169610 Tel: (65) 6436 8000 Fax: (65) 6225 6283 www.nccs.com.sg
Editorial Advisors
Prof Kon Oi Lian Prof Soo Khee Chee Dr Tan Hiang Khoon
Editorial Consultant
Mr Sunny Wee
Medical Editor
Dr Richard Yeo
Executive Editors
Ms Charissa Eng Ms Veronica Lee Ms Rachel Tan
Members, Editorial Board
Ms Lita Chew Dr Mohd Farid Mr Mark Ko Ms Sharon Leow Ms Jenna Teo Dr Melissa Teo Dr Teo Tze Hern Dr Deborah Watkinson