safety of fluoxetine: comparison with fluvoxamine
TRANSCRIPT
PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL 1: 11 1-1 17 (1992)
ORIGINAL REPORT
Safety of fluoxetine: comparison with fluvoxamine
JOHN PRICE PhD’, PATRICK WALLER MD’. SUSAN WOOD MD’, A N D ANGUS MACKAY FRCPsych’ ‘Medicines Confrol Agency arid ‘Comniittee on Safety of’kledicines, Department ofHealth, 1 Nine Elms Lane,
Vauxhall, London S W8 5NQ, UK
SUMMARY This review examines data on the safety of two 5-HT reuptake inhibitors, fluoxetine and fluvoxamine. A comparison of the spontaneous reports of suspected adverse reactions to each drug sent to the UK Committee on Safety of Medicines has been made. This does not reveal important differences in their safety profile.
KEY WORDS - Fluoxetine, fluvoxamine. spontaneous adverse drug reaction reports.
INTRODUCTION
The last decade has witnessed the introduction of a new group of antidepressants which act by inhi- biting the neuronal reuptake of 5-hydroxytrypta- mine (5-HT, serotonin). The first of these, zimeldine, was withdrawn because of its association with Guillain-Barre syndrome.’ In the UK the available drugs with this mode of action now include fluvoxamine, fluoxetine, paroxetine and sertraline. There has been considerable controversy concerning the safety of fluoxetine, with allegations that i t increases suicidal and hostile behaviour. Much clinical information has accumulated for this drug and the purpose of this review is to examine these data and, where appropriate, to make com- parisons with another 5-HT reuptake inhibitor, flu- voxamine, which has not excited the same degree of controversy.
PHARMACOLOGY
Fluoxetine (N-methyl-3-phenyl-3-propylamine) is a bicyclic antidepressant which was marketed in the UK in 1989. I t is believed to exert its antidepres- sant effects through inhibition of neuronal 5-HT reuptake. This results in decreased 5-HT turnover through a negative feedback process, and reduced numbers of 5-HT binding sites. Studies demon- strate a high degree of selectivity for the 5-HT reup-
take system, with over a hundredfold lower potency on noradrenaline and dopamine reuptake.’ In addition, fluoxetine has a very low affinity for other neurotransmitter receptors, including muscarinic receptors.
Fluvoxamine (5-Methoxy-4’-tri-fluoromethylva- lerophenone 0-2-amenoethyloxime) maleate is a monocyclic antidepressant which became available in the UK in 1987. Like fluoxetine it is a much more potent inhibitor of 5-HT than catecholamine r e ~ p t a k e . ~
PHARMACOKINETICS
Fluoxetine is well absorbed after oral adminis- tration and is metabolized in the liver to desmethyl- fluoxetine, which is also a potent inhibitor of 5-HT reuptake though less active than the parent com- pound.’ Desmethylfluoxetine, together with its glu- curonide-conjugate is excreted in the urine; further metabolism by dealkylation also occurs in the liver. Metabolism and excretion proceed slowly: fluoxe- tine and desmethylfluoxetine have elimination half- lives of 1-3 and 7-15 days, respectively, so that steady state levels are achieved only after weeks.234 Plasma levels of drug and metabolite may be detected several weeks after discontinuation, par- ticularly in patients who have taken high doses.5 Plasma levels after single doses are not affected by renal impairment, but clearance is reduced in
1053-856919210301 I 1 -07$05.00 0 1992 by John Wiley & Sons. Ltd.
Received 13 February 1991 Accepted 22 March 1992
patients with hepatic dysfunction. These obser- vations are particularly relevant to the use of other centrally active drugs in patients stopping fluoxe- tine.
Fluvoxamine is well absorbed after oral adminis- tration. It has a much shorter elimination half-life than fluoxetine of 15 hours.6 Elimination of fluvox- amine is by urinary excretion of metabolites.
REPORTS OF ADVERSE REACTIONS
In early clinical trials the most common adverse reactions were nausea (up to 24%), nervousness, insomnia, headache, tremor and anxiety (around 160/0), which were rarely sufficiently severe to lead to drug d iscont in~at ion .~*~-~ Comparative trials showed that anticholinergic effects were less com- mon than with tricyclic antidepressants, while nau- sea was more common with fluoxetine and other adverse reactions occurred with a similar fre- quency.lO-" These reactions were dose related. Doses below 20 mg/day have not been extensively studied; there is some evidence that 5 mgiday is less effective.I6 There is little evidence that higher doses confer greater effi~acy, '~ and so dosage with 20 mg/day appears to represent the optimum efficacy:adverse reaction ratio.
Comparison of fluoxetine and fluvoxamine by Prescription Event Monitoring has shown that early adverse events (occurring in the first month of treatment) were recorded more often with flu- voxamine than fluoxetine.'* Events recorded in more than 1% of recipients were similar for the two drugs, with nausea, vomiting, lassitude and malaise being the most common with fluoxetine. Other gastrointestinal symptoms, drowsiness, headache and insomnia were more frequent with fluvoxamine, although direct comparison between the studies is affected by the different periods for which the two drugs have been available.
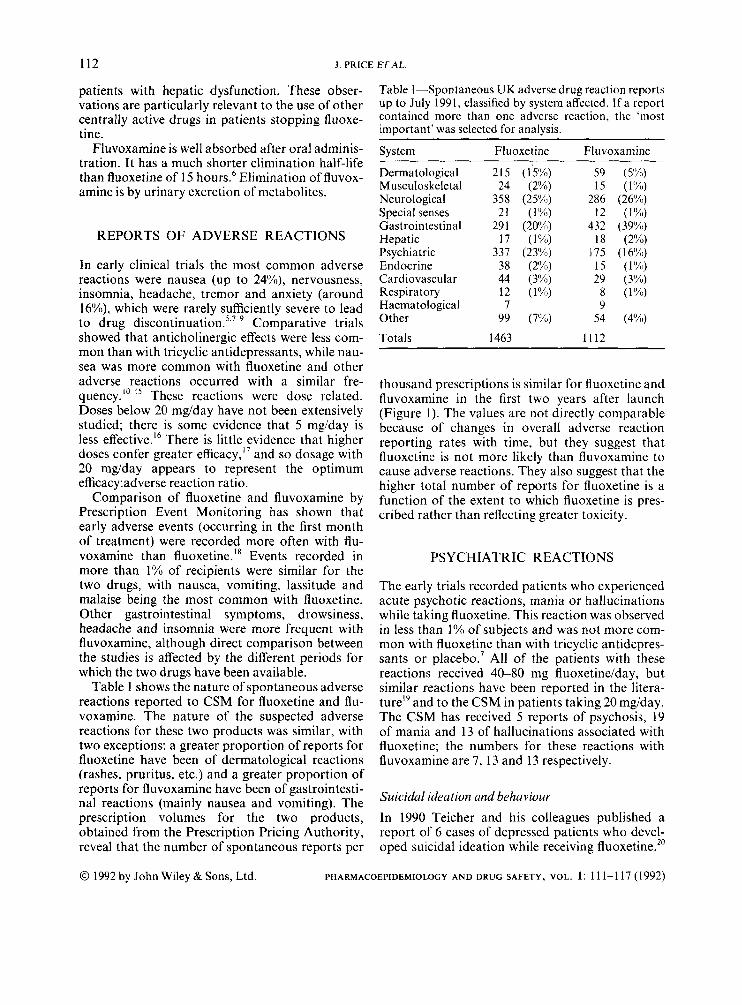
Table 1 shows the nature of spontaneous adverse reactions reported to CSM for fluoxetine and flu- voxamine. The nature of the suspected adverse reactions for these two products was similar, with two exceptions: a greater proportion of reports for fluoxetine have been of dermatological reactions (rashes, pruritus, etc.) and a greater proportion of reports for fluvoxamine have been of gastrointesti- nal reactions (mainly nausea and vomiting). The prescription volumes for the two products, obtained from the Prescription Pricing Authority, reveal that the number of spontaneous reports per
Table I-Spontaneous UK adverse drug reaction reports up to July 1991, classified by system affected. If a report contained more than one adverse reaction, the 'most important' was selected for analysis.
System FI uoxet ine Fluvoxamine
Dermatological Musculoskeletal Neurological Special senses Gastrointestinal Hepatic Psychiatric Endocrine Cardiovascular Respiratory Haematological Other
Totals
215 24
358 21
29 1 17
337 38 44 12 7
99
1463
(1 5%) (2%)
(25%) (1%)
(20%) (1%)
(2Y") (3%) ( 1%)
(7%)
(23%)
59 15
286 12
432 18
175 15 29
8 9
54
1112
(5%) ( 1%)
(26%) ( 1 %)
(39%) (2%)
( 16%~) ( 1 1%)
(3%) ( 1 1%)
(4%)
112 .I. PRICE ETAL.
0 1992 by John Wiley & Sons, Ltd. PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 1: 11 1-1 17 (1992)
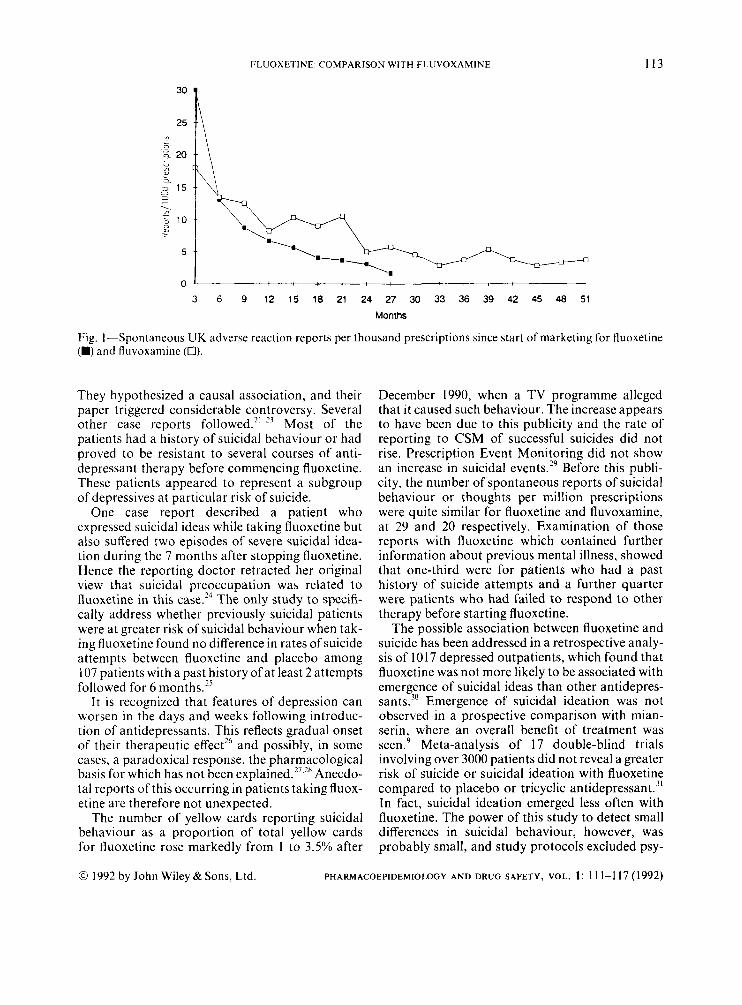
thousand prescriptions is similar for fluoxetine and fluvoxamine in the first two years after launch (Figure 1). The values are not directly comparable because of changes in overall adverse reaction reporting rates with time, but they suggest that fluoxetine is not more likely than fluvoxamine to cause adverse reactions. They also suggest that the higher total number of reports for fluoxetine is a function of the extent to which fluoxetine is pres- cribed rather than reflecting greater toxicity.
PSYCHIATRIC REACTIONS
The early trials recorded patients who experienced acute psychotic reactions, mania or hallucinations while taking fluoxetine. This reaction was observed in less than 1 % of subjects and was not more com- mon with fluoxetine than with tricyclic antidepres- sants or p l a ~ e b o . ~ All of the patients with these reactions received 40-80 mg fluoxetine/day, but similar reactions have been reported in the litera- ture" and to the CSM in patients taking 20 mgiday. The CSM has received 5 reports of psychosis, 19 of mania and 13 of hallucinations associated with fluoxetine; the numbers for these reactions with fluvoxamine are 7, 13 and 13 respectively.
Suicidal ideation and behaviour In 1990 Teicher and his colleagues published a report of 6 cases of depressed patients who devel- oped suicidal ideation while receiving fluoxetine.''
FLUOXETINE COMPARISON WITH FLUVOXAMINE 113
3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Months
Fig. I --Spontaneous UK adverse reaction reports per thousand prescriptions since start of marketing for fluoxetine (H) and fluvoxamine (0).
They hypothesized a causal association, and their paper triggered considerable controversy. Several other case reports followed.'' '' Most of the patients had a history of suicidal behaviour or had proved to be resistant to several courses of anti- depressant therapy before commencing fluoxetine. These patients appeared to represent a subgroup of depressives at particular risk of suicide.
One case report described a patient who expressed suicidal ideas while taking fluoxetine but also suffered two episodes of severe suicidal idea- tion during the 7 months after stopping fluoxetine. Hence the reporting doctor retracted her original view that suicidal preoccupation was related to fluoxetine in this case.24 The only study to specifi- cally address whether previously suicidal patients were at greater risk of suicidal behaviour when tak- ing fluoxetine found no difference in rates of suicide attempts between fluoxetine and placebo among 107 patients with a past history of at least 2 attempts followed for 6 months."
It is recognized that features of depression can worsen in the days and weeks following introduc- tion of antidepressants. This reflects gradual onset of their therapeutic effect" and possibly, in some cases, a paradoxical response, the pharmacological basis for which has not been Anecdo- tal reports of this occurring in patients taking fluox- etine are therefore not unexpected.
The number of yellow cards reporting suicidal behaviour as a proportion of total yellow cards for fluoxetine rose markedly from 1 to 3.5% after
December 1990, when a TV programme alleged that i t caused such behaviour. The increase appears to have been due to this publicity and the rate of reporting to CSM of successful suicides did not rise. Prescription Event Monitoring did not show an increase in suicidal event^.'^ Before this publi- city, the number of spontaneous reports of suicidal behaviour or thoughts per million prescriptions were quite similar for fluoxetine and fluvoxamine, at 29 and 20 respectively. Examination of those reports with fluoxetine which contained further information about previous mental illness, showed that one-third were for patients who had a past history of suicide attempts and a further quarter were patients who had failed to respond to other therapy before starting fluoxetine.
The possible association between fluoxetine and suicide has been addressed in a retrospective analy- sis of 1017 depressed outpatients, which found that fluoxetine was not more likely to be associated with emergence of suicidal ideas than other antidepres- sants.30 Emergence of suicidal ideation was not observed in a prospective comparison with mian- serin, where an overall benefit of treatment was seen.9 Meta-analysis of 17 double-blind trials involving over 3000 patients did not reveal a greater risk of suicide or suicidal ideation with fluoxetine compared to placebo or tricyclic antidepre~sant.~' In fact, suicidal ideation emerged less often with fluoxetine. The power of this study to detect small differences in suicidal behaviour, however, was probably small, and study protocols excluded psy-
0 1992 by John Wiley & Sons, Ltd. PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 1: 1 11-1 17 (1992)

114 J PRICE E T A L
0 1992 by John Wiley & Sons, Ltd. PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 1: I 1 1-1 17 (1992)
chotic patients and those considered to be at high risk. Nevertheless, these negative findings do not support the view that fluoxetine is causally asso- ciated with suicidal behaviour.
Aggressive behaviour
Fluoxetine has been alleged to induce anti-social, aggressive behaviour. Anecdotal reports have received widespread coverage in the media, and the alleged association has been used in legal defence of violent behaviour. Interpretation of the anecdo- tal reports is hindered by the possibility that aggres- sion might develop in some depressed patients regardless of the nature of their therapy.
Reduced 5-HT metabolism has been implicated in aggressive b e h a ~ i o u r . ~ ~ An association between fluoxetine and hostile behaviour may therefore be biologically plausible. However, early clinical trials do not report the development of aggressive behav- iour among fluoxetine recipients. The CSM has received 25 reports of aggressive reactions with fluoxetine (1.7% of total reports) and six with flu- voxamine (0.5%). The small difference appears to be due to stimulation of reporting by adverse publi- city: over the first 2 years of marketing, and prior to the media publicity which commenced at the end of 1990, the reporting rate to CSM in numbers of reports per million prescriptions written was 2 1 for fluoxetine and 20 for fluvoxamine. These figures do not suggest a greater tendency for fluoxetine to be associated with such behaviour than fluvoxa- mine. In half of the reported aggressive reactions to fluoxetine for whom further information was supplied there was a history of aggressive or crimi- nal behaviour, or alcohol or drug abuse. As in the case of reports of suicidal behaviour, these reports have been more likely to arise in patients with a high risk.
The association between abnormal 5-HT regula- tion and aggression has also led to the suggestion that fluoxetine might reduce hostile behaviour in some patients. Three uncontrolled studies of patients with antisocial behaviour showed that in some 'high-risk' patients, aggressive behaviour was not aggravated by fluoxetine therapy, but actually improved.33 3s These observations tend to counter the reports of aggression in some depressed patients taking fluoxetine, but no controlled studies of the association between fluoxetine administration and hostile behaviour have yet been published.
NEUROLOGICAL TOXICITY
The ability of fluoxetine to exacerbate an underly- ing epileptogenic potential is recognized and in this respect it is similar to other antidepressants of all types including fluvoxamine. Among the reports in Table 1 are 42 reports of seizures in patients taking fluoxetine (3.1% of all adverse reactions reported) and 32 in patients taking fluvoxamine (2.9%).
Analysis of the individual reports reveals that all except two patients who developed a seizure while taking fluoxetine had a past history of epi- lepsy, were on concomitant drugs known to be epi- leptogenic, or had significant pathology which could lower the seizure threshold. It seems likely that fluoxetine has a low potential to induce epi- lepsy de now.
CARDIOVASCULAR REACTIONS
One of the important advantages claimed for the 5-HT reuptake inhibitors is lack of cardiovascular toxicity, which is particularly relevant to the elderly population, and to the potential for successful sui- cide by overdose. However recent evidence suggests a role for 5-HT in coronary artery spasm.36 so car- diovascular reactions might be anticipated with a drug which inhibits neuronal5-HT reuptake.
Fluoxetine does not alter the pressor response to noradrenaline or tyramine over short or long periods in normal volunteer^.^ The early clinical
did not reveal cardiotoxicity or hypoten- sion even in the elderly,37 and analyses of ECGs and cardiac function in patients receiving fluoxe- tine did not provide evidence of cardiac dis- o r d e r ~ . ~ ~ , ~ ~ In comparative trials fluoxetine compared favourably with the tricyclic antidepres- sants which have well-established cardiovascular toxi~i ty .~" Some adverse reactions reported as non- serious can be markets of more sinister reactions, for example dizziness due to heart block, but the early trials showed such reactions also occurred less often with fluoxetine than control drugs. How- ever. the results of these clinical trials of limited size and highly selected patients do not exclude the possibility that toxicity would become apparent when fluoxetine was used more widely and in patients with underlying cardiovascular disease. Indeed, cardiovascular toxicity was reported rarely in these trials, even among the patients taking con-

FLUOXETINE: COMPARISON WITH FLUVOXAMINE 115
trol antidepressants, representing the problem of selection bias.
There have been isolated case reports of arrhyth- mias occurring in association with f l~oxet ine.~ ' 44
Severe reactions have not been reported in the liter- ature.
Among the adverse reactions reported to the CSM shown in the table are 44 reports of suspected cardiovascular reactions to fluoxetine and 29 to fluvoxamine. Most suspected reactions were not serious. However there were 15 cardiovascular reactions with fatal outcome with fluoxetine and four with fluvoxamine during the first 30 months from launch of each product, rates of 52 and 28 per million prescriptions respectively. The apparent difference is probably not real. During the same time the overall rates of reports with a fatal out- come from all causes were 71 and 96 per million prescriptions, respectively. Furthermore, of the 15 who died of a cardiovascular cause during fluoxe- tine treatment, only one patient was not elderly or suffered from underlying cardiovascular patho- logy. Spontaneous reporting data do not suggest that fluoxetine exhibits significant cardiovascular toxicity in patients without underlying pathology, and there is no good evidence that it contributes to a fatal outcome in patients with cardiovascular disease.
OTHER ADVERSE REACTIONS
A reversible syndrome of inappropriate ADH secretion has been reported in publication^'^^^'^^^ and through the UK spontaneous adverse reaction reporting scheme, and this appears to be a rare adverse reaction to fluoxetine.
Isolated reports of alopecia have appeared in the and six cases have been reported to
CSM. The neuroleptic malignant syndrome has been reported in the l i terat~re ,~ ' and to the CSM in a patient who had received fluoxetine in addition to various phenothiazines and haloperidol. There have been case reports of movement disorders in patients taking fluoxetine,'y.50 53 which may be due to an inhibitory effect of 5-HT on dopaminergic neurotransniission in the striato-nigral pathways. Sexual dysfunction has been reported in the litera- t ~ r e . " , ' ~ A single case of glaucoma with apparent temporal relationshi to fluoxetine administration has been published.' Causal relationships of these more unusual reactions have not been established.
P
CONCLUSIONS
Those working in drug development strive to intro- duce agents that are not only as effective but also safer than the older antidepressants. The main advantages are beneficial effects on patient com- pliance, and for patients who suffer other diseases as well as depression, or who intentionally over- dose. The toxicity of fluoxetine as representative of the new class of antidepressants, the selective serotonin reuptake inhibitors (SSRIs), is therefore of interest.
To date, the overall reaction profile of fluoxetine is similar to that of fluvoxamine, although fluoxe- tine is more likely to be associated with adverse dermatological reactions, while gastrointestinal reactions are more likely to occur with fluvoxa- mine. It is premature to reach any conclusions on their comparative safety with other classes of anti- depressants.
Concerns remain over the possible association between fluoxetine and suicidal behaviour and aggression. It seems likely that fluoxetine is not causally related to either suicidal or aggressive behaviour, though information on high-risk patients is lacking.
There is insufficient information to examine criti- cally the nature and frequency of the adverse effects of other 5-HT reuptake blockers which have recently been marketed or which are at an early stage of development. The different pharmacody- namic and pharmacokinetic characteristics of these products may result in different safety profiles, or in advantages for their use in particular patient sub- groups.
REFERENCES
1. Awad, A. G. New antidepressants - the serotonin reuptake inhibitors. Psychiatr. J . Univ. Otr. 1987; 12: 31-34.
2. Benfield, P., Heel, R . C. and Lewis, S. P. Fluoxetine: a review of its pharmacodynamic and pharmacokine- tic properties, and therapeutic efficacy in depressive illness. Drugs 1986; 32: 481-508.
3. Reynolds, J . E. F. Fluvoxamine maleate. In Martin- dale: The Extra Pharmacopoea, 29th edition. Phar- maceutical Press, London, 1989, p. 362.
4. Lemberger, L., Bergstrom, R . F., Wolen, R . L., Farid, N. A., Enas, G. G. and Aronoff, G. R. Fluoxe- tine: clinical pharmacology and physiologic disposi- tion. J. Clin. Psychiatry 1985; 46(3): 14-19.
5. Pato, M. T., Murphy, D. L. and DeVane, C. L. Sus- tained plasma concentrations of fluoxetine and/or
0 1992 by John Wiley & Sons, Ltd. PHARMACOEPIDEMIOLOGY A N D DRUG SAFETY, VOL. 1: 11 1-1 17 (1992)
116 J . PRICE E T A L
norfluoxetine four and eight weeks after fluoxetine discontinuation. J. Clin. Psychopharrnucol. 1991; 11: 224-225.
6. Benfield, P. and Ward, A. Fluvoxamine: a review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in depressive ill- ness. Drugs 1986; 32: 3 13-334.
7. Wernicke, J. F. The side effect profile and safety of fluoxetine. J. Clin. Psychiatry 1985; 46: 59-67.
8. Cooper, G. L. The safety of fluoxetine - an update. Br. J. Psychiatry 1988; 153 (Suppl. 3): 77-86.
9. Muijen, M., Roy, D., Silverstone, T., Mehmet, A. and Christie, M. A comparative clinical trial of fluoxetine, mianserin and placebo in depressed out- patients. Acta Psychiatr. Scand. 1988; 78: 384390.
10. Altamura, A. C., Percudani, M., Guercetti, G. and Invernizzi, G. Efficacy and tolerability of fluoxetine in the elderly: a double-blind study versus amitripty- line. Int. Clin. Psychopharrnacol. 1989; 4 (Suppl 2):
1 I . Feighner, J . P. and Cohn, J. B. Double-blind com- parative trials of fluoxetine and doxepin in geriatric patients with major depressive disorder. J. Clin. P.sy- chiarry 1985; 46: 20-25.
12. Chouinard, G. A double-blind controlled clinical trial of fluoxetine and amitriptyline in the treatment of outpatients with major depressive disorder. J . Clin. Psychiutry 1985; 46: 32-37.
13. Bremner, J. D. Fluoxetine in depressed patients: a comparison with imipramine. J. Clin. Psychiutry 1984; 45: 414419.
14. Cohn, M. D. and Wilcox, C. A comparison offluoxe- tine, imipramine and placebo in patients with major depressive disorder. J. Clin. Psychiatry 1985; 46: 26- 31.
15. Feighner, J. P. A comparative trial of fluoxetine and amitriptyline in patients with major depressive dis- order. J. Clin. Psychiatry 1985; 46: 369-372.
16. Hall, J. Fluoxetine: efficacy against placebo and by does - an overview. Br. J . Psychiurry 1988; 153 (Suppl. 3): 59-63.
17. Altamura, A. C . , Montgomery, S. A. and Wernicke, J. F. Br. J. Psychialry 1988; 153 (Suppl. 3): 109-1 12. The evidence for 20 mg a day of fluoxetine as the optimal dose in the treatment of depression.
18. Inman, W. Antidepressants and anxiolytics. PEM News 199 1 ; 7: 36-39.
19. Levinson, M. L., Lipsky, R. J. and Fuller, D. K. Adverse effects and drug interactions associated with fluoxetine therapy. DICP, The Amah of Pharrnu- cotherapy 1991; 25: 657-661.
20. Teicher, M. H., Glod, C. and Cole, J . 0 . Emergence of intense suicidal preoccupation during fluoxetine treatment. Am. J. Psychiatry 1990; 147: 207-210.
21. Masand, P., Gupta, S. and Dewan, M. Suicidal idea- tion related to fluoxetine. N . Engl. J. Med. 1991; 324: 420.
22. Dasguptd, R. Additional cases of suicidal ideation
103-106.
0 1992 by John Wiley & Sons, Ltd. PHARMAC
association with fluoxetine. Am. J . Psychiatry 1990; 147: 1570.
23. Hoover, C. E. Additional cases of suicidal ideation associated with fluoxetine. Am. J. Psycl?iutry 1990; 147: 1571.
24. Hoover, C. E. Suicidal ideation not associated with fluoxetine. Am. J . Psychiatry 199 1 ; 148: 543.
25. Montgomery, D. B., Baldwin, D., Green, M., Bul- lock, T. and Montgomery, S. A. Pharmacotherapy in the prevention of suicidal behaviour. Abstract, presented at the World Congress of Biological Psy- chiatry, Florence. 1991.
26. Oswald, I., Brazinova, V., and Dunleavy, D. L. F. On the slowness of action of tricyclic antidepressant drugs. Br. J . P.sychiutry 1972; 120: 673-677.
27. Soloff, P. H., George, A., Netran, R. S., Schultz, P. M., and Perel, J. M. Paradoxical efrects ofamitrip- tyline on borderline patients. Am. J. P.~ychiutry 1986; 143: 1603- 1605.
28. Damluji, N. F. and Ferguson, J. M. Paradoxical wor- sening ofdepressive symptomatology caused by anti- depressants. J. Clin. Psychophermacol 1988; 8: 347- 349.
29. Inman, W. ‘Prozac’ on trial by TV. PEM News 1991; 7: 39-40.
30. Fava, M. and Rosenbaum, J . F. Suicidality and fluoxetine: is there a relationship? New Research Abstract 475, American Psychiatric Association meeting, New York, 1990.
31. Beasley, C. M., Dornseif, B. E., Bosomworth, J. C., Sayler, M. E., Rampey, A. H., Heiligstein, J. H., Thompson, V. L., Murphy, D. J. and Masica, D. N. Fluoxetine and suicide: a meta-analysis of con- trolled trials of treatment for depression. Br. &fed,
32. Van Praag, H. M. Serotonergic dysfunction and aggression control. Psychol. Med. 1991; 21: 15--19.
33. Norden, M. J. Fluoxetine in borderline personality disorder. Prog. Neuropsychophurinurol. B id . Psy- chiatry 1989; 13: 885-893.
34. Cornelius, J. R. , Soloff, P. H., Perel, J. M. and Ulrich, R. F. A preliminary trial of fluoxetine in refractory borderline patients. J. Clin. Psychophar- rnacol. 1991; 11: 116-120.
35. Coccaro, E. F., Astill, J. L., Herbert, J. L. and Schut, A. G. Fluoxetine treatment of impulsive aggression in DSM-111-R personality disorder patients. J. Clin. Psychopharrnucol. 1990; 10: 373-375.
36. Hillis, L. D. and Lange, R. A. Serotonin and acute ischaemic heart disease. N . Engl. J . Med. 1991; 324: 688-690.
37. Falk, W. E., Rosenbaum, J . F., Otto, M. W., Zusky, P. M., Weilburg, J. B. and Nixon, R. A. Fluoxetine versus trazodone in depressed geriatric patients. J . Geriatr. Psychiatry Neurol. 1991; 2: 208-214.
38. Fisch, C. Effect of fluoxetine on the electrocardio- gram. J. Clin. Psychiatry 1985; 46: 4 2 4 4 .
39. Upward, J. W., Edwards, J. G., Goldie, A., and
J . 199 1 ; 303: 685-692.
:OEPIDEMIOLOGY AND DRUG SAFETY, VOL. 1: I 1 1-1 17 (1992)

FLUOXETINE COMPARISON WITH FLUVOXAMINE 117
Waller D. G. Comparative effects of fluoxetine and amitriptyline on cardiac function. Br. J . C h . Phur- mucol. 1988; 26: 399--402.
40. Halper, J. P. and Mann, J. .I. Cardiovascular effects of antidepressant medications. BY. J . Pxychiutry 19x8; 153 (Suppl 3), 87-98.
41. Gardner, S. F., Rutherford, W. F., Munger, M . A,, and Panacek, E. A. Drug-induced supraventricular
case report of fluoxetine. Ann. Emrrg. Med. 1991; 20: 19&197.
42. Buff, D. D., Brenner, R., Kirtane, S. S. and Gilboa, R . Dysrhythinia associated with fluoxetine treatment
elderly patient with cardiac disease. J. Clin. iutrj, 1991; 52: 174176.
43. Feder, R. Bradycardia and syncope induced by fluoxetine. J. Clir~. Psjdiiutry 1991; 52: 139.
44. Ellison, J . H., Milofsky, J. E., Ely, E. Fluoxetine- induced bradycardia and syncope in two patients.
45. Marik, P. E., van Heerden, W. and Steenkamp, V. Fluoxetine-induced syndrome of inappropriate anti- diuretic hormone excretion. s. Aj?. Med. J . 1990; 78: 760-761.
46. Staab, J . P, Yerkes, S. A,, Cheney, E. M. and Clayton A. H. Transient SIADH associated with fluoxetine. Am. J. P.syc/iiutry 1990; 147: 1569-1570.
J. c / in PSJ’ClliUtrJ’ 1990; 51: 385-386.
47. Jenike, M. A. Severe hair loss associated with fluoxe- tine use. Am. J . Psychiutry 1991; 148: 392.
48. Gupta, S. and Major, L.’F. Hair loss associated with fluoxetine. Br. J. Psychiatry 199 I ; 159: 737-738.
49. Halman, M. and Goldbloom, D. S. Fluoxetine and neuroleptic malignant syndrome. Biol Psj*chiutry
50. Tate, J . L. Extrapyramidal symptoms in a patient taking haloperidol and fluoxetine. Am. J. Psychiatry 1989; 146: 399400.
51. Bouchard. R. H., Pourcher, E. and Vincent, P. Fluoxetine and extrapyramidal side effects. Am. J. Psychiurry 1989; 146: 1352-1353.
52. Brod, T. M. Fluoxetine and extrapyramidal side effects. Am. J. Psychiatry 1989; 146: 1353.
53. Baldwin, D., Fineberg, N. and Montgomery, S. Fluoxetine, fluvoxamine and extrapyramidal tract disorders. Int . Clin. Psychopharmacol. 191; 6: 51-58.
54. Zajecka, J . , Fawcett, J . , Schaff, M., JeKriess, H . and Guy, C. The role of serotonin in sexual dysfunction: fluoxetine-associated orgasm dysfunction. J. Clin. Psychiutry 1991; 52: 66-68.
55. Ahmad, S. Fluoxetine and glaucoma. DZCP, The Annuls ofPhurmucothrrapy 1991; 25: 436.
( 1 990); 28: 5 18-52 1 .
0 1992 by John Wiley & Sons, Ltd. PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 1: 11 1-1 17 (1992)