safety and secondary pharmacology, uk
TRANSCRIPT

Safety Pharmacology Society 12th Annual Meeting
Combined Safety Pharmacology and Toxicology Studies
Functional cardiovascular, CNS and respiratory endpoints in repeat-dose
toxicity studies: advantages and pitfalls
Will Redfern, PhD Safety Assessment UK
Alderley Park Cheshire
United Kingdom
October 04, 2012 Phoenix, Arizona


Aileen McHarg, PhD Cardiovascular Safety Pharmacologist
Syntex (Edinburgh) and Pfizer (Sandwich and La Jolla) SPS stalwart Bon viveur
1961-2011
Dedicated to a former colleague


Disclaimer
The views expressed are no longer affected by jet lag, but may be subject to hangover.
• Drivers: Scientific and Regulatory • Advantages and pitfalls • Examples for each of the 3 organ functions • Summary
Overview

• Drivers: Scientific and Regulatory • Advantages and pitfalls • Examples for each of the 3 organ functions • Summary
Overview

Doing it in addition to standalone safety
pharmacology studies
Scientific drivers Doing it instead of standalone safety
pharmacology studies
Regulatory drivers
Rationale: •To provide early warning flags well ahead of the regulatory GLP SP core battery studies (by incorporating into early tox/MTD studies). •To assess whether findings in acute SP studies persist, intensify, or diminish after repeated dosing, and to demonstrate recovery after cessation of dosing. •To provide functional correlates of histopathological findings in previous tox studies. •To assess potential effects that may only develop after prolonged exposure.
Rationale: To opt for the minimum regulatory requirement for FTIM: ICHS6 (Biologics) ICHS9 (Oncology Products) FDA Guidance on Exploratory IND Studies by incorporating SP core battery assessments into the 1-month regulatory tox studies.
Functional measurements in repeat-dose toxicity studies
I’m OK with this. Let’s have more of it!
I have reservations about this.

Scientific drivers

Neglect of function and obsession with structure in toxicity testing
G. Zbinden
Institute of Toxicology, University of Zurich, Switzerland
Proceedings of 9th International Congress of Pharmacology Vol 1, pp. 43-49. New York: Macmillan Press, 1984
The title says it all…
28 years later, this is still the case!

Attrition due to inadequate safety – why?
11
Shortcoming Impact Solution? 1. Lack of early detection of safety signals
‘Doomed’ compounds enter in vivo tox phase
Improve frontloaded screening: in silico and in vitro
2. Lack of detection of safety hazards preclinically
‘Doomed’ compounds enter clinical development
Improve quality and increase information content of safety pharmacology and toxicology studies
3. Lack of confidence/knowledge/ precision in preclinical-clinical translation
Defective risk assessment: ‘Doomed’ compounds may be let through, anticipating a large safety margin; ‘safe’ compounds may be stopped, anticipating an inadequate safety margin.
Improve risk assessment and decision-making by better understanding of the translation of the preclinical signals to humans.
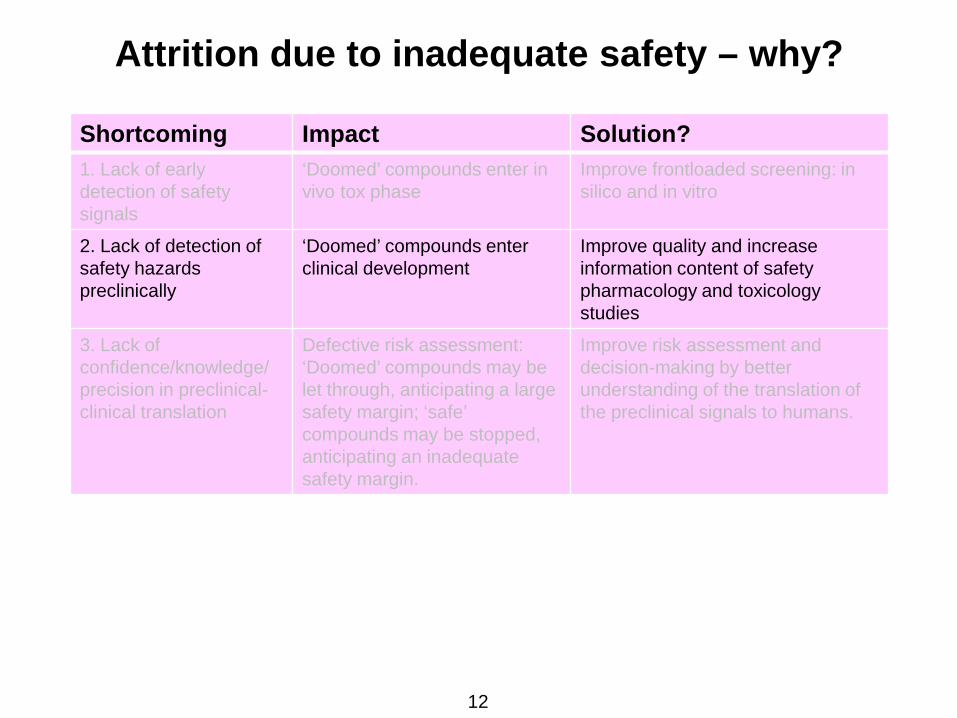
Attrition due to inadequate safety – why?
12
Shortcoming Impact Solution? 1. Lack of early detection of safety signals
‘Doomed’ compounds enter in vivo tox phase
Improve frontloaded screening: in silico and in vitro
2. Lack of detection of safety hazards preclinically
‘Doomed’ compounds enter clinical development
Improve quality and increase information content of safety pharmacology and toxicology studies
3. Lack of confidence/knowledge/ precision in preclinical-clinical translation
Defective risk assessment: ‘Doomed’ compounds may be let through, anticipating a large safety margin; ‘safe’ compounds may be stopped, anticipating an inadequate safety margin.
Improve risk assessment and decision-making by better understanding of the translation of the preclinical signals to humans.

Increase in attrition rate in Phase I from 1990-2004
F Pammolli et al. (2011) Nature Reviews Drug Discovery 10: 428-438.
Most Phase I stops are likely to be safety-related

Kola & Landis (2004)
Kola & Landis (2004)
Arrowsmith (2011)
Kola & Landis (2004) Nature Reviews: Drug Discovery 3: 711-715. Arrowsmith J (2011) Nature Reviews: Drug Discovery 10: 87; 328-329.
Values are contribution of safety as % of total attrition

Impact of adverse effects of drugs by organ function throughout the pharmaceutical life cycle
Phase ‘Nonclinical’ Phase I Phase I-III Phase III/ Marketing
Post-Marketing
Post-Marketing
Information: Causes of attrition
Serious ADRs Causes of attrition
ADRs on label Serious ADRs Withdrawal from sale
Source: Car (2006) Sibille et al. (1998)
Olson et al. (2000)
BioPrint® (2006) Budnitz et al. (2006)
Stevens & Baker (2008)
Sample size: 88 CDs stopped 1,015 subjects 82 CDs stopped 1,138 drugs 21,298 patients 47 drugs
Cardiovascular: 27% 9% 21% 36% 15% 45% Hepatotoxicity: 8% 7% 21% 13% 0% 32%
Haematology/BM: 7% 2% 4% 16% 10% 9% Nervous system: 14% 28% 21% 67% 39% 2%
Immunotox; photosensitivity: 7% 16% 11% 25% 34% 2% Gastrointestinal: 3% 23% 5% 67% 14% 2%
Reprotox: 13% 0% 1% 10% 0% 2% Musculoskeletal: 4% 0% 1% 28% 3% 2%
Respiratory: 2% 0% 0% 32% 8% 2% Renal: 2% 0% 9% 19% 2% 0%
Genetic tox: 5% 0% 0% 0% 0% 0% Carcinogenicity: 3% 0% 0% 1% 0% 0%
Other: 0% 0% 4% 16% 2% 2%
Adapted from Redfern WS et al. SOT 2010
1-9% 10-19% >20% 0%
The various toxicity domains have been ranked first by contribution to products withdrawn from sale, then by attrition during clinical development.
Impact of adverse effects of drugs by organ function throughout the pharmaceutical life cycle

Impact of adverse effects of drugs by organ function throughout the pharmaceutical life cycle
Phase ‘Nonclinical’ Phase I Phase I-III Phase III/ Marketing
Post-Marketing
Post-Marketing
Information: Causes of attrition
Serious ADRs Causes of attrition
ADRs on label Serious ADRs Withdrawal from sale
Source: Car (2006) Sibille et al. (1998)
Olson et al. (2000)
BioPrint® (2006) Budnitz et al. (2006)
Stevens & Baker (2008)
Sample size: 88 CDs stopped 1,015 subjects 82 CDs stopped 1,138 drugs 21,298 patients 47 drugs
Cardiovascular: 27% 9% 21% 36% 15% 45% Hepatotoxicity: 8% 7% 21% 13% 0% 32%
Haematology/BM: 7% 2% 4% 16% 10% 9% Nervous system: 14% 28% 21% 67% 39% 2%
Immunotox; photosensitivity: 7% 16% 11% 25% 34% 2% Gastrointestinal: 3% 23% 5% 67% 14% 2%
Reprotox: 13% 0% 1% 10% 0% 2% Musculoskeletal: 4% 0% 1% 28% 3% 2%
Respiratory: 2% 0% 0% 32% 8% 2% Renal: 2% 0% 9% 19% 2% 0%
Genetic tox: 5% 0% 0% 0% 0% 0% Carcinogenicity: 3% 0% 0% 1% 0% 0%
Other: 0% 0% 4% 16% 2% 2%
Adapted from Redfern WS et al. SOT 2011
1-9% 10-19% >20% 0%
The various toxicity domains have been ranked first by contribution to products withdrawn from sale, then by attrition during clinical development.
Impact of adverse effects of drugs by organ function throughout the pharmaceutical life cycle
No change in 10 years! Increased contribution from Nervous System
AEs in 2010
2010 Update:

As it’s now October, here’s the impact of functional adverse effects on drug development –
during any typical October* (2010 in this case)!
Source: DIA Daily October 2010
Company Drug Therapeutic indication
Functional adverse effect
Outcome
Boehringer Fibanserin Female hypoactive sexual desire disorder
Depression, anxiety, fatigue Development abandoned
Abbott Meridia (sibutramine) Obesity Increased risk of heart attack & stroke
Withdrawn from market (US)
Alexza Adusuve Staccato (loxapine - inhalation)
Agitation during schizophrenia/bipolar
disorder
Respiratory (impaired expiration) Non-approval (US)
Amylin Bydureon Type II diabetes QT risk FDA requested TQT study (after reviewing
NDA)
Various GnRH agonists Prostate cancer Metabolic syndrome leading to MI, stroke Labelling (US)
Roche/Abbott Saquinavir-ritonavir (in combination) HIV QT prolongation,
torsade de pointes Labelling (US)
Vivus Qnexa (phentermine/topiramate) Obesity
Tachycardia, suicidal ideation, impaired
memory & concentration (also birth defects;
kidney stones)
Non-approval (US)
*Any typical October

As it’s now October, here’s the impact of functional adverse effects on drug development –
during any typical October* (2010 in this case)!
Source: DIA Daily October 2010
Company Drug Therapeutic indication
Functional adverse effect
Outcome
Boehringer Fibanserin Female hypoactive sexual desire disorder
Depression, anxiety, fatigue Development abandoned
Abbott Meridia (sibutramine) Obesity Increased risk of heart attack & stroke
Withdrawn from market (US)
Alexza Adusuve Staccato (loxapine - inhalation)
Agitation during schizophrenia/bipolar
disorder
Respiratory (impaired expiration) Non-approval (US)
Amylin Bydureon Type II diabetes QT risk FDA requested TQT study (after reviewing
NDA)
Various GnRH agonists Prostate cancer Metabolic syndrome leading to MI, stroke Labelling (US)
Roche/Abbott Saquinavir-ritonavir (in combination) HIV QT prolongation,
torsade de pointes Labelling (US)
Vivus Qnexa (phentermine/topiramate) Obesity
Tachycardia, suicidal ideation, impaired
memory & concentration (also birth defects;
kidney stones)
Non-approval (US)
*in Phoenix
At this rate, we will lose another candidate drug while we’re at the SPS Meeting...

...not quite, just a ‘bad news story’ from yesterday:
Still a couple of days to go...

Could more inclusion of functional measurements in toxicology studies help to reduce this?
Even marginally?
By contributing to ‘the aggregation of marginal gains’?
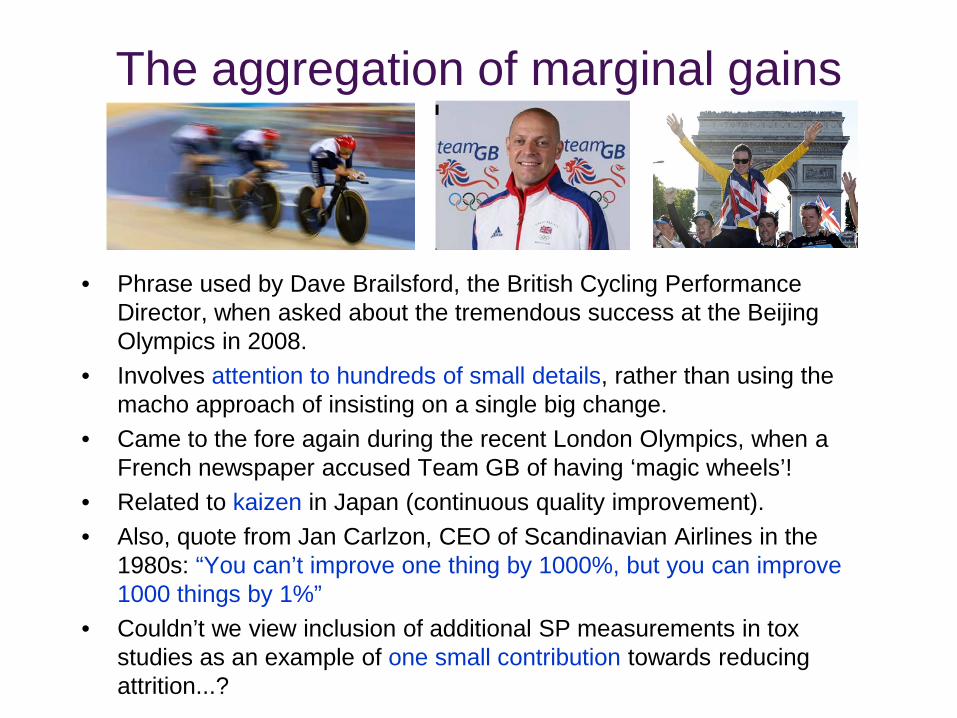
The aggregation of marginal gains
• Phrase used by Dave Brailsford, the British Cycling Performance Director, when asked about the tremendous success at the Beijing Olympics in 2008.
• Involves attention to hundreds of small details, rather than using the macho approach of insisting on a single big change.
• Came to the fore again during the recent London Olympics, when a French newspaper accused Team GB of having ‘magic wheels’!
• Related to kaizen in Japan (continuous quality improvement). • Also, quote from Jan Carlzon, CEO of Scandinavian Airlines in the
1980s: “You can’t improve one thing by 1000%, but you can improve 1000 things by 1%”
• Couldn’t we view inclusion of additional SP measurements in tox studies as an example of one small contribution towards reducing attrition...?

Regulatory drivers
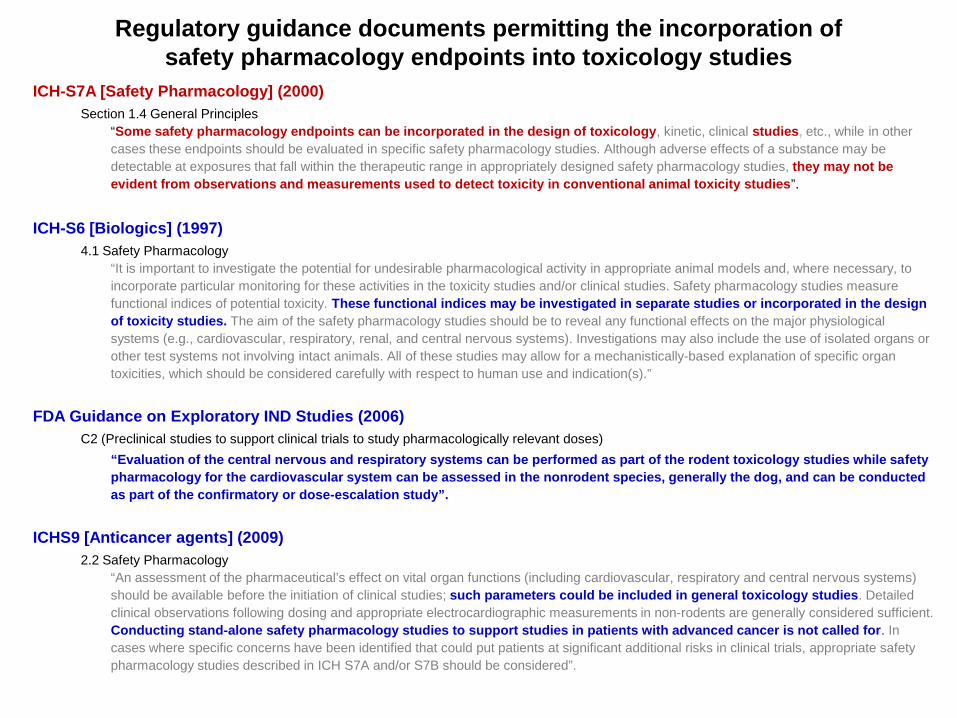
ICH-S7A [Safety Pharmacology] (2000) Section 1.4 General Principles
“Some safety pharmacology endpoints can be incorporated in the design of toxicology, kinetic, clinical studies, etc., while in other cases these endpoints should be evaluated in specific safety pharmacology studies. Although adverse effects of a substance may be detectable at exposures that fall within the therapeutic range in appropriately designed safety pharmacology studies, they may not be evident from observations and measurements used to detect toxicity in conventional animal toxicity studies”.
ICH-S6 [Biologics] (1997) 4.1 Safety Pharmacology
“It is important to investigate the potential for undesirable pharmacological activity in appropriate animal models and, where necessary, to incorporate particular monitoring for these activities in the toxicity studies and/or clinical studies. Safety pharmacology studies measure functional indices of potential toxicity. These functional indices may be investigated in separate studies or incorporated in the design of toxicity studies. The aim of the safety pharmacology studies should be to reveal any functional effects on the major physiological systems (e.g., cardiovascular, respiratory, renal, and central nervous systems). Investigations may also include the use of isolated organs or other test systems not involving intact animals. All of these studies may allow for a mechanistically-based explanation of specific organ toxicities, which should be considered carefully with respect to human use and indication(s).”
FDA Guidance on Exploratory IND Studies (2006) C2 (Preclinical studies to support clinical trials to study pharmacologically relevant doses) “Evaluation of the central nervous and respiratory systems can be performed as part of the rodent toxicology studies while safety
pharmacology for the cardiovascular system can be assessed in the nonrodent species, generally the dog, and can be conducted as part of the confirmatory or dose-escalation study”.
ICHS9 [Anticancer agents] (2009) 2.2 Safety Pharmacology
“An assessment of the pharmaceutical’s effect on vital organ functions (including cardiovascular, respiratory and central nervous systems) should be available before the initiation of clinical studies; such parameters could be included in general toxicology studies. Detailed clinical observations following dosing and appropriate electrocardiographic measurements in non-rodents are generally considered sufficient. Conducting stand-alone safety pharmacology studies to support studies in patients with advanced cancer is not called for. In cases where specific concerns have been identified that could put patients at significant additional risks in clinical trials, appropriate safety pharmacology studies described in ICH S7A and/or S7B should be considered”.
Regulatory guidance documents permitting the incorporation of safety pharmacology endpoints into toxicology studies

• Drivers: Scientific and Regulatory • Advantages and pitfalls • Examples for each of the 3 organ functions • Summary
Overview

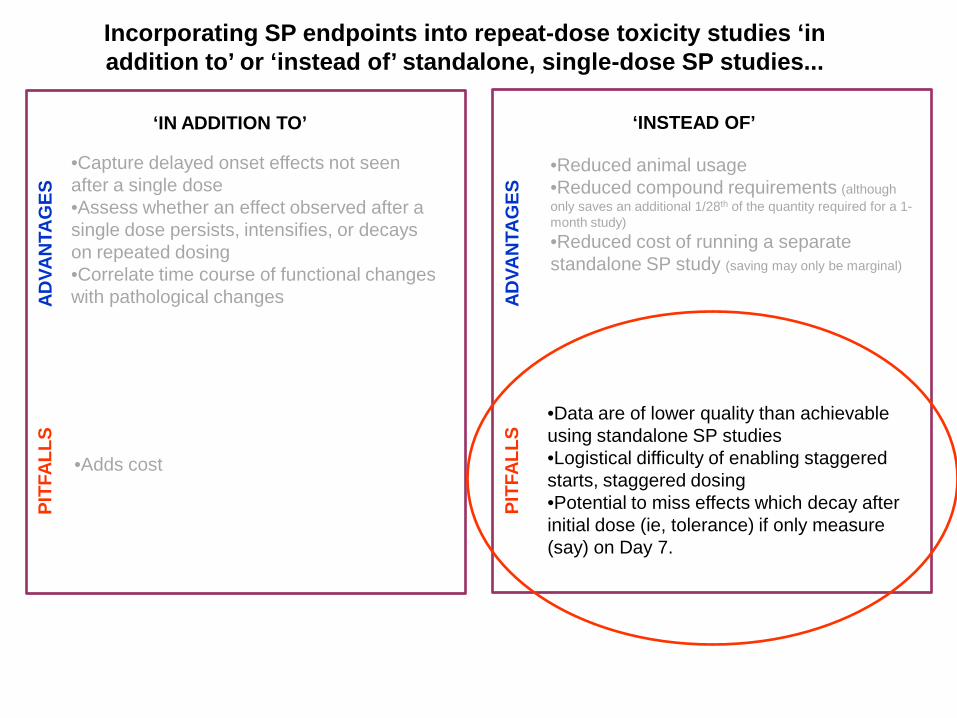
•Capture delayed onset effects not seen after a single dose •Assess whether an effect observed after a single dose persists, intensifies, or decays on repeated dosing •Correlate time course of functional changes with pathological changes
•Reduced animal usage •Reduced compound requirements (although only saves an additional 1/28th of the quantity required for a 1-month study) •Reduced cost of running a separate standalone SP study (saving may only be marginal)
‘IN ADDITION TO’ ‘INSTEAD OF’
•Adds cost
•Data are of lower quality than achievable using standalone SP studies •Logistical difficulty of enabling staggered starts, staggered dosing •Potential to miss effects which decay after initial dose (ie, tolerance) if only measure (say) on Day 7.
ADVA
NTA
GES
PI
TFAL
LS
Incorporating SP endpoints into repeat-dose toxicity studies ‘in addition to’ or ‘instead of’ standalone, single-dose SP studies...
ADVA
NTA
GES
PI
TFAL
LS
•Capture delayed onset effects not seen after a single dose •Assess whether an effect observed after a single dose persists, intensifies, or decays on repeated dosing •Correlate time course of functional changes with pathological changes
•Reduced animal usage •Reduced compound requirements (although only saves an additional 1/28th of the quantity required for a 1-month study) •Reduced cost of running a separate standalone SP study (saving may only be marginal)
‘IN ADDITION TO’ ‘INSTEAD OF’
•Adds cost
•Data are of lower quality than achievable using standalone SP studies •Logistical difficulty of enabling staggered starts, staggered dosing •Potential to miss effects which decay after initial dose (ie, tolerance) if only measure (say) on Day 7.
ADVA
NTA
GES
PI
TFAL
LS
Incorporating SP endpoints into repeat-dose toxicity studies ‘in addition to’ or ‘instead of’ standalone, single-dose SP studies...
ADVA
NTA
GES
PI
TFAL
LS

Safety pharmacology studies General toxicology studies Dosing staggered to accommodate functional measurements
Animals dosed all in one session (usually a.m.)
TK sample taken after key functional measurements
TK sampling takes priority
No necropsy to consider Scheduled to accommodate necropsy slots
Studies powered to detect the functional effect Studies adequate to detect histopathological effects
Behavioural studies usually require young rats Sexually mature animals used
Usually restricted to male animals Equal numbers of both sexes used
May require non-standard strains (e.g. pigmented rats)
Restricted to standard strains
Functional measurements may require pre-training of animals
Rarely required
Functional measurements require a quiet room Sometimes anything but!
Equipment/software may not be fully GLP-compliant
GLP sacrosanct
Should be run by experienced safety pharmacologists and technicians fully au fait with safety pharmacology measurements and data interpretation
Toxicology facilities may be geographically remote from available safety pharmacology expertise, or such expertise may not be available within the company.
Differences in in-life environments (etc.)

Example of a custom-designed, fit-for-purpose rodent safety pharmacology suite
Features: •Testing labs located remote from corridor noise (e.g., trundling of cage racks; loud conversations). •Primary access to suite via single entry door, with warning to limit entry to essential visits and to minimise noise level. •Staff requiring access to the other animals on the study can do so without disturbing the safety pharmacology observations/measurements. •Entry to the testing labs restricted to staff involved in the observations/measurements. •Designed to accommodate bulky test equipment, ergonomically. •Lighting control with local (manual) override.
Functional measurements
done here...
...and here

Example of rodent toxicology study holding rooms with ante room
Drawbacks (for CNS safety pharmacology observations/measurements): •Testing area adjacent to corridor noise (e.g., trundling of cage racks; loud conversations). •Access from corridor directly into testing area. •Staff requiring access to the other animals on the study disturb the safety pharmacology observations/measurements. •Entry to the testing area unrestricted. •Bulky test equipment may be difficult to accommodate ergonomically. •Automated lighting control with no manual override.
Functional measurements
done here

Statistical power Toxicology studies in non-rodents are generally underpowered relative to stand-alone safety pharmacology studies (although this is not always the case).
For example, sensitivity of detection of changes in QT interval using conventional (manual) ECG in dog tox studies is lower than in telemetered dog safety pharmacology studies:
Hammond TG et al. (2001) Cardiovasc Res 49: 741-750. Tattersall ML et al. (2006) J Pharmacol Toxicol Methods 53: 11-19

Have you thought through the logistics…?
If you choose to go down this route (replacing the standalone safety pharmacology study), it is preferable to conduct functional measurements on Day 1 of the repeat-dose toxicity studies for the reasons outlined earlier (ie, you may miss an acute response that diminishes with repeat-dosing). But Day 1 of a tox study is usually mayhem, with timed TK bleeds etc. So, you could do the measurements on Day 2 of the repeat-dose study. However, you may struggle to get through all the Irwin tests (multiple time points) and whole-body plethysmography (WBP) measurements (4 hours’ recordings) on the vehicle and 3 dose levels (Irwin: 24 rats; WBP: 32 rats) in one day. So you could do (say) the Irwin tests on Day 2 and the WBP measurements on Day 3. Even then, you still may struggle to complete these evaluations in a single day. So you may have to stagger the start of the rodent 1-month study, e.g.: MON TUE WED THU Day 1 Start cohort 1 Day 2 cohort 1: Irwin Day 3 cohort 1: WBP Day 4 cohort 1 Day 1 Start cohort 2 Day 2 cohort 2: Irwin Day 3 cohort 2: WBP And you may have to reduce the standard number of time points in the Irwin test. Do you have enough quiet space to run Irwin and WBP simultaneously, close to the tox holding room…?
Good luck!

Drug Therapeutic target
Effects
Opiate analgesics Pain Rapid tolerance to most effects develops on repeat-dosing
Baclofen Spasticity Tolerance develops to muscle relaxant effects due to down-regulation of GABA-B receptors
Benzodiazepines Anxiety Tolerance develops to initial sedative effect
L-DOPA; bromocriptine Parkinson’s Reduced efficacy
SSRI’s Depression Reduced efficacy
Haloperidol; chlorpromazine
Schizophrenia Reduced efficacy
Anticonvulsants Epilepsy Reduced efficacy
Nitrates Hypertension Reduced efficacy
Beta-blockers Hypertension Reduced efficacy
DECREASE in response/clinical efficacy with repeat-dosing
Drug Therapeutic target Effects
Amiodarone Class III antiarrhythmic Requires several days’ administration before clinical efficacy (incl. QT prolongation) is achieved.
Antidepressants Depression Require ~2 weeks before clinical efficacy is achieved.
Clonidine Hypertension Initial hypertensive response followed by hypotension, losing the initial hypertensive response on repeat-dosing.
INCREASE in response/clinical efficacy with repeat-dosing
• Neuropathy (e.g. paclitaxel); • Cardiomyopathy (e.g. doxorubicin); • Retinopathy (e.g. quinine).
SLOW/DELAYED development of adverse effect
Changes in response with repeat-dosing
‘‘Some form of adaptive syndrome is the inevitable consequence of the reciprocal interaction between most or all classes of drugs and the organism’’. W Haefely (1986)

Example of both directions (and no change) in the same study with the same compound!
Day 1 Day 2 Day 3 Effect Abnormal respiration
6/6 3/6 2/6 Diminishing
Decreased activity
6/6 6/6 6/6 Stable
Increased scratching
0/6 0/6 3/6 Delayed onset
Effects of once-daily dosing with baclofen (10 mg/kg po) in the Irwin test in rats (3M; 3F)
Conclusion: Change in magnitude of effect over repeated dosing is both pharmacology- and parameter-specific
Data courtesy of Lorna Ewart

•Capture delayed onset effects not seen after a single dose •Assess whether an effect observed after a single dose persists, intensifies, or decays on repeated dosing •Correlate time course of functional changes with pathological changes
•Reduced animal usage •Reduced compound requirements (although only saves an additional 1/28th of the quantity required for a 1-month study) •Reduced cost of running a separate standalone SP study (saving may only be marginal)
‘IN ADDITION TO’ ‘INSTEAD OF’
•Adds cost
•Data are of lower quality than achievable using standalone SP studies •Logistical difficulty of enabling staggered starts, staggered dosing •Potential to miss effects which decay after initial dose (ie, tolerance) if only measure (say) on Day 7.
ADVA
NTA
GES
PI
TFAL
LS
Incorporating SP endpoints into repeat-dose toxicity studies ‘in addition to’ or ‘instead of’ standalone, single-dose SP studies...
ADVA
NTA
GES
PI
TFAL
LS
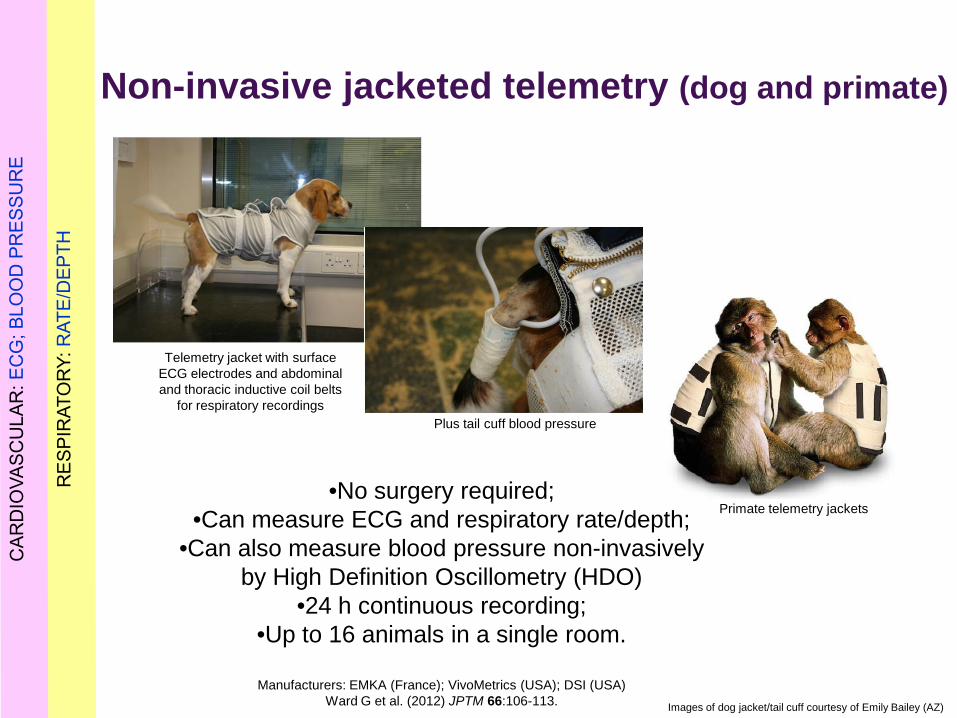
•No surgery required; •Can measure ECG and respiratory rate/depth;
•Can also measure blood pressure non-invasively by High Definition Oscillometry (HDO)
•24 h continuous recording; •Up to 16 animals in a single room.
Manufacturers: EMKA (France); VivoMetrics (USA); DSI (USA)
Ward G et al. (2012) JPTM 66:106-113.
Telemetry jacket with surface ECG electrodes and abdominal and thoracic inductive coil belts
for respiratory recordings Plus tail cuff blood pressure
Primate telemetry jackets
Images of dog jacket/tail cuff courtesy of Emily Bailey (AZ)
Non-invasive jacketed telemetry (dog and primate)

CVS endpoint (Lead II ECG from jacket) included in dog tox studies Data quality comparable to “gold standard” invasive telemetry*
“Follow-up” studies: ECG (incl. QT) in vivo
*Prior H et al. (2009) Non-invasive telemetric electrocardiogram assessment in conscious beagle dogs. J Pharmacol Toxicol Methods 60: 167-173.

Does jacketed ECG telemetry improve data quality?
Lower resting heart rate than ‘snapshot’ ECG; QTcV equivalent
Does jacketed ECG telemetry require more time resource (manhours)?
Requires less time resource than repeated snapshots
Data: Pierre Lainée
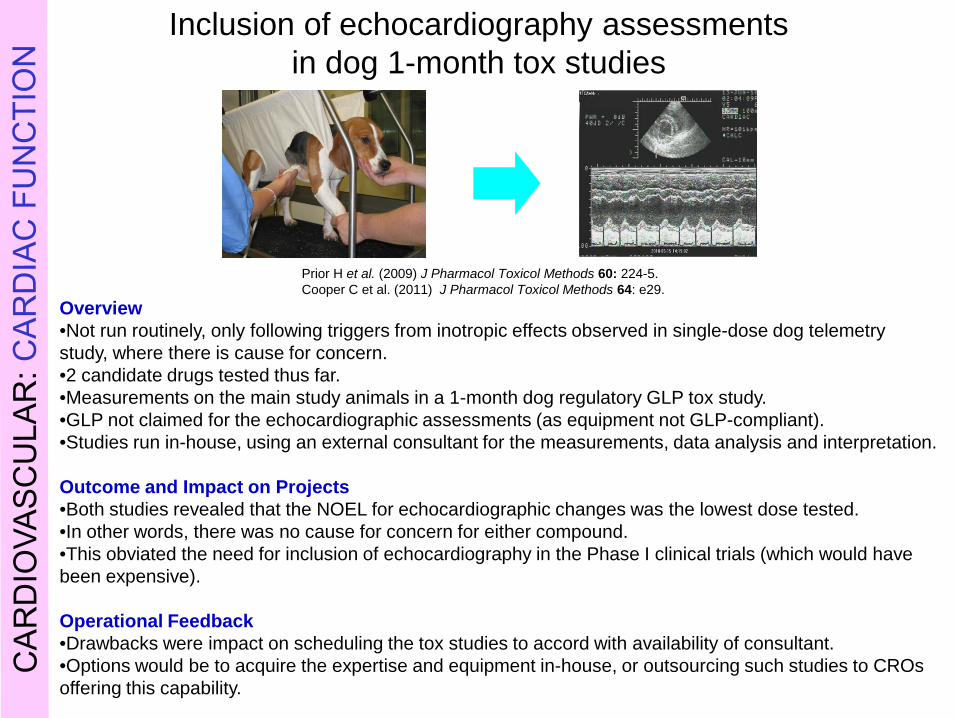
Inclusion of echocardiography assessments in dog 1-month tox studies
Overview •Not run routinely, only following triggers from inotropic effects observed in single-dose dog telemetry study, where there is cause for concern. •2 candidate drugs tested thus far. •Measurements on the main study animals in a 1-month dog regulatory GLP tox study. •GLP not claimed for the echocardiographic assessments (as equipment not GLP-compliant). •Studies run in-house, using an external consultant for the measurements, data analysis and interpretation. Outcome and Impact on Projects •Both studies revealed that the NOEL for echocardiographic changes was the lowest dose tested. •In other words, there was no cause for concern for either compound. •This obviated the need for inclusion of echocardiography in the Phase I clinical trials (which would have been expensive). Operational Feedback •Drawbacks were impact on scheduling the tox studies to accord with availability of consultant. •Options would be to acquire the expertise and equipment in-house, or outsourcing such studies to CROs offering this capability.
Prior H et al. (2009) J Pharmacol Toxicol Methods 60: 224-5. Cooper C et al. (2011) J Pharmacol Toxicol Methods 64: e29.

Individual videotracking of group-housed monkeys
Rose C et al. (2012) Quantified tracking and monitoring of diazepam treated socially housed cynomolgus monkeys. Regulatory Toxicology & Pharmacology 62:292-301.
Also note that jacketed telemetry systems for dogs and monkeys are fitted with an inbuilt accelerometer for registering movement/activity
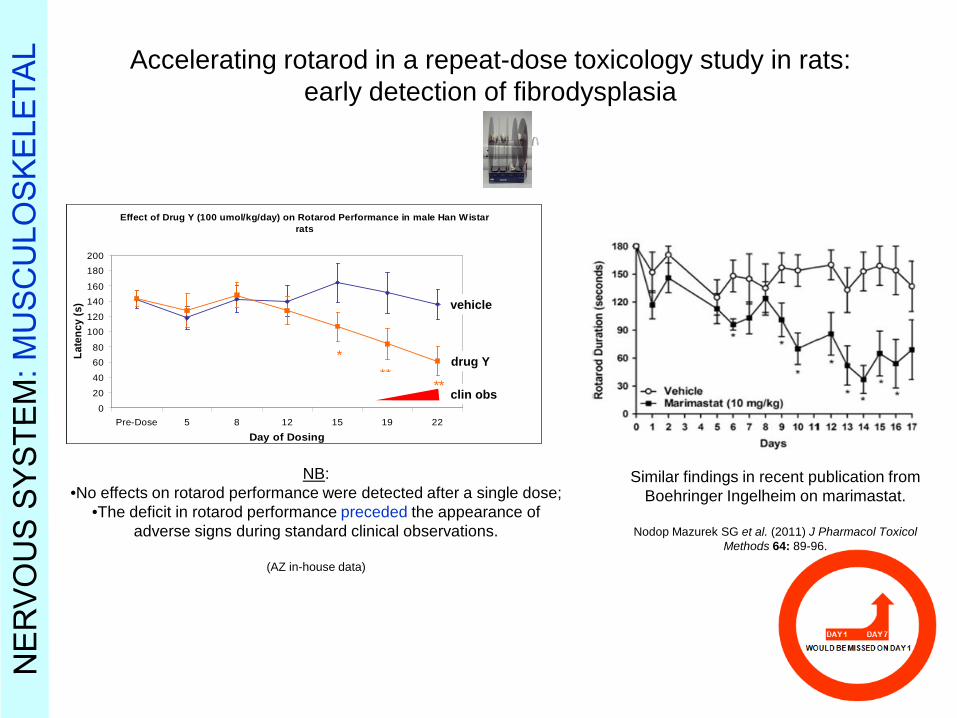
Accelerating rotarod in a repeat-dose toxicology study in rats: early detection of fibrodysplasia
NB: •No effects on rotarod performance were detected after a single dose;
•The deficit in rotarod performance preceded the appearance of adverse signs during standard clinical observations.
(AZ in-house data)
Effect of Drug Y (100 umol/kg/day) on Rotarod Performance in male Han Wistar rats
0
20
40
6080
100120
140160
180200
Pre-Dose 5 8 12 15 19 22
Day of Dosing
Late
ncy
(s)
***
**
vehicle
drug Y
clin obs
Effect of Drug Y (100 umol/kg/day) on Rotarod Performance in male Han Wistar rats
0
20
40
6080
100120
140160
180200
Pre-Dose 5 8 12 15 19 22
Day of Dosing
Late
ncy
(s)
***
**
vehicle
drug Y
clin obs
Similar findings in recent publication from Boehringer Ingelheim on marimastat.
Nodop Mazurek SG et al. (2011) J Pharmacol Toxicol
Methods 64: 89-96.

Pupillary light reflex in a repeat-dose toxicology study in rats: detection of mydriasis
0.0
0.5
1.0
1.5
2.0
2.5
Pupil
diam
eter
(mm
)
**
******
****
***
Day 8pre
Day 74 h
Day 4pre
Day 34 h
Day 1 4 h
Day 2pre
Day -1
Vehicle AZD400 AZD500 AZD750 AZD1500
(slow)
(slow) (slow) (slow)
Drug X µmol/kg po
(n = 6 each)
Redfern WS et al. (2007) A simple method for estimating pupil diameter in conscious rats and dogs during repeat-dose toxicity studies. J Pharmacol Toxicol Methods 56: e50.
(No further dosing at high dose level)

Pupillary light reflex in a repeat-dose toxicology study in rats: detection of mydriasis
0.0
0.5
1.0
1.5
2.0
2.5
Pupil
diam
eter
(mm
)
**
******
****
***
Day 8pre
Day 74 h
Day 4pre
Day 34 h
Day 1 4 h
Day 2pre
Day -1
Vehicle AZD400 AZD500 AZD750 AZD1500
(slow)
(slow) (slow) (slow)
Drug X µmol/kg po
(n = 6 each)
Redfern WS et al. (2007) A simple method for estimating pupil diameter in conscious rats and dogs during repeat-dose toxicity studies. J Pharmacol Toxicol Methods 56: e50.
(No further dosing at high dose level)

Saliva production in dogs: detection of initial increase, diminishing with repeat-dosing
7 14 21 280.0
0.1
0.2
0.3
0.4
0.5Sa
liva
weig
ht (g
)
Day of dosing
vehicle (n = 12) high dose (n = 12)
**Salivation quantified by placing a pre-weighed gauze swab inside a jowl for 20 s; removed and re-weighed.
(NS)

Saliva production in dogs: detection of initial increase, diminishing with repeat-dosing
7 14 21 280.0
0.1
0.2
0.3
0.4
0.5Sa
liva
weig
ht (g
)
Day of dosing
vehicle (n = 12) high dose (n = 12)
**Salivation quantified by placing a pre-weighed gauze swab inside a jowl for 20 s; removed and re-weighed.

0 7 14 21 28 35 420
20
40
60
80
100
*****
**
**
visual acuityperipheral retinal damage%
max
imal
dam
age
or d
efici
t
Time post-dose (days)
central retinal damage
*
First time point is 2 h after iv administration of sodium iodate (50 mg/kg) in male Han Wistar rats; n = 6 per time point. *P<0.05, **P<0.01, between central and peripheral retinal damage.
Visual acuity deficit after a single dose of sodium iodate (50 mg/kg iv) in Han Wistar rats followed up to 6 weeks: comparison of functional
and histopathological outcomes
Redfern WS et al. (2011) Evaluation of a convenient method of assessing rodent visual function in safety pharmacology studies: Effects of sodium iodate on visual acuity and retinal morphology in albino and pigmented rats and mice. J Pharmacol Toxicol Methods 63: 102-114.

Respiratory parameters in rats recorded over 28 days using whole-body plethysmography
-2 2 6 8 15 17 20 240
100
200
300
** *** *** ** **
Day
Res
pira
tory
Rat
e (b
pm)
Importance of ‘settling time’ in chamber prior to recordings:
red: 5 minutes blue: 15 minutes.
Ewart L et al. (2008) SOT Meeting Abstracts.
In fact, we would now put the rats in for 45 min, recording only for the last 15 min (ie, 30 min settling time).
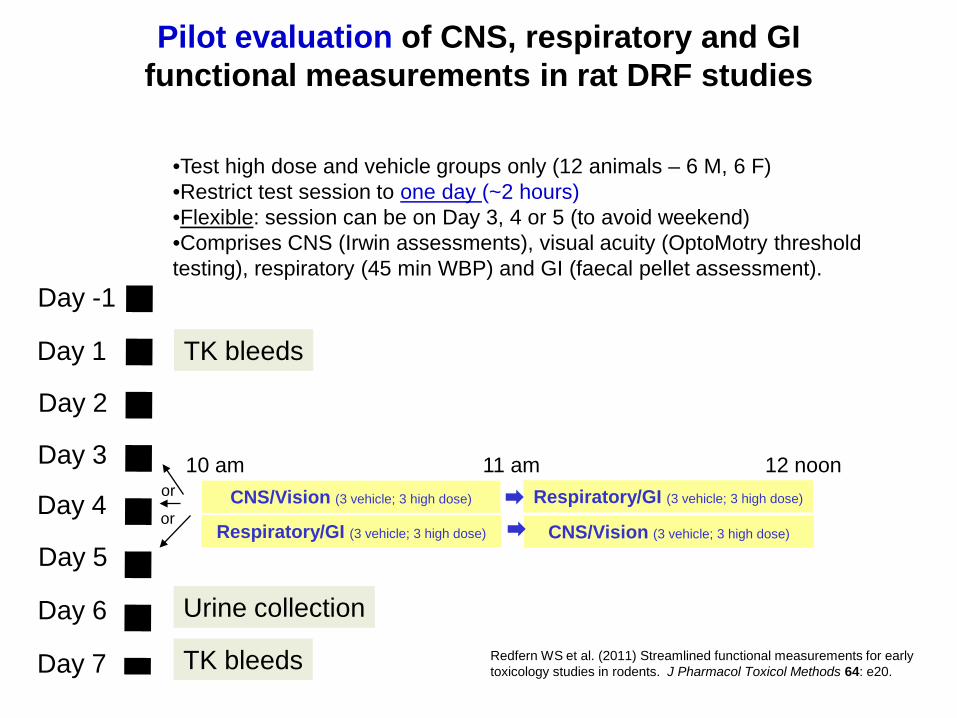
Day -1
Day 1
Day 2
Day 3
Day 4
Day 5
Day 6
Day 7
TK bleeds
TK bleeds
Urine collection
CNS/Vision (3 vehicle; 3 high dose) Respiratory/GI (3 vehicle; 3 high dose)
•Test high dose and vehicle groups only (12 animals – 6 M, 6 F) •Restrict test session to one day (~2 hours) •Flexible: session can be on Day 3, 4 or 5 (to avoid weekend) •Comprises CNS (Irwin assessments), visual acuity (OptoMotry threshold testing), respiratory (45 min WBP) and GI (faecal pellet assessment).
or
or
Pilot evaluation of CNS, respiratory and GI functional measurements in rat DRF studies
CNS/Vision (3 vehicle; 3 high dose) Respiratory/GI (3 vehicle; 3 high dose)
10 am 11 am 12 noon
Redfern WS et al. (2011) Streamlined functional measurements for early toxicology studies in rodents. J Pharmacol Toxicol Methods 64: e20.
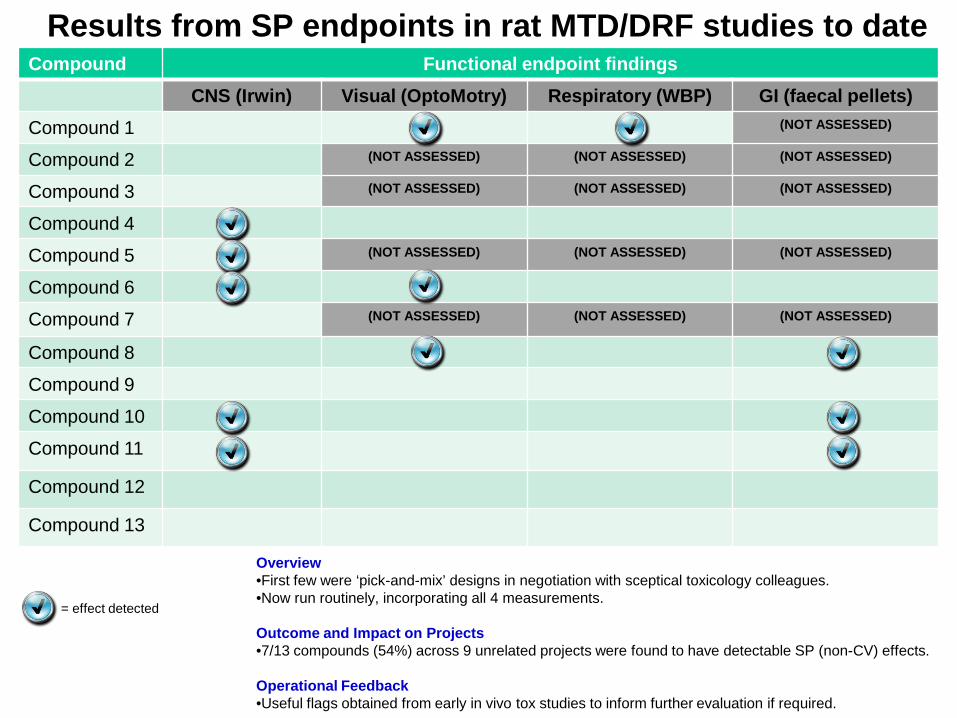
Compound Functional endpoint findings CNS (Irwin) Visual (OptoMotry) Respiratory (WBP) GI (faecal pellets)
Compound 1 (NOT ASSESSED)
Compound 2 (NOT ASSESSED) (NOT ASSESSED) (NOT ASSESSED)
Compound 3 (NOT ASSESSED) (NOT ASSESSED) (NOT ASSESSED)
Compound 4
Compound 5 (NOT ASSESSED) (NOT ASSESSED) (NOT ASSESSED)
Compound 6
Compound 7 (NOT ASSESSED) (NOT ASSESSED) (NOT ASSESSED)
Compound 8
Compound 9
Compound 10
Compound 11
Compound 12
Compound 13
Results from SP endpoints in rat MTD/DRF studies to date
Overview •First few were ‘pick-and-mix’ designs in negotiation with sceptical toxicology colleagues. •Now run routinely, incorporating all 4 measurements.
Outcome and Impact on Projects •7/13 compounds (54%) across 9 unrelated projects were found to have detectable SP (non-CV) effects. Operational Feedback •Useful flags obtained from early in vivo tox studies to inform further evaluation if required.
= effect detected
• Drivers: Scientific and Regulatory • Advantages and pitfalls • Examples for each of the 3 organ functions • Summary
Overview

Summary Ask yourself this question. You know the translation from safety pharmacology data to Phase I clinical outcomes isn’t as good as you’d like to think it is. So, do you: (a) degrade the data quality even further, or (b) try to augment it?
Acknowledgements
Colleagues in Safety Pharmacology, General Toxicology Sciences,
and Laboratory Animal Sciences at AstraZeneca Alderley Park:
Lorna Ewart; Sally Robinson; Mark Pinches; Sharon Storey; Helen Prior; Claire Grant; Jackie Moors; Karen Philp, Jason Schofield; Matt Skinner; Louise Marks; Emily Bailey; Kat Greenwood; Claire Barnard; Lisa Williams; Dave Simpson; Liz
Fantham; Des Cobey; Liz Martin; Claire Sadler; Charles Humfrey; Wendy Davies; Ian Slater; Mark Anderton; Ruth Roberts; Jean-Pierre Valentin
Colleagues formerly at AstraZeneca Alderley Park:
Ian Wakefield; Nick McMahon; Isobel Strang; Pierre Lainée; Karen Tse; Qasim Hussain; Khine-Phu Maung; Andrea Tait; Graham Vickery; Charlotte Cooper; Emily
Bailey; Victoria Motyer.