safety and efficacy of fsh drugs in art for polycystic ovarian disease m. aboulghar cairo, egypt
TRANSCRIPT

Safety and efficacy of FSH drugs in ART for
polycystic ovarian disease
M. AboulgharCairo, Egypt

Safety of FSH

Urinary and recombinant gonadotrophins are being used for many
years with 100% safety record concerning
transmission of infection and with no serious
allergic reaction.
The only risk of the use of both types of FSH is
the development of OHSS. This is not
uncommon complication in PCO patients as those patients are particularly
liable to OHSS.

Ovarian stimulation for PCOS patients is associated with complications.
Under- and over-stimulation are relatively common (Urman 2004).

Polycystic ovaries and OHSS: a systematic
review (Tummon et al 2005) 10 studies were included with PCOS
and available data on OHSS. Combined OR for OHSS was 6.8 (CI
4.9 – 9.6) There is a significant consistent
relation between PCOS and OHSS.

How can we prevent OHSS in PCOS?
Smaller dose of FSH Close monitoring. Coasting Use of GnRH antagonist as a
protocol of stimulation or to prevent OHSS in hyperstimulated patients.
Small dose of hCG 5000 IU.

Efficacy of FSH in ART for PCOS

Outcome IVF in PCO and controls matched for age, cause of
infertility and stimulation protocol (MacDougall et al 1993)
PCO Non PCO PN 76 76 NSFSH Smaller
doseHigher dose
S
E2 Higher Lower SOocytes More Less SFR Less More SPR 25.4% 23% NSOHSS 10.5% Zero S
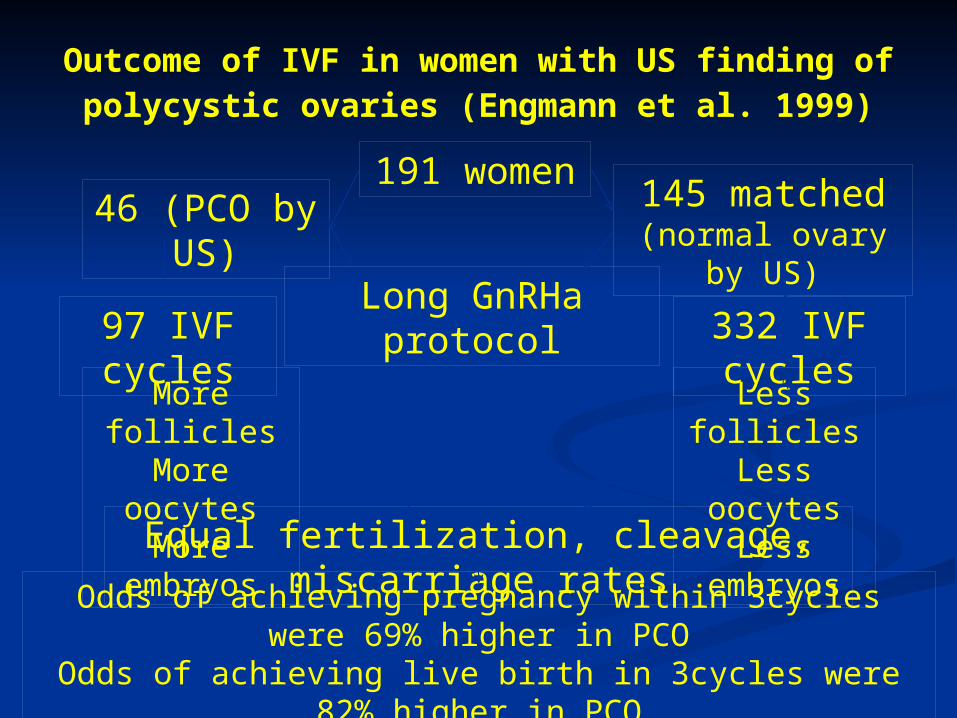
Outcome of IVF in women with US finding of polycystic ovaries (Engmann et al. 1999)
191 women46 (PCO by
US)
145 matched (normal ovary by
US)Long GnRHa
protocol97 IVF cycles
332 IVF cycles
More folliclesMore
oocytesMore
embryos
Less follicles
Less oocytes
Less embryos
Equal fertilization, cleavage, miscarriage ratesOdds of achieving pregnancy within 3cycles were 69%
higher in PCOOdds of achieving live birth in 3cycles were 82%
higher in PCO

During simple ovulation induction for PCOS
patients, hMG, urinary FSH, and recombinant FSH appear to be equal in achieving pregnancy (Van Wely et al 2003)

A meta-analysis of outcomes of IVF in PCOS and a matched non PCOS group (Heijnen 2006)
458 PCOS patients (From 9
studies)Rotterdam criteria
694 non PCOS patients.
Significantly more oocytes retrieved in PCOS (OR = 3.4, 95%
CI = 1.7 – 5.1)
793cycles 1116 cycles
No significant difference between mean number of
fertilized oocytesNo significant difference in PR (OR = 1.0 95% CI = 0.8 – 1.3)OHSS was rarely reported.

Oocyte quality in patients with severe ovarian hyperstimulation syndrome.
(Aboulghar et al 1997; Fabregues 2004)
Significantly more oocytes Significantly lower FR Similar number and quality of
available embryos Similar implantation and pregnancy
rates.
We will present the results of the first prospective randomized study in the world literature
comparing highly purified FSH with recombinant FSH for
IVF/ICSI in PCOS patients. (Aboulghar et al Fertil Steril, in
press).

Declaration of conflict of interest
This randomized study was sponsored in part by IBSA Institute Biochimique SA
Study design:
A prospective randomized study of IVF/ICSI for patients with PCOS comparing recombinant FSH (Gonal F, Merk-Serono) and highly purified urinary FSH (Fostimon, IBSA).
A sample size of 42 women in each arm is sufficient to detect a difference of 10% in oocyte maturity to ensure a power of 80% based on the oocyte maturity in our study (Aboulghar et al. 1997).
Protocol of treatment We used our routine long GnRHa protocol
(Aboulghar et al.2008) Start dose of FSH was 2-3 ampoules
depending on age and weight of patient, from day 6 of stimulation, adjustment could be done.
Frequency of E2 assays depended on the number of follicles, and the rate of growth.
Triggering ovulation when follicle reaches 18 mm (according to our routine protocol). (Aboulghar et al.2008)

In case of risk of OHSS, coasting was performed
according to our coasting protocol (Mansour et al 2005). We stopped FSH treatment when the lead
follicle reached 15-16 mm and waited until E2 level dropped to 3000 pg/ml or less, then a dose of 10,000
hCG was given.
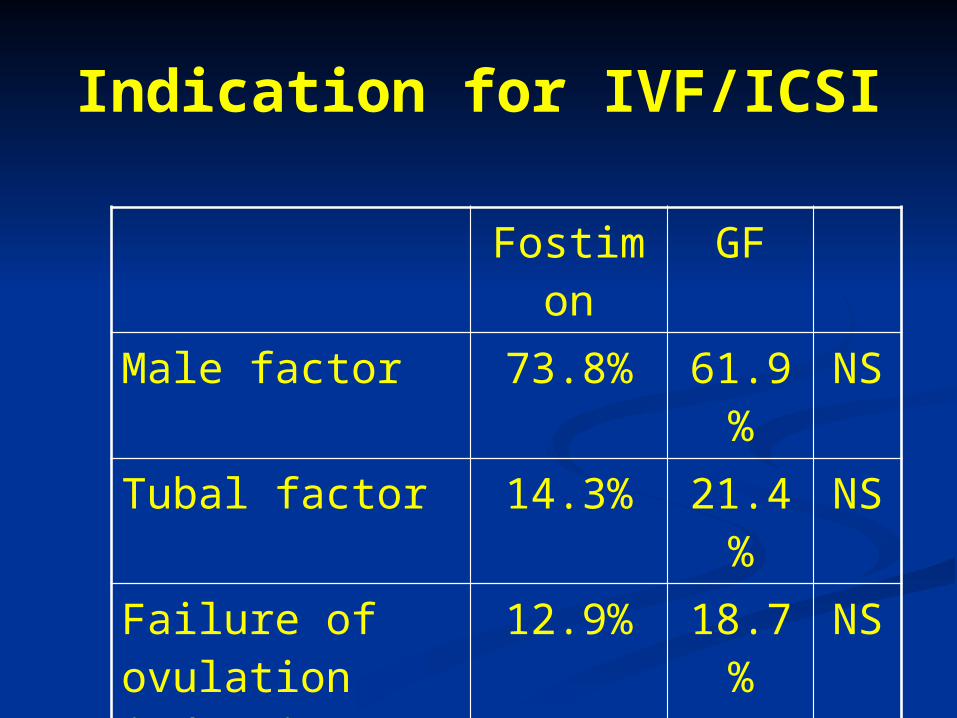
Indication for IVF/ICSI
Fostimon
GF
Male factor 73.8% 61.9%
NS
Tubal factor 14.3% 21.4%
NS
Failure of ovulation induction
12.9% 18.7%
NS

Patients’ characteristics
Fostimon GF
Age 28.29±4.04
27.36±3.50
NS
Period of infertility
5.03±3.60
5.77±3.42
NS
BMI 29.80±4.74
29.90±4.65
NS

Ovarian stimulation data
FSH dose and duration Fostimon GF p
Start FSH dose (Ampoules) 2.71±0.46 2.67±0.47 NS
Mean Total ampoules 29.98±9.17 28.29±7.95 NS
Days of stimulation 11.05±2.59 11.21±2.82 NS
Days of coasting 1.88±0.96 1.80±0.77 NS

Coasting
Done in 16 patients in fostimon Done in 20 patients in Gonal F 15 patients: one day 13 patients: two days 7 patients: three days 1 patient: four days

Fostimon GF p
Retrieved oocytes 17.1±8.66 13.83±7.07 0.064 NS
Mature Oocytes 12.8±7.78 10.45±5.69 0.106 NS
Fertilized oocytes 9.52±6.78 6.76±5.44 0.043
Fertilization rate 74.5±20.14 62.96±24.2 0.021
Top quality embryos 2.79±0.55 2.18±0.95 0.021
Good quality embryos 2.64±0.85 2.19±0.75 0.060 NS
Outcome in both groups

Fostimon GF p
Patients with frozen embryos 28 (66.7%) 14 (33.3%) 0.006
Total n of cryo embryos 207 96
No. of embryos transferred
2.88±0.55 2.80±0.51 NS
Frozen embryos per patient 4.9±6.4 2.57±4.5 0.015 *
Positive BHCG 26 (63.4%) 24 (58.5%) NS
Clinical pregnancies 21 (50%) 22 (50.2%) NS
Ongoing pregnancies 19 (45.2%) 20 (47.6%) NS
Outcome in both groups
In the current study, 84 patients of IVF/ICSI were
performed for one or more of these indications in a single large center
during the relatively short period of 8 months,
denoting that the indication for IVF/ICSI in
PCOS patients in not uncommon.

In previous studies on IVF/ICSI for PCOS(Urman et al 2004)
Small dose of FSH for fear of OHSS
High FSH dose for fear
of cancellation
High cancellation rate was reportedDue to

In the present study only 2 cycles out of 84 cycles were canceled due to poor response.
Coasting used liberally in 36 out of 84 patients (42.8%) in our study and without affecting the clinical pregnancy rate which was 50%.

Dose of FSH and BMIFostimone GF
Mean starting dose 2.71±0.5 2.67±0.5
BMI 29.8±4.8 29.9±4.6
We noted that the use of small dose of FSH in patients with high
BMI frequently result in high cancellation rate

The study reported a high clinical pregnancy rate, 21
pregnancies (50%) in Group A and 22 pregnancies
(50.23%). However, the study also reported very
high multiple pregnancies, 9 out of 22 in Group A and 11 out of 22 in Group B.

The difference in the mean fertilized oocytes, fertilization rate, top quality embryos and
number of cryopreserved embryos could possibly be explained by the
difference in the FSH isoform composition of commercial
gonadotrophin preparations. The difference although statistically significant did not reflect on the clinically important pregnancy
rate. However, FSH isoform composition is usually considered
to have negligible effect on clinical outcome (Andersen et al 2004)
On the other hand, the distribution of FSH isoforms in human-derived products may have a higher average
glycosylation as compared to the recombinant ones. Thus
the urinary product may possibly provide some
balancing to the excessive activity of granulosa cells of PCOS, which could result in
some clinical benefits (Sharron et al 2007).

During fresh cycles, the best available embryos were
selected for transfer in both groups. The significantly more cryopreserved embryos in the
urinary FSH group may possibly make a difference in the pregnancy rate between both groups after embryo transfer of frozen-thawed
embryos.

The multiple pregnancy is extremely high in the
present study and our policy of transferring between two and three embryos should be in the future restricted to a maximum of two embryos
transferred. The final solution to the problem of multiple pregnancy will be achieved by single embryo
transfer (Gelbaya et al 2009)

Our study has shown that IVF/ICSI in PCOS
patients, even with high BMI can be managed safely with minimal
occurrence of OHSS and with an excellent
pregnancy rate. Both highly purified and recombinant FSH produce similar pregnancy rates.

Conclusions
IVF/ICSI results in excellent pregnancy rate in PCOS patients.
There is a high risk of OHSS in PCOS which could be minimized by proper preventive methods.
Although highly purified FSH resulted in a significantly higher fertilization rate, higher number of fertilized oocytes and higher number of top quality and frozen embryos as compared to recombinant FSH, yet there was no difference in clinical or ongoing pregnancy rates.

This study has shown that ovarian stimulation for
IVF/ICSI in PCOS patients can result in excellent pregnancy rates and if carefully managed and precautions to prevent
OHSS are taken, the high risk of OHSS could be
avoided to a great extent.

As clinical pregnancy rate is not significantly different between both
groups, the cost of medicine may play a role
in the choice of FSH product.

The Egyptian IVF-ET Center
Clinical directors:• M. Aboulghar, M. D.• G. Serour, M. D.
- Clinical associates:• Y. Amin, M. D.• M. Sattar, M. D.• A. Ramzy, M. D.• L. Mansour, M. D.• M. Metwally, M. D.• H. Aboulghar, M. D.• M. Aboulghar, M. D.• H. Al Inany, M. D.• A. Abou-Setta, M. D.
- Andrology:• I. Fahmy, M. D.• A. El-Gindy
Scientific director & Program manager:• Ragaa Mansour, M. D., Ph. D.
- Embryology and micromanipulation• S. Mansour, M. D.• A. Kamal, M. D. • A. Mostafa, M. D.• N. Tawab, B.Sc.• G. Afifi, B.Sc.• M. Hammam, B.A.
- Cytogenetics• H. Fayek, Ph. D.• A. Abdel-Razek, M. D.• A. Amer, B.Sc.• A. Khalil, Ph. D.• A. Naser, Ph. D.• O. Kamal, B.S.• S. Mostafa
- Cryobiology and Andrology
• D. Saad, B.Sc.• Y. Demery, B.Sc.• A. Barakat, B.Sc.• M. Serour , B.Sc.• N. Salah , B.Sc.• H. Fanous , B.Sc.• A. Mohamed , B.Sc.