safe nursing and midwifery staffing policy
TRANSCRIPT
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 1
Edition No: 1 ID Number: POLCNM016
Dated: March 2014 Review Date: March 2015
Document ID: Policy Document Type: Corporate
Directorate: Nursing
Category: Nursing and Midwifery
Department(s): Nursing
Author: Chris Terrahe Assistant Chief Nurse
Sponsor: Steve Hams Chief Nurse
Policy Dissemination
Intranet Senior Sisters and Charge Nurses Matrons Heads of Nursing and Midwifery Associate Directors of Operations Executive Directors
Consultation Process
Name of Individuals Consulted
Heads of Nursing and Midwifery Matrons Head of Governance and Risk Deputy Chief Nurse Assistant Chief Nurse Critical Care Nurse Consultant Head of Operational Human Resources
Name of Specialised Committee / Group Consulted
Joint Staff Side Committee March 2014
Corporate Approval
Committee Title Nursing and Midwifery Strategy Group
Date: 26.03.2014
Committee Title Workforce Committee Date: March 2014
Document Control / History
Edition No
Reason for change
1 Replaces Dealing with Unpredictable Nursing & Midwifery Staff Shortages - POLCNM003
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 2
Document Ref No
References:
Francis Report http://www.midstaffspublicinquiry.com/
Keogh Review http://www.nhs.uk/nhsengland/bruce-keogh-review/documents/outcomes/keogh-review-final-report.pdf
Berwick Review https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/226703/Berwick_Report.pdf
Compassion in Practice http://www.england.nhs.uk/wp-content/uploads/2012/12/compassion-in-practice.pdf
National Quality Board safe staff strategy http://www.england.nhs.uk/wp-content/uploads/2013/11/nqb-how-to-guid.pdf
National Quality Board and NHS England The Hard Truth http://www.england.nhs.uk/2014/04/01/hard-truths/
Royal College of Midwives Staffing Standards in Midwifery Services www.rcm.org.uk/EasySiteWeb/GatewayLink.aspx?alId=57039
Trust Associated Documents:
Major incident Policy
Maternity, Acute staff shortage on the delivery suite
© Medway NHS Foundation Trust [2014]

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 3
Table of Contents
1 INTRODUCTION 4
2 AIM & OBJECTIVE 4
3 DEFINITION 5
4 ROLES & RESPONSIBILTIES 5
5 EQUALITY IMPACT ASSESSMENT STATEMENT 16
6 MONITORING & REVIEW 16
7 APPENDIX 1 MINIMUM AGREED STAFFING LEVELS FOR THE WARD AREAS 17
8 APPENDIX 2.1 SAFER CARE NURSING TOOLS LEVELS OF CARE AND MULTIPLIERS 18
9 APPENDIX 2.2 BIRTHRATE PLUS INCLUDING MULTIPLIERS 20
10 APPENDIX 3 SUMMARY OF ROSTERING GUIDELINES 20
11 APPENDIX 4 DIVISIONAL ACTION CARD ERROR! BOOKMARK NOT DEFINED.
12 APPENDIX 5 SITE SAFETY CRITERIA 23
13 EQUALITY IMPACT ASSESSMENT TOOL – APPENDIX 24
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 4
To be read in conjunction with any policies listed in Trust Associated Documents.
1 INTRODUCTION
1.1 In the wake of The Francis Report (2013), The Keogh Reviews (2013) and the Cavendish review (2013) there has been a raft of literature available with the focus on determining both minimum nurse staffing levels such as the Safer Nursing Care Tool (SCNT) and Skill Mix of Staff (Royal College of Nursing Guidance).
1.2 Midwifery was in essence a step ahead of Adult Nursing with the Royal College of Midwives Safer Childbirth guidelines (2007) (Birth-rate plus) determining the minimum Midwife to Women ration of 1:29
1.3 The National Quality Board (NQB) 2013 sets out clear expectations regarding the process and principles surrounding staffing decisions and responsibilities’.
1.4 There is a clear need within any organisation for defined processes around both the determination for nurse staffing numbers to meet patient needs, how these are implemented on a day by day, shift by shift bases, the processes and mitigating actions in place when staffing numbers and or skill mix does not meet patient need and the flow of information both internally and externally to provide true transparency.
1.5 Minimum staffing levels within the Trust vary from ward to ward and specialty to specialty. In 2013 there was a review of staffing across the organisation utilising both the Safer Nursing Care Tool and Dr Keith Hurst to review data to determine the required establishments for each ward
1.6 Medway NHS FT adopts both the RCN Guidance on skill mix with a 65:35 split for registered and unregistered staff and the minimum staffing ratio of 1:8 trained staff.
1.7 As part of Medway NHS FT drive toward delivering “Better Care Together” and ensuring that the right staff are in place to meet patients needs in a robust and transparent way Medway NHS FT are partnering with a local NHS Trust to have a system of external peer review of staffing utilising the SCNT / NQB and the National Institute for Health Care Excellence (NICE) guidelines once released in 2014
2 AIM & OBJECTIVE
2.1 To determine and define Medway NHS FT expected Nursing and Midwifery staffing levels to meet patient needs and deliver “Better Care Together”
2.2 To clearly define expectations around Rota management and the usage of temporary staffing.
2.3 To ensure that the patient is at the centre of nurse staffing decision making
2.4 To ensure that the safety of the patient and the quality of patient experience in maintained.
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 5
2.5 To define the process for the booking of temporary staff including agency
2.6 To determine both funded establishments required and skill mix for any given area
2.7 To define the process of escalation and action if staffing does not match determined staffing levels
2.8 To ensure that governance around nurse staffing levels and decision making is robust and transparent, defining the flow of information from ward to board
2.9 To define responsibilities’ within the escalation and governance flow
2.10 To define how Medway NHS FT will demonstrate compliance to national staffing guidance namely the National Quality Board
3 DEFINITION
3.1 Minimum Nurse and Midwifery Staffing Expectations for Ward areas to deliver safe care:
3.1.1 Appendix 1 provides a breakdown per ward of expected registered Nurse / Midwife staffing levels both on a shift-by-shift and total whole time equivalent (WTE) basis.
3.1.2 It is recognised that patient flow, cohorts and needs vary and change, therefore to ensure that nurse and midwife staffing meets the needs of the patients daily acuity and dependency scoring utilising the Safer Nursing Care Tool will be implemented across the appropriate wards and Birthrate Plus being utilised across Midwifery (Appendix 2 provides a breakdown of acuity and dependency scoring using SNCT and a summary Birthrate plus catagories)
3.1.3 As part of Medway NHS FT drive toward delivering “Better Care Together” and ensuring that the right staff are in place to meet patients needs in a robust and transparent way Medway NHS FT are partnering with a local NHS Trust to have a system of external peer review of staffing utilising the SNCT / NQB and NICE guidelines once released in 2014
3.1.4 Medway NHS FT will undertake and publish 6 monthly staffing reviews in line with the National Quality Board Hard Truths using the Safer Care Nursing Tool and yearly reviews for Midwifery utilising Birthrate Plus
4 ROLES & RESPONSIBILTIES
4.1 Nurse or Midwife Charge (NIC)
4.1.1 To ensure that the staffing for the shift and the following shift are in line with the Minimum agreed staffing criteria for the ward Review the acuity and dependency of the ward and escalate to the Senior Sister or Matron the need for increase staffing as needed

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 6
4.1.2 Escalate to the Senior Sister, Matron or Site Team Out of hours and weekends any shortfall in staffing to meet criteria or patient need.
4.1.3 In case of unplanned absence from a member of staff the NIC will escalate to the Senior Sister, Matron or Site Team out of hours and weekends
4.1.4 If staff call in sick for the next shift this needs to escalated and if required additional staff booked via NHSP
4.1.5 Complete the Site Safety Summary before 09:30 and 19:30 on a daily basis including staffing levels
4.1.6 Update staffing levels to reflect actual levels on the ward if change across the 3 shifts
4.1.7 When staffing levels fall below agreed minimum levels complete DATIX incident report
4.1.8 Escalate to Chief Nurse or a member of the corporate team if there is insufficient support through the escalation process
4.2 Senior Sister / Senior Charge Nurse / Senior Midwife
4.2.1 Complete the rota at least 6 weeks in advance of first day worked
4.2.2 Ensure as establishment allows a consistent deployment of established staff across the whole duty, there should be at least two thirds of staffing on any shift with established staff.(on a unit with 3 registered and 3 unregistered as a minimum ,2 established RNs and 2 CSW should be rostered from the established workforce)
4.2.3 Complete Rota in line with Rota Guidelines ( Appendix 3)
4.2.4 Review the acuity and dependency of the patient cohort on a daily basis with the NIC and adjust staffing to meet needs
4.2.5 Ensure completion of the daily site safety summary by 09:30 and 19:30 including the expected and actual staffing across the shifts
4.2.6 Review staffing on an ongoing basis to ensure patient need or staff absence does not impact on service delivery
4.2.7 Adjust rota to ensure continuous established staff deployment
4.2.8 Escalate to Matron or Site Team any unresolved staffing issues effecting patient care
4.2.9 Take first line actions in line with action cards ( Appendix 4) and escalate to Matron or Site team if situation remains unresolved
4.2.10 Ensure all staff absence is managed in line with policy
4.2.11 When staffing levels fall below agreed minimum levels complete DATIX incident report
4.2.12 Accountable for the efficient and effective deployment of staff in line with clinical needs

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 7
4.2.13 Escalate to Chief Nurse or a member of the corporate team if there is insufficient support through the escalation process
4.3 Matron
4.3.1 Review Rota completed by ward team to ensure established staff deployment in line with policy
4.3.2 Authorise rota to allow 6 week publish date and the use of temporary staff to achieve minimum agreed staffing levels
4.3.3 Support ward team to review acuity and dependency on a daily basis
4.3.4 Attend the site safety summary meeting ,ensure wards have completed and address poor compliance through the 1:1 process
4.3.5 Review staffing across area of responsibility to mitigate risk of staff absence and maintain minimum agreed staffing limits or support need for staffing
4.3.6 Authorise use of agency staff to meet shortfalls in maintaining safe staffing levels
4.3.7 Escalate to Head of Nursing or Head of Midwifery if staffing shortfalls are unresolved
4.3.8 Review and reallocate staffing across area of responsibility / division to ensure actions do not compromise service delivery.
4.3.9 When staffing levels fall below agreed minimum levels ensure DATIX incident report is completed
4.3.10 Accountable for the efficient and effective deployment of staff in line with clinical needs
4.3.11 Support annual review of clinical area establishments in line with acuity and dependency.
4.3.12 Escalate to Chief Nurse or a member of the corporate team if there is insufficient support through the escalation process
4.4 Head of Nursing / Head of Midwifery / Associate Chief Nurse ( Divisional)
4.4.1 Ensure that ward establishments meet patient needs
4.4.2 Attend weekly staffing / Site safety summary meeting
4.4.3 Support the Matrons and Senior Sisters in the review of daily acuity and dependency reviews
4.4.4 Ensure third line actions are taken in line with divisional action cards
4.4.5 Review and reallocate staffing across the division to ensure staffing meets minimum safe staffing levels or increase acuity

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 8
4.4.6 Ensure all staff absence is managed in line with policy
4.4.7 Authorise staff rotas to support 6 week publish timeframe and rota meets guidelines
4.4.8 Review ward variance from staffing criteria and manage through 1:1 process
4.4.9 Active member of recruitment steering group and support proactive recruitment of staff
4.4.10 Participate in twice yearly formal staffing reviews plus formal review of staffing due to service change
4.4.11 Escalate to Corporate Team unresolved staffing issues and actions taken
4.5 Assistant Chief Nurse
4.5.1 Chair the daily Site Safety Summary Meeting or allocate alternative
4.5.2 Chair Recruitment steering group
4.5.3 Chair Weekly staffing and site safety meeting with Heads of Nursing and Midwifery
4.5.4 Ensure all 1st, 2nd and 3rd line actions are taken in line with divisional action cards
4.5.5 Instigate 4th line actions ( trust wide review and reallocation of staffing ) as appropriate
4.5.6 Escalate to the Chief Nurse or Deputy any un resolved staffing issue that are compromising patient, staff or organisational safety
4.5.7 Co ordinate 6 monthly external / peer review of staffing across the organisation
4.5.8 Authorise the use of Agency staff as required
4.5.9 Provide monthly updates to board on registered nurse and registered midwife staffing levels against optimal as per staffing reviews and minimum agreed limits including a recruitment update
4.6 Chief Nurse
4.6.1 With the board holds ultimate responsibility for Nurse/ Midwife staffing levels
4.6.2 Lead Trust wide external / peer review of Nurse / Midwife staffing levels
4.6.3 Presents monthly updates to board on Nurse / Midwife staffing levels on a shift by shift basis.
4.6.4 Presents 6 monthly updates to public board describing Nurse / Midwife staffing levels on a shift by shift basis as well as overall position against expected in terms of whole time equivalent
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 9
4.6.5 Determines trust response to unresolved staffing issues and instigates level 5 actions from divisional action cards including declaring a major incident / diverting ambulances / closing beds
4.6.6 Leads discussions with CCG's re Nurse / Midwife staffing levels
4.6.7 Final authoriser for nurse staffing levels including minimum levels
4.6.8 Lead Review of ad hoc rota review to ensure established staff deployed as per service need
4.6.9 Formally agreeing establishments on a yearly basis
4.6.10 Review staffing levels and patient needs on clinical walk rounds
4.7 If staffing on the ward does not meet patient needs or minimum agreed safe levels then the shift coordination needs to escalate to the Matron in hours or Clinical Site Practitioner out of hours, weekends and bank holidays and complete a DATIX Incident Report as per local escalation flow chart.

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 10
Figure 1.0 Local Escalation Flow Chart
Nurse in charge identifies staffing or potential staffing shortage
Escalate to Matron in hours / site Practitioner OOH
Review•Skill Mix•Acuity •Dependency•Capacity•Staffing Numbers
Review duty rotacan staff be
swapped around?
Contact NHSP
Matron contacts Head of Nursing /
General Manager in hours
Review across locality .•Skill Mix•Acuity •Dependency•Capacity•Staffing NumbersAdjust staffing across locality
Review across directorate•Skill Mix•Acuity •Dependency•Capacity•Staffing NumbersAdjust staffing across directorate
Review across trust•Skill Mix•Acuity •Dependency•Capacity•Staffing NumbersAdjust Staffing across the trust
Escalate to On call manager / Corporate Team
Escalate to Execute Team
OOH
Contact NHSP
Authorise Agency
Reduce Capacity to
mitigate risk
Reduce Demand to
mitigate Risk
Shift capacity to mitigate
Risk
Actions Owner
Nursing Staff at or above minimum set levels Staffing meets patients acuity and dependency
1. Review acuity, dependency and activity and ensure patient needs can be met
2. Review Rota for the flowing shift and ensure staffing levels going forward meet patient needs
Nurse in Charge Senior Sister
Nursing Staff below minimum set criteria or does not meet patient acuity and dependency
1. Review acuity, dependency and activity can current staffing meet acuity, dependency and activity, if so reduce RAG to green
2. Escalate to Matron or Site Management out of hours 3. Review rota can staff be moved to ensure patient safety 4. Contact NHSP re support from Temp staffing 5. Review staffing, acuity dependency and activity across the cluster to
reallocate staff to ward 6. Escalate to Head of Nursing if unable to mitigate risk 7. Review Staffing across Division to reallocate staff 8. Review CNS activity to support wards 9. Authorise the use of agency staff
Nurse in Charge Senior Sister Matron / Site Team OOH Head of Nursing / General Manger / Site Team OOH
Nursing staff numbers cannot maintain patient safety All Amber actions have not mitigated the risk
1. Review staffing across the organisation and reallocate to patient need with discussion of Heads of Nursing and General Managers
2. Review and reallocate CNS’s, PDN’s and Clinical Matrons to support the ward
3. Review and divert internal patient flow to reduce demand on challenged areas
4. Reduce active bed base to maintain patient safety
Site Team Corporate Nursing Team
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 11
Shift By Shift Review 4.8 Ward Staffing Boards:
4.8.1 All wards will have a ward Nurse / Midwifery staffing board near the entrance to the ward, which clearly indicates the expected staffing levels for the ward on a shift-by-shift basis and what the skill mix should be. It will also clearly identify how many staff are on duty and the skill mix in place
4.8.2 It is the responsibility of the nurse in charge or midwife in charge to ensure that the board is updated on a shift-by-shift basis at the beginning of the shift. The Matron for the area will monitor accuracy and ensure it is reflective of the actual staff on duty and patient need.
4.8.3 Any omissions or outdated information will be addressed at the time and continued intervention will be managed through the formal 1:1 process between the senior sister and matron
4.9 Site Safety Index Matrix (SSIM)
4.9.1 To assist the organisation in managing staffing and mitigating risk across the whole of the organisation Medway NHS FT has a Site Safety Index (SSIM) in place. This system allows an overview of the whole organisation at the daily SSIM Meeting.
4.9.2 The system requires that each ward enters a RAG (Red, Amber, Green) risk status for the following dimensions, the criteria are attached in appendix 5
4.9.2.1 Staffing against template on a shift by shift basis.
4.9.2.2 Acuity (Demand on nursing time due to acute illness requiring intervention)
4.9.2.3 Dependency (Demand on nursing time to meet activities of daily living)
4.9.2.4 Patient Placement
4.9.2.5 Infection Prevention and Control
4.9.3 It is the responsibility of the nurse in charge to enter the information on the system before the 09:30 SSIM meeting and the 19:30 SSIM meeting to allow an accurate overview of the organization and to make changes to the system including staffing numbers to reflect the actual position.
4.9.4 A representative Matron from each division will attend the SSIM meeting and compare the information added to system compared to walk round and update the system with actions taken as necessary.
4.9.5 Staffing information from the SSIM will be made available to the trust and public via Qlickview and a staffing dashboard

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 12
4.10 Site Safety Index Matrix Meeting:
4.10.1 The SSIM Meeting occurs prior to the patient flow meeting Monday to Friday but will form part of the Patient flow meeting out of hours and weekends
4.10.2 Monday to Friday the SSIM will occur at 09:30 and 19:30 and be chaired by a senior nurse usually the Assistant Chief Nurse or Site Management.
4.10.3 This meeting is held in the site office
4.10.4 Expected attendees include:
4.10.4.1 Matron from each Division
4.10.4.2 Matron from Critical Care or a representative
4.10.4.3 Head of Nursing for Site management or representation
4.10.5 The meeting will review all wards on the SSIM and empower / support the movement of staff across the whole organisation to meet patient needs. Directorates will enact actions and report to the corporate team as needed. All actions will be logged on the SSIM system for monitoring and supporting information in reviews and analysis
4.10.6 Meeting will review staffing on a shift by shift basis with all actions taken to mitigate risk documented on the SSIM system and closed once action completed.
4.11 Weekly Staffing Review Meeting:
4.11.1 The weekly staffing review meeting will be held on Fridays at 09:00, the Assistant Chief Nurse or Deputy Chief Nurse will chair this meeting.
4.11.2 The meeting will be held in the staff canteen
4.11.2.1 Expected attendees will be:
4.11.2.1.5 Head of Nursing for Medicine
4.11.2.1.6 Head of Nursing for Surgery
4.11.2.1.7 Head of Midwifery
4.11.2.1.8 Head of Nursing for Paediatrics
4.11.2.1.9 Head of Nursing for Site Management
4.11.2.1.10 Lead Nurse Risk Management
4.11.3 The meeting will have a standard agenda and be action focused with actions minuted. The meetings will last 30 minutes.
4.11.4 Meeting will review Datix incidents related to staffing issues

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 13
4.11.5 Department and Directorate Actions:
4.11.5.1 As per the local escalation flow chart and RAG triggers each area will have locally agreed action cards. These set out the sequence of events against risk and RAG status with the intention of returning to (Green) business as normal within a short as possible timeframe. The action cards are included in Appendix 4 of this policy but will form part of the local business continuity plans and be available on the shared drive for reference as needed.
4.12 Temporary Staffing
4.12.1 The number of staff authorised to book agency is controlled within each division. It is the GM’s responsibility to maintain an accurate log of their Permitted Authorisers. Only the Deputy Chief Nurse or Chief Nurse can alter the list that is held with the supplier, NHSP.
4.12.2 Agencies that are not part of the GPS should not be used unless an SLA agreement is in place with the Trust. These “off framework” agencies are not subject to the same scrutiny and therefore may pose a safety/governance and financial risk to the Trust.
4.12.3 Staff currently employed by Medway FT can only work additional hours through NHSP. This will be monitored via the weekly staffing meetings and local action taken.
4.12.4 It is not expected that agency staff will be secured without involving NHSP, this should only occur in exceptional cases.
4.12.5 Should this become necessary then the following applies:
4.12.5.1 Only a permitted authoriser may contact agencies directly.
4.12.5.2 Only agencies who are on the approved GPS list can be used by permitted authorisers.
4.12.5.3 Agencies must be advised that payment rates must be in line with the approved GPS terms as a condition for engagement and payment.
4.12.5.4 NHSP will provide a monthly report to the Chief Nurse regarding agency shifts fill rate and retrospectively booked shifts ( ie. Those arranged with agencies independently and then later added to the NHSP system for payment. ) This will be cross checked with the booking party.
4.12.6 NHS Professionals (NHSP) work in partnership with Medway NHS FT to recruit and maintain a bank staffing service to manage the Trust’s flexible workforce requirements. Substantive staff and temporary workers are signed up and compliance checked through NHSP prior to working for the Trust.
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 14
4.12.7 An office is located on site during business hours Monday to Friday and a reduced service at weekends. There is a contact line for enquiries outside of these hours which is 0845 450 3364.
4.13 Escalation areas:
4.13.1 It is recognised that at times of increased demand on beds it may be necessary to open additional capacity both on existing wards or opening escalation wards in a planned and coordinated approach.
4.13.2 A Medway NHS FT Registered Nurse must be the Nurse in charge of any escalation area opened 24/7.
4.13.3 NHSP staff will be used to support both the established ward and escalation ward to ensure nurse staffing meets patient needs
4.13.4 The staffing establishment for these areas will be in line with the principles set out at the beginning of the document.
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 15
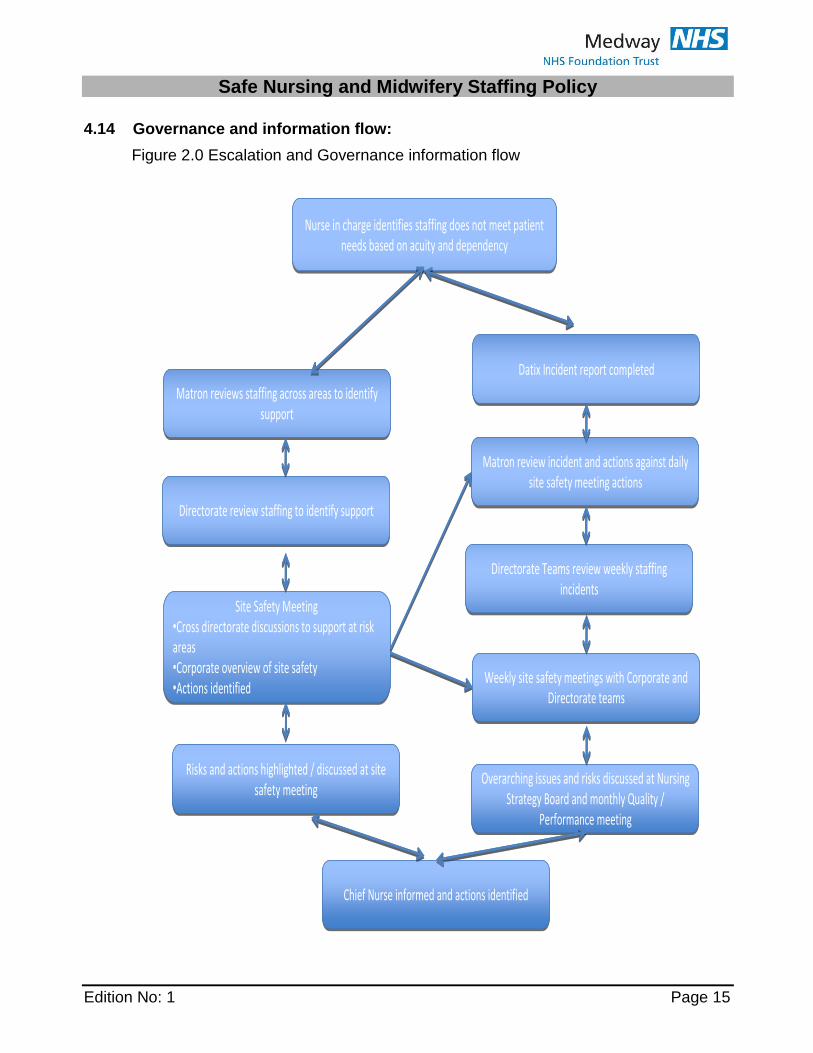
4.14 Governance and information flow:
Figure 2.0 Escalation and Governance information flow
Matron reviews staffing across areas to identify support
Matron reviews staffing across areas to identify support
Directorate review staffing to identify supportDirectorate review staffing to identify support
Nurse in charge identifies staffing does not meet patient needs based on acuity and dependency
Nurse in charge identifies staffing does not meet patient needs based on acuity and dependency
Risks and actions highlighted / discussed at site safety meeting
Risks and actions highlighted / discussed at site safety meeting
Site Safety Meeting•Cross directorate discussions to support at risk areas•Corporate overview of site safety•Actions identified
Site Safety Meeting•Cross directorate discussions to support at risk areas•Corporate overview of site safety•Actions identified
Chief Nurse informed and actions identifiedChief Nurse informed and actions identified
Datix Incident report completedDatix Incident report completed
Matron review incident and actions against daily site safety meeting actions
Matron review incident and actions against daily site safety meeting actions
Directorate Teams review weekly staffing incidents
Directorate Teams review weekly staffing incidents
Weekly site safety meetings with Corporate and Directorate teams
Weekly site safety meetings with Corporate and Directorate teams
Overarching issues and risks discussed at Nursing Strategy Board and monthly Quality /
Performance meeting
Overarching issues and risks discussed at Nursing Strategy Board and monthly Quality /
Performance meeting
Matron reviews staffing across areas to identify support
Matron reviews staffing across areas to identify support
Directorate review staffing to identify supportDirectorate review staffing to identify support
Nurse in charge identifies staffing does not meet patient needs based on acuity and dependency
Nurse in charge identifies staffing does not meet patient needs based on acuity and dependency
Risks and actions highlighted / discussed at site safety meeting
Risks and actions highlighted / discussed at site safety meeting
Site Safety Meeting•Cross directorate discussions to support at risk areas•Corporate overview of site safety•Actions identified
Site Safety Meeting•Cross directorate discussions to support at risk areas•Corporate overview of site safety•Actions identified
Chief Nurse informed and actions identifiedChief Nurse informed and actions identified
Datix Incident report completedDatix Incident report completed
Matron review incident and actions against daily site safety meeting actions
Matron review incident and actions against daily site safety meeting actions
Directorate Teams review weekly staffing incidents
Directorate Teams review weekly staffing incidents
Weekly site safety meetings with Corporate and Directorate teams
Weekly site safety meetings with Corporate and Directorate teams
Overarching issues and risks discussed at Nursing Strategy Board and monthly Quality /
Performance meeting
Overarching issues and risks discussed at Nursing Strategy Board and monthly Quality /
Performance meeting

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 16
5 EQUALITY IMPACT ASSESSMENT STATEMENT
5.1 All public bodies have a statutory duty under the Equality Act 2010 to have due
regard to the elimination of discrimination, harassment, victimisation and any other conduct prohibited by the Act
5.2 The Trust aims to design and implement services, policies and measures that meet the diverse needs of our service, population and workforce, ensuring that none is placed at a disadvantage over others. This document was found to be compliant with this philosophy.
5.3 Equality Impact Assessments will ensure discrimination does not occur also on the grounds of any of the protected characteristics covered by the Equality Act 2010. Refer to appendix ?.
6 MONITORING & REVIEW
What will be monitored How/Method/ Frequency
Lead Reporting to
Deficiencies/ gaps Recommendations and actions
Policy First review in one year and then every two years through senior nursing team
Chief Nurse NMSG Review, amend and replace edition on intranet.
Compliance with daily updates on SSIM
Weekly at site safety meeting
Deputy or Assistant Chief Nurse
Chief Nurse Heads of Nursing to cascade through line management structure to improve compliance
Weekly review of staffing datix submissions
Weekly at site safety meeting
Deputy or Assistant Chief Nurse
Chief Nurse Heads of Nursing to action against trends Cascade down line management structure

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 17
7 Appendix 1 Minimum agreed Staffing levels for the ward areas
The table below represents the minimum agreed staffing levels; this does not include the Senior Sister in a supervisory role. These are not the optimum staffing levels as outlined within the staffing policy and strategy. These numbers should be used as a guide for the decision around authorisation of agency both at Ward and senior level
Emergency Department
Day Twilight Night
RN CSW ENP CSW RN CSW
Ward/Department Day Night
RN/M CSW RN/M CSW RN/M CSW
Byron 3 3 3 2 3 2
Milton 4 3 3 2 3 2
Tennyson 3 3 3 2 3 2
ADL 2 4 2 4 - -
AMU 5 2 5 3 3 2
Bronte 3 1 3 1 3 0
Cardiac Catheter Suite 6 0 0 0 0 0
Dickens 3 3 3 2 3 2
Galton Day Unit 5 3 5 3 0 0
Gundulph 4 3 4 3 3 2
Harvey 3 3 3 2 3 2
Keats 3 3 3 2 3 2
Nelson 3 3 3 2 3 2
Wakeley 4 3 4 3 3 2
Will Adams 3 3 3 2 3 2
Lawrence 3 2 3 2 3 1
CCU 2 0 2 0 2 0
ICU 9 1 9 0 9 0
Kingfisher 2 2 2 2 2 -
SAU 2 2 2 2 2 2
POCU (Lister) Admission 2 2 2 1 - -
Sunderland Day theatres 22 6 22 6 - -
SDCC Ward 14 beds 2 2 2 2 2 1
SDCC day case ward 6 2 6 2 - -
Theatres 38 9 38 9 6 1
Trafalgar 5 1 5 1 5 -
Arethusa 5 3 4 3 4 3
Pembroke 4 3 3 3 3 2
Victory 2 2 2 2 2 2
McCulloch 4 3 4 3 4 2
Phoenix 4 2 4 2 4 2
NICU 9 0 9 0 9 0
Paediatrics 7 1 7 1 7 1
Obstetric Theatre Emergency 3 1 3 1 2 1
Obstetric Theatre 3 1 3 1 3 1
Maternity Unit 14 6 14 6 13 6
Ocelot 2 1 2 1 2 1

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 18
9 Appendix 2.1 Safer Care Nursing Tools Levels of Care and Multipliers
Acuity / Dependency Score
Sample Criteria Multiplier
0 Patient requires Hospitalisation
Elective medical or surgical admission
May have underlying medical condition requiring on-going treatment
Patients awaiting discharge
Post-operative / post-procedure care - observations recorded half hourly initially then 4-hourly
Regular observations 2 - 4 hourly
Early Warning Score is within normal threshold.
ECG monitoring
Fluid management
Oxygen therapy less than 35%
Patient controlled analgesia
Nerve block
Single chest drain
Confused patients not at risk
Patients requiring assistance with some activities of daily living, require the assistance of one to mobilise or experiences occasional incontinence
0.99
1a Acutely ill patients requiring intervention or those who are UNSTABLE with a GREATER POTENTIAL to deteriorate
Increased level of observations and therapeutic interventions
Early Warning Score - trigger point reached and requiring escalation.
Post-operative care following complex surgery
Emergency admissions requiring immediate therapeutic intervention.
Instability requiring continual observation/invasive monitoring
Oxygen therapy greater than 35% +/- chest physiotherapy 2 - 6 hourly
Arterial blood gas analysis - intermittent
Post 24 hours following insertion of tracheostomy, central lines, epidural or multiple chest or extra ventricular drains
Severe infection or sepsis
1.39
1b Patients who are in a STABLE condition but are dependant on nursing care to meet most or all of the activities of daily living.
Complex wound management requiring more than one nurse or takes more than one hour to complete.
VAC therapy where ward-based nurses undertake the treatment
Patients with spinal instability / spinal cord injury
Mobility or repositioning difficulties requiring the
1.72

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 19
Acuity / Dependency Score
Sample Criteria Multiplier
assistance of two people
Complex Intravenous Drug Regimes - (including those requiring prolonged preparatory/administration / post-administration care)
Patient and / or carers requiring enhanced psychological support due to poor disease prognosis or clinical outcome
Patients on End of Life Care Pathway
Confused patients who are at risk or requiring constant supervision
Requires assistance with most or all activities of daily living
Potential for self-harm and requires constant observation
Facilitating a complex
2 May be managed within clearly identified, designated beds, resources with the required expertise and staffing level OR may require transfer to a dedicated Level 2 facility / unit
Deteriorating / compromised single organ system
Post operative optimisation (pre-op invasive monitoring)/extended post-op care.
Patients requiring non-invasive ventilation/respiratory support; CPAP / BiPAP in acute respiratory failure
First 24 hours following tracheostomy insertion
Requires a range of therapeutic interventions including:
Greater than 50% oxygen continuously
Continuous cardiac monitoring and invasive pressure monitoring
Drug Infusions requiring more intensive monitoring e.g. vasoactive drugs (amiodarone, inotropes, gtn) or potassium, magnesium
Pain management - intrathecal analgesia
CNS depression of airway and protective reflexes
Invasive neurological monitoring
1.97
3 Patients needing advanced respiratory support and / or therapeutic support of multiple organs.
Monitoring and supportive therapy for compromised/collapse of two or more organ / systems
Respiratory or CNS depression/compromise requires mechanical /invasive ventilation
Invasive monitoring, vasoactive drugs, treatment of hypovolaemia /haemorrhage/sepsis or neuro protection
5.96
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 20
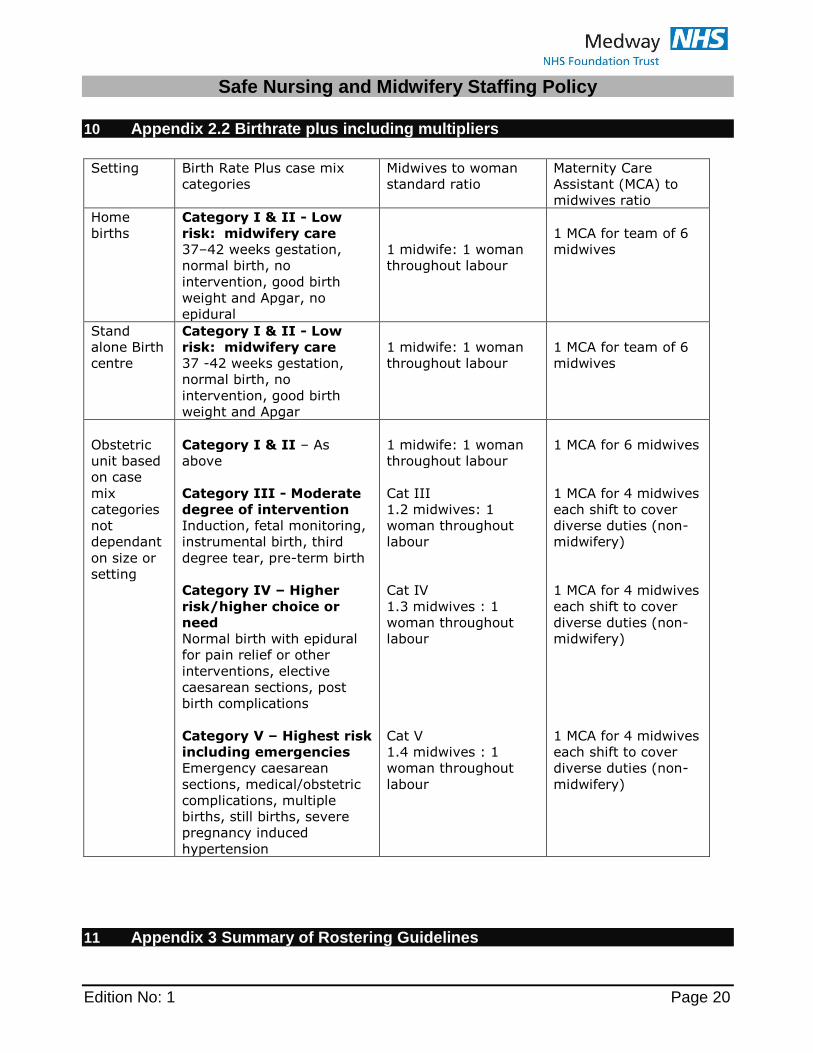
10 Appendix 2.2 Birthrate plus including multipliers
Setting Birth Rate Plus case mix
categories
Midwives to woman
standard ratio
Maternity Care
Assistant (MCA) to
midwives ratio
Home
births
Category I & II - Low
risk: midwifery care
37–42 weeks gestation,
normal birth, no
intervention, good birth
weight and Apgar, no
epidural
1 midwife: 1 woman
throughout labour
1 MCA for team of 6
midwives
Stand
alone Birth
centre
Category I & II - Low
risk: midwifery care
37 -42 weeks gestation,
normal birth, no
intervention, good birth
weight and Apgar
1 midwife: 1 woman
throughout labour
1 MCA for team of 6
midwives
Obstetric
unit based
on case
mix
categories
not
dependant
on size or
setting
Category I & II – As
above
Category III - Moderate
degree of intervention
Induction, fetal monitoring,
instrumental birth, third
degree tear, pre-term birth
Category IV – Higher
risk/higher choice or
need
Normal birth with epidural
for pain relief or other
interventions, elective
caesarean sections, post
birth complications
Category V – Highest risk
including emergencies
Emergency caesarean
sections, medical/obstetric
complications, multiple
births, still births, severe
pregnancy induced
hypertension
1 midwife: 1 woman
throughout labour
Cat III
1.2 midwives: 1
woman throughout
labour
Cat IV
1.3 midwives : 1
woman throughout
labour
Cat V
1.4 midwives : 1
woman throughout
labour
1 MCA for 6 midwives
1 MCA for 4 midwives
each shift to cover
diverse duties (non-
midwifery)
1 MCA for 4 midwives
each shift to cover
diverse duties (non-
midwifery)
1 MCA for 4 midwives
each shift to cover
diverse duties (non-
midwifery)
11 Appendix 3 Summary of Rostering Guidelines
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 21
A summary of the guidelines from the rostering policy to support the completion of local roster to meet service needs.
All rotas should be completed 6 weeks ahead of time to be worked
All rotas should be on the standard trust template until moved across to Eroster
All working weeks will start on a Monday
All rotas will be for 4 week periods
Names should be by Surname and listed by grade and alphabetically
Minimum of two thirds of total for the shift should be established registered nurses on or greater if establishment allows i.e. 2 out of 3
Minimum of two thirds of total for the shift should be established care support workers on or greater if establishment allows i.e. 2 out of 3
Annual leave should be limited to percentage of available staff rather than establishment
There is a built percentage for Annual Leave, Short Term Sickness and Study leave so this should be planned within your establishment
Only Maternity Leave, Long Term Sickness and unplanned absence not including short notice annual leave sit outside of the establishment
Short notice leave should only be granted if the rota can support without the use of temporary staffing
The Senior Sister should be supervisory in the first instance but should support the ward if staffing falls below agreed limits or acuity and dependency increases
The should be clear identification of the Nurse in charge
Band 6 Sisters should be rostered every day
All unfilled shifts should be with NHSP 4 weeks before worked
Agency Staff can only be utilised to ensure minimum agreed levels are maintained or increase in acuity / dependency or specialling is required in line with the specialling policy and risk assessment.

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 22
12 Appendix 4 Divisional Action Card
Actions Owner
Nursing Staff at or above minimum set levels Staffing meets patients acuity and dependency
1. Review acuity, dependency and activity and ensure patient needs can be met
2. Review Rota for the flowing shift and ensure staffing levels going forward meet patient needs
Nurse in Charge Senior Sister
Nursing Staff below minimum set criteria or does not meet patient acuity and dependency
1. Review acuity, dependency and activity can current staffing meet acuity, dependency and activity, if so reduce RAG to green
2. Escalate to Matron or Site Management out of hours 3. Review rota can staff be moved to ensure patient safety 4. Contact NHSP re support from Temp staffing 5. Review staffing, acuity dependency and activity across the cluster to
reallocate staff to ward 6. Escalate to Head of Nursing if unable to mitigate risk 7. Review Staffing across Division to reallocate staff 8. Review CNS activity to support wards 9. Authorise the use of agency staff
Nurse in Charge Senior Sister Matron / Site Team OOH Head of Nursing / General Manger / Site Team OOH
Nursing staff numbers cannot maintain patient safety All Amber actions have not mitigated the risk
1. Review staffing across the organisation and reallocate to patient need with discussion of Heads of Nursing and General Managers
2. Review and reallocate CNS’s, PDN’s and Clinical Matrons to support the ward
3. Review and divert internal patient flow to reduce demand on challenged areas
4. Reduce active bed base to maintain patient safety
Site Team Corporate Nursing Team
Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 23
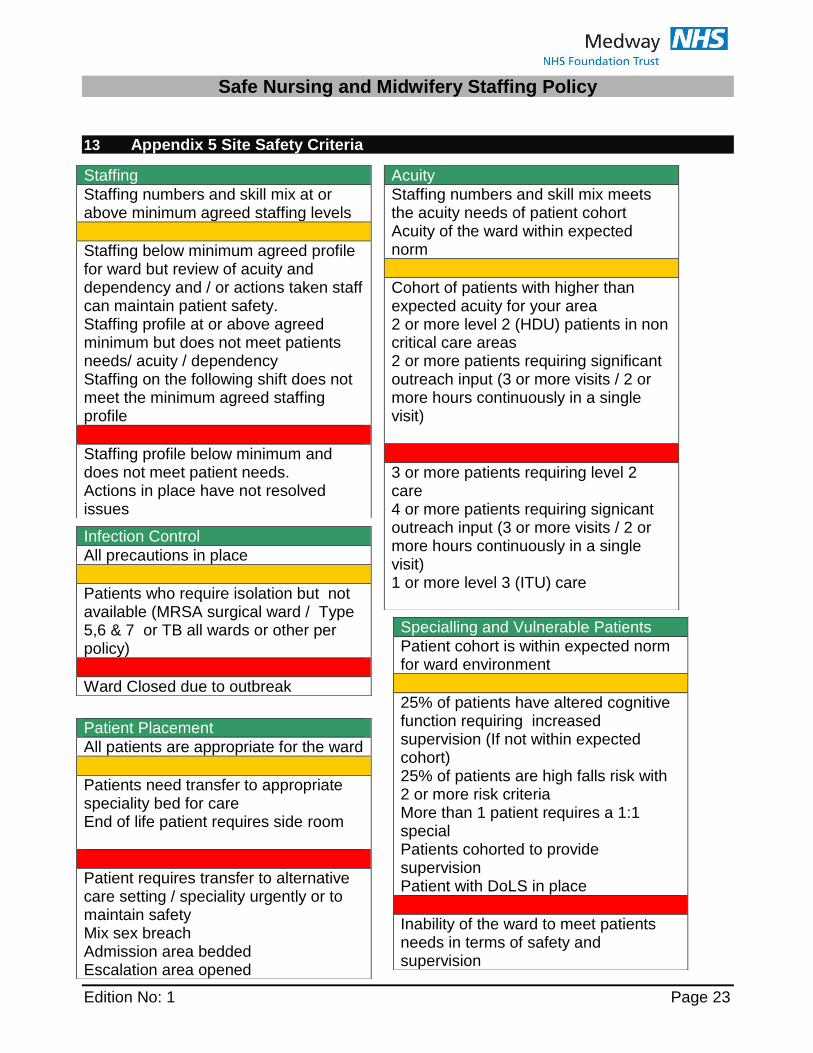
13 Appendix 5 Site Safety Criteria
Staffing
Staffing numbers and skill mix at or above minimum agreed staffing levels
Staffing below minimum agreed profile for ward but review of acuity and dependency and / or actions taken staff can maintain patient safety. Staffing profile at or above agreed minimum but does not meet patients needs/ acuity / dependency Staffing on the following shift does not meet the minimum agreed staffing profile
Staffing profile below minimum and does not meet patient needs. Actions in place have not resolved issues
Acuity
Staffing numbers and skill mix meets the acuity needs of patient cohort Acuity of the ward within expected norm
Cohort of patients with higher than expected acuity for your area 2 or more level 2 (HDU) patients in non critical care areas 2 or more patients requiring significant outreach input (3 or more visits / 2 or more hours continuously in a single visit)
3 or more patients requiring level 2 care 4 or more patients requiring signicant outreach input (3 or more visits / 2 or more hours continuously in a single visit) 1 or more level 3 (ITU) care
Infection Control
All precautions in place
Patients who require isolation but not available (MRSA surgical ward / Type 5,6 & 7 or TB all wards or other per policy)
Ward Closed due to outbreak
Specialling and Vulnerable Patients
Patient cohort is within expected norm for ward environment
25% of patients have altered cognitive function requiring increased supervision (If not within expected cohort) 25% of patients are high falls risk with 2 or more risk criteria More than 1 patient requires a 1:1 special Patients cohorted to provide supervision Patient with DoLS in place
Inability of the ward to meet patients needs in terms of safety and supervision
Patient Placement
All patients are appropriate for the ward
Patients need transfer to appropriate speciality bed for care End of life patient requires side room
Patient requires transfer to alternative care setting / speciality urgently or to maintain safety Mix sex breach Admission area bedded Escalation area opened

Safe Nursing and Midwifery Staffing Policy
Edition No: 1 Page 24
14 Appendix 6 Equality Impact Assessment Tool – Appendix
Yes/No Comments
1 Does the policy/guidance affect one group less or more favourably than another on the basis of:
Age no
Disability no
Gender reassignment no
Marriage and civil partnership no
Pregnancy and maternity no
Race no
Religion or belief no
Sex no
Sexual orientation no
2 Is there any evidence that some groups are affected differently?
no
3 If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
no
4 Is the impact of the policy/guidance likely to be negative?
no
5 If so can the impact be avoided? n/a
6 What alternatives are there to achieving the policy/guidance without the impact?
n/a
7 Can we reduce the impact by taking different action?
n/a
END OF DOCUMENT