sa1272 myeloid derived suppressor cell frequencies are increased in active refractory celiac disease
TRANSCRIPT
AG
AA
bst
ract
s
Sa1271
A Clinical Predictive Model for Differentiation of Celiac Disease and Non-Celiac Gluten SensitivityToufic A. Kabbani, Rohini R. Vanga, Javier A. Villafuerte-Galvez, Kumar Pallav, RupaMukherjee, Melinda Dennis, Daniel A. Leffler, Ciaran P. Kelly
Background: Differentiating between Celiac Disease (CD) and Non-Celiac Gluten Sensitivity(NCGS) is important for appropriate management yet often challenging. Currently, there is alack of evidence based recommendations for evaluation of patients reporting gluten responsivesymptoms to identify those with CD versus NCGS. Methods: We retrospectively reviewedrecords from 238 patients who presented to our center for evaluation of symptoms responsiveto the gluten free diet (GFD). Demographics, presenting symptoms, serologic, genetic andhistologic data, nutrient deficiencies, personal history of autoimmune diseases and familyhistory of celiac disease were recorded. NCGS was defined as symptoms responsive to aGFD in the setting of negative serology and duodenal biopsies or in the setting of negativeHLA DQ2/DQ8 testing. Results: 52.5% and 42.4% of the cohort subjects had NCGS andCD respectively. Nine subjects (3.8%) had non-celiac enteropathy (NCE) and three (1.3%)had an indeterminate diagnosis (Figure 1). 76.2% and 78.4% of the CD and NCGS subjectswere female respectively (p=0.8). NCGS subjects had a significantly earlier age of onset ofsymptoms compared to CD subjects (38.0 years vs. 42.2 years, p=0.003). CD subjectspresented with typical malabsorptive symptoms 67.3% of the time compared to only 24.8%of the GS subjects (p,0.0001). Additionally, CD subjects were significantly more likely tohave family history of CD, personal history of auto-immune diseases or nutrient deficiencies(Table 1). The sensitivity and specificity of a .2x ULN tTG or DGP with clinical responseto GFD for CD were 97% (CI: 91.5%-99%) and 100% (CI: 97.3%-100%), respectively(Figure 1). Similarly, the sensitivity and specificity of the combination of gluten responsivesymptoms and negative tTG or DGP on a regular diet for NCGS were 93.6% (CI: 87.9%-96.7%) and 90.3% (CI: 83.4%-94.5%), respectively (Figure 1). When individuals withnegative tTG or DGP also lacked malabsorptive symptoms or signs (weight loss, diarrhea,and nutrient deficiencies) and CD risk factors (personal history of autoimmune diseases andfamily history of CD), the specificity for NCGS increased to 100% (Figure 2). Conclusions:We analyzed findings from patients presenting with gluten responsive symptoms to developa clinical algorithm for differentiation between CD and NCGS. Celiac serologies (tTG or
S-248AGA Abstracts
DGP) are an important first step. Those with positive serology are highly likely to have CD.Those with borderline serology can undergo HLA typing to determine the need for biopsy.Those with negative serology who also lack clinical evidence of malabsorption and CD riskfactors are highly likely to have NCGS and may not require biopsy.Clinical and demographic differences between CD and NCGS
*Nutrient deficiency is defined as vitamin D, iron, vitamin B12, or Zn deficiency.
Abbreviations: .2x ULN; more than twice the upper limit of normal, CD; Celiac Disease,NCGS; Non-Celiac Gluten Sensitivity, NCE; Non-Celiac Enteropathy
Sa1272
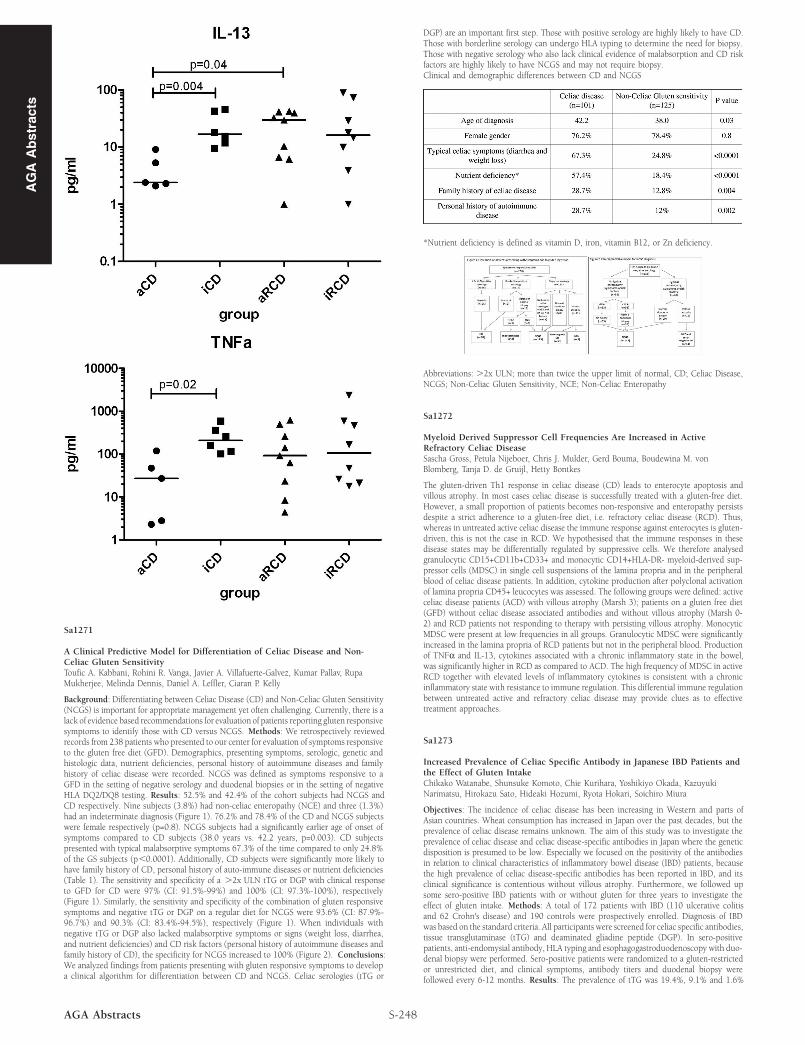
Myeloid Derived Suppressor Cell Frequencies Are Increased in ActiveRefractory Celiac DiseaseSascha Gross, Petula Nijeboer, Chris J. Mulder, Gerd Bouma, Boudewina M. vonBlomberg, Tanja D. de Gruijl, Hetty Bontkes
The gluten-driven Th1 response in celiac disease (CD) leads to enterocyte apoptosis andvillous atrophy. In most cases celiac disease is successfully treated with a gluten-free diet.However, a small proportion of patients becomes non-responsive and enteropathy persistsdespite a strict adherence to a gluten-free diet, i.e. refractory celiac disease (RCD). Thus,whereas in untreated active celiac disease the immune response against enterocytes is gluten-driven, this is not the case in RCD. We hypothesised that the immune responses in thesedisease states may be differentially regulated by suppressive cells. We therefore analysedgranulocytic CD15+CD11b+CD33+ and monocytic CD14+HLA-DR- myeloid-derived sup-pressor cells (MDSC) in single cell suspensions of the lamina propria and in the peripheralblood of celiac disease patients. In addition, cytokine production after polyclonal activationof lamina propria CD45+ leucocytes was assessed. The following groups were defined: activeceliac disease patients (ACD) with villous atrophy (Marsh 3); patients on a gluten free diet(GFD) without celiac disease associated antibodies and without villous atrophy (Marsh 0-2) and RCD patients not responding to therapy with persisting villous atrophy. MonocyticMDSC were present at low frequencies in all groups. Granulocytic MDSC were significantlyincreased in the lamina propria of RCD patients but not in the peripheral blood. Productionof TNFα and IL-13, cytokines associated with a chronic inflammatory state in the bowel,was significantly higher in RCD as compared to ACD. The high frequency of MDSC in activeRCD together with elevated levels of inflammatory cytokines is consistent with a chronicinflammatory state with resistance to immune regulation. This differential immune regulationbetween untreated active and refractory celiac disease may provide clues as to effectivetreatment approaches.
Sa1273
Increased Prevalence of Celiac Specific Antibody in Japanese IBD Patients andthe Effect of Gluten IntakeChikako Watanabe, Shunsuke Komoto, Chie Kurihara, Yoshikiyo Okada, KazuyukiNarimatsu, Hirokazu Sato, Hideaki Hozumi, Ryota Hokari, Soichiro Miura
Objectives: The incidence of celiac disease has been increasing in Western and parts ofAsian countries. Wheat consumption has increased in Japan over the past decades, but theprevalence of celiac disease remains unknown. The aim of this study was to investigate theprevalence of celiac disease and celiac disease-specific antibodies in Japan where the geneticdisposition is presumed to be low. Especially we focused on the positivity of the antibodiesin relation to clinical characteristics of inflammatory bowel disease (IBD) patients, becausethe high prevalence of celiac disease-specific antibodies has been reported in IBD, and itsclinical significance is contentious without villous atrophy. Furthermore, we followed upsome sero-positive IBD patients with or without gluten for three years to investigate theeffect of gluten intake. Methods: A total of 172 patients with IBD (110 ulcerative colitisand 62 Crohn's disease) and 190 controls were prospectively enrolled. Diagnosis of IBDwas based on the standard criteria. All participants were screened for celiac specific antibodies,tissue transglutaminase (tTG) and deaminated gliadine peptide (DGP). In sero-positivepatients, anti-endomysial antibody, HLA typing and esophagogastroduodenoscopy with duo-denal biopsy were performed. Sero-positive patients were randomized to a gluten-restrictedor unrestricted diet, and clinical symptoms, antibody titers and duodenal biopsy werefollowed every 6-12 months. Results: The prevalence of tTG was 19.4%, 9.1% and 1.6%