sa tb guidelines the interface with advanced clinical care
TRANSCRIPT

SA TB Guidelines – The interface
with Advanced Clinical Care
Dr Kogie Naidoo (MBCHB, PHD)
Head: CAPRISA Treatment Research Programme
Honorary Lecturer - UKZN Department of Public Heath Medicine
Annual Workshop on Advanced Clinical Care
ICC Durban
6 October 2016

Presentation Outline
• Diagnostic algorithm for DR and DS TB
• Retreatment TB: Revised definitions and
treatment regimen
• ART initiation in TB patients
• Special considerations:
Aluvia with TB treatment
Atazanavir in TB
Ethambutol in Renal failure
Moxifloxacin and streptomycin indications
• TB prevention in HIV infected patients
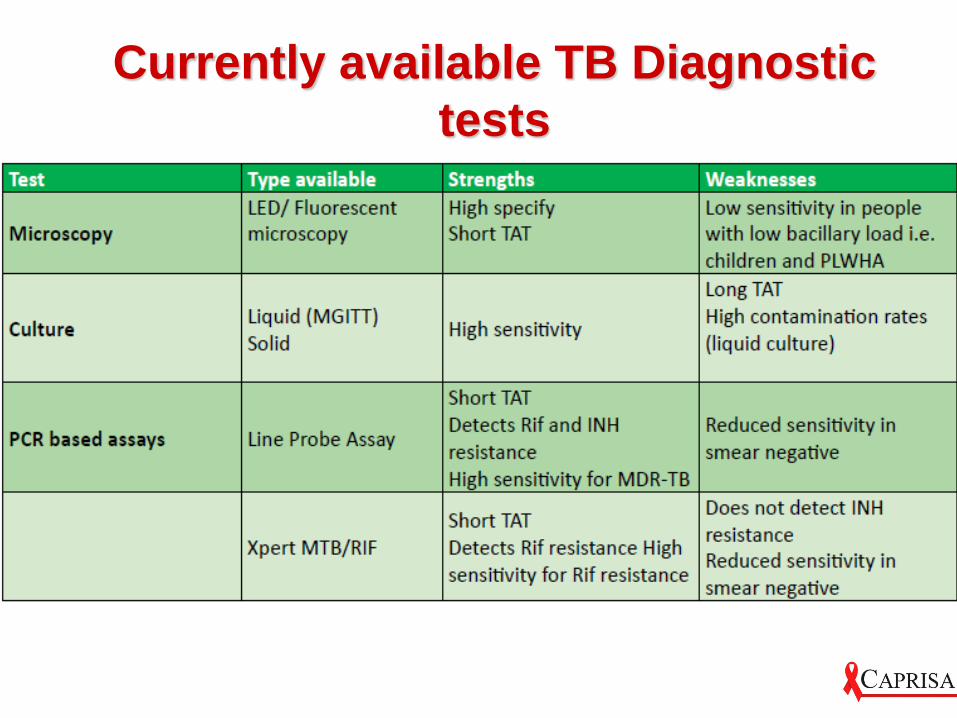
Currently available TB Diagnostic
tests
Which initial TB diagnostic test does
WHO recommend for HIV + people with
suspected TB?
1. Smear Microscopy
2. Xpert MTB/RIF
3. Culture
Which initial TB diagnostic test does
WHO recommend for HIV + people with
suspected TB?
1. Smear Microscopy
2. Xpert MTB/RIF
3. Culture
Where GeneXpert (GXP) is available,
culture may still be required for:
1. HIV positive TB suspects, who have a negative GXP test
2. TB cases diagnosed as Rifampicin(Rif) resistant on GXP
for susceptibility testing of other drugs
3. Despite a Rif susceptible result, the patient is failing
treatment and treatment adherence is good and thus
resistance to drugs other than Rif is suspected
4. All of the above

TB SUSPECTS
TB and DR-TB contacts, non-contact symptomatic individuals, re-treatment after relapse, failure and default
Collect one sputum specimen at the health facility under supervision
GXP positive
Rifampicin susceptible
GXP positive
Rifampicin resistant
GXP positive
Rifampicin
unsuccessful
GXP negative GXP unsuccessful
Treat as TB
Start on Regimen 1
Send one specimen for
microscopy
Treat as MDR-TB
Refer to MDR-TB
facility
Treat as TB
Start on Regimen 1
Collect one specimen
for microscopy
Culture & DST / LPA
Collect one sputum
specimen for a
repeat GXP
HIV positive HIV negative
Collect one specimen for culture and
LPA or culture and DST (for R and H)
Treat with antibiotics and review after 5
days
Do chest x-ray
Treat with antibiotics
Poor response to
antibiotics
Clinically TB
TB on chest x-ray
LPA/ DST results
Resistant to R
and H/ R only
Good response
No further follow
up
Advise to return
when symptoms
recur
Poor response
Consider other
diagnosis
Refer for further
investigation
Treat as MDR-TB
Refer to MDR-TB Unit
Treat as TB
Start on Regimen 1
Review culture results
Follow up with
microscopy
Collect one specimen for
microscopy, culture and
DST for Rifampicin,
Isoniazid, fluoroquinolone
and Aminoglycoside
Follow up with
microscopy and culture

Where GeneXpert (GXP) is available,
culture may still be required for:
1. HIV positive TB suspects, who have a negative GXP test
2. TB cases diagnosed as Rifampicin(Rif) resistant on GXP
for susceptibility testing of other drugs
3. Despite a Rif susceptible result, the patient is failing
treatment and treatment adherence is good and thus
resistance to drugs other than Rif is suspected
4. All of the above

Streptomycin is indicated for:
1. All categories of DS TB
2. All categories of retreatment TB
3. For patients that cannot tolerate first line
TB medication
4. All of the above
5. None of the above

TB SUSPECTS
TB and DR-TB contacts, non-contact symptomatic individuals, re-treatment after relapse, failure and default
Collect one sputum specimen at the health facility under supervision
GXP positive
Rifampicin susceptible
GXP positive
Rifampicin resistant
GXP positive
Rifampicin
unsuccessful
GXP negative GXP unsuccessful
Treat as TB
Start on Regimen 1
Send one specimen for
microscopy
Treat as MDR-TB
Refer to MDR-TB
Unit
Treat as TB
Start on Regimen 1
Collect one specimen
for microscopy
Culture & DST / LPA
Collect one sputum
specimen for a
repeat GXP
HIV positive HIV negative
Collect one specimen for culture and
LPA or culture and DST (for R and H)
Treat with antibiotics and review after 5
days
Do chest x-ray
Treat with antibiotics
Poor response to
antibiotics
Clinically TB
TB on chest x-ray
LPA/ DST results
Resistant to R
and H/ R only
Good response
No further follow
up
Advise to return
when symptoms
recur
Poor response
Consider other
diagnosis
Refer for further
investigation
Treat as MDR-TB
Refer to MDR-TB Unit
Treat as TB
Start on Regimen 1
Review culture results
Follow up with
microscopy
Collect one specimen for
microscopy, culture and
DST for Rifampicin,
Isoniazid, fluoroquinolone
and Aminoglycoside
Follow up with
microscopy and culture

Streptomycin is indicated for:
1. All categories of DS TB
2. All categories of retreatment TB
3. For patients that cannot tolerate first line
TB medication
4. All of the above
5. None of the above
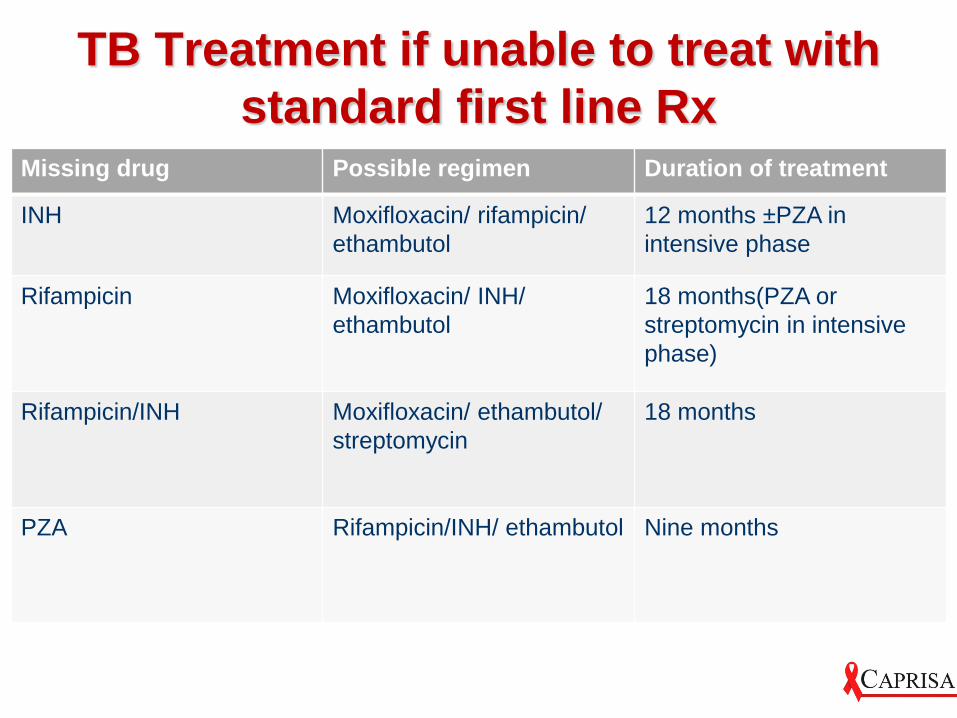
TB Treatment if unable to treat with
standard first line RxMissing drug Possible regimen Duration of treatment
INH Moxifloxacin/ rifampicin/
ethambutol
12 months ±PZA in
intensive phase
Rifampicin Moxifloxacin/ INH/
ethambutol
18 months(PZA or
streptomycin in intensive
phase)
Rifampicin/INH Moxifloxacin/ ethambutol/
streptomycin
18 months
PZA Rifampicin/INH/ ethambutol Nine months
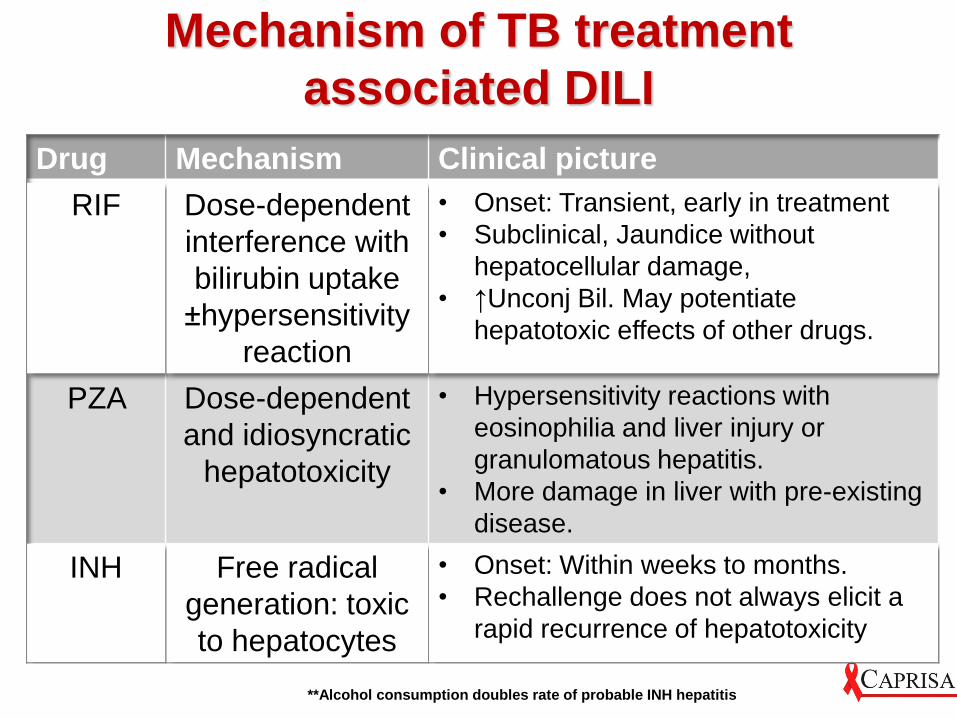
Mechanism of TB treatment
associated DILI
Drug Mechanism Clinical picture
RIF Dose-dependent
interference with
bilirubin uptake
±hypersensitivity
reaction
• Onset: Transient, early in treatment
• Subclinical, Jaundice without
hepatocellular damage,
• ↑Unconj Bil. May potentiate
hepatotoxic effects of other drugs.
PZA Dose-dependent
and idiosyncratic
hepatotoxicity
• Hypersensitivity reactions with
eosinophilia and liver injury or
granulomatous hepatitis.
• More damage in liver with pre-existing
disease.
INH Free radical
generation: toxic
to hepatocytes
• Onset: Within weeks to months.
• Rechallenge does not always elicit a
rapid recurrence of hepatotoxicity
**Alcohol consumption doubles rate of probable INH hepatitis

Definition of DILI
SA HIV Clinician’s Society
DILI guidelines:
ALT level > 120 IU/L and symptomatic
(Nausea, vomiting, abdominal pain,
jaundice) or
ALT level >200 IU/L and asymptomatic
or
Total serum bilirubin concentration > 40
umol/L

Risk factors for DILIModifiable Non-modifiable
• HIV infection
• Hepatitis B Surface
antigen positivity
• Hepatitis C co-
infection
• Malnutrition
• Hypo-albuminaemia
• Abnormal baseline
ALT
• Alcohol use
• Underlying liver
disease
• Age >35 years
• Childhood
• Slow acetylator status
• Female sex

Management of TB DILI
• Limited data
• Most guidelines are based on expert opinion

Principles of TB DILI
management• Moderate to severe liver damage STOP
drugs
• Investigate for other causes of hepatitis
• Confirm the diagnosis of TB
Green card
Intensive phase/ continuation phase
Search for pending TB culture results
Re-investigate for TB

TB Drug Rechallenge in DILI
• If patient presented in liver failure:
TB drug re-challenge is not recommended
• Otherwise, re-challenge
Rates of DILI recurrence in re-challenge is 12 %
• Rechallenge method: Regimen Rechallenge vs Sequential
Drug Rechallenge - latter in full doses vs incremental doses
• RCT data on Rates of DILI recurrence by type of Rechallenge
method: Regimen Rechallenge (14%) vs Sequential Drug
Rechallenge in full (10%) vs incremental (9%) doses
Case 1
• Miss HS is a HIV positive 34 year old female.
• She is clinically stable on an FDC.
• She is diagnosed with TB Lymphadenopathy
based on AFB demonstrated in LN aspirate
following a 2 month duration of fever and LOA.
• She tolerates TB Rx well and has resolution of
constitutional symptoms.
• On routine LFT is as follows:
ALT= 79 IU/L AST= 60 IU/L
Normal Total bilirubin Normal ALP and GGT

What is the most appropriate
management?
1. Refer for admission, Stop TB treatment, Stop
ART
2. Continue TB treatment and ART, discharge
from follow up
3. Continue TB treatment and ART, repeat ALT
and Bili in 1 week
4. Continue TB treatment and ART, repeat ALT
and Bili daily

What is the most appropriate
management?
1. Refer for admission, Stop TB treatment, Stop
ART
2. Continue TB treatment and ART, discharge
from follow up
3. Continue TB treatment and ART, repeat ALT
and Bili in 1 week
4. Continue TB treatment and ART, repeat ALT
and Bili daily

Mild DILI
Clinically well
ALT <200 and Total Bili <40
• Continue TB drugs
• Continue ART if already initiated
• Repeat ALT and Bili in 1 week
• If ALT and bili improving or normal then stop Lab
monitoring
• If ALT and Bili continue to rise, treat as moderate
or severe DILI

Moderate DILI
Clinically well
ALT> 200 irrespective of Total Bili
• Stop TB regimen
• Discontinue Bactrim prophylaxis and other hepatotoxic drugs
• Start ETH/ MOX/ STR if treatment necessary
• Stop ART unless on a stable ART regimen for > 6 months
• Repeat ALT and Bili in 3 (Inpt) or 7 (Outpt) days
• When ALT < 100 and Bili is normal, attempt rechallenge

TB Drugs in Renal failure
• INH, rifampicin, PZA : biliary excretion normal doses
•Streptomycin and ethambutol : can maintain at reduced dose – monitor for uveitis
•Safest regimen: INH, Rifampicin, pyrazinamide X 4 months followed by INH and Rifampicin x 2 months

Managing TB treatment
Interruption
• Less than 1 month: extend treatment for the number of days that patient did not take treatment
• 1-2 months missed: do geneXpert Sensitive: add number of days that patient did not take
treatment.
Resistant: stop treatment: refer to MDR-TB unit
• More than 2 months missed (loss to follow up) do geneXpert Sensitive : restart treatment
Resistant : refer MDR-TB

Integration of TB HIV Services
• Screening for TB and HIV at same visit
• Early initiation of ARVs
• Co-management of Drug toxicities common
to both
• Consideration of Drug interactions
• Early detection and management of TB IRIS
• Initiation of INH prophylaxis
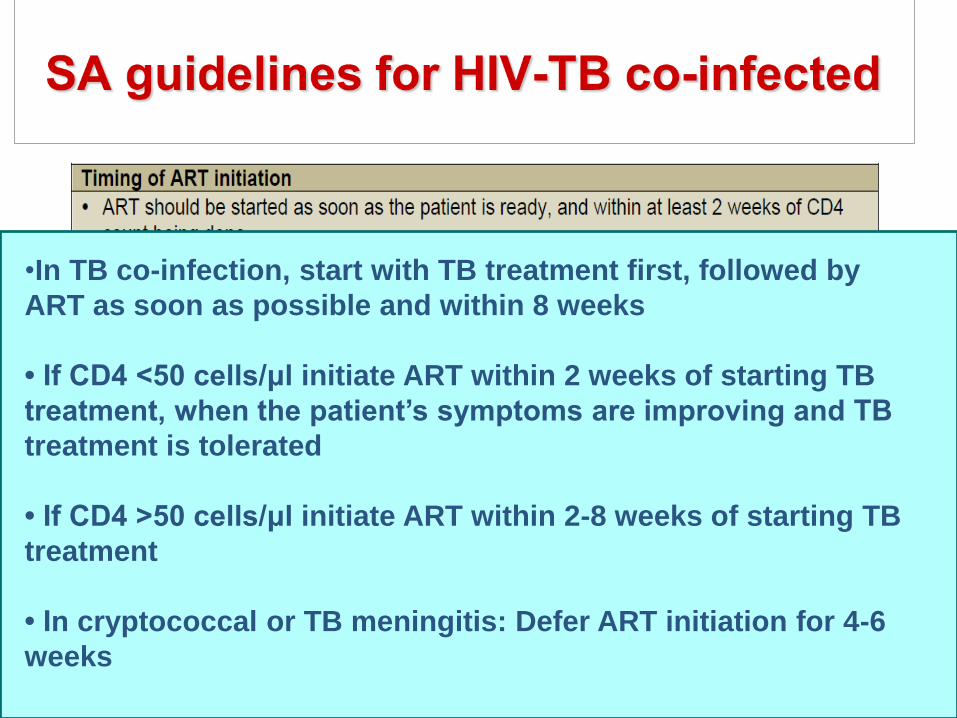
•In TB co-infection, start with TB treatment first, followed by
ART as soon as possible and within 8 weeks
• If CD4 <50 cells/μl initiate ART within 2 weeks of starting TB
treatment, when the patient’s symptoms are improving and TB
treatment is tolerated
• If CD4 >50 cells/μl initiate ART within 2-8 weeks of starting TB
treatment
• In cryptococcal or TB meningitis: Defer ART initiation for 4-6
weeks
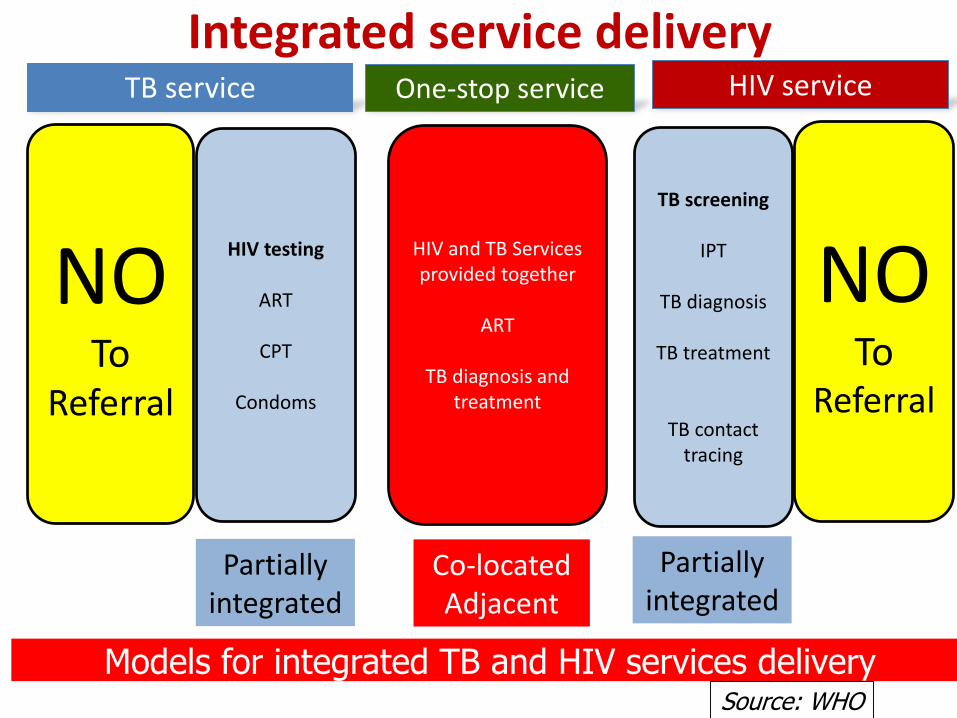
TB service One-stop service HIV service
NOTo
Referral
HIV testing
ART
CPT
Condoms
Partiallyintegrated
HIV and TB Services provided together
ART
TB diagnosis and treatment
Co-locatedAdjacent
NOTo
Referral
TB screening
IPT
TB diagnosis
TB treatment
TB contact tracing
Partiallyintegrated
Models for integrated TB and HIV services delivery
Integrated service delivery
Source: WHO

Concerns of co-treating TB and HIV
• Overlapping Toxicity
• Drug Interactions
• IRIS

What are the overlapping drug toxicities with TB treatment and ARVs?
1. Liver Injury
2. Rash
3. Psychosis
4. All of the above
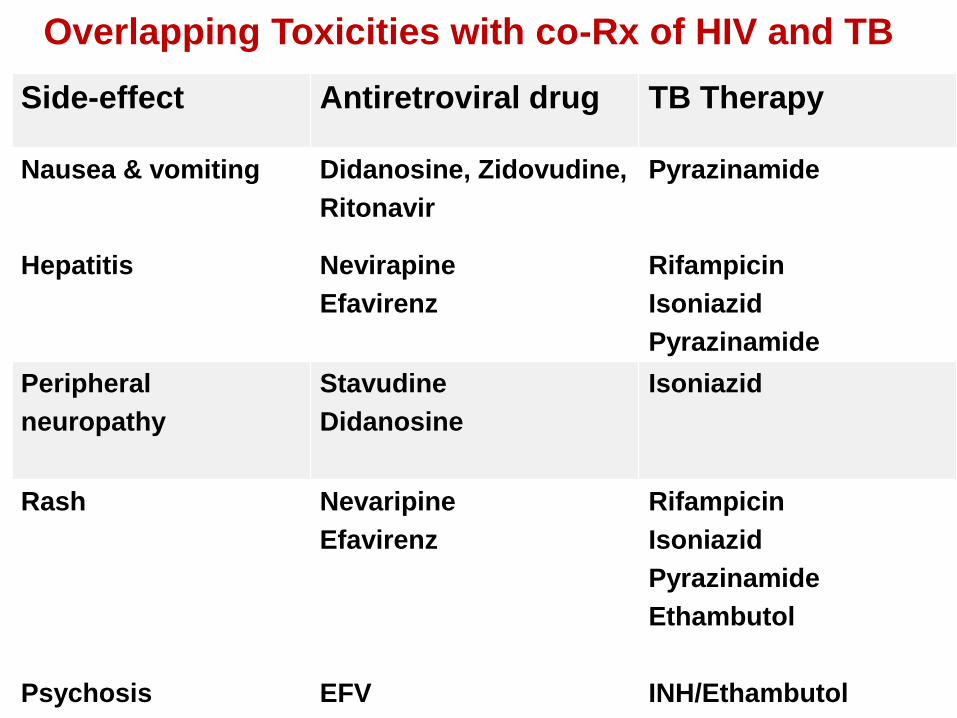
Side-effect Antiretroviral drug TB Therapy
Nausea & vomiting Didanosine, Zidovudine,
Ritonavir
Pyrazinamide
Hepatitis Nevirapine
Efavirenz
Rifampicin
Isoniazid
Pyrazinamide
Peripheral
neuropathy
Stavudine
Didanosine
Isoniazid
Rash
Psychosis
Renal Toxicity
Nevaripine
Efavirenz
EFV
Tenofovir
Rifampicin
Isoniazid
Pyrazinamide
Ethambutol
INH/Ethambutol
Rifampicin
Overlapping Toxicities with co-Rx of HIV and TB

What are the overlapping drug toxicities with TB treatment and ARVs?
1. Liver Injury
2. Rash
3. Psychosis
4. All of the above

Case 2
• Mrs AA is HIV + since 2010. She was
initially started on TDF / 3TC and EFV.
• In 2014, she was changed to ABC / 3TC
and Alluvia due to treatment failure.
• She now presents with night sweats, loss
of appetite and abdominal pain.
• The Gene Xpert test on ascitic fluid is
positive for Rif sensitive MTB

How to do you manage further?
1. Start TB Rx, double the dose of Aluvia
immediately
2. Start TB Rx, double the dose of Aluvia over 2
weeks
3. Double the dose of Aluvia over 2 weeks then
start TB Rx

How to do you manage further?
1. Start TB Rx, double the dose of Aluvia
immediately
2. Start TB Rx, double the dose of Aluvia over
2 weeks
3. Double the dose of Aluvia over 2 weeks then
start TB Rx

Mrs AA improves on TB Rx and completes the
course. Her symptoms and signs have
resolved, and her exit sputum is negative for
AFB. How do you manage further?
1. Reduce Aluvia dose to 2T bd immediately
2. Continue TB Rx for two weeks longer
3. Continue the double dose (4T bd) of
Aluvia until 2 weeks after TB Rx is
completed

Mrs AA improves on TB Rx and completes the
course. Her symptoms and signs have
resolved, and her exit sputum is negative for
AFB. How do you manage further?
1. Reduce Aluvia dose to 2T bd immediately
2. Continue TB Rx for two weeks longer
3. Continue the double dose (4T bd) of
Aluvia until 2 weeks after TB Rx is
completed

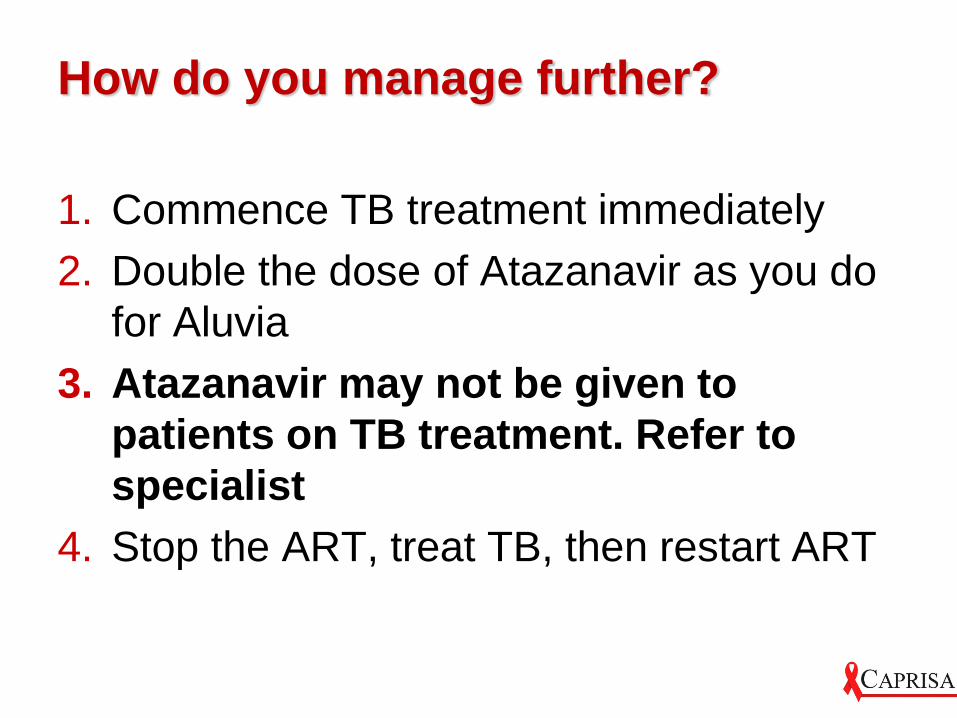
Case 3
• Mr E has been on a second line regimen
for a year.
• His regimen includes AZT/3TC/ATZ/rit
because he had severe diarrhoea whilst
on Aluvia.
• He now presents with fever and productive
cough.
• His sputum Gene Xpert is positive for Rif
sensitive MTB.

How do you manage further?
1. Commence TB treatment immediately
2. Double the dose of Atazanavir as you do
for Aluvia
3. Atazanavir may not be given to patients
on TB treatment. Refer to specialist
4. Stop the ART, treat TB, then restart ART
How do you manage further?
1. Commence TB treatment immediately
2. Double the dose of Atazanavir as you do
for Aluvia
3. Atazanavir may not be given to
patients on TB treatment. Refer to
specialist
4. Stop the ART, treat TB, then restart ART

Drug Interactions: 1. RIF and EFV
• Previously reported that Rif caused a 30%
decrease in EFV trough concentrations,
particularly in patients >50kg.
• An increase in EFV dose recommended by FDA
(USA)
• Later reports → clearance of EFV is reduced in
black African patients, due to CYP enzyme
polymorphisms (therefore drug levels actually
increased by 30-50%)
• No increase in EFV dose recommended in SA

2. RIF and PI• PI metabolized by CYP 3A4: induced by Rifampicin and
inhibited by Ritonavir
• Significant reduction of plasma drug levels of most PI’s, except Ritonavir
• LPV/r (Aluvia): Ritonavir boosted Lopinavir (400/100mg)
• Increase Ritonavir to 400mg daily to overcome the enzyme induction – double Aluvia dose
Usual 2T BD, increased to 3T BD for 1 wk then 4T BD
Maintain escalated dose of PI until 2 wks after TB Rx completion
• Rif accelerated Atazanavir/r metabolism, cannot be overcome by boosting with Ritonavir
Referral to higher centre to change PI or change Rifampicin to Rifabutin

TB IRIS
TB diagnosed & treatment started
before ART initiation
No TB diagnosis before ART initiation
ART Initiation
Clinical deterioration of TB as a result of
ART-induced immune recovery =
Paradoxical TB IRIS
Atypical inflammatory presentation of TB as a result of ART-induced
immune recovery = Unmasking IRIS
Lawn Expert Rev Anti Infect Ther, 2011.

TB IRIS incidence, risk factors and
outcomes• Unmasking TB IRIS Incidence 4.8% (most
common )
• Paradoxical TB-IRIS Incidence 18%
• Onset 14 days after ART initiation in 48%
• Hospitalisation 25%
• Mortality 7%, death attributed to TB IRIS 2%
• Increased mortality in CNS IRIS
• Risk Factors: Low CD4 count, Short interval
between TB treatment and ART, Disseminated
TB

TB IRIS Management
• Double-blind, placebo-controlled RCT• Intervention: Prednisone 1.5mg/kg/day x 2 wks then
0.75mg/kg/day x 2 wks• Primary outcome = hospital days• Findings: Steroid arm - fewer days in hospital and fewer
procedures. IRIS associated mortality same in both arms, except CNS disease
• Excl other causes of patient deterioration: MDR TB etc

What are the current guidelines for IPT for patients on ART?
1. 36 months IPT for all patients
2. 12 months IPT for all patients
3. 6 months IPT for all patients
4. 36 months IPT for TST positive, 12 months for TST negative, 6 months for TST unknown
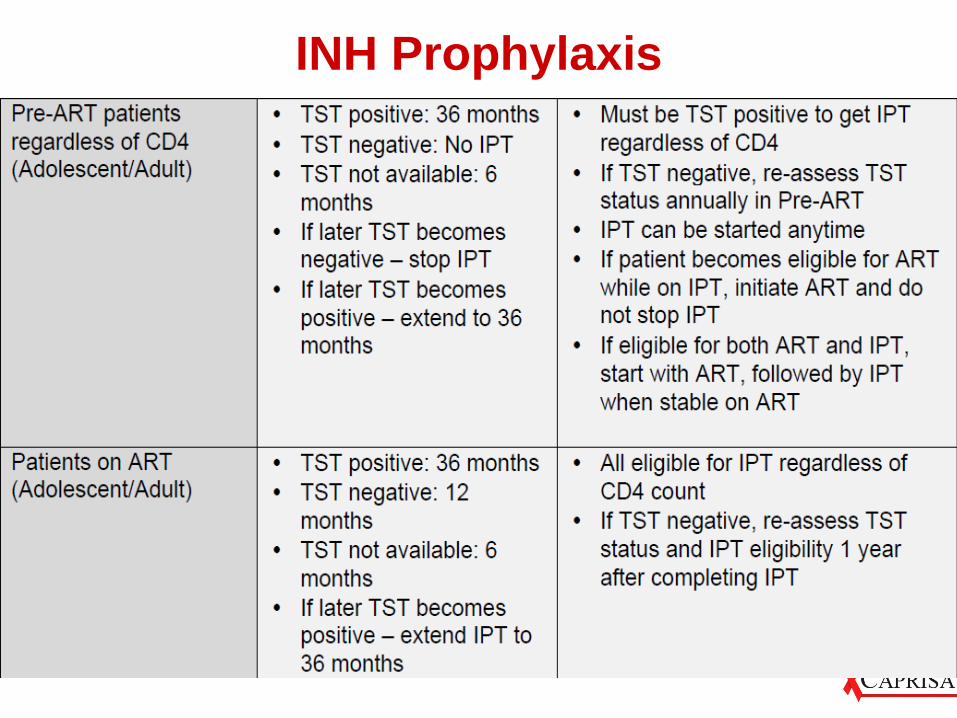
INH Prophylaxis

What are the current guidelines for IPT for patients on ART?
1. 36 months IPT for all patients
2. 12 months IPT for all patients
3. 6 months IPT for all patients
4. 36 months IPT for TST positive, 12 months for TST negative, 6 months for TST unknown

Questions
Are patients eligible for more IPT post TB therapy completion?
1. Yes: can be started immediately after TB treatment in all patients
2. No: patients no longer at risk for TB, having just completed TB treatment
3. Yes: can be started immediately after TB treatment but only in patients with documented bacteriologic cure
Questions
Are patients eligible for more IPT post TB therapy completion?
1. Yes: can be started immediately after TB treatment in all patients
2. No: patients no longer at risk for TB, having just completed TB treatment
3. Yes: can be started immediately after TB treatment but only in patients with documented bacteriologic cure

Summary
• Diagnostic algorithm for DR and DS TB
• Retreatment TB: Revised definitions and
treatment regimen
• ART initiation in TB patients
• Special considerations:
Aluvia with TB treatment
Atazanivir in TB
Ethambutol in Renal failure
Moxifloxacin and streptomycin indications
• TB prevention in HIV infected patients
Acknowledgements
This training was supported by the
Grant or Cooperative Agreement
Number U2G GH001142, funded by
the Centers for Disease Control and
Prevention. Its contents are solely
the responsibility of the presenters
and do not necessarily represent the
official views of the U.S. Centers for
Disease Control and Prevention or
the U.S. Department of Health and
Human Services