s ward rotation manual may 2011
TRANSCRIPT

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 1/41
DIVINE WORD UNIVERSITY
Health Extension Department
CLINICAL SURGERY 2
UNIT: HE313
WARD ROTATION
HAND BOOK
Bob Simon
Clinical Lecturer
2011

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 2/411
Contents Page
Introduction ……………………………………………………………………………… 2
Clinical Performance Assessment ………………………………………….….. 5
Weekly Program ……………………………………………………………………..… 10
Clinical Attachment Grouping …………………………………………………… 11
Ward Duty Roster …………………………………………………………..………… 12
Unit Outline …………………………………………………………………..………… 13
Clinical Supervisor Weekly Program ………………………………..……… 16
Attendance record ………………………………………………………..……….. 16
History Taking & Clinical Exam (guide) …………………………..………. 17
Assessment Task ……………………………………………………………..…….. 22
Referencing Procedures …………………………………………………..…….. 23
Assessment Cover Sheet ................................................ 26

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 3/41 2
Introduction
Students cover surgical unit by doing eight weeks of fulltime clinical practical. This means that
students will work during working hours, from 8am to 4pm, some roosted on duty after hours from
6pm to 10pm, night duty from 10pm to 7am and weekends). You are expected to do clinical
observations and perform clinical practical and procedures under supervision in surgical Departmentof Modilon Hospital. This is supplemented with teaching ward rounds, bedside tutorials, case
presentations by hospital Medical Officers and tutorial sessions with a clinical supervisor on the
university campus. This unit is designed to equip Rural Health students the knowledge and skills in
the triaging and the fundamental basics in managing surgical conditions in a competent manner in
rural Papua New Guinea..
WARD DUTIES
Please read before starting Ward Clinical Rotation.
While you are attached to Surgical Unit (Ward 3), you will become part of the health team caring forall patients in this ward.
1. ADMISSIONS:
You will be responsible for admitting all patients. Each student should have approximately
equal numbers of patients to care for, once you admit a patient, that patient becomes you
responsibility until he is discharged or you change rotations. You must give any stat
treatment and sign the treatment sheet for new admission.
2. DISCHARGE:
When a patient is discharge, you must:
(a) Write a discharge form.
(b) Write a summary in the clinic book.
(c) Write a letter to the referring centre (if the patient was referred) and tick the
appropriate space on the front of the chart
(d) Arrange any necessary follow up.
(e) Make sure discharge medications are supplied and that the parent/guardian knows
how to give them.
3. WEIGHT:
All patients should be weighed on admission.
4. LABORATORY TESTS
You must chase up all of your patients results.
5. BLOOD SLIDE:

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 4/41
3
Blood slide should be taken on patients who are sick or have fever.
6. HAEMOGLOBIN AND FULL BLOOD COUNT:
Routinely haemoglobin should be done to all new admissions. HB and FBC on all cancerpatients weekly.
7. OTHER TEST: May be ordered as necessary.
8. WARD ROUNDS:
Ward rounds begin at 8:00am Mondays, Wednesdays, and Fridays. You are expected to have
seen your patients before this round begins. During the round you will present a summary of
each patient’s history and examination that you are caring for and your management plan.
After discussion with the Medical Officer or your clinical tutor, you will then be expected to
make sure that all treatment, tests, etc, are carried out.
9. OPERATING THEATRE
Tuesdays and Thursdays are operating days. Those students who are listed to observe
surgical procedures must be in the theatre by 8am. There should be no more than four
students at any one time. Theatre rules must be followed. Priority to year three & four HE
students.
10 PROCEDURES:
When you carry out the procedure, e.g. Put up I.V. drip, do I & D, you are responsible forcleaning up after words and repacking any tray you may have used and return it to CSD.
11. AFTER HOURS DUTY:
A roster needs to be made to cover this and you should each have a turn at making up a
roster. When you are on after normal working hours, you are responsible for all admissions,
and any other sick patients in the ward. If there are problems you are not sure how to
handle, you need to discuss these with Medical Officer on call to cover the ward for that
time, (see roster on notice board).
12. WARDS:
Ward three A is where all new admissions go. (Clean cases)
Ward three B & C is where all dirty cases are admitted (dirty cases)
13. INPATIENT EDUCATION:
While patient is in the hospital, you need to educate him about:
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 5/414
(a) His disease and its likely outcome.
(b) The treatment for that disease and how long he is likely to be in hospital.
(c) Nutrition, if the patient is malnourished.
14. HANDOVER:
When leaving this ward rotation, you must write a summary in the chard for the person who
will be caring for the patient next and tell them about your patients before you leave.
When you are handing over to someone else for after hour’s duties, you must tell them of
all problems in the ward.
15. DURATION:
Your ward rotation begins at 8:00am on the first Monday and ceases at 10.30pm on the
Sunday eight weeks later, except for those students whose rotation ceases at term break
when the rotation ceases at 4.00pm on the Friday.
16. ASSISTANCE IN WARD.
Do not hesitate to ask your RHEO, RMO, surgical registrar or SMO if you need assistance in
clinical practice. Ask the nursing officers for any general nursing procedures.
17. ILLNESS:
If you are sick, you must contact one of the Medical Officers or clinical lecturer. You should
arrange for someone else to care for your patients and do your on call while you remain ill.Make sure to obtain Medical Certificate from the medical officer or registrar if you are too
sick to attend duties.
18. STAFF RELATIONSHIP:
You will be part of a team while working in this ward. If you help others on the team, they
will help you. If you make it hard for others, they will probably do the same to you. Make
the most of your time in the ward, and in the long run it will be you who gain most benefit.
19. DRESSINGS
Make sure that you have your clinical shirt on, name tag/ID Card, good foot wear, hand
watch with second hand and finally neat dressing before you go to the ward for practical.
20. STAT DOSES OF MEDICATION
Stat dose must be given by you to all patients that you admit.
21. ASSESSMENT:

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 6/41
5
The SMO, Registrar, Clinical lecturer and Nursing Officers will assess you during your ward
practical. Three areas will be assessed.
(a) Knowledge
(b) Practical skills
(c) Attitude
NB: Final clinical Examination is at the end of the rotation.
..............................................................................................................

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 7/41
6
YEAR THREE
CLINICAL PERFORMANCE ASSESSMENT FORM
ATTITUDE ASSESSMENT:
CRITERIA LOW RATING SCALE HIGH RATING
Attitude to work Lazy, not interested 1 2 3 4 5 Industrious, very interested
Desire to learn Not willing to learn 1 2 3 4 5 Very willing to learn
Initiative Not shown at all 1 2 3 4 5 Takes the initiative often
Punctuality Not punctual or constantly
late
1 2 3 4 5 Punctual, on time
Appearance Not appropriately dressed 1 2 3 4 5 Appropriately dressed
Organising ability Either he cannot or will not
motivate and organise others
1 2 3 4 5 Demonstrated ability to
motivate and organise others
Reliability Fails to carry out requests
and instructions
1 2 3 4 5 Intelligently completes all
requests and instructions
Relationship to
patients and
guardians
Arrogant and insensitive 1 2 3 4 5 Cooperative, warm
approachable.
Relationship to
other staff
Arrogant, insensitive does
accept criticism.
1 2 3 4 5 Cooperative approachable.
Use of guide books
and referencebooks.
Fails to use the guide books
in the correct way.
1 2 3 4 5 Intelligently carries out the
management as shown in theguide books and notes.
TOTAL MARKS: …. /50
Signed: ……………………
Doctor/Tutor Date: ………………….
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 8/41 7
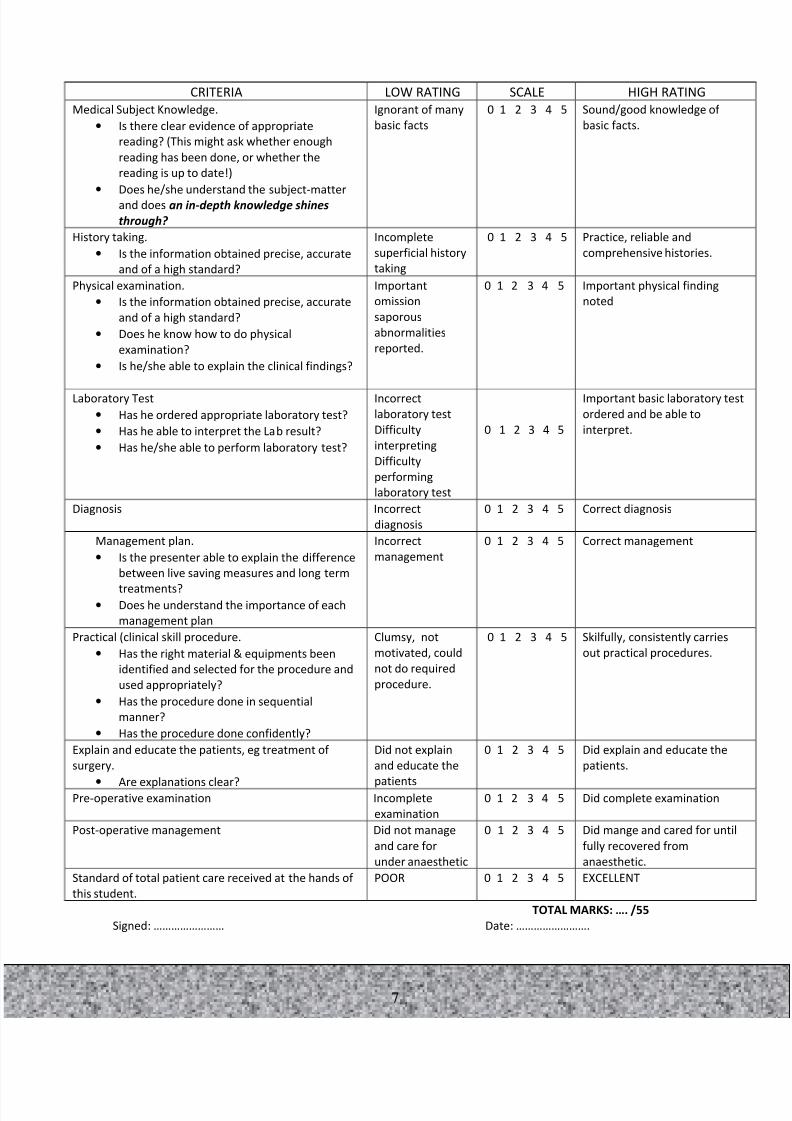
TOTAL MARKS: …. /55
Signed: …………………… Date: …………………….
CRITERIA LOW RATING SCALE HIGH RATING
Medical Subject Knowledge.
• Is there clear evidence of appropriate
reading? (This might ask whether enough
reading has been done, or whether the
reading is up to date!)
• Does he/she understand the subject-matter
and does an in-depth knowledge shines
through?
Ignorant of many
basic facts
0 1 2 3 4 5 Sound/good knowledge of
basic facts.
History taking.
• Is the information obtained precise, accurate
and of a high standard?
Incomplete
superficial history
taking
0 1 2 3 4 5 Practice, reliable and
comprehensive histories.
Physical examination.
• Is the information obtained precise, accurate
and of a high standard?
• Does he know how to do physical
examination?
• Is he/she able to explain the clinical findings?
Important
omission
saporous
abnormalities
reported.
0 1 2 3 4 5 Important physical finding
noted
Laboratory Test
• Has he ordered appropriate laboratory test?
• Has he able to interpret the Lab result?
• Has he/she able to perform laboratory test?
Incorrect
laboratory test
Difficulty
interpreting
Difficulty
performing
laboratory test
0 1 2 3 4 5
Important basic laboratory tes
ordered and be able to
interpret.
Diagnosis Incorrect
diagnosis
0 1 2 3 4 5 Correct diagnosis
Management plan.
• Is the presenter able to explain the difference
between live saving measures and long term
treatments?• Does he understand the importance of each
management plan
Incorrect
management
0 1 2 3 4 5 Correct management
Practical (clinical skill procedure.
• Has the right material & equipments been
identified and selected for the procedure and
used appropriately?
• Has the procedure done in sequential
manner?
• Has the procedure done confidently?
Clumsy, not
motivated, could
not do required
procedure.
0 1 2 3 4 5 Skilfully, consistently carries
out practical procedures.
Explain and educate the patients, eg treatment of
surgery.
• Are explanations clear?
Did not explain
and educate the
patients
0 1 2 3 4 5 Did explain and educate the
patients.
Pre-operative examination Incomplete
examination
0 1 2 3 4 5 Did complete examination
Post-operative management Did not manage
and care for
under anaesthetic
0 1 2 3 4 5 Did mange and cared for until
fully recovered from
anaesthetic.
Standard of total patient care received at the hands of
this student.
POOR 0 1 2 3 4 5 EXCELLENT

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 9/41 8
KEYS:
0. = The student consistently demonstrates an inadequate level of ability with maximum
supervision from staff required (0 marks).
1. = The student usually demonstrates an inadequate level of ability with maximum
supervision from staff required (1 mark).
2. = The student usually demonstrates an adequate level of ability, with moderate
supervision from staff (2 marks).
3. = The student consistently demonstrates a good level of ability, with minimum to
moderate supervision from staff (3 marks)
4. = The student consistently demonstrates an outstanding level of ability, with minimum
supervision from staff (4 marks).
5. = Excellent student with minimal supervision (5 marks)
KNOWLEDGE ASSESSMENT
All marks will be given as a percentage and the final theory mark is also given as a percentage:
TYPE OF ASSESSMENT
No Types Marks %
1 Clinical case write up & Presentation 20%
2
3
Case presentation( Bedside)K & S)
Attitude & Behaviour
30%
10
Total Marks 60
FINAL MARKS:
1. Attitude & Behaviour ________________10%
2. Knowledge & Skills: ________________30%
3. Clinical case write up & Presentation ________________20%
Final Exam; _______________40%
COMMENTS: (if applicable)
_______________________________________________________________________________
Signed: ……………………
Doctor/Tutor Date: …………………….
60%
40%

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 10/41
9
CLINICAL
PRESENTATION ASSESSMENT FORM
Students Name: _____________________________
Year: ________________________
Presentation Skills 0 1 2 3 4
Has the presenter gained the audience’s attention?
Are the objectives clearly stated, and achieved?
Is the presentation carefully planned, well
structured and organised, including the timing?
Is the communication well paced, clear and
effective?
Could notes be taken easily?Are explanations clear?
Is the presenter verbally ¯ uent? Is intonation
varied?
Is the presenter simply reading the information in a
manner suggesting poor preparation?
Is eye contact maintained with the audience?
Are they simplied to illustrate the point or are they
too complex?
Are they left up for long enough to be
interpreted/used?
Is the presenter confident with the material?Are questions confidently answered or is the
presenter uncertain?
Is the presenter enthusiastic?
TOTAL MARKS 52
Academic Content
Has the right material been selected for the
presentation?
Is it all relevant?
Is the vocabulary appropriate and pitched at thecorrect level?
Is there clear evidence of appropriate reading? (This
might ask whether enough reading has been done,
or whether the reading is up to date!)
Are the main issues made clear?
Is the information given precise, accurate and of
a high standard?
Is the information put into a broader context?
Does the presenter understand the subject-matter
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 11/41
10
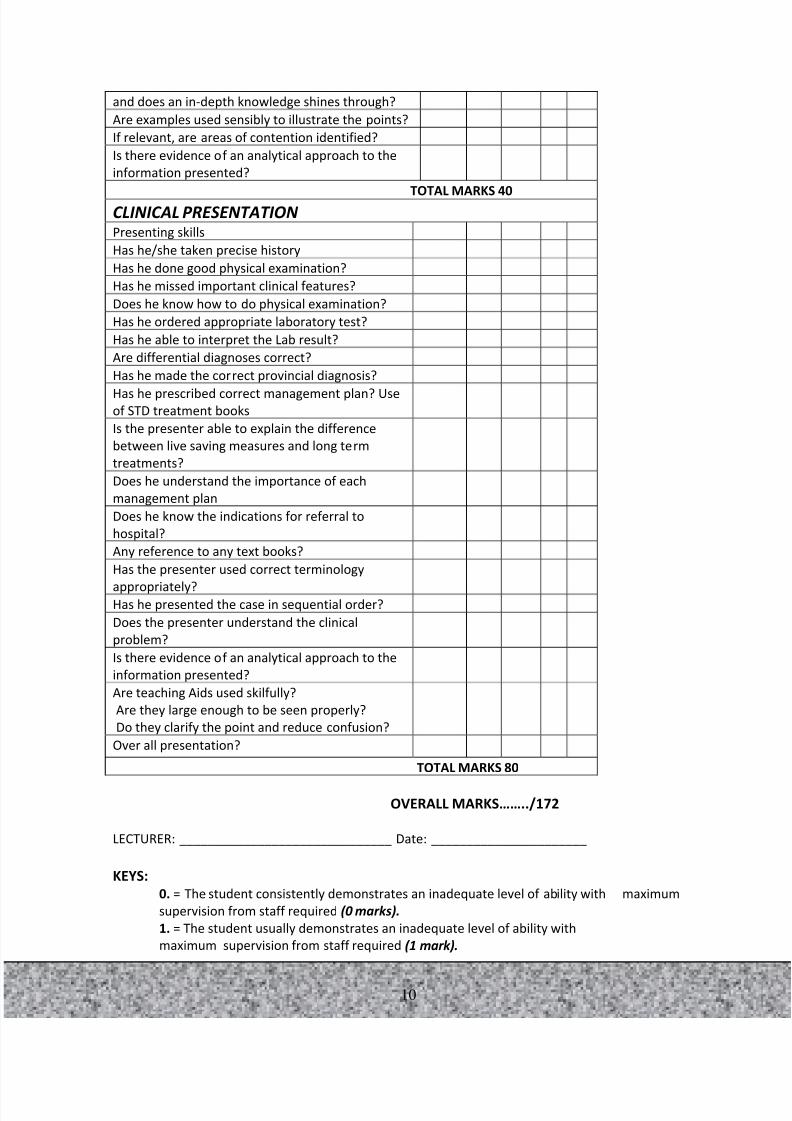
and does an in-depth knowledge shines through?
Are examples used sensibly to illustrate the points?
If relevant, are areas of contention identified?
Is there evidence of an analytical approach to the
information presented?
TOTAL MARKS 40CLINICAL PRESENTATION Presenting skills
Has he/she taken precise history
Has he done good physical examination?
Has he missed important clinical features?
Does he know how to do physical examination?
Has he ordered appropriate laboratory test?
Has he able to interpret the Lab result?
Are differential diagnoses correct?
Has he made the correct provincial diagnosis?
Has he prescribed correct management plan? Useof STD treatment books
Is the presenter able to explain the difference
between live saving measures and long term
treatments?
Does he understand the importance of each
management plan
Does he know the indications for referral to
hospital?
Any reference to any text books?
Has the presenter used correct terminology
appropriately?Has he presented the case in sequential order?
Does the presenter understand the clinical
problem?
Is there evidence of an analytical approach to the
information presented?
Are teaching Aids used skilfully?
Are they large enough to be seen properly?
Do they clarify the point and reduce confusion?
Over all presentation?
TOTAL MARKS 80
OVERALL MARKS……../172
LECTURER: ______________________________ Date: ______________________
KEYS:
0. = The student consistently demonstrates an inadequate level of ability with maximum
supervision from staff required (0 marks).
1. = The student usually demonstrates an inadequate level of ability with
maximum supervision from staff required (1 mark).

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 12/41
11
2. = The student usually demonstrates an adequate level of ability, with moderate
supervision from staff ( 2 marks).
3. = The student consistently demonstrates a good level of ability, with minimum to
moderate supervision from staff (3 marks).
4. = The student consistently demonstrates an outstanding level of ability, with
minimum supervision from staff (4 marks).
...................................................................................................................................................
Weekly Program
DAY MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY
TIME
8am – 10am
Ward round
& Work
Operating
Theatre(G1)
Ward round
& Work
Operating
Theatre(G1)
Ward round
& Work
10am – 11am
Bedside tutorial
Post
Operative
care (G2)
Bedside tutorial
Post Operative
care (G2)11am-12.30pm Dr Kuzma
(Tutorial)LUNCH BREAK
1.30-2.30pm Ward
tutorial/Ward
work
Operating
Theatre
Dr Kuzma
(Tutorial)
Operating
Theatre Tutorial
2.30-4.00pm Lecture HE213
Main Campus
Lecture HE213
Main Campus
Lecture HE213
Main Campus
NB: 1. All patients admitted to the Surgical Ward to be seen by R.H,
students for case studies.
2. Full history and clinical examination must be done on
admission.
3. All treatment ordered by R.H Trainee must be double check
by Clinical Tutor, or Medical Officer.
4. All admission after 4.06pm must be notified to M.O. on
call. This includes weekends.
5. Contact Medical Officers or SMO for any seriously ill patients on admission
immediately.
Dr. Kuzma MR.BOB SIMONSSMO Surgery Clinical Supervisor

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 13/41
12
HE3 CLINICAL ATTACHMENT GROUPING
Accident & Emergency (A) Medicine (B)
NO REG NO FIRST NAME SURE NAME NO REGNO
FIRST NAME SURE NAME
1 4894 Amenda NAWAK 1 4879 Anniephine MARKRAWA
2 5131 Budsy BILIMO 2 4904 Emmanuel TOBIAS
3 5203 Clodia MANORH 3 4874 Cedrick YUWORONONG
4 4898 Hariet TOPA,A 4 5133 Harry JOBBIE
5 5173 Jack WANTUM 5 4902 Jill YOPO
6 4886 Julianne VEOLI 6 5132 Julie YASEPSA
7 4895 Keren KOVE 7 5134 Keroline KOLAPEN
8 4892 Mellonson JOHN 8 5238 Ripson MURA
9 5166 Peter TOWANLOGO 9 5186 Petronella DAVID
10 5152 Renate ZUVANI 10 5184 Samson YATENG
11 5245 Tandam YAMO 11 4875 Tekla JACOB
O & G C Peadiatrics DNO REG NO FIRST NAME SURE NAME NO REG
NO
FIRST NAME SURE NAME
1 4887 Bathseba KEANGA 1 4882 Br.Geoffery LIRIA
2 4925 Christopher APIYEP 2 4893 Clerisa ANALUVA
3 5146 Emsop LUNICA 3 4876 Ezekkial ROKA
4 5163 Helen MIAG 4 4889 Ismael ERI
5 4901 Joe PUTT 5 4881 Jonathan BOMAI
6 4905 Junior KILUWA 6 4884 Keren MIUL
7 4908 Konia FRANCIS 7 Mathew OKSAP
8 5168 Nathan KAWA 8 4897 Nellie AKAI
9 4890 Philomena TATIRETA 9 4896 Pison JAKAWA
10 4885 Sharol ROKENTUO 10 4891 Sharon MAULUDU
11 4872 Verolyne KAVANAMUR 11 5171 Yapi OPI
Surgery (E) NO REG NO FIRST NAME SURE NAME
1 4878 Carolyne HEMO
2 5280 Cliford KOSU
3 4903 Gladlyn MALAK
4 5286 Jacenold PUKEHUN
5 5273 Judith PUGA6 5153 Kenning DABANG
7 4871 Mathilda WALOM
8 5156 Paul DISIN
9 5206 Rachel TUTANA
10 4899 Shirlyna LOWAGIPO
11 5172 Zuaru THEROW

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 14/41
13
NB: EIGHT WEEKS ROTATION IN EACH UNIT
..........................................................................................................................................
WARD DUTY ROSTER
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
8am
To
4pm
NB: After hours and weekend students are not allowed in the hospital wards.
.....................................................................................................................
UNIT TITLE: CLINICAL SURGERY 2
UNIT CODE: HE313
CREDIT POINTS 8 (seven week block rotation at Modilon hospital)
PREREQUISITES: HE221 Surgery I and Anesthetics.
DESCRIPTIONStudents cover this unit by doing seven weeks of fulltime clinical practical (working hours, after
hours and weekends) clinical observations and supervised practical experiences in the accidents and
emergency section of Modilon Hospital. This is supplemented with tutorial sessions with a lecturer
on the university campus. This unit will teach practical skills in diagnosis and management of the
most common surgical problems in Papua New Guinea. Stress will be placed on developing critical
clinical thinking, assessment of patients’ condition and formulating management plan. Studentsreceive theoretical and practical instruction regarding performing basic minor surgical procedures.
LEARNING OUTCOMES
Students are able to:
1. Describe characteristic clinical features of the commonest surgical diseases
2. Collect and critically analyze clinical data and assess patients condition
3. Arrive at most probable diagnosis
4. Formulate therapeutic plan for surgical patients
5. Outline preventive plan for the commonest surgical problems
DATE A & E MEDICINE O & G PEDIATRICS SURGERY COMMENTS
A B C D E
B C D E A
C D E A B
SEMESTER BREAK
D E A B CE A B C D

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 15/41
14
6. Demonstrate understanding and application of basic minor surgical procedures and perform
some of minor surgical procedures
CONTENT Week 1
Ward rounds, in bed teachingPresentation and discussion:
• Assessment and primary management of head trauma
• Management of patients with spinal injury
• Diagnosis and primary management of chest trauma
History taking and characteristic of surgical examination
Tasks: Admit a surgical patient, report findings from history taking and examination history,
Performing surgical nursing procedures: insertion of I.V. cannula, parenteral drugapplication,
NGT insertion, dressing etc.
Week 2
Ward rounds, in bed teachingPresentation and discussion:
• Abdominal trauma, post spleenectomy after care
• Burns management, skin graft
• Diagnosis and primary management of limb-threatening injuries
Tasks: Admit a surgical patient, report findings from history taking and examination history,
formulating management plan
Performing surgical nursing procedures: insertion of I.V. cannula, parenteral drug application,
NGT insertion, dressing etc.
Week 3Ward rounds, in bed teaching
Presentation and discussion:
• Reduction of commonest dislocations
• Fractures of the upper limb, Hand injuries
• Fractures of the lower limb, prevention and management of complications associated with
POP
Tasks: Admit a surgical patient, report findings from history taking and examination history,\
writing discharges, formulating management plan
Performing surgical minor procedures: application of skin traction, application of POP.
Practical test: Write a surgical patient history, differential diagnosis and management plan
Week 4Ward rounds, in bed teaching
Presentation and discussion:
• Hernias – differential diagnosis, strangulation, aftercare
• • Acute appendicitis – differential diagnosis
• Bowel obstruction
Tasks: Admit a surgical patient, report findings from history taking and examination history,
writing discharges, formulating management plan

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 16/41
15
Performing surgical procedures: insertion of I.V. cannula, parenteral drug application, NGT
insertion, dressing etc.
Week 5
Ward rounds, in bed teaching
Presentation and discussion:• Urological emergencies
• Rectal diseases, haemorrhoids
• Breast cancer
Tasks: Admit a surgical patient, report findings from history taking and examination history,
writing discharges, formulating management plan
Performing surgical minor procedures and nursing procedures: insertion of I.V. cannula,
parenteral drug application, NGT insertion, dressing etc.
Week 6
Ward rounds, in bed teaching
Presentation and discussion:• Prevention of Hospital cross-infections, aseptic technique
• Rehabilitation of surgical patients
Tasks: Admit a surgical patient, report findings from history taking and examination history,
writing discharges, formulating management plan
Practical exam:
Collect clinical data
Conduct differential diagnosis with formulating most likely diagnosis
Formulate management plan including discharge instruction and possible preventive measures
Comment on the outcome
During this practical placement a student should
• Assist surgeon working in the surgical clinic (at least twice)
• Observe and assist work at the Operating Theatre (at least 6 times)
Week 7
Ward rounds, in bed teaching
Presentation and discussion:
• Prevention of Hospital cross-infections, aseptic technique
• Rehabilitation of surgical patients
Tasks: Admit a surgical patient, report findings from history taking and examination
history, writing discharges, formulating management plan
Practical exam:Collect clinical data
Conduct differential diagnosis with formulating most likely diagnosis
Formulate management plan including discharge instruction and possible preventive
measures
Comment on the outcome
During this practical placement a student should
• Assist surgeon working in the surgical clinic (at least twice)
• Observe and assist work at the Operating Theatre (at least 6 times)

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 17/41
16
ASSESSMENTS
Assignment 1: Clinical case write up
Task: Research project and presentation
Criteria: Case write up 10% and presentation 10%
Length: Up to 1,500 words and 30 minutes presentations
Weight: 20%
Assignment 2: Clinical case presentation(bedside)skills
Task: Perform all clinical requirements
Criteria: The extent to which students can demonstrate knowledge, skills and understanding
of clinical surgery
Length: 7 weeks
Weight: 30%
Assignment 3: Attitude & behaviour
Task: Clinical practical attachment in hospital
Criteria: The extent to which students must Demonstrated ability to carry out responsibility,
take inititive, and committments during clinical attachment.
Length: 7 weeks
Weight: 10%
Assignment 3: End of semester examTask: Written exam
Criteria: The extent to which students can demonstrate knowledge and understanding of
clinical surgery
Length: 2 hours
Weight: 40%
REFERENCESAdams JC, Hamblen DL. 1999. Outline of Fractures. London: Churchill Livingstone.
Adams JC, Hamblen DL. 2001. Outline of Orthopedics. London: Churchill Livingstone.
Australian First Aid, 1989, 2nd EDN, St. John Ambulance Australia, Canberra
Kuzma J. 2006. Surgery for primary health care workers in PNG, DWU Press. Madang
Simon B. 1998. Anaesthesia for HEO. 3rd Edn, DWU, Madang
Watters DAK, Wilson IH, Leaver RJ. 2004. A Care for critically ill patient in the tropics.
SUPERVISOR WEEKLY PROGRAM

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 18/41
17
Attendance record
NB: HE 213 . Pharmacology lecture for HE 2 Class at the main campus.
...............................................................................................................................................
DAY MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY
TIME
8am – 10am Ward round Operating
Theatre
Ward round
Operating
Theatre
Ward round
10.30am – 12MD
Ward Tutorial
(HE 313)
Ward Tutorial
(HE 313)
Ward Tutorial
(HE 313)
TEA BREAK
10.30am –12MDWard Tutorial
(HE 313)
Operating
Theatre
Ward Tutorial
(HE 313)
Operating
Theatre
Ward Tutorial
(HE 313)
LUNCH BREAK
14.30pm – 15.30pm Lecture
HE213 MM2
Lecture
HE213 MM2
Lecture
HE213 MM2
Operating
Theatre
R415 – 14.30
Tutorial
HE311
R415
1.30-2.30pm
DATES COMMENTS
NAME

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 19/41
18
History Taking and Clinical Examination
DiagnosisIn general, diagnosis (plural diagnoses) has two distinct dictionary definitions. The first
definition is "the recognition of a disease or condition by its outward signs and
symptoms", while the second definition is "the analysis of the underlying
physiological/biochemical cause(s) of a disease or condition".
In medicine, diagnosis or diagnostics is the process of identifying a medical condition or
disease by its signs, symptoms, and from the results of various diagnostic procedures.
The conclusion reached through this process is called a diagnosis. The term "diagnostic
criteria" designates the combination of symptoms which allows the doctor to ascertain the
diagnosis of the respective disease.
Typically, someone with abnormal symptoms will consult a physician, who will then
obtain a history of the patient's illness and examine him for signs of disease. The
physician will formulate a hypothesis of likely diagnoses and in many cases will obtainfurther testing to confirm or clarify the diagnosis before providing treatment.
Medical tests commonly performed are measuring blood pressure, checking the pulse
rate, listening to the heart with a stethoscope, urine tests, fecal tests, saliva tests, blood
tests, medical imaging, electrocardiogram, hydrogen breath test and occasionally biopsy.
Relationship of diagnosis to medical practiceA physician's job is to know the human body and its functions in terms of normality
(homeostasis). The four cornerstones of diagnostic medicine, each essential for
understanding homeostasis, are: anatomy (the structure of the human body), physiology(how the body works), pathology (what can go wrong with the anatomy and physiology)
and psychology (thought and behavior). Once the doctor knows what is normal and can
measure the patient's current condition against those norms, she or he can then determine
the patient's particular departure from homeostasis and the degree of departure. This is
called the diagnosis. Once a diagnosis has been reached, the doctor is able to propose a
management plan, which will include treatment as well as plans for follow-up. From this
point on, in addition to treating the patient's condition, the doctor educates the patient
about the causes, progression, outcomes, and possible treatments of his ailments, as well
as providing advice for maintaining health.
Diagnostic procedureDiagnosis is a fluid process in which the physician responds to information garnered
from the patient and others, from a physical examination of the patient, and from medical
tests performed upon the patient.
The doctor then conducts a physical examination of the patient, studies the patient's
medical record, and asks further questions as he goes, in an effort to rule out as many of
the potential conditions as possible. When the list is narrowed down to a single condition,
this is called the differential diagnosis, and provides the basis for a hypothesis of what is
ailing the patient.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 20/41
19
Once the physician has completed the diagnosis, he explains the prognosis to the patient
and proposes a treatment plan which includes therapy and follow-up (further
consultations and tests to monitor the condition and the progress of the treatment, if
needed), usually according to the guideline provided by the medical field on the treatment
of the particular illness.
Treatment itself may indicate a need for review of the diagnosis if there is a failure to
respond to treatments that would normally work.
Medical historyThe medical history or anamnesis of a patient is information gained by a physician or
other healthcare professional by asking specific questions, either of the patient or of other
people who know the person and can give suitable information (in this case, it is
sometimes called heteroanamnesis), with the aim of obtaining information useful in
formulating a diagnosis and providing medical care to the patient. This kind of
information is called the symptoms, in contrast with clinical signs, which are ascertained
by direct examination.
The information obtained in this way, together with clinical examination, enables the
physician to form a diagnosis and treatment plan. If a diagnosis cannot be made then a
provisional diagnosis may be formulated, and other possibilities (the differential
diagnosis) may be added, by convention listed in order of likelihood. The treatment plan
may then include further investigations to try and clarify the diagnosis.
A physician typically asks questions to obtain the following information about the
patient:
Identification and demographics: The name, age, height, weight.
The "chief complaint (CC)" — the major health problem or concern, and its time
course.
History of present illless (HOPI) - details about the complaints enumerated in the
CC.
History of past illness (HPI)(including major illnesses, any previous
surgery/operations, any current ongoing illness, eg diabetes)
Review of systems(ROS) Systematic questioning about different organ systems
Family diseases
Childhood diseases
Social history - including living arrangements, occupation, drug use (including
tobacco, alcohol, other recreational drug use), recent foreign travel and exposure
to environmental pathogens through recreational activities or pets.
Regular medications (including those prescribed by doctors, and others obtained
over the counter or alternative medicine)
Allergies Sex life, obstetric/gynecological history and so on as appropriate.
History-taking may be comprehensive history taking (a fixed and extensive set of
questions are asked, as practised only by medical students) or iterative hypothesis testing
(questions are limited and adapted to rule in or out likely diagnoses based on information
already obtained, as practised by busy clinicians).

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 21/41
20
SymptomStrictly, a symptom is a sensation or change in health function experienced by a
patient. Thus, symptoms may be loosely classified as strong, mild or weak. In
this, medically correct, sense of the word, it is a subjective report, as opposed to a
sign, which is objective evidence of the presence of a disease or disorder.
Medical signSimply, a sign is an indication of some fact or quality; and, in everyday English, a
medical sign is an "objective" indication of some medical fact or quality that is detected
by a physician during a physical examination of a patient—such as elevated blood
pressure.
Signs versus symptomsSigns are commonly distinguished from symptoms as follows: a symptom is something
abnormal, that is relevant to disease, experienced by a patient, whilst a sign is something
abnormal, that is relevant to disease, discovered by the physician during his examinationof the patient:
…a sign is an objective symptom of a disease; a symptom is a subjective sign of
disease.
Types of signsMedical signs may be classified by the type of inference that may be made from their
presence, for example:
Prognostic signs (from progignokein, προγιγνωσκειν, "to know beforehand"):
signs that indicate the outcome of the current bodily state of the patient (i.e.,
rather than indicating the name of the disease). Prognostic signs always point tothe future.
Anamnestic signs "able to recall to mind"):
signs that (taking into account the current state of a patient's body), indicate the
past existence of a certain disease or condition. Anamnestic signs always point to
the past .
Diagnostic signs "able to distinguish"): signs
that lead to the recognition and identification of a disease (i.e., they indicate the
name of the disease).
Pathognomonic signs "skilled in diagnosis", "judge"): the particular signs whose presence means,
beyond any doubt, that a particular disease is present. They represent a marked intensification of adiagnostic sign. Singular pathognonomic signs are relatively uncommon.
[Thus] a symptom is a phenomenon, caused by an illness and observable directly
in experience. We may speak of it as a manifestation of illness. When the
observer reflects on that phenomenon and uses it as a base for further inferences,
then that symptom is transformed into a sign. As a sign it points beyond itself —
perhaps to the present illness, or to the past or to the future. That to which a sign
points is part of its meaning, which may be rich and complex, or scanty, or any
gradation in between.
In medicine, then, a sign is thus a phenomenon from which we may get a message,

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 22/41
21
a message that tells us something about the patient or the disease. A phenomenon
or observation that does not convey a message is not a sign. The distinction
between signs and symptom rests
Signs as tests
In some senses, the process of diagnosis is always a matter of assessing the likelihood that a given condition is present in the patient. In a patient who presents with haemoptysis
(coughing up blood), the haemoptysis is very much more likely to be caused by
respiratory disease than by the patient having broken their toe. Each question in the
history taking allows the medical practitioner to narrow down their view of the cause of
the symptom, testing and building up their hypotheses as they go along.
Examination, which is essentially looking for clinical signs, allows the medical
practitioner to see if there is evidence in the patient's body to support their hypotheses
about the disease that might be present.
A patient who has given a good story to support a diagnosis of tuberculosis might be
found, on examination, to show signs that lead the practitioner away from that diagnosis
and more towards sarcoidosis, for example. Examination for signs tests the practitioner's
hypotheses, and each time a sign is found that supports a given diagnosis, that diagnosis
becomes more likely.
Special tests (blood tests, radiology, scans, a biopsy, etc.) also allow a hypothesis to be
tested. These special tests are also said to show signs in a clinical sense. Again, a test can
be considered pathognonomic for a given disease, but in that case the test is generally
said to be "diagnostic" of that disease rather than pathognonomic. An example would be
a history of a fall from a height, followed by a lot of pain in the leg. The signs (a swollen,
tender, distorted lower leg) are only very strongly suggestive of a fracture; it might not
actually be broken, and even if it is, the particular kind of fracture and its degree of
dislocation need to be known, so the practitioner orders an x-ray. The x-ray film shows a
fractured tibia, so the film is said to be diagnostic of the fracture.
Examples of signs Ascites (fluid in the abdomen)
Cachexia (loss of weight, muscle
atrophy)
Caput medusae (dilated umbilical
veins)
Clubbing (deformed nails)
Cough
Death rattle ( last moments of life ina person/animal)
Gynecomastia (excessive breast
tissue in males)
Hemoptysis (blood-stained sputum)
Hepatosplenomegaly (enlarged liver
and spleen)
Icterus ("jaundice")
Lymphadenopathy (swollen lymph
nodes)

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 23/41
22
Palmar erythema (reddening of
Physical examinationPhysical examination or clinical examination is the process by which a health care
provider investigates the body of a patient for signs of disease. It generally follows the
taking of the medical history — an account of the symptoms as experienced by thepatient. Together with the medical history, the physical examination aids in determining
the correct diagnosis and devising the treatment plan
Vital SignsTemperature
Temperature recording gives an indication of core body temperature which is normally
tightly controlled (thermoregulation) as it affects the rate of chemical reactions.
The main reason for checking body temperature is to solicit any signs of systemic
infection or inflammation in the presence of a fever
Blood pressureThe blood pressure is recorded as two readings, a high systolic pressure which is the
maximal contraction of the heart and the lower diastolic or resting pressure. Usually the
blood pressure is taken in the right arm unless there is some damage to the arm.
PulseThe pulse is the physical expansion of the artery. Its rate is usually measured either at the
wrist or the ankle and is recorded as beats per minute. The pulse commonly is taken is the
radial artery at the wrist. Sometimes the pulse cannot be taken at the wrist and is taken at
the elbow (brachial artery), at the neck against the carotid artery (carotid pulse), behind
the knee (popliteal artery), or in the foot dorsalis pedis or posterior tibial arteries. The
pulse rate can also be measured by listening directly to the heartbeat using a stethoscope.
The pulse varies with age. A newborn or infant can have a heart rate of about 130-150
beats per minute. A toddler's heart will beat about 100-120 times per minute, an older
child's heartbeat is around 90-110 beats per minute, adolescents around 80-100 beats per
minute, and adults pulse rate is anywhere between 50 and 80 beats per minute.
Respiratory rate
Varies with age, but the normal reference range is 16-20 breaths/minute.
General appearanceObvious apparent features as the patient enters the consulting room and in the course of
taking the history (e.g. mobility problem or deafness)
JACCOL, a mnemonic for Jaundice, suggestion of Anaemia (pale colour of skin
or conjunctiva), Cyanosis (blue coloration of lips or extremities), Clubbing
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 24/41
23
Inspection (medicine)
In medicine, inspection (Latin word "Inspectio" or the act of beholding) is the thorough
and unhurried visualization of the client. This requires the use of the naked eye.
During inspection, the examiner observes:
External signs:
Body features and symmetry appearance
Nutritional state or weight
Skin color
Frequency and volume of breaths during respiration
Movement of the abdomen and each side of the chest during respiration
Hair distribution
divercation of recti muscle
umbilicus (site-shape-color- infiltration)
Gait and manner of speaking
Gross Deviation:
Abnormal contour
Scars and striae
Visible masses
Discoloration
Swelling
Tremor
In medical practice, inspection is however not limited to visual information alone.
Inspection also involves:
Listening to any sounds emanating from the client
Odors that may be present
Palpation
Palpation is a method of examination in which the examiner feels an object to determine
its size, shape, firmness, or location. Medical doctors, for example, may palpate body
parts to check for swelling or disease.
Percussion (medicine)
Percussion is a method used by a clinican to find out about the changes in the thorax or
abdomen. It is done by tapping on a surface to determine the underlying structure. It is
one of the four methods of clinical examination: inspection, palpation, percussion and
auscultation. It is done with the middle finger of right hand tapping on the middle finger
of the left hand, which is positioned with the whole palm on the body.
Auscultation
Auscultation is the technical term for listening to the internal sounds of the body, usually
using a stethoscope. Auscultation is normally performed for the purposes of examiningthe circulatory system and respiratory system (heart sounds and breath sounds), as well as
the gastrointestinal system (bowel sounds). Auscultation is a skill that requires substantial clinical
experience, and good listening skills.
……………………………………………………………………………………………………………………………..

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 25/41
24
Assessment Task(Case presentation)
Presentation format.
Comprehensive format headed with;
Definition (Topic) ( 5 marks)
Epidemiology
The epidemiology describes the incidence and prevalence of disease. (5 marks)
Pathology
The pathology relates to the Aetiology and pathogenesis of disease. (5 marks)
Scope of disease (complications)
Disease can present as primary condition or as a result of a secondary complication.
(5 marks)
Clinical features (5 marks)
This relates mainly to symptoms and examination features of disease and any other associated
complications.
investigations,Lab Test (5 marks)
Further investigations refer to investigations not usually performed for all patients with clinical
features suggestive of the underlying disease, as well as more invasive or specific investigations for
patients with specific indications or associated complications.
Initial management (5 marks)Initial management provides information and instruction on simple first line measures on
the management of disease or the important first step of emergency management.
Medical management (5 marks)
Medical management refers to all non surgical management and usually describes risk-factor
modification and drug treatment, although it may include any other intervention performed by
physician.
Surgical management (5 marks)
Surgical management describes the surgical management, procedure, result and complications,
usually in sufficient detail to obtain informed consent.
Indication for referral (5 marks)
What are the indications for referral from Health centre/District hospital
Prognosis (5 marks)
The prognosis is used to describe the natural history of untreated disease as well as the result of
treatment.
References. (5 marks)

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 26/41
\25
.................................................................................................................
REFERENCING PROCEDURES
Introductory comments
In academic writing, an author almost always gets information from the writings of others. It is
essential that these sources be acknowledged. These acknowledgements provide evidence of
professional reading and give support to the points being made. University students are expected to
demonstrate this practice.
There is no one simple internationally used set of referencing procedures. This can be seen as you
look at referencing styles in different academic publications. The style being described in these
notes uses the author-date format from the Style Manual (Australian Government Publishing Service
1994). This is used by public servants and also by many publishers, authors, editors, businesses,
private individuals and educational and other institutions in Australia.
Consistency in how you apply a referencing style is important. You may use a recognised style otherthan the one in the AGPS Style Manual but the important thing is to use it consistently.
A. Reference list at end of text
List in alphabetical order by the surname of the author. If typing, use italics for titles of books and
journals. Do not underline as this covers the down strokes of letters and slows down reading
comprehension. Only in hand-written work is underlining used to indicate book and journal titles.
1.1 One author
Marsh, C.J. 1992, Key Concepts for Understanding Curriculum, The Falmer Press, London.
1.2 Two or more authorsHuling, L., Hall, G., Hord, S. & Rutherford, W. 1983, A Multi-Dimensional Approach for Assessing
Implementation Success, Southwest Educational Development Laboratory, Austin, Texas.
1.3 Edition of a book
Barry, K. & King, L. 1998, Beginning Teaching and Beyond, 3rd
edn, Social Science Press, Australia.
1.4 One editor
Guthrie, G. (ed.) 1987, Basic Research Techniques, Report No. 55 Educational Research Unit,
University of Papua New Guinea.
1.5 Two editors
Pigdon, K. & Woolley, M. (eds) 1992, The Big Picture: Integrating Children’s Learning, Eleanor
Curtain, Armadale.
1.6 Chapter or article in a collection
Smith, Geoffrey 1972, ‘Education, history and development’, in Encyclopaedia of Papua New Guinea,
Peter Ryan (ed.), Melbourne University Press, Australia, pp. 315-330.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 27/41
\26
1.7 Article from a journal
N’Drawii, J. 2003, ‘Social problems faced by female student teachers at Madang Teachers College’,
MTC Search, vol. 6, no. 4, pp. 6-10.
1.8 Article from a newspaper with known author
Kapigeno, J. 2004, ‘Schools warned against sending children home’, Weekend National, 13-15 February, p. 6.
1.9 Article from a newspaper, author not indicated
Weekend National, 13-15 February 2004, ‘Lae tax officer charged with K26,000 fraud’, p. 7.
1.10 Paper presented at a meeting, seminar or conference
Tivinarlik, A. & Nongkas, C. 2002, Catholic leadership in Papua New Guinea secondary schools,
paper presented at the Australian Catholic University conference on leadership.
1.11 Unpublished thesis
Tivinarlik, A. 2000, Leadership styles of New Ireland high school administrators: a Papua New Guineastudy , PhD thesis, University of Iowa, USA.
1.12 Dictionary, thesaurus, atlas. Bible etc
The Macquarie Dictionary 1991, 2nd
edn, Macquarie University, Australia.
1.13 Two or more publication by same author in same year
Department of Education 2000a, National Education Plan 1995-2004 Update 1, Waigani, Papua New
Guinea.
Department of Education 2000b, Primary Education Handbook , 2nd
edn, Waigani, Papua New
Guinea.
1.14 Films and video recordings – title, format, date
First Contact (video recording) 1981.
Haus and Home (television production) 2 March 2004, EMTV.
1.15 author, date, title, www address
Curriculum Reform Implementation Project 2004, ‘Upper primary student resources for PNG
Department of Education, www.pngcurriculumreform.ac.pg, accessed 12 June 2007.
B. In-text references
2.1 author-date, and sometimes page
Matane (1986) was the first to suggest a philosophical change.
Matane (1986, p. 4) stressed the importance of integral human development.Research into leadership styles (Tivinarlik & Nongkas 2002) found …
Several studies (Dorrow & O’Neal 1979, Mullaney 1978, Talpers 1981) found …
2.2 et al (and others) for three or more authors
The concerns-based adoption model (Huling, et al. 1983) was trialled widely.
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 28/41
\27
2.3 Quotation – less than three lines – single quotation marks
The Ministerial Committee argued that ‘education should not be considered as a passport to a paid
job’ (Matane 1986, p. 1) and described how attitudes of educators, parents and young people must
change.
2.4 Citation in text – more than three lines– indent, block, no quotation marks
Josephs (2000, p. 29) argued that:
The greatest single factor affecting quality is the teacher. Pre-service and in-service
opportunities for teachers are important indicators, but for some children the
presence of a teacher in the classroom would be a welcome bonus. It is common
knowledge that some teachers absent themselves from classrooms regularly and
without authority.
C. Some other points concerning academic writing
3.1 Abbreviations contain the initial letter and other letters of a word or words but not the final
letter.
vol. no. p. pp. i.e. e.g. ed.
Abbreviations using capital letters are written without full stops.PhD PNG UPNG PO UNESCO
3.2 A contraction has at least the first and last letter of a word. It is written without a full stop
eds (editors), edn (edition), Dept (Department), Mr (Mister), Dr (Doctor)
3.3 Non-discriminatory and inclusive language is to be used. Avoid using ‘man’ in a generic sense
and use alternatives such as headteacher, police officer, chairperson etc. Avoid the awkward use of
he/she, him/her by rewriting the sentence in the plural.
3.4 Use full stops at the end of sentences but not headings and sub-headings. Use single quotation
marks to enclose exact words of a writer or speaker. Do not hyphenate words at the ends of lines,put the whole word on the next line.
3.5 Lists. A colon is used to introduce a list. Punctuation is not needed at the ends of items in a list.
The last listed item is followed by a full stop. Avoid unnecessary numbering in lists unless it is
needed to show order, e.g. to make something.
3.6 Use headings and sub-headings to organize your text. Avoid creating sub-subheadings.
3.7 The first time an acronym is used, give the words in full followed by the letters in parentheses,
e.g. Divine Word University (DWU). After that, the acronym can be used by itself.
Approved by DWU Academ
…………………………………………………………………………………………………………………………
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 29/41
\28
ASSESSMENT COVER-SHEET
DIVINE WORD UNVIVERSITY
Degree Rural Health
ASSESSMENT COVER-SHEET
STUDENT NAME: DUE DATE
UNIT TITLE: UNIT CODE:
ASSESSMENT TITLE:
LECTURER:
Your assessment should meet the following requirements. Please confirm by ticking boxes before
submitting your assessment. Assessment presentation is your responsibility.
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 30/41
\29
Your name and the essay title as footer on
each page
Assessment is presented on A4 paper
Printed single sided, page numbers on
bottom right corner
Pages firmly stapled together
Top & bottom margins 2cms minimum
Left margin 4cm & right margin 3cm
Double or 1½ line spacing
Text left justified
Typed, spell checked and paginated
Referencing is consistent and
thorough
Declaration below is completed
Copy retained by student
Declaration:
This essay / assessment is all my own work, except where duly acknowledged. Ideas taken from
other sources are indicated with footnotes; words or passages taken from other sources are
marked with quotation marks, citations and appropriate references.
Signed: Date:
.............................................................................………………….........………………...........
OPERATION NOTES
Name: ……………………………Age/Sex………………Admission No……..……...
Date: ……………………….
Operative Diagnosis: …………………………
Indications: …………………………………...
Operation: ……………………………………
SURGEON: …………………………….. ANAESTHETIST: …………………
Incision/Approach:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Finding:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 31/41
\30
Procedure:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Post operative instruction:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
...............................................................................................................................
REFERRAL FORM
Bundi Health Centre
P.O.Box 10
BUNDI
Madang Province
20th February 2011
To: ________________________
________________________
________________________
________________________
Dear Sir,
We are referring you ………………………………age of 20 years for your help and attention.
Clinical Details:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 32/41
\31
We should be grateful if you would kindly take over the management of this patient, and
let us know in due course of the patient’s progress.
Yours sincerely,
______________________
Health Extension Officer (OIC)
..............................................................................
CODE OF ETHICS
The following code of ethics has been approved by the Health Extension Officers
Association. It is an attempt to help members of the association with common ethicalproblems which may be expected to arise in the course of our members’ professional
practice.
Members who may be confronted with ethical problems requiring individual consideration,
or if he/she is in doubt about the course of action to take in any professional difficulty,
he/she should seek proper assistance through the Secretary, Papua New Guinea H.E.O.
Association.
Disciplinary matters over registration of H.E.O.’s is the responsibility of the P.N.G. Medical
Board.
The H.E.O. Association has the responsibility of informing its members about their duties
and the ethical demands placed upon them by the H.E.O. profession. “Professionalmisconduct” should be interpreted as follows:
“An H.E.O. who, in the course of professional practice, has done something which will bereasonably regarded as disgraceful by other members of the H.E.O. profession with a high
standard of behavior shall be regarded as having committed professional misconduct.”
GENERAL PRINCIPLE
Members of the H.E.O. profession accept the following principles for which they strive:
To observe truth and non-violence at all times and to be dedicated to the well being
of his/her country and fellow citizens.
To actively support moves to change policies that will improve the health status of
people of Papua New Guinea, especially those living in the rural areas.
To render service in activities other than health, that may be carried out withincommunities from time to time to establish a society where justice and equality shall
prevail.
To realize and work towards the ideal that maximum well being and happiness of
humanity can only be achieved when within communities people are non-violently
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 33/41
\32
organized as self-reliant rural and urban communities where scientific and other
values are harmoniously combined for the welfare of all.
1. DUTIES OF H.E.O.’s IN GENERAL
1.1. An H.E.O. must maintain the highest stand and of professional conduct
towards individuals and society
1.2. An H.E.O. must regard his/her profession as a service to individuals and
society and not simply a profit making organization. To this end, an H.E.O
must not allow himself/herself to be influenced by how much he/she can get,
but rather, how much and what he/she can give.
1.3. It is unethical for an H.E.O. to receive or demand to be given in connection
with services he/she give to a patient or community other than paid to
him/her by the employing agency.
1.4. Under no circumstances is an H.E.O. to do anything that would weaken the
mental or physical resistance of a human being except from strictlytherapeutic or prophylactic indications imposed in the interest of the patient.
1.5. When an H.E.O. is called upon to give evidence or a certificate, he/she should
only state the facts that can be proved.
1.6. It is the responsibility of the H.E.O. to assure himself/herself of the
competence of nurses, C.H.W’s and other auxiliary staff.
1.7. An H.E.O. must not exercise favoritism to any one individual on the staff
when dealing with disciplinary matters.
2. DUTIES OF H.E.O.’s TO THE SICK
2.1 An H.E.O. must always remember the importance of preserving life from the
foetus until death.
2.2 No matter who the patient is, or how sick he is, an H.E.O. must give his/her
best care and attention to his/her patient. An H.E.O. must never discriminate
on the basis of race, religion, tribe, social position, political party or ability topay, suffer from pain of body and mind when he is under the care of an H.E.O.
2.3 An H.E.O. must keep in mind that patients may change their attitudes
because of diseases he may acquire, becoming too demanding, mentally
unstable and un-cooperative. In all these circumstances, and H.E.O. must always keep calm and be polite and friendly to the patient.
2.4 An H.E.O. must accept consequences of his/her professional judgment or
practice and report to the appropriate authority at once when mistakes are
being made.
2.5 An H.E.O. owes to his/her patient complete loyalty and all the resources of
his /her knowledge. It only appropriate therefore when an examination or
treatment is beyond his/her capacity, that he/she should consult another
H.E.O. who may have the necessary ability, seek the opinion of a doctor or
transfer the patient to the hospital where a doctor could take over theresponsibility of caring of the patient.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 34/41
\33
2.6 An H.E.O. because he/she owes his/her knowledge to the patient, must keep
all information which has been disclosed to him/her by the patient
absolutely confidential. An H.E.O. must never betray the confidence
entrusted to him/her by the patient.
2.7 Occasionally, an H.E.O. will be permitted to break the bond of secrecy
without the specific consent of the patient.
a: In the interest of the patient, his spouse and H.E.O.
An H.E.O. may discuss with a wife or a husband the condition of a marriage
partner. This is a day to day occurrence. The H.E.O.’s common sense tells
him/her what information can be disclosed.
b: Statutory requirements
There are certain cases where an H.E.O. is required by law to disclose
confidential information about a patient. These cases are few and clearly
defined. For instance, H.E.O.’s are required by law to notify the Department
of Health in cases of certain diseases, mainly the communicable diseases.
c: The medical witness
An H.E.O. may be required by law to disclose confidential information
concerning his/her patients on the direction of a court of law. However, the
H.E.O. may express reluctance to divulge certain information. He would be
guided by the decision of the judge.
d: Danger to society
The H.E.O. may feel duty bound to disclose confidential information about a
patient who is in danger to a society. Such occasions are rare and are
necessitated only by the public safety. For example, the uncontrolled
epileptic who refuses to surrender his/her driving license cannot be
expected to be entitled to the confidence enjoyed by other patients. The
H.E.O. may then pass the necessary information on to the appropriate
authorities.
e: Cruelty to a child
When cruelty to a child is discovered during course of professional practice,the H.E.O. should not hesitate to bring the information to the attention of the
appropriate authorities.
f: Criminal cases
No H.E.O. must withhold knowledge of marked crime. Secrecy is certainly not
desirable where a patient appears to die of a criminal act (e.g. poisoning,maltreatment). A death certificate should not be signed in these cases until
permission to do so has been given by the coroner. On the other hand, an
H.E.O. should not b agent of the police, or a private detective. An H.E.O.
should be guided by his/her conscience as to when it is essential that he/she
reveal information obtained in confidence from a patient.
2.8 Consent of examination and treatment
a: No one is obliged to submit himself/herself to examination or treatment except in a few obvious cases where the law requires it. an H.E.O. should
8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 35/41
\34
remember that it is the patient’s consent which makes it lawful for the H.E.O.
to examine or treat him/her.
b: On most occasions, consent for treatment and examination is implied. This is
when the patient does not express his/her consent, but it is implied by
his/her action in submitting to examination or treatment.
c: Expressed consent
Occasionally, it is desirable that the patient gives consent in more positive
terms. This is required when procedures requiring loss of the patient’s
consciousness are indicated. On all these occasions, patients consent can be
expressed verbally or in writing. An H.E.O. is advised to seek writtenauthority from the patient as this carries more authority and permanence.
A verbal consent, if appropriate, must be given in the presence of a reliable
witness who can be called upon to confirm it. a consent should always be
obtained before pre-medication is given. Before an H.E.O. examines a female
patient, he must always have a second female person present.
d: The injured, unconscious patient
whatever his age, the unconscious patient should be treated immediately in
whatever way is necessary, without wasting time in seeking the consent of
relatives, which in any event would probably have no legal validity.
e: The mentally incapable
A mental patient legally detained has been deprived of his/her rights to
decide for himself/herself and the H.E.O. in whose care he/she has been
placed, may authorize procedures he/she thinks necessary for the patient’s
welfare.
f: The young
Only in the very young, thus incapable of providing their own consent, has
the consent of the parents or guardians real validity and this should obtained
if possible. At the age of 16 years, a person of normal intelligence should
make his/her own decisions in regard to treatment or examination should becarried out on the basis of the young person’s consent alone.
g: Blood transfusion
if an adult adamantly refuses his consent to blood transfusion (e.g. on the
grounds of religious conviction), even if his/her life would be imperiled if transfusion were withheld, such an adult should have his/her beliefs
respected. The H.E.O. should refer the matter to a doctor who will decide
appropriate courses of action. In the case of a child under 16 years whose
legal guardian objects to blood transfusion of the child and transfusion is
definitely indicated for the child (e.g. following an accident to the child), then
transfusion should not be withheld.
h: Contraception
The introduction of an IUCD into a married woman without her husband’s
consent, unless done for the health and safety of the wife, is unwise. The

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 36/41
\35
husband may thus be deprived of the opportunity of procreation by an action
of which he neither knows nor approves, and there is the possibility of action
for damages being taken against the H.E.O. in such a case.
With regard to pills, the final act in contraception is taken by the wife in
swallowing them, and the H.E.O. is thus a more remote agent. However,
unless it is undesirable for medical reasons that she become pregnant, to
provide the pill to the wife of a disapproving husband is unwise.
In regard to the provision of contraception to an unmarried female of 16
years or more, known by the H.E.O. to be having sexual intercourse, the
H.E.O. will by guided by the principles that he/she will do what is best for the
welfare of his/her patient. He/she is certainly breaking no law in providingcontraception to such a patient.
2.9 Informing the patient
A patient has the right to know the facts and opinion about his case. In
serious illness, especially where likelihood of recovery is slight or absent, the
H.E.O. should use great care in deciding what he/she tells the patient andhow he/she tells him, bearing in mind that he/she must act on the patient’s
best interests. It should perfectly ethical to inform near and responsible
relatives of the true state of affairs in such a case and to discuss how far
he/she the H.E.O, should go in giving his /her opinion when the patient
demands it.
2.10 An H.E.O must give the necessary treatment in emergency.
2.11 An H.E.O. may cease attending a case if he/she feels that the professional
relationship is unsatisfactory due to the conduct of the patient or the
patient’s guardians or where confidence has been lost, or when the case is
beyond his/her ability, provided:
a: the fullest allowance has been made for the patient’s unsatisfactory conduct.
b: arrangements for the transfer of the patient have been adequately made.
c: withdrawal of attendance does not interfere with the patient’s welfare or
treatment.
2.12 Sexual intercourse with a patient or relatives of a patient is forbidden. Every
family and every community has the right to expect their special relationship
with the H.E.O. to be guaranteed against abuse.
2.13 An H.E.O. while on duty, if incapable of looking after his/her patient’sproperly because of drunkenness or drug abuse, is guilty of serious
professional misconduct.
3. DUTIES OF H.E.O’s TO THE COMMUNITY
3.1 An H.E.O. must provide his/her services equally to all individuals in a
community regardless of race, tribe, political beliefs, or where an individual
comes from. An H.E.O. must never exercise the “wantok” system when
providing his/her service to the community.
3.2 An H.E.O. must respect the integrity of the community.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 37/41
\36
3.3 An H.E.O. must also get involved in community heath related activities.
3.4 An H.E.O. must show courtesy, respect for or the village elders, and
community when dealing with the village community feelings when
conducting public health programs and other community health orientated
activities.
3.5 An H.E.O. must not undermine the traditional cultures of the village
communities.
3.6 An H.E.O. must not abuse a member of the opposite sex when carrying out
public health programs within a village.
3.7 For instance, it would be improper for an H.E.O. to have a sexual intercourse
with a village girl or a woman when he/she carrying out a patrol.
3.8 An H.E.O. must have sympathetic attitudes towards the need of the
community. He/she must not use bulldozing tactics in getting a village
community to participation in the delivery of health services, (e.g. if there is atraditional ceremony being held by the village community coinciding with
the H.E.O. program the H.E.O. should not interfere with these ceremonies).
3.9 An H.E.O. must not use his/her status to influence the community (e.g. when
campaigning for election to Parliament).
3.10 An H.E.O. must be helpful to the community by example rather than by
telling (e.g. an H.E.O. should take part in projects like digging of toilets, water
supply, instead of telling people to do the work.
3.11 An H.E.O. must not behave in a drunken manner towards an individual
member of the community.
An H.E.O. must not be involved in drunken brawls within the community.
4. DUTIES OF H.E.O’s TO THE NATION
4.1 An H.E.O. must be loyal to the government of the day.
4.2 An H.E.O must never ask what the nation should do for him/her, but rather
he/she must ask him/herself what he/she can do for the nation.
5. DUTIES OF H.E.O’s TO THE EMPLOYER
5.1 An H.E.O. must abide by the rules and regulations set down by his/her employer inthe interest of the nation.
5.2 An H.E.O. must be loyal to his/her employer, (e.g. he/she must never criticism made
by the H.E.O. against his/her employer must be constructive and must be made in
confidence).
5.3 An H.E.O. must obey instructions given to him/her by his/her employer within
reason, (e.g. if an H.E.O. is posted to serve in an area where his/her employers
consider to have a greater need, the H.E.O. must be willing to go).
5.4 An H.E.O. must be cautious in the utilization of available resources, in the persuit of his/her employer’s aim (e.g. an H.E.O. must not misuse funds allocated to him/her,
the H.E.O. must not misuse his employer’s properties under his/her care.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 38/41
\37
5.5 An H.E.O. must use drugs wisely; he/she must discourage wastage of drugs.
5.6 An H.E.O. must never allow wastage through inefficiency or lack of concern for
maintenance of health center supplies and equipment, (e.g. he/she must never allow
a refrigerator to run out of kerosene which could ultimately lead to the wastage
vaccines).
6. DUTIES OF H.E.O’s TO THE PROFESSION
6.1 An H.E.O. must be loyal to his/her profession. For instance, an H.E.O, must carry out
all his/her duties to the best of his/her ability.
6.2 An H.E.O. must strive to maintain a high standard of professional conduct. An H.E.O.
must set a good example in the maintenance of good health, and maintaining a high
standard of health as required by his/her profession, (e.g. maintain a clean
environment of health centre, maintain a high standard of cleanliness in his/her
personal appearance.
7. DUTIES OF H.E.O’s TO OTHERS
An H.E.O. must behave towards others as he/she would have them behave towards
him/her.
a: Doctors
An H.E.O. must give due respect to a doctor, regardless of personal differences.
An H.E.O. must never allow professional jealousy between him/her and a doctor to
over ride the H.E.O’s concern for his/her patients or the community he/she serves.
b: Supervisors
An H.E.O. must carry out instructions given to him/her by his/her supervisors. If an
H.E.O. has good reasons to disagree with his/her supervisor’s instructions, he/she
should communicate his/her disagreement in a polite and respectful manner.
c: Nurses
An H.E.O. must establish and maintain effective co-operation between him/her and
the nurses. He/she must never allow him/herself to think of nurses as having and
inferior status to this own.
d: Environment Health Officer (E.H.O’s)
An H.E.O. must never regard him/herself as superior to Environmental Health
Officers. An H.E.O. must ensure a high standard of working relationship between
him/herself and the Environment Health Officer in the interest of their communities
and the nation as a whole.
e: Dental Therapist
An H.E.O. must observe similar relationships applicable to the H.E.O. and the E.H.O’s
and nurses.
f: Malaria Eradication Officers

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 39/41
\38
An H.E.O. must maintain relationships with the malaria eradication officers similar
to the type of relationship he/she maintains with E.H.O’s, nurses and dental
therapist.
8. DUTIES OF H.E.O’s TO EACH OTHER
8.1 An H.E.O has a moral obligation to his/her patients. If he/she lacks the necessary
ability to examine or to treat a patient, he/she must consult with another H.E.O. to
seek advice and assistance in the treatment of the patient. An H.E.O. must never
think that asking his/her fellow H.E.O. is below his/her dignity.
8.2 It is unethical for an H.E.O. to gossip about a fellow H.E.O. to others. In the interest of
the H.E.O. profession, H.E.O’s are expected to discuss problems affection each otherdirectly instead of resorting to malicious gossip.
8.3 As colleagues, H.E.O’s must support each other morally and professionally. It is
unethical for a H.E.O. to criticize the inability and inefficiency of another H.E.O. in
front of a patient or individual of a community. Criticism of a colleague must be done
courteously with professional interest being the aim. H.E.O’s should never be
offended when criticisms against them are made by a colleague on the basis of professional practice.
9. DUTIES OF H.E.O’s TO HIMSELF/HERSELF
9.1 An H.E.O. must continually seek to better him/herself professionally. This implies
that H.E.O’s learning does not end once he/she graduates from the college. An H.E.O.
must continue to keep up with the latest development in the field of H.E.O. education
and must accept personal responsibility to keep him/herself informed of educational
development in the H.E.O. profession.
9.2 An H.E.O. must actively seek to better him/herself by developing responsible
attitudes towards him/herself, (e.g. an H.E.O. must avoid excessive consumption of
alcohol. This could lead to personal disaster). He/she must have the welfare of
him/herself and his/her family safe-guided against undesirable consequences.
9.3 An H.E.O. must protect him/herself from diseases that may lead to possible bad
effect on his/her professional efficiency.

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 40/41
\39
HUMANITY
This criterion requires all who are concerned with the delivery of health care
to treat those whom they service as fellow human being, entitled to respect,
understanding and sympathy. Entitled also to be treated in a manner free
from arrogance or disc

8/3/2019 s Ward Rotation Manual May 2011
http://slidepdf.com/reader/full/s-ward-rotation-manual-may-2011 41/41