s retina pearls management of uveal effusion …retinatoday.com/pdfs/0918rt_pearls.pdf · retina...
TRANSCRIPT

s
RETINA PEARLS
18 RETINA TODAY | SEPTEMBER 2018
Uveal effusion, also referred to as choroidal detachment, can occur secondary to a number of ocular conditions that result in inflam-matory or hydrostatic changes,
including scleritis, posterior uveitis, and hypotony after glaucoma surgery.1 When no cause can be identified, this entity is termed uveal effusion syndrome (UES). It is by definition idiopathic but can be associated with nanophthalmia or hyper-metropia in some cases.
The disease course is typically relaps-ing and remitting. Gradual superior visu-al field loss is the most common initial complaint, but patients may also report blurred vision or metamorphopsia.2 The magnitude of choroidal elevation in UES is highly variable, but it typically begins in the periphery. Simultaneous exuda-tive retinal detachment that can involve the macula may occur (Figure 1A). Deep retinal or subretinal exudates may appear prior to serous detachment, and optic nerve edema may be present.2,3 There may be mild to moderate vitreous cell.2 Hyperpigmented changes in the retinal pigment epithelium (RPE), termed leopard spots, and permanently reduced VA can occur with chronic disease (Figure 1B).4 Spontaneous resolu-tion occurs in most cases but may take months or several years.2
EPIDEMIOLOGY UES is extremely rare. Patients
are typically middle-aged men.2 Approximately 65% of cases are
bilateral. Approximately half of those requiring surgical interven-tion to reverse the condition in one eye will require surgery in the fellow eye.1 Nanophthalmos itself is always bilateral and may be sporadic or famil-ial with either dominant or recessive patterns of inheritance.5
THEORIES OF PATHOGENESIS Analyses of imaging with ultrasound
biomicroscopy and MRI suggest that the sclera may be abnormally thickened in patients with UES.6 Histologic speci-mens of excised sclera in nanophthalmic eyes and eyes with UES demonstrate disruption of collagen fibers and the presence of glycosaminoglycan-like material within the interfibrillary spaces.5,7-9 The subretinal fluid in these
eyes contains two to three times greater concentration of albumin and other proteins than in healthy eyes. In 50% of cases, cerebrospinal fluid protein is also elevated without pleo-cytosis.10 These findings suggest that transscleral exit of albumin may be impaired, leading to a hyperosmotic gradient into the choroid.11
Another hypothesis is that compres-sion of the scleral veins by swollen or abnormal scleral tissue results in cho-roidal fluid retention.10,12 Gass et al also reported hypoplastic or missing vortex veins in eyes with UES of both nanoph-thalmic and normal axial lengths.2,10 In nanophthalmic eyes with chronic angle closure, dilated episcleral veins and blood in Schlemm canal can be seen. These findings are indicative of
MANAGEMENT OF UVEAL EFFUSION SYNDROME
Several surgical methods have been proposed to manage this rare condition.
BY ZACHARY BODNAR, MD; and PRITHVI MRUTHYUNJAYA, MD, MHS
AT A GLANCE
s
Uveal effusion syndrome (UES) is a rare idiopathic cause of choroidal detachment that may be associated with nanophthalmos and increased scleral thickness.
s
Diagnosis of UES is often delayed due to an overlap in clinical findings with posterior uveitis and intraocular lymphoma.
s
The authors describe their own technique for surgical management of UES, which involves creation of scleral windows in four quadrants.

RETINA PEARLS s
SEPTEMBER 2018 | RETINA TODAY 19
increased resistance to venous drain-age from the eye.10
These proposed mechanisms are not mutually exclusive, and the end result is believed to be transudative exit of fluid from the choriocapillaris into the surrounding potential space. This leads to choroidal swelling and detachment. Fluid may also accumulate in the sub-retinal space, resulting in concurrent exudative retinal detachment.
Not all eyes with UES have been shown to have abnormalities of the sclera. Uyama et al performed lamellar sclerectomy in 19 eyes of 16 patients with UES. Histologic analysis of the excised sclera revealed disorganized collagen and deposition of proteoglycans in the extracellular matrix of the nanophthalmic eyes and eyes with thickened sclera but not in normal-sized eyes with normal scleral thickness. This may have implications for treatment, as the normal-sized, normal thickness eyes did not respond to sclerectomy.13
EVALUATION UES is a diagnosis of exclusion. The
clinician should first rule out other causes of choroidal effusion and serous retinal detachment, such as posterior scleritis and uveitis, choroidal neopla-sia such as uveal lymphoma, paraneo-plastic syndromes, metastatic tumors of the choroid or retina, hypertensive choroidopathy, postoperative inflam-mation from cryotherapy or photoco-agulation, and persistent hypotony.
IOP is usually normal in UES, and abnormal tonometry should prompt a search for other causes, as should signs of ocular inflammation. Central serous chorioretinopathy with mul-tiple detachments of RPE can have a similar appearance to UES, but choroidal thickening and choroidal detachment will be absent.2 Dark-appearing choroidal detachments can be mistaken for suprachoroidal hemorrhage, peripheral exudative hemorrhagic chorioretinopathy, or choroidal melanoma.3,14
IMAGING B-scan ultrasonography can be
used to document the presence of retinal and/or choroidal detachment. Often, the choroid and/or sclera will
be thickened. It is not uncommon to see annular thickening of the anterior choroid, often captured best with ultrasound biomicroscopy. Ultrasound is helpful in identifying
Figure 1. Widefield color fundus photograph of an eye with UES depicting peripheral choroidal effusions with overlying serous retinal detachment (A). Postoperative appearance of the same eye after the creation of scleral windows shows flattening of the choroidal effusions and resolution of the serous retinal detachment with VA of 20/30. Persistent leopard spot hyperpigmentation is seen (B).
A
B

s
RETINA PEARLS
20 RETINA TODAY | SEPTEMBER 2018
secondary causes of observed fundus changes, including choroidal tumors or the T-sign seen in posterior scleritis (a hyporeflective layer of fluid in the Tenon space surrounding the nerve).3,15 In ruling out other conditions such as scleritis, standardized A-scan ultrasound provides accurate axial length measure-ments to identify nanophthalmos.
Fluorescein angiography in UES typically shows areas of hypofluores-cence corresponding to leopard-spot pigmentation, with angiographic leak-age rarely identified.2,4 In the acute setting, the leopard spots will appear as hyperfluorescent on fundus autofluo-rescence (FAF), but over time this may change to a mix of hyper- and hypo-autofluorescence on FAF (Figure 2). Corresponding OCT through the spots will reveal focal thickening of the RPE. Both of these findings may diminish with resolution of subretinal fluid, but typically the FAF changes will persist.16
Enhanced-depth OCT demonstrates increased choroidal thickness compared with normal eyes and the presence of large areas of hypo-reflectivity that may correspond to engorged choroidal veins or expan-sion of the suprachoroidal space.17 Indocyanine green angiography appears to confirm the presence of dilated choroidal vessels.18 ERG may be abnormal but is nonspecific.2
NONSURGICAL MANAGEMENT Much of the literature suggests
that UES is refractory to medical management. Several reports have indicated that systemic corticosteroids and immunomodulating agents produce neither a dramatic nor last-ing response.2,4,10 However, some more recent studies provide evidence that a subset of eyes with UES may respond well to oral, periocular, or topical steroids and poorly to surgi-cal treatment.13 A large retrospective study by Shields et al analyzed the response of eyes with UES and normal axial length without evidence of scleral thickening to oral, periocular, or topical
corticosteroids or a combination there-of. Of 104 eyes, 95% had resolution of effusions after a median of 3 months of steroid therapy, and only 5% required scleral window surgery.19
Other proposed nonsurgical thera-pies include laser photocoagulation and topical application of a prostaglan-din analogue. Kumar et al reported improvement in chronic exudative retinal detachment and modest improvement in vision in two patients with UES after treatment with long-term slow-release indomethacin and scatter laser photocoagulation, but the authors acknowledged that the improvement may have been spontaneous.18 Several other reports found no lasting benefit of laser photocoagulation to areas of angio-graphic leakage.2,4
In principle, prostaglandin analogues could be helpful by increasing uveo-scleral outflow.11,20 Derk et al reported resolution of effusions after 3 months in three patients with bilateral disease who were treated with a combination of topical latanoprost and oral acetazol-amide.21 Prostaglandin analogues have not been evaluated for the treatment of UES in any large clinical studies.
SURGICAL MANAGEMENT Several surgical treatments have
been described, with the surgical goals being (1) direct (internal or external) drainage of the subretinal fluid, (2) reduction in scleral resistance to allow fluid evacuation from the
suprachoroidal space, (3) unroofing of the vortex veins, or (4) a combination of approaches.
A common approach is to create full-thickness sclerectomies to facilitate the egress of suprachoroidal fluid. In a series of 23 eyes with UES and normal axial length, Johnson and Gass reported ana-tomic improvement within 6 months in 83% of eyes after a single procedure to create sclerectomies. After one or two procedures, 96% of eyes demon-strated anatomic improvement. The average time to reattachment was 2 to 3 months, with recurrence in 23% of eyes. Final VA improved by 2 or more lines in 56% of eyes, remained stable in 35% of eyes, and worsened in 9%. The median final VA improved from 20/100 preoperatively to 20/60.4 Jackson et al reported full resolution of choroidal effusions in seven of 14 eyes using this same technique.22 Two case reports describe a modification of this tech-nique using mitomycin C applied to the sclerectomy bed to reduce scarring.23,24
Sabrosa et al reported a successful revision of a failed deep sclerectomy surgery using a scleral punch and mito-mycin C.25 Yepez and Aravalo used Ex-Press Glaucoma Filtration Device (Alcon) shunts to maintain patency of the sclerotomies.26 Schneiderman and Johnson described a case in which pars plana vitrectomy and internal drain-age of subretinal fluid with C3F8 gas tamponade was combined with partial thickness sclerectomies in a 73-year-old patient with UES.27
Uyama et al described a technique they called subscleral sclerectomy in which two-thirds–thickness scleral flaps measuring 4 mm by 5 mm are made in the inferotemporal and inferonasal quadrants. Beneath each flap, the remaining sclera is excised to expose the choroid. The edges of the scleral wounds are then cauter-ized, and the flap is loosely sutured. If a second procedure is required, additional sclerectomies can be per-formed in the upper quadrants. The authors also administered mannitol
Figure 2. FAF demonstrates leopard spots.
RETINA PEARLS s
SEPTEMBER 2018 | RETINA TODAY 21
and acetazolamide postoperatively to attempt to hasten the resolution of fluid. They reported that their surgical approach resulted in resolu-tion of subretinal fluid and choroidal thickening in nanopthalmic eyes and normal-sized eyes with scleral thick-ening but not in eyes with normal axial length and scleral thickness.13
Ghazi et al described a modified technique wherein preoperative or intraoperative B-scan ultrasound is used to identify areas of maximal scler-al choroidal thickening in each involved quadrant. These sites are then chosen for sclerostomy placement using a Kelly punch. For sites located anterior to the equator, a single sclerostomy punch within a 4-mm circumferential incision is made. At posterior sites, a 4-by-4-mm, two-thirds–thickness sclerectomy is also performed. These authors reported complete resolution of choroidal thickening and subretinal fluid in five of six eyes using this tech-nique, and the majority resolved within 3 to 4 months.15
Faulborn and Kölli reported rapid resolution of choroidal effusions and serous retinal detachment in five eyes of four patients using another modified technique. They created 2-by-8-mm full-thickness scleral flaps without sclerectomy, 4 mm posterior to the limbus in each quadrant. The flaps were not secured with sutures.1 As there is a risk of hemorrhage asso-ciated with the creation of scleral windows, Bausili et al reported use of a CO2 laser to perform simultaneous tis-sue dissection and cautery.28
Surgical decompression of the vortex veins where they exit the sclera has also been described. This procedure may be combined with drainage of choroidal or subretinal fluid with intra-vitreal injection of air.12 A technique described by Brockhurst combines scleral resection to unroof the vortex veins with sclerotomies to drain the suprachoroidal fluid. The sclerectomy begins at the insertion of the rectus muscles and extends to the exit of the
vortex veins in each quadrant. Separate, smaller full-thickness sclerotomies are made in each scleral dissection bed for fluid drainage. In Brockhurst’s original report, retinal reattachment was achieved in eight of 10 eyes.12 Yue et al subsequently reported successful treat-ment of two nanophthalmic eyes with UES using this technique.9
Ozgonul et al suggested using a staged approach beginning with partial thickness sclerectomies. If a second surgery is required, revision of the flap using mitomycin C can be considered. Full-thickness sclerostomy, as per the Ghazi method, or unroofing of the vortex veins may be considered in eyes that are refractory to revision with
mitomycin C.29
Each of the surgical approaches described above is an attempt to cre-ate a durable, low-resistance pathway for choroidal fluid to exit. Matlach et al proposed that it may be sufficient to drain the fluid intraoperatively using a penetrating diathermy probe to access the suprachoroidal space, with ante-rior chamber infusion placed to create a pressure differential. Complete flat-tening of the choroid can be achieved by the end of surgery using this tech-nique, the authors asserted, but one of two eyes in the small series they reported required a repeat procedure for late recurrence.30
Our own preference is to perform
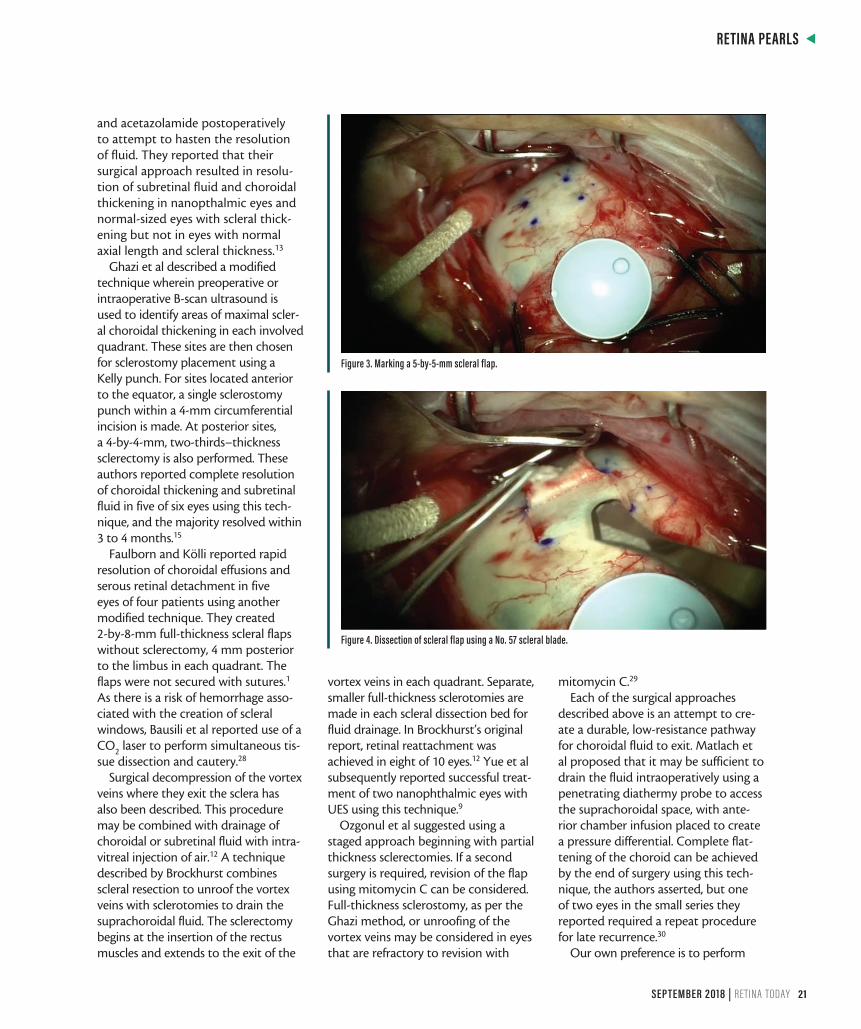
Figure 3. Marking a 5-by-5-mm scleral flap.
Figure 4. Dissection of scleral flap using a No. 57 scleral blade.

s
RETINA PEARLS
22 RETINA TODAY | SEPTEMBER 2018
four-quadrant scleral windows. After the conjunctiva is exposed, the four rectus muscles are isolated and the oblique quadrants revealed. A mark is made to outline a 5-by-5-mm scleral flap in mid-quadrant, about 4 mm from the rectus muscle insertion (Figure 3). Using a No. 57 scleral blade (Alcon), an 80% scleral thickness lamellar flap is outlined and dissected (Figure 4). Then a smaller, inner scleral 3-mm incision is made down to the glistening fibers of the outer choroid but clearly into the suprachoroidal space. It is important not to have any thin lamella of tissue covering the uveal tissue. Next, using a Kelly punch, the inner lip of the remain-ing scleral lamellar fibers are removed to create a round circle of exposed uveal tissue (Figure 5). The outer scleral flap is then amputated. (Alternatively, it can be sutured back without significant tension.) This is repeated in the other three quadrants if there is adequate exposure. We do not purposely try to unroof or disturb the vortex veins. Rarely, if there is a highly bullous exu-dative retinal detachment, secondary drainage of the fluid can be added, but this is often not necessary.
IT PAYS TO KNOW ABOUT UES UES is a rare idiopathic cause of
choroidal detachment that may be associated with nanophthalmos and increased scleral thickness.
Concomitant chronic serous retinal detachment involving the macula can lead to permanent vision loss. Multimodal imaging can be helpful to confirm UES and differentiate it from other causes of choroidal effusion.
Although some eyes with normal axial length and no scleral thickening may respond to treatment with oral, topical, or periocular cortico-steroids, many will require surgical intervention to facilitate the flow of fluid from the choroid through the sclera. However, a delay in diagnosis of this condition prior to definitive surgery may result in chronic visual compromise. The review provided above may be helpful for clinicians who encounter patients with this rare but potentially serious condition. n
1. Faulborn J, Kölli H. Sclerotomy in uveal effusion syndrome. Retina. 1999;19(6):504-507.2. Gass JD, Jallow S. Idiopathic serous detachment of the choroid, ciliary body, and retina (uveal effusion syndrome). Ophthalmology. 1982;89(9):1018-1032.3. Elagouz M, Stanescu-Segall D, Jackson TL. Uveal effusion syndrome. Surv Ophthalmol. 2010;55(2):134-145.4. Johnson MW, Gass JD. Surgical management of the idiopathic uveal effu-sion syndrome. Ophthalmology. 1990;97(6):778-785.5. Brockhurst RJ. Nanophthalmos with uveal effusion. A new clinical entity. Arch Ophthalmol. 1975;93(12):1989-1999.6. Lam A, Sambursky RP, Maguire JI. Measurement of scleral thickness in uveal effusion syndrome. Am J Ophthalmol. 2005;140(2):329-331.7. Trelstad RL, Silbermann NN, Brockhurst RJ. Nanophthalmic sclera. Ultra-structural, histochemical, and biochemical observations. Arch Ophthalmol. 1982;100(12):1935-1938.8. Ward RC, Gragoudas ES, Pon DM, Albert DM. Abnormal scleral findings in uveal effusion syndrome. Am J Ophthalmol. 1988;106(2):139-146.9. Yue BY, Duvall J, Goldberg MF, et al. Nanophthalmic sclera. Morphologic and tissue culture studies. Ophthalmology. 1986;93(4):534-541.10. Gass JD. Uveal effusion syndrome: a new hypothesis concerning pathogenesis and technique of surgical treatment. 1983. Retina. 2003;23(6 Suppl):159-163.11. Jackson TL, Hussain A, Salisbury J, et al. Transscleral albumin diffusion and
suprachoroidal albumin concentration in uveal effusion syndrome. Retina. 2012;32(1):177-182.12. Brockhurst RJ. Vortex vein decompression for nanophthalmic uveal effusion. Arch Ophthalmol. 1980;98(11):1987-190.13. Uyama M, Takahashi K, Kozaki J, et al. Uveal effusion syndrome: clinical features, surgical treatment, histologic examination of the sclera, and pathophysiology. Ophthalmology. 2000;107(3):441-449.14. Davies EW, Sanders MD, Harry J. Annular serous detachment of the choroid. Trans Ophthalmol Soc U K. 1973;93(0):145-159.15. Ghazi NG, Richards CP, Abazari A. A modified ultrasound-guided surgical technique for the management of the uveal effusion syndrome in patients with normal axial length and scleral thickness. Retina. 2013;33(6):1211-1219.16. Okuda T, Higashide T, Wakabayashi Y, et al. Fundus autofluorescence and spectral-domain optical coherence tomography findings of leopard spots in nanophthalmic uveal effusion syndrome. Graefes Arch Clin Exp Ophthalmol. 2010;248(8):1199-1202.17. Harada T, Machida S, Fujiwara T, et al. Choroidal findings in idiopathic uveal effusion syndrome. Clin Ophthalmol. 2011;5:1599-1601.18. Kumar A, Kedar S, Singh RP. The indocyanine green findings in idiopathic uveal effusion syndrome. Indian J Ophthalmol. 2002;50(3):217-219.19. Shields CL, Roelofs K, Di Nicola M, et al. Uveal effusion syndrome in 104 eyes: Response to corticosteroids - The 2017 Axel C. Hansen lecture. Indian J Ophthalmol. 2017;65(11):1093-1104.20. Kerstetter JR, Brubaker RF, Wilson SE, Kullerstrand LJ. Prostaglandin F2 alpha-1-isopropylester lowers intraocular pressure without decreasing aqueous humor flow. Am J Ophthalmol. 1988;105(1):30-34.21. Andrijević Derk B, Benćić G, Corluka V, et al. Medical therapy for uveal effusion syndrome. Eye (Lond). 2014;28(8):1028-1031.22. Jackson TL, Hussain A, Morley AM, et al. Scleral hydraulic conductivity and macromolecular diffusion in patients with uveal effusion syndrome. Invest Ophthalmol Vis Sci. 2008;49(11):5033-5040.23. Akduman L, Adelberg DA, Del Priore LV. Nanophthalmic uveal effusion managed with scleral windows and topical mitomycin-C. Ophthalmic Surg Lasers. 1997;28(4):325-327.24. Suzuki Y, Nishina S, Azuma N. Scleral window surgery and topical mito-mycin C for nanophthalmic uveal effusion complicated by renal failure: case report. Graefes Arch Clin Exp Ophthalmol. 2007;245(5):755-757.25. Sabrosa NA, Smith HB, MacLaren RE. Scleral punch method with topical mitomycin C for safe revision of failed deep sclerectomy in nanophthalmic uveal effusion syndrome. Graefes Arch Clin Exp Ophthalmol. 2009;247(7):999-1001.26. Yepez JB, Arevalo JF. Ex-Press shunt for choroidal fluid drainage in uveal effusion syndrome type 2: a potentially novel technique. JAMA Ophthalmol. 2015;133(4):470-471.27. Schneiderman TE, Johnson MW. A new approach to the surgical management of idiopathic uveal effusion syndrome. Am J Ophthalmol. 1997;123(2):262-263.28. Bausili MM, Raja H, Kotowski J, et al. Use of fiberoptic-guided CO2 laser in the treatment of uveal effusion. Retin Cases Brief Rep. 2017;11(3):191-194.29. Ozgonul C, Dedania VS, Cohen SR, Besirli CG. Scleral surgery for uveal effusion. Retina. 2017;37(10):1977-1983.30. Matlach J, Nowak J, Göbel W. A novel technique for choroidal fluid drainage in uveal effusion syndrome. Ophthalmic Surg Lasers Imaging Retina. 2013;44(3):274-277.
ZACHARY BODNAR, MDn Second-Year Vitreoretinal Surgery Fellow, Stanford
University, Paolo Alto, Californian [email protected] Financial disclosure: None
PRITHVI MRUTHYUNJAYA, MD, MHSn Associate Professor of Ophthalmology, Ocular
Oncology, and Vitreoretinal Surgery, Byers Eye Institute at Stanford University, Palo Alto, California
n [email protected] Financial disclosure: Consultant (Castle
Biosciences, Optos, Spark Therapeutics)
Figure 5. Creation of sclerostomy using Kelly punch.