rural track first meeting orientation to the rural track interactive session: what is “rural”? 1
TRANSCRIPT

Rural Track First Meeting
• Orientation to the Rural Track• Interactive session: What is
“rural”?
1

Orientation to the Rural Track
– Who we are– Curriculum overview– What are our goals– Our communication methods
2

Curriculum Overview• Phase I and II seminars and workshops• Rural Grand Rounds• Social events• Summer:
– Immersion week and preceptorship month
• Intersession meetings• Advising for all, MSA for some• Phase III longitudinal rural clerkship• Phase IV elective(s) – in progress• Post-graduation follow-up
3

Goals of the Rural Track
• Attract, admit and nurture students interested in being future rural physicians, particularly in primary care.
• Offer information and experiences that will help you make informed decisions about your future career directions.
• Conduct educational research 4

5
Residency Match Results of Rural Track Students
2009 Grads
2010 Grads
2011 Grads
2012 Grads
2013 2014 Totals
Family Medicine
7 (5 in CO)
6 (2 in CO) 8 (2 in CO)
4 (1 in CO)
11 (2 in CO)
4 40
Pediatrics
2 (1 in CO)
0 0 0 1 1 4
Internal Medicine
0 3 (2 in CO) 2 0 1 5 11
Med Peds
0 0 0 0 0 1 1
Emergency Medicine
2 (1 in CO)
3 (1 in CO) 1 3 (1 in CO)
4 2 15
General Surgery
1 in CO 1 in CO 2 0 1 in CO 5
Other 0 5 (1 in CO) 3 2 5 (1 in CO)
5 20
Total 12 (8 in CO)
18 (7 in CO)
16 (2 in CO)
9 (2 in CO)
23 (4 in CO)
18 96

What and where are RT Grads Practicing?
• 28 of the 96 have completed residency and entered clinical practice. 82% are in primary care, 61% are in Family Medicine,
• 50% are in rural practice and 30% are in rural practice in Colorado.
6

CU SOM Overall
• 19% Primary care practice• ? % rural
7

Communication
•Email•Website•Office hours•Periodic surveys
8

What is Rural?
CU SOM Rural TrackMark Deutchman MD
9

Objectives• Understand the various definitions
of “rural” and look at the Colorado map
• Understand some of the parameters that are used to assess rural health and healthcare
• Review how healthcare is organized and delivered in rural areas.
• List resources for information about rural health and healthcare
10

Exercise # 1
• Write down how you would answer a classmate who asks “what is rural”?
11

Sources of Definitions (and who cares?)
• US Census Bureau• Office of Management and Budget• Economic Research Service of the
U.S. Department of Agriculture (USDA)
• Office of Rural Health Policy• Conventional wisdom
12

13
Urban is better defined than rural
• US census bureau defines “urban” as “places of > 2500 people.
• US OMB defines a “metropolitan area” as “core area containing a large population nucleus, together with adjacent communities having a high degree of economic and social integration with that core.”

14
Urbanized area (OMB)
• “A central place and its “urban fringe”, or surrounding territory, which is populated by at least 50,000 people.”
• Colorado’s UA’s:– Boulder, Colorado Springs, Denver,
Fort Collins, Grand Junction, Greeley, Longmont, Louisville, and Pueblo.

Urban Cluster (OMB)
• A core with a total land area of less than two square miles and a population density of 1,000 persons per square mile. They may contain adjoining territory with at minimum 500 persons per square mile and encompass a population of at least 2,500 but less than 50,000 persons.
15

Micropolitan Statistical Area
• Nonmetro county with an urban cluster of at least 10,000 persons or more. As with metro areas, outlying counties are included if commuting to the central county is 25 percent or higher, or if 25 percent of the employment in the outlying county is made up of commuters from the central county.
16

RUCA Codes• Rural-Urban Commuting Area codes• Census tract-based classification• Use standard Bureau of Census urban
area and place definitions in combination with commuting information to characterize all of the nation's census tracts regarding their rural and urban status and relationships.
17

RUCA Codes• Based on 2010 census and the 2006-10
American Community Survey. • Two levels:
– Whole numbers (1-10) delineate metropolitan, micropolitan, small town, and rural commuting areas based on the size and direction of the primary (largest) commuting flows.
– Further subdivided based on secondary commuting flows, providing flexibility in combining levels to meet varying definitional needs and preferences
18

19
Primary RUCA Codes, 2010 Codes 4-10 are generally considered “rural”
1 Metropolitan area core: primary flow within an urbanized area (UA)
2 Metropolitan area high commuting: primary flow 30% or more to a UA
3 Metropolitan area low commuting: primary flow 10% to 30% to a UA
4Micropolitan area core: primary flow within an Urban Cluster of 10,000 to 49,999 (large UC)
5Micropolitan high commuting: primary flow 30% or more to a large UC
6 Micropolitan low commuting: primary flow 10% to 30% to a large UC
7Small town core: primary flow within an Urban Cluster of 2,500 to 9,999 (small UC)
8 Small town high commuting: primary flow 30% or more to a small UC
9 Small town low commuting: primary flow 10% to 30% to a small UC
10 Rural areas: primary flow to a tract outside a UA or UC
99Not coded: Census tract has zero population and no rural-urban identifier information

Colorado county Ruca Codes in County
Larimer and El Paso 1,2,7
Weld 1,2,3,4,10
Mesa and Pueblo 1,2,10
Montrose and La Plata 4,5,10
Garfield 4,5,7
Chaffee 7
Park 2,10
Gunnison 7,8,10
Alamosa 7,8
Morgan 4,7,10
Prowers 7,8,10
Broomfield 1,10
Baca, Lincoln RioBlanco, Washington, Dolores, Sedgwick
1020
21
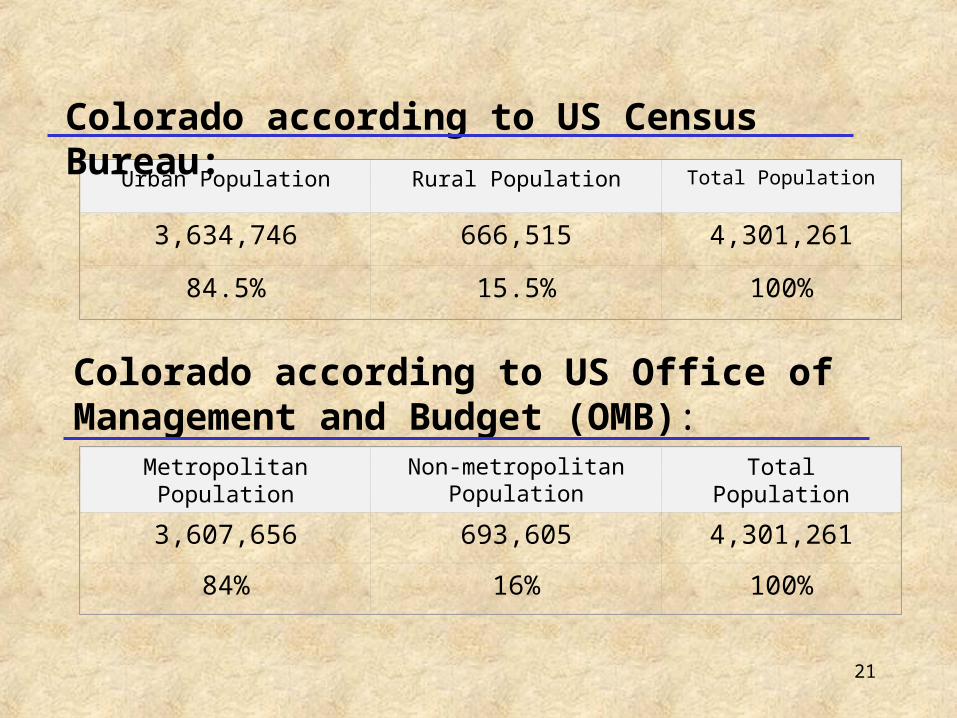
Urban Population Rural Population Total Population
3,634,746 666,515 4,301,261
84.5% 15.5% 100%
Metropolitan Population
Non-metropolitan Population
Total Population
3,607,656 693,605 4,301,261
84% 16% 100%
Colorado according to US Census Bureau:
Colorado according to US Office of Management and Budget (OMB):

22
Colorado’s Metropolitan Areas
(16 counties in white)
23
Frontier• “A county with six (6) or fewer people
per square mile. • Based on counties. • 23 of Colorado’s 64 counties:
– 43% of land mass– 3% of population

Exercise # 2
• Write down some adjectives that you think apply to the demographics and health of rural people.
24

People & Health in Rural COParameter Rural V. Urban
Median Age
Median Household Income
Children in poverty
Un-insurance
Suicide rates
MVA deaths/100,000
Births to teens
Monthly health insurance
25https://coruralhealth.org/?post_type=resources&p=17385

People & Health in Rural COParameter Rural V. Urban
Median Age 45-64, versus 18-44
Median Household Income
$45,307 compared to $61,642
Children in poverty 24.5% compared to 15.8%
Un-insurance 20.6% compared to 15.1%
Suicide rates Higher in rural
MVA deaths/100,000 20 v. 12.3
Births to teens 1.6 times higher in rural
Monthly health insurance
$ 532 V. $352
26https://coruralhealth.org/?post_type=resources&p=17385

HPSA• Health Professional Shortage Areas
may be designated as having a shortage of primary medical care, dental or mental health providers. They may be urban or rural areas, population groups or medical or other public facilities.
• Primary Care: population to practitioner ratio of > 2,000:1
• Dental : a population to practitioner ratio of > 3,000:1
• Mental Health: a population to practitioner ratio of 10,000:1
27

MUA
• Medically Underserved Areas/Populations Medically Underserved Areas (MUA) may be a whole county or a group of contiguous counties, a group of county or civil divisions or a group of urban census tracts in which residents have a shortage of personal health services
28

MUP
• Medically Underserved Populations (MUPs) may include groups of persons who face economic, cultural or linguistic barriers to health care.
29

Colorado’s HPSAs
30

Colorado MUAs and MUPs
31



Exercise # 3
• List some of the types of healthcare organizations that are important to rural healthcare delivery.
34

Critical Access Hospital
• Must be or have been a licensed hospital in the past 10 years
• Must be located in a rural area. • Must have no more than 25 beds; any combination of swing beds or acute. • Must maintain an average length of stay of
no more than 4 days, or 96 hours, annually.
•Must have written agreements with another, larger hospital(s) for appropriate transfer and communication about patients.

36
37
A Rural Health Clinic (RHC) is a primary healthcare clinic located in a non-urbanized area that has been shown to have a shortage of healthcare services or healthcare providers, and has been certified as a Rural Health Clinic under Medicare.
•The greatest benefit of the program is cost-based (enhanced) reimbursement from Medicare and Medicaid.
• There are about 44 RHCs in Colorado.
Certified Rural Health Clinic

38
• Be located in a non-urbanized area;• Be located in a MUA or HPSA that was designated within the past 3 years• Provide outpatient primary care services;• Utilize the services of at least one mid-level practitioner
at least 50% of the time the clinic is open• Have a physician to provide medical direction• Meet health and safety requirements set by Medicare
and/or Medicaid.
What is required to become a certified RHC?

39

40

What is a FQHC ?
41
http://www.ask.hrsa.gov/downloads/fqhc-rhccomparison.pdf

Required Services
42

Cost-based reimbursement
43
http://www.ask.hrsa.gov/downloads/fqhc-rhccomparison.pdf

44

Access to care
• “Access” and “Coverage” are two distinctly different things that are often confused.
• “Coverage” refers to a payment system and the services that are included in that payment
• “Access” refers to how readily available services are.
45

Percent of Colorado Population without Health Insurance and Below 200% FPL,
2000
46

Exercise #4
• List some adjectives that describe your impression of “primary care”
47

Primary CarePrimary care is that care provided by physicians specifically trained for
and skilled in comprehensive first contact and continuing care for persons with any undiagnosed sign, symptom, or health concern (the "undifferentiated" patient) not limited by problem origin (biological, behavioral, or social), organ system, or diagnosis.
Primary care includes health promotion, disease prevention, health maintenance, counseling, patient education, diagnosis and treatment of acute and chronic illnesses in a variety of health care settings (e.g., office, inpatient, critical care, long-term care, home care, day care, etc.). Primary care is performed and managed by a personal physician often collaborating with other health professionals, and utilizing consultation or referral as appropriate.
Primary care provides patient advocacy in the health care system to accomplish cost-effective care by coordination of health care services. Primary care promotes effective communication with patients and encourages the role of the patient as a partner in health care
48

Primary Care PracticeA primary care practice serves as the patient's first point of entry into the health care
system and as the continuing focal point for all needed health care services. Primary care practices provide patients with ready access to their own personal physician, or to an established back-up physician when the primary physician is not available.
Primary care practices provide health promotion, disease prevention, health maintenance, counseling, patient education, diagnosis and treatment of acute and chronic illnesses in a variety of health care settings (e.g., office, inpatient, critical care, long-term care, home care, day care, etc.).
Primary care practices are organized to meet the needs of patients with undifferentiated problems, with the vast majority of patient concerns and needs being cared for in the primary care practice itself. Primary care practices are generally located in the community of the patients, thereby facilitating access to health care while maintaining a wide variety of specialty and institutional consultative and referral relationships for specific care needs. The structure of the primary care practice may include a team of physicians and non-physician health professionals.
49

Primary Care PhysicianA primary care physician is a generalist physician who provides
definitive care to the undifferentiated patient at the point of first contact and takes continuing responsibility for providing the patient's care. Such a physician must be specifically trained to provide primary care services.
Primary care physicians devote the majority of their practice to providing primary care services to a defined population of patients. The style of primary care practice is such that the personal primary care physician serves as the entry point for substantially all of the patient's medical and health care needs - not limited by problem origin, organ system, or diagnosis. Primary care physicians are advocates for the patient in coordinating the use of the entire health care system to benefit the patient.
50

Midlevel Provider
• Physician Assistant• Nurse Practitioner• Certified Nurse Midwife• May or may not be involved in
primary care
51

How does presence of primary care affect access
to care?
52

Colorado 2002Colorado 2002Colorado 2002Colorado 2002

Colorado without Family MedicineColorado without Family MedicineColorado without Family MedicineColorado without Family Medicine

Primary Care Health Professions Shortage AreasBy County




Primary Care Health Professions Shortage AreasWith Family Physicians Removed in 1999

60

61

Benefits of Primary Care • Access• Quality• Prevention• Earlier management of problems• More appropriate care• More cost-effective care• Greater patient satisfaction
63
Classic article:http://www.commonwealthfund.org/usr_doc/Starfield_Milbank.pdf

What does the US physician workforce look like compared to other countries ?
“In every other developed country, 50 to 70 percent of the physicians are generalists. In the United States, however, the proportion of generalists (family physicians, general internists, and general pediatricians) has declined from 42 percent in 1965 to less than 30 percent today. Because fewer than 15 percent of medical students graduating in 1991 and 1992 intended to become generalists, this precipitous decline has actually picked up speed.”
Source: Specialty Distribution of U.S. Physicians -- The Invisible Driver of Health Care Costs NEJM Volume 328:961-963 April 1, 1993 Number 13

Exercise # 5
• Write down some questions that you would like to answer for yourself about your future in healthcare.
65

66

67
Http://www.coruralhealth.org
www.coloradohealthinstitute.org
http://www.raconline.org/
https://www.ruralcenter.org/
http://www.ruralhealthweb.org/
http://www.ers.usda.gov/
http://www.hrsa.gov/ruralhealth/policy
http://www.traindocsrural.org/