ruolo della chirurgia nei linfomi addominali / …chped.it/gico/ancona_2015/relazioni/lelli chiesa-...
TRANSCRIPT

U.O. Clinicizzata di Chirurgia Pediatrica – P.O. di Pescara
Cattedra di Chirurgia Pediatrica – Università di Chieti-Pescara
Professore Pierluigi Lelli Chiesa
RUOLO DELLA CHIRURGIA NEI LINFOMI
ADDOMINALI / INTESTINALI
P. Lelli Chiesa, G. Lauriti

Pediatric Gastrointestinal Tumors, Murphy JT and Foglia RP,
in Pediatric Surgery 7th edition , 2012
EPIDEMIOLOGIA
Lymphoma is the most common small bowel malignancy in children, with
high-grade non-Hodgkin lymphoma (NHL) comprising 74% of these tumors.
Burkitt lymphoma constitutes the most common histologic subtype. The
majority of patients (50% to 93%) present with lymphoma localized to the
distal small bowel, although tumor may occur anywhere from the stomach
to the rectum.

GASTROINTESTINAL TUMORS
Gastrointestinal tumors in children and adolescents, Ladd AP and Grosfeld JL, Sem Ped Surg 2006
Non-Hodgkin’s lymphoma (NHL) remains the most common malignancy of
the GI tract in children.

Non-Hodgkin’s Lymphoma
• 3a più frequente neoplasia in età pediatrica
• 3 sottotipi istologici:
- 65% Non-Hodgkin’s lymphoma (NHL) a cellule B
linfoma di Burkitt
linfoma diffuso a grandi cellule B
- 20% Linfoma linfoblastico
- 15% Linfoma anaplastico a grandi cellule
Il Linfoma di Burkitt da solo rappresenta il 40-50% dei NHL pediatrici.

Site distribution of lymphomas
Kohno S et al,
Histopathology 2003
Primary gastrointestinal tract lymphoma in the
pediatric patient: review of 265 patients from the
SEER registry. Kassir N et al, J Pediatr Surg 2011

St Jude’s staging system for Burkitt lymphoma
Clinical implications and surgical management of intussusception in pediatric patients with Burkitt lymphoma,
Gupta H et al, J Pediatr Surg 2007
Stage I A single tumor (extranodal) or involvement of a single anatomical area(nodal), with the exclusion of the mediastinum and abdomen.
Stage II A single tumor (extranodal) with regional node involvement.Two or more nodal areas on the same side of diaphragm.Two single extra nodal tumors, with or without regional node involvementon the same side of the diaphragm.A primary gastrointestinal tract tumor (usually in the ileocecal area), withor without involvement of associated mesenteric nodes, that iscompletely resectable.
Stage III Two single tumors (extranodal) on opposite sides of diaphragm.Two or more nodal areas above and below the diaphragm.Any primary intrathoracic tumor (mediastinal, pleural, or thymic).Extensive primary intraabdominal disease.Any paraspinal or epidural tumor, whether or not other sites are involved.
Stage IV Any of the above findings with initial involvement of the central nervoussystem, bone marrow, or both.

The very rapid growth of this lesion gives us a clue about
the diagnosis. Burkitt’s lymphoma has the shortest
doubling time of cancers in humans and thus was our
leading diagnosis.Case 11-2013: A 4-Year-Old Boy with Fever and
Abdominal Pain. Ryan DP et al, N Engl J Med 2013
BURKITT’S LYMPHOMA
La rapidità del raddoppio volumetrico di questa neoplasia porta
frequentemente a una presentazione di addome acuto che può
essere confusa con altre malattie (occlusione intestinale secondaria
ad invaginazione ileo-cecale causata dalla crescita tumorale,
occlusione intestinale o sanguinamento; alcuni casi possono esordire
con un quadro simile all’appendicite acuta).
Primary gastrointestinal tract lymphoma in the pediatric patient: review of 265 patients from the
SEER registry. Kassir N et al, J Pediatr Surg 2011

• The most common complaint is abdominal pain that has
been present for several weeks before diagnosis
• Weight loss occurs in nearly half of patients and nausea
and vomiting are common
• A palpable mass is found in one third of cases
• Those children that present with colicky abdominal pain
and heme positive stools may have intussusception from
an intramural mass in the distal ileum or cecum
• Fever is seen in 26% of children and an initial diagnosis of
appendicitis may be made
PRESENTAZIONE CLINICA
Lymphoma, Billmire D.F., in The Surgery of Childhood Tumors 2nd edition, 2008

The role of surgery in abdominal non-Hodgkin's lymphoma: experience from the
Childrens Cancer Study Group. LaQuaglia MP et al, J Pediatr Surg 1992
The multicenter Children’s Cancer Study Group experience revealed a
similar pattern with correct preoperative diagnosis in 15% of patients.
In this series, more than half of children had an urgent operation and
most of those were felt to have appendicitis or intussusception.
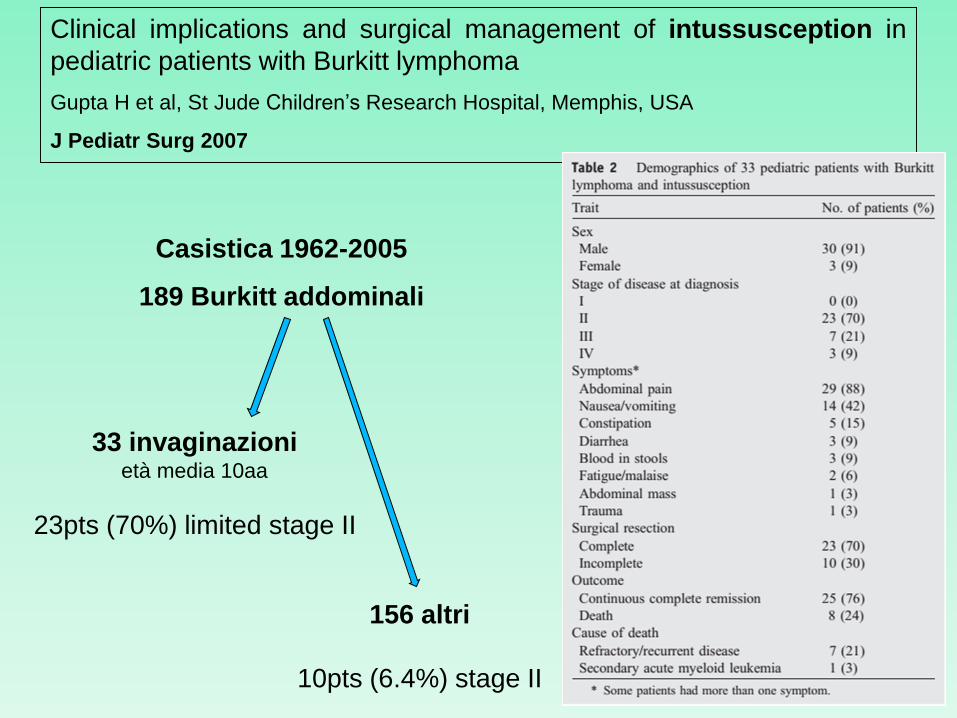
Casistica 1962-2005
189 Burkitt addominali
33 invaginazionietà media 10aa
23pts (70%) limited stage II
156 altri
10pts (6.4%) stage II
Clinical implications and surgical management of intussusception in
pediatric patients with Burkitt lymphoma
Gupta H et al, St Jude Children’s Research Hospital, Memphis, USA
J Pediatr Surg 2007

Wayne et al [J Pediatr Surg 1976] reported a series of 378
patients with intussusception; only 12 patients were older than 6
years, and 6 of these 12 patients had lymphosarcoma
(lymphoma).
Therefore, they recommended that in children older than 6 years, even if
hydrostatic reduction is done, extensive small bowel reflux should be observed and an
upper gastrointestinal series performed after the evacuation of barium to rule out any
pathologic lead points.
However, it is generally believed that intussusception caused by lymphomas is unlikely to
be completely reduced by an air-contrast or barium enema.
Intussusception - Lymphoma
Clinical implications and surgical management of intussusception in pediatric patients with Burkitt lymphoma,
Gupta H et al, J Pediatr Surg 2007

Surgical approach to intussusception in older children: Influence of lead points, Banapour P et al,
J Pediatr Surg 2015
Intussusception
Children older than 5 years are much more likely to have a pathologic
lead point and early surgical intervention should be considered. Enema
reduction was safe but minimally beneficial in this age group.
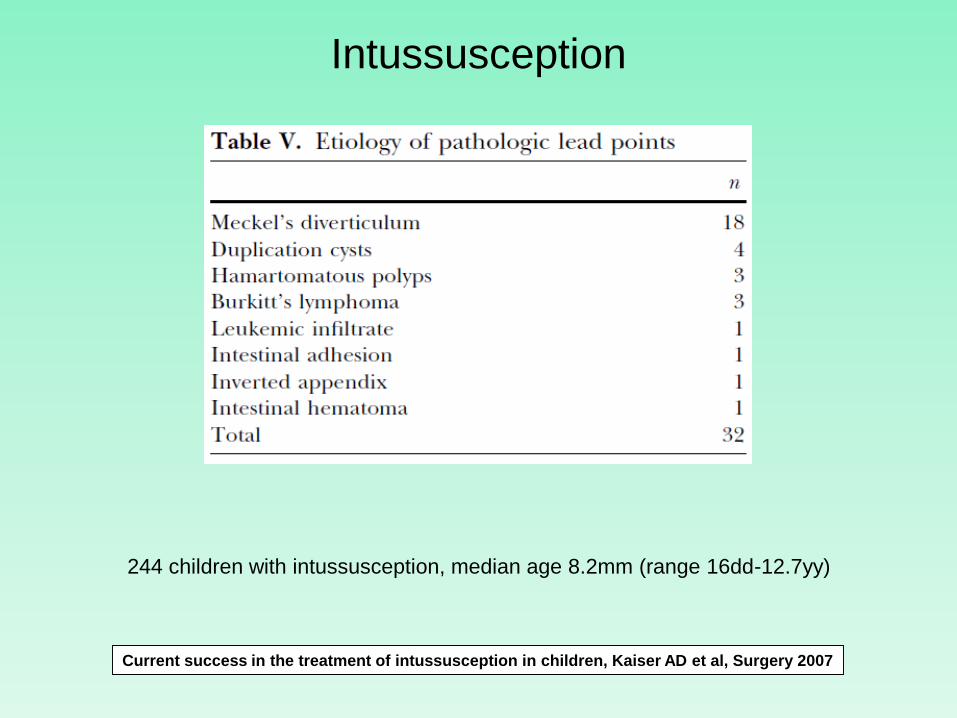
Intussusception
244 children with intussusception, median age 8.2mm (range 16dd-12.7yy)
Current success in the treatment of intussusception in children, Kaiser AD et al, Surgery 2007

Caso clinico 1 – C.F.
• 2 anni e 4 mesi, maschio, da circa 10 giorni coliche addominali ricorrenti,
episodi di vomito anche biliare, alvo tendenzialmente stitico (evacuazione di feci
abbondanti, gommose e di odore fetido dopo clisteri evacuativi), irritabilità,
inappetenza e perdita di peso
• Eco Addome c/o altra sede: sospetta invaginazione intestinale clinicamente
intermittente con immagine ecografica fissa da 48 ore (“in fianco-ipocondrio dx
persistenza di ansa intestinale di pertinenza colica, con aspetto “a bersaglio” con
Ø trasversale di 3.5cm ad estensione cranio-caudale di 7cm”)
• Trasferito c/o la nostra U.O.C.. Eco Addome: a livello della flessura colica
destra ansa intestinale fissa con immagine a coccarda tipica di invaginazione
intestinale; in corrispondenza della testa dell’invaginato si rileva un’immagine
rotondeggiante di circa 3x2.5cm, ad eco struttura omogeneamente fine.”
• Rx clisma opaco: non risoluzione dell’invaginazione
Caso clinico 1 – C.F.
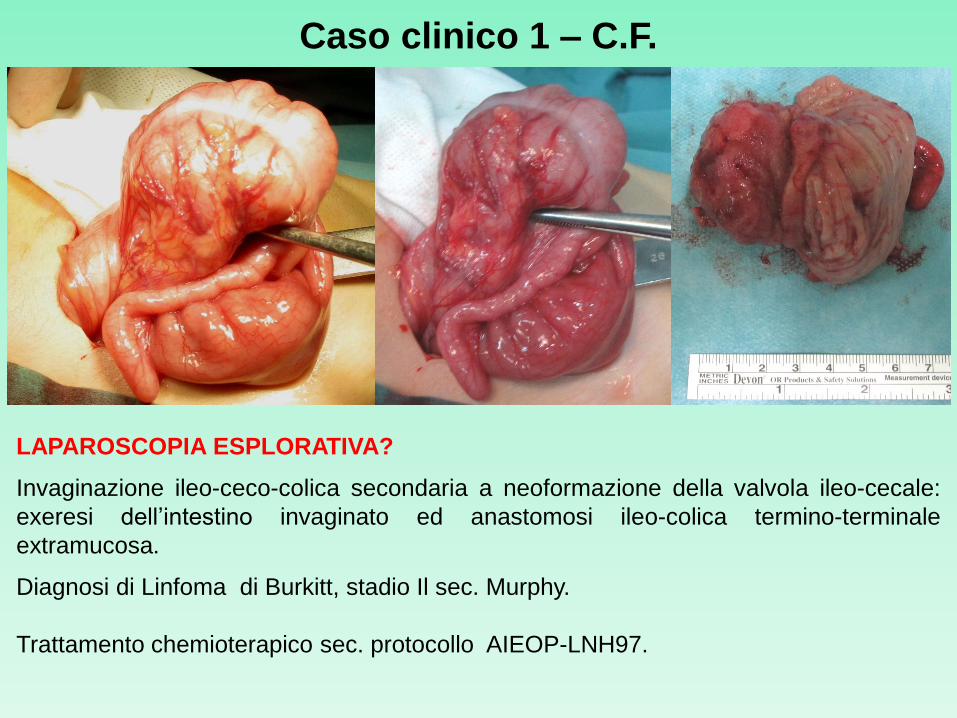
LAPAROSCOPIA ESPLORATIVA?
Invaginazione ileo-ceco-colica secondaria a neoformazione della valvola ileo-cecale:
exeresi dell’intestino invaginato ed anastomosi ileo-colica termino-terminale
extramucosa.
Diagnosi di Linfoma di Burkitt, stadio Il sec. Murphy.
Trattamento chemioterapico sec. protocollo AIEOP-LNH97.
Caso clinico 1 – C.F.

Quadro istopatologico a “cielo stellato” (starry sky), tipico del Linfoma di Burkitt

Caso clinico 2 – R.C.
• 11 mesi di età, femmina, circa 15 giorni prima episodio di gastroenterite
autolimitatosi. Da >24 ore la piccola ha iniziato ad accusare crisi di pianto
inconsolabile con flessione delle gambe e cosce sull’addome, intervallati da
episodi di sonno e prostrazione, alternati a nuove crisi di pianto. Comparsa di
vomito alimentare e successivamente evacuazione di feci miste a muco e sangue
• La paziente giunge c/o la nostra U.O.C.. Riscontro di materiale muco ematico al
sondaggio rettale
• Rx clisma opaco: “regolare risalita del mdc fino al colon ascendente ove si
osserva interruzione del lume. Dopo ripetuti tentativi: parziale opacizzazione del
cieco che appare dismorfico, con visualizzazione dell’appendice. Reperti riferibili
verosimilmente ad invaginazione con successiva parziale ricanalizzazione del
colon. Non opacizzata l’ultima ansa ileale.”

Caso clinico 2 – R.C.
Laparotomia (ore 2am) Invaginazione ileo-ceco-colica secondaria a
neoformazione polipoide sessile della valvola ileo-cecale: exeresi
dell’intestino invaginato ed anastomosi ileo-colica termino-terminale
extramucosa.
Diagnosi: iperplasia follicolare linfoide reattiva ileo-colica, appendicolare e
linfonodale – prevalente a carico della mucosa cecale e della valvola ileo-
cecale – associata a flogosi erosiva e ad aspetti rigenerativi dell’epitelio
ghiandolare.

Surgery at 3am
D.M. Hays (Los Angeles, CA): I would like you to visualize
yourself in the operating room at 3am with an intussusception
that can't be reduced by hydrostatic pressure and the question
comes up as to what it is. Is it an irreducible intussusception, is it
really a tumor, how do you make this distinction? Do you do
biopsies? Can you tell right away? How do you handle it?
M.P. LaQuaglia (response): I can't be definitive about I think that
many of these patients are going to present urgently and that
you just have to rely on surgical judgment. It may be that you will
have to do a sleeve resection. The only caveat, you can't do
cytogenetics and immunophenotyping on formalin tissue so that
some awareness of the possibility that an appendicitis,
intussusception, or bowel perforation may be a lymphoma may
be helpful in term of getting some of the tissue stored in the
refrigerator so that the more esoteric studies can be done.
The role of surgery in abdominal non-Hodgkin's lymphoma: experience from the Childrens
Cancer Study Group. LaQuaglia MP et al, J Pediatr Surg 1992

Paziente di 14 anni, maschio, da circa 24 ore vomito alimentare e quindi biliare
associato ad intenso e continuo dolore addominale, diffuso a tutti i quadranti ma
più accentuato in fossa iliaca destra, associato ad alvo chiuso alle feci da 5
giorni. Rx Diretta Addome: multipli livelli idro-aerei.
Caso clinico 3 – D. P. G.
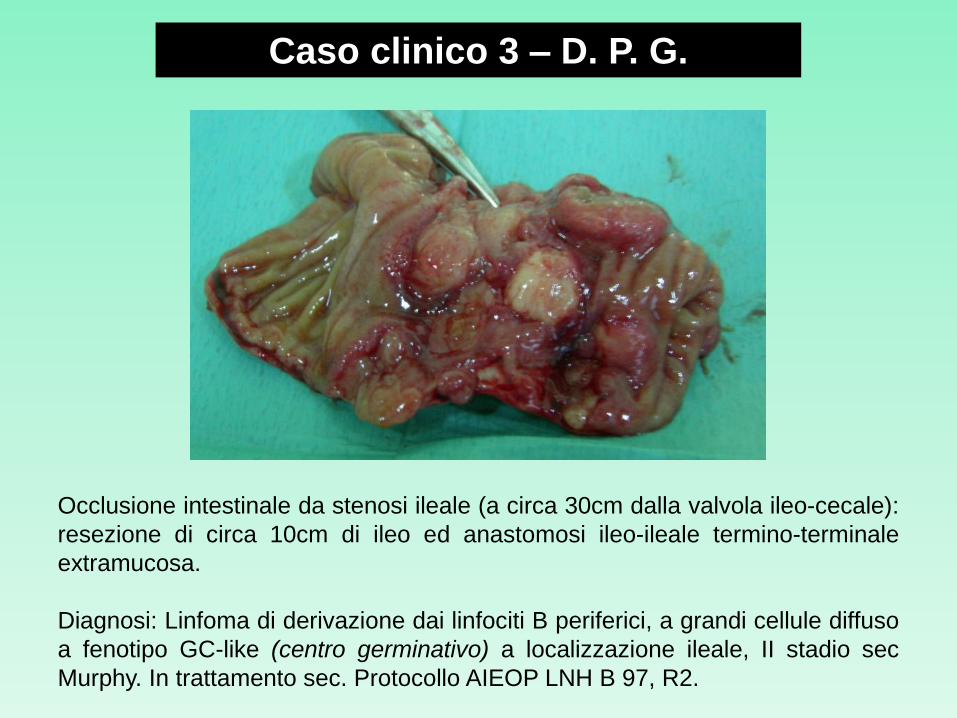
Occlusione intestinale da stenosi ileale (a circa 30cm dalla valvola ileo-cecale):
resezione di circa 10cm di ileo ed anastomosi ileo-ileale termino-terminale
extramucosa.
Diagnosi: Linfoma di derivazione dai linfociti B periferici, a grandi cellule diffuso
a fenotipo GC-like (centro germinativo) a localizzazione ileale, II stadio sec
Murphy. In trattamento sec. Protocollo AIEOP LNH B 97, R2.
Caso clinico 3 – D. P. G.

The surgeon’s approach to non-Hodgkin’s
lymphoma in the abdomen will be dictated by the
clinical scenario and anatomic findings.
Approximately half of the cases will involve the
gastrointestinal tract and the vast majority of those
will arise in the distal ileum or the right colon.
Most of the gastrointestinal lymphomas will present
as an acute abdomen due to tenderness or
obstruction and many are focal lesions that are
amenable to straightforward resection with
anastomosis.
RUOLO DELLA CHIRURGIA
Lymphoma, Billmire D.F., in The Surgery of Childhood Tumors 2nd edition, 2008

Surgical intervention is focused on either complete resection or palliative
intervention for the relief of bowel obstruction, in addition to a definitive
tumor biopsy.
Frozen section analysis of unexpected tumors should be obtained
intraoperatively to make a correct diagnosis and determine appropriate
therapy.
The mainstay of treatment for isolated gastrointestinal lymphoma is
complete surgical resection when possible, including excision of regional
lymph nodes.
Nearly 50% of children with gastrointestinal NHL will have tumor infiltrates
confined to the gastrointestinal tract with possible regional lymph node
involvement.
Children that are amenable to localized resection have an 80% survival at
2 years. Those children with more extensive spread of disease have a 33%
2-year survival.
RUOLO DELLA CHIRURGIA
Gastrointestinal tumors in children and adolescents, Ladd AP and Grosfeld JL, Sem Ped Surg 2006
?

Clinical implications and surgical management of
intussusception in pediatric patients with Burkitt lymphoma.
Gupta H et al, St Jude Children’s Research Hospital, Memphis, USA, J Pediatr Surg 2007
Today, almost all patients with stage II disease and over 80% of those with
stage III or IV disease can be cured with chemotherapy. Complete resection of
the tumor would allow less intensive therapy and improve quality of life of the
survivors.
Complete tumor resection with minimal complication is possible in most patients who
present with intussusception; thus, their stage of disease can be downgraded to
stage II.
Importantly, the surgeon should thoroughly explore all the peritoneal surfaces, collect
ascitic fluid, and examine liver, spleen, and retroperitoneal nodes. The presence of
residual disease indicates that the patient has stage III disease and requires a much
more intense chemotherapy regimen for cure.
If extensive disease is noted in the abdomen such that complete resection is not
feasible, biopsy alone should be done.
Aggressive surgical resection should be avoided in cases of advanced disease,
because this approach not only would fail to completely resect the disease, but could
increase the risk of surgical complications and delay the start of curative
chemotherapy.

Primary gastrointestinal tract lymphoma in the pediatric patient: review of 265 patients
from the SEER registry. Kassir N et al, J Pediatr Surg 2011
RUOLO DELLA CHIRURGIA NEI LINFOMI
GASTRONTESTINALI PEDIATRICI
RUOLO DELLA CHIRURGIA NEI LINFOMI
GASTRONTESTINALI PEDIATRICI
In our evaluation of the 265 pediatric patients in the SEER
(Surveillance, Epidemiology and End Result) database from 1973 to
2006, by univariate analysis, surgery did not improve long-term
survival but was found to significantly decrease 10-year overall
and DSS in patients 10 years or older. There was no difference in
overall or DSS for those younger than 10 years who underwent
surgical extirpation.
Primary gastrointestinal tract lymphoma in the pediatric patient: review of 265 patients
from the SEER registry. Kassir N et al, J Pediatr Surg 2011
Without question, urgent surgery is required in patients with primary
GI tract lymphomas who develop obstruction or perforation of the
alimentary tract. However, in cases where these clinical findings are not
present, arguments against the use of surgery have been largely based on
the rate of surgical complications requiring prolonged hospitalizations and
leading to delays in the initiation of chemotherapy.

Burkitt lymphoma
Bowel Obstruction after Treatment of Intra-Abdominal Tumors, Aguayo P et al,
Eur J Pediatr Surg 2010
In the patients with Burkitt’s lymphoma who underwent
an abdominal operation, the incidence of p.o. small bowel
obstruction was 17.6%. As in procedures to resect Wilm’s
tumor or rhabdomyosarcoma, operations for Burkitt’s
lymphoma are often major procedures.

Abdominal Burkitt’s Lymphoma
Diagnosis in Childhood Abdominal Burkitt’s Lymphoma, Vural S et al, Ann Surg Oncol 2010

Caso clinico 4 – A. I.
• Paziente di 4 anni, femmina, ricovero c/o la ns. UOC il 12.06 per addome
globoso e riscontro accidentale di massa addominale sinistra all’esame
ecografico (formazione solida diffusamente ipo-ecogena, Ø 10x8cm,
polilobulata con aree necrotico-emmorragiche al suo interno ed aree di
vascolarizzazione all’eco-color doppler.
• TC Addome con mdc 15.06 massa Ø 20x14cm a contenuto disomogeneo
senza calcificazioni, posta lateralmente allo stomaco dislocato verso destra,
anteriore a milza e pancreas, che si estende in basso fino allo scavo pelvico;
evidenti aree di consolidamento in sede polmonare basale bilateralmente.
• 16.06 biopsia percutanea eco-guidata con Tru-cut e posizionamento di
CVC tipo Broviac
• Diagnosi istologica: Linfoma non Hodgkin a grandi cellule B diffuso cs III,
sottoposta a trattamento sec. protocollo AIEOP LNH97 gruppo R4.

Caso clinico 4 – A. I.
• Durante il trattamento le dimensioni della lesione sono state controllate mediante Eco
addome a cadenza bisettimanali. Rivalutazione TC addome a 2 mesi (17.08):
riduzione dimensioni della massa (Ø 11x6cm), scomparsa delle aree di consolidazione
parenchimale in sede polmonare basale bilateralmente.
• Data la modesta riduzione della massa alla TC addome a 3 mesi (12.09), Ø 8x4cm, ed
alla Eco addome del 05.10 (Ø 8x5cm), si esegue second look chirurgico il 13.10:
laparotomia sovra-ombellicale trasversa sinistra, exeresi en bloc della massa tumorale
tenacemente adesa all’ilo splenico ed alla coda del pancreas, con asportazione di
piccola area della coda del pancreas e tessuto splenico polare inferiore (1cm), con
conservazione della milza.
• Esame istologico: massa diffusamente necrotica con reazione xantomatosa.
• Alla luce del quadro anatomo-patologico, non essendovi evidenza di malattia attiva, si
conviene di sottoporre la paziente ad un ultimo ciclo di chemioterapia, non sussistendo
indicazione a terapia ad alte dosi.
RUOLO DELLA CHIRURGIA NEI LINFOMI
GASTRONTESTINALI PEDIATRICI
La chirurgia gioca ancora un ruolo importante in situazioni
esattamente definite:
• resezione completa della malattia localizzata
• trattamento della malattia complicata (occlusione intestinale,
invaginazione, perforazione…)
• biopsia diagnostica *
• second look
N.B. * Va evitato qualunque intervento di chirurgia maggiore che possa portare ad
una più alta incidenza di complicanze post-operatorie e conseguentemente
ad un ritardo nell’inizio della chemioterapia.
Clinico-Pathological Features and Outcome of Management of Pediatric Gastrointestinal
Lymphoma. Morsi A et al, J Egypt Natl Canc Inst. 2005

Today, almost all patients with stage IIdisease and over 80% of those with stage IIIor IV disease can be cured withchemotherapy. Complete resection of thetumor would allow less intensive therapyand improve quality of life of the survivors.
Clinical implications and surgical management of intussusception in pediatric patients with Burkitt lymphoma.Gupta H et al, St Jude Children’s Research Hospital, Memphis, USA, J Pediatr Surg 2007

RUOLO DELLA LAPAROSCOPIA
Diagnostico
• Come tempo preliminare essenziale in ogni paziente >5-6 anni con
invaginazione non riducibile
• Per esplorare accuratamente le superfici peritoneali, collezionare liquido
ascitico ed esaminare fegato, milza e linfonodi retroperitoneali
• Per prelievi bioptici in caso di malattia estesa
• Anche come second look post-chemioterpia
Terapeutico?
“The open surgical approach is still the gold standard in most pediatric
surgical facilities.”
Ileocolic intussusception due to Burkitt lymphoma: a case report
Balanescu NR et al, J Med Life 2013