root coverage outcome may be affected by heavy smoking: a 2-year follow-up study
TRANSCRIPT

Root Coverage Outcome May BeAffected by Heavy Smoking: A 2-YearFollow-Up StudyDenise C. Andia,* Angela G. Martins,† Marcio Z. Casati,‡ Enilson A. Sallum,‡
and Francisco H. Nociti Jr.‡
Background: Although subepithelial connective tissue graft(CTG) has been reported to be a predictable procedure for rootcoverage, the impact of smoking on the long-term outcome ofperiodontal plastic surgery is unclear. Hence, the aim of thisstudy was to evaluate the effect of smoking, on a long-term ba-sis, on the stability of gingival tissue following CTG treatmentof gingival recession.
Methods: Twenty-two defects were treated by CTG in ca-nine and premolar Miller Class I and II gingival recessions(11 smokers and 11 non-smokers). The following clinical mea-surements were obtained at baseline and at 1, 2, 3, 4, 6, 12,18, and 24 months after surgery: plaque and gingival indexes,extension of gingival recession (GR),probing depth (PD), clinicalattachment level (CAL), and gingival thickness. Individualssmoking ‡20 cigarettes/day for ‡5 years were consideredsmokers.
Results: Data analysis demonstrated that both groups pre-sented similar plaque and gingival indexes (P >0.05), and anintragroup analysis showed that CTG was able to promoteroot coverage and increase gingival thickness in both groupsover time (P <0.05). However, at 24 months postoperatively,statistical analysis showed that smokers presented pooreroutcomes with regard to PD, GR, and CAL (P <0.05); in addi-tion, a more satisfactory stabilization of the gingival tissue wasfound in the non-smoker group.
Conclusion: Smoking may represent a challenge to rootcoverage outcome for CTG because smoking significantly af-fected the stability of gingival tissue over time. J Periodontol2008;79:647-653.
KEY WORDS
Follow-up studies; gingival recession; root coverage;smoking.
Gingival recession, i.e., the locationof marginal tissue apical to thecemento-enamel junction (CEJ),
leading to an exposed root surface, is acommon periodontal problem; the prev-alence for adults older than 30 yearsmay be as high as 58%.1 The clinicalindications for exposed root coverageare esthetic need, and management ofroot hypersensitivity, cervical abrasions,and shallow root caries lesions.2 Variousmethods for performing mucogingivalgrafts to cover denuded root surfacesare available: these include the coro-nally positioned flap,3 laterally slidingflap,4 free gingival graft plus coronallypositioned flap,5 and acellular dermalmatrix graft.6 Since the introduction ofthe subepithelial connective tissue graft(CTG) in the 1980s,7,8 an enhancedpredictability for obtaining esthetic rootcoverage has been reported,9,10 estab-lishing this technique as a standard pro-cedure for the treatment of gingivalrecession (GR).9
In an animal model, cigarette smokingreduced the self-healing capacity of peri-odontal tissues.11 Human studies havesuggested that the damaging effects ofsmoking may manifest mainly by dis-turbing the vascular12-14 and immu-nologic systems,15,16 which are basiccomponents of the host response. Hence,smoking may adversely affect healing insubjects following periodontal therapy.Experimental evidence demonstrated that
* Department of Morphology, School of Dentistry at Piracicaba, University of Campinas,Piracicaba, SP, Brazil.
† Department of Health, Feira de Santana State University, Feira de Santana, BA, Brazil.‡ Department of Prosthodontics and Periodontics, Division of Periodontics, School of
Dentistry at Piracicaba, University of Campinas.
doi: 10.1902/jop.2008.070471
J Periodontol • April 2008
647

cigarette smoking is associated with poorer periodon-tal therapy outcomes17,18 and with a potential negativeimpact on the results of root coverage on a short-termbasis.19-23 Thus, this study was designed to evaluatethe effect of smoking, following CTG treatment of GRdefects, and the stability of gingival tissue for 2 yearsafter surgery.
MATERIALS AND METHODS
Subjects and Recession DefectsAll subjects were selected consecutively from patientsreferred for dental treatment to the School of Dentistryat Piracicaba, State University of Campinas. Thesepatients had requested treatment for esthetic and/ordentin hypersensitivity by a root coverage procedureduring the period of March 2002 to December 2003.The study was approved by the Ethical Committee forResearch of the State University of Campinas, andinformed consent was signed by each subject afterexplanations were provided. Based on previous stud-ies from our group and a preliminary study,20,21 thesample size was determined by sample-size calcula-tions for a power of 0.80 with a = 0.05. The inclusioncriteria were as follows: individuals were periodontallyand systemically healthy and had not taken any med-ications that could interfere with periodontal tissuehealing; none of the participants exhibited probingdepths >3 mm; each patient had at least one MillerClass I or II24 buccal GR involving either a maxillarycanine or premolar or mandibular premolars; defectswere ‡3 mm deep and 4 mm wide and presented amargin of ‡2 mm keratinized tissue surrounding thedefect. For cases with multiple recessions, root hyper-sensitivity and esthetic and/or cosmetic needs wereconsidered to decidewhich recession would be treated.Twenty-two subjects were included in this parallelsingle-maskedstudy(11smokersand11non-smokers;eight men and 14 women aged 27 to 55 years [meanage: 39.64 – 6.48 years]). In the present 2-year study,seven subjects were added to the 15 subjects (sevensmokers and eight non-smokers) reported previouslyin the original 4-month evaluation,20 who also com-pleted the 2-year follow-up. Individuals were consideredheavy smokers if they had smoked ‡20 cigarettes perday for ‡5 years prior to the beginning of the study;occasional and former smokers were excluded. Thesmoking status of all subjects enrolled in the presentstudy was confirmed continuously over time to makesure that it remained the same as at the beginning ofthe study. Individuals who had never smoked made upthe non-smoker group.
Initial Treatment and Clinical ParametersAll subjects received an initial treatment consisting of acomplete periodontal examination, explanations to
eliminate the habits related to the cause of recession(use of a traumatic brushing technique and a hardtoothbrush), oralhygiene instructions and prophylaxis,removal of plaque-retentive areas, and multiple ses-sions of scaling and root planing. After 8 weeks, whenthe subjects demonstrated an acceptable standard oforal hygiene, the following parameters were evaluated(immediatelybefore surgery); they were reevaluated at1, 2, 3, 4, 6, 12, 18, and 24 months after surgery. Thepresence of plaque and bleeding on probing were re-corded dichotomously at the buccal aspect of the toothto be treated.25 PD was measured using an automatedperiodontal probe,§ GR was measured as the distancebetween the CEJ and the most apical point of thegingival margin of the buccal surface of the tooth,and clinical attachment level (CAL) was measured asthe distance from the CEJ to the base of the pocket.Pre- andpost-surgical gingival thickness (GT) wasob-tained in a mid-buccal location ;2 mm apical to thegingival margin as follows: a #15 endodontic reamerwas pierced perpendicularly to the mucosal surfacethrough the soft tissue with light pressure until a hardsurface was felt; a silicone disk stop was placed in tightcontact with the soft tissue surface and stabilized by adrop of an adhesive, and penetration depth was ob-tained with a digital caliper to the nearest 0.1 mm.Clinical parameters were obtained by one calibratedexaminer (intraclass correlation = 0.94).
Surgical ProcedureSurgical procedures were carried out by one operator,masked to the smoking status of the subject. Extraoralantisepsis was performed with a 2.0% chlorhexidinesolution, and intraoral antisepsis was performed witha 0.12% chlorhexidine rinsei for 1 minute; local anes-thesia was obtained with 2% lidocaine and 1:100,000epinephrine. At the level of the CEJ, an intrasulcularincision was made horizontally to the center of the in-terdental gingiva mesial and distal to the defects, andtwo apically divergent vertical incisions were made.The full-thickness flap was continued approximately3 to 5 mm beyond the mucogingival junction as a par-tial-thickness flap to enable coronal elongation of theflap, without tension.26 The papillae that were mesialand distal to the recession defects were deepithelial-ized to provide an appropriate wound bed for healing.Following flap elevation, the exposed root surface wasscaled and planed gently with sharp curets. Donorconnective tissue was obtained from the palate usinga previously described technique8 and was positionedimmediately on the root surface. The graft stabilitywas achieved by two interproximal bioabsorbable4-0 sutures,¶ and the flap was positioned coronally
§ Florida Probe, Gainesville, FL.i Proderma Farmacia de Manipulacxao, Piracicaba, SP, Brazil.¶ Vicryl, Ethicon, Somerville, NJ.
Smoking and Root Coverage Volume 79 • Number 4
648
to cover the graft. It was sutured in position with inter-rupted sutures,# with special care to avoid excessiveflap tension.
Post-Surgical CareThe subjects were instructed to consume only softfoods during the first week after surgery. Acetamino-phen was prescribed for pain control, and the subjectswere told to use a 0.12% chlorhexidine rinse twice aday for 8 days without brushing and flossing the sur-gical areas. Sutures were removed 8 to 10 days aftersurgery, and 0.12% chlorhexidine was applied locallyover the surgical sites with a cotton swab twice a dayfor 1 month. After 30 days, subjects reestablished me-chanical plaque control in the area of the recession.This healing phase was supplemented by professionalplaque control, performed by the same operator whoprovided the surgical procedure, every 2 weeks for thefirst 2 months after surgery.
Statistical AnalysisData are reported as medians and ranges, and all sta-tistical analyses were performed using a statisti-cal program.** The non-parametric Mann-Whitneyand Friedman tests were used to detect differencesbetween the groups and within each group, respec-tively, for all evaluated parameters over time. Thelevel of significance was set at 5%. Twenty-two sub-jects were considered the unit of analysis for all ana-lyses.
RESULTS
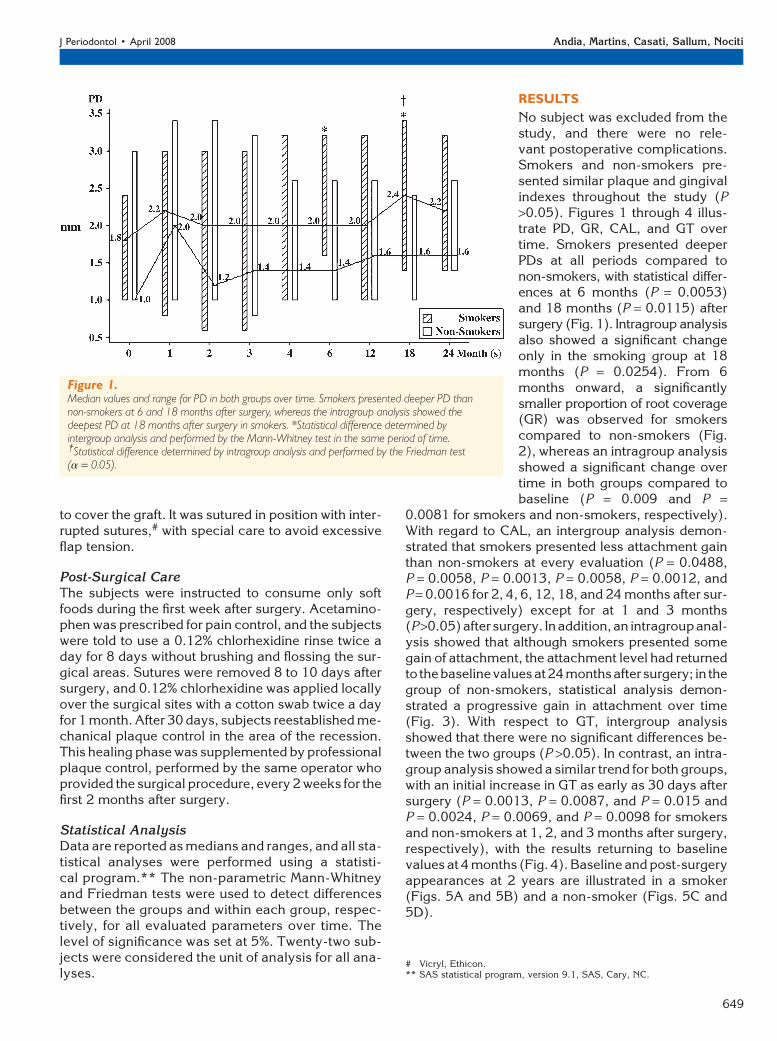
No subject was excluded from thestudy, and there were no rele-vant postoperative complications.Smokers and non-smokers pre-sented similar plaque and gingivalindexes throughout the study (P>0.05). Figures 1 through 4 illus-trate PD, GR, CAL, and GT overtime. Smokers presented deeperPDs at all periods compared tonon-smokers, with statistical differ-ences at 6 months (P = 0.0053)and 18 months (P = 0.0115) aftersurgery (Fig. 1). Intragroup analysisalso showed a significant changeonly in the smoking group at 18months (P = 0.0254). From 6months onward, a significantlysmaller proportion of root coverage(GR) was observed for smokerscompared to non-smokers (Fig.2), whereas an intragroup analysisshowed a significant change overtime in both groups compared tobaseline (P = 0.009 and P =
0.0081 for smokers and non-smokers, respectively).With regard to CAL, an intergroup analysis demon-strated that smokers presented less attachment gainthan non-smokers at every evaluation (P = 0.0488,P = 0.0058, P = 0.0013, P = 0.0058, P = 0.0012, andP = 0.0016 for 2, 4, 6, 12, 18, and 24 months after sur-gery, respectively) except for at 1 and 3 months(P >0.05)after surgery. Inaddition,an intragroupanal-ysis showed that although smokers presented somegain of attachment, the attachment level had returnedto thebaselinevaluesat24monthsafter surgery; in thegroup of non-smokers, statistical analysis demon-strated a progressive gain in attachment over time(Fig. 3). With respect to GT, intergroup analysisshowed that there were no significant differences be-tween the two groups (P >0.05). In contrast, an intra-group analysis showed a similar trend for both groups,with an initial increase in GT as early as 30 days aftersurgery (P = 0.0013, P = 0.0087, and P = 0.015 andP = 0.0024, P = 0.0069, and P = 0.0098 for smokersand non-smokers at 1, 2, and 3 months after surgery,respectively), with the results returning to baselinevalues at 4 months (Fig. 4). Baseline and post-surgeryappearances at 2 years are illustrated in a smoker(Figs. 5A and 5B) and a non-smoker (Figs. 5C and5D).
Figure 1.Median values and range for PD in both groups over time. Smokers presented deeper PD thannon-smokers at 6 and 18 months after surgery, whereas the intragroup analysis showed thedeepest PD at 18 months after surgery in smokers. *Statistical difference determined byintergroup analysis and performed by the Mann-Whitney test in the same period of time.†Statistical difference determined by intragroup analysis and performed by the Friedman test(a = 0.05).
# Vicryl, Ethicon.** SAS statistical program, version 9.1, SAS, Cary, NC.
J Periodontol • April 2008 Andia, Martins, Casati, Sallum, Nociti
649

DISCUSSION
The aim of this study was to longitudinally comparethe stability of the gingival tissue in smokers andnon-smokers who received CTG as a treatment for
Miller Class I and II GR defects.The results demonstrated thatCTG might provide benefits forsmokers and non-smokers, de-creasing the extension of GR andincreasing GT. However, even un-der the high oral hygiene standardsthat were maintained throughoutthe entire study period and withsimilar plaque and gingival in-dexes between groups, smokerspresented deeper PDs, larger resid-ual GR, and less gain of attachment.Thus, cigarette consumption sig-nificantly affected therapy out-come because the root coverageobtained with CTGs was reducedin the smoking group, and conse-quently, smokers presented a ten-dency toward greater residual GRover time.
Silva et al.21 treated Miller ClassI GR defects in 10 smokers and 10non-smokers, using the coronallypositioned flap (CPF). After 6months, smokers presented a sig-nificantly lower mean percentageof root coverage than non-smokers(69.3% and 91.3%, respectively),with a higher frequency of completeroot coverage in non-smokers(0% versus 50%). Trombelli andScabbia22 analyzed the results ofnine smokers and 13 non-smokerspresenting Miller Class I or II GR de-fects that were treated by guidedtissue regeneration (GTR). At 6months, the mean root coveragewas lower in smokers (57% versus78%), and complete root coveragewas significantly greater in non-smokers. Erley et al.23 treated 22Miller Class I or II GR defects byCTG; at 6 months, the mean rootcoverage was lower in smokers(98.3% versus 82.3%), and com-plete root coverage was signifi-cantly greater in non-smokers(80% versus 25%). Miller19 treatedsubjects with free gingival graftsand reported a 100% correlationbetween failure to obtain root cov-
erage and heavy smoking. Limited information isavailable with respect to the impact of smoking onroot coverage outcome on a long-term basis. In arecent report, Silva et al.27 followed 20 subjects for
Figure 2.Median and range for the residual extension of GR in both groups over time. There was asignificant reduction of the GR extension in smokers and non-smokers as early as 30 days aftersurgery compared to baseline. In addition, there was an increase in the residual extension of GR insmokers starting at 6 months after surgery, whereas non-smokers tended to present a decrease inthe residual GR extension. *Statistical difference determined by intergroup analysis and performedby the Mann-Whitney test in the same period of time. †Statistical difference determined byintragroup analysis and performed by the Friedman test (a = 0.05).
Figure 3.Median and range for CAL over time. There was a trend for clinical attachment gain in bothgroups, but non-smokers had more gain, starting as early on as at 60 days after surgery.*Statistical difference determined by intergroup analysis and performed by the Mann-Whitneytest in the same period of time. The letters (a, b, c, ab, and bc) represent the statistical differencesbetween the evaluated periods (baseline and 1, 2, 3, 4, 6, 12, 18, and 24 months) determined byintragroup analysis and performed by the Friedman test (a = 0.05).
Smoking and Root Coverage Volume 79 • Number 4
650

24 months and showed that smokers presented asignificantly greater residual recession comparedto non-smokers following CPF (1.28 – 0.58 mmand 0.50 – 0.41 mm for smokers and non-smokers,respectively).
Regardless of the fact that dif-ferent procedures, including CTG,CPF, free gingival graft, andGTR, were used in these stud-ies,19,21-23,27 the findings of thepresent longitudinal investigationare in line with these previous re-ports showing less root coveragefor smokers. In the present study,after 6 months, smokers pre-sented a tendency toward an in-crease in root exposure, leadingto a slight recurrence in GR,whereas the opposite tendencywas found for non-smokers overtime. The percentage of root cov-erage after 2 years was 50% (1.8mm; range of residual recession:1.0 to 2.6 mm) and 77.8% (2.8mm; range of residual recession:0.0 to 1.8 mm) for smokers andnon-smokers, respectively.There-fore, although both groups pre-sented some creeping attachment,this was more evident for non-smokers. In the present 2-yearstudy, complete root coverage wasfound in 27% of the non-smokers,whereas none of the smokers pre-sented complete root coverage. Inthis regard, similar findings werereported by Silva et al.,27 who re-ported complete root coverage for20% of the non-smokers at 2 yearsafter CPF surgeries, whereas noneof the smokers obtained 100%root coverage. In contrast to thesestudies,19,21-23,27 some reports28-30
did not find any association be-tween poor root coverage out-come and smoking. The reasonsfor these different findings arenot clear, but they may reflectthe fact that none of these studieswas designed to assess the effectof smoking after root coverageprocedures.
CAL, the distance from the CEJto the base of the pocket/sulcus,and PD, the distance from the gin-gival margin to the base of the
pocket/sulcus, are used frequently to assess peri-odontal treatment outcomes. In the present study,smoking resulted in significantly deeper PD and lessgain of attachment over time in the sites treated withCTG. These results are in agreement with several
Figure 5.Upper canine in a smoker at baseline (A) and at 24 months post-surgery (B). First upper molarin a non-smoker at baseline (C) and at 24 months post-surgery (D).
Figure 4.Median and range for GT in both groups over time. A similar trend was found for both groups, withan initial increase as early as 30 days after surgery; results returned to the baseline values startingat 4 months. The letters (a, c, ab, bc, and abc) represent the statistical differences between theevaluated periods (baseline and 1, 2, 3, 4, 6, 12, 18, and 24 months) determined by intragroupanalysis and performed by the Friedman test. There were no intergroup differences (a = 0.05).
J Periodontol • April 2008 Andia, Martins, Casati, Sallum, Nociti
651

other studies that emphasized that smoking nega-tively influenced treatment outcomes in terms of PDreduction and CAL gain. These investigations re-ported data for studies on CTG treatment20,23 as wellas for non-surgical periodontal therapy.31-34 Jinet al.31 reported that smokers had different treatmentresponse patterns and healing dynamics compared tonon-smokers following non-surgical therapy, suggest-ing the importance of a more intensive treatment regi-men for smoking subjects.
With respect to GT, we reported previously that GT,when achieved soon after surgery (30 days), pre-sented a tendency to decrease after 4 months of fol-low-up.20 In the present study, the tendency for adecrease in GT continued to be observed in a similarfashion for smokers and non-smokers 24 months af-ter surgery, with the GT reaching the baseline valuesas early as 120 days after surgery. Although thevalues were similar in both groups, smokers had aslightly thicker gingival tissue at the end of the study;in addition, smokers presented greater keratinized tis-sue during the entire experiment (data not shown).
In general, the precise mechanisms by which ciga-rette smoking interferes with root coverage remainunclear. It was reported that smoking has a primaryinfluence on the self-healing capacity of periodontaltissues,11 possibly by disturbing the vascular12-14
and immunological systems.15,16 Nicotine was alsoshown to affect in vitro gingival fibroblast prolifera-tion, increase collagenase activity,35 and inhibit fibro-blast synthesis of fibronectin and type I collagen.36
Moreover, impaired oxygen transport and metabo-lism, caused by carbon monoxide or enzyme poison-ing by hydrogen cyanide, further reduce the oxidativemetabolism needed for cellular repair.37 Althoughthese changes could contribute to the poorer healingreported for smokers, further studies are required todetermine the mechanisms by which smoking nega-tively influences the long-term outcome following rootcoverage procedures.
The stability of the gingival margin following CTG totreat Miller Class I and II recession defects was reportedfor non-smokers. For the present investigation, the fi-nal root coverage obtained for the group of non-smokers after 6 months (77%) and 2 years (78%)is within the range of 52% to 99%, as reported byBouchard et al.9 in a review of 11 studies at 6 months,and 84.3% at 2 years, as reported by Moses et al.38 Inthe present study, because of the ethical reasons in-volved, the subjects were informed about the possiblenegative effects of smoking on the periodontal tissuesafter the surgery as well as on their general health. Thesubjects were encouraged to quit smoking during therecall visits. None of the subjects quit smoking duringthe experimental period; therefore, all smokers ini-tially enrolled in the study were followed over time.
CONCLUSIONS
To the best of our knowledge, this was the first com-parative and longitudinal evaluation of the stabilityof the periodontal tissues in smokers versus non-smokers following CTG. Smoking significantly af-fected the long-term stability of CTG outcome, withsmokers presenting a greater residual recession at2 years. Taken together, the data presented hereinand from other studies19,21-23,27 strongly suggest anassociation between smoking and poor root coverageoutcome and failure, regardless of the surgical proce-dure used. Future investigations are necessary andshould address whether smoking status (light, moder-ate, or severe) affects clinical outcome differentially,whether smoking cessation improves therapy out-come, and alternative approaches to provide smokerswith reliable and predictable results.
ACKNOWLEDGMENTS
Dr. Nociti was supported by the National ResearchCouncil, Brazil (grant 305471/2006-6). In addition,the authors thank Prof. Glaucia Maria Ambrosano,Department of Biostatistics, University of Campinas,for her assistance with the statistical analyses of thedata. The authors report no conflicts of interest relatedto this study.
REFERENCES1. Albandar JM, Kingman A. Gingival recession, gingival
bleeding, and dental calculus in adults 30 years of ageand older in the United States, 1988-1994. J Peri-odontol 1999;70:30-43.
2. Wennstrom J, Pini Prato GP. Mucogingival therapy.In: Lindhe J, Karring T, Lang NP, eds. Clinical Peri-odontology and Implant Dentistry. Copenhagen:Munksgaard; 1997:569-591.
3. Harris RJ, Harris AW. The coronally positioned pediclegraft with inlaid margins: A predictable method ofobtaining root coverage of shallow defects. Int JPeriodontics Restorative Dent 1994;14:228-241.
4. Guinard EA, Caffesse RG. Treatment of localizedgingival recessions. Part I: Lateral sliding flap. J Peri-odontol 1978;49:351-356.
5. Caffesse RG, Guinard EA. Treatment of localized gin-gival recessions. Part II: Coronally repositioned flap witha free gingival graft. J Periodontol 1978;49:357-361.
6. Cortes Ade Q, Martins AG, Nociti FH Jr., Sallum AW,Casati MZ, Sallum EA. Coronally positioned flap withor without acellular dermal matrix graft in the treat-ment of Class I gingival recessions: A randomizedcontrolled clinical study. J Periodontol 2004;75:1137-1144.
7. Raetzke PB. Covering localized areas of root exposureemploying the ‘‘envelope’’ technique. J Periodontol1985;56:397-402.
8. Langer B, Langer L. Subepithelial connective tissuegraft technique for root coverage. J Periodontol1985;56:715-720.
9. Bouchard P, Malet J, Borghetti A. Decision-making inaesthetics: Root coverage revisited. Periodontol 20002001;27:97-120.
Smoking and Root Coverage Volume 79 • Number 4
652

10. Harris RJ. The connective tissue and partial thicknessdouble pedicle graft: A predictable method of obtain-ing root coverage. J Periodontol 1992;63:477-486.
11. Benatti BB, Cesar-Neto JB, Goncalves PF, Sallum EA,Nociti FH Jr. Smoking affects the self-healing capacityof periodontal tissues. A histological study in the rat.Eur J Oral Sci 2005;113:400-403.
12. Bergstrom J, Bostrom L. Tobacco smoking and peri-odontal hemorrhagic responsiveness. J Clin Periodon-tol 2001;28:680-685.
13. Nair P, Sutherland G, Palmer R, Wilson RF, Scott DA.Gingival bleeding on probing increases after quittingsmoking. J Clin Periodontol 2003;30:435-437.
14. Morozumi T, Kubota T, Sato T, Okuda K, Yoshie H.Smoking cessation increases gingival blood flow andgingival crevicular fluid. J Clin Periodontol 2004;31:267-272.
15. Morozumi T, Kubota T, Sugita N, Itagaki M, Yoshie H.Alterations of gene expression in human neutrophilsinduced by smoking cessation. J Clin Periodontol2004;31:1110-1116.
16. Soder B, Jin LJ, Wickholm S. Granulocyte elastase,matrix metalloproteinase-8 and prostaglandin E2 ingingival crevicular fluid in matched clinical sites insmokers and non-smokers with persistent periodonti-tis. J Clin Periodontol 2002;29:384-391.
17. Kaldahl WB, Johnson GK, Patil KD, Kalkwarf KL.Levels of cigarette consumption and response toperiodontal therapy. J Periodontol 1996;67:675-681.
18. Johnson GK, Hill M. Cigarette smoking and the peri-odontal patient. J Periodontol 2004;75:196-209.
19. Miller PD Jr. Root coverage with the free gingival graft.Factors associated with incomplete coverage. J Peri-odontol 1987;58:674-681.
20. Martins AG, Andia DC, Sallum AW, Sallum EA, CasatiMZ, Nociti FH Jr. Smoking may affect root coverageoutcome: A prospective clinical study in humans. JPeriodontol 2004;75:586-591.
21. Silva CO, Sallum AW, Lima AFM, Tatakis DN. Coro-nally positioned flap for root coverage: Poorer out-comes in smokers. J Periodontol 2006;77:81-87.
22. Trombelli L, Scabbia A. Healing response of gingivalrecession defects following guided tissue regenerationprocedures in smokers and non-smokers. J ClinPeriodontol 1997;24:529-533.
23. Erley KJ, Swiec GD, Herold R, Bisch FC, Peacock ME.Gingival recession treatment with connective tissuegrafts in smokers and non-smokers. J Periodontol2006;77:1148-1155.
24. Miller PD. A classification of marginal tissue recession.Int J Periodontics Restorative Dent 1985;5(2):8-13.
25. Ainamo J, Bay I. Problems and proposals for record-ing gingivitis and plaque. Int Dent J 1975;25:229-235.
26. Pini Prato G, Pagliaro U, Baldi C, et al. Coronallyadvanced flap procedure for root coverage. Flap withtension versus flap without tension: A randomized
controlled clinical study. J Periodontol 2000;71:188-201.
27. Silva CO, de Lima AF, Sallum AW, Tatakis DN.Coronally positioned flap for root coverage in smokersand non-smokers: Stability of outcomes between 6months and 2 years. J Periodontol 2007;78:1702-1707.
28. Tolmie PN, Rubins RP, Buck GS, Vagianos V, Lanz JC.The predictability of root coverage by way of freegingival autografts and citric application: An evalua-tion by multiple clinicians. Int J Periodontics Restora-tive Dent 1991;11:261-271.
29. Harris RJ. The connective tissue with partial thicknessdouble pedicle graft: The results of 100 consecutively-treated defects. J Periodontol 1994;65:448-461.
30. Amarante ES, Leknes KN, Skavland J, Lie T. Coro-nally positioned flap procedures with or without abioabsorbable membrane in the treatment of humangingival recession. J Periodontol 2000;71:989-998.
31. Jin L, Wong KY, Leung WK, Corbet EF. Comparison oftreatment response patterns following scaling and rootplaning in smokers and non-smokers with untreatedadult periodontitis. J Clin Dent 2000;11:35-41.
32. Bergstrom J, Eliasson S, Dock J. A 10-year prospec-tive study of tobacco smoking and periodontal health.J Periodontol 2000;71:1338-1347.
33. Tomasi C, Wennstrom JL. Locally delivered doxycy-cline improves the healing following non-surgical peri-odontal therapy in smokers. J Clin Periodontol 2004;31:589-595.
34. Hughes FJ, Syed M, Koshy B, et al. Prognostic factorsin the treatment of generalized aggressive periodonti-tis: II. Effects of smoking on initial outcome. J ClinPeriodontol 2006;33:671-676.
35. Peacock ME, Sutherland DE, Schuster GS, et al. Theeffect of nicotine on reproduction and attachment ofhuman gingival fibroblasts in vitro. J Periodontol 1993;64:658-665.
36. Tipton DA, Dabbous MK. Effects of nicotine on prolif-eration and extracellular matrix production of humangingival fibroblasts in vitro. J Periodontol 1995;66:1056-1064.
37. Hanes PJ, Schuster GS, Lubas S. Binding, uptake andrelease of nicotine by human gingival fibroblasts. J Peri-odontol 1991;62:147-152.
38. Moses O, Artzi Z, Sculean A, et al. Comparative studyof two root coverage procedures: A 24-month follow-up multicenter study. J Periodontol 2006;77:195-202.
Correspondence: Dr. Francisco Humberto Nociti Jr.,Avenida Limeira, 901, Department of Prosthodontics andPeriodontics, Division of Periodontics, School of Dentistry atPiracicaba, University of Campinas, Piracicaba, SP, Brazil.Fax: 55-19-2106-5301; e-mail [email protected].
Submitted August 22, 2007; accepted for publicationOctober 23, 2007.
J Periodontol • April 2008 Andia, Martins, Casati, Sallum, Nociti
653