root cementum may modulate gene expression during periodontal regeneration: a preliminary study in...
TRANSCRIPT
Root Cementum May Modulate GeneExpression During PeriodontalRegeneration: A Preliminary Studyin HumansPatricia F. Goncxalves,* Liana L. Lima,† Enilson A. Sallum,† Marcio Z. Casati,†
and Francisco H. Nociti Jr.†
Background: Previous data demonstrated that root cemen-tum may affect periodontal regeneration. As such, this studyaimed to explore further possible mechanisms involved inthis process by investigating in humans whether root cemen-tum modulates gene expression in the regenerating tissueformed under membrane-protected intrabony defects.
Methods: Thirty subjects with deep intrabony defects (‡5mm; 2- or 3-wall) were selected and assigned to the controlor test group. The control group received scaling and rootplaning with the removal of granulation tissue and root cemen-tum; the test group underwent removal of granulation tissueand soft microbial deposits by cleaning the root surface witha microbrush and saline solution, aiming at cementum preser-vation. Guided tissue regeneration (GTR) was applied to bothgroups. Twenty-one days later, the newly formed tissue underthe membrane was assessed for the expression of the followinggenes: alkaline phosphatase (ALP), osteopontin (OPN), oste-ocalcin (OCN), platelet-derived growth factor-alpha (PDGFA),bone sialoprotein (BSP), and basic fibroblast growth factor(bFGF).
Results: Data analysis demonstrated that mRNA levels forPDGFA, BSP, and bFGF were higher in the sites where rootcementum was kept in place compared to the sites where rootcementum was removed completely as part of the periodontaltherapy (P <0.05); in contrast, OCN levels were lower (P <0.05).No difference for ALP or OPN was observed between the con-trol and test groups (P >0.05).
Conclusion: Root cementum may modulate the expressionof growth and mineral-associated factors during periodontalregeneration. J Periodontol 2008;79:323-331.
KEY WORDS
Cementum; gene expression; periodontal regeneration.
The major challenge in periodontaltherapy is to restore the structureand function of the dental attach-
ment apparatus lost during the courseof the disease. Although there has beensome success in periodontal regenera-tion techniques, including the use ofbarrier membranes for guided tissue re-generation (GTR), growth factors, andenamel matrix proteins, these approacheshave not resulted in predictable out-comes, especially regarding new cemen-tum formation and attachment.1 Tissueengineering also has been proposed as amethod to promote regeneration.2 Al-though promising results have beenreported with the application of the tis-sue engineering principle,3,4 a greaterunderstanding of the cellular and mo-lecular mechanisms involved in peri-odontal healing and regeneration is stillrequired to achieve predictability.
During the progression of periodontaldisease, root cementum becomes ex-posed to the subgingival and/or oral en-vironment as attachment loss occursand progresses. Changes affecting theexposed root cementum5-7 have formedthe basis for the mechanical treatment ofthe root surface in sites with periodontitis;however, a gentler approach has beenproposed based on the observation thatendotoxin does not penetrate deeplyinto the root cementum.8,9 It was
* Department of Dentistry, Division of Periodontics, School of Biologic and Health Sciences,Federal University of Vales of Jequitinhonha and Mucuri, Diamantina, MG, Brazil.
† Department of Prosthodontics and Periodontics, Division of Periodontics, School ofDentistry at Piracicaba, University of Campinas, Piracicaba, SP, Brazil.
doi: 10.1902/jop.2008.070327
J Periodontol • February 2008
323

demonstrated that periodontal health can be achievedby polishing the root surface,10,11 signifying that theremoval of the root cementum for the purpose of elim-inating endotoxins may not be necessary. In fact,there is accumulating evidence that cementum maybe critical for appropriate maturation of the periodon-tium during formation and regeneration.12,13 Furtherevidence has suggested that preservation of the rootcementum may be an important factor for favoringperiodontal regeneration, providing a suitable micro-environment for new cementum formation to oc-cur.14,15 Although an in vitro study16 demonstratedthat the cementum matrix may modulate the activityof various cell types, very little is known about themechanisms that regulate the effects of preexistingcementum on the periodontal healing process follow-ing periodontal disease. Thus, to further understandthe effect of the preexisting cementum on periodontalhealing in sites previously affected by chronic peri-odontal disease, the present study aimed to assess geneexpression of growth and mineral-associated factorsin the regenerating tissue formed under membrane-protected intrabony defects in the presence or ab-sence of root cementum.
MATERIALS AND METHODS
Study PopulationThirty subjects (18 females and 12 males; aged 39 to59 years) with deep intrabony defects (‡5 mm, 2- or3-wall), located in anterior or posterior teeth with arecommendation for extraction, were included in thisstudy. Subjects were selected from the pool of patientsof the Dental School at Piracicaba, University of Cam-pinas, from January 2005 to July 2006. All subjectswere free of systemic complications, and none weresmokers. Subjects were instructed as to the characterand purpose of the study, and all signed an informedconsent. The Institutional Ethical Committee on HumanResearch approved the consent and study protocol.
The inclusion criteria for the study were: adult sub-jects with chronic periodontitis (chronic periodontitiswas defined as multiple sites [at least eight] with aprobing depth ‡5 mm associated with bleeding onprobing and bone loss evaluated by radiographs)and a tooth recommended for extraction with deep in-trabony defects (‡5 mm, 2 or 3 walls) and withoutendodontic treatment, dental mobility, caries, or res-torations close to the gingival margin.
The exclusion criteria were: pregnant or lactatingwomen; anti-inflammatory, antibiotic, or hormoneuse during the 6 months before the study; evidenceof systemic modifiers of periodontal disease, suchas osteoporosis, smoking, diabetes, or the use ofdrugs that influence periodontal tissues; and peri-odontal treatment for 6 months before the study for
the control group and any previous periodontal treat-ment for the test group.
Study Design and Surgical ProcedureFollowing supragingival instrumentation and the plaque-control phase, the defects were accessed surgically.Intrasulcular incisions were made, and buccal and lin-gualmucoperiosteal flapswere raised.Then, treatmentwas performed according to the group assignment.
In the control group (N = 15), the defects were ac-cessed, granulation tissue was removed from the defect,and the tooth surface was debrided completely byscaling and root planing, using curets and diamond-coated burs, aiming at total cementum removal. Thenthe root surface facing the defect was cleaned with amicrobrush‡ and saline solution.
In the testgroup (N = 15), the defectswereaccessed,granulation tissue was removed from the defect, dentalcalculus was detached carefully (without scaling androot planing), and the root surface facing the defectwas cleaned only with a microbrush and sterile salinesolution, aiming at maximum cementum preservation.
In both groups, the defects were treated accordingto GTR principles using a non-resorbable expandedpolytetrafluoroethylene membrane§ covering the de-fect area and 2 to 3 mm of the adjacent bone. In allsites, the flaps were positioned coronally to coverthe membrane and sutured.i Subjects were prescribedantibiotics for 7 days (amoxicillin, 500 mg, four timesa day) and analgesic medication for 2 days. Chlorhex-idine rinses (0.12%), used twice daily, were prescribedthroughout the experimental period (21 days), asso-ciated with the topical application of 1% chlorhexidinegel. The membrane was removed 21 days after thesurgery, and the regenerating tissue under the mem-brane was collected carefully, rinsed with cold ster-ile saline solution, and stored in a tube containing asolution¶ to preserve RNA integrity at -70�C for as-sessing gene expression by the quantitative polymer-ase chain reaction (PCRq) technique. Then, the teethwere extracted and fixed for standard histologic pro-cedures. Three teeth of the 15 from each group wereselected randomly for scanning electron microscopy(SEM) analysis. Patients were instructed for the stan-dard concerns in the postoperative period, such as nophysical exercise, feeding advice, and plaque-controltechniques, and sutures were removed after 7 to 10days. The surgical procedures for the control and testgroups are illustrated by Figures 1 and 2, respectively.
Histologic AnalysisTeeth were fixed in a 4% neutral buffered formalinsolution for 2 days at room temperature. Then
‡ Microbrush Regular Size, Microbrush International, Grafton, WI.§ Gore-Tex, W.L. Gore and Associates, Flagstaff, AZ.i Gore-Tex sutures, W.L. Gore and Associates.¶ RNAlater, Ambion, Austin, TX.
Root Cementum and Periodontal Regeneration Volume 79 • Number 2
324

specimens were washed and decalcified in a 10% buff-ered EDTA solution (pH = 7.2 to 7.6) at room temper-ature for 3 months. Mesio-distal serial sections (7 mmthick) were obtained and stained with hematoxylinand eosin for light microscopy observation. Sectionswere assessed histologically to confirm the absence orthe presence of root cementum for the control and testgroups, respectively.
SEM AnalysisAfter extraction, teeth werefixed in Karnovsky’s solutionfor 1 hour at room tempera-ture, rinsed in deionized wa-ter, post-fixed in osmiumtetraoxide for 1 hour atroom temperature, and rinsedagain in deionized water for 5minutes. After fixation, spec-imens were dehydrated in25%, 50%, 75%, and 90% ac-etone (20 minutes each),dried to the critical point,fixed on stubs, and coatedwith a gold layer ;100 to200 A thick. Specimens wereanalyzed with SEM# at amagnification ·270 to ·900and 5 to 20 kV to documentfurther the root surface to-pography in the control andtest groups.
Gene-Expression AnalysisRNA extraction. The regen-erating tissue under the mem-brane was harvested, rinsedwith cold sterile saline solu-tion, and stored in a tube con-taining a solution to preserveRNA integrity** at -70�C forquantitativelyassessingmRNAlevels of the following genes:alkaline phosphatase (ALP),osteopontin (OPN), osteo-calcin (OCN), platelet-derivedgrowth factor-alpha(PDGFA),bone sialoprotein (BSP), andbasic fibroblast growth factor(bFGF). Total RNA was ex-tracted†† following the man-ufacturer’s recommendation.RNA samples were resus-pended in diethylpyrocar-bonate-treated water andstored at -70�C. The RNAconcentration was deter-
mined from the optical density.‡‡
PCRq. Reverse transcription. Total RNA was trea-ted with DNase,§§ and 1 mg was used for complemen-tary DNA (cDNA) synthesis. The reaction was carried
Figure 1.Treatment procedure for the control group. A) Mucoperiosteal flaps were raised and the defect wassurgically accessed. B) Granulation tissue was curetted, and scaling and root planing was performed.C) The membrane was positioned and sutured, covering the defect. D) Flaps were positioned coronally andsutured. E) Twenty-one days later: clinical aspect of the newly formed tissue, after membrane removal.F) The newly formed tissue was harvested carefully. G) Tissue was stored in a tube containing solution topreserve RNA integrity. H) The tooth was extracted, and the flap was sutured.
# JSM5600, Jeol, Tokyo, Japan.** RNAlater, Ambion.†† TRIZOL method, Gibco BRL Life Technologies, Rockville, MD.‡‡ Biophotometer, Eppendorf, Hamburg, Germany.§§ DNA-free, Ambion.
J Periodontol • February 2008 Goncxalves, Lima, Sallum, Casati, Nociti
325
out using the transcriptor first-strand cDNA synthesiskit,ii following the manufacturer’s recommendations.
Primer design. Primers were designed using probedesign software¶¶ (Table 1). Experiments were runtwice with comparable results.
PCRq. PCRq was performed.##*** For each run,water was used as a negative control. The reaction
product was quantified witha relative quantification toolusing GAPDH as the refer-ence gene.
Statistical AnalysisThe data were averaged, andan intergroup analysis wasdone using the Student t test(a = 0.05) to test the hypoth-esis that the preexisting ce-mentum may modulate geneexpression in the regenerat-ing tissue in membrane-protected intrabony defects.
RESULTS
Clinical ObservationsDuring the healing period, nosuppuration or abscess for-mation was observed. Gingi-val recession (>1 mm), withexposure of the coronal partof the membrane, was no-ticed in two sites (one in eachgroup). These cases werecontrolled with topical appli-cation of 1% chlorhexidinegel during the experimentalperiod, and they showed nofurther complications. At theend of the experimental pe-riod, i.e., 21 days after thesurgical procedure, soft tis-sues had healed totally andexhibited no clinical signs ofinflammation.
Structural andUltrastructural FindingsLight microscopy analysisshowed that preexisting ce-mentum was present alongthe root surface of the defectin test sites and was com-pletely absent in controlsites, where dentin was ex-posed. SEM also was usedto illustrate the topographyof the root surfaces for the
control and experimental groups and confirmed thatdental cementum was present along the entire rootsurface in all of the evaluated test sites, whereas in
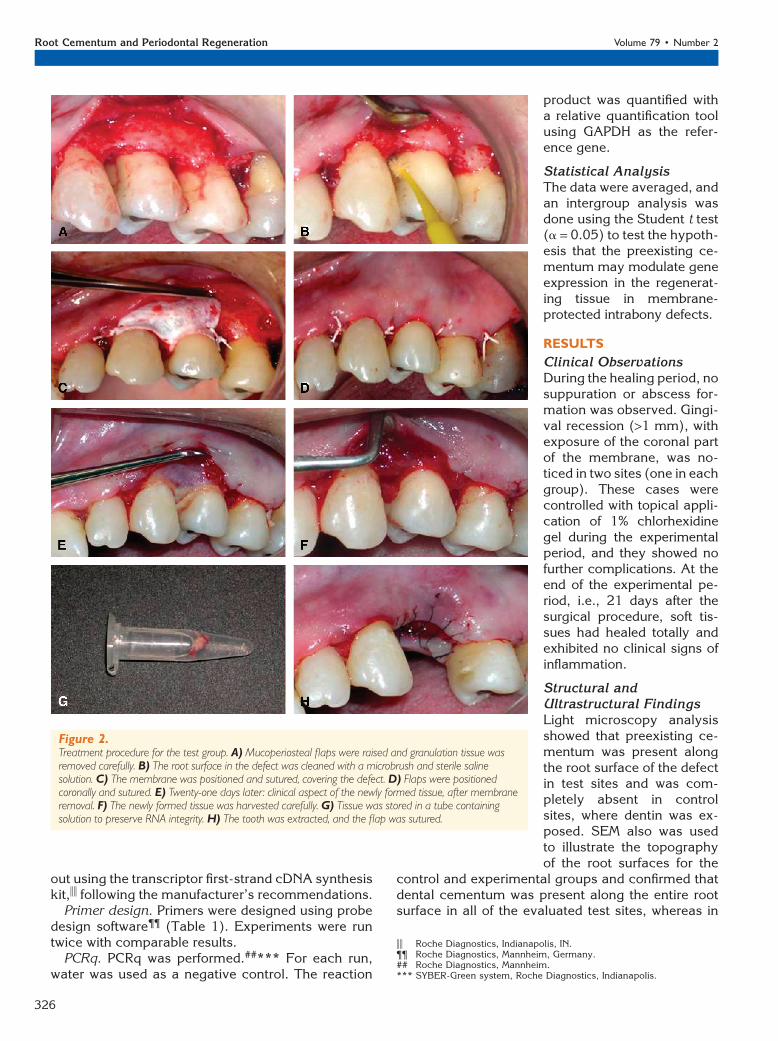
Figure 2.Treatment procedure for the test group. A) Mucoperiosteal flaps were raised and granulation tissue wasremoved carefully. B) The root surface in the defect was cleaned with a microbrush and sterile salinesolution. C) The membrane was positioned and sutured, covering the defect. D) Flaps were positionedcoronally and sutured. E) Twenty-one days later: clinical aspect of the newly formed tissue, after membraneremoval. F) The newly formed tissue was harvested carefully. G) Tissue was stored in a tube containingsolution to preserve RNA integrity. H) The tooth was extracted, and the flap was sutured.
ii Roche Diagnostics, Indianapolis, IN.¶¶ Roche Diagnostics, Mannheim, Germany.## Roche Diagnostics, Mannheim.*** SYBER-Green system, Roche Diagnostics, Indianapolis.
Root Cementum and Periodontal Regeneration Volume 79 • Number 2
326

the control sites, dentin was observed along the com-plete extension of the defect (Fig. 3). In the areaswhere cementum was maintained inplace (testgroup),domes or small circular mounds were observed on theroot surface, giving them a pebbly appearance. Noconnective tissue fibrils were observed, and the rootsurface was mostly free of calculus because all visiblecalculuswas removedduring the surgical procedure. Inthe areas where cementum was removed completely(control group), scaling and root planing resulted inthe removal of all calculus and all cementum. In addi-tion, some debris was found in these specimens, asso-ciated with the presence of distinct areas of dentinaltubules.
Gene-Expression AnalysisIn test samples, root cementum was maintained onroots that previously had been exposed to the dentalbiofilm and intentionally kept in place by a gentleapproach for root decontamination. To determinewhether the presence of root cementum would mod-ulate gene expression in vivo, the regenerating tissueformed under a membrane-protected intrabony de-fect was assessed quantitatively for the expressionof the following genes: ALP, OPN, OCN, PDGFA,BSP, and bFGF. Data analysis demonstrated that,except for ALP and OPN, mRNA levels for all of thefactors were affected significantly by the preexistingroot cementum. PDGFA, BSP, and bFGF levels werehigher in the sites where root cementum was kept inplace compared to the sites where root cementum
was removed completelyas part of the periodontaltherapy (P <0.05); in con-trast, OCN levels werelower (P <0.05). No differ-ences were observed forALP and OPN expressionsbetween the control andtest groups (P >0.05). Fig-ure 4 illustrates the gene-expression data.
DISCUSSION
Available regenerative tech-niques are unpredictableand reflect the complexityof periodontal wound heal-ing, which involves the in-teraction of four distincttissues: gingivae, periodon-tal ligament, cementum,and bone. A recent study,14
which investigated, in vivo,the effect of root cementumon periodontal regeneration
in Class III furcation defects created in dogs, demon-strated that root cementum preservation resulted in asuperior formation of new cementum and new boneand less soft tissue in the defect following the use ofGTR. In this study, ;55% and 22% of the defects inthe test (root cementum preserved) and control (rootcementum removal) groups, respectively, exhibitedcomplete filling of the furcation. Furthermore, the pro-portions of true periodontal regeneration along the rootsurface were 65.38% and 25.95% for the test and con-trol group, respectively. Thus, the present study wasdesigned to further investigate possible mechanismsinvolved in the modulation of periodontal regenerationby root cementum, assessing the expression of anumber of genes reported to play a role in periodon-tal healing, in the regenerating tissue formed undermembrane-protected intrabony defects in human. Be-cause the presence of root cementum was a critical as-pect in this study, histologic procedures also wereperformed to ensure that cementum was removedcompletely or preserved along the entire defect areafor the control and test groups, respectively. Light mi-croscopy and SEM analysesconfirmed thatpreexistingcementum was present along the root surface of thedefect in test sites, whereas it was completely absentin control sites, where dentin was exposed. In addition,although topographical observation was not the mainpurpose of the present investigation, our findings reit-erate previous reports17,18 that showed root cementumalterations, such as hypermineralization and no con-nective tissue fibers, in the areas where exposure to
Table 1.
Primer Sequences, Annealing Temperatures, and GenBankNumber for Each Gene
Gene Primer Sequence (59 / 39) Temperature (�C) GenBank Number
GAPDH GAAGGTGAAGGTCGGAGTC 53.6 NM_002046GAAGATGGTGATGGGATTTC 51.4
OCN AGCTCAATCCGGACTGT 60.4 NM_199173GGAAGAGGAAAGAAGGGTGC 60.8
ALP CGGGCACCATGAAGGAAA 60.1 NM_000478GGCCAGACCAAAGATAGAGTT 60.4
BSP GAGGGCAGAGGAAATACTCAAT 60.5 NM_004967ATTCAAAGCCAAGTTCAGAGATGTAAA 60.1
OPN AAAGCCAATGATGAGAGCAA 59.6 NM_000582ATTTCAGGTGTTTATCTTCTTCCTTAC 60.0
PDGFA GGGAAGGCCTAGGGAGT 60.6 NM_002607ACATAGTAGGTTCAGGAATGTAACAC 59.9
bFGF AACATCTCCTAACTTGTTTAAATGTCC 60.0 NM_002006ATCCGGTGCTTCCACGA 59.7
J Periodontol • February 2008 Goncxalves, Lima, Sallum, Casati, Nociti
327

contaminants occurred. Caries, root resorption, andbacterial contaminants were not found in the examinedfields.
In the present investigation, gene-expression anal-ysis demonstrated that the presence of preexisting ce-mentum along the root surface adjacent to the healingarea affected mRNA levels of molecules necessary forperiodontal regeneration in the newly formed tissueunder the membrane. Although there was no modula-tion in ALP and OPN mRNA levels, the test group ex-hibited a significant increase in the mRNA levels ofPDGFA, bFGF, and BSP and a decrease in the mRNAlevels of OCN. These findings confirm previous re-ports19,20 showing that periodontal tissues, formedin defects treated by GTR, contain molecules associ-ated with bone/cementum and growth factors.
Growth factors, such as PDGF, one of the firstgrowth factors to be described, can stimulate and en-hance periodontal wound healing and regeneration. Invitro studies demonstrated that PDGF can stimulatemitogenic activity and chemotaxis in osteoblasts,21
affect the proliferative rate, and have a potent mito-genic effect on cells from the periodontal ligament.22-24
In addition, PDGF can influence mitogenesis, the gene-expression profile, and the biomineralization potentialof cementoblastic cells.12 In vivo, PDGF was demon-
strated to promote regenera-tion of bone, cementum, andperiodontal ligament.25-28
Recent clinical trials29-31
showed that treatment withrecombinant human PDGFisoform BB stimulated a sig-nificant increase in the rateof clinical attachment levelgain and improved bone fillcompared to controls. bFGFis a member of the fibroblastgrowth factor (FGF) familyand is a potent mitogen andchemoattractant for endo-thelial cells and a variety ofmesenchymal cells, includ-ing fibroblasts and osteo-blasts. An in vitro study32
showed that periodontalligament cells have FGF re-ceptors and that bFGF stimu-lated mitogenic activity andchemotaxis in periodontalligament cells. Additionally,in vivo studies33,34 suggesteda beneficial effect of bFGF onmatrix formation during thebone-healing process.
Moreover, in the presentinvestigation, mRNA levels for mineral-associatedfactors, including ALP, BSP, OCN, and OPN, alsowere assessed by PCRq. BSP and OCN are highly spe-cific to mineralized tissues, including bone and devel-oping and mature cementum.35,36 Evidence suggeststhat BSP is a nucleator of hydroxyapatite crystal for-mation, whereas OCN seems to play a role in the earlyphases of mineralization and in the regulation of crys-tal growth.37 An in vitro study38 also demonstratedthat BSP promoted periodontal and bone cell attach-ment. Growth factors, such as PDGF, were shown toregulate BSP and OCN expression in cementoblasticand osteoblastic cells in vitro.12,39 Finally, Matsuuraet al.40 demonstrated in vivo, by immunostaining, thatBSP was restricted to the area of new cementum andnew bone formed in periodontal defects created indogs and treated by the GTR technique. ALP andOPN also were expressed in the regenerating tissueunder the membrane 21 days after the surgical proce-dures in the control and test groups, but neither of thegenes was affected by the presence of the preexistingcementum after root decontamination. ALP and OPNare differentiation markers for osteoblastic and ce-mentoblastic cell phenotypes;39,41 therefore, the ex-pression of both genes in the newly formed tissue inthe membrane-protected intrabony defects for both
Figure 3.SEM images of the root surface at the defect sites. A and B) Control group: aspect of the dentin surfaceexposed; no cementum is present. (Original magnification: A, ·270; B, ·900). C and D) Test group: aspectof the root cementum covering the entire root surface of the defect area. (Original magnification: C, ·330;D, ·900).
Root Cementum and Periodontal Regeneration Volume 79 • Number 2
328

groups strongly suggests that there is an intrinsic po-tential for hard tissue regeneration in such an area.
The results of the present study should not be in-terpreted to indicate that root planing should not beperformed before GTR therapy. Removal of hard de-posits, such as calculus and mineralized surface coat-ings, must, for practical reasons, involve removal ofthe cementum. However, the results presented hereclearly demonstrate that root cementum may ac-tively take part in periodontal regeneration throughits effect on the expression of factors involved inthe development and regeneration of mineralizedand soft tissues, as observed by histometric analysisin previous studies.14,15 Nevertheless, an importantlimitation of the present study is the fact that datapresented here represented one time point (21 days).Therefore, caution should be used to interpret thesefindings, and future studies should be considered toinvestigate further the role of root cementum in peri-odontal regeneration, regarding the mechanisms in-volved, in a time-sequence manner, and to elucidatethe clinical predictability of this gentler approach ona long-term basis.
ACKNOWLEDGMENTS
This study was supported by Sao Paulo State Re-search Foundation (FAPESP #05/51215-0). This ar-ticle is based on Liana L. Lima’s thesis researchconducted at the School of Dentistry at Piracicaba,Campinas State University, in partial fulfillment ofthe requirements for a Master’s degree. The authorsreport no conflicts of interest related to this study.
REFERENCES1. Wang HL, Cooke J. Periodontal regeneration tech-
niques for treatment of periodontal diseases. Dent ClinNorth Am 2005;49:637-659.
2. Bartold PM, McCulloch CA, Narayanan AS, Pitaru S.Tissue engineering: A new paradigm for periodontalregeneration based on molecular and cell biology.Periodontol 2000 2000;24:253-269.
3. Yamada Y, Ueda M, Hibi H, Baba S. A novel approachto periodontal tissue regeneration with mesenchymalstem cells and platelet-rich plasma using tissue engi-neering technology: A clinical case report. Int J Peri-odontics Restorative Dent 2006;26:363-369.
4. Bartold PM, Xiao Y, Lyngstaadas SP, Paine ML, SneadML. Principles and applications of cell delivery
Figure 4.Graphic representation of the mean values and standard deviation for the mRNA levels of ALP, OPN, BSP, OCN, PDGFA, and bFGF for the control (N =15) and test (N = 15) groups, relative to the levels of GAPDH. No more than one sample was obtained per subject and used for gene-expressionanalysis. *Statistically different by the Student t test (P <0.05).
J Periodontol • February 2008 Goncxalves, Lima, Sallum, Casati, Nociti
329

systems for periodontal regeneration. Periodontol 20002006;41:123-135.
5. Selvig KA. Ultrastructural changes in cementum andadjacent connective tissue in periodontal disease.Acta Odontol Scand 1966;24:459-600.
6. Aleo JJ, De Renzis FA, Farber PA, Varboncoeur AP.The presence and biologic activity of cementum-bound endotoxin. J Periodontol 1974;45:672-675.
7. Adriaens PA, Edwards CA, De Boever JA, Loesche WJ.Ultrastructural observations on bacterial invasion incementumandradiculardentinofperiodontallydiseasedhuman teeth. J Periodontol 1988;59:493-503.
8. Cheetham WA, Wilson M, Kieser JB. Root surfacedebridement. An in vitro assessment. J Clin Periodon-tol 1988;15:288-292.
9. Smart GJ, Wilson M, Davies EH, Kieser JB. Theassessment of ultrasonic root surface debridement bydetermination of residual endotoxin levels. J ClinPeriodontol 1990;17:174-178.
10. Nyman S, Sarhed G, Ericsson I, Gottlow J, Karring T.Role of diseased root cementum in healing followingtreatment of periodontal disease. An experimentalstudy in the dog. J Periodontal Res 1986;21:496-503.
11. Nyman S, Westfelt E, Sarhed G, Karring T. Role ofdiseased root cementum in healing following treat-ment of periodontal disease. A clinical study. J ClinPeriodontol 1988;15:464-468.
12. Saygin NE, Giannobile WV, Somerman MJ. Molecularand cell biology of cementum. Periodontol 2000 2000;24:73-98.
13. Schupbach P, Gaberthuel T, Lutz F, Guggenhein B.Periodontal repair or regeneration: Structures of dif-ferent types of new attachment. J Periodontal Res 1993;28:281-293.
14. Goncxalves PF, Gurgel BC, Pimentel SP, et al. Rootcementum modulates periodontal regeneration inClass III furcation defects treated by the guided tissueregeneration technique: A histometric study in dogs.J Periodontol 2006;77:976-982.
15. Goncxalves PF, Gurgel BC, Pimentel SP, et al. Effect oftwo different approaches for root decontaminationon new cementum formation following guided tissueregeneration: A histomorphometric study in dogs.J Periodontal Res 2006;41:535-540.
16. Grzesik WJ, Narayanan AS. Cementum and periodon-tal wound healing and regeneration. Crit Rev Oral BiolMed 2002;13:474-484.
17. Carrassi A, Abati S, Santarelli G. The role of scanningelectron microscopy in periodontal research. Scan-ning Microsc 1988;2:1123-1138.
18. Barton NS, Van Swol RL. Periodontally diseased vs.normal roots as evaluated by scanning electron mi-croscopy and electron probe analysis. J Periodontol1987;58:634-638.
19. Amar S, Petrungaro P, Amar A, Van Dyke TE. Immu-nolocalization of bone matrix macromolecules in hu-man tissues regenerated from periodontal defectstreated with expanded polytetrafluoroethylene mem-branes. Arch Oral Biol 1995;40:653-661.
20. Amar S, Chung KM, Nam SH, Karatzas S, Myokai F, VanDyke TE. Markers of bone and cementum formationaccumulate in tissues regenerated in periodontal de-fects treated with expanded polytetrafluoroethylenemembranes. J Periodontal Res 1997;32:148-158.
21. Heldin CH, Ostman A, Ronnstrand L. Signal transduc-tion via platelet-derived growth factor receptors. Bio-chim Biophys Acta 1998;1378:F79-F113.
22. Piche JE, Carnes DL Jr., Graves DT. Initial character-ization of cells derived from human periodontitis.J Dent Res 1989;68:761-767.
23. Matsuda N, Lin WL, Kumar NM, Cho MI, Genco RJ.Mitogenic, chemotactic, and synthetic responses ofrat periodontal ligament fibroblastic cells to polypep-tide growth factors in vitro. J Periodontol 1992;63:515-525.
24. Oates TW, Rouse CA, Cochran DL. Mitogenic effectsof growth factors on human periodontal ligament cellsin vitro. J Periodontol 1993;64:142-148.
25. Lynch SE, Williams RC, Polson AM, et al. A combina-tion of platelet-derived and insulin-like growth factorsenhances periodontal regeneration. J Clin Periodontol1989;16:545-548.
26. Giannobile WV, Finkelman RD, Lynch SE. Compari-son of canine and non-human primate animal modelsfor periodontal regenerative therapy: Results followinga single administration of PDGF/IGF-I. J Periodontol1994;65:1158-1168.
27. Giannobile WV, Hernandez RA, Finkelman RD, et al.Comparative effects of platelet-derived growth factor-BB and insulin-like growth factor-I, individually and incombination, on periodontal regeneration in Macacafascicularis. J Periodontal Res 1996;31:301-312.
28. Nevins M, Camelo M, Nevins ML, Schenk RK, LynchSE. Periodontal regeneration in humans using re-combinant human platelet-derived growth factor-BB(rhPDGF-BB) and allogenic bone. J Periodontol 2003;74:1282-1292.
29. Howell TH, Fiorellini JP, Paquette DW, OffenbacherS, Giannobile WV, Lynch SE. A phase I/II clinical trialto evaluate a combination of recombinant humanplatelet-derived growth factor-BB and recombinanthuman insulin-like growth factor-I in patients withperiodontal disease. J Periodontol 1997;68:1186-1193.
30. Nevins M, Giannobile WV, McGuire MK, et al. Platelet-derived growth factor stimulates bone fill and rate ofattachment level gain: Results of a large multicenterrandomized controlled trial. J Periodontol 2005;76:2205-2215.
31. Sarment DP, Cooke JW, Miller SE, et al. Effect ofrhPDGF-BB on bone turnover during periodontal re-pair. J Clin Periodontol 2006;33:135-140.
32. Terranova VP, Odziemiec C, Tweden KS, SpadoneDP. Repopulation of dentin surfaces by periodontalligament cells and endothelial cells. Effect of basicfibroblast growth factor. J Periodontol 1989;60:293-301.
33. Eppley BL, Connolly DT, Winkelmann T, Sadove AM,Heuvelman D, Feder J. Free bone graft reconstructionof irradiated facial tissue: Experimental effects of basicfibroblast growth factor stimulation. Plast ReconstrSurg 1991;88:1-11.
34. Frenkel SR, Herskovits MS, Singh IJ. Fibroblast growthfactor: Effects on osteogenesis and chondrogenesisin the chick embryo. Acta Anat (Basel) 1992;145:265-268.
35. Ganss B, Kim RH, Sodek J. Bone sialoprotein. Crit RevOral Biol Med 1999;10:79-98.
36. Somerman MJ, Sauk JJ, Foster RA, Norris K,Dickerson K, Argraves WS. Cell attachment activityof cementum: Bone sialoprotein II identified in cemen-tum. J Periodontal Res 1991;26:10-16.
37. Hunter GK, Hauschka PV, Poole AR, Rosenberg LC,Goldberg HA. Nucleation and inhibition of hydroxyapatite
Root Cementum and Periodontal Regeneration Volume 79 • Number 2
330

formation by mineralized tissue proteins. Biochem J1996;317:59-64.
38. Somerman MJ, Fisher LW, Foster RA, Sauk JJ.Human bone sialoprotein I and II enhance fibroblastattachment in vitro. Calcif Tissue Int 1988;43:50-53.
39. Strayhorn CL, Garrett JS, Dunn RL, Benedict JJ,Somerman MJ. Growth factors regulate expression ofosteoblast-associated genes. J Periodontol 1999;70:1345-1354.
40. Matsuura M, Herr Y, Han KY, Lin WL, Genco RJ, Cho MI.Immunohistochemical expression of extracellular matrixcomponents of normal and healing periodontal tissuesin the beagle dog. J Periodontol 1995;66:579-593.
41. Kitagawa M, Tahara H, Kitagawa S, et al. Character-ization of established cementoblast-like cell lines fromhuman cementum-lining cells in vitro and in vivo.Bone 2006;39:1035-1042.
Correspondence: Dr. Francisco Humberto Nociti Jr., Divi-sion of Periodontics, School of Dentistry at Piracicaba,University of Campinas, Av. Limeira, 901, Areiao, Piraci-caba, SP, Brazil, CEP: 13414-903. Fax: 55-19-21065301;e-mail: [email protected].
Submitted June 6, 2007; accepted for publication August1, 2007.
J Periodontol • February 2008 Goncxalves, Lima, Sallum, Casati, Nociti
331