rom j morphol embryol 2014, 55(2 suppl):597–602 r j m e ... · pdf filerom j morphol...
TRANSCRIPT
Rom J Morphol Embryol 2014, 55(2 Suppl):597–602
ISSN (print) 1220–0522 ISSN (on-line) 2066–8279
OORRIIGGIINNAALL PPAAPPEERR
Technological update of the video-endoscopic approach of the diagnosis and staging of tumors in children
ISABELA-MAGDALENA DRĂGHICI1,2), DRAGOŞ-CONSTANTIN LUCA3,4), MARIA-DELIA POPESCU1,2), LIVIU DRĂGHICI1,5)
1)Department of Surgery, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 2)Department of Pediatric Surgery, “Maria Skłodowska Curie” Emergency Clinical Hospital for Children, Bucharest, Romania 3)Department of Pediatric Pathology, The George Washington University, Washington, D.C., USA 4)Department of Hematopathology & Flow Cytometry, Children’s National Medical Center, Washington, D.C., USA 5)Department of General Surgery, “Sf. Ioan” Emergency Clinical Hospital, Bucharest, Romania
Abstract The pediatric patient is often difficult to diagnose, especially since the surgical pathology is tumoral. Establishing the histopathological diagnosis of a tumor, staging of a disease and certifying the existence of rare pediatric affections are three of the motives for which the specialists frequently appeal to an exploratory laparoscopy, accompanied by biopsy procedures. The paper presents the laparoscopic biopsy experience of the team from the Department of Pediatric Surgery, “Maria Skłodowska Curie” Emergency Clinical Hospital for Children, Bucharest, Romania. From 2000 to 2013, 95 such procedures were performed (7.76% of a total of 1224 laparoscopic interventions). In many cases, the laparoscopy had an exclusive diagnostic purpose, of whose success has been primarily responsible the targeted biopsy. Current issues are discussed, centered on the most advanced technologies used in minimally invasive approach of pediatric malignancies, referring to the effect of minimizing the possible complications that can arise from this type of intervention. The authors concluded that laparoscopic technique is the method of choice in comparison to other ways of biopsy (classical surgery, ultrasound guidance, tomography, etc.), and it is characterized by a high diagnostic value.
Keywords: laparoscopy, exploratory, biopsy, pediatric pathology.
Introduction
In adult surgery, the first biopsies performed using laparoscopic technique were reported by Conn and Bagley et al. in 1972, while Cognat et al. (1974) published a study including 60 pediatric cases subjected to pelvic exploratory celioscopy, the smallest patient being 6-month-old [1–3].
Minimally invasive technique for the diagnosis and staging is widely used today to assess pediatric patients with gastrointestinal, hepatic or genital malignancies. The association of intraoperative ultrasonography during a laparoscopic inspection net improves diagnostic accuracy compared with conventional imaging techniques and as such must be considered an integral part of staging purpose laparoscopic procedure [4–8]. In addition, laparoscopic examination provides the only way to detect small peritoneal dissemination (1–5 mm) and avoid unnecessary laparotomies in at least 20% of patients [4, 5].
Laparoscopy and laparoscopic ultrasonography are minimally invasive procedures that have recently become important components in the staging algorithm for tumors. Other methods for staging disease include magnetic resonance imaging (MRI) and positron emission tomo-graphy (PET). Investigational modalities include peritoneal-fluid cytology and molecular staging techniques [9].
Materials and Methods
In the reviewed 2000–2013 period, the Department of Pediatric Surgery, “Maria Skłodowska Curie” Emergency
Clinical Hospital for Children, Bucharest, Romania, 95 laparoscopic biopsies were performed for diverse conditions, representing 7.76% of the total of 1224 laparoscopic interventions performed in children. In most of these cases, laparoscopy had only a diagnostic purposes, for whose success has been primarily responsible the targeted biopsy, performed with mono or bipolar electrocoagulation forceps and later using the LigaSure. For some of these patients, subsequent open curative procedures have been proposed.
Preoperative, in our Department, the majority of tumors currently are diagnosed by ultrasonography (US), computer tomography (CT) and magnetic resonance imaging (MRI). Although we used it less, the peritoneal lavage plays an important role in the detection of intra-abdominal malignancies and remains a sensitive modality. At our institution, laparoscopic-guided liver biopsy and the laparoscopic excision are the preferred techniques for this pediatric population. In each case, the entire peritoneal surface, including the liver and spleen was inspected allowing for the assessment of both diffuse and localized pathology.
A number of other non-surgical diseases, whose treatments require histopathological confirmation, were diagnosed performing laparoscopic biopsy (glomeruli-nephritis, lupus nephropathy, diffuse hemangiomatosis, miliary tuberculosis, etc.). We used both regular and the small laparoscopic instrumentation kit comprising 2 mm and 3 mm trocars, 5 mm telescope (300), electrosurgical devices mono/bipolar and LigaSure forceps. Electro-
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

Isabela-Magdalena Drăghici et al.
598
coagulation technique using radiofrequency (Habib laparo-scopic forceps) is undoubtedly the newest and most efficient method of hemostasis for parenchymal organs surgery, but it is still little used in practiced in our country because of the acquisition costs.
Results
The majority of patients show no significant findings on examination and the development of specific physical signs usually indicates metastatic disease. The presence of an intra-abdominal mass, hepatomegaly, or ascites is usually due to extensive and incurable disease. The asymptomatic patients diagnosed with M1 disease at laparoscopy avoided a laparotomy and were discharged, usually the day after surgery. In contrast, patients who had M1 disease noted at open laparotomy were hospitalized for an average of seven days. Interestingly, patients diagnosed with M1 disease by laparoscopy did not require a subsequent open procedure for bleeding, perforation, or obstruction. Further, these patients had similar survivals to those of historical controls with M1 disease.
Some of the cases with uncertain preoperative diagnosis, non-surgical, but with a significant gravity and whose histological confirmation was imperative to the therapeutic conduct, benefited of the advantage of video-endoscopic biopsy techniques. Another group of patients included cases that had a bad prognosis of various stages of neoplastic tumors, some complicated, in which histological confirmation was also necessary for establishing the neo-adjuvant cancer treatment, palliative measures. For the latter, curative surgery was virtually excluded from the outset. Most laparoscopic biopsies we recorded for liver tumors (15 cases) and malignant lymphoma (14 cases) (Table 1).
Table 1 – Laparoscopic biopsy: target organs and histopathological diagnosis
Target organ
Histopatological diagnosis
No. of cases
Total (% of 1224
laparoscopies)Right hepatic lobe
tumor 15
Chronic liver disease 7 Diffuse
hemangiomatosis 1
Liver
Biliary cirrhosis 3
26 (2.12%)
Glomerulonephritis 10
Chronic renal failure 4
Lupus nephropathy 4 Kidney
Nephrotic syndrome 7
25 (2.04%)
Retro-peritoneum
Retroperitoneum tumor
6 6 (0.49%)
Malignant lymphoma 14 Lymph nodes Inflammatory lymph
nodes 8
22 (1.79%)
Carcinomatosis 8 Peritoneum
Miliary tuberculosis 8 16 (1.30%)
Total 95 (7.76%)
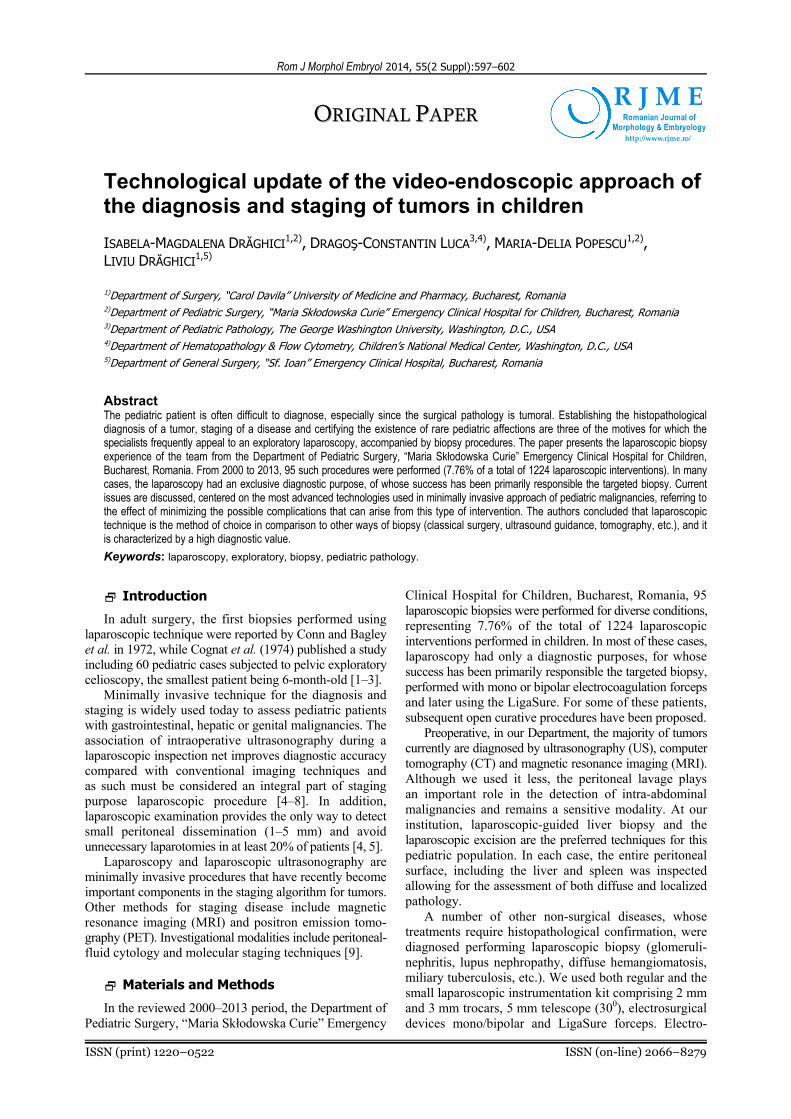
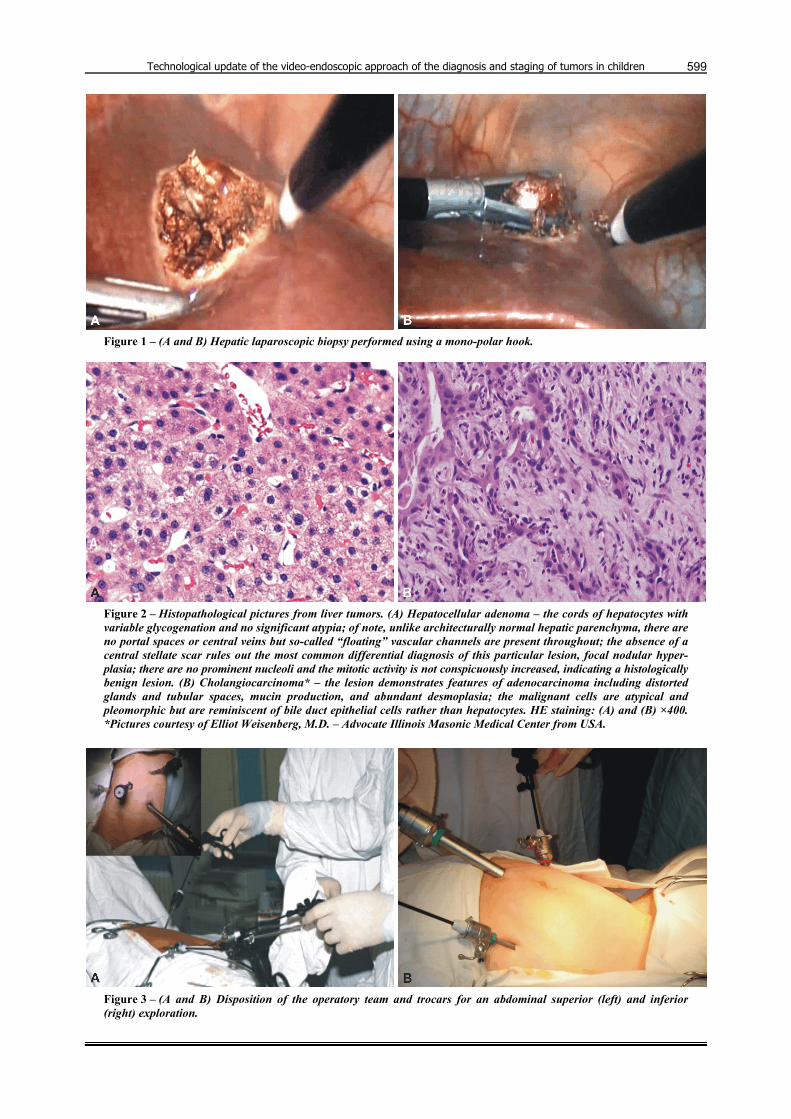
The value of laparoscopy resides not only in direct visualization of the lesions, but also that permits the practice of targeted biopsy, which allowed microscopic examination of the bioptic fragments (Figures 1 and 2).
Trocars disposition for a laparoscopic liver biopsy will respect the principle of triangulation of specific tools as
so: 10 mm telescope through the umbilical trocar, a 5 mm trocar placed in the epigastrium and a second working trocar placed in the right upper quadrant, below the costal margin (Figure 3). Optical trocar insertion should be achieved using the open method and the optical telescope adequate for easy viewing of inaccessible areas (under the diaphragm, splenic box) is that of 300. This display-cement avoids placing additional trocars. The 5 mm telescope is preferred since it is possible to change its position on another trocar during intervention to increase visibility.
The biopsy is usually performed simply, with the help of scissors with which a piece of tumor tissue excised. Specially designed for this purpose, laparoscopic kits include a biopsy forceps, whose jaws are hollow and sharp, so cutting and sampling is performed on the biopsy material. In case of bleeding incidence at the excision placement, hemostasis mst be rigorously performed using electrocoagulation or by application of hemostatic films. In lymph node biopsies (Figure 4), we proceed to node dissection, maneuver that involves placing two additional trocars for specific working instruments.
We recommend using as a principle the collecting bags, endo-bag type, for minimized handling of tumor fragments into the peritoneal cavity and to avoid contamination of the trocar wall gates, thereby reducing the risk of neoplastic dissemination. In this attempt, the increasing of the parietal gap is mandatory (Figure 5).
Modern instrumentation (LigaSure, Harmonic and Habib) allows biopsies under rigorous hemostasis, minimizing the risk of bleeding. Special attention will be given to new technologies that revolutionize the hemostasis principles and techniques. A modern machine, very useful and efficient for excision and resection biopsy of paren-chymal tissue, is the radiofrequency generator, which uses high waves – RITA (Radiofrequency Interstitial Tissue Ablation). This technology is also based on the principle of a minimally invasive procedure in which an electrode, thin as a needle, is inserted in a liver or spleen lesion, injury that otherwise would be inoperable by using ultrasound guided or CT techniques. Electricity is passed through the electrode to produce heat energy in the cells around it, making a perfect hemostasis. When all cells in the lesion, as well as a sufficient margin cells around them, were heated above the lethal threshold (530C), the procedure is deemed complete (approximately 11 minutes for a ablation zone, 4 cm length). The active piece of the RITA generator is the laparoscopic Habib clamp, which is equipped with four RF electrodes, that confer safely and rapidity to ablative techniques (Figure 6).
Discussion
In the face of a disease whose gravity is suspected by using of the imaging examinations, tactics should focus on gathering reliable information based on histo-pathological evidence that can be obtained by minimally invasive celioscopic approach. In other words, we aimed to obtain a maximum diagnostic benefit with a minimal surgical trauma, relieving patient suffering by not using laparotomy. New devices and technologies provide an extra comfort for the laparoscopic approach in organ biopsy, reducing the risk of bleeding incidents.
Technological update of the video-endoscopic approach of the diagnosis and staging of tumors in children
599
Figure 1 – (A and B) Hepatic laparoscopic biopsy performed using a mono-polar hook.
Figure 2 – Histopathological pictures from liver tumors. (A) Hepatocellular adenoma – the cords of hepatocytes with variable glycogenation and no significant atypia; of note, unlike architecturally normal hepatic parenchyma, there are no portal spaces or central veins but so-called “floating” vascular channels are present throughout; the absence of a central stellate scar rules out the most common differential diagnosis of this particular lesion, focal nodular hyper-plasia; there are no prominent nucleoli and the mitotic activity is not conspicuously increased, indicating a histologically benign lesion. (B) Cholangiocarcinoma* – the lesion demonstrates features of adenocarcinoma including distorted glands and tubular spaces, mucin production, and abundant desmoplasia; the malignant cells are atypical and pleomorphic but are reminiscent of bile duct epithelial cells rather than hepatocytes. HE staining: (A) and (B) ×400. *Pictures courtesy of Elliot Weisenberg, M.D. – Advocate Illinois Masonic Medical Center from USA.
Figure 3 – (A and B) Disposition of the operatory team and trocars for an abdominal superior (left) and inferior (right) exploration.

Isabela-Magdalena Drăghici et al.
600
Figure 4 – (A and B) Iliac vessels and biopsy of external iliac lymph nodes.
Figure 5 – (A and B) Extraction of the biopsy material using an improvised plastic bag (“surgical glove finger ligated”).
Figure 6 – (A and B) Laparoscopic Habib forceps: dissection using RF waves.
Regarding liver tumors, the laparoscopic exploration utility, in combination with intraoperative ultrasonography was reported long ago. Laparoscopic-ultrasound is effective and sensitive for the detection of liver metastases and may lead to changes of therapeutic decisions made based on inadequate preoperative conventional imaging: trans-parietal ultrasound, CT, MRI and cholangio-MRI [10]. Percutaneous video guided needle biopsy is practiced using special devices, and their intraperitoneal locations
and tracks are carefully supervised and monitored [11]. Biopsies range is vast, from peritoneal lesions, lymph-
adenopathy and tumors, and ending with abdominal viscera [12]. Classical Hodgkin’s disease staging performing laparotomy can also be replaced by laparoscopy, thus avoiding lung or peritoneal complications [11, 13].
Lobe and Schropp, performed routinely exploratory celioscopies in children with liver tumors, neuroblastomas and other malignancies, highlighting the possibility of

Technological update of the video-endoscopic approach of the diagnosis and staging of tumors in children
601
changing the therapeutic protocol based on intraoperative observations. They reported the case of a teenager in whom after the imaging investigations, the diagnosis had been unresectable liver tumor, that included the entire liver, but in whom the laparoscopic exploration revealed a left lateral free segment, allowing successful curative hepatectomy [11].
The introduction of laparoscopy to the diagnostic armamentarium has had a dramatic effect on the staging of gastric tumors. Laparoscopy allows direct visualization of the primary tumor as well as assessment of the liver and peritoneal cavity. Sub-radiological metastatic disease can be identified. Proponents of laparoscopy note that 20% to 40% of patients with clinically localized M0 disease will be up-staged by laparoscopy and have their management changed [14–20]. In this kind of pathology, the laparoscopy is especially sensitive for detecting small peritoneal and hepatic implants that are not detected by CT [14, 15, 18, 21]. The addition of ultrasonography to laparoscopy (laparoscopic ultrasonography – LUS) partially compensates for the lack of tactile sensation and may improve the surgeon’s ability to determine tumor depth and to detect lymph node metastases [22–24].
Particular attention should be paid to the presence of metastatic tumors. The presence of liver metastases and/or peritoneal, signifies often patients inoperability and obliges to palliative interventions. The protocol for the diagnosis of metastases, along with ultrasound, computed tomography, magnetic resonance and various explorations using radioisotopes have to include the laparoscopic biopsy. The collection of biopsy materials for any tumor suspected of being metastatic (tumor diameter 1–2 mm to 1.5–2 cm escape often other imaging tests ) or cytological examination carried out in ascites fluid (possibly by peritoneal lavage cytology) are two of the objectives exploratory celioscopy performed for the assessment inoperability and detection of metastases [25].
If the biopsied fragments have a larger size, it is recommended to use the L.A.S.E.R. techniques, electro-coagulation or forceps-type clamps which prevents electrical aggression to the tissue [10]. If the biopsy requires a liver resection then we face the need for a laparoscopic suture similar to that performed in open surgery. Applying L.A.S.E.R. techniques allow these resections without suture [25].
Lobe and Schropp use KTP/532 Laserscope at about 12 to 15 W, or Nd:YAG to approximately 40–60 W to obtain a hemostatic excision of a liver segment. In this way, the tissue is not altered by heat and can be easily interpreted by the pathologist. By comparison, electro-coagulation techniques offer the same hemostasis quality but are encumbered by important tissue destructions that make an adequate histopathological examination difficult [11].
Laparoscopic ovarian biopsy is indicated mainly in tumor diagnosis and also in secondary amenorrhea result of Turner’s syndrome. In this respect, the role of bilateral celioscopic gonads inspection maneuver consists in measurement and sampling of tissue for histopatho-logical examination. These targeted biopsies do not trigger significant bleeding. If the maneuver is accompanied by bleeding, this may be controlled by electrocoagulation
or laser techniques, without causing injury to the residual ovarian tissue or adjacent structures [26]. Staging ovarian tumors can be performed laparoscopically including peritoneal fluid aspiration, assessment of the intra-peritoneal disseminations, association of omentectomies and liver biopsy. In case of detection of a malignancy, histology of the lesion may warrant additional procedures [27].
Conclusions
Assimilation need of new technologies in laparoscopic practice arose with the rise of the standard diagnostic and therapeutic measures aimed at eliminating unnecessary surgery, sometimes dangerous for pediatric patients. When after ultrasound and computed tomography the diagnosis remains uncertain or when it is necessary to harvest tissue for histopathological examination, laparoscopy remains the only effective method of approach.
References [1] Conn HO, Percutaneous versus peritoneoscopic liver biopsy,
Gastroenterology, 1972, 63(6):1074–1075. [2] Bagley CM Jr, Roth JA, Thomas LB, Devita VT Jr, Liver
biopsy in Hodgkin’s disease. Clinicopathologic correlations in 127 patients, Ann Intern Med, 1972, 76(2):219–225.
[3] Cognat M, Papathanassiou Z, Gomel V, Laparoscopy in infants and adolescents, J Reprod Med, 1974, 13(1):11–12.
[4] Philippe P, Becmeur F, Bax NM, Endoscopic surgery of diaphragmatic anomalies: a multicentric study of the GECI: posterolateral hernias and eventrations, XIth Annual Congress for Endosurgery in Children, May 2–4, 2002, Genoa, Italy.
[5] Shah S, Matthews BD, Sing RF, Heniford BT, Laparoscopic repair of a chronic diaphragmatic hernia, Surg Laparosc Endosc Percutan Tech, 2000, 10(3):182–186.
[6] van der Zee DC, Bax NM, Laparoscopic repair of congenital diaphragmatic hernia in a 6-month-old child, Surg Endosc, 1995, 9(9):1001–1003.
[7] Merritt DF, Torsion of the uterine adnexa: a review, J Pediatr Adolesc Gynecol, 1991, 4(1):3–13.
[8] Quillin SP, Siegel MJ, Transabdominal color Doppler ultra-sonography of the painful adolescent ovary, J Ultrasound Med, 1994, 13(7):549–555.
[9] Weiser MR, Conlon KC, Chapter 12: Diagnosis and staging of gastric cancer. In: Posner MC, Vokes EE, Weichselbaum RR (eds), Cancer of the upper gastrointestinal tract, BC Dekker Inc., Hamilton, 2002, 237–251, http://web.squ.edu.om/med Lib/MED_CD/E_CDs/Cancer%20of%20the%20Upper%20Gastrointinal%20Tract/docs/ch12.pdf.
[10] Catheline JM, Abdel Waab W, Efficacité de l’écho-laparoscopie pour la detection des metastases hepatiques des cancers colorectaux, Chirurgie Endoscopique, 2000, 9(1):27–28.
[11] Lobe TE, Schropp KP, Pediatric laparoscopy and thoraco-scopy, W.B. Saunders Company, Philadelphia, 1994, 1–177.
[12] Duca S, Chirurgia laparoscopică, ediţia a II-a, Ed. Paralela 45, Piteşti, 2001, 103–119.
[13] Callery M.P, Swanson RS, Laparoscopic staging of intra abdominal malignancy. In: Eubanks WS, Swanstrom LL, Soper NJ, Leonard M, Mastery of laparoscopic surgery, Lippincott Williams & Wilkins, Philadelphia, 1999, 73–83.
[14] Feussner H, Omote K, Fink U, Walker SJ, Siewert JR, Pretherapeutic laparoscopic staging in advanced gastric carcinoma, Endoscopy, 1999, 31(5):342–347.
[15] Arnold JC, Neubauer HJ, Zöpf T, Schneider A, Benz C, Adamek HE, Riemann JF, Improved tumor staging by diagnostic laparoscopy, Z Gastroenterol, 1999, 37(6):483–488.
[16] Hünerbein M, Rau B, Hohenberger P, Schlag PM, The role of staging laparoscopy for multimodal therapy of gastro-intestinal cancer, Surg Endosc, 1998, 12(7):921–925.
[17] Asencio F, Aguiló J, Salvador JL, Villar A, De la Morena E, Ahamad M, Escrig J, Puche J, Viciano V, Sanmiguel G,

Isabela-Magdalena Drăghici et al.
602
Ruiz J, Video-laparoscopic staging of gastric cancer. A pros-pective multicenter comparison with noninvasive techniques, Surg Endosc 1997, 11(12):1153–1158.
[18] Burke EC, Karpeh MS, Conlon KC, Brennan MF, Laparoscopy in the management of gastric adenocarcinoma, Ann Surg, 1997, 225(3):262–267.
[19] Possik RA, Franco EL, Pires DR, Wohnrath DR, Ferreira EB, Sensitivity, specificity, and predictive value of laparoscopy for the staging of gastric cancer and for the detection of liver metastases, Cancer, 1986, 58(1):1–6.
[20] Jimenez RE, Warshaw AL, Rattner DW, Willett CG, McGrath D, Fernandez-del Castillo C, Impact of laparoscopic staging in the treatment of pancreatic cancer, Arch Surg, 2000, 135(4):409–414; discussion 414–415.
[21] D’Ugo DM, Coppola R, Persiani R, Ronconi P, Caracciolo F, Picciocchi A, Immediately preoperative laparoscopic staging for gastric cancer, Surg Endosc, 1996, 10(10):996–999.
[22] Conlon KC, Karpeh MS Jr, Laparoscopy and laparoscopic ultrasound in the staging of gastric cancer, Semin Oncol, 1996, 23(3):347–351.
[23] Romijn MG, van Overhagen H, Spillenaar Bilgen EJ, Ijzermans JN, Tilanus HW, Laméris JS, Laparoscopy and laparoscopic ultrasonography in staging of oesophageal and cardial carcinoma, Br J Surg, 1998, 85(7):1010–1012.
[24] Goletti O, Buccianti P, Chiarugi M, Pieri L, Sbragia P, Cavina E, Laparoscopic sonography in screening metastases from gastrointestinal cancer: comparative accuracy with traditional procedures, Surg Laparosc Endosc, 1995, 5(3):176–182.
[25] Orlando R, Lirussi F, Okolicsanyi L, Laparoscopy and liver biopsy: further evidence that the two procedures improve the diagnosis of liver cirrhosis. A retrospective study of 1,003 consecutive examinations, J Clin Gastroenterol, 1990, 12(1): 47–52.
[26] Nezhat F, Nezhat C, Silfen SL, Videolaseroscopy for oophor-ectomy, Am J Obstet Gynecol, 1991, 165(5 Pt 1):1323–1330.
[27] Johns A, Laparoscopic oophorectomy/oophorocystectomy, Clin Obstet Gynecol, 1991, 34(2):460–466.
Corresponding author Isabela-Magdalena Drăghici, Lecturer, MD, PhD, Department of Pediatric Surgery, “Maria Skłodowska Curie” Emergency Hospital for Children, “Carol Davila” University of Medicine and Pharmacy, 20 Constantin Brâncoveanu Avenue, Sector 4, 041451 Bucharest, Romania; Phone +40744–364 856, e-mail: [email protected] Received: January 19, 2014
Accepted: August 4, 2014