robert arthur kyle, md: a conversation with the … proceedings/2010 vol 23/no. 4...laboratory...
TRANSCRIPT
400
r. Robert A. Kyle, Professor of Medicine and Laboratory Medicine and Pathology at Mayo Clinic College of Medicine, Rochester, Minnesota, presented the Marvin J. Stone Lectureship, an annual lectureship at Baylor
University Medical Center at Dallas, on March 23, 2010. After that well-received lecture entitled “Utilization of Risk Manage-ment of Multiple Myeloma with Novel Agents,” Dr. Kyle pro-vided the present interview. He was born on March 17, 1928, in Bottineau, North Dakota, and he grew up on a farm 6 miles from that city. Although neither parent fi nished high school, all fi ve boys graduated from college and several also had additional postgraduate degrees. After high school, Robert Kyle enrolled in the North Dakota School of Forestry in Bottineau, where he remained for 2 years, and then he transferred to the University of North Dakota in Grand Forks, where he received a bachelor’s degree in June 1948, graduating Phi Beta Kappa. From there he went to Northwestern University Medical School in Chicago, graduating with distinction in June 1952. He had a rotating internship at Evanston Hospital, a major teaching hospital of Northwestern Medical School at the time. After serving 2 years in the Air Force in Alaska, he completed his medical residency at Mayo Clinic in December 1959 and a hematology fellow-ship at Tufts University in Boston in August 1961, including a 1-year postdoctoral research fellowship from the National Cancer Institute. He then returned to Mayo Clinic, where he has been ever since. By July 1975, he was a full professor of medicine and 6 years later a full professor of laboratory medicine at Mayo Medical School.
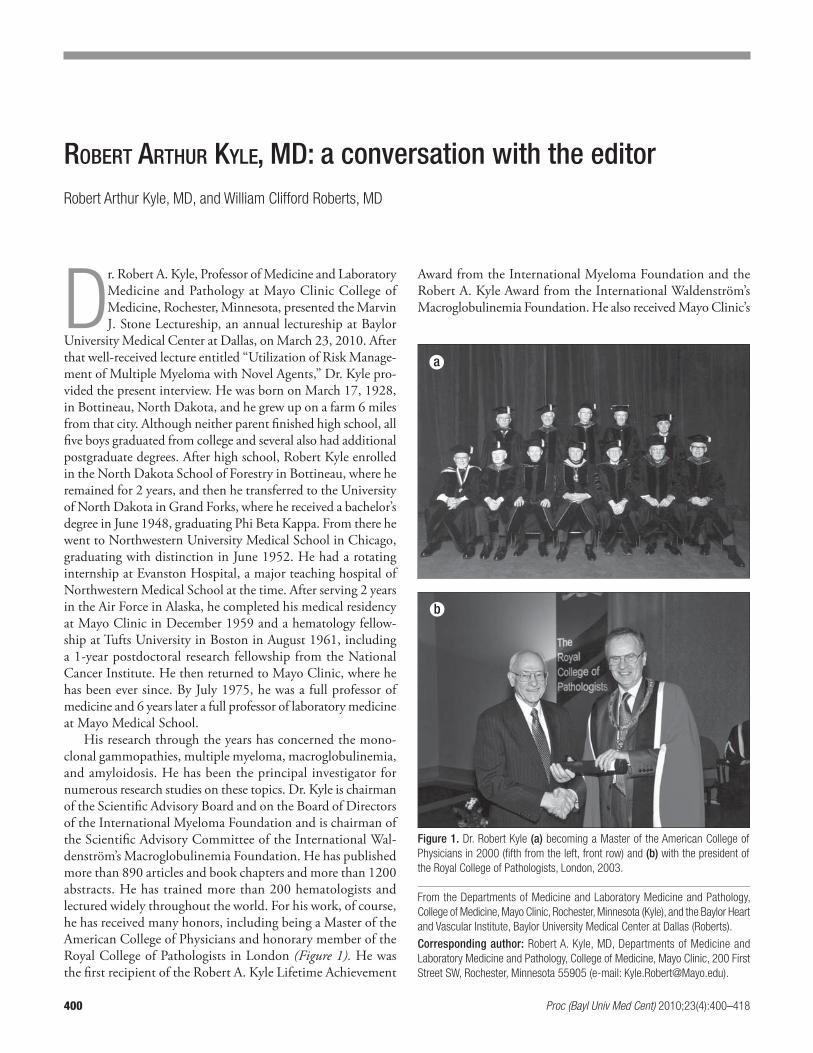
His research through the years has concerned the mono-clonal gammopathies, multiple myeloma, macroglobulinemia, and amyloidosis. He has been the principal investigator for numerous research studies on these topics. Dr. Kyle is chairman of the Scientifi c Advisory Board and on the Board of Directors of the International Myeloma Foundation and is chairman of the Scientifi c Advisory Committee of the International Wal-denström’s Macroglobulinemia Foundation. He has published more than 890 articles and book chapters and more than 1200 abstracts. He has trained more than 200 hematologists and lectured widely throughout the world. For his work, of course, he has received many honors, including being a Master of the American College of Physicians and honorary member of the Royal College of Pathologists in London (Figure 1). He was the fi rst recipient of the Robert A. Kyle Lifetime Achievement
Award from the International Myeloma Foundation and the Robert A. Kyle Award from the International Waldenström’s Macroglobulinemia Foundation. He also received Mayo Clinic’s
From the Departments of Medicine and Laboratory Medicine and Pathology,
College of Medicine, Mayo Clinic, Rochester, Minnesota (Kyle), and the Baylor Heart
and Vascular Institute, Baylor University Medical Center at Dallas (Roberts).
Corresponding author: Robert A. Kyle, MD, Departments of Medicine and
Laboratory Medicine and Pathology, College of Medicine, Mayo Clinic, 200 First
Street SW, Rochester, Minnesota 55905 (e-mail: [email protected]).
ROBERT ARTHUR KYLE, MD: a conversation with the editorRobert Arthur Kyle, MD, and William Clifford Roberts, MD
D
Figure 1. Dr. Robert Kyle (a) becoming a Master of the American College of
Physicians in 2000 (fifth from the left, front row) and (b) with the president of
the Royal College of Pathologists, London, 2003.
a
b
Proc (Bayl Univ Med Cent) 2010;23(4):400–418

October 2010 401
Henry S. Plummer Distinguished Internist Award, Distin-guished Clinician Award, and Distinguished Alumni Award, as well as the David A. Karnofsky Award and Lecture from the American Society of Clinical Oncology and the Wallace Coulter Award from the American Society of Hematology.
He and his wife are the proud parents of four off spring. He has been an active member of the First Presbyterian Church of Rochester for over 50 years, formerly president of his local parent/teacher association, and chairman of a local Boy Scout troop. It was an honor for Baylor University Medical Center at Dallas to have such a distinguished and gracious individual stimulate our intellects, and we are indebted to Dr. Marvin Stone for bringing Dr. Kyle to our medical center.
William Clifford Roberts, MD (hereafter, Roberts): Th ank you, Dr. Kyle, and also Dr. Stone, for making our discus-sion possible. To start, could you talk about your early childhood, your parents, your siblings, and your environment growing up?
Robert Arthur Kyle, MD (hereafter, Kyle): I was born in Bottineau, North Dakota, on March 17, 1928—St. Patrick’s Day. At the time, my father was owner of a vulcanizing shop (tire shop), which he operated for several years. Two years after my birth we moved to a farm he had purchased because he felt that working with tires was unhealthy. He had contracted tuber-culosis during World War I when he was in the Army Aviation Corps. His parents and a sister had died of tuberculosis (“white death”). Our farm was 6 miles from Bottineau, which then had a population of 2500. I visited a rural one-room school when I was 5 years of age just for fun and enjoyed it and said that I wanted to start school that fall. Th ere was no kindergarten at that time. My father was on the school board and there were very few regulations then about entering school. I started fi rst grade at age 5 (Figure 2). In North Dakota students had to pass state examinations at the end of the seventh grade—health, English, history, etc. My teacher suggested that I take the examinations to get experience for when I really had to take them the next year. I took them and got one of the highest grades in the county. When I passed, they promoted me to the eighth grade. I was 2 years younger than my classmates.
In the eighth grade students had to pass three other examina-tions to graduate. In the one-room school there were 15 to 20 children in all eight grades and one teacher. At age 12, I entered
high school, which was in Bottineau 6 miles away. No one drove during the winter since the weather was so severe. My mother arranged for me to stay with her brother and his wife during my ninth grade year. I didn’t really like this arrangement. Most kids from the farms would rent a room in town and do their own cooking. Later, I rented a room in my uncle and aunt’s home. Th ere were three or four other students staying there also. I would go home on Friday night and then my father would bring me back on Monday morning. At the time I weighed 90 pounds and was 4´10´́ tall. I hadn’t even reached puberty and here I was in high school.
I enjoyed school. I preferred school to farm work. I gradu-ated from high school in 1944 (during World War II). I was virtually the only boy in my high school graduating class who did not go directly into military service. I took the Army Special-ized Training Exam when I was 15 and passed it, but I was too young to enter the service. After graduating from high school, I worked that summer for the US Forest Service in Idaho as a lookout-fi reman in a lookout tower. Th en I went to the North Dakota School of Forestry, which was a junior college in my hometown. My parents believed that at 16 I was too young to go away to university, so I went to the Forestry for 2 years. I took science courses mainly and graduated with an associate degree and then went to the University of North Dakota.
One of my Forestry professors worked for the Bureau of En-tomology and Plant Quarantine during the summertime. Th is was a mobile crew that traveled through Washington, Oregon, and British Columbia looking for abandoned pear orchards because they were considered to be the potential sites of an insect called pear psylla. We would spend a couple of weeks in one town searching for pear trees and then move on to another town. It was wonderful and I had my own truck and search area to cover. For a student, it was a well-paying job.
Roberts: Where is the University of North Dakota?Kyle: It’s in Grand Forks, which is 200 miles southeast of
Bottineau. It’s on the Red River, 70 miles north of Fargo.Roberts: During your entire elementary period, only 15 stu-
dents were in the one-room school?Kyle: Yes, 15 in the entire one-room school with grades 1
to 8 and all students taught by one teacher. She would com-bine third-, fourth-, and fi fth-grade English and seventh- and eighth-grade history, etc. It was like the more modern Mon-tessori schools where children “proceed at their own speed.” I could hear the teacher’s presentations to the other children in other grades. When it was time for my class to interact with the teacher we would move up to the fi rst row. Th e teacher would discuss a subject with us for about 15 to 20 minutes and then we would go back to our regular seats.
Roberts: What time did school start?Kyle: It started at 9:00 am and fi nished at 4:00 pm. Students
brought their lunches because we lived a mile from the school. Th e teacher was paid $60 a month.
Roberts: Th at was between 1933 and 1940?Kyle: Yes. I started high school in 1940. I lived in town
with my aunt and uncle the fi rst year of high school and then on my own the remaining 3 years of high school. I cooked my
Figure 2. “Bobby” at about age 5.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4402
own meals during that time. Even when I went to the Forestry, I cooked my own meals. My younger brother later joined me.
Roberts: He was your only sibling?Kyle: No. I had four brothers (Figure 3). Roberts: Where are you in the hierarchy?Kyle: I’m the oldest. Roberts: What are your brothers’ ages and names?Kyle: My next brother, Bill, was 2 years younger than I.
He fi nished 2 years of junior college and 2 years at Wahpeton School of Science and became a plumber/pipe-fi tter. He passed away 10 years ago. Th e next, Jack, is 4 years younger than I; he went to Jamestown College, a Presbyterian college, and to Princeton Th eological Seminary and became a Presbyterian minister. He is now 78 years old and still serving in Western Pennsylvania. My next brother, Don, was born in 1936. He initially went to the Forestry, then to the University of North Dakota, and then to Northwestern University Dental School. He is a practicing dentist in Rockford, Illinois. My young-est brother, David, also went to the Forestry and then to the University of North Dakota, majoring in mathematics. By the time he graduated my father was rather old and wasn’t able to farm. David decided to stay and help my father on the farm, and he still farms today.
Roberts: Did your mother and father have the opportunity of going to college?
Kyle: No. My father was orphaned when he was 8 or 9 years old. His parents contracted tuberculosis brought home by a daughter who taught school. He was the youngest of eight children. His older sisters took care of him until they married and moved away. He never went to high school. My mother was born on a farm and started high school but became very
Figure 3. The Kyle brothers (a) in 1964 (front row: David, Bob, Don; back row:
Bill, Jack) and (b) in 2002 (left to right: Jack, David, Bob, Don).
a
Figure 4. Kyle Farms. (a) About 2002. (b) Bob at Kyle Farms, 1999.
a
b
b

October 2010 403
lonely and went home. She started working in a depart-ment store after her fam-ily had moved to Bottineau. Both of my parents regretted the fact that they had no edu-cation to speak of. Although he did not like farming, my father did it. From day one, we kids knew that we would all go to college. Our parents didn’t care what we studied, but we were going to get an education because they were unable to.
Roberts: How many acres did the farm consist of?
Kyle: My father started with 160 acres. Th at’s the usual homestead size throughout the West. During the time I was growing up he accumulated more land, and when I was in high school he was farming 720 acres, a pretty good sized farm at that time (Figure 4). Now my brother farms about 5000 acres, and that is why the population of Bottineau County was higher in 1914 than it is today. In 1914, every farmer lived on a home-stead of 160 acres and had a relatively large family because it took a lot of kids to do the work. Now, one man can do all of the farming due to mechanization.
Roberts: What were your parents’ names?Kyle: Arthur Nicol, born in 1892, and Mabel Crandall,
born in 1900 (Figure 5). Roberts: When did they marry?Kyle: 1924. Roberts: Th ey both lived in Bottineau at the time they met?Kyle: He was living with a brother in a small town about
30 miles away. When he came to the store in Bottineau he saw a young lady who was the clerk and things progressed from there. When they married, he had moved to Bottineau and was running the vulcanizing shop.
Roberts: What is the winter weather like in Bottineau?Kyle: It was often –40° with lots of snow. I would walk
to school and, being a young tough guy, wouldn’t wear earmuff s.
Roberts: Th at’s when you were living in town?Kyle: Yes, all the rural children stayed in homes in town.
When I went to the rural school, I would walk initially, but my father would walk three quarters of the mile with me and then would stand on the corner and watch me go the rest of the way. Going home, I walked with an older girl who lived farther than I did. When I was 5, my parents had to make sure I didn’t get lost. When I became older I rode a pony to school (Figure 6).
Roberts: What was your home like on the farm? Kyle: It was pleasant. I enjoyed it. I read a lot. My younger
brother was much more mechanically skilled so he wanted to work with his hands and drive the tractor. I was happy doing the labor. My father planted several hundred trees around our
home because there weren’t any. It was my job to weed the trees in the summertime.
Roberts: How many months of the year would snow be on the ground?
Kyle: Snow would come in November and melt off by the fi rst of April.
Roberts: Was the evening meal at your home a big deal?Kyle: Yes, but I don’t remember a lot about it. I remember
that chicken and gravy was a favorite. Cakes, bread, and rolls were my mother’s specialty. We ate after working all day and oftentimes there was something to do at night. I would read whenever I had a chance.
Roberts: On the farm there is never a time when there is not something to do?
Kyle: Correct. I didn’t really like it. My brother who be-came the Presbyterian minister didn’t like it either. We both went to the Forest Service during the summers. My brother cooked, and he cooked for the fi refi ghters when they were fi ghting a fi re. He did this for 7 or 8 years, all through college and seminary.
Roberts: What was your father like?Kyle: He was very quiet and didn’t say much, but he was a
good thinker and very successful in what he did. Roberts: Was he close to the fi ve boys?Kyle: Not as close as my mother was. My mother was a real
people person. She knew everybody in the county and everyone knew her. She drove her car until a day before she died at age 94. She was remarkable.
Roberts: When did your parents die?Kyle: My father died in 1967 and my mother in 1994. She
was a widow for almost 30 years. She really missed him.Roberts: Th ey had a close marriage?Kyle: Yes. Even though he didn’t say much and wasn’t de-
monstrative, they respected each other and had a close marriage. Life was never the same for her after he died.
Roberts: You said you read a lot as a child. Did you read fast?
Kyle: Yes.Roberts: Where did you get the reading material?
Figure 5. Arthur and Mabel Kyle,
1964. Figure 6. Bob on his pony, King, en route to school, 1939.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4404
Kyle: Th e town library. Most of the time we went to Bot-tineau once a week for groceries and other supplies, and the kids would all go to the library and check out a bunch of books.
Roberts: What did you enjoy reading?Kyle: Virtually everything from biography to history.Roberts: Was anybody in your extended family a physician?Kyle: No. Roberts: What turned you onto medicine?Kyle: My mother was talking to a friend one day when
I was around 10 years old, and they were discussing what I should do with my life. Th e friend suggested that I become a doctor. I thought that was a good idea. I kept it in the back of my mind. During high school the library carried the Annual from the University of North Dakota and I would look at the 2-year medical school section. I liked science. When I was at the Forestry my brother lived with me. We couldn’t go home on weekends when the weather was particularly bad. We could not have made it home.
One Sunday morning after arising, my brother had diffi culty speaking. I didn’t know what was wrong but realized that he was seriously ill. I walked to the doctor’s offi ce, which was a mile away, and got him to come back with me to our house. My brother was semicomatose by this time and the doctor and I carried him downstairs and then drove him to the hospital. Th e doctor was a very capable physician. He had graduated from the University of Minnesota and had taken his internship at Detroit Receiving Hospital. He diagnosed meningitis clini-cally and did a spinal tap to confi rm it. He put him on sulfa. Th en he said that he wanted me to nurse him. I didn’t know anything about nursing but he told me what to do. I stayed in my brother’s room for nearly 2 weeks. Th e doctor said that I had already been exposed and it would not make any diff erence for me. Th at experience increased my interest in medicine.
Roberts: How old were you at that time?Kyle: Sixteen.Roberts: And your brother was 14? Did he recover all right?Kyle: Yes, he recovered perfectly. He had no neurological
residuae.Roberts: Your parents had tuberculosis?Kyle: My father apparently did. It was during World War
I but I’m not sure of the diagnosis. He had an abnormal chest x-ray but he was never in a sanitarium. He was told to get “good air.” In fact, he spent a winter in Kansas City and another in Denver for the weather. He never had overt disease. I have a positive skin test for tuberculosis.
Roberts: Your father was in the Army Aviation Corps in World War I?
Kyle: Yes. He was an airplane mechanic. We had a picture on our dresser with him sitting in an airplane with a good head of hair. I don’t remember him with hair. He was always bald. He was at Randolph Field in Texas initially and then Langley Field in Virginia. He always said that it was the hot and humid weather in Virginia that made him lose his hair.
Roberts: How many students were in your high school?Kyle: Th ere were about 170 students in the high school, 38
in my graduating class.
Roberts: Did you graduate fi rst in your class?Kyle: No, two girls were fi rst. I was third. We had our 65th
high school reunion in 2009.Roberts: There were no sporting activities in your high
school?Kyle: We played football, softball, and basketball without
coaches. We played tackle football without equipment. But those were unoffi cial games because of the lack of coaches dur-ing World War II.
Roberts: Everything was intramural sports?Kyle: Yes and very disorganized. And I was younger than
everyone else.Roberts: How many students did the Forestry have?Kyle: Probably 40 students.Roberts: Th e reason you went there was because you were too
young to enter the service and because your parents did not think you were old enough to go away to college?
Kyle: Correct. Th e local college was easy to get to and they didn’t really like a 16-year-old going 200 miles away. Th at was a long distance at that time for someone so young. My parents were frugal and watched money carefully, but when it came to school we always had our tuition paid for, including medical school for me. I went to Northwestern, which was an “expen-sive” school. It was school fi rst. None of us had any school debt when we graduated from college or graduate school.
Roberts: All siblings worked during the summer?Kyle: Yes, but tuition was considerably lower back then,
and working in the summer gave us spending money for the rest of the year.
Roberts: Did your family ever travel for a vacation?Kyle: We never traveled except to visit relatives in Canada
or relatives in the area. Once a year we went to Minot, 80 miles away. Th at was the closest “large” city.
Roberts: What did you do there?Kyle: We would spend the whole day. We always went in the
fall. One year my parents bought my brother and me sheepskin coats. Minot was a big event. My mother bought clothing—corduroys, fl annel shirts, things we needed for school.
Roberts: What was the Forestry community college like? Kyle: It was very small. I was active in dramatics and acted
in several plays. We had no athletics because there were no coaches. And, I was the only boy!
Roberts: Why were you the only boy?Kyle: Because everyone else was in the military service. Th is
was during World War II. On May 8, 1945, the announcement came that Germany had been defeated.
Roberts: But you still expected to be in the Pacifi c arena?Kyle: Absolutely. When I reached 18 I had the mumps
and I couldn’t register with the draft board on the 17th of March—my birthday. It was the law to register on one’s birth-day. I was home and couldn’t register until the 27th of March. I was immediately sent by train to Fort Snelling in Minneapolis for a physical examination. I was told that I would be taken into the army and not allowed to fi nish my sophomore year of college, but within 2 or 3 months of Germany’s falling, the federal government decided not to draft teenagers any longer.

October 2010 405
When I went for the physical, they said I should sign up and do 1 year of active duty and my military service would be over. I decided not to do that and to continue in school. I fi nished my sophomore year and that fall took the train to the University of North Dakota in Grand Forks.
Roberts: You didn’t have much choice about which university you would go to?
Kyle: Th ere was never a consideration of going anyplace else. Th e University of North Dakota was considered the best school in the state and the largest. My brother did go to Jamestown College, a liberal arts college, which was much smaller, but he was already interested in the ministry. Th e rest of us went to the University of North Dakota. Th ere wasn’t even a thought of going to the University of Minnesota. It was too far away.
Roberts: Did your family go to church every Sunday? Kyle: Yes, on Sunday mornings. Our parents drove us to
town and we went to Sunday School class every Sunday. Roberts: You all piled into one car?Kyle: No, because my youngest brother was born in 1943
when I was basically gone. But prior to that, yes. My father would take us into town but he didn’t stay for Sunday school and my mother was usually at home. Th en, he would go visit relatives and pick us up after it was over. During high school I would stay in town and go to the church service and my parents would bring in my younger siblings. But my father didn’t go to church much. It was my mother who insisted upon it. She was born and raised a Lutheran and my father was born and raised a Presbyterian. In fact, his father was born in Ireland. All fi ve boys have been very active in the church: one brother is a minister; the brother in Rockford is very active in the Presbyte-rian Church; my youngest brother is active in the Presbyterian Church in Bottineau; and I’ve been a member of the Presbyte-rian Church in Rochester for over 50 years.
Roberts: Do you go to Sunday school now?Kyle: No. My wife doesn’t enjoy Sunday school, so she meets
me halfway and we go to church together. Roberts: What was the University of North Dakota like since
this was the fi rst time you were really away from home?Kyle: It was tough. I had signed up for a dormitory room.
Th is was in 1946 when the veterans were coming back, and it was very congested. My dormitory room was like barracks. I took one look and couldn’t believe it. How was I going to study? Th ere were 50 double-bunk beds just like barracks! I was told I would be able to study in the library. I knew that wasn’t going to work. I saw a note on the wall in the registrar’s offi ce that said “Room and board available—no smoking and no drinking and will share a room with my nephew.” I went to see this setup since it was near the campus. Th e nephew was a freshman. He and I shared this small room and his aunt, my landlady, prepared our meals. I was able to study. Th ey were very strict and very religious and they even took me to their church, United Brethren. Every Sunday I had to go to church. I snuck away especially during my senior year and became active in the Presbyterian youth group. But I still felt obligated to go to their church on Sunday mornings.
Roberts: How far was that from the school?
Kyle: About 2 miles.Roberts: How many students were at the University of North
Dakota when you were there? And how many were in your class?Kyle: In my graduating class, 220. Th e entire school prob-
ably had about 1400 students. I came as a junior. Th at junior class consisted mainly of female students and a few 4Fs. Th e bulk of the male students were in the fi rst 1 to 2 years of college, having just gotten out of military service.
Roberts: How did you handle being the only male in the Forestry college?
Kyle: I was 2 years younger than anybody. I was friends with all the girls. Th ey treated me like a kid-brother.
Roberts: What did you study at the University of North Dakota?
Kyle: Organic chemistry was the make-or-break course. You either got an A or at worst a B. Anything lower prevented acceptance into medical school. In my junior year I told the dean of the medical school that I was interested in medical school. Th e dean said that things were bad and that the medi-cal school building had been condemned. He stated that the medical school would close unless a state referendum passed. He suggested that I apply to Harvard, Pennsylvania, or Johns Hopkins if I wanted to be a professor of medicine. But, if I wanted to be a real doctor, I should go to Northwestern! Guess where the dean had graduated from? I applied to Northwestern and also to Penn and to one other school. He told me that if I didn’t get accepted by one of these three then I had a place at the University of North Dakota. He advised that I take another year of college—any courses I wanted—because I was only 18 years old. So I did. I got accepted at Northwestern, and a couple of weeks later, to Penn, which I turned down. (Some years later one of my neurology colleagues at Mayo Clinic had gone to Penn and graduated in 1952, the same year that I graduated from Northwestern. Frank was on the alternate list at Penn, and I always told him that I was responsible for his going to medical school because he got my place!)
Roberts: At the University of North Dakota did you have fraternities or other nonscholastic activities?
Kyle: I did not join a fraternity because it would have cost more than I had. I was getting my meals and room for $40 a month, which was a fair amount of money then. I felt that I needed to conserve. I wasn’t interested in partying. I was still studying hard and had taken the advice of my organic chem-istry teacher who told us to spend more time at our desks in a hard-backed chair.
Roberts: How did you rank in your class?Kyle: I don’t know. I believe that I would have been in the
top few percent. Th ere were some very serious students there. Th e place was fi lled with students who had been in the military and many were married with children. Th ey were very competi-tive for those As.
Roberts: Were there any teachers from grade school to university years who had a particular infl uence on you?
Kyle: Yes. In the rural grade school there was Helen Gibbons, a wonderful woman who taught me for 3 years. She was the one who suggested that I take the seventh-grade exam
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4406
early. She grew tired of teaching, went to Minneapolis, learned to be a lab technician, and returned home and worked for our family doctor. Unfortunately, she had a cholecystectomy fol-lowed by a pulmonary embolus 2 days later and died. Another memorable grade school teacher was Ethel Sanderson. Th e grade school teachers had very little college experience. When I gradu-ated from high school in 1944, most of the girls in my high school graduating class went to Minot State Teacher’s College for 3 months in the summertime and started teaching at a rural school in September of that same year. Th en, to maintain their licenses they had to go to summer school each year. Th ere was no fancy curriculum planning. Th ese were high school graduates who taught kids. In high school I had a very impressive history teacher, Frank Szczys. He was second-generation Polish. He was very interesting and stimulating. In college, Th omas Street, my zoology/botany teacher, was very stimulating. He was the one who got me the job with the Bureau of Entomology and Plant Quarantine. My organic chemistry teacher, Walter Moran, at the university was very tough. Dr. George Abbott, head of the chemistry department, was kind and nice to the students.
Roberts: You certainly have a wonderful memory. Your capac-ity to know these people must have been very good.
Kyle: I got that from my mother (Figure 7). She knew eve-ryone in the county.
Roberts: Was alcohol ever a part of your life?Kyle: Not until I went to medical school and it consisted only
of beer at fraternity parties. Th ere, I did join a fraternity. Students lived in Abbott Hall, a 20-story building, on Lake Shore Drive. It was half a block from the medical school in downtown Chicago.
During the fi rst week I joined Alpha Kappa Kappa. One of their initiatives was to have big tutoring sessions for the freshmen. Each fraternity had a fl oor at Abbott Hall. Th ere was one other fraternity that had its own house where they had great parties and lots of fun. I knew to stay away from that fraternity.
I shared a room with a fellow from Evanston. His father was an obstetrician-gynecologist. After the fi rst year Bud moved back home and commuted to school. By that time I had met another fellow from Indiana who had gone to both Northwest-ern and West Point and in the same class as Glenn Davis and Doc Blanchard, the football All-Americans. Doc Blanchard was a very smart guy according to my roommate; Glenn Davis was not. My roommate, Cal Rumbaugh, and I had the same study habits. We went to bed at 11:00 every night. At that time medi-cal students had to memorize everything. Even in bacteriology, we had to memorize the characteristics of the bacteria. (In real life you just open the page in the book and look.) We would get up sometimes at 5:00 am and study until exam time. Many of our classmates would study all night during fi nals week but Cal and I would study throughout the year and did not have to cram during fi nals. We stayed roommates for 3 years in medi-cal school and both interned at Evanston Hospital, and then he became a neuroradiologist at Peter Bent Brigham Hospital. He retired to California (Santa Barbara) but has a condo at Charter House in Rochester, Minnesota. He comes back three or four times a year.
Roberts: Northwestern was a big deal for you?Kyle: Oh, yes (Figure 8).Roberts: Did anyone else
from the University of North Dakota get in there?
Kyle: Not as a freshman, but the University of North Dakota did have a very good reputation for the 2 years of basic science. At the end of 2 years, Harvard usually took two or three, Penn took two or three, and Northwestern took three or four students.
Roberts: How many were in your class at Northwestern?
Kyle: 128. When the dean greeted us, he said that they had selected us from over 2000 applicants and that we had the ability to pass in medical school. It was all up to us.
Roberts: Were there surprises for you in medical school?Kyle: All students were good and serious. Our professor
of surgery was Loyal Davis, the stepfather of Nancy Reagan. He was from Galesburg, Illinois, and I think he had a major inferiority complex. He considered himself absolutely brilliant. During our freshman year of medical school, every Saturday morning we had a surgery seminar. At the very fi rst one, one of my very good friends, Harry Miller, walked into the back of the room in a yellow sweater and Dr. Davis asked, “Who is that guy in the yellow sweater? I never want to see that again.” My
Figure 7. With Mabel Kyle, age 87.
Figure 8. At Northwestern University
Medical School, 1950.

October 2010 407
friend just about fell to the fl oor. Davis was mean. He consid-ered himself an expert on everything, including the anatomy of the hand. Allen Kanavel in the 1930s was considered the father of hand surgery and described the compartments of the hand. One day Dr. Davis asked us to draw the compartments of the hand on our palms and then hold our hands up. He walked up and down the rows slapping the palms saying, “Wrong, wrong, wrong.”
Th e worst was during the junior year’s formal surgery course, which was didactic with periodic exams by the various surgical professors. Our fi nal grade was dependent upon a personal in-terview with Loyal Davis in his private offi ce on North Michigan Avenue. When I walked into his offi ce my knees were virtually knocking together. He asked some anatomical questions and ap-parently must have thought I did not do well in that examination because he gave me a B– for the whole surgical grade despite the fact that I made As on all the periodic examinations. Subse-quently, I learned that I was the top student in the class who did not make Alpha Omega Alpha. I think there were 13 who made it. I don’t hold any malice toward Davis, but he was a miserable person and I am not the only one to have thought so.
Davis drove away good professors. Frederick Christopher, a senior surgeon at Evanston Hospital when I was an intern there, was a splendid teacher and highly regarded by the housestaff . He edited Christopher’s Textbook of Surgery, which was the major text for surgery in most medical schools. I scrubbed with him on several occasions as an intern. He was a wonderful person to work with. Davis virtually drove him out of the medical school. Karl Meyer and Peter Rosi were renowned gastrointes-tinal surgeons in Chicago, and they would have nothing to do with Davis. Th e only staff surgeons at Northwestern were young assistant professors, who kowtowed to Davis.
Roberts: In medical school did you have diffi culty deciding on your life specialty?
Kyle: No. I had always planned to do family medicine. But, during a clerkship at Passavant Hospital, where Loyal Davis was, I decided that I would do medicine and that’s why I went to Evanston Hospital where Davis was not! Evanston was considered to have the best internal medicine program at Northwestern and the best internist there was Frank Kyser, who had trained at Mayo Clinic. He had been in practice for about 10 years and had a wonderful general medical practice. If an intern could get on his service early in the rotation and did well, Kyser would write a recommendation for Mayo Clinic in Rochester and you would go. I did that.
During my internship (Figure 9), I rotated on anoth-er service where a staff member had just come from Mayo Clinic and seemed to know everything. Th at consolidated my wanting to go to Rochester, Minnesota. Th e chairman of medicine at Evanston, a wonderful teacher, told me to stay at Evanston and not go to “the mecca of mediocrity.” I didn’t listen to him. I was happy that I went.
During the time at Evanston the Korean War was going on and I was called up for my physical exam during my internship. I passed and was ready to go into the military when I fi nished my internship. Th en, just a month or two before going into
the Air Force, I was called and told that no more offi cers were needed. I had been accepted at Rochester beginning in 1955 because I had planned to be in the military for 2 years after completion of my internship. I immediately called Mayo Clinic, and they allowed me to start in October 1953.
When arriving in Rochester I was assigned to physical medi-cine. At that time residents in internal medicine spent a year in the outpatient clinics. I told them I came for internal medicine, but they told me that physical medicine would count as a quar-ter of internal medicine. It was one of the best experiences that I had. Frank Krusen was head of that department and considered to be the father of physical medicine in the United States. I saw many neurological and orthopedic patients and learned to use heat, massage, and exercise for backache. Th is experience proved very helpful later in taking care of internal medicine patients. I was allowed to take a month of that 3-month period at the rehabilitation center at Saint Marys Hospital. I had the clinic outpatient experiences for the remainder of my fi rst year.
Th en, I got a notice to report to my draft board in Bottineau with one set of underclothing and toilet articles. I was assigned to basic infantry training at Camp Chaff ee in Arkansas. I called my draft board and asked if they really wanted me as an infantry-man. Th ey had forgotten to tell me that my draft number had come up but said that I should ignore that order and apply for a commission. I applied for a commission after having been at the clinic for only 9 months. A friend told me to say I’d been there a year because one would be classifi ed as an internist rather than a general medical offi cer. I did and it took 6 additional months to get my orders. Th en, the Air Force made a mistake and sent me to a fi ghter wing at Wold-Chamberlain Field in Minneapolis instead of sending me to Gunther Air Force Base, Alabama, for my 3-week indoctrination. When I got to Minneapolis they wanted to know what I was doing there because they had never seen a medical offi cer before. A couple of days later my orders came. I was assigned to Alaska but fi rst had to drive to Fort Lawton in Seattle, Washington. I was told to go to McChord Air Force Base in Tacoma (50 miles from Seattle), which my wife
Figure 9. Interns at Evanston Hospital, Evanston, Illinois, 1952–1953. (R. Kyle
is second from the right in the first row.)
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4408
and I did, to purchase a uniform, a requirement to get on the troopship. I was a fi rst lieutenant with 5 or 6 other army ROTC second lieutenant offi cers when we shipped out. Th ey were all assigned duty in the hold during the 5-day trip to Anchorage, Alaska. It was pretty rough. Many soldiers got sick. I was assigned to the Dispensary at the 5005th Air Force Hospital, and I saw sick-call in the morning (80 to 100 troops) giving out elixir of terpin hydrate for their coughs, etc. Th ey would drink it because it had a lot of alcohol in it. Or, they would have backaches and couldn’t do the undesirable tasks they had been assigned to that day. In the afternoons we saw the dependents.
About 3 weeks after arrival at the base I told the colonel that I was an “internist,” a 9386D, the lowest level. (He was a psy-chiatrist.) I asked if I could be transferred to the hospital. After 3 weeks or so they sent me to the 5005th Air Force Hospital where there were three “real” internists (Figure 10). One had trained at Brooke Army Hospital in cardiology, one had trained at Stanford in gastroenterology, and another had spent 2 years at Queens Square Neurological Hospital in London. Initially, I was assigned to the least desirable infectious disease ward, where I saw a lot of tuberculosis. (At that time tuberculosis was just being successfully treated with para-aminosalicylic acid and streptomycin.) In the dependents’ ward, I saw many young women with pyelonephritis with high temperatures, something I had never seen before. It was a good experience. After about 6 months, I was transferred to the major medical ward of the hospital, a 32-bed ward all to myself. Th ere was a lot of paperwork involved. Th e consultants—previously mentioned—didn’t want to do that. Th ey gave it to me but they were very good at helping me out with consults. I learned more practical internal medicine in the Air Force than I would have ever learned in any sort of residency. After fi nishing my Air Force duty, I returned to Mayo Clinic. Residents had to spend 6 months doing research in a laboratory.
Roberts: At this time you still wanted to be a “real doctor”?Kyle: I wanted to be an internist. Th e research options were
pathology doing autopsies for 6 months; physiology, mainly cardiovascular catheterization (the fellow had to be catheter-ized—something not very appealing to me); and hematology,
consisting of 6 months looking at bone marrows and peripheral blood smears. Because I knew less about it than any of the other subspecialties, hematology was my choice. My project was ac-quired hemolytic anemia in chronic lymphocytic leukemia and lymphoma. I wrote the written exam for my master’s degree and then wrote a thesis. My thesis showed that this group of 27 pa-tients with severe anemia and hemolysis contrasted with patients with chronic lymphocytic leukemia and lymphoma who also had severe anemia but a packed bone marrow. Most of these hemolytic anemia patients had a positive Coombs test and responded to corticosteroid therapy. I thought that I was pretty smart at making this observation, although there had been a few case reports earlier. But then I discovered that Pappenheim, the German physician for whom Pappenheim bodies are named, wrote in 1906 a paper that described the same basic fi ndings as mine. Th e only new thing that I had done was mention the Coombs test, which hadn’t been described until 1950, and the use of cortisone, which hadn’t been introduced until 1948. Pappenheim had the correct concept as well. Th e discovery of the earlier observation by Pappenheim made a big impression on me. I have tried to impart to students that physicians 50 to 200 years ago were just as bright and able, if not more so, than many of our Nobel prize winners today.
During those 6 months of laboratory service I realized that I hadn’t had any experience in clinical hematology, so I signed up for such a rotation. Two things happened on the hematology hospital service that altered my future scientifi c life. First, I saw an electrophoretic pattern for the fi rst time and asked Dr. Edwin Bayrd, the consultant on the service, what that meant. He said that he didn’t know but they saw those big spikes in patients with myeloma and macroglobulinemia. He suggested that I look into it. Serum protein electrophoresis, a new test in clinical labora-tories, was started at Mayo in 1956. It was now 1959 and over 6000 electrophoretic patterns had been performed at the clinic.
Figure 10. As a first lieutenant at Elmendorf Air Force Base, Anchorage, Alaska,
1955.
Figure 11. With Jan Waldenström, about 1991.

October 2010 409
I looked at all of those and devised a formula: height vs. width. I discovered that if the height was greater than 4 to 1 over the width at the midline of the peak then that patient had my-eloma or macroglobulinemia; in contrast, if the ratio was lower then that patient most likely had a chronic infection or chronic active hepatitis, rheumatoid arthritis, or some infl ammatory process. My observation was before Waldenström (Figure 11) had described monoclonal or polyclonal gammopathy. I didn’t know what I was talking about until he published his work in 1960 to 1961. Th e other infl uential event was a patient admit-ted to our hematology service with a diagnosis of “scleroderma.” Th e consulting dermatologist did a skin biopsy that disclosed amyloid. I’d never seen such a patient. It dawned on me that some of those patients I had seen with smaller spikes on the elec-trophoretic patterns had systemic amyloidosis. I then reviewed all 81 cases of primary amyloidosis seen at Mayo Clinic from 1935 to 1959. I made the point that all these patients had abnormal plasma cells in the bone marrow and that some of these patients had frank multiple myeloma. I left it at that.
In 1965, Elliot Osserman at Columbia University in New York described 35 patients with primary amyloidosis, and all of them had Bence Jones proteinuria. Dr. Osserman remarked in his article that Bence Jones protein was very closely related to multiple myeloma. Osserman was roundly criticized by the academic hematologists of the day for his “crazy” theory. Os-serman dropped his work on amyloidosis and moved to acute leukemia, discovering lysozyme in the urine of patients with acute myelocytic leukemia.
Peter Miescher, editor for 30 years of Seminars in Hematol-ogy, published Osserman’s paper in the journal’s fi rst volume. Miescher told me later that the paper was criticized by many investigators. Th en nothing happened until 1971 at the clinical meetings in Atlantic City when George Glenner described three patients with primary amyloidosis in whom he had isolated amyloid fi brils and then sequenced the amino acids in the fi brils. From the same three patients, Glenner found that the Bence Jones proteins were virtually identical to the sequence of amino acids in the amyloid fi brils. Th us, Bence Jones protein, bone marrow plasma cells, myeloma, and amyloid were all in one closely related group. At that same meeting, I bumped into Alan Cohen, who had discovered that amyloid was not a homogenous substance but consisted of fi brillar proteins. (Alan went on to found the Amyloid Center at Boston University.) When I asked him what he thought about Glenner’s work he was doubtful and advised confi rmation. I talked to Ed Franklin, Professor and Chairman of Immunology at New York University, who described gamma heavy-chain disease. Some people still call it Franklin’s disease. (He unfortunately died in his early 50s of a brain tumor.) He was doubtful also about this fi nding.
Th e interesting thing was that Osserman and I were he-matologists and Cohen and Franklin were rheumatologists, and the type of amyloid they saw was AA amyloid, which had nothing to do with monoclonal plasma cells. We were look-ing at a diff erent animal. Glenner went to the University of California San Diego at the end of his career at the National Institutes of Health, where he recognized that amyloid was
present in the brain of Alzheimer patients. He subsequently developed heart failure, later found to be due to senile cardiac amyloidosis!
Roberts: Th is research took place during your fi rst year of fellowship?
Kyle: No, I had actually come to Rochester in October 1953 as a fellow in internal medicine. Th en after 8 or 9 months I got the draft notice and was gone for 2 years before return-ing. During the last few months of my training, the head of the personnel committee invited me into his offi ce and said that I had done well and that they would like me to consider staying at Mayo Clinic. He then looked at his notes and said that they had positions in rheumatology, gastroenterology, and something else, but none in hematology. Th e position would be an “assistant to the staff ,” the equivalent of a very junior faculty member. I accepted (Figure 12).
Roberts: Th is was when?Kyle: 1959. Although assigned to the hematology outpa-
tient area, I wanted more training in hematology. I visited Carl Moore at Washington University in St. Louis. He was a wonder-ful person and a very impressive individual, but the position he off ered me was mainly research and I was more interested in the clinical aspects at that time. I then visited the University of Rochester in New York and visited with Larry Young, who was the head of the division and a very well-known hematologist, and also with Scott Swisher, his associate who also was well recognized. On that visit, they introduced me to Dr. Whipple, of Whipple’s disease and pernicious anemia fame. Th en, I went on to Boston and had an interview with William Dameshek (Figure 13). He was, in my opinion, one of two leading clini-cal hematologists in the country. He was at Tufts. He was the founding editor of Blood, our journal in hematology. Th e other well-known person in the country was Maxwell Wintrobe at the University of Utah who was famous for his textbook on hematology. I had heard during my internship that Wintrobe could be diffi cult so I decided that I wouldn’t visit him.
I accepted the position with Dr. Dameshek and had a won-derful time. After I was there a few months he asked me if I
Figure 12. With Charlene and son, John, at home in Quonset Hut for Mayo
Clinic fellows, 1957.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4410
would assume the responsibility of leading the other fellows in hema-tology around—checking the i r patients’ admitting examinations, etc. For that I would no longer have any night call. I accept-ed. Consequently, I saw all cases ad-mitted. After a few months, Dameshek invited me to work a couple of after-noons each week in his private offi ce. He was the only professor at Tufts
who had a private practice outside of the university. Th is was because he was recruited in the late 1930s to Tufts New Eng-land Medical Center, which also included the Pratt Diagnostic Institute. (Pratt had been a student of Osler.) When Dameshek came to Tufts he insisted upon the opportunity of continuing his own private practice. He built it up during World War II, doing consulting hematology. When a request would come in from Portland, Maine, or Manchester, New Hampshire, or Worcester, Massachusetts, or Groton, Connecticut, he went to those places to give a consultation and he would take his offi ce technician with him. He would go in, introduce himself to the patient, take a drop of blood, do a bone marrow examination, and then his tech, Edith, would stain the slides. He would continue with the history, examine the patient, then look at the peripheral blood and bone marrow smears, make his diagnosis, write his consultation note, and hop in the car and drive back to Boston. (At this time Minot and Murphy were at the Th orndike Laboratory, Harvard Medical School. Minot discovered the role of liver in pernicious anemia. He was the king of hematology but not particularly interested in the clinical aspects, let alone consulting for physicians in the area.) Dameshek built a won-derful practice. When I saw patients in the afternoon I had to write the consulting letter to the referring physician that same day. It was a good lesson for me. He kept his records in a fi ling cabinet. Th e records of patients who had died were put in a dif-ferent fi ling cabinet. I learned, unfortunately, that the number of patient records in the “deceased” fi ling cabinet were larger than the number in the “living” fi ling cabinet. Th at demonstrates what happened to hematology patients at that time.
My expectant wife, two children, and I left Rochester in December 1959. After I was with Dr. Dameshek for a few months I got a call from the head of hematology at Mayo Clinic, who off ered me a position if I was interested in coming back. In the meantime, Dr. Dameshek had taken a liking to me and off ered me a position with him. But Dr. Dameshek was already
60 years old and the university had mandatory retirement at age 65. I knew that I would be washed out with him in 5 years because the new professor and chairman would probably want his own faculty and would retain few, if any, of the current staff . I also noted that a number of Dameshek’s previous fellows, who had elected to stay in Boston, were struggling to develop their own private practice even after a decade. When this off er came from Rochester, I accepted without a second thought. I liked Rochester and the people at the clinic. I came back in August 1961 and have been here ever since.
Roberts: You were with Dameshek how long?Kyle: A little under 2 years. I had had the laboratory expe-
rience at Mayo Clinic for 6 months during my 3-year fellow-ship, then a 3-month hematology hospital service experience, and then experience as assistant to the staff in the division of hematology. Th us, when returning to the clinic I had had a fair bit of hematologic clinical experience and I also had had 2 years of internal medicine experience in the Air Force. I was quite used to taking care of patients. I think it was that reason that Dr. Dameshek invited me to work in his offi ce and to supervise the fellows.
Roberts: You were how old when you returned to Mayo Clinic?
Kyle: 33.Roberts: What is your present age?Kyle: 82. In January 2011 I will have been on the Mayo
Clinic staff for 50 years.Roberts: And you have never stopped?Kyle: I stopped seeing patients in 1999 at the age of 71. Th en
I ran the Special Protein Laboratory for an additional 5 years. Since age 76, I have been in hematology research entirely.
Roberts: Did you do any bone marrow transplants with Dameshek?
Kyle: Yes. Dr. Dameshek became interested in bone mar-row transplantation and he sent another fellow and me to Cooperstown, New York, where Don Th omas was working. He was doing bone marrow transplantation in children with acute leukemia.
Roberts: Th is was what year?Kyle: 1960. Don showed the two of us how to do bone mar-
row transplants. We came back to Boston and did transplants on patients with aplastic anemia. One patient, a 15-year-old boy, had been given chloramphenicol for an upper respiratory infection and developed aplastic anemia. When seen, the teenager was bleeding so vigorously that we had to irrigate his bladder because blood clots were plugging the urethra. Dr. Dameshek believed that a splenectomy needed to be done fi rst and then the bone mar-row transplant. Th e patient is now perfectly well 49 years after the transplant! Early after my return to Mayo I saw a similar patient who also had a great response to bone marrow transplantation. In 1969, we did another transplant and since that time I have done no transplants. Both of the patients are alive—however, each had an identical twin as a donor. I quit while I was ahead!
Roberts: Why did you quit?Kyle: I became more interested in the plasma-cell disorders.
When I came to the clinic, I was in the Department of Internal
Figure 13. William Dameshek, professor of hema-
tology at Tufts University in Boston, 1960.

October 2010 411
Medicine with hematology as my subspecialty. Like all internists at the clinic, I saw patients with general internal medicine prob-lems such as hypertension in addition to hematology. I did many annual physical examinations.
I tried to see as many myeloma and amyloid patients as I could. Th e system was such that all appointments were booked 2 years in advance. We would get a call from a physician with a multiple myeloma patient who he wanted to be examined at Mayo Clinic. I would tell him that I would see the patient and then I would go to the front desk and check to see if there were any cancellations since we were booking so far ahead. A cancellation would be found in approximately two thirds of cases. I would see the rest of the patients as “extras.” Th en, there would be off -the-fl oor consultations. A cardiologist might call for a hematologist and the hematologist would go to the cardiology fl oor and see the patient. In most cases, the cardi-ologist wouldn’t be interested in a myeloma patient and the hematologist would take over and the patient would become part of one’s practice.
At that time, we really did not have an eff ective laboratory to perform immunoelectrophoresis on these patients to identify the type of protein and to determine whether it was monoclonal or polyclonal. Th e clinical chemist who did the electrophoresis was supposed to do the immunoelectrophoresis, but he was very disorganized and not very interested in this. I felt that this had to be done. I went to the National Institutes of Health and spent a week visiting John Fahey and Bill Terry who ran the im-munology laboratory. I learned about electrophoresis and then I spent a week in New York with Elliot Osserman, particularly with his technician, Sylvia Lawler. I learned how to do immu-noelectrophoresis. After a year the head of laboratory medicine gave me permission to establish a laboratory.
Roberts: What year was this?
Kyle: 1968. I trained a housewife to do immunoelectro-phoresis, and she did it very well. Th e volume gradually grew. Shortly after this, I established a clinic for patients with dyspro-teinemias, i.e., myeloma, macroglobulinemia, and amyloidosis. Th at was a wonderful opportunity because I could see the patient and then do the electrophoresis and immunoelectrophoresis in the laboratory. I monitored all of the electrophoretic patterns that came through the clinic every day. If there was a monoclonal protein then I would call the physician and give my advice of what testing needed to be done. I would volunteer to see their patient in the dysproteinemia clinic and they would agree. Af-ter a couple of years the head of laboratory medicine asked if I would be responsible for the electrophoresis laboratory. I said no. My laboratory was for immunoelectrophoresis, and we also tested serum for cryoglobulins and for viscosity (Figure 14). I limited myself to this small area because I knew if I agreed to any of these other tests it would take from my clinical time, and I was still seeing general patients, myeloma patients, and amyloid patients. I still did the hospital service as well as the hematology consulting service, and I didn’t want to reduce my time for clini-cal work. In the 1960s I did most of the chemotherapy for the acute leukemia patients. We were members of Acute Leukemia Group B when Tom Frei was the chairman. It was a very active group and a fun association over those years.
As time went on, I got more referrals for patients with myeloma. For the past 25 years of my practice more than 95% of the patients I saw had protein disorders. I vowed never to refuse to see my previously seen patients if they still wanted to see me. Th at is what makes medicine so rewarding. Th e patient contact here is wonderful, and I have had the opportunity of following many patients for many years.
Roberts: How many publications do you have now?Kyle: I have about 890 peer-reviewed articles and chapters
in books (Figure 15). I also have published about 1200 abstracts, but approximately 500 of them are stamp vignettes that were published in JAMA for 15 years and then the last 25 years in Mayo Clinic Proceedings (Figure 16).
Figure 14. In the Special Protein Laboratory, 2003.
Figure 15. With bound volumes of reprints.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4412
Roberts: How have you been able to be so productive in your research endeavors and carry on the active clinical care of patients? Th rough the years—for example, let’s take 1980—what time did you come to Mayo Clinic in the mornings?
Kyle: I would usually get to work at 7:30 am. I endeavored to see every patient who needed a consultation. Many times I have started a new consult at 6:00 pm and sometimes at 7:00 am. Generally, I would fi nish by 6:30 pm and then the whole family would eat dinner together. I would read to the children and help get them ready for bed and then go to my den while my wife would relax after a day of running after four kids.
Roberts: What time did you go to bed?Kyle: We always went to bed at 11:00 pm.Roberts: You worked 2 to 2½ hours at home most evenings?Kyle: Yes.Roberts: What about weekends?Kyle: When I joined the staff , Mayo Clinic faculty worked
5½ days a week. Th at meant fi nishing on Saturdays around 1:30 pm. In 1968, the clinic decided to go to a 5-day week. Th at decision was made without consultation with the medical staff , which was very upset because we felt that it was a hardship for the patients. Th e patient who was being seen on Friday would then have to wait until Monday, and the staff thought that was bad for the patient. Th at move, however, turned out to be a real bonus for me because I would come in about 6:30 am on Saturdays and work until noon on my research projects.
In the 1960s, I started a record system for collecting data on patients with myeloma and related disorders. I initially used IBM punch cards, which had only 80 entries, so we had to use only a single digit for each entry. After about 10 years, data management improved and I was able to increase the number of entries on each patient. To this day, we keep that system. We now have almost 42,000 patients in that database: over 24,000 with monoclonal gammopathy of undetermined signifi cance, more than 7000 with myeloma, and nearly 4000 with AL amy-loid. I later incorporated that into the Special Protein Labora-tory data. Now, our datasystem is all directly on computer. Our research survey system sends out letters each year to any patient who has not been heard from in the previous year. If
the patient doesn’t respond, then a second letter goes out and if the patient doesn’t respond to that, a telephone call is made. Th ese follow-ups are invaluable, and that was how I was able to develop the concept of monoclonal gammopathy of undeter-mined signifi cance, which I described in 1978. Th is was done by simply going back and looking at all of those records.
Roberts: Nobody in the world has seen the numbers of these types of patients—41,000?
Kyle: Yes, my colleagues and I have seen over 41,000 patients with a monoclonal plasma cell proliferative disorder. I worked backwards to 1960 so we have all patients from 1960 to the cur-rent time. Th e other thing that I did was to save serum samples sent to the laboratory, and we put them in a freezer. We now have probably 250,000 frozen serum samples on these patients.
Roberts: Th e storage facility for all these samples must be in-credible.
Kyle: We have many freezers and the administrators peri-odically ask me if I really need all these freezers, especially the old ones. I tell them that the old ones are the most valuable. I’ve been able to maintain all of these freezers over the years in a warehouse off site.
Roberts: How many patients come to Mayo Clinic each day?Kyle: Over 1350.Roberts: Out of the 1350, how many come into the hospital?Kyle: About 20% of the total, about 270 a day. Roberts: How many beds are in your two hospitals?Kyle: Th e number of beds in Saint Marys is almost 1200,
and in Methodist, 800. Th ose are the number of beds they are approved for. About 1500 are used daily.
Roberts: How much time did you spend in the hospital when you had a lot of patients?
Kyle: I would take the hospital service about 2 to 3 times per year for 4 weeks, or about 2 or 3 months each year. Rounds would take about a half day on the hospital service. We would have 15 to 20 patients at a time. In the afternoon I would go to the laboratory for a couple of hours and then go back and see outpatients.
Roberts: When you were on the hospital service, what time did you get home?
Kyle: About 6:00 or 7:00 pm. I had to dictate at night. My writing was more limited when I was on the hospital service.
Roberts: You made rounds on the weekends?Kyle: Yes, both Saturday and Sunday.Roberts: Did you have any administrative responsibilities?Kyle: I served as a section head in hematology for 10 years
and then became chairman of the Division of Hematology for 5 years (Figure 17). I preferred to do other things and stepped down in order to resuscitate our program project grant on monoclonal gammopathies.
Roberts: How did you get into stamp collecting?Kyle: In 1965, I got up from my chair in my offi ce one
day to examine a patient and I felt a snap in my back, but I didn’t pay much attention to it. Th e next morning I had spasms and was unable to tie my shoes. Later that day while sitting in the hematology lab, the pain became worse and I called an orthopedist, who hospitalized me. I was there for
Figure 16. Bob and colleague, Marc Shampo, authors of Medicine and Stamps,
3rd ed., 2005.

October 2010 413
40 days. I decided on a con-servative approach rather than surgery. Although I had had a passing interest in stamps and bought panes of commemorative stamps at the post offi ce, I decided at that time to examine stamp collecting more closely. I bought the Scott Stamp Catalogs, which have every stamp from every country in the world. At that time there were 4 or 5 volumes. I paged through each volume looking for stamps that com-
memorated blood transfusion or cancer. Th en, I began accu-mulating these stamps. For my blood transfusion collection, there was a stamp from Mongolia issued in 1963, but I could not fi nd that stamp anywhere. Later, I looked at every stamp store I came across in various cities. I had a friend who worked for the Los Angeles County blood bank, and he scoured the West Coast. Th en a friend of mine, Marc Shampo, got an ac-cumulation of stamps in a shoe box, and lo and behold there were two of these Mongolian stamps. He gave me one. What do you suppose that stamp was worth? 40¢! Probably the only people in the world who were looking for that stamp were my friend and me.
I then wrote a number of papers on blood transfusion and stamps. At that time, a pediatrician in Philadelphia, Irv Wolman, was very interested in getting a stamp for blood trans-fusion in the USA. We wrote a couple of articles and didn’t make much headway until the American Association of Blood Banks got behind this eff ort. Such a stamp was issued in 1971. I was invited to the First Day Ceremony in New York. I also became interested in cancer stamps. I collected all of those that were in the Scott catalogs. I wrote about them. A number of stamps are called “semi-postal stamps,” in which the stamps sell for a few cents more and those few pennies go for cancer control. Th e US breast cancer stamp is an example. I then wrote to many foreign countries and asked them what they did with the money.
Over the years my wife and I exhibited our collections at na-tional stamp shows. Th en, I got a call from one of the JAMA edi-tors asking me to edit some previously published stamp vignettes that they wanted to publish in a book. I asked my colleague, Marc Shampo, who worked in the Publications Department at Mayo Clinic and who also was interested in stamps, to help in revamping the vignettes. Th en JAMA asked us to continue writing stamp vignettes. When JAMA stopped, Mayo Clinic Proceedings took over.
Roberts: How many have you done so far?Kyle: About 500. I purchased, at auction, a fantastic collec-
tion of cancer stamps. I have been very active in stamp circles. In fact, I am a Distinguished Medical Topical Philatelist from the American Topical Association and served as president of the Medical Subjects Unit for 4 years.
Roberts: How much time have you spent a week on stamps through the years?
Kyle: I don’t spend as much time on it now as I did. I still get Scott’s monthly and I still record the stamps, but it’s harder to get the stamps now. I used to have a dealer who would send out a list and I would check off the ones I wanted and send it back. Now if I send a wish list to a dealer they pay little atten-tion to it. Th e dealers now are mainly interested in the rare and valuable stamps.
Roberts: How many shelves does your collection consist of?Kyle: I have a number of volumes and several shelves full.Roberts: In actuality, that lower back pain turned out to be
a blessing?Kyle: Yes. Th ree years later I had a relapse and was out for
3 weeks. A couple of years after that I had another episode and was out for a few days. I wore a back brace for 11 years and haven’t had back pain since.
Roberts: And you’ve never had surgery?Kyle: Never. Th e only residua is that my back is stiff and I
can’t touch my toes, but aside from that, no pain.Roberts: And you are a healthy man?Kyle: Yes. I feel good. My energy level is very good and I
walk up 6 fl ights of stairs to my laboratory and offi ce. Roberts: Your ideal body weight is what?Kyle: I actually weigh 8 or 10 pounds less than I did when
I was 30 years old.Roberts: How tall are you?Kyle: 5´9´́ . Roberts: How much do you weigh? Kyle: 163 pounds. I work out 3 days a week for about an
hour each time.Roberts: Tell me about your wife. What is her name and how
did you meet?Kyle: Her name is Charlene Showalter. She was born in Co-
lumbus, Ohio, and grew up in Harrisburg, Pennsylvania, and Rockford, Illinois. She had 2 years of college and then 3 years of nursing. She was a senior nursing student when I was an intern at Evanston Hospital. I saw this cute nursing student who winked at me all the time when Dr. Raleigh was trying to teach me cardiology (Figure 18). She, of course, says absolutely not!
Roberts: How old were you at that time?
Kyle: I was 24 and Char-lene was 22.
Roberts: You have four children?
Kyle: Our oldest is John, born in Alaska in 1956. He teaches physical sciences in high school.
Mary was born in 1958. She studied environmental sciences in college with a mi-nor in parks and recreation. After graduating from col-lege, she was engaged to be
Figure 18. Charlene Mae Showalter,
1952.
Figure 17. As chairman of the Division
of Hematology, 1988.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4414
married to a graduate student and got a job in a laboratory working for a professor. She had very little laboratory experience but either read about the experiment or learned how to do it from another lab. Th e professor took a liking to her and after a year or so asked if she would like to get a master’s degree. He arranged her coursework, and she got a mas-ter’s in soil fertility. Th en she worked as a lab tech for 3 years while her husband fi nished his postdoctoral fellowship and they moved to Battelle Laboratories in the Tri-Cities of Washington and he has been on the staff for 25 years. Th ree years ago Mary decided that she wanted to be a nurse. She got her RN and now she works nights on a medical/surgical fl oor and loves it at age 52.
Barbara was born in 1960 in Boston. She graduated in nursing from the University of Minnesota and has a master’s degree in epi-demiology. She has worked in the Twin Cit-ies since then. She worked for 15 years as the director of the teenage pregnancy program in Hennepin County, Minneapolis, and last year took a new job as nurse manager of the Minneapolis School Health Nurses.
Jean was born in 1963. She studied criminal justice and women’s studies. When she graduated from college, the oppor-tunities were mainly being a parole offi cer or working in a jail, and she didn’t like that very much. She took a job as a counselor for Th e Bush Foundation, in which she managed teenagers who had problems that didn’t allow them to stay at home but weren’t serious enough for them to be incarcerated. She stayed there for a year and found out it was a very challenging job. Th en she en-rolled in law school. She is now a public defender for Hennepin County in Minneapolis and has been so for 20 years.
Roberts: Do you have any grandchildren?Kyle: We have fi ve (Figure 19). Roberts: How do you like being a granddaddy?Kyle: Fine. None of my grandchildren live in Rochester, so
we don’t see them on a daily basis. Th ree live in Washington and the oldest boy graduated from college 3 years ago with majors in chemistry and biology. Th e year prior to his graduation he obtained a summer undergraduate research fellowship here at the clinic. It’s a recruiting mechanism for our graduate school, and he spent the 3 months in a Mayo laboratory. I introduced him to a number of physicians and he made rounds on trans-plantation. I thought he might want to get an MD/PhD, but the medical part didn’t appeal to him. He decided to go to the University of Washington, where he is working on a doctorate in pharmacology. I didn’t want to exert any pressure on him to come to Mayo, but my wife was crushed because we really enjoyed having him with us during his fellowship. He is now in his third year and doing very well.
Roberts: How many professional trips do you go on a year?Kyle: Probably two or three a month. I’m on the board of
directors of the International Waldenström’s Macroglobuline-
mia Foundation. It is a board of 15 persons, and I am the only one who does not have Waldenström’s macroglobulinemia! It’s a phenomenal organization. Th ese people include a chemical engineer, a pharmacist, physicians, engineers, executives, and a retired administrator from the National Institutes of Health. Th ey are very able and talented. I am astounded by what they do. Th ose board meetings are four times a year.
I’m also on the board of directors of the International Myeloma Foundation. Th ey have three or four patient seminars each year, and I usually speak at two or three of their meet-ings. I’m also chairman of the foundation’s Scientifi c Advisory Board, which consists of over 70 physicians around the world who are interested in myeloma. Also, there is an amyloidosis support group, and I do a couple of lectures for them each year. I travel about 150,000 miles a year. I served as president of the International Society of Amyloidosis. My travels include four or fi ve trips annually, usually to Europe, South America, or Asia (Figure 20). I received an honorary doctorate from Palacky University in Olomouc, Czech Republic.
Roberts: Rochester, Minnesota, is not the easiest place to travel in and out of.
Kyle: Th e only nonstops are to Minneapolis, Detroit, and Chicago. I fl y with Northwest—now Delta—and go through Minneapolis or Detroit. I don’t use American Airlines going to Chicago for two reasons: weather can be bad in Chicago and if it is, O’Hare is very diffi cult to get through, and if you get stalled in O’Hare an overnight stay is required. In Min-neapolis, if the fl ight is stalled or canceled I am only 1½ hours from Rochester. I enjoy traveling and meeting people at these meetings.
Roberts: I was very impressed when you came to Baylor Uni-versity Medical Center; both of your talks were loaded with data. You didn’t give generalizations. Th ere are not too many investigators who at 82 years of age give fundamental data talks. You’ve spent the last 9 years essentially in research?
Figure 19. Charlene, Bob, siblings, children, and grandchildren at the International Myeloma Foundation
Lifetime Achievement Award Ceremony, 2003.

October 2010 415
Kyle: For 4 of those years I was still running the Special Protein Laboratory. Th e last 6 years I have been in this offi ce.
Roberts: You are working as hard now at 82 as you did at 42?Kyle: Not really because I don’t have the pressure of pa-
tients sitting in the waiting room. At that time everything was scheduled, and now I can leave when I need to. We only live a 10-minute walk from the offi ce (Figure 21). In fact, my wife has not driven since she was a teenager. She had a minor accident that frightened her so that she hasn’t driven since.
Roberts: What about vacation time? Do you take much time off ?
Kyle: Yes. We always take driving vacations. When the children were small we would go to a lake resort in northern Minnesota for a week every year. Often we would go to North Dakota where my family lived and stop at other sightseeing places along the way. Over the last 30 years we have done a lot of driving trips. Each summer we drive 5000 to 9000 miles (about 3 weeks). John, being a teacher and having the summer off , does all the driving and all the planning. He has a clipboard with a sheet for each day, and each sheet contains the mileage from town to town and each of the sites we are going to see. He would pick out mines and craters and all of those physical abnormalities. I’m interested in history and geography. We’ve been to Yellowstone National Park 8 to 10 times and the Grand Canyon—North and South Rim—5 to 6 times; we’ve even climbed Mt. Lassen in California. We do these trips every sum-mer. I also go to Europe 4 or 5 times a year and I always travel or do something extra. Charlene is not nearly as much a traveler as I. If she’s been somewhere once or twice, that’s enough.
Roberts: Do you read a lot of nonmedical things?Kyle: Not too much. I’m busy writing. I read enough medi-
cal history to do the vignettes. I’ve read all of the Sherlock Holmes books. I have visited a number of the sites of the sto-
ries, including the Moors in England where the Hound of the Baskervilles took place as well as the Falls of Reichenbach in Meiringen, Switzerland, where Holmes “fell to his death” while fi ghting with the evil Professor Moriarty.
Roberts: Do you read fast?Kyle: Yes. I took a course to read even faster. But I don’t
have enough time to read a lot of nonfi ction or fi ction.Roberts: Are you going to work forever?Kyle: I don’t know that. I’ll work as long as my colleagues
tolerate me and as long as I feel good. Over at Charter House, where we live, there are a number of my senior colleagues who are retired, and they just putter around every day. I just couldn’t tolerate that sort of thing at this time in life.
Roberts: Do you get as much thrill out of a publication now at age 82 as you did at 42?
Kyle: Not as much enjoyment, but when I hit Th e New England Journal of Medicine I am very happy. I’ve had about 20 articles there, and those are my prime papers.
Roberts: Is there anything else that you would like to talk about that we haven’t discussed?
Kyle: Th e best thing is that I’ve been blessed by the people here. My clinical secretary has been with me for 33 years. When I was active I had two full-time secretaries—one for clinical and one for the laboratory. Th e laboratory secretary was the one who typed my papers and grants. My clinical secretary is still with me after 33 years while my laboratory secretary retired after 26 years.
In 1974, I started a program project entitled “Studies in Monoclonal Gammopathies,” which was funded by the Na-tional Institutes of Health. Th at is still continuing but I am not the principal investigator any longer. I turned that over to my colleagues about 10 years ago, but I am still a coinvestigator.
Roberts: How many are on the faculty at Mayo Clinic?
Figure 21. Charlene and Bob Kyle, 2010.
Figure 20. Travels: (a) at the 5th Symposium on Amyloidosis, Hakone, Japan, with Morie Gertz, Alex Tong,
and Marvin Stone, 1987; (b) at the Torch Lighting Ceremony, Waldenstrom’s Macroglobulinemia Workshop,
Athens, Greece, 2002; (c) receiving an honorary doctorate in medicine from Palacky University, Olomouc,
Czech Republic, 2000; (d) with son, John, on Harbor Bridge, Sydney, Australia, 2005.
a b
c d
Robert Arthur Kyle, MD: a conversation with the editor
Baylor University Medical Center Proceedings Volume 23, Number 4416
Kyle: About 1500 permanent staff . Roberts: How many of those are age 82 or more?Kyle: Th ree of us: Peter Dyck, Dick Emslander, and I are
all 82. It’s quite unusual for a person to have the opportunity of staying on this long at Mayo Clinic. Generally speaking, when a consultant retires at Mayo Clinic he or she is done. Today, when you retire you can become a “supplemental consultant”; that’s what I’m called.
Roberts: Do you have to retire at a certain age?Kyle: No. It’s a federal law. One can become a supplemental
consultant and continue to see patients on a regular basis. I’m fortunate that I don’t see patients any longer and yet I have an offi ce with a secretary. It used to be that at age 65 one was completely retired and only a few people were able to stay on for an extra 1 to 2 years. Th ere are some people who stay on 4 to 5 years but that is about it.
Roberts: Is there anything else you would like to talk about?Kyle: It’s wonderful to have the opportunity of interacting
with patients. Roberts: You still have that vigor and enthusiasm and desire to
learn and create and fi nd new things. Th at is what keeps you young!Kyle: I’m not nearly as smart as the young guys. Th ey talk
about statistics and molecular biology, but a lot of it is beyond me.
Roberts: I’m not so sure about that. I appreciate your time with me.
Kyle: It was fun talking about all this. Th ank you!
RAK’S BEST PUBLICATIONS AS SELECTED BY HIM1. Kyle RA, Kiely JM, Stickney JM. Acquired hemolytic anemia in chronic
lymphocytic leukemia and the lymphomas: survival and response to ther-apy in twenty-seven cases. AMA Arch Intern Med 1959;104(1):61–67.
2. Kyle RA, Bayrd ED, McKenzie BF, Heck FJ. Diagnostic criteria for elec-trophoretic patterns of serum and urinary proteins in multiple myeloma. Study of one hundred and sixty-fi ve multiple myeloma patients and of seventy-seven nonmyeloma patients with similar electrophoretic patterns. JAMA 1960;174:245–251.
3. Kyle RA, Bayrd ED. “Primary” systemic amyloidosis and myeloma. Discussion of relationship and review of 81 cases. Arch Intern Med 1961;107:344–353.
4. Mills SD, Kyle RA, Hallenbeck GA, Pease GL, Cree IC. Bone-marrow transplant in an identical twin. JAMA 1964;188:1037–1040.
5. Kyle RA, Pease GL. Hematologic aspects of arsenic intoxication. N Engl J Med 1965;273:18–23.
6. Kyle RA, Bayrd ED. “Benign” monoclonal gammopathy: A potentially malignant condition? Am J Med 1966;40:426–430.
7. Kyle RA, Kottke BA, Schirger A. Orthostatic hypotension as a clue to primary systemic amyloidosis. Circulation 1966;34(5):883–888.
8. Ellison RR, Holland JF, Weil M, Jacquillat C, Boiron M, Bernard J, Sawitsky A, Rosner F, Gussoff B, Silver RT, Karanas A, Cuttner J, Spurr CL, Hayes DM, Blom J, Leone LA, Haurani F, Kyle R, Hutchison JL, Forcier RJ, Moon JH. Arabinosyl cytosine: a useful agent in the treatment of acute leukemia in adults. Blood 1968;32(4):507–523.
9. Kyle RA, Linman JW. Chronic idiopathic neutropenia. A newly recognized entity? N Engl J Med 1968;279(19):1015–1019.
10. Kyle RA, Nobrega FT, Kurland LT. Multiple myeloma in Olmsted County, Minnesota, 1945–1964. Blood 1969;33(5):739–745.
11. Kyle RA, Shampo MA. Medicine and Stamps. Chicago: American Medical Association, 1970.
12. Kyle RA, Bieger RC, Gleich GJ. Diagnosis of syndromes associated with hyperglobulinemia. Med Clin North Am 1970;54(4):917–938.
13. Kyle RA, Herber L, Evatt BL, Heath CW Jr. Multiple myeloma. A com-munity cluster. JAMA 1970;213(8):1339–1341.
14. Kyle RA, Pierre RV, Bayrd ED. Multiple myeloma and acute myelomono-cytic leukemia. N Engl J Med 1970;283(21):1121–1125.
15. Kyle RA, Gleich GJ, Bayrid ED, Vaughan JH. Benign hypergammaglobu-linemic purpura of Waldenström. Medicine (Baltimore) 1971;50(2):113–123.
16. Kyle RA, Heath CW Jr, Carbone P. Multiple myeloma in spouses. Arch Intern Med 1971;127(5):944–946.
17. Kyle RA, Finkelstein S, Elveback LR, Kurland LT. Incidence of mono-clonal proteins in a Minnesota community with a cluster of multiple myeloma. Blood 1972;40(5):719–724.
18. Kyle RA. Multiple myeloma (plasmacytic myeloma). In Conn FH, ed. Current Th erapy. Philadelphia: W. B. Saunders, 1973:288–290.
19. Kyle RA, Maldonado JE, Bayrd ED. Idiopathic Bence Jones proteinuria—a distinct entity? Am J Med 1973;55(2):222–226.
20. Kyle RA, Maldonado JE, Bayrd ED. Plasma cell leukemia. Report on 17 cases. Arch Intern Med 1974;133(5):813–818.
21. Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clin Proc 1975;50(1):29–40.
22. Kyle RA, Bayrd ED. Amyloidosis: review of 236 cases. Medicine (Balti-more) 1975;54(4):271–299.
23. Kyle RA, Jowsey J, Kelly PJ, Taves DR. Multiple-myeloma bone disease. Th e comparative eff ect of sodium fl uoride and calcium carbonate or pla-cebo. N Engl J Med 1975;293(26):1334–1338.
24. Kyle RA, Bayrd ED. Th e Monoclonal Gammopathies: Multiple Myeloma and Related Plasma-Cell Disorders. Springfi eld, IL: C. C. Th omas, 1976.
25. Kyle RA. Monoclonal gammopathy of undetermined signifi cance. Natural history in 241 cases. Am J Med 1978;64(5):814–826.
26. Kyle RA, Greipp PR. Primary systemic amyloidosis: comparison of mel-phalan and prednisone versus placebo. Blood 1978;52(4):818–827.
27. Kyle RA. Stamps help lick blood shortages around the globe. AABB Review 1979(Spring);2:4–8.
28. Kyle RA. Multiple myeloma. In Conn HF, ed. Current Th erapy. Th e Blood and Spleen. Philadelphia: W. B. Saunders, 1979:310–313.
29. Kyle RA. Blood transfusion and stamps. Forum Med 1979;2(11):730–732.30. Kyle RA. Natural history of chronic idiopathic neutropenia. N Engl J Med
1980;302(16):908–909.31. Kyle RA, Greipp PR. Smoldering multiple myeloma. N Engl J Med
1980;302(24):1347–1349.32. Kyle RA, Shampo MA. Medicine and Stamps, vol. 2. Huntington, NY:
Krieger, 1980.33. Kyle RA, Greipp PR, Banks PM. Th e diverse picture of gamma heavy-
chain disease. Report of seven cases and review of literature. Mayo Clin Proc 1981;56(7):439–451.
34. Kyle RA, Robinson RA, Katzmann JA. Th e clinical aspects of biclonal gammopathies. Review of 57 cases. Am J Med 1981;71(6):999–1008.
35. Kyle RA, Greipp PR. “Idiopathic” Bence Jones proteinuria: long-term follow-up in seven patients. N Engl J Med 1982;306(10):564–567.
36. Kyle RA. Second malignancies associated with chemotherapeutic agents. Semin Oncol 1982;9(1):131–142.
37. Kyle RA. Th e laboratory evaluation of immunosecretory states. Clin Lab Ann 1982;1:383–434.
38. Kyle RA, Gleich GJ. IgG subclasses in monoclonal gammopathy of un-determined signifi cance. J Lab Clin Med 1982;100(5):806–814.
39. Kyle RA. Long-term survival in multiple myeloma. N Engl J Med 1983;308(6):314–316.
40. Kyle RA, Greipp PR. Multiple myeloma. Houses and spouses. Cancer 1983;51(4):735–739.
41. Kyle RA. ‘Benign’ monoclonal gammopathy. A misnomer? JAMA 1984;251(14):1849–1854. Also translated and published in Italian and French JAMA editions.
42. Kyle RA, Schreiman JS, McLeod RA, Beabout JW. Computed tomography in diagnosis and management of multiple myeloma and its variants. Arch Intern Med 1985;145(8):1451–1452.

October 2010 417
43. Dewald GW, Kyle RA, Hicks GA, Greipp PR. Th e clinical signifi cance of cytogenetic studies in 100 patients with multiple myeloma, plasma cell leukemia, or amyloidosis. Blood 1985;66(2):380–390.
44. Kyle RA, Garton JP. Th e spectrum of IgM monoclonal gammopathy in 430 cases. Mayo Clin Proc 1987;62(8):719–731.
45. Kyle RA. IgD multiple myeloma: a cure at 21 years. Am J Hematol 1988;29(1):41–43.
46. Frassica DA, Frassica FJ, Schray MF, Sim FH, Kyle RA. Solitary plasma-cytoma of bone: Mayo Clinic experience. Int J Radiat Oncol Biol Phys 1989;16(1):43–48.
47. Kyle RA, Gertz MA. Systemic amyloidosis. Crit Rev Oncol Hematol 1990;10(1):49–87.
48. Kyle RA, Gertz MA, Linke RP. Amyloid localized to tenosynovium at carpal tunnel release. Immunohistochemical identifi cation of amyloid type. Am J Clin Pathol 1992;97(2):250–253.
49. Kyle RA, Linos A, Beard CM, Linke RP, Gertz MA, O’Fallon WM, Kurland LT. Incidence and natural history of primary systemic amy-loidosis in Olmsted County, Minnesota, 1950 through 1989. Blood 1992;79(7):1817–1822.
50. Kyle RA. “Benign” monoclonal gammopathy—after 20 to 35 years of follow-up. Mayo Clin Proc 1993;68(1):26–36.
51. Kyle RA, Dyck PJ. Amyloidosis and neuropathy. In Dyck PJ, Th omas PK, Griffi n JW, Low PA, Poduslo JF, eds. Peripheral Neuropathy, 3rd ed. Philadelphia: W. B. Saunders, 1993:1294–1309.
52. Kyle RA, Beard CM, O’Fallon WM, Kurland LT. Incidence of multiple myeloma in Olmsted County, Minnesota: 1978 through 1990, with a review of the trend since 1945. J Clin Oncol 1994;12(8):1577–1583.
53. Bladé J, Lust JA, Kyle RA. Immunoglobulin D multiple myeloma: pre-senting features, response to therapy, and survival in a series of 53 cases. J Clin Oncol 1994;12(11):2398–2404.
54. Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol 1995;32(1):45–59.
55. Kyle RA, Gertz MA, Greipp PR, Witzig TE, Lust JA, Lacy MQ, Th erneau TM. A trial of three regimens for primary amyloidosis: colchicine alone, melphalan and prednisone, and melphalan, prednisone, and colchicine. N Engl J Med 1997;336(17):1202–1207.
56. Kyle RA, Gertz MA, Greipp PR, Witzig TE, Lust JA, Lacy MQ, Th erneau TM. Long-term survival (10 years or more) in 30 patients with primary amyloidosis. Blood 1999;93(3):1062–1066.
57. Kyle RA. Sequence of testing for monoclonal gammopathies. Arch Pathol Lab Med 1999;123(2):114–118.
58. Kyle RA, Greipp PR, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Th erneau TM. Waldenström’s macroglobulinaemia: a prospective study comparing daily with intermittent oral chlorambucil. Br J Haematol 2000;108(4):737–742.
59. Kyle RA. Multiple myeloma: an odyssey of discovery. Br J Haematol 2000;111(4):1035–1044.
60. Kyle RA. Amyloidosis: a convoluted story. Br J Haematol 2001;114(3):529–538.
61. Kyle RA. Henry Bence Jones—physician, chemist, scientist and biogra-pher: a man for all seasons. Br J Haematol 2001;115(1):13–18.
62. Kyle RA, Th erneau TM, Rajkumar SV, Off ord JR, Larson DR, Plevak MF, Melton LJ 3rd. A long-term study of prognosis in monoclonal gammopa-thy of undetermined signifi cance. N Engl J Med 2002;346(8):564–569.
63. Kyle RA. Multiple myeloma. In Dollinger M, Rosenbaum EH, Tempero M, Mulvihill SJ, eds. Everyone’s Guide to Cancer Th erapy, 4th ed. Kansas City: Andrews McMeel Publishing, 2002:676–684.
64. Kyle RA, Gertz MA, Lacy MQ, Dispenzieri A. Localized AL amyloidosis of the colon: an unrecognized entity. Amyloid 2003;10(1):36–41.
65. Kyle RA, Treon SP, Alexanian R, Barlogie B, Björkholm M, Dhodapkar M, Lister TA, Merlini G, Morel P, Stone M, Branagan AR, Leblond V. Prognostic markers and criteria to initiate therapy in Waldenstrom’s macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom’s Macroglobulinemia. Semin Oncol 2003;30(2):116–120.
66. Dispenzieri A, Kyle RA, Gertz MA, Th erneau TM, Miller WL, Chan-drasekaran K, McConnell JP, Burritt MF, Jaff e AS. Survival in patients
with primary systemic amyloidosis and raised serum cardiac troponins. Lancet 2003;361(9371):1787–1789.
67. Kyle RA, Child JA, et al. Criteria for the classifi cation of monoclonal gam-mopathies, multiple myeloma and related disorders: a report of the Interna-tional Myeloma Working Group. Br J Haematol 2003;121(5):749–757.
68. Wiernik PH, Goldman JM, Dutcher JP, Kyle RA, eds. Neoplastic Diseases of the Blood, 4th ed. Cambridge, UK: Cambridge University Press, 2003.
69. Kyle RA, Rajkumar SV. Monoclonal gammopathies of undetermined signifi cance: a review. Immunol Rev 2003;194:112–139.
70. Kyle RA, Th erneau TM, Rajkumar SV, Remstein ED, Off ord JR, Larson DR, Plevak MF, Melton LJ 3rd. Long-term follow-up of IgM monoclonal gammopathy of undetermined signifi cance. Blood 2003;102(10):3759–3564.
71. Durie BG, Kyle RA, Belch A, Bensinger W, Blade J, Boccadoro M, Child JA, Comenzo R, Djulbegovic B, Fantl D, Gahrton G, Harousseau JL, Hungria V, Joshua D, Ludwig H, Mehta J, Morales AR, Morgan G, Nouel A, Oken M, Powles R, Roodman D, San Miguel J, Shimizu K, Singhal S, Sirohi B, Sonneveld P, Tricot G, Van Ness B; Scientifi c Advisors of the International Myeloma Foundation. Myeloma management guidelines: a consensus report from the Scientifi c Advisors of the International My-eloma Foundation. Hematol J 2003;4(6):379–398.
72. Malpas JS, Bergsagel DE, Kyle RA, Anderson KC, eds. Myeloma: Biology and Management, 3rd ed. Philadelphia: Saunders, 2004.
73. Grateau G., Kyle RA, Skinner M, eds. Amyloid and Amyloidosis. Boca Raton, FL: CRC Press, 2004.
74. Kyle RA, Th erneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ 3rd. Long-term follow-up of 241 patients with monoclonal gammopathy of undetermined signifi cance: the original Mayo Clinic series 25 years later. Mayo Clin Proc 2004;79(7):859–866.
75. Kyle RA, Rajkumar SV. Multiple myeloma. N Engl J Med 2004;351(18):1860–1873.
76. Kyle RA, Th erneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ 3rd. Incidence of multiple myeloma in Olmsted County, Minnesota: trend over 6 decades. Cancer 2004;101(11):2667–2674.
77. Rajkumar SV, Kyle RA, Th erneau TM, Clark RJ, Bradwell AR, Melton LJ 3rd, Larson DR, Plevak MF, Katzmann JA. Presence of monoclonal free light chains in the serum predicts risk of progression in monoclonal gammopathy of undetermined signifi cance. Br J Haematol 2004;127(3):308–310.
78. Shampo M, Kyle RA, eds. Medicine and Stamps, vol. 3. Montvale, NJ: Dowden Health Media, Inc., 2004.
79. Melton LJ 3rd, Kyle RA, Achenbach SJ, Oberg AL, Rajkumar SV. Fracture risk with multiple myeloma: a population-based study. J Bone Miner Res 2005;20(3):487–493.
80. Dewald GW, Th erneau T, Larson D, Lee YK, Fink S, Smoley S, Pater-noster S, Adeyinka A, Ketterling R, Van Dyke DL, Fonseca R, Kyle R. Relationship of patient survival and chromosome anomalies detected in metaphase and/or interphase cells at diagnosis of myeloma. Blood 2005;106(10):3553–3558.
81. Rajkumar SV, Kyle RA. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc 2005;80(10):1371–1382.
82. Barlogie B, Kyle RA, Anderson KC, Greipp PR, Lazarus HM, Hurd DD, McCoy J, Moore DF Jr, Dakhil SR, Lanier KS, Chapman RA, Cromer JN, Salmon SE, Durie B, Crowley JC. Standard chemotherapy compared with high-dose chemoradiotherapy for multiple myeloma: fi nal results of phase III US Intergroup Trial S9321. J Clin Oncol 2006;24(6):929–936.
83. Kyle RA, Rajkumar SV. Multiple myeloma. In Rakel RE, Bope ET, eds. Conn’s Current Th erapy 2006. Philadelphia: Saunders Elsevier, 2006:568–574.
84. Kyle RA, Leong T, Li S, Oken MM, Kay NE, Van Ness B, Greipp PR. Complete response in multiple myeloma: clinical trial E9486, an Eastern Cooperative Oncology Group study not involving stem cell transplanta-tion. Cancer 2006;106(9):1958–1966.
85. Kyle RA, Th erneau TM, Rajkumar SV, Larson DR, Plevak MF, Of-ford JR, Dispenzieri A, Katzmann JA, Melton LJ 3rd. Prevalence of monoclonal gammopathy of undetermined signifi cance. N Engl J Med 2006;354(13):1362–1369.
Robert Arthur Kyle, MD: a conversation with the editor

Baylor University Medical Center Proceedings Volume 23, Number 4418
86. Dingli D, Kyle RA, Rajkumar SV, Nowakowski GS, Larson DR, Bida JP, Gertz MA, Th erneau TM, Melton LJ 3rd, Dispenzieri A, Katzmann JA. Immunoglobulin free light chains and solitary plasmacytoma of bone. Blood 2006;108(6):1979–1983.
87. Zhu X, Wentworth P Jr, Kyle RA, Lerner RA, Wilson IA. Cofactor-containing antibodies: crystal structure of the original yellow antibody. Proc Natl Acad Sci U S A 2006;103(10):3581–3585.
88. Kyle RA, Rajkumar SV. Monoclonal gammopathy of undetermined signifi cance. Br J Haematol 2006;134(6):573–589.
89. Kyle RA, Rajkumar SV. Multiple myeloma. In Rakel RE, Bope ET, eds. Conn’s Current Th erapy 2007. Philadelphia: Saunders Elsevier, 2007:546–551.
90. Kyle RA, Remstein ED, Th erneau TM, Dispenzieri A, Kurtin PJ, Hodnefi eld JM, Larson DR, Plevak MF, Jelinek DF, Fonseca R, Melton LJ 3rd, Rajkumar SV. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med 2007;356(25):2582–2590.
91. Kyle RA, Yee GC, Somerfi eld MR, Flynn PJ, Halabi S, Jagannath S, Orlowski RZ, Roodman DG, Twilde P, Anderson K; American Society of Clinical Oncology. American Society of Clinical Oncology 2007 clinical practice guideline update on the role of bisphosphonates in multiple myeloma. J Clin Oncol 2007;25(17):2464–2472.
92. Kyle RA, Rajkumar SV. Epidemiology of the plasma-cell disorders. Best Pract Res Clin Haematol 2007;20(4):637–664.
93. Kyle RA, Dispenzieri A. Monoclonal gammopathies. In Rich RR, Fleisher TA, Shearer WT, Schroeder HW Jr, Frew AJ, Weyand CM, eds. Clinical Immunology: Principles and Practice, 3rd ed. Philadelphia: Mosby Elsevier, 2008:1167–1180.
94. Kyle RA, Rajkumar SV. ASH 50th anniversary review: Multiple my-eloma. Blood 2008;111(6):2962–2972.
95. Kyle RA, Rajkumar SV. Multiple myeloma. In Ko A, Dollinger M, Rosenbaum E, eds. Everyone’s Guide to Cancer Th erapy: How Cancer is Diagnosed, Treated, and Managed Day to Day, 5th ed. Kansas City: Andrews McMeel Publishing, 2008:740–747.
96. Anderson KC, Kyle RA, Rajkumar SV, Stewart AK, Weber D, Richard-son P; ASH/FDA Panel on Clinical Endpoints in Multiple Myeloma. Clinically relevant end points and new drug approvals for myeloma. Leukemia 2008;22(2):231–239.
97. McKenna RW, Kyle RA, Kuehl WM, Grogan TM, Harris NL, Coupland RW. Plasma cell neoplasms. In Swerdlow SH, Campo E, Harris NL, Jaff e ES, Pileri SA, Stein H, Th iele J, Vardiman JW, eds. WHO Classifi cation of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: International Agency for Research on Cancer, 2008:200–213.
98. Creach KM, Foote RL, Neben-Wittich MA, Kyle RA. Radiotherapy for extramedullary plasmacytoma of the head and neck. Int J Radiat Oncol Biol Phys 2009;73(3):789–794.
99. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratifi cation and response assessment of multiple myeloma. Leukemia 2009;23(1):3–9.
100. Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, Palumbo A, Jagannath S, Blade J, Lonial S, Dimopoulos M, Comenzo R, Einsele H, Barlogie B, Anderson K, Gertz M, Harousseau JL, Attal M, Tosi P, Sonneveld P, Boccadoro M, Morgan G, Richardson P, Sezer O, Mateos MV, Cavo M, Joshua D, Turesson I, Chen W, Shimizu K, Powles R, Rajkumar SV, Durie BG; International Myeloma Working Group. International Myeloma Working Group guidelines for serum-free
light chain analysis in multiple myeloma and related disorders. Leukemia 2009;23(2):215–224.
101. Bida JP, Kyle RA, Th erneau TM, Melton LJ 3rd, Plevak MF, Larson DR, Dispenzieri A, Katzmann JA, Rajkumar SV. Disease associations with monoclonal gammopathy of undetermined signifi cance: a popula-tion-based study of 17,398 patients. Mayo Clin Proc 2009;84(8):685–693.
102. Landgren O, Kyle RA, Hoppin JA, Beane Freeman LE, Cerhan JR, Katzmann JA, Rajkumar SV, Alavanja MC. Pesticide exposure and risk of monoclonal gammopathy of undetermined signifi cance in the Agri-cultural Health Study. Blood 2009;113(25):6386–6391.
103. Kyle RA, Benson J, Larson D, Th erneau T, Dispenzieri A, Melton LJ 3rd, Rajkumar SV. IgM monoclonal gammopathy of undetermined signifi cance and smoldering Waldenström’s macroglobulinemia. Clin Lymphoma Myeloma 2009;9(1):17–18.
104. Vachon CM, Kyle RA, Th erneau TM, Foreman BJ, Larson DR, Colby CL, Phelps TK, Dispenzieri A, Kumar SK, Katzmann JA, Rajkumar SV. Increased risk of monoclonal gammopathy in fi rst-degree relatives of patients with multiple myeloma or monoclonal gammopathy of un-determined signifi cance. Blood 2009;114(4):785–790.
105. Landgren O, Kyle RA, Pfeiff er RM, Katzmann JA, Caporaso NE, Hayes RB, Dispenzieri A, Kumar S, Clark RJ, Baris D, Hoover R, Rajkumar SV. Monoclonal gammopathy of undetermined signifi cance (MGUS) consistently precedes multiple myeloma: a prospective study. Blood 2009;113(22):5412–5417.
106. Kyle RA, Jacobus S, Friedenberg WR, Slabber CF, Rajkumar SV, Greipp PR. Th e treatment of multiple myeloma using vincristine, carmustine, melphalan, cyclophosphamide, and prednisone (VBMCP) alternating with high-dose cyclophosphamide and �2� interferon versus VBMCP: results of a phase III Eastern Cooperative Oncology Group Study E5A93. Cancer 2009;115(10):2155–2164.
107. Kyle RA, Rajkumar SV. Treatment of multiple myeloma: a comprehen-sive review. Clin Lymphoma Myeloma 2009;9(4):278–288.
108. Kyle RA. Monoclonal gammopathies of undetermined signifi cance and smoldering multiple myeloma. In Greer JP, Foerster J, Rodgers GM, Paraskevas F, Glader B, Arber DA, Means RT Jr, eds. Wintrobe’s Clini-cal Hematology, 12th ed., vol. 2. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2009:2352–2371.
109. Rajkumar SV, Kyle RA. Treatment of newly diagnosed multiple myeloma. In Rajkumar SV, Kyle RA, eds. Treatment of Multiple Myeloma and Re-lated Disorders. New York: Cambridge University Press, 2009:26–36.
110. Kyle RA, Durie BG, Rajkumar SV, Landgren O, Blade J, Merlini G, Kröger N, Einsele H, Vesole DH, Dimopoulos M, San Miguel J, Avet-Loiseau H, Hajek R, Chen WM, Anderson KC, Ludwig H, Sonneveld P, Pavlovsky S, Palumbo A, Richardson PG, Barlogie B, Greipp P, Vescio R, Turesson I, Westin J, Boccadoro M; Interna-tional Myeloma Working Group. Monoclonal gammopathy of un-determined signifi cance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management. Leuke-mia 2010;24(6):1121–1127.
111. Dispenzieri A, Katzmann JA, Kyle RA, Larson DR, Melton LJ 3rd, Colby CL, Th erneau TM, Clark R, Kumar SK, Bradwell A, Fonseca R, Jelinek DF, Rajkumar SV. Prevalence and risk of progression of light-chain monoclonal gammopathy of undetermined signifi cance: a retrospective population-based cohort study. Lancet 2010;375(9727):1721–1728.