risks, benefits and current management strategies of ... · meta-analysis 18,686 dm patients...
TRANSCRIPT
Risks, Benefits and Current Management Strategies of Statin
Therapy
Katherine Gambino, CRNP Erin Henry, CRNP
Teri Miller, CRNP
Objectives
• Participant will be able to verbalize the latest guidelines for statin therapy
• Participant will be able to state the benefits of statins in terms of reducing cardiovascular morbidity and mortality
• Participant will be able to state the adverse effects/intolerances related to statin use
• Participant will be able to describe the current practice patterns regarding the use of statin therapy in the Cleveland Clinic Preventive Cardiology.


What are statins?
• Statins inhibit the HMG-CoA reductase enzyme therefore reducing the production of cholesterol in the liver.
• Metabolized in the liver
• Impact all components of a lipid panel (TC, TG, HDL, LDL) but mostly the LDL.
• Reduces LDL by 25-63%
FDA Indications • Labeled indications:
-Prevention of cardiovascular disease -Treatment of dyslipidemia -Treatment of heterozygous familial hypercholesterolemia.
• Primary prevention: Lipid reduction before disease occurs
• Secondary prevention: After the development of disease
What are the statins?
• Rosuvastatin (Crestor) – high potency
• Atorvastatin (Lipitor) – high potency
• Simvastatin (Zocor)
• Pravastatin (Pravachol)
• Lovastatin (Mevacor)
• Pitavastatin (Livalo)
• Fluvastatin (Lescol XL)
Trivia question!!
• Trivia question
• What was the first statin, and when was it FDA approved for use?

• Boring
• Award busies
Primary Prevention Trials
• EPIDEMIOLOGIC STUDIES
• WOSCOPS Pravastatin 40mg reduced non-fatal MI/CHD mortality in men with LDLs >155.
• AFCAPS/TEXCAPS Lovastatin 20-40mg reduced incidence 1st major CVE in low risk
male/females, average LDL 150s with lower HDLs.
• ASCOT LAA Atorvastatin 10mg reduced MI/ total CVE/Stoke in htn patients or those with 3+ risk factors.
• JUPITOR 15,000 patients multicenter trial, rosuvastatin 20mg in those with LDL<130 and CRP
>2.0 showed marked reduction 1st CVE : MI, CVA, need for CABG PTCA, all cause mortality. Those taking statin compared with placebo had 54% lower chance MI, 48% CVA, 46% PTCA/CABG/20% dying any cause. Stopped early. Normal LDL, inc CRP benefit.
• METEOR Rosuvastatin in low risk groups comparing CIMT; stat sign diff CIMT and LDL.
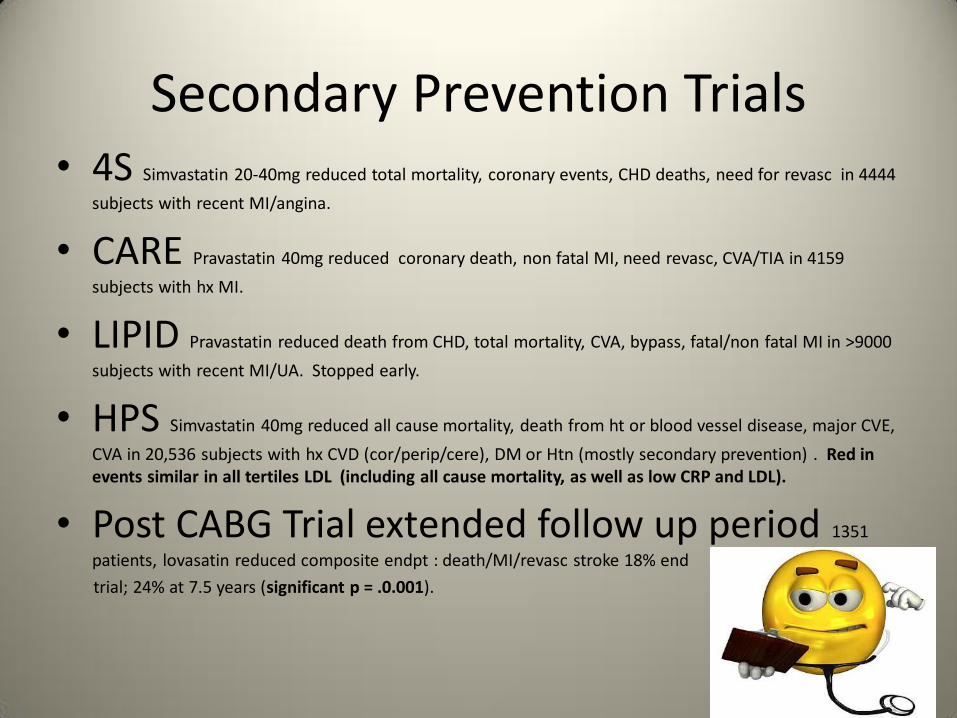
Secondary Prevention Trials • 4S Simvastatin 20-40mg reduced total mortality, coronary events, CHD deaths, need for revasc in 4444
subjects with recent MI/angina.
• CARE Pravastatin 40mg reduced coronary death, non fatal MI, need revasc, CVA/TIA in 4159
subjects with hx MI.
• LIPID Pravastatin reduced death from CHD, total mortality, CVA, bypass, fatal/non fatal MI in >9000
subjects with recent MI/UA. Stopped early.
• HPS Simvastatin 40mg reduced all cause mortality, death from ht or blood vessel disease, major CVE,
CVA in 20,536 subjects with hx CVD (cor/perip/cere), DM or Htn (mostly secondary prevention) . Red in events similar in all tertiles LDL (including all cause mortality, as well as low CRP and LDL).
• Post CABG Trial extended follow up period 1351
patients, lovasatin reduced composite endpt : death/MI/revasc stroke 18% end
trial; 24% at 7.5 years (significant p = .0.001).
Regression Trials Statins
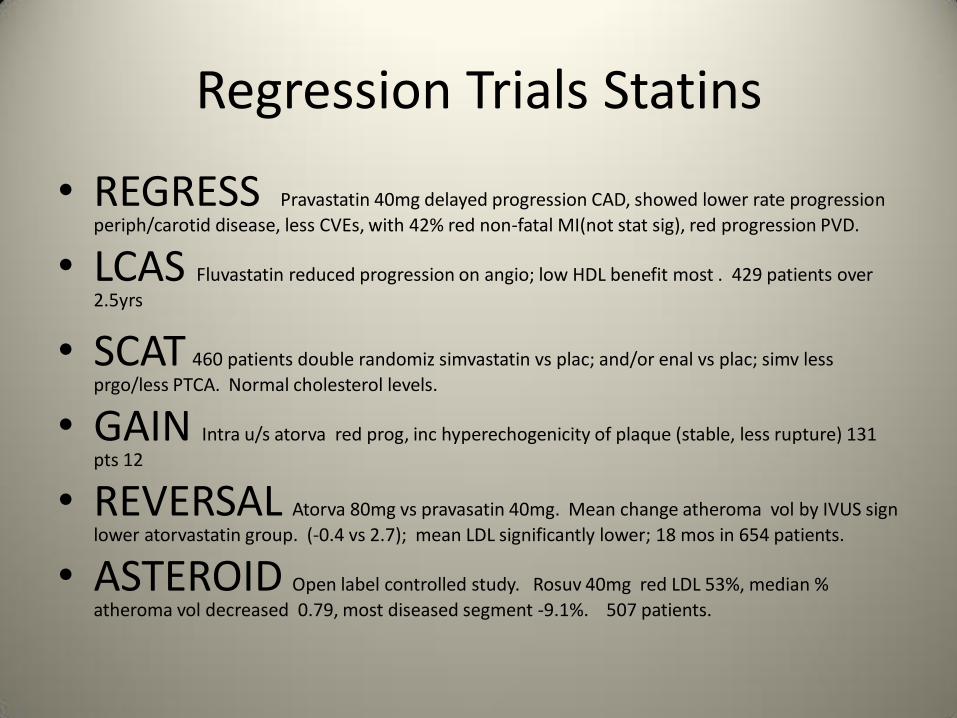
• REGRESS Pravastatin 40mg delayed progression CAD, showed lower rate progression
periph/carotid disease, less CVEs, with 42% red non-fatal MI(not stat sig), red progression PVD.
• LCAS Fluvastatin reduced progression on angio; low HDL benefit most . 429 patients over
2.5yrs
• SCAT 460 patients double randomiz simvastatin vs plac; and/or enal vs plac; simv less
prgo/less PTCA. Normal cholesterol levels.
• GAIN Intra u/s atorva red prog, inc hyperechogenicity of plaque (stable, less rupture) 131
pts 12
• REVERSAL Atorva 80mg vs pravasatin 40mg. Mean change atheroma vol by IVUS sign
lower atorvastatin group. (-0.4 vs 2.7); mean LDL significantly lower; 18 mos in 654 patients.
• ASTEROID Open label controlled study. Rosuv 40mg red LDL 53%, median %
atheroma vol decreased 0.79, most diseased segment -9.1%. 507 patients.
Statins and usCRP
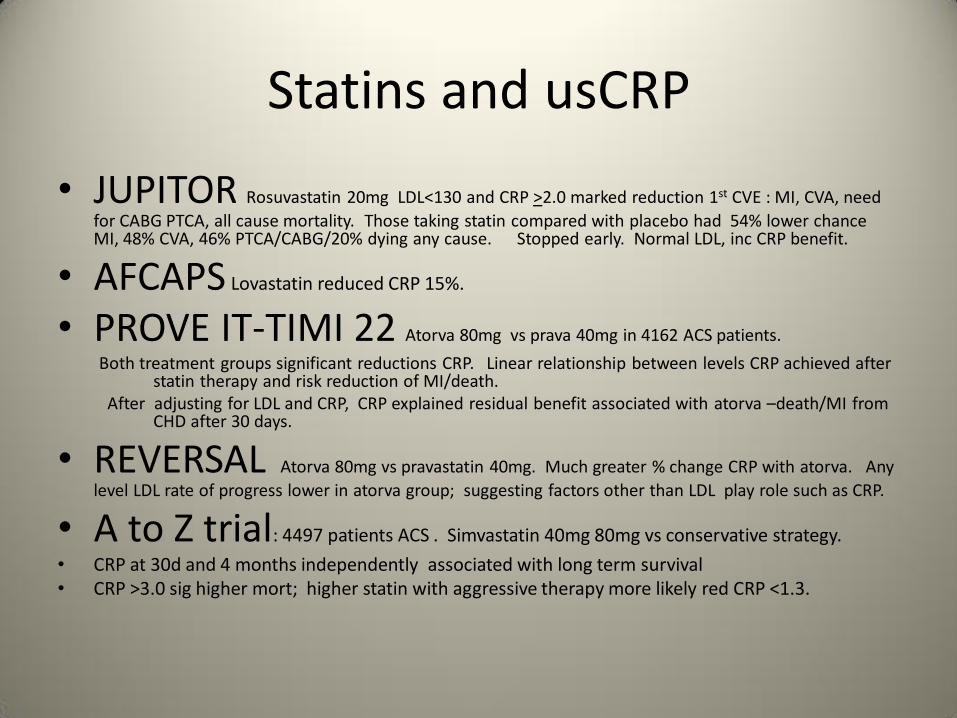
• JUPITOR Rosuvastatin 20mg LDL<130 and CRP >2.0 marked reduction 1st CVE : MI, CVA, need
for CABG PTCA, all cause mortality. Those taking statin compared with placebo had 54% lower chance MI, 48% CVA, 46% PTCA/CABG/20% dying any cause. Stopped early. Normal LDL, inc CRP benefit.
• AFCAPS Lovastatin reduced CRP 15%.
• PROVE IT-TIMI 22 Atorva 80mg vs prava 40mg in 4162 ACS patients.
Both treatment groups significant reductions CRP. Linear relationship between levels CRP achieved after statin therapy and risk reduction of MI/death. After adjusting for LDL and CRP, CRP explained residual benefit associated with atorva –death/MI from CHD after 30 days.
• REVERSAL Atorva 80mg vs pravastatin 40mg. Much greater % change CRP with atorva. Any
level LDL rate of progress lower in atorva group; suggesting factors other than LDL play role such as CRP.
• A to Z trial: 4497 patients ACS . Simvastatin 40mg 80mg vs conservative strategy.
• CRP at 30d and 4 months independently associated with long term survival • CRP >3.0 sig higher mort; higher statin with aggressive therapy more likely red CRP <1.3.
Lower LDLs the Better Trial Secondary Prevention
• TNT 10,000 patients atorva 10mg vs 80mg.
LDLs < 100 vs 75; significant reduction in primary endpoint MCVEs with aggressive targets for LDL.
• PROVE-IT TIMI 22 prava 40mg vs atorava 80g in 4182 patients ACS
LDLs <100 to LDLs <70 . Significant reduction primary endpt with HR 0.84 in aggressive therapy group. Primary endpoint death/MI/UA/revasc/CVA.
• REVERSAL Atorva 80mg vs pravastatin 40mg
Progression atheroma IVUS correlated with reduction LDL; each 10% red LDL correlated with 1% red in change of atheoma volume. Supports lower LDLs.

Statins and Diabetes
• Cholesterol Treatment Trialists Collaborators Meta-analysis 18,686 DM patients revealed significant reductions of the following with statins:
major vasc events 21%, CVA 21%, major coronary event 22%,coronary revasc 25%
• HPS 3982 subjects . Simvastatin in subgroup with DM with no CVD reduced MI/CVA 28%.
• CARDS Atorva 10mg reduced CVEs in DM with no CVD 37%.
2838 patients with additional risk (prot, sm, ret , htn), stopped early. LDL < > 120.
• MEGA 8214 Japanese men/post men females study diet vs pravastatin 10-20 in primary or
DM reduced 1st occurrence CHD HR 0.67 Asian benefits similar to american.
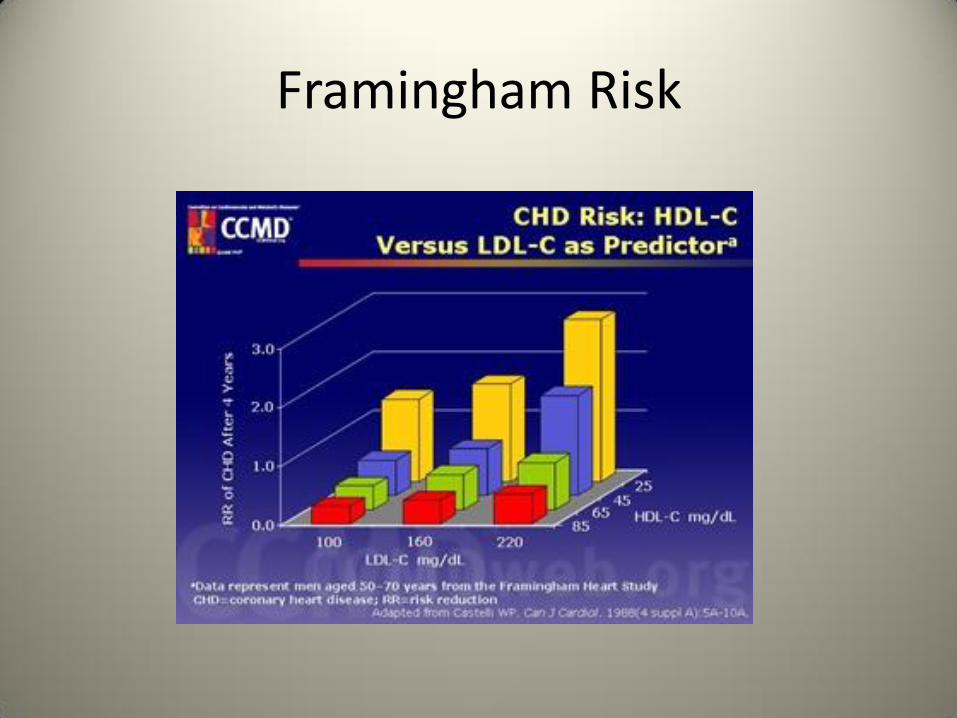
Framingham Risk
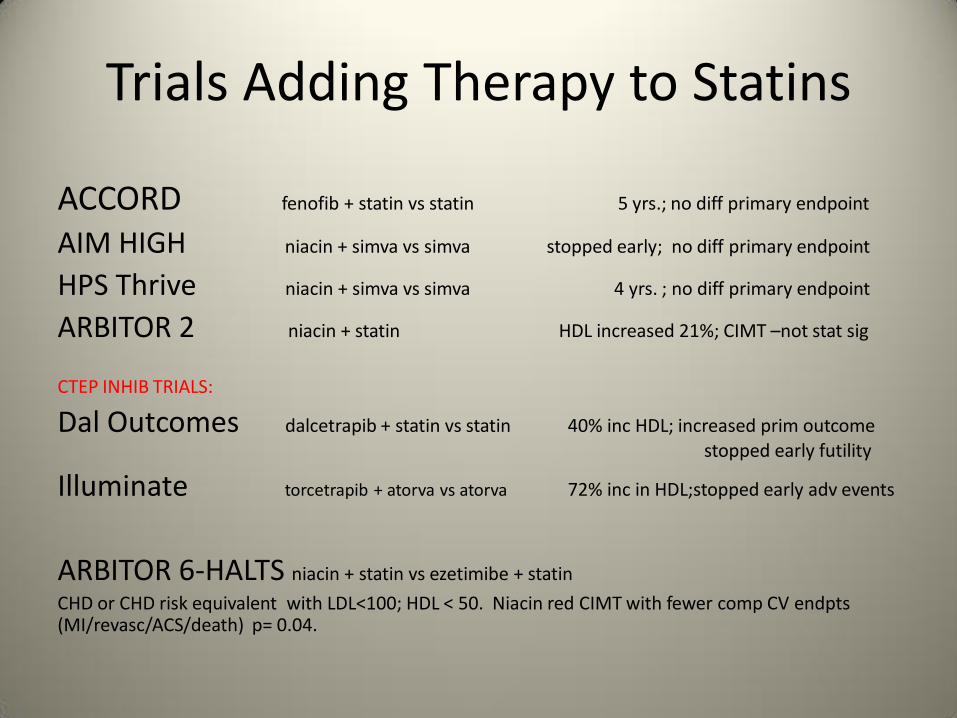
Trials Adding Therapy to Statins
ACCORD fenofib + statin vs statin 5 yrs.; no diff primary endpoint
AIM HIGH niacin + simva vs simva stopped early; no diff primary endpoint
HPS Thrive niacin + simva vs simva 4 yrs. ; no diff primary endpoint
ARBITOR 2 niacin + statin HDL increased 21%; CIMT –not stat sig
CTEP INHIB TRIALS:
Dal Outcomes dalcetrapib + statin vs statin 40% inc HDL; increased prim outcome stopped early futility
Illuminate torcetrapib + atorva vs atorva 72% inc in HDL;stopped early adv events
ARBITOR 6-HALTS niacin + statin vs ezetimibe + statin
CHD or CHD risk equivalent with LDL<100; HDL < 50. Niacin red CIMT with fewer comp CV endpts (MI/revasc/ACS/death) p= 0.04.
Early Use of Statins After ACS Large Randomized Trials
• MIRACL 3086 patients with UA or non-Q wave MI
Atorva 80mg vs placebo.
Atorva 80mg reduced symptomatic ischemia requiring hospitalization;
not death, resucsciation after arrest or MI/ revascularization
• PROVE IT-TIMI 22:
compared atorvastatin 80mg with pravasatin 40mg in 4162 patients with ACS
LDL lower: 62 vs 96
combined endpoint (death any cause, MI, UA coronary revasc,CVA ) sign lower atorvastatin group with HR 0.84 CRP lower with atrovastatin.
Reduction in Stroke
• SPARCL: Atorvastatin reduced stroke, CAD events. No reduction in all cause mortality.
• HPS: Simvastatin reduced risk of first stroke (ischemic) compared to placebo.
• CARE: Pravastatin reduced risk of CAD event, CVA and CVA + TIA.
• ASCOTT-LLA: In high risk primary prev. patients with HTN and normal lipids, the risk of CVA was lower with Atorvastatin than placebo.
Pleiotropic benefits
• Plaque stabilization
• Reduces inflammation
• Improves endothelial function
• Promotes angiogenesis
• Repair endothelial injury
• Stabilizes arterial plaque
• Prevents cardiovascular and cerebrovascular events
Side Effects

Hepatic Dysfunction
• High aminotransferaces (ALT) • 0.5-3% occurrence of persistent elevations of
LFT’s in patients on statins. – Highest occurrence first 3-4 months of therapy
• Overall incidence of hepatic failure is no different than the incidence in the general population.
• FDA recommended in 2012 to check LFT’s prior to initiating statin therapy and when clinically indicated (fatty liver disease, statin intolerance, prior history of elevations).
• Routine LFT monitoring is not indicated. • Change or lower statin dose if ALT > 3x ULN
Myopathic Syndromes • Myalgia: Muscle discomfort (aches, soreness,
stiffness, tenderness) with a normal CK – 2-11% chance. Resolves days to weeks after
discontinuing
• Myopathy: Muscle weakness with or without CK elevation
• Myositis: Muscle inflammation (with elevated CK) – 0.5% chance
• Myonecrosis: Elevated CK compared with baseline – Clinically significant if CK is > 10 times normal with
muscle symptoms
– Occurs in < 0.5% of patients in clinical trials
Rhabdomyolysis
• Rhabdomyolysis: Myonecrosis with myoglobinuria or ARF.
– < 0.1% chance
• Rhabdomyolysis with ARF has primarily been seen when a statin is used with cyclosporine, gemfibrozil or protease inhibitors
Myopathic Syndromes
• Increased susceptibility with acute or chronic renal failure, obstructive liver disease and hypothyroidism
• Consider re-challenging or switching to another statin
• Pravastatin and fluvastatin - less muscle toxicity
CK elevation
• Other causes: hypothyroidism, trauma from athletics or high impact sports (running, hockey, etc)
• Discontinue statin if CK > 10 x ULN
• Consider switching statins
• Routine CK monitoring is not recommended
• Check baseline CK before statin therapy is initiated.
Renal Dysfunction
• Statins can cause proteinuria. Most reports are with Simvastatin and Rosuvastatin.
• Believed to be a benign finding
Memory Loss • Review of adverse events reported
to the FDA from 11/1997 – 2/2002 found 60 reports of memory changes. Most were with lipophilic statins (Atorvastatin and Simvastatin).
• Annals of Internal Medicine (2013) published a review of randomized trials and observational studies that did not suggest that statins harm cognition. Quality of evidence was low to moderate, especially with high-intensity therapy.
Prevention of Dementia
• Retrospective studies have shown that statins may prevent dementia.
• The Rotterdam study (n=6992) showed a decreased risk of Alzheimer's Disease
• Randomized controlled trials with dementia or cognitive decline as a primary endpoint are needed to determine this risk.
Diabetes Mellitus
• Jupiter Trial, IDEAL, TNT, A to Z, PROVE IT – TIMI 22, SEARCH raised concern for new onset diabetes
• Increased incidence with higher dose statin therapy vs. moderate dose therapy
• One case DM for every 500 patients treated with intensive rather than moderate statin therapy
• Benefit of statins on cardiovascular events and mortality outweigh risks.
Pregnancy
• Category X
• Discontinue prior to conception
• Risk is likely small with statin use
– Increase in congenital CNS and limb abnormalities with exposure of lipophilic statins in the 1st trimester.
• Use discouraged while breastfeeding
Cancer
• 4S – 10 year follow up
• West of Scotland Coronary Prevention Study (WOSCOPS) – 10 year follow up
• Heart Protection Study (HPS) – 11 year follow up
Statins have no effect on cancer incidence or mortality
Cataracts
• Large cohort studies from England, Wales and US military health system found association of statins and increased cataracts
• Randomized trial in the British Journal of Ophthalmology (1995) showed no increase in risk of cataracts.
– Most case control and cohort studies also support this.
Possible Risks
• Neuropathy – causal association with statin use
• Lupus – drug induced by statins
• Androgen synthesis
– Men: Not clinically significant
– Women: May reduce androgen levels
Special Populations
Chronic liver disease + statin
• Used to decrease cardiovascular risk
• Abstinence from alcohol
• Low dose Pravastatin (preferred)
• No increased risk with baseline aminotransferace elevation + statin
• Safe with Gilbert’s syndrome
• Primary biliary cirrhosis + Atorvastatin showed significant elevation in transaminases
– Avoid statins with significant cholestasis
CKD + Statin
• Atorvastatin and Fluvastatin do not require dose adjustment in severe CKD
– Pravastatin may be safer than other remaining options
• Dose adjustment is warranted with other statins with CrCl < 30 mL/min
Interactions • CYP3A4: Cyclosporine, macrolide antibiotics,
HIV protease inhibitors, CCB’s, Amiodarone, Antifungal agents
– Grapefruit juice: 8-oz glass or one-half of a grapefruit or less is unlikely to cause a problem
• Fibrates: ex. Gemfibrozil, fenofibrate
• Niacin
NEW STATIN GUIDELINES
11/12/2013: New guidelines for cholesterol to reduce risk of ASCVD (atherosclerotic cardiovascular disease) in adults Joint task force from the ACC (American College Of Cardiology) and AHA (American Heart Association) 12 years ago guidelines from ATP III- (Adult Treatment Panel, previous gold standard) with emphasis on LDL lowering for high risk patients
33,000 more
people on
STATINS!!!!
What’s known, what’s new
KNOWN:
• LDL matters- increased “bad” cholesterol leads to heart disease
NEW:
• 4 different “Statin Benefit Groups”:
• ID whose at the highest risk for having CVD and prescribe statin therapy
What’s different with new guidelines?
• Only evidence based randomized controlled trials used to provide the most compelling data
• New cardiovascular risk calculator
• Paradigm shift
4 Groups
• ACS (acute coronary syndrome)
• CAD, MI, CABG, stent
• PAD or history of arterial revascularization
• Stroke, TIA (new)
Statin Benefit Groups
• Whose with established ASCVD or established heart disease (secondary prevention)
• No history of heart disease, but LDL-C levels of >190 mg/dl or higher (primary prevention)
• Diabetics: 40-75 y/o with LDL 70-189 mg/dl without heart disease
• 40-75 y/o with LDL-C levels 70-189 with a 10 year risk of 7.5% or higher (no diabetes)
Not in the Recommended Group?
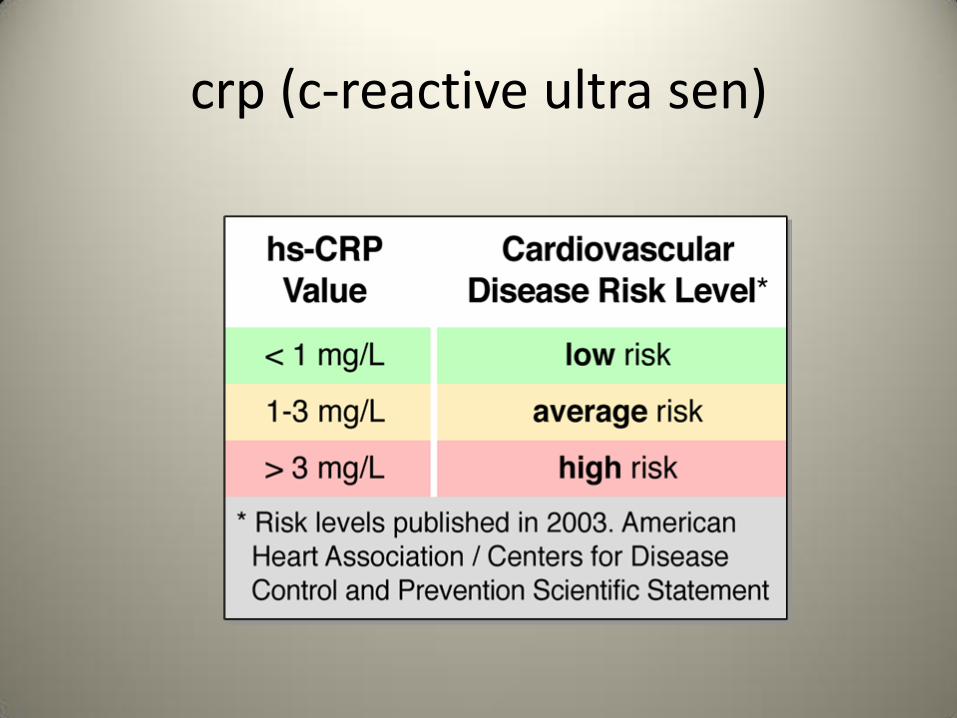
• Elevated high-sensitivity CRP 2 mg/L or higher- marker of inflammation
• Familial hyperlipidemia
• Family history – ASCVD onset in 1st degree male >55 or female >65
• Elevated coronary artery calcium score
• Elevated LP(a)
Guidelines Include:
• CAD
• STROKE
• PAD (peripheral arterial disease)
• DIABETES
Dislikes
• New risk assessment calculator to identify 10 year risk of CV disease likelihood- untested
• No recommendations for lowering triglycerides
• No benchmark for LDL goals
• Emphasis on high or moderate dose statins challenging with statin intolerance
2013 Risk Calculator • The calculator uses nine pieces of
information—sex, age, race, total cholesterol, HDL cholesterol, systolic blood pressure, current treatment for high blood pressure, diagnosis of diabetes, smoking habits.
• The new guidelines recommend a statin for seemingly healthy people with a risk of 7.5% or higher
Risk Calculator
• http://myamericanheart.org/professional/ • “Something is terribly wrong,” Dr. Nissen said.
Using the calculator’s results, he said, “your average healthy Joe gets treated, virtually every African-American man over 65 gets treated.”
- EMPHASIS ON AGE AND SEX. DOES NOT INCLUDE FAMILY HISTORY, TRIGS, CRP, LP(A)
65 year old male s/p MI at age 56, not active, no special diet
• TG : 365
• HDL-C : 35
• LDL-C : 78
• Glucose: :144
• What would you do first? Hint: new guidelines don’t address triglyceride levels
Average Jane
• 30 year old female, father died of MI at age 45
• total cholesterol of 270 mg/dL
• Triglycerides: 360 mg/dL
• HDL- 45
• LDL-180
• Due to her young age, risk calculator doesn’t apply. Should we wait 10 years to treat??
AVERAGE JOE
65 y/o AA male, primary prevention, no history of CAD, DM, HPTN. LP(a) normal. Fasting lipids: Total cholesterol 190 mg/dL HDL: 64 Triglycerides: 125 LDL-76 BP 130 systolic New calculator: 10 year risk score of CV disease= 7.5% Recommend moderate intensity statin treatment (overtreatment)
Do I really need a statin? Individualize!
Statin
All Statins are NOT Created Equal
• Generic:
• Pravastatin (gentle)
• Simvastatin (restrictions past 40 mg)
• Atorvastatin (lipitor)
• Not Generic:
• Rosuvastatin (crestor)
• Pitavastatin
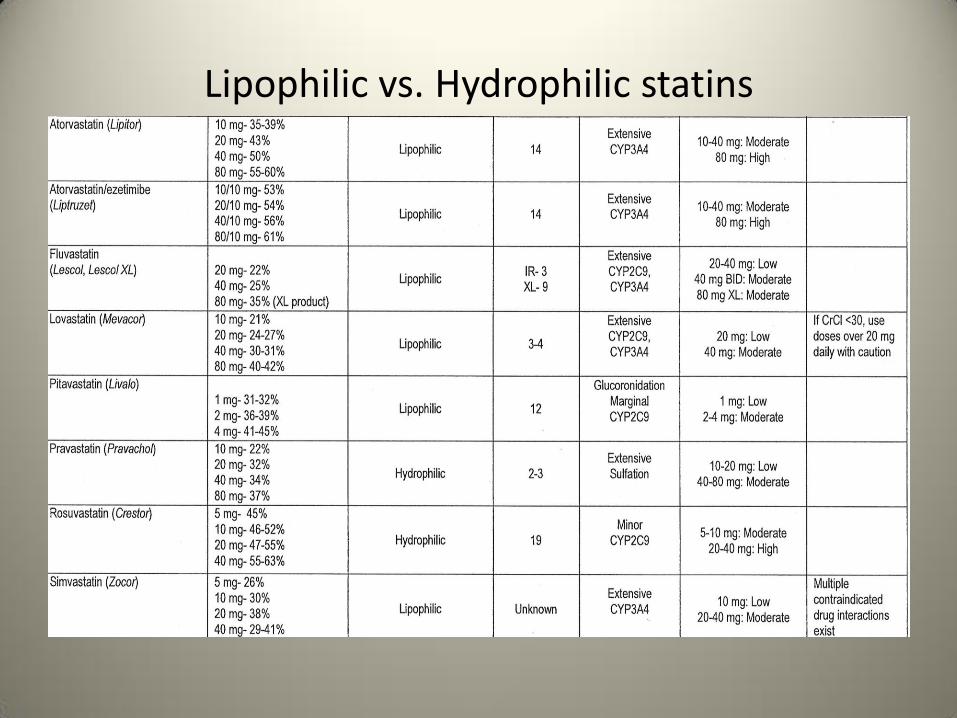
Lipophilic vs. Hydrophilic statins
Preventive Cardiology Jb-1
• Clear LDL goals: may be as high as 130 mg/dL or as low as 70 mg/dL
• Lifestyle management is addressed: diet, weight, exercise, co-morbidities, risk factors
- start statin lowest dose and increase as tolerated
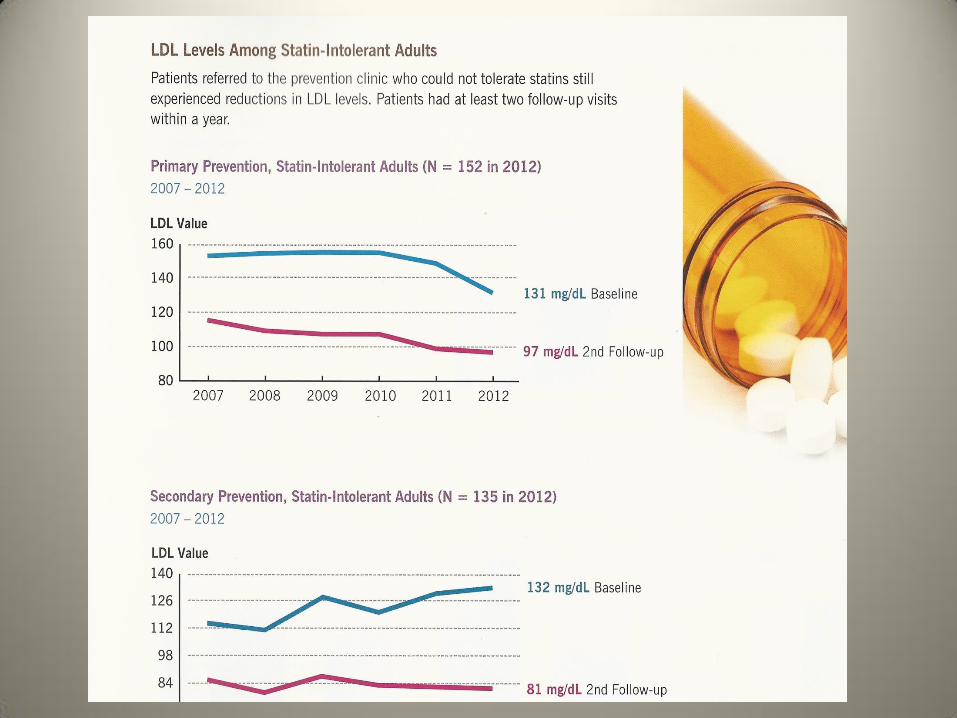
Statin Intolerance
• Literature suggests statin related events 5-10% in RCT
• Clinical practice: 20% or more of patients experience subjective intolerance
• Muscle aches, weakness, constant, often bilateral. Symptoms relieved within days after stopping statins
Therapies for statin intolerance
• Co-enzyme Q-10
• Treating vitamin D deficiency
• Switching statins
• Adding non-statin therapy
• Drug holiday- re-challenge
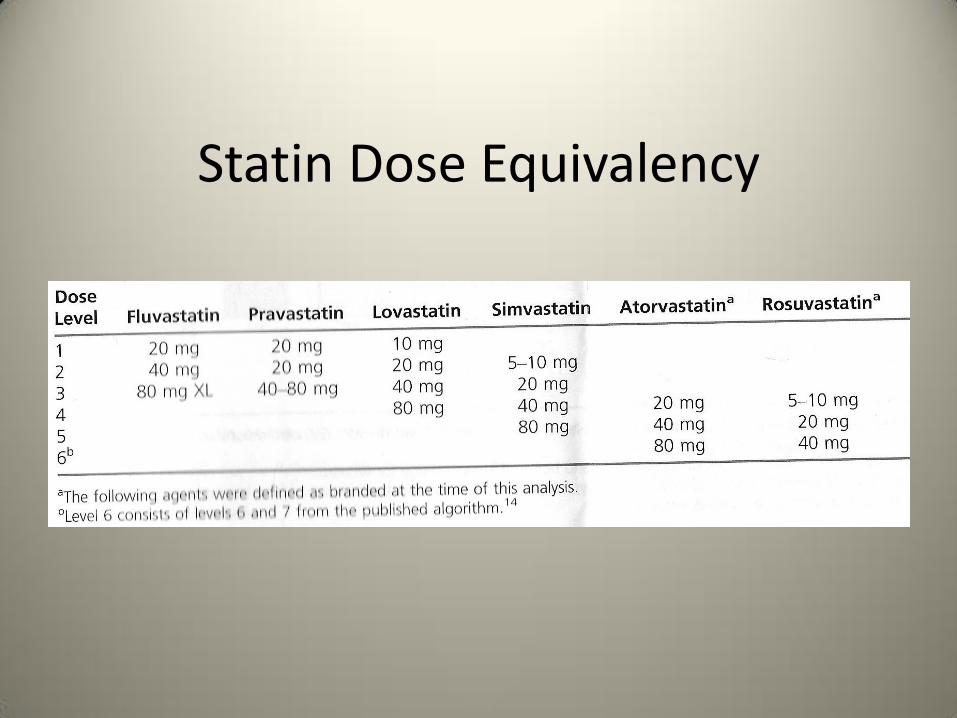
Statin Dose Equivalency
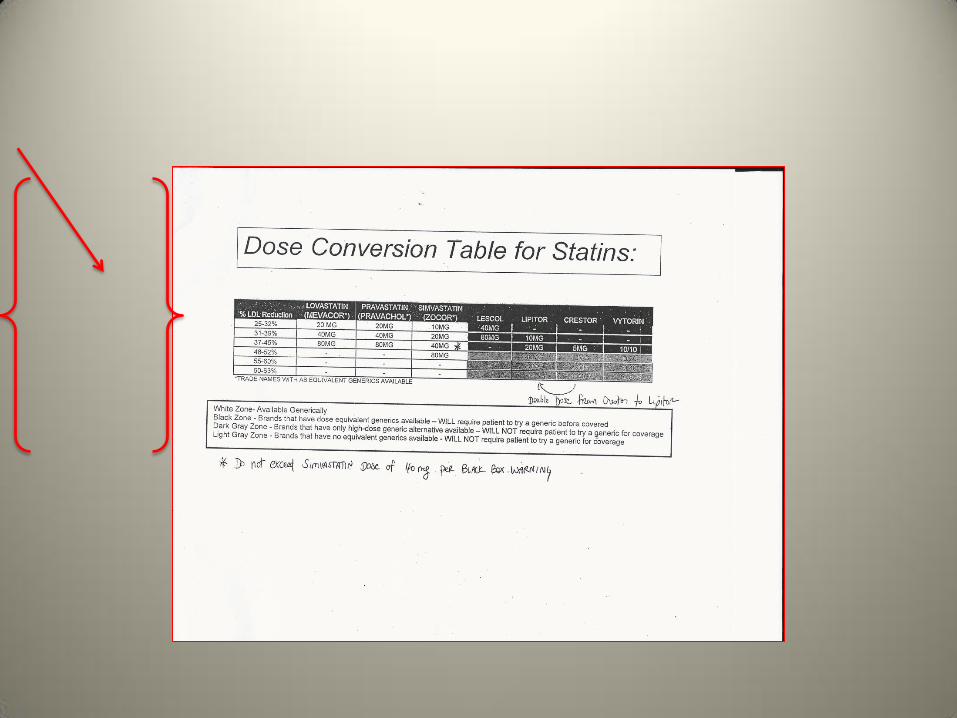
Caution: FDA warning
• Simvastatin: limit dosing to no > than 40 mg daily
• No more than 10 mg simvastatin if patient on amiodarone, diltiazem, verapamil: FDA alert 2011 (considered low dose statin)due to risk of myopathy
• Amlodipine, ranexa- no more than simvastatin 20 mg
• Simva contraindicated: antifungal –azole, antimicrobials-mycins, HIV protease inhibitors
Intermittent dosing
Rosuvastatin (Crestor) in particular can effectively be dosed as low as 2.5 mg twice weekly due to:
– Long half-life
– High potency
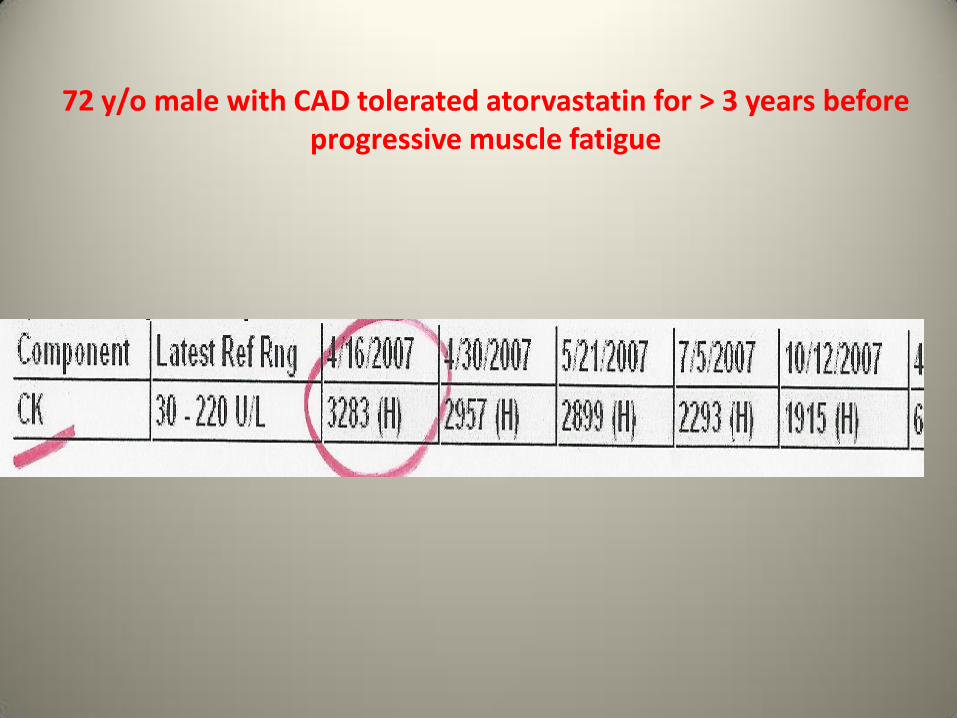
72 y/o male with CAD tolerated atorvastatin for > 3 years before progressive muscle fatigue
CK elevation
• While on statins if CK> 2.5 times normal stop the statin and monitor symptoms
If CK back down to normal after stopping statin, can re-challenge with different drug or dose
Cleveland Clinic Experience
• PC analyzed EMR of 1,605 patients with documented intolerance to at least two statins (between 1995-2010)
• Study showed most patients can tolerate some statin as opposed to none at all
3 groups analyzed
Daily statins, intermittent statin, no statin use
LDL lowering and all cause mortality analyzed
Trend toward a survival benefit for those who could tolerate some statin vs. no statin group
An Apple A Day?
• 150 year old proverb has withstood the test of time
• Apple + statin to >50 age group for primary prevention in the UK theorized
• BMJ 2013: 347, p. 1-6
It’s Complicated:
• 3/14/2014 YouTube Dr. Oz
Apple vs. Statin
References
• Kakavas PW, McManus JL, Wolfe TA, et al. The Need for a Systemic Approach to Statin Switching. Journal of Cardiovascular Nursing. 2012; 28 (6): 565-572.
• Lamb MM, Downes JM, Lackey KT. Cholesterol Management Update. The RX Consultant. 2014; 23 (3):1-7.
• Briggs AD, Mizdrak A, Scarborough P. A statin a day keeps the doctor away: comparative proverb assessment modelling study. British Medical Journal. 2013: 347: 1-6.
• Mantle D. Pharmacology of coenzyme Q10: Relevance to cardiovascular and other disorders. Nurse Prescribing. 2013; 11 (12): 602-607.
• Fernandez G, Spatz ES, Jablecki C. Statin myopathy: A common dilemma not reflected in clinical trials. Cleveland Clinic Journal of Medicine. 2011; 75 (6): 393-402.
• Darrach D. Making Progress on MS: Neurology Now. Aug/Sept 2013: 48-51. • Sakamoto, T, Kojima, S, Ogawa, H. Usefulness of Hydrophilic vs Lipophilic Statins
After Acute Myocardial Infarction. Circulation Journal. 2007;71: 1348-53.
• Stone NJ, Robinson JG, Lichtenstein AH, et al. Clinical Guideline: Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Disease Risk in Adults: Synopsis of the 2013 ACC/AHA Cholesterol Guideline. Annals of Internal Medicine. www.annals.org on 28 January 2014.
• Mampuya WM, Frid D, Rocco M, et al. Treatment strategies in patients with statin intolerance: The Cleveland Clinic Experience. American Heart Journal. 2013: 166 (3): 597-603.
• Raymond C, Cho L, Rocco M, et al. New cholesterol guidelines: Worth the wait? Cleveland Clinic Journal of Medicine. 2013; 81 (1): 11-19.
• Yan YL, Qiu B, Hu LJ, et al. Efficacy and safety evaluation of intensive statin therapy in older patients with coronary heart disease: a systematic review and meta-analysis. Eur J Clin Pharmacol. 2013; 69: 2001-09.
• Saint-Gerons DM, Fuente Honrubia C, Montero Corominas D, et al. Standard and intensive lipid-lowering therapy with statins for the primary prevention of vascular diseases: a population-based study. Eur J Clinic Pharmacol. 2014; 70: 99-108.
• Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA 2001; 285:1711.
• Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004; 350:1495.
References • Amarenco P, Bogousslavsky J, Callahan A 3rd, et al. High-dose atorvastatin after stroke or
transient ischemic attack. N Engl J Med 2006; 355:549. • Collins R, Armitage J, Parish S, et al. Effects of cholesterol-lowering with simvastatin on stroke
and other major vascular events in 20536 people with cerebrovascular disease or other high-risk conditions. Lancet 2004; 363:757.
• Plehn JF, Davis BR, Sacks FM, et al. Reduction of stroke incidence after myocardial infarction with pravastatin: the Cholesterol and Recurrent Events (CARE) study. The Care Investigators. Circulation 1999; 99:216.
• Sever PS, Dahlöf B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003; 361:1149.
• Kjekshus J, Apetrei E, Barrios V, et al. Rosuvastatin in older patients with systolic heart failure. N Engl J Med 2007; 357:2248.
• Cleland JG, McMurray JJ, Kjekshus J, et al. Plasma concentration of amino-terminal pro-brain natriuretic peptide in chronic heart failure: prediction of cardiovascular events and interaction with the effects of rosuvastatin: a report from CORONA (Controlled Rosuvastatin Multinational Trial in Heart Failure). J Am Coll Cardiol 2009; 54:1850.
• Gissi-HF Investigators, Tavazzi L, Maggioni AP, et al. Effect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet 2008; 372:1231.
• Björnsson E, Jacobsen EI, Kalaitzakis E. Hepatotoxicity associated with statins: reports of idiosyncratic liver injury post-marketing. J Hepatol 2012; 56:374.
• Cohen DE, Anania FA, Chalasani N, National Lipid Association Statin Safety Task Force Liver Expert Panel. An assessment of statin safety by hepatologists. Am J Cardiol 2006; 97:77C.
• Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002; 360:7.
• Charles EC, Olson KL, Sandhoff BG, et al. Evaluation of cases of severe statin-related transaminitis within a large health maintenance organization. Am J Med 2005; 118:618.
• http://www.fda.gov/Drugs/DrugSafety/ucm293101.htm (Accessed on February 28, 2012). • Weismantel D, Danis P. Clinical inquiries. What laboratory monitoring is appropriate to detect
adverse drug reactions in patients on cholesterol-lowering agents? J Fam Pract 2001; 50:927. • Gotto AM Jr. Safety and statin therapy: reconsidering the risks and benefits. Arch Intern Med
2003; 163:657. • Wagstaff LR, Mitton MW, Arvik BM, Doraiswamy PM. Statin-associated memory loss: analysis
of 60 case reports and review of the literature. Pharmacotherapy 2003; 23:871. • Richardson K, Schoen M, French B, et al. Statins and cognitive function: a systematic review.
Ann Intern Med 2013; 159:688. • Wolozin B, Kellman W, Ruosseau P, et al. Decreased prevalence of Alzheimer disease
associated with 3-hydroxy-3-methyglutaryl coenzyme A reductase inhibitors. Arch Neurol 2000; 57:1439.
• Jick H, Zornberg GL, Jick SS, et al. Statins and the risk of dementia. Lancet 2000; 356:1627. • Rodriguez EG, Dodge HH, Birzescu MA, et al. Use of lipid-lowering drugs in older adults with
and without dementia: a community-based epidemiological study. J Am Geriatr Soc 2002; 50:1852.
• Haag MD, Hofman A, Koudstaal PJ, et al. Statins are associated with a reduced risk of Alzheimer disease regardless of lipophilicity. The Rotterdam Study. J Neurol Neurosurg Psychiatry 2009; 80:13.
• Li G, Shofer JB, Rhew IC, et al. Age-varying association between statin use and incident Alzheimer's disease. J Am Geriatr Soc 2010; 58:1311.
• Vidt DG, Cressman MD, Harris S, et al. Rosuvastatin-induced arrest in progression of renal disease. Cardiology 2004; 102:52.
• Sidaway JE, Davidson RG, McTaggart F, et al. Inhibitors of 3-hydroxy-3-methylglutaryl-CoA reductase reduce receptor-mediated endocytosis in opossum kidney cells. J Am Soc Nephrol 2004; 15:2258.
• Alsheikh-Ali AA, Ambrose MS, Kuvin JT, Karas RH. The safety of rosuvastatin as used in common clinical practice: a postmarketing analysis. Circulation 2005; 111:3051.
• Grundy SM. The issue of statin safety: where do we stand? Circulation 2005; 111:3016. • www.fda.gov/cder/drug/infopage/rosuvastatin/crestor_CP.pdf (Accessed on June 10, 2005). • Schlienger RG, Haefeli WE, Jick H, Meier CR. Risk of cataract in patients treated with statins.
Arch Intern Med 2001; 161:2021. • Smeeth L, Hubbard R, Fletcher AE. Cataract and the use of statins: a case-control study. QJM
2003; 96:337. • Klein BE, Klein R, Lee KE, Grady LM. Statin use and incident nuclear cataract. JAMA 2006;
295:2752. • Harris ML, Bron AJ, Brown NA, et al. Absence of effect of simvastatin on the progression of lens
opacities in a randomised placebo controlled study. Oxford Cholesterol Study Group. Br J Ophthalmol 1995; 79:996.
• Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366:1267.
• Dale KM, Coleman CI, Henyan NN, et al. Statins and cancer risk: a meta-analysis. JAMA 2006; 295:74.
• Browning DR, Martin RM. Statins and risk of cancer: a systematic review and metaanalysis. Int J Cancer 2007; 120:833.
• Gaist D, Jeppesen U, Andersen M, et al. Statins and risk of polyneuropathy: a case-control study. Neurology 2002; 58:1333.
• Anderson JL, Muhlestein JB, Bair TL, et al. Do statins increase the risk of idiopathic polyneuropathy? Am J Cardiol 2005; 95:1097.
• Dobs AS, Schrott H, Davidson MH, et al. Effects of high-dose simvastatin on adrenal and gonadal steroidogenesis in men with hypercholesterolemia. Metabolism 2000; 49:1234.
• Davidson MH, Stein EA, Dujovne CA, et al. The efficacy and six-week tolerability of simvastatin 80 and 160 mg/day. Am J Cardiol 1997; 79:38.
• Santini SA, Carrozza C, Lulli P, et al. Atorvastatin treatment does not affect gonadal and adrenal hormones in type 2 diabetes patients with mild to moderate hypercholesterolemia. J Atheroscler Thromb 2003; 10:160.
• Sathyapalan T, Kilpatrick ES, Coady AM, Atkin SL. The effect of atorvastatin in patients with polycystic ovary syndrome: a randomized double-blind placebo-controlled study. J Clin Endocrinol Metab 2009; 94:103.
• Can Fam Physician 2003; 49:747. • Edison RJ, Muenke M. Central nervous system and limb anomalies in case reports of first-
trimester statin exposure. N Engl J Med 2004; 350:1579. • Kazmin A, Garcia-Bournissen F, Koren G. Risks of statin use during pregnancy: a systematic
review. J Obstet Gynaecol Can 2007; 29:906. • Taguchi N, Rubin ET, Hosokawa A, et al. Prenatal exposure to HMG-CoA reductase inhibitors:
effects on fetal and neonatal outcomes. Reprod Toxicol 2008; 26:175. • Costantine MM, Cleary K, Eunice Kennedy Shriver National Institute of Child Health and
Human Development Obstetric--Fetal Pharmacology Research Units Network. Pravastatin for the prevention of preeclampsia in high-risk pregnant women. Obstet Gynecol 2013; 121:349.
• Stojakovic T, Putz-Bankuti C, Fauler G, et al. Atorvastatin in patients with primary biliary cirrhosis and incomplete biochemical response to ursodeoxycholic acid. Hepatology 2007; 46:776.
• Sorokin A, Brown JL, Thompson PD. Primary biliary cirrhosis, hyperlipidemia, and atherosclerotic risk: a systematic review. Atherosclerosis 2007; 194:293.
• Cohen DE, Anania FA, Chalasani N, National Lipid Association Statin Safety Task Force Liver Expert Panel. An assessment of statin safety by hepatologists. Am J Cardiol 2006; 97:77C.
• Rosenson RS, Baker SK, Jacobson TA, et al. An assessment by the Statin Muscle Safety Task Force: 2014 update. J Clin Lipidol 2014; 8:S58.
• Norman DJ, Illingworth DR, Munson J, Hosenpud J. Myolysis and acute renal failure in a heart-transplant recipient receiving lovastatin. N Engl J Med 1988; 318:46.
• East C, Alivizatos PA, Grundy SM, et al. Rhabdomyolysis in patients receiving lovastatin after cardiac transplantation. N Engl J Med 1988; 318:47.
• Pierce LR, Wysowski DK, Gross TP. Myopathy and rhabdomyolysis associated with lovastatin-gemfibrozil combination therapy. JAMA 1990; 264:71.
• Yan, Y., Qiu, B., Hu, L., Jing, X., Liu, Y., Deng, S., ... She, Q. (2014). Efficacy and safety evaluation of intensive statin therapy in older patients with coronary heart disease: A systematic review and meta-analysis. European Journal of Clinical Pharmacology, 69, 2001-2009. Retrieved September 30, 2014.
• Shepardson NE, Shankar GM, Selkoe DJ. Cholesterol level and statin use in Alzheimer disease: II. Review of human trials and recommendations. Arch Neurol 2011; 68:1385.
• Haag MD, Hofman A, Koudstaal PJ, et al. Statins are associated with a reduced risk of Alzheimer disease regardless of lipophilicity. The Rotterdam Study. J Neurol Neurosurg Psychiatry 2009; 80:13.
• Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA 2011; 305:2556.
• Carter AA, Gomes T, Camacho X, et al. Risk of incident diabetes among patients treated with statins: population based study. BMJ 2013; 346:f2610.
• Efficacy of cholesterol lowering therapy in 18,686 patients with diabetes in 14 randomized trials of statins : a meta-analysis. Cholesterol Treatment Trialists’ (CTT ) Collaborators. Lancet 2008; 371: 117-25.
• Taylor AJ, Villines TC, Stanek EJ, et al. Extended-release niacin or ezetimibe and carotid intima-media thickness. N Engl J Med 2009; 361:2113.
• AIM-HIGH Investigators, Boden WE, Probstfield JL, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011; 365:2255.
• de Lemos JA, Blazing MA, Wiviott SD, et al. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA 2004; 292:1307.
• Ridker PM, Pradhan A, MacFadyen JG, et al. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: an analysis from the JUPITER trial. Lancet 2012; 380:565.
• Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes, and implications on outcomes in the general population. J Am Coll Cardiol 2012
• Ridker, PM, Rifai N, Clearfield M, et al. Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events.
NEJM 2001; 344:1959-65. • Ridker, PM, Danielson, MIA, Fonceca, FAH, et al. Rosuvastatin to prevent vascular events in
men and women with elevated C-reactive protein. NEJM 359; 2159-2207. • Post CABG: Aggressive lipid lowering improves the outcomes after CABG. Trial Knatterud, GL,
Rosen ber, Y, Campeau L, et al. Circ 2000; 102:157. • Merck Announces HPS-2 –THRIVE Study of TREDAPTIVE (Extended-Release Niacin/Laropiprant)
Did Not Achive Primary Endpoint [press release]. http: //www.mercknewsroom.com/press-release/prescription-medicine-news/merck – announces-hps2-thrive-study-tredaptive-entended-relea. Accessed Jan 11,2013.
• Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995; 333:1301.
• Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA 1998; 279:1615.
• Sever PS, Dahlöf B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003; 361:1149.
• Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994; 344:1383.
• Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998; 339:1349.
• LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005; 352:1425.
• Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med 1996; 335:1001.
• Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002; 360:7.
• Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004; 364:685.
• ACCORD Study Group, Ginsberg HN, Elam MB, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med 2010; 362:1563.
• Nakamura H, Arakawa K, Itakura H, et al. Primary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): a prospective randomised controlled trial. Lancet 2006; 368:1155.
• Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004; 350:1495.
• AIM-HIGH Investigators, Boden WE, Probstfield JL, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011; 365:2255.
• Rosengren, A, hagman, M, Wedel, H et al. Relationship between cholesterol level and mortaltiy among patients with CHD. European Heart Journal 1997; 18: 754.
• Effect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: the METEOR Trial. JAMA. 2007;297(12):1344.
• Jukema JW, Bruschke AV, van Boven AJ, et al. Effects of lipid lowering by pravastatin on progression and regression of coronary artery disease in symptomatic men with normal to moderately elevated serum cholesterol levels. The Regression Growth Evaluation Statin Study (REGRESS). Circulation 1995; 91:2528.
• Aronow HD, Topol EJ, Roe MT, et al. Effect of lipid-lowering therapy on early mortality after acute coronary syndromes: an observational study. Lancet 2001; 357:1063.
• Cashin-Hemphill L, Mack WJ, Pogoda JM, et al. Beneficial effects of colestipol-niacin on coronary atherosclerosis. A 4-year follow-up. JAMA 1990; 264:3013.
Pekkanen J, Linn S, Heiss G, et al. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N Engl J Med 1990; 322:1700. Schartl M, Bocksch W, Koschyk DH, et al. Use of intravascular ultrasound to compare effects of different strategies of lipid-lowering therapy on plaque volume and composition in patients with coronary artery disease. Circulation 2001; 104:387. Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004; 291:1071. Nissen SE, Nicholls SJ, Sipahi I, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA 2006; 295:1556. ACCORD Study Group, Ginsberg HN, Elam MB, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med 2010; 362:1563. Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA 2001; 285:1711. Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004; 350:1495. Norman DJ, Illingworth DR, Munson J, Hosenpud J. Myolysis and acute renal failure in a heart-transplant recipient receiving lovastatin. N Engl J Med 1988; 318:46. East C, Alivizatos PA, Grundy SM, et al. Rhabdomyolysis in patients receiving lovastatin after cardiac transplantation. N Engl J Med 1988; 318:47. Pierce LR, Wysowski DK, Gross TP. Myopathy and rhabdomyolysis associated with lovastatin-gemfibrozil combination therapy. JAMA 1990; 264:71. Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med 2007; 357:2109.
• Strandberg TE, Pyörälä K, Cook TJ, et al. Mortality and incidence of cancer during 10-year follow-up of the Scandinavian Simvastatin Survival Study (4S). Lancet 2004; 364:771.
• Ford I, Murray H, Packard CJ, et al. Long-term follow-up of the West of Scotland Coronary Prevention Study. N Engl J Med 2007; 357:1477.
• Heart Protection Study Collaborative Group, Bulbulia R, Bowman L, et al. Effects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in 20,536 high-risk individuals: a randomised controlled trial. Lancet 2011; 378:2013.
• Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005; 352:20.
• Tobert JA. Efficacy and long-term adverse effect pattern of lovastatin. Am J Cardiol 1988; 62:28J.
• Dujovne CA, Chremos AN, Pool JL, et al. Expanded clinical evaluation of lovastatin (EXCEL) study results: IV. Additional perspectives on the tolerability of lovastatin. Am J Med 1991; 91:25S.
• Boccuzzi SJ, Bocanegra TS, Walker JF, et al. Long-term safety and efficacy profile of simvastatin. Am J Cardiol 1991; 68:1127.
• Pedersen TR, Berg K, Cook TJ, et al. Safety and tolerability of cholesterol lowering with simvastatin during 5 years in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1996; 156:2085.