risks and costs associated with the ... & costs associated with the management of infectious...
TRANSCRIPT
RISKS AND COSTS ASSOCIATED WITH THE MANAGEMENT OF INFECTIOUS WASTES
Prepared for:
WHO/WPRO Manila, Philippines
By:
L.F. Diaz and G.M. Savage
Manila, Philippines December 2003

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 i
CONTENTS
Background..................................................................................................................................... 1 Environmental and Health Risks � General ................................................................................... 2
Occupational Health � Health care workers ............................................................................... 2 Occupational Health � Solid waste management workers......................................................... 2 Immunization campaigns ............................................................................................................ 3 Definitions.................................................................................................................................... 4
Waste Characterization .................................................................................................................. 6 Quantity ....................................................................................................................................... 6 Bulk Density .............................................................................................................................. 11 Other Characteristics ................................................................................................................ 12 Conclusions............................................................................................................................... 15
Treatment/Disposal Methods........................................................................................................ 15 Land Disposal............................................................................................................................ 16 Burial in Special Pits ................................................................................................................. 16 Encapsulation............................................................................................................................ 17
Risks Associated with Land Disposal ................................................................................... 19 Potential Impacts ................................................................................................................... 20
Microwave Disinfection Systems .............................................................................................. 29 Typical Microwave Disinfection System................................................................................ 29 Emissions .............................................................................................................................. 30
Autoclaves................................................................................................................................. 31 Other Considerations............................................................................................................. 32 Types of HCW that Can be Treated...................................................................................... 33 Types of HCW that Should Not be Treated .......................................................................... 33 Solid Residues from the Process .......................................................................................... 33 Liquid and Gaseous Emissions from the Process ................................................................ 34
Chemical Disinfection................................................................................................................ 34 Types of HCW that Can be Treated...................................................................................... 38 Types of HCW that Should Not be Treated .......................................................................... 38 Emissions and Residues from the Process .......................................................................... 39
Combustion ............................................................................................................................... 39 Low Technology Combustion................................................................................................ 40 Medium and High-Technology Combustion.......................................................................... 41 Types of Risks Associated with Combustion ........................................................................ 42 Potential Impacts ................................................................................................................... 44 Emission Control ................................................................................................................... 55
Emerging Technologies ............................................................................................................ 57 Plasma................................................................................................................................... 57 Pyrolysis................................................................................................................................. 57
Cost ........................................................................................................................................... 58 Trends ....................................................................................................................................... 59 Conclusions............................................................................................................................... 60 Recommendations .................................................................................................................... 60

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 ii
Urban Areas........................................................................................................................... 61 Rural Areas............................................................................................................................ 62 Small Island Communities..................................................................................................... 62
Relevant International Conventions and Protocols ...................................................................... 63 Stockholm Convention (2001)................................................................................................... 63 Montreal Protocol on Substances that Deplete the Ozone Layer (1987) ................................ 65 Convention on Long-Range Transboundary Air Pollution (1979) ............................................ 65 The United Nations Framework Convention on Climate Change ............................................ 66
Background............................................................................................................................ 66 Major Provisions of the Kyoto Protocol ................................................................................. 67 Status of Signatories & Ratification of the Convention ......................................................... 67
The Kyoto Protocol.................................................................................................................... 68 Status of the Kyoto Protocol.................................................................................................. 68
References.................................................................................................................................... 69

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 iii
EXECUTIVE SUMMARY
Every year, relatively large quantities of potentially infectious and hazardous wastes are generated in health care facilities throughout the world. Unfortunately, most economically developing countries suffer financial and other constraints to adequately manage these wastes. Generally in developing countries, few individuals in the staff of the health care facility are familiar with the procedures required for an effective and efficient waste management program. Health care workers as well as solid waste workers face the risk of injury or of infection as part of their occupation. Although, proper management of health care wastes includes a number of activities and several members of the staff, this report focuses on the treatment and final disposal of the wastes. It has been demonstrated that there is not a single method of waste treatment or disposal that completely eliminates all risks to the public or to the environment. In general, depending upon the type of technology, the residues are transformed from one phase to another. This report deals with the risks associated with treatment and disposal of health care wastes by means of technologies that have been demonstrated in the field. Specifically, the reports covers: land disposal, autoclaves, microwaves, chemical treatment, and incineration. Information regarding the risks associated with each one of the treatment or disposal methods was obtained from the results of research and in, some cases, from research conducted on the treatment or disposal of MSW. Definitions commonly used for various types of health care wastes are suggested and the results of waste characterization studies are provided. The total amount of hospital waste generated in all of the health care facilities evaluated in developing countries varied from 0.54 to 1.39 kg/bed-day. The reported amount of infectious (clinical, yellow bag) waste varied from 0.30 to 0.34 kg/bed-day. For comparison purposes, the daily production of medical waste in hospitals in Portugal is reported. The data are reported for four different types of waste (Group I to Group IV) and under two levels of segregation (usual practices and rigorous practices). Generally, according to this system of characterization, the level of risk to humans increases from Group I to Group IV. The total amount of health care waste is fairly constant and varied from 3.5 to 3.9 kg/bed-day. Due to a rigorous process of segregation, the amount of Group IV waste was reduced from 0.08 to 0.4 kg/bed-day and the amount of Group III waste increased from 1.6 to 1.9 kg/bed-day. The amount of Group I waste remained constant at about 1.9 kg/bed-day. As expected, a rigorous level of segregation at the point of generation reduces the amount of Group IV (wastes that under the law require incineration) and, at the same time, increases the amount of Group III (waste that presents biological risk). Thus, the information presented by the researchers in Portugal indicates that the quantity of wastes that require special treatment can be reduced from 10% to 2% by weight.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 iv
The average bulk density for non-infectious waste varied from 151 to 211 kg/m3, while that for infectious fluctuated from 226 to 262 kg/m3. The percentage of total health care waste of the total amount of municipal solid waste generated is on the order of 0.72% (the range can be vary from 0.36% to 1.44%) whereas the percentage of infectious waste of the municipal solid waste generated is about 0.27% (similarly the range can fluctuate from about 0.14% to 0.54%). The risks on the public health and on the environment are discussed for each of the options evaluated. The risks are presented due to liquid, gaseous, and solid discharges from the various alternatives. The report also presents the various costs (both capital and operation and maintenance) related to the alternatives assessed. Finally the report provides brief discussions on the relevant multilateral environmental agreements (conventions and protocols) that may have an impact on the treatment and disposal of HCW.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 1
Risks and Costs Associated with the Management of Infectious Wastes
Background Wastes generated in health care facilities in economically developing countries have raised serious concerns due to the inadequate treatment and final disposal practices accorded to them. Inappropriate treatment and final disposal of the wastes can lead to negative impacts on public health and on the environment. In addition, hazardous health care wastes, when inappropriately managed, may compromise the quality of patient care (lead to intra-hospital infections) and pose occupational health risks to those who care for the patients, as well as to those who participate in the management of the wastes within and outside the health care facility. Another relatively large population that is exposed to the risks posed by improperly treated health care wastes is the scavenger population that is working on the streets or at the final disposal facilities. Every year, relatively large quantities of potentially infectious and hazardous wastes are generated in health care facilities throughout the world. Unfortunately, most economically developing countries suffer financial and other constraints to adequately manage these wastes. Generally in developing countries, few individuals in the staff of the health care facility are familiar with the procedures required for an effective and efficient waste management program. Furthermore, the management of wastes is delegated to poorly educated laborers who perform most activities without proper guidance and insufficient protection. The environment where we live, work, study, and rest plays a major impact on our health. The risks to our health can take place in a number of ways i.e., the quality of our water supply as well as the quality of our ambient air. Health care workers are exposed to blood and body fluids as part of their occupation. As such, health care workers face the risk of infection due to bloodborne pathogens. There are several pathways for the transmission of disease in health care workers. Some of the most important pathways are: percutaneous injuries with contaminated sharps, contamination through the fecal-oral route (e.g., salmonellosis, hepatitis A), and contamination through airborne transmission (e.g., tuberculosis, measles). It has been reported that percutaneous exposures account for 66% to 95% of all occupational exposures to bloodborne pathogens (CCOHS, 2000; Puro, et al., 2001; Romea, et al., 1995). Injuries due to needle sticks account for 62% to 91% of percutaneous exposures (NaSH, 1999; Puro, et al., 2001; Romea, et al., 1995). An effective and efficient program for the management of health care wastes is a critical component of the facility�s infection control program and consequently plays an important role on the quality of care, as well as on the occupational health of the entire staff of the facility.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 2
Although, proper management of health care wastes includes a number of activities and several members of the staff, this report focuses on the treatment and final disposal of the wastes. It has been demonstrated that there is not a single method of waste treatment or disposal that completely eliminates all risks to the public or to the environment. In general, depending upon the type of technology, the residues are transformed from one phase to another. For example, in incineration, the combustible components of the wastes are converted into gaseous byproducts (CO2, H2O, CO and other gases) and non-combustible components remain as ash. With respect to risk reduction associated with microorganisms, the most important objective is to destroy them prior to release of the contaminated material into the environment. Pathogen destruction can be achieved through thermal, chemical, and irradiative treatment. Every human being is exposed to a great variety of risks to his health throughout his entire life. The risks can take a number of forms such as natural disasters, violence, food consumption, and communicable or non-communicable diseases. The generally accepted definition of risk is: "the probability of an adverse outcome, or a factor that increases that probability." This report deals with an evaluation of the risks and the costs associated with the treatment of health care wastes in economically developing countries.
Environmental and Health Risks – General
Occupational Health – Health care workers The three infections that are most commonly transmitted to health care workers are: hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV). Among the 35 million health care workers worldwide, it has been estimated that about 3 million receive percutaneous exposures to bloodborne pathogens each year, 2 million of those to HBV, 0.9 million to HCV, and 170,000 to HIV. These injuries may result in 15,000 HCV, 70,000 HBV, and 500 HIV infections. More than 90% of these infections take place in developing countries (WHO 2002). The risk of transmission of HIV, HCV, and HBV following a percutaneous exposure to sharps used on an infected source patient has been estimated precisely from a number of cohort studies conducted among health care workers (Bell, 1997; Gerberding, 1995; Ippolito, et al., 1993; Puro, et al., 2001; Mitsui, et al., 1992).
Occupational Health – Solid waste management workers Workers involved in the collection and treatment of the wastes (either at the health care facility or offsite) also are exposed to a certain amount of risk. A limited number of studies have been carried out to examine exposure to potentially infectious agents in the solid waste stream by
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 3
workers in the solid waste sector. Some of these studies were carried out more than 30 years ago. Gellin and Zavon examined 97 waste workers employed by the City of Cincinnati (USA) from January to February 1968 for skin disorders (Gellin and Zavon, 1970). Forty-one cases of bacterial, fungal, or viral dermatitis were observed in this group. However, all of the cases were classified as non-occupational in origin. Cimino reviewed health records for waste workers employed by the New York City Sanitation Department working between 1968 and 1969 (Cimino, 1975). Needle stick injuries were reported due to the presence of uncontained needles in the waste collected from hospitals, physician's and dentist's offices, and needles discarded by drug addicts. Workers who reported needle stick injuries were given gamma globulin prophylaxis and no cases of hepatitis were reported. In 1979, Clark, et al. evaluated the incidence of viral infection among 43 waste collection workers. Sera antibody levels for 18 viruses were examined from blood samples collected during the spring and fall. The authors did not find any evidence of increased occupational risk to bloodborne viral infections (Clark, et al., 1979). In 1990, Turnberg and Frost reported the results of a study to examine occupational exposure of waste industry workers to blood-contaminated waste and discarded hypodermic needles in the waste stream in the State of Washington (USA). In this study, a total of 940 survey forms were distributed to waste workers and 438 survey forms or 47% were returned. Some of the most pertinent results include: 32% of the respondents indicated having direct contact with blood and 21% of the respondents reported having been stuck or scratched by hypodermic needles in the waste. Waste workers reported that needles were identified originating from both health care facilities as well as from residential sources (Turnberg and Frost, 1990).
Immunization campaigns One of the WHO's major programs deals with the implementation of immunization programs in a number of countries throughout the world. Immunization programs result in the production of a sizeable number of used syringes and needles. Proper treatment and disposal of the used syringes and of the needles is necessary due to the following reasons:
• to keep the public and in particular health care workers from injury by accidentally touching them; and
• to prevent the reuse of used syringes and needles. The barrel and the plunger of a "conventional" plastic syringe are made out of polyethylene (PE). In theory, the syringe, if incinerated, does not generate toxic compounds such as dioxins because PE does not contain chlorine. With respect to the needles, the part that connects them to the syringe may be made out polyvinyl chloride (PVC), which may generate PCDDs, PCDFs, and coplanar PCBs. In addition, the needles are generally made out of a heat-treatable stainless steel or carbon steel. Many needles are plated with nickel to prevent corrosion.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 4
The WHO defines a safe injection as one that meets the following conditions: 1) does not harm the recipient, 2) does not expose the injection provider to any avoidable risk, and 3) does not result in waste that is dangerous to other people. Recommended best infection control practices by the WHO (Hutin, et al., 2003) for preventing infections among injection providers deal with:
• the prevention of movements of patients, • the prevention of unsafe recapping of needles, and • the collection of contaminated sharps in puncture- and liquid-proof containers.
Definitions Definitions for wastes that are generated in health care facilities have not been agreed upon on a worldwide basis. This situation leads to confusion and misinterpretation of findings from research and other work. Given the present situation, a few definitions have been selected from various sources that seem to be the most commonly used. Health care waste is produced in all conventional facilities dedicated to the treatment of patients such as hospitals, clinics, medical posts, and others. Other facilities or establishments that generate health care wastes include: veterinary hospitals, dental and medical offices where treatment is provided, analytical laboratories, dialysis facilities, blood banks, university laboratories and similar facilities, tattooing and body piercing facilities, mortuaries, and others. Health care wastes refers to all materials, biological or non-biological, that are discarded in any health care facility and are not intended for any other use. In the most global definition, health care waste would include solid, liquid, and gaseous residues. However, for the purpose of this report definitions are limited to the solid medium. A modern, large facility would generate waste such as paper, cardboard, glass, metals and similar materials from administrative offices, residues from food preparation from the dietary facilities, grass clippings and prunings from maintenance of the grounds, as well as a variety of other materials that would be generated as the result of treatment of patients. General waste refers to that portion of the health care waste that poses a minimum degree of risk to human health as it is primarily composed of materials similar to those found in domestic waste such as paper products, glass, metals, kitchen wastes, and other non-infectious materials. Medical waste (sometimes known as Clinical waste) is defined as any solid waste that is generated in the diagnosis, treatment, or immunization of human beings or animals, in research pertaining thereto, or in the production or testing of biological materials, including but not limited to:
• soiled or blood-soaked bandages; • culture dishes and other glassware; • discarded surgical gloves; • discarded surgical instruments (i.e., scalpels); • needles - used to give injections or draw blood; • cultures, stocks, swabs used to inoculate cultures; and
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 5
• removed body parts or body organs. Infectious waste means that fraction of medical waste that can potentially transmit an infectious disease. In some countries, this is referred to as �regulated medical waste� or �RMW.� Infected "sharps" are a sub-category of infectious wastes. Pathological waste is defined as that waste that consists of blood, body fluids, tissue, organs, body parts, human fetuses, and animal carcasses. Recognizable human or animal body parts are also called anatomical waste. This category generally is considered a part of infectious waste even though it may contain non-infectious components. Radioactive waste means all materials contaminated with radionuclides (radionuclides are used in health care facilities for treatment, diagnosis, and research), which spontaneously emit particles and/or rays by the disintegration of the nuclei of their atoms. Pharmaceutical waste means all products, drugs, drug residuals, and therapeutic chemicals that have been returned from wards, have been spilled, are outdated or contaminated, or have to be disposed of because they are no longer required. Hazardous waste means all materials that can cause harm to human beings or animals or to the environment due to their biological, physical, or chemical characteristics (infectivity, sharpness, flammability, corrosivity, and others). In some cases, these wastes are further sub-divided into chemical wastes, and pressurized containers. Work conducted in several countries indicates that only a relatively small fraction of health care wastes (between 10% and 20% by weight) is hazardous and contain materials or compounds that may be infectious, toxic, or radioactive (Prüss, et al., 1999). Sharps is the term used to denote wastes, which could cause physical injury (cuts or punctures) due to their nature. These materials include needles (and syringes), scalpels, saws, blades, broken glass, knives, and other similar materials. A simplified diagram showing health care wastes and other wastes as sub-sets is presented in Figure 1.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 6
Health Care Wastes
Medical Wastes
Infectious Wastes
Figure 1. Explanation of Health Care Wastes and Some of its Components
Waste Characterization One of the most important and initial steps in the development of a plan or in the performance of risk or cost analyses in the field of solid waste management involves a thorough understanding of the quantities and properties of the material that needs to be evaluated or treated. In this particular case, the material to be dealt with is health care waste. Unfortunately, there is a limited amount of reliable information in the open literature on the quantities and characteristics of the various types of wastes that are generated in health care facilities. Furthermore, most of the reports dealing with analyses and evaluations conducted on the performance of a particular type of treatment method either in industrialized or in developing countries do not clearly specify or characterize the quality of the waste undergoing the treatment. This section of this report attempts to provide basic information on the quantities and characteristics of the solid wastes generated in various types of health care facilities located in industrialized and in developing countries. The majority of the information has been obtained from the open literature although some data have been collected from reports available to the authors. Care has been taken to only report and interpret data that were collected within the last ten years following a prescribed methodology and under controlled conditions.
Quantity The quantities of waste generated in various government hospitals in Peru are reported Table 1. The data in the table for total hospital waste generation are reported as a function of various parameters such as kg/bed-day, kg/patient-day, and kg/worker-day. The data show that, based

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 7
on the most common means of reporting, the six hospitals generated an average of 0.76 kg/bed-day of total waste. In addition, the information in the table shows waste generation rates for various services such as Outpatient, Surgery, and Delivery Room. The data in Table 2 indicate the amount of clinical, general, and kitchen waste generated in a provincial hospital in Viet Nam. As shown in the table, the average amount of clinical (in this case infectious) waste amounts to about 0.30 kg/patient-day. On the other hand, the average amount of general waste was 0.75 kg/patient-day and that of food/kitchen waste was 0.35 kg/patient-day for a total of about 1.39 kg/patient-day. The information presented in Table 3 indicates the amount of clinical waste generated by the various departments reported in kg/patient-day. As shown in the table, the generation ranges from 0.005 (for outpatient) to 0.68 (for obstetrics and gynecology) kg/patient-day. The amounts of waste generated in hospitals in Metropolitan Manila, Philippines are reported in Table 4. The information in the table presents the quantity of yellow bag (waste that requires special treatment) and black bag (waste considered similar to municipal waste) as reported by two different studies. As shown in the table, the amount of yellow bag waste was 0.31 kg/bed-day and that of black bag waste was 0.39 kg/bed-day giving a total of approximately 0.56 kg/bed-day (total waste 0.87 kg/bed-day). Another study conducted in a hospital in Metropolitan Manila reported the quantities of infectious and non-infectious wastes generated in the institution and are shown in Table 5. The amount of infectious waste was 0.34 kg/bed-day (63%) and that of non-infectious waste was 0.20 kg/bed-day (37%). The total waste production was about 0.54 kg/bed-day. Furthermore, information collected during this same study show that the percentage of total health care waste of the total amount of municipal solid waste generated is on the order of 0.72% (the range can vary from 0.36% to 1.44%) whereas the percentage of infectious waste of the municipal solid waste generated is about 0.27% (similarly the range can fluctuate from about 0.14% to 0.54%).
Table 1. Unit Generation of Solid Wastes in Hospitals by Source of Generation in Various Health Care Facilities in Peru
Hospital - Total Generation Outpatient Surgery Delivery Room
Institution Kg/bed/
day Kg/patient/
day Kg/worker/
day Kg/consult/
day Kg/surgery/
day Kg/delivery/
day Jose Olavarria (Tumbes) 0.71 2.21 0.48 0.095 2.71 2.23
Docente (Trujillo) 1.40 2.00 0.45 0.056 3.50 4.44
Regional of Ica (Ica) 0.62 1.31 0.42 0.039 1.20 1.95
Regional of Cusco (Cusco) 0.49 1.13 0.34 0.026 1.10 1.50
Daniel A. Carrion (Huancayo) 0.76 1.38 0.35 0.036 1.80 0.73
Regional of Loreto (Iquitos) 0.59 7.56 0.45 0.032 0.91 0.97
Average 0.76 2.60 0.42 0.047 1.87 1.97 Source: Ministerio de Salud, 1995.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 8
Table 2. Waste Generation Analysis by Major Sources in a Provincial Hospital in Viet Nam (1992)
Ward
Date Number of
Patients Clinical
(kg) General
(kg)
Total Ward
Food Kitchen
Total Waste
1 92 29 57 86 25 111
2 89 28 53 81 41 122
3 97 33 64 97 30 127
4 95 37 57 94 37 131
5 96 27 68 95 37 132
6 83 29 76 105 32 137
7 97 23 53 76 32 108
8 95 28 55 83 42 125
9 93 19 89 108 22 130
10 79 26 56 82 32 114
11 68 21 83 104 21 125
12 87 23 88 111 20 131
Average 89.25 26.92 66.58 93.50 30.92 124.42
Kg/patient 0.30 0.75 1.05 0.35 1.39 Source: Saw and Hoo, 1998.
Table 3. Clinical Waste Generation by Source in a Provincial Hospital in Viet Nam (1992)
Source Clinical Waste Generation
(Avg. kg/patient-day) Medical ward 0.09
Surgical ward 0.21
Obstetrics and gynecology 0.68
Pediatric 0.1
Orthopedics -
Ophthalmology -
Ear, nose, throat -
Psychiatry -
Intensive Care Unit -
Outpatient 0.005
Accidents and emergencies 0.05
Dental Clinic 0.02
Total 2.155 Source: Saw and Hoo, 1998.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 9
Table 4. Quantities of Wastes Generated in Hospitals
in Metro Manila, Philippines (1999 and 2002)
Type of Waste Quantity* (kg/day) Percent
Waste Quantity
(kg/day-bed)
Waste Quantity
(kg/day-bed)
Yellow bag
Pathological 27.9 0.06
Infectious 29.79 0.06
Sharps 28.24 0.06
Total yellow bag 85.93 30.37 0.17 0.31 Black bag
Domestic 158.85 0.32
Paper 38.21 0.08
Total black bag 197.06 69.63 0.39 N/A
Totals 282.99 100.00 0.56 Source: Asian Development Bank, 2003. N/A: Not Available. Yellow bag: require special management.
Table 5. Quantities of Waste Generated in Hospitals in Metro Manila, Philippines (2003)
Source of Waste Total five days (kg)
Average (kg/day)
Average (kg/bed-day)
Infectious
Total Infectious 1016 203 0.34 Non-Infectious
PICU 106 21 0.04
Ward 274 55 0.09
OPD 68.3 14 0.02
ER-Surgery 138 28 0.05
Total Non-infectious 586.3 117 0.20
Totals 1602.3 320 0.54 Source: Asian Development Bank, 2003.
Recognizing that the information for Viet Nam was collected in a provincial hospital and assuming that the number of patients reported by Viet Nam is equivalent to the number of occupied beds, then we can conclude that the total amount of hospital waste generated in all of these facilities varied from 0.54 to 1.39 kg/bed-day. On the other hand, the reported amount of
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 10
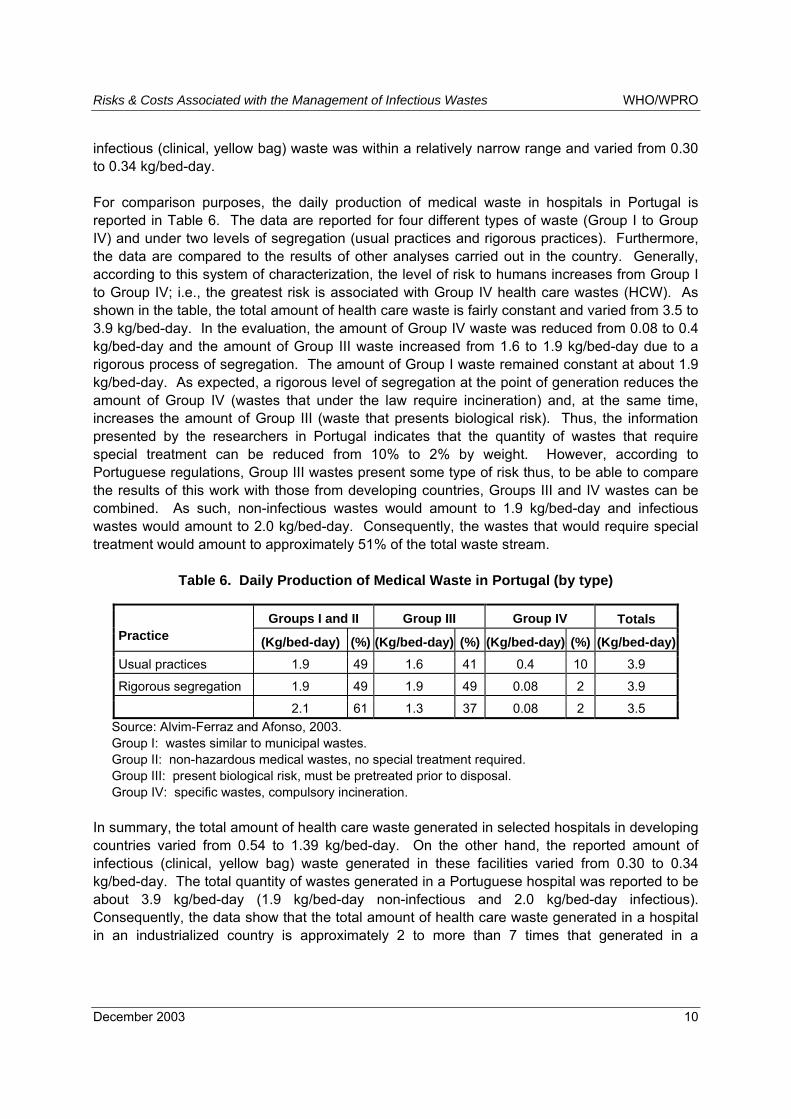
infectious (clinical, yellow bag) waste was within a relatively narrow range and varied from 0.30 to 0.34 kg/bed-day. For comparison purposes, the daily production of medical waste in hospitals in Portugal is reported in Table 6. The data are reported for four different types of waste (Group I to Group IV) and under two levels of segregation (usual practices and rigorous practices). Furthermore, the data are compared to the results of other analyses carried out in the country. Generally, according to this system of characterization, the level of risk to humans increases from Group I to Group IV; i.e., the greatest risk is associated with Group IV health care wastes (HCW). As shown in the table, the total amount of health care waste is fairly constant and varied from 3.5 to 3.9 kg/bed-day. In the evaluation, the amount of Group IV waste was reduced from 0.08 to 0.4 kg/bed-day and the amount of Group III waste increased from 1.6 to 1.9 kg/bed-day due to a rigorous process of segregation. The amount of Group I waste remained constant at about 1.9 kg/bed-day. As expected, a rigorous level of segregation at the point of generation reduces the amount of Group IV (wastes that under the law require incineration) and, at the same time, increases the amount of Group III (waste that presents biological risk). Thus, the information presented by the researchers in Portugal indicates that the quantity of wastes that require special treatment can be reduced from 10% to 2% by weight. However, according to Portuguese regulations, Group III wastes present some type of risk thus, to be able to compare the results of this work with those from developing countries, Groups III and IV wastes can be combined. As such, non-infectious wastes would amount to 1.9 kg/bed-day and infectious wastes would amount to 2.0 kg/bed-day. Consequently, the wastes that would require special treatment would amount to approximately 51% of the total waste stream.
Table 6. Daily Production of Medical Waste in Portugal (by type)
Groups I and II Group III Group IV Totals Practice (Kg/bed-day) (%) (Kg/bed-day) (%) (Kg/bed-day) (%) (Kg/bed-day)Usual practices 1.9 49 1.6 41 0.4 10 3.9
Rigorous segregation 1.9 49 1.9 49 0.08 2 3.9
2.1 61 1.3 37 0.08 2 3.5 Source: Alvim-Ferraz and Afonso, 2003. Group I: wastes similar to municipal wastes. Group II: non-hazardous medical wastes, no special treatment required. Group III: present biological risk, must be pretreated prior to disposal. Group IV: specific wastes, compulsory incineration.
In summary, the total amount of health care waste generated in selected hospitals in developing countries varied from 0.54 to 1.39 kg/bed-day. On the other hand, the reported amount of infectious (clinical, yellow bag) waste generated in these facilities varied from 0.30 to 0.34 kg/bed-day. The total quantity of wastes generated in a Portuguese hospital was reported to be about 3.9 kg/bed-day (1.9 kg/bed-day non-infectious and 2.0 kg/bed-day infectious). Consequently, the data show that the total amount of health care waste generated in a hospital in an industrialized country is approximately 2 to more than 7 times that generated in a

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 11
developing country. On the other hand, the percent of infectious waste of the total health care waste stream in developing countries was about 63%, versus 51% in industrialized countries.
Bulk Density Bulk density is defined as the space that a particular material occupies without any degree of compaction. Bulk density generally is reported as mass per unit of volume or kg/m3. In waste management, it is important to know the bulk density of the waste or components of the waste for a number of applications. Some of these include: determination of storage space, definition of size for the collection vehicle and estimation of the requirements for processing equipment (compaction, size reduction, disinfection, and others). The results of analyses conducted in Peru and in the Philippines to determine the bulk density of various types of health care wastes are presented in Tables 7 and 8. The data in Table 7 show that the bulk density for the entire waste stream ranged from 137 to 359 kg/m3 and the average was 218 kg/m3. The average bulk density for common (general) waste was 211 kg/m3, that for contaminated waste was 226 kg/m3 and that for special waste was 139 kg/m3. The results on analyses conducted in one hospital in Metro Manila presented in Table 8 show that the bulk density for non-infectious waste was 151 kg/m3, while that for infectious waste was 262 kg/m3.
Table 7. Bulk Density of Hospital Wastes by Type of Generator in Peru (kg/m3)
Hospital Total Waste Common Contaminated Special Jose Olavarria (Tumbes) 142 130 164 -
Docente (Trujillo) 137 121 155 -
Regional of Ica 261 220 273 550
Regional of Cusco 237 242 216 -
Daniel A. Carrion (Huancayo) 170 210 140 -
Regional of Loreto (Iquitos) 359 343 407 286
Average 218 211 226 139 Source: Ministerio de Salud, 1995.
Table 8. Bulk Density of Wastes Generated
by Hospitals in Metro Manila, Philippines
Type of Waste Bulk Density*
(kg/m3) Non-infectious 151
Infectious 262 Source: Asian Development Bank, 2003. * Moisture Content as received.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 12
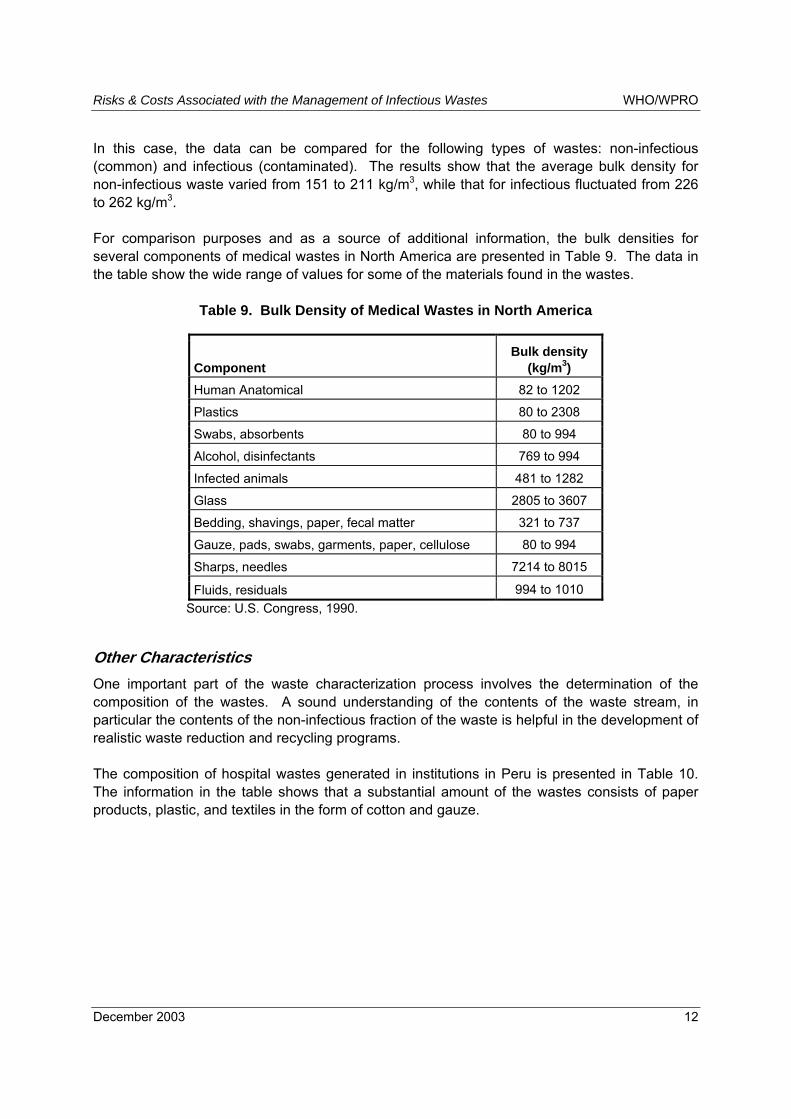
In this case, the data can be compared for the following types of wastes: non-infectious (common) and infectious (contaminated). The results show that the average bulk density for non-infectious waste varied from 151 to 211 kg/m3, while that for infectious fluctuated from 226 to 262 kg/m3. For comparison purposes and as a source of additional information, the bulk densities for several components of medical wastes in North America are presented in Table 9. The data in the table show the wide range of values for some of the materials found in the wastes.
Table 9. Bulk Density of Medical Wastes in North America
Component Bulk density
(kg/m3) Human Anatomical 82 to 1202
Plastics 80 to 2308
Swabs, absorbents 80 to 994
Alcohol, disinfectants 769 to 994
Infected animals 481 to 1282
Glass 2805 to 3607
Bedding, shavings, paper, fecal matter 321 to 737
Gauze, pads, swabs, garments, paper, cellulose 80 to 994
Sharps, needles 7214 to 8015
Fluids, residuals 994 to 1010 Source: U.S. Congress, 1990.
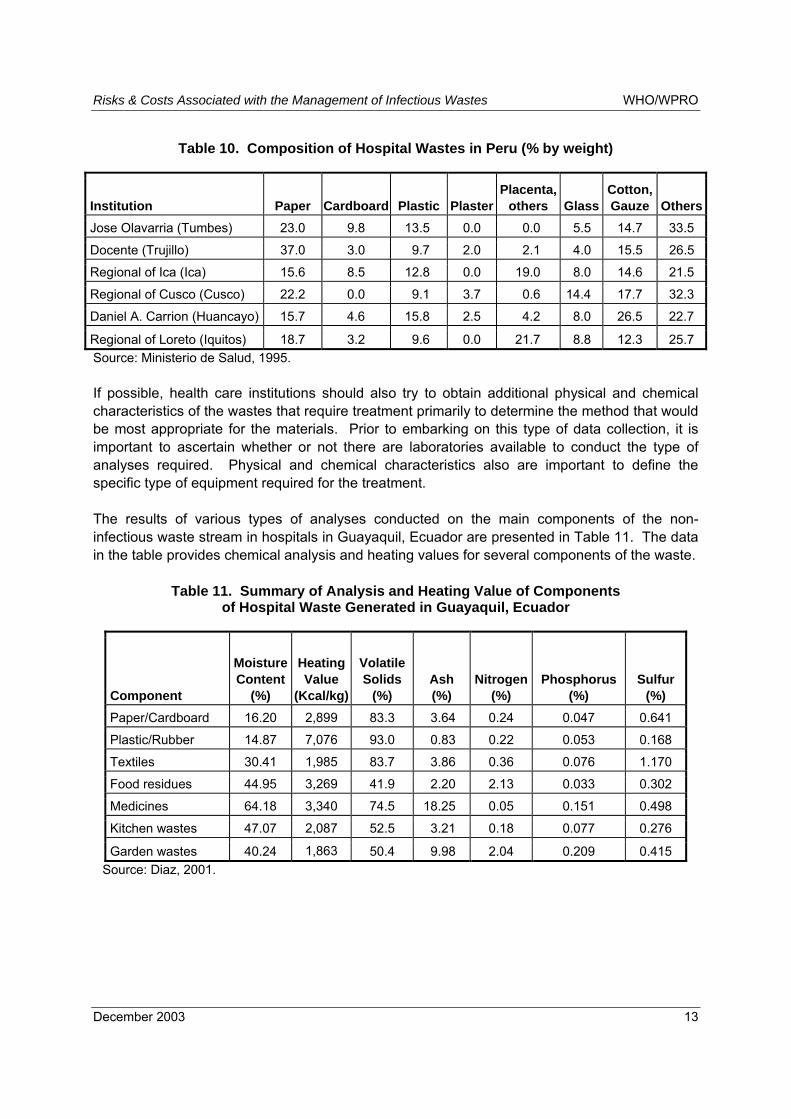
Other Characteristics One important part of the waste characterization process involves the determination of the composition of the wastes. A sound understanding of the contents of the waste stream, in particular the contents of the non-infectious fraction of the waste is helpful in the development of realistic waste reduction and recycling programs. The composition of hospital wastes generated in institutions in Peru is presented in Table 10. The information in the table shows that a substantial amount of the wastes consists of paper products, plastic, and textiles in the form of cotton and gauze.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 13
Table 10. Composition of Hospital Wastes in Peru (% by weight)
Institution Paper Cardboard Plastic PlasterPlacenta,
others Glass Cotton, Gauze Others
Jose Olavarria (Tumbes) 23.0 9.8 13.5 0.0 0.0 5.5 14.7 33.5
Docente (Trujillo) 37.0 3.0 9.7 2.0 2.1 4.0 15.5 26.5
Regional of Ica (Ica) 15.6 8.5 12.8 0.0 19.0 8.0 14.6 21.5
Regional of Cusco (Cusco) 22.2 0.0 9.1 3.7 0.6 14.4 17.7 32.3
Daniel A. Carrion (Huancayo) 15.7 4.6 15.8 2.5 4.2 8.0 26.5 22.7
Regional of Loreto (Iquitos) 18.7 3.2 9.6 0.0 21.7 8.8 12.3 25.7 Source: Ministerio de Salud, 1995. If possible, health care institutions should also try to obtain additional physical and chemical characteristics of the wastes that require treatment primarily to determine the method that would be most appropriate for the materials. Prior to embarking on this type of data collection, it is important to ascertain whether or not there are laboratories available to conduct the type of analyses required. Physical and chemical characteristics also are important to define the specific type of equipment required for the treatment. The results of various types of analyses conducted on the main components of the non-infectious waste stream in hospitals in Guayaquil, Ecuador are presented in Table 11. The data in the table provides chemical analysis and heating values for several components of the waste.
Table 11. Summary of Analysis and Heating Value of Components of Hospital Waste Generated in Guayaquil, Ecuador
Component
Moisture Content
(%)
Heating Value
(Kcal/kg)
Volatile Solids
(%) Ash (%)
Nitrogen (%)
Phosphorus (%)
Sulfur (%)
Paper/Cardboard 16.20 2,899 83.3 3.64 0.24 0.047 0.641
Plastic/Rubber 14.87 7,076 93.0 0.83 0.22 0.053 0.168
Textiles 30.41 1,985 83.7 3.86 0.36 0.076 1.170
Food residues 44.95 3,269 41.9 2.20 2.13 0.033 0.302
Medicines 64.18 3,340 74.5 18.25 0.05 0.151 0.498
Kitchen wastes 47.07 2,087 52.5 3.21 0.18 0.077 0.276
Garden wastes 40.24 1,863 50.4 9.98 2.04 0.209 0.415 Source: Diaz, 2001.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 14
Other physical-chemical characteristics for hospital wastes in São Paulo, Brazil (by type of generator) are presented in Table 12. The data in the table show the wide ranges in characteristics exhibited by the wastes. The moisture contents and heating values for several components of medical waste in North America are given in Table 13.
Table 12. Physical-Chemical Characteristics of Hospital Wastes by Type of Generator in São Paolo, Brazil
Point of Generation
Moisture Content (%)
Carbon (%)
Hydrogen (%)
Sulfur (%)
Volatile Solids (%)
LHV (Kcal/Kg)
HHV (Kcal/kg)
Chlorine (%)
Maternity 59.3 32.3 4.7 0.3 94.3 1589 4,990 0
Nursing 24.1 30.8 3.6 0 95.8 2858 4,236 0
Orthopedics 7.8 27.6 2.9 1.4 - - 3,826 0
Surgery 28.6 27.9 3.9 0.5 89.5 2417 3,893 0
Emergency 12.2 32 3.6 0.3 95.9 3463 4,303 0 Source: Ministerio de Salud, 1995. LHV: low heating value HHV: high heating value
Table 13. Moisture Content and Calorific Value of Medical Wastes in North America
Component Moisture Content
(wt %) Heating value
(kcal/kg) Human Anatomical 70 to 90 444 to 2000
Plastics 0 to 1 7700 to 11100
Swabs, absorbents 0 to 30 3100 to 6700
Alcohol, disinfectants 0 to 0.2 6100 to 7800
Infected animals 60 to 90 500 to 3600
Glass 0 0
Bedding, shavings, paper, fecal matter 10 to 50 2200 to 4500
Gauze, pads, swabs, garments, paper, cellulose 0 to 30 3100 to 6700
Sharps, needles 0 to 1 0 to 33
Fluids, residuals 80 to 100 0 to 1100 Source: U.S. Congress, 1990.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 15
Conclusions 1. The literature review points out the need to reach consensus on a worldwide basis on
the terms and characteristics used to describe the various types of wastes generated in health care facilities. One reason for resolving this shortcoming is that comparative analyses such as this one, as well as the exchange of information, are severely compromised by ill-defined and ambiguous terms. Without well-defined terms, major difficulties and misunderstandings are bound to occur when discussing and analyzing HCW characteristics. For example, the terms hospital waste, biological waste, clinical waste, yellow bag waste, and others seem to be used interchangeably among reviewed references.
2. Based on data reviewed and analyzed in this study, the range of total hospital waste generation varied from 0.54 to 1.39 kg/bed-day. On the other hand, the reported amount of infectious (clinical, yellow bag) waste varied from 0.30 to 0.34 kg/bed-day.
3. The percentage of total health care waste of the total amount of municipal solid waste generated is on the order of 0.72% (the range can be vary from 0.36% to 1.44%) whereas the percentage of infectious waste of the municipal solid waste generated is about 0.27% (similarly the range can fluctuate from about 0.14% to 0.54%).
4. Other characteristics of the components of the waste stream such as the bulk density and the calorific value have a substantial variability. This is probably due to the moisture contents of the waste.
Treatment/Disposal Methods Some of the most common treatment and disposal methods utilized in the management of infectious health care wastes in developing countries include:
• disposal on the ground (dumpsite, controlled landfill, pits, and sanitary landfill); • autoclave; • microwave; • chemical disinfection; and • combustion (low-technology, medium-technology and high-technology).
In addition, residues from immunization campaigns (primarily needles and syringes) generally are managed through the following options: burial in specific pits with a cover, encapsulation by means of immobilizing compounds (primarily cement and plastics), point-of-use needle destruction technologies, mechanical destruction (compaction or size reduction). The WHO strongly recommends that vaccination programs should incorporate the use of safety boxes or sharps containers for the temporary storage of used needles, syringes, and other sharps. These boxes generally consist of rectangular containers made out of materials that are impermeable and resistant to punctures. Used syringes, needles and other contaminated sharps should be placed in these boxes; once the boxes are approximately 75% full, they should be closed and stored in a secure location until the boxes and their contents can be properly treated or disposed. Ideally, safety boxes should only be filled once and destroyed. This report will only deal with �treatment and final disposal� methods.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 16
Land Disposal At the present time, the most common method of land disposal of solid wastes in developing countries is the open dump. Because of the uncontrolled nature of disposal, this method also is the least cost option, but at the same time, it is the one that causes the most negative impacts to the public and to the environment. Consequently, open dumping should be discontinued as soon as possible and in particular should not be used for the disposition of health care wastes. Open dumps, at the very least, should be upgraded to controlled landfills and eventually to sanitary landfills. A controlled landfill is a land disposal facility which: it is sited according to basic hydrogeological conditions, restricts access to the area by means of a fence, control scavenging, keeps waste discharges to a small working area, makes use of a soil cover on a regular basis, controls surface water and drainage, maintains basic records, manages the landfill gas, and applies a final cover and vegetation once filled. A sanitary landfill is an engineered waste disposal facility which, among other factors, includes in its design: sited in accordance with hydrological, geological, social, and other factors; should be lined with a natural or a synthetic layer of an impermeable material; leachate and landfill gas should be collected and properly managed; maintain groundwater monitoring wells; makes use of daily, intermediate and final covers; and provides a comprehensive closure and post-closure plan.
Burial in Special Pits Burial in special pits is particularly applicable to small health care facilities located in relatively isolated (rural) areas where the geological and hydrological conditions are suitable and the area is sparsely populated. Suitability primarily is dependent upon the amount of waste generated, the type of soil in the area, the distance to groundwater, and the distance to the nearest receptor. The pit should be about 2 to 3 meters deep and approximately 2 meters wide. If possible, the entire pit should be lined with a 30 cm layer of clay or any other suitable impermeable material. If sufficient quantities of the impermeable material are not readily available then only the bottom of the pit should be lined such that percolation of any liquids into the soil below is reduced to a minimum. The top portion of the pit should be slightly elevated and properly sloped to keep surface waters from entering the pit. Preferably, the pit should be covered with a simple, but sturdy removable cover. The pit should be built by persons that are knowledgeable in construction so that it is done efficiently and, most importantly, to prevent the sides from collapsing. The entire site should be properly fenced off to keep unauthorized personnel or animals from entering into the area. This type of pit may be used by relatively small health care facilities but may not be suitable for large-scale immunization campaigns due to the large number of used needles and syringes that would be produced. Once the pit is full, the top opening should be sealed with soil or with cement and the area clearly identified. A diagram of a pit is presented in Figure 2.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 17
Slope Slope
Removable Cover
2 m0.3 m
Waste
2 to 3 meters
at least 1.5 meters
Clay or OtherImpermeable Material
Groundwater Level
Figure 2. Schematic Diagram of a Pit
If sufficient funds are available, the pit should preferably be constructed entirely out of cement much like a septic tank including a solid cover as shown in Figure 3. The pit or vault can be built with a hinged, lockable cover for additional security.
Encapsulation Encapsulation is a procedure that has been widely used in the hazardous waste management business and it is a procedure that can be used for the treatment of sharps and more specifically hypodermic needles. In the process, the sharps are placed in containers. The containers can be made out of cardboard, plastic, or metal. The size of the containers varies from a fraction of a liter to about 100 liters. When the containers are almost full, a material known to immobilize the sharps is added. The most common immobilizing materials are cement, plastic foams, resins, and clay. Once the immobilizing material is dry or has hardened, the container should be properly sealed and disposed. Disposal can take place in a municipal disposal site or through onsite burial.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 18
Slope SlopeCover
2 meters
Waste
2 to 3 meters
at least 1.5 meters
Cement
Groundwater Level
Figure 3. Schematic Diagram of a Cement Pit (Vault)
Cement encapsulation can also be utilized for a large immunization campaigns either using large containers as described in the previous section by building a sufficiently large pit to accommodate the wastes (see Burial in Special Pits section). In this particular case, it is important to calculate the size of the pit or trench that will be required to hold the �volume� of needles and syringes produced. Ideally, the pit or trench should be built as described in the previous section and lined with an impermeable layer. The wastes should be carefully placed in the pit. If a flexible membrane is used to line the pit, then the sharps should be contained in boxes or similar containers to avoid punctures. Once the sharps are all in the pit, the cement mixture is added. For optimum results, the mixture should be prepared as follows:
• 1 part cement; • 1 part lime; • 4 parts sand; and • 1/2 part water.
A sufficient quantity of this mixture should be added to enclose the entire mass of waste in the pit. After the mixture has �set or hardened,� the pit should be covered with soil, properly contoured to reduce the amount of water infiltration and identified to denote the type of waste buried on the site. A schematic diagram of the process is presented in Figure 4.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 19
Slope Slope
2 to 3 meters
at least 1.5 meters
Groundwater Level
Final Cover
Cement
Figure 4. Schematic Diagram of Cement Encapsulation in a Special Pit
This process is relatively inexpensive, and uses a simple technology. In addition, encapsulation keeps personnel in the waste management system and scavengers at the disposal sites from being injured. No data have been found on the survival of microorganisms under encapsulation conditions. The specific location of land disposal sites should be accurately and clearly identified in maps for future reference.
Risks Associated with Land Disposal Risks posed by health care wastes (HCW) to operators of land disposal sites and other persons living or working on or near these types of sites are primarily those associated with solid, liquid, or gaseous emissions emanating from the raw waste or from its byproducts of decomposition, and those associated with pathogenic microorganisms. The type and rate of emissions and exposures are fundamentally a function of the characteristics of the waste, local meteorological and soil conditions, and of the design and methods of operation of the land disposal facility. In the case of open (uncontrolled) dumping, facility design generally is not an element of consideration, and methods of operation, if any, are crude at best. On the other hand, modern engineering design and operating methods are the key elements and basis of sanitary landfilling. HCW can be disposed on the land in essentially two ways: disposal of HCW-only or co-disposal of HCW, along with municipal solid waste (MSW) in the same disposal facility. Another term for disposal of HCW-only is �dedicated� HCW disposal. Land disposal of HCW can be performed

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 20
only using disposal facility designs similar to those used for MSW sanitary landfills, or for controlled landfills. As it was discussed in a previous section, another form of dedicated HCW disposal is the use of a pit or a vault. Vaults manufactured from concrete or steel could also be used to dispose HCW. These units would be fabricated of materials similar to those typically used for septic tanks. An analysis of the risks associated with land disposal of waste has to bear in mind the following particularity. Land disposal of waste can generate adverse risks to the environment or public health through two generic sources: 1) the waste itself, and 2) vehicles. In the case of incremental effects of HCW versus those of MSW disposal, the motor vehicle effects should be approximately similar on a unit mass disposed basis. However, in analyzing the sources of certain risks associated with land disposal of waste, sometimes the reported data do not allow a distinction to be made between the contribution of the waste and of the motor vehicles to the measured concentrations. Benzene, a common constituent found in landfill gas (LFG), is but one example of this situation. Benzene is present in the exhaust of internal combustion engines and in landfill gas, and both sources would contribute to concentrations of benzene measured outside of the boundary of the land disposal site. While much data have been collected on emissions from landfill facilities, scientific risk assessments of land disposal are few. In fact, only recently have methods of modern risk assessment been applied to land disposal of solid waste. Methods and procedures for analysis of risk and of required data for performing the analyses are only now beginning to be examined (Belgiorno, et al., 2003; Butt and Oduyemi, 2002). Most methods of modern risk assessment have been developed for hazardous (toxic) waste management or for incineration of solid waste.
Potential Impacts The substantial environmental and health and safety risks associated with uncontrolled (open) dumping of solid waste have been well established through many studies performed in developing countries. Based on prior studies, substantial percentages of scavengers (including children) at land disposal sites in Metro Manila and India were shown to have experienced a number of ailments. One study in Metro Manila examined 194 children �working� at an open dump (Smokey Mountain, Balut) in Metro Manila in 1991. Approximately 30% of the children were found to have skin rashes, hypopigmentation, fungal infections, or boils. In addition, about 18% of the children had lacerations and wounds. Approximately 31% of the children had bronchitis, 28.6% asthma, and 25.1% pneumonia. The results of the study also identified other medical ailments (Torres, et al., 1991). Another study, although less comprehensive than the one conducted by Torres, et al., was also carried out at the same site in 1981. The evaluation of children living and working on the site showed similar results to those found by Torres, et al., including a high incidence of parasitism (Adan, et al., 1982). A study in Calcutta, India found that approximately 70% of scavengers working at an open dump had respiratory diseases, as opposed to approximately 35% for a control population (Nath, et al., 1990).
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 21
Water Resources and Landfill Leachate
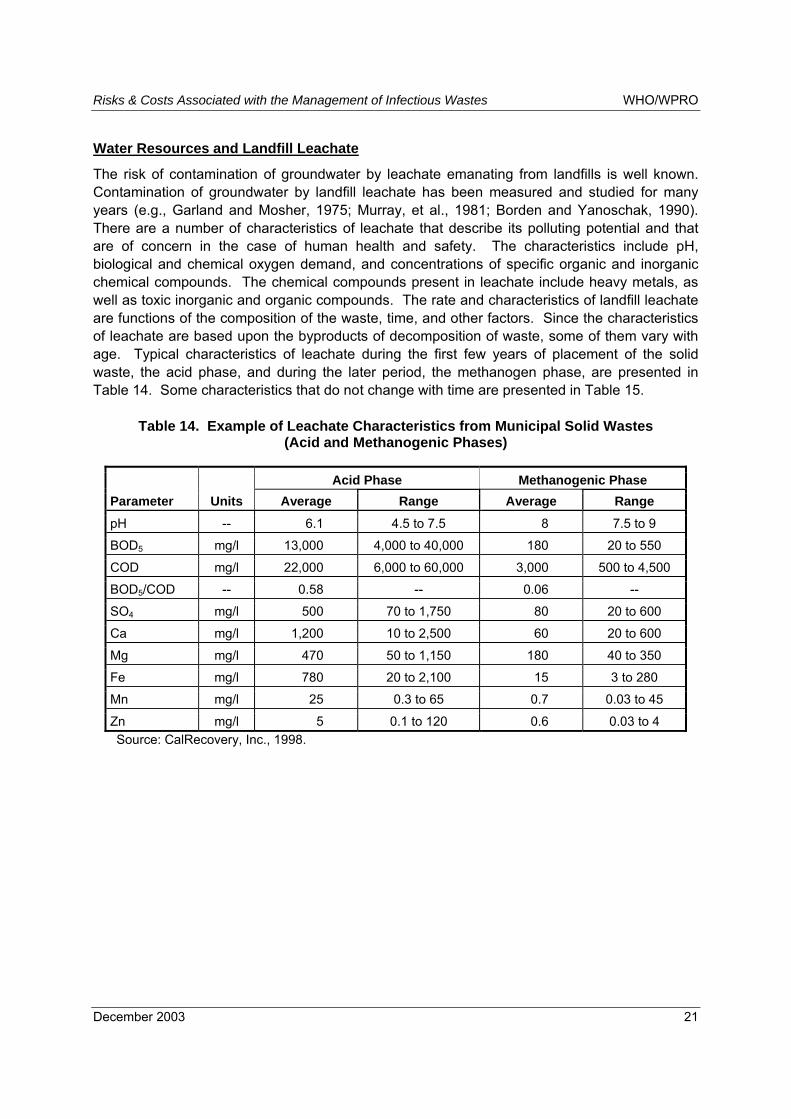
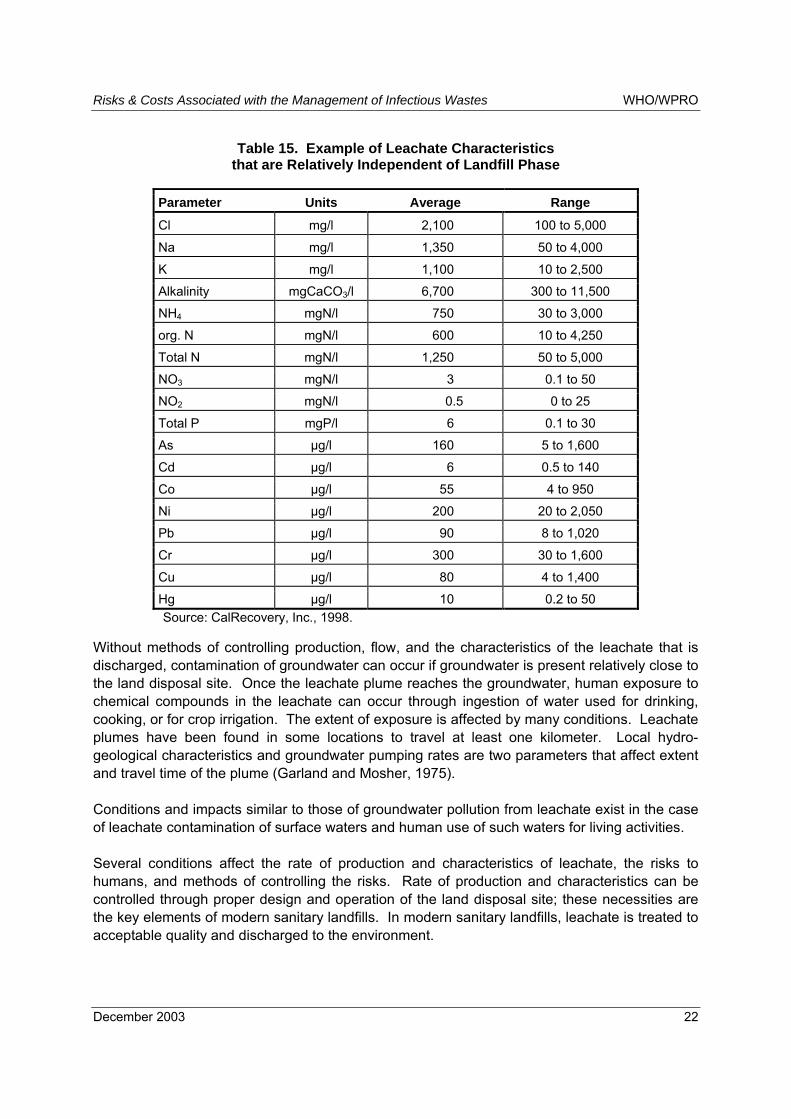
The risk of contamination of groundwater by leachate emanating from landfills is well known. Contamination of groundwater by landfill leachate has been measured and studied for many years (e.g., Garland and Mosher, 1975; Murray, et al., 1981; Borden and Yanoschak, 1990). There are a number of characteristics of leachate that describe its polluting potential and that are of concern in the case of human health and safety. The characteristics include pH, biological and chemical oxygen demand, and concentrations of specific organic and inorganic chemical compounds. The chemical compounds present in leachate include heavy metals, as well as toxic inorganic and organic compounds. The rate and characteristics of landfill leachate are functions of the composition of the waste, time, and other factors. Since the characteristics of leachate are based upon the byproducts of decomposition of waste, some of them vary with age. Typical characteristics of leachate during the first few years of placement of the solid waste, the acid phase, and during the later period, the methanogen phase, are presented in Table 14. Some characteristics that do not change with time are presented in Table 15.
Table 14. Example of Leachate Characteristics from Municipal Solid Wastes (Acid and Methanogenic Phases)
Acid Phase Methanogenic Phase Parameter Units Average Range Average Range pH -- 6.1 4.5 to 7.5 8 7.5 to 9
BOD5 mg/l 13,000 4,000 to 40,000 180 20 to 550
COD mg/l 22,000 6,000 to 60,000 3,000 500 to 4,500
BOD5/COD -- 0.58 -- 0.06 --
SO4 mg/l 500 70 to 1,750 80 20 to 600
Ca mg/l 1,200 10 to 2,500 60 20 to 600
Mg mg/l 470 50 to 1,150 180 40 to 350
Fe mg/l 780 20 to 2,100 15 3 to 280
Mn mg/l 25 0.3 to 65 0.7 0.03 to 45
Zn mg/l 5 0.1 to 120 0.6 0.03 to 4 Source: CalRecovery, Inc., 1998.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 22
Table 15. Example of Leachate Characteristics that are Relatively Independent of Landfill Phase
Parameter Units Average Range
Cl mg/l 2,100 100 to 5,000
Na mg/l 1,350 50 to 4,000
K mg/l 1,100 10 to 2,500
Alkalinity mgCaCO3/l 6,700 300 to 11,500
NH4 mgN/l 750 30 to 3,000
org. N mgN/l 600 10 to 4,250
Total N mgN/l 1,250 50 to 5,000
NO3 mgN/l 3 0.1 to 50
NO2 mgN/l 0.5 0 to 25
Total P mgP/l 6 0.1 to 30
As µg/l 160 5 to 1,600
Cd µg/l 6 0.5 to 140
Co µg/l 55 4 to 950
Ni µg/l 200 20 to 2,050
Pb µg/l 90 8 to 1,020
Cr µg/l 300 30 to 1,600
Cu µg/l 80 4 to 1,400
Hg µg/l 10 0.2 to 50 Source: CalRecovery, Inc., 1998.
Without methods of controlling production, flow, and the characteristics of the leachate that is discharged, contamination of groundwater can occur if groundwater is present relatively close to the land disposal site. Once the leachate plume reaches the groundwater, human exposure to chemical compounds in the leachate can occur through ingestion of water used for drinking, cooking, or for crop irrigation. The extent of exposure is affected by many conditions. Leachate plumes have been found in some locations to travel at least one kilometer. Local hydro-geological characteristics and groundwater pumping rates are two parameters that affect extent and travel time of the plume (Garland and Mosher, 1975). Conditions and impacts similar to those of groundwater pollution from leachate exist in the case of leachate contamination of surface waters and human use of such waters for living activities. Several conditions affect the rate of production and characteristics of leachate, the risks to humans, and methods of controlling the risks. Rate of production and characteristics can be controlled through proper design and operation of the land disposal site; these necessities are the key elements of modern sanitary landfills. In modern sanitary landfills, leachate is treated to acceptable quality and discharged to the environment.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 23
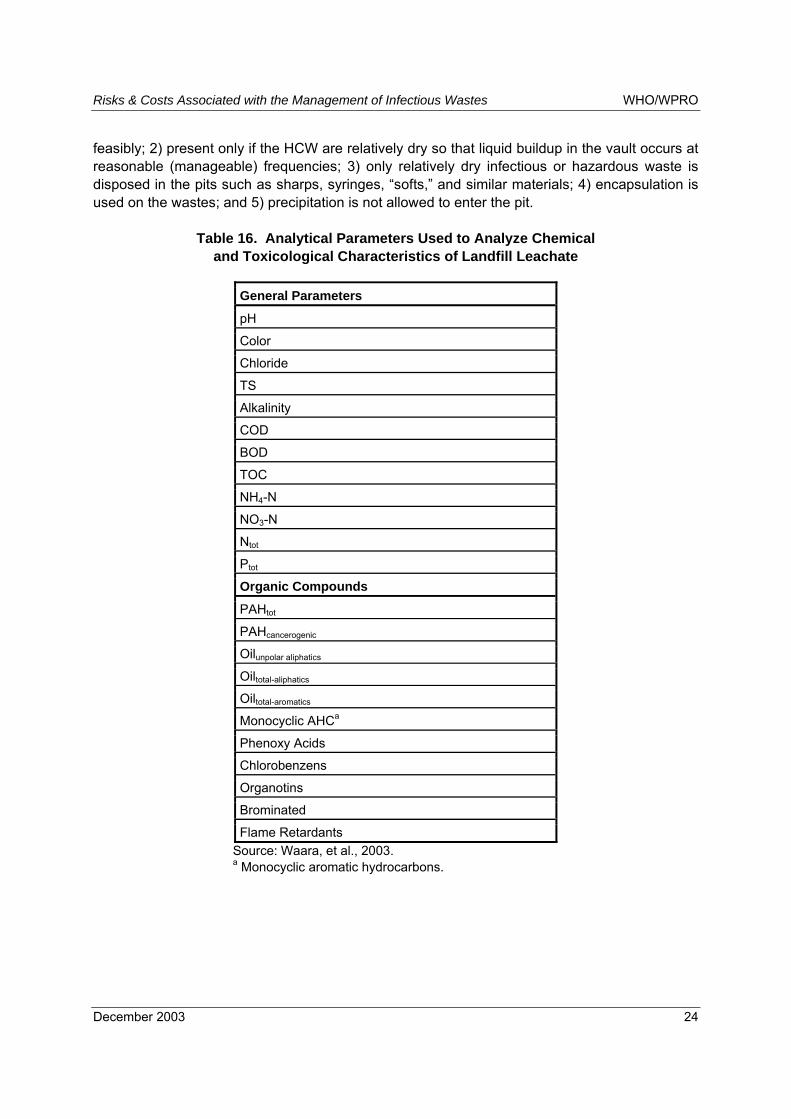
Some analyses and risks assessments have been performed on landfill leachates. Several studies have indicated that raw leachates contain a variety of toxic chemical compounds (Khare and Dondero, 1977; Barker, 1987; Först, et al., 1989) and have a high toxicity (Clément and Merlin, 1995; Öman, et al., 2000; Kjeldsen, et al., 2002; Marttininen, et al., 2002). Other studies have shown that measurable concentrations of xenobiotics are found in landfill leachates and that they can have a negative effect on the environment (Kjeldsen, et al., 2002; Öman, et al., 2000). Carcinogenic PAHs have been reported in landfill leachate (Kamiya, et al., 1989). One study examined the chemical and toxicological characteristics of two different types of landfill leachate, both before and after various types of treatment (Waara, et al., 2003). Thus, some insight on the effect of treatment on leachate toxicity can be gained from this study. The list of generic analytical parameters monitored during the study is presented in Table 16. Chemical concentrations, and several methods of determining acute toxicity and hormonal effects were used to characterize the toxicology of the leachates. In the case of raw (untreated) leachates, concentrations above the Canadian environmental quality guidelines for freshwater and maximum permissible concentrations for freshwater (based on regulations of The Netherlands) were measured for four specific species in the PAH family, chlorobenzene, and one specific specie of the phenoxy acid group. Measurable estrogenic and androgenic effects were obtained for both types of raw leachate. Biological treatment of the leachates was found to dramatically reduce the acute toxicity and estrogenic effects of the leachates. The results of the analyses indicated that the reduction of the androgenic effect might require both biological treatment and ozonation and carbon filtering, depending on the specific leachate characteristics. The concentrations of oil, PAH, monocyclic aromatics, phenoxyacids, and chlorobenzene organic compounds were effectively decreased with biological treatment. As indicated in the preceding paragraphs, the potential of pollution of water resources and risk to humans increases with a reduction of the degree of control exercised over a land disposal operation. The risks are greatest to human communities in the case of no exercise of control, i.e., open dumping, and where local hydro-geological conditions and distance to human populations are such that exposure to agents in leachate is likely. Dedicated disposal only of HCW, in a pit, a vault, or similar structure, would result in higher concentrations of pathogens, pharmaceuticals, and perhaps of liquids than if HCW were co-disposed with MSW. The higher concentration of dangerous materials and of water represents a greater risk to workers and potential of generation of liquid and gaseous emissions than in the case of co-disposal. The review of leachate data and risk factors has already established the toxicity and hormonal effects of raw leachate from MSW. These effects would likely be substantially accentuated in the case of dedicated land disposal of HCW. At some point, accumulation of liquid would exceed the capacity of the disposal volume, and thus would require that the liquid be collected and removed. The raw leachate would have high concentrations of the constituents previously discussed and, if not treated, would represent a substantial risk to the environment, the public, or both. Also, the higher constituent concentrations in the leachate from this method of disposal would translate to increased risk to the health and safety of operators of the disposal system. An advantage of an enclosed and covered disposal structure, such as a pit or vault, is the barrier to precipitation that would not exist in the case of a site for disposal of MSW. However, the extent of this advantage in the practical sense is: 1) limited to situations producing a relatively small amount of HCW so that below-surface vaults can be used
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 24
feasibly; 2) present only if the HCW are relatively dry so that liquid buildup in the vault occurs at reasonable (manageable) frequencies; 3) only relatively dry infectious or hazardous waste is disposed in the pits such as sharps, syringes, �softs,� and similar materials; 4) encapsulation is used on the wastes; and 5) precipitation is not allowed to enter the pit.
Table 16. Analytical Parameters Used to Analyze Chemical and Toxicological Characteristics of Landfill Leachate
General Parameters pH
Color
Chloride
TS
Alkalinity
COD
BOD
TOC
NH4-N
NO3-N
Ntot
Ptot
Organic Compounds
PAHtot
PAHcancerogenic
Oilunpolar aliphatics
Oiltotal-aliphatics
Oiltotal-aromatics
Monocyclic AHCa
Phenoxy Acids
Chlorobenzens
Organotins
Brominated
Flame Retardants Source: Waara, et al., 2003. a Monocyclic aromatic hydrocarbons.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 25
Air Quality and Airborne Landfill Emissions
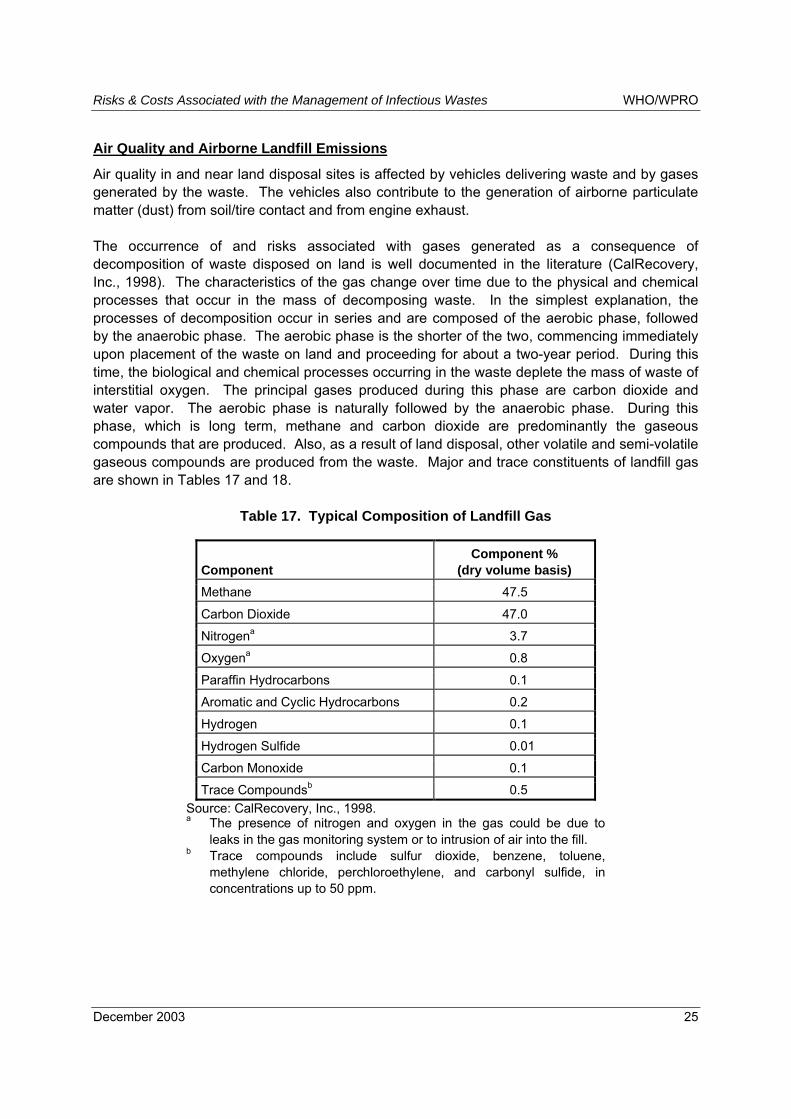
Air quality in and near land disposal sites is affected by vehicles delivering waste and by gases generated by the waste. The vehicles also contribute to the generation of airborne particulate matter (dust) from soil/tire contact and from engine exhaust. The occurrence of and risks associated with gases generated as a consequence of decomposition of waste disposed on land is well documented in the literature (CalRecovery, Inc., 1998). The characteristics of the gas change over time due to the physical and chemical processes that occur in the mass of decomposing waste. In the simplest explanation, the processes of decomposition occur in series and are composed of the aerobic phase, followed by the anaerobic phase. The aerobic phase is the shorter of the two, commencing immediately upon placement of the waste on land and proceeding for about a two-year period. During this time, the biological and chemical processes occurring in the waste deplete the mass of waste of interstitial oxygen. The principal gases produced during this phase are carbon dioxide and water vapor. The aerobic phase is naturally followed by the anaerobic phase. During this phase, which is long term, methane and carbon dioxide are predominantly the gaseous compounds that are produced. Also, as a result of land disposal, other volatile and semi-volatile gaseous compounds are produced from the waste. Major and trace constituents of landfill gas are shown in Tables 17 and 18.
Table 17. Typical Composition of Landfill Gas
Component Component %
(dry volume basis) Methane 47.5
Carbon Dioxide 47.0
Nitrogena 3.7
Oxygena 0.8
Paraffin Hydrocarbons 0.1
Aromatic and Cyclic Hydrocarbons 0.2
Hydrogen 0.1
Hydrogen Sulfide 0.01
Carbon Monoxide 0.1
Trace Compoundsb 0.5 Source: CalRecovery, Inc., 1998. a The presence of nitrogen and oxygen in the gas could be due to
leaks in the gas monitoring system or to intrusion of air into the fill. b Trace compounds include sulfur dioxide, benzene, toluene,
methylene chloride, perchloroethylene, and carbonyl sulfide, in concentrations up to 50 ppm.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 26
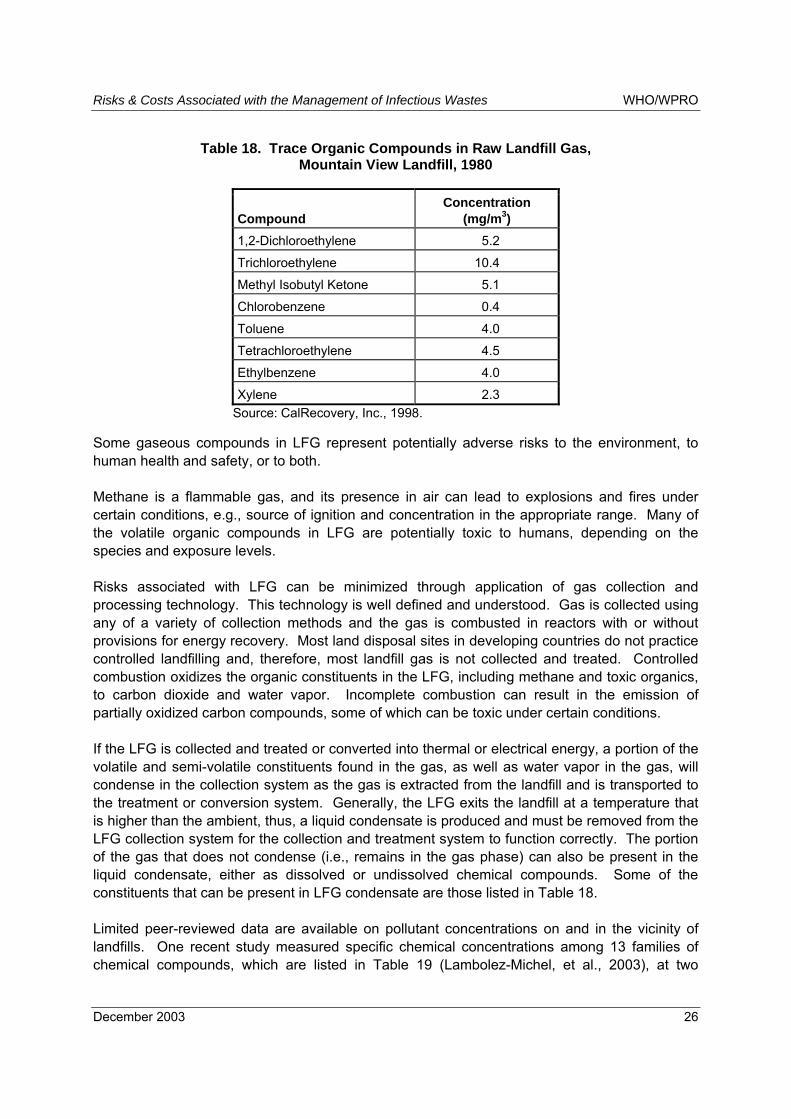
Table 18. Trace Organic Compounds in Raw Landfill Gas, Mountain View Landfill, 1980
Compound Concentration
(mg/m3) 1,2-Dichloroethylene 5.2
Trichloroethylene 10.4
Methyl Isobutyl Ketone 5.1
Chlorobenzene 0.4
Toluene 4.0
Tetrachloroethylene 4.5
Ethylbenzene 4.0
Xylene 2.3 Source: CalRecovery, Inc., 1998.
Some gaseous compounds in LFG represent potentially adverse risks to the environment, to human health and safety, or to both. Methane is a flammable gas, and its presence in air can lead to explosions and fires under certain conditions, e.g., source of ignition and concentration in the appropriate range. Many of the volatile organic compounds in LFG are potentially toxic to humans, depending on the species and exposure levels. Risks associated with LFG can be minimized through application of gas collection and processing technology. This technology is well defined and understood. Gas is collected using any of a variety of collection methods and the gas is combusted in reactors with or without provisions for energy recovery. Most land disposal sites in developing countries do not practice controlled landfilling and, therefore, most landfill gas is not collected and treated. Controlled combustion oxidizes the organic constituents in the LFG, including methane and toxic organics, to carbon dioxide and water vapor. Incomplete combustion can result in the emission of partially oxidized carbon compounds, some of which can be toxic under certain conditions. If the LFG is collected and treated or converted into thermal or electrical energy, a portion of the volatile and semi-volatile constituents found in the gas, as well as water vapor in the gas, will condense in the collection system as the gas is extracted from the landfill and is transported to the treatment or conversion system. Generally, the LFG exits the landfill at a temperature that is higher than the ambient, thus, a liquid condensate is produced and must be removed from the LFG collection system for the collection and treatment system to function correctly. The portion of the gas that does not condense (i.e., remains in the gas phase) can also be present in the liquid condensate, either as dissolved or undissolved chemical compounds. Some of the constituents that can be present in LFG condensate are those listed in Table 18. Limited peer-reviewed data are available on pollutant concentrations on and in the vicinity of landfills. One recent study measured specific chemical concentrations among 13 families of chemical compounds, which are listed in Table 19 (Lambolez-Michel, et al., 2003), at two

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 27
controlled landfills in France that comply with the latest regulations associated with collection and treatment of leachate and LFG. The study found that the measured concentrations of chemical pollutants in the air at the two sites were low and below threshold values. On the other hand, airborne dust and microorganisms were present in sufficient concentrations to warrant concern with regard to causing respiratory and immuno-allergic disorders among personnel on the site. Concentrations of dust and microorganisms measured beyond the boundary of the landfill sites were below levels judged to represent a significant health risk outside of the landfill site. The sources of the airborne pollutants were composed of both vehicular sources and land disposed waste.
Table 19. List of Chemical Compounds Monitored in Ambient Air in the Vicinity of Landfills
Family of Compounds Pollutants Toxicity Criteria
1 Monocyclic aromatic hydrocarbons (such as BTEX, etc.)
Neurotoxicity � Carcinogenicity of benzene
2 Ketonex, aldehydes, alcohols Irritants � Neurotoxicity � Carcinogenicity of formaldehyde
3 Cyclic hydrocarbons, phenols, Halogen compounds
Neurotoxicity � Potential carcinogenicity of tri- and tetrachloroethylene
4 Polycyclic aromatic hydrocarbons Diesel emission tracers � Carcinogenicity of certain polycyclic aromatic hydrocarbons
5 Organic sulphur compounds (mercaptans)
Irritants
6 Mineral and organic acids (HCI, HF) Irritants
7 Phtalates Potential carcinogenicity
8 H2S, NH3 Acute toxicity
9 CO, CO2, and O3 Irritant � Acute toxicity
10 NO2, Nox, and Sox Chronic respiratory toxicity
11 Gaseous and particulate metals: As, Pb, Mn, Cd, Ni, Cr
Systemic toxicity, including neurotoxicity � Carcinogenicity of Cd, Cr, and Ni
12 Total (Ǿ 0.5 � 20 µm) and alveolar (Ǿ 0.5 � 5 µm) dust
Inhalable dust
13 Asbestos Carcinogenicity Source: Lambolez-Michel, et al., 2003.
Soil and Soil Contamination
Chemical constituents and microorganisms present in solid waste or HCW can be transported from a land disposal site to the soil through a variety of transport processes unless control measures are purposely exercised. Natural mechanisms in some soils can somewhat attenuate migration of certain, but by no means all, contaminants generated by land disposal of waste. However, high levels of control of migration require modern engineering designs of land
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 28
disposal facilities and properly operated systems. Contamination of soils by heavy metals, volatile and semi-volatile organic compounds, and other pollutants as a consequence of insufficiently controlled waste disposal has occurred in the past in many industrialized and economically developing countries. High concentrations of toxic or otherwise undesirable pollutants in soils have several potentially severe adverse consequences; among them are included phytotoxicity and human toxicity.
Pathogens and Pathogen Transport
The fate of pathogens in land disposal sites has been the subject of several evaluations. Some investigators have found high survival rates for fecal coliforms and streptococci in residential or hospital waste that had been removed from lysimeters after nine years (Donnelly, et al., 1982). The same study found that pathogenic indicator microorganisms survived after nine years in a solid waste landfill (Pahren, 1987). Data regarding landfill leachate (Cooper, et al., 1974) and compost leachate (Diaz, et al., 1977) indicate that up to twelve months might be required for concentrations of total coliforms, fecal coliforms, and fecal streptococci to reach satisfactorily low levels. Thus, disease microorganisms apparently are present in land disposal sites after years of being on the site, as well as at the time of delivery of HCW to the disposal site. Thus, some pathogens may be available for dispersion into the environment outside of the disposal site via airborne or liquid transport mechanisms. However, at least two studies found that the mobility of pathogenic microorganisms in soils was limited due to the processes of ion-exchange, adsorption, and for other mechanisms (Aulenbach, et al., 1974; Ware, 1980). Other analyses and compilations of research results have shown that pathogen movement through soils to groundwater is inversely proportional to particle size of the soil and that various types of soil can absorb over 99% of viruses (Lance, 1977). Additionally, the results of several studies indicate that the probability is very low for migration of disease microorganisms for a properly designed and operated sanitary landfill (Ware, 1980; U.S. Congress, 1989; Turnberg, 1988). There is a lack of information available in the literature related to the degree of survival, proliferation, and viability of different types of pathogenic microorganisms in solid waste and solid waste leachate. Environmental conditions within solid waste, HCW, or a mixture of the two would seem to govern against substantial proliferation of pathogenic microorganisms once the host was sufficiently decomposed. The environment within decomposing waste heavily favors the proliferation of non-pathogenic microorganisms at the expense of the proliferation of pathogenic species. Containment of microorganisms within the disposal site minimizes opportunities and routes of exposures of whatever concentrations of pathogens that may be present regardless of time since initial placement. Systems designed and operated to control transport of microorganisms at land disposal facilities reduce the risk of both occupational and public exposure to pathogens. Control strategies include covering of wastes immediately upon delivery, particulate control (such as dust suppression), leachate collection and treatment systems, and adequate distance between the land disposal operations and human receptors. Sanitary landfills have many of these types of controls, controlled land disposal areas have less rigorous controls, and open dumps have no controls at all.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 29
Microwave Disinfection Systems Microwaves are very short waves in the electromagnetic spectrum and are within the range of the radio frequency band. Microwaves have wavelengths in the centimeter range and fall below the range for infrared waves and above the ultra-high frequency waves used for television. Microwaves are generated by means of klystrons, magnetrons, and traveling wave oscillators. These units convert electrical energy into microwave energy. The microwaves are then guided into a metallic channel known as the �wave guide.� The guide focuses the microwaves into a particular location. Microwaves cycle very quickly between positive and negative at an extremely high frequency (around 2.4 billion times per second). The high frequency makes the molecules in the receiving body (liquid or solid) vibrate very rapidly as they attempt to align to the changing electromagnetic field. The very high level of vibration results in friction. The friction generates substantial amounts of heat. It has been demonstrated that disinfection in the microwave units is not a result of the microwaves. The steam produced from the moisture in the waste by the microwave energy brings about the destruction of the pathogenic organisms in the waste. Consequently, typically microwave systems in the health care waste sector require the addition of water (or steam) into the waste during the treatment process.
Typical Microwave Disinfection System Microwave disinfection systems consist of three major types of equipment: 1) material handling equipment, 2) the disinfection process itself, and 3) environmental control equipment. The disinfection area or enclosure includes a hermetically enclosed chamber where the materials to be treated are placed and into which the microwaves from the magnetron are focused. Microwave systems are designed and built in a variety of sizes ranging from a few kg per hour to more than 400 kg per hour. The units can be operated as a batch process or in a semi-continuous mode. Large-scale systems can have from 1 to 6 microwave generators (magnetrons). Generally, each magnetron has a power output on the order of 1.2 kW. A flow diagram showing a typical large-scale system is presented in Figure 5. As shown in the figure, the waste to be treated is placed in carts and transported to the treatment facility. The carts are lifted by a hydraulic mechanism, a gate that seals the hopper opens, and the waste is discharged into the hopper. As the waste is introduced into the hopper, steam is injected into the hopper and air is extracted from the unit. All extracted air is passed through a high efficiency particulate air (HEPA) filter. The waste in the hopper is forced into a shredder. The shredded waste is transported via a rotating screw, exposed to steam, and then heated to between 95°C and 100°C by means of microwaves. The treated waste may be passed through a secondary shredder to achieve a higher degree of particle size reduction than with only one shredder. Secondary size reduction is particularly important in the event that sharps are part of the waste stream.
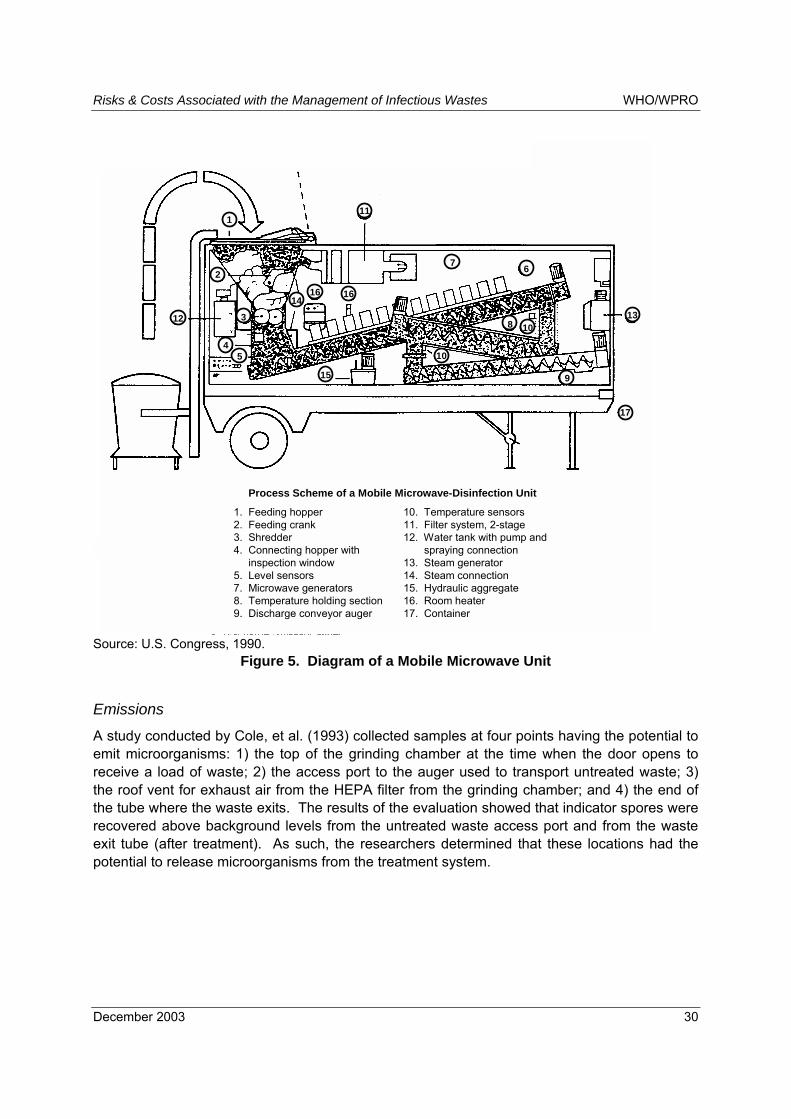
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 30
Process Scheme of a Mobile Microwave-Disinfection Unit
1. Feeding hopper 10. Temperature sensors2. Feeding crank 11. Filter system, 2-stage3. Shredder 12. Water tank with pump and 4. Connecting hopper with spraying connection
inspection window 13. Steam generator5. Level sensors 14. Steam connection7. Microwave generators 15. Hydraulic aggregate8. Temperature holding section 16. Room heater9. Discharge conveyor auger 17. Container
1
2
3
45
67
8
9
10
11
12 1314
15
16
17
16
10
Source: U.S. Congress, 1990.
Figure 5. Diagram of a Mobile Microwave Unit
Emissions A study conducted by Cole, et al. (1993) collected samples at four points having the potential to emit microorganisms: 1) the top of the grinding chamber at the time when the door opens to receive a load of waste; 2) the access port to the auger used to transport untreated waste; 3) the roof vent for exhaust air from the HEPA filter from the grinding chamber; and 4) the end of the tube where the waste exits. The results of the evaluation showed that indicator spores were recovered above background levels from the untreated waste access port and from the waste exit tube (after treatment). As such, the researchers determined that these locations had the potential to release microorganisms from the treatment system.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 31
Autoclaves The utility of heat, in particular, moist heat in achieving disinfection has been known for decades. Health care facilities have been using steam for disinfecting reusable instruments for a very long time. There are two basic types of units that utilize mainly steam for disinfecting health care wastes: autoclaves and retorts. Both of these units require a supply of steam. The steam is generated by means of a boiler. The boiler can be one used for other services in the health care facility or it can be one specifically for the treatment of the wastes (a �dedicated boiler�). Before we begin a description of autoclaves and retorts, a brief explanation of steam generation, and other parameters important in the field of steam production and heat transfer is given so that the readers can get a general appreciation of the entire process. As liquids are heated, their temperature increase until the temperature reaches what is known as its boiling point. The temperature at which a liquid boils or, in this particular case, when water is turned into steam is called the saturation temperature. The saturation temperature of liquids is impacted by pressure, as the pressure increases, the saturation temperature also increases. At standard atmospheric pressure (100 kPa or 14.7 psia), the saturation temperature of water is 100°C (212°F). The steam that is produced at saturation temperature is known as saturated steam (these parameters at these conditions also are known as standard temperature and pressure, or STP). In practice, steam is produced in a piece of equipment called a boiler. Usually boilers are heated by means of conventional fuels such as gas, diesel, coal, or biomass. Some boilers have also been designed to use electricity for heating the water and even waste oil. The use of waste oil as fuel must use specialized burners and must be carefully monitored to avoid substantial air emissions. Furthermore, some countries may require special permits to use waste oil as fuel. For safety reasons, the boilers must be designed and built under careful design parameters. Since the contents of the boiler, particularly industrial-size units, generally are under high temperatures and pressures, the design parameters must take under consideration a number of safety issues. These design parameters have been widely accepted by several countries. To achieve optimum operation and maximum efficiency, the input water must be properly treated to reduce the build up of salts and other compounds on the surfaces of the boiler and thus reducing the boiler�s ability to transfer heat. Steam boilers are rated in horsepower, BTUs or Kw. A boiler must be properly selected such that its output (the amount and quality of the steam) will match the requirements of the particular application (in this case the autoclave or retort). Autoclave: An autoclave essentially is a metal vessel (usually made out of steel). The vessel is hermetically sealed with a hinged door (with gaskets) and designed to resist high temperatures and pressures. Normally a steam jacket surrounds the vessel. The steam jacket is incorporated into the design to reduce the amount of condensation on the inside wall of the vessel and thus reduce heat loss. Disinfection in an autoclave is carried out in batches. That is, the unit is loaded, disinfection carried out and then the contents are removed from the unit. The entire process from loading to unloading is called a cycle. During a typical operation of an autoclave, the material to be

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 32
disinfected is loaded into the unit and air is evacuated. Air is removed from the interior of the vessel because of the air�s insulating characteristics (i.e., if not removed then heat transfer to the waste would be reduced and thus increasing the amount of fuel required). Air generally is removed from the autoclave by using a vacuum pump at the beginning of the cycle and prior to steam injection (these units are called high-vacuum) or by relying on the fact that air is more dense than steam such that as the steam is injected into the vessel, the air has the tendency to migrate to the bottom. The air at the bottom of the vessel is removed via a drain port. The high-vacuum method is the most effective and fastest of the two. Speed in this process is important as it reduces the overall time required per cycle. The air evacuated from the vessel should be properly treated. Steam is injected into both the interior of the vessel as well as into the steam jacket. A schematic diagram of a boiler is shown in Figure 6.
Source: U.S. Congress, 1990.
Figure 6. Diagram of an Autoclave
Retort: This particular type of disinfection unit is similar in design as the autoclave. The major difference between the two is that the design of the retort does not incorporate a steam jacket. The absence of a steam jacket results in inefficiencies in heat transfer and consequently higher temperatures are required for a retort than are required for an autoclave. Retorts normally are utilized in large-scale operations.
Other Considerations In the overall waste management process in a health care facility, the waste to be treated typically is stored in plastic bags (placed inside rigid containers). The bags are collected in carts or in bins previously lined with special plastic sheeting to prevent the bags from adhering to the carts when heated. The bags should also be made of a particular type of plastic that is resistant to the high temperatures inside the autoclave and at the same time be permeable to the steam in the direction towards the waste (i.e., allow the steam to penetrate the bag and go through into

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 33
the waste). At the beginning of the cycle, steam is introduced into the outer jacket of the autoclave (this step is known as �pre-heating�). The loaded bins or carts are introduced into the autoclave and the door is sealed. At this point air is evacuated from the unit either by vacuum or by introducing steam into the vessel. Steam is forced into the unit until the required temperature is achieved. Steam is added as necessary in order to maintain a set temperature for a given period of time. In some countries or states, it is necessary to record the time-temperature history for each load undergoing treatment. This generally is accomplished by means of a chart recorder. Upon reaching the necessary time-temperature requirements, vents in the unit are opened and the steam is released through a condenser (so the water can be re-used). Once the waste has reached ambient temperatures or it is cool enough to be handled, the material is removed and taken to the disposal site or treated mechanically. Mechanical treatment generally involves size reduction, compaction, or both. From time to time, either biological or chemical indicators are inserted in waste loads to evaluate the degree of disinfection.
Types of HCW that Can be Treated Autoclaves generally are used to treat the following types of materials:
• sharps; • cultures; • items contaminated with blood; • residues from surgery and from isolation wards; • bandages, gauze, linen, gowns, and other similar materials also known as �softs�; and • non-chemical laboratory wastes.
In some especial circumstances, it is technically possible to disinfect body parts. However, in the case of items with a large mass, care must be taken to achieve the necessary time-temperature relationships. In addition, any time body parts are treated in an autoclave one must deal with cultural, ethical, legal, and other factors that would impact this procedure.
Types of HCW that Should Not be Treated Health care facilities produce a variety of chemical and hazardous substances that should not be treated in an autoclave. These types of wastes include: wastes from chemotherapy treatment, mercury, volatile and semi-volatile organic compounds, radioactive wastes, and other hazardous chemical wastes. In general, it is not advisable to treat large body parts, animal carcasses, or other large items that, because of their mass and other characteristics, make it difficult or time consuming for the entire material to reach the prescribed temperatures.
Solid Residues from the Process Waste materials that are treated in an autoclave do not change considerably from their original state. Waste that is treated in an autoclave would look essentially the same as it did prior to the treatment. In fact, due to the addition of water and depending upon the type of unit, the mass of

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 34
the waste may increase. Consequently, in order to meet local regulations, some manufacturers incorporate into their systems some type of mechanical processing and most commonly size reduction, compaction or both. Size reduction essentially changes the appearance of the waste and increases the bulk density of the mixture thereby reducing the volume that the mass would occupy by 60% to 80%.
Liquid and Gaseous Emissions from the Process In addition to the treated solid matter, a typical autoclave would release liquid and gaseous discharges. A limited number of analyses have been conducted on the gaseous and liquid emissions from autoclaves in the recent past. A study was conducted by the U.S. National Institute of Occupational Safety and Health in 1997 (NIOSH, 1997). The study was conducted in a facility that used an autoclave. The results of the study indicated that volatile organic compounds (VOCs) found in the work area or in the worker�s personal air space did not exceed the limits set forth by the U.S. Occupational Safety and Health Administration. In addition, the study reported that the highest concentration of VOC in the facility was 643 mg of 2-propanol/m3. Cole and co-workers conducted research work using indicator organisms (Bacillus stearothermophilus and Bacillus subtillis var. niger) and using onsite hospital laboratory medical waste treatment gravity displacement autoclaves and a large commercial vacuum autoclave (Cole, et al., 1993). Sampling was carried out from air and fluids exhausted from the chamber before, during, and after treatment conditions. In addition, sampling was conducted from the plume exiting the chamber as the door was opened. The results of the evaluation indicated that no indicator organisms were recovered above background levels from any of the sampling points. In particular, no indicators were recovered from the initial exhausting and pressurization phase of the chamber. Initially this phase of the operation was considered to offer the greatest potential for emissions of microorganisms. A comparison of the cancer risks from three autoclave facilities with those from an incinerator is presented in Table 20. In addition, the emissions from a steam device are compared to those of an incinerator in Table 21. The data in the table show that depending upon the composition of the waste to be treated, the emissions will be in the gaseous form or in the solid form.
Chemical Disinfection Chemical disinfectants have been utilized in the health care sector for a long time. Disinfectants have been used in a variety of applications from preparing a particular area in the body prior to an injection to cleaning a variety of surfaces in the working areas. Chemical disinfection has also been applied to the treatment of health care wastes. In this particular section, we will examine the various options available for the treatment of health care wastes. Chemical disinfection relies on the particular properties of the chemical agent to inactivate pathological organisms. The effectiveness of a certain chemical agent depends upon temperature, pH, and on the possible presence of other compounds, which can have a negative

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 35
impact on the effectiveness of the compound. Any or all of these factors play a role on the ability of the chemical to act on the cells of the particular microorganism. Furthermore, it has been determined that some microorganisms are more resistant to chemical treatment than others. The most resistant microorganisms to chemical treatment include: bacterial spores and hydrophilic viruses. On the other hand, some of the least resistant to chemical treatment include: fungal spores and vegetative bacteria.
Table 20. Comparison of Cancer Risks from Three Autoclave Facilities
Inhalation Cancer Risk (chances/million) Pollutant Incinerator Autoclave
Mercury 0.07
Beryllium 0.04 < 0.01
Cadmium 0.14 < 0.01
Chromium IV < 0.01
Nickel 0.04
Benzene 0.17 < 0.01
Dioxin T.E. 0.29
Acetaldehyde 0.19
Formaldehyde 0.13
Chloroform 0.12
Perchloroethylene 0.01
Totals 0.75 0.48 Source: Jones and Konheim, 1994.
Table 21. Comparison of Emissions between an Incinerator and a Steam Device
Pollutants Incinerator (kg/year)
Steam Device (kg/year)
In Ash/Steamed Waste
Cadmium 0.03 0.09
Lead 8.18 189.54
Mercury 0.61 15.91
In Air Emission
Cadmium BDL 0.28
Lead 0.10 1.11
Mercury 0.29 1.86 Source: Olson, 1995. BDL = Below detection limit.
Antimicrobial agents act at the cellular and at the molecular levels. At the cellular level, these agents can damage the cell wall or the membrane of the cell. On the other hand, at the

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 36
molecular level, antimicrobial agents can alter protein and DNA synthesis or cause inhibition through enzymatic reactions. Chemical methods of microbial control include antiseptics and disinfectants, which are non-specific for the cells that they affect. Antiseptics are used on animate objects while disinfectants are used on inanimate objects. Sterilization can be achieved by using several chemical compounds in the gaseous form. These compounds such as formaldehyde and ethylene oxide are extremely toxic. A variety of chemicals can be used to achieve chemical disinfection, some of these chemicals include: alcohols, acids, alkalis, phenols, halogens, heavy metal compounds, detergents (including quaternary ammonium compounds), anti-metabolites, and peroxides. Ideally, a disinfectant should have the following characteristics:
• capable of destroying all microorganisms as well as viruses; • possess a high degree of stability; • not be toxic to humans or to animals; • be soluble in water; • be tasteless and odorless; and • be relatively inexpensive.
Acids and bases are effective compounds because they release hydrogen (acids) and hydroxyl ions (bases). Enzymes are very sensitive to pH and are inactivated by very acid or very basic compounds Some of the types of disinfectants and antiseptics include (Meyer, 1997): Alcohols: These compounds usually are used as skin antiseptics. Alcohols are surfactants and also coagulate proteins. Ethanol, isopropanol, and benzyl alcohol are effective at concentrations of 50% to 70%. Alcohols are not effective in destroying, fungi, spores, or most viruses. Phenol (carbolic acid) and its derivatives (cresol, orthophenylphenol, and others) are used for sterilizing surfaces. Phenols act mostly by coagulation and by damaging plasma membranes. They tend to remain on surfaces. The effectiveness of phenols is similar to that of alcohols. The strengths of new disinfectants are expressed by comparison to phenol. This is known as the phenol coefficient. Halogens � especially iodine and chlorine are widely used as antiseptics and disinfectants. Iodine and chlorine are lethal to a large variety of fungi, bacteria, and viruses through the inactivation of proteins. Tincture of iodine (a solution of 1% to 2% iodine in alcohol) is widely used for wounds. The iodine reacts with hydroxyl groups and inactivates proteins. Chlorine gas reacts with water to form hydrochloric acid (HCl) and hydrogen peroxide. Both of these compounds are strong oxidants, which destroy microbial cells. They have been commonly used to disinfect public water supplies and sewage, and they have been widely used in the dairy industry. The common household bleach consists of 5.25% sodium hypochlorite.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 37
Aldehydes such as formaldehyde (8%) and glutaraldehyde (2%) are alkylating agents that react with the amines, some groups of proteins (such as sulfhydryl and carboxyl) and small organic molecules to inactivate them. Aldehydes essentially destroy all forms of microbial life, but their application is limited due to their noxious vapors. Heavy metals precipitate proteins and therefore are effective as antimicrobial agents. Silver nitrate is used in the eyes of newborn babies, copper sulfate has been used in swimming pools, and some mercury compounds are used in the clothing and flower industries. Merbromin (mercurochrome) has been used extensively as an antiseptic. Heavy metal compounds are primarily bactericidal. Detergents include soaps and synthetic detergents. Soaps are potassium or sodium salts of higher fatty acid content. Detergents are mainly surfactants and are used to wash away debris from surfaces. Synthetic detergents are manufactured such that they have some soap properties. Essentially there are three types of detergents:
1) anionic detergents (e.g., sodium lauryl sulfate); 2) cationic detergents (e.g., alkybenzyl sulfonates and quaternary ammonium compounds,
such as zeepryn and zephiran. These compounds are effective against bacteria and fungi.); and
3) nonionic detergents. Gases, due to their ability to alkylate and penetrate in a closed system, are excellent disinfectants and are effective against all forms of microbial life. Some of the gases most commonly used are ethylene oxide, propylene oxide, and beta-propiolactone. Sulfur dioxide is commonly used as a food preservative. Hydrogen peroxide (H2O2) is a mild antiseptic. Hydrogen peroxide is commonly used on wounds to destroy anaerobic bacteria. Some of the most common disinfectants used in the treatment of health care waste used to be chlorine based. Of these, sodium hypochlorite (commonly known as bleach) was one of the most common solutions used for disinfection. However, due to chlorine's negative health effects and since it has been demonstrated that chlorine is a precursor to the formation of dioxins in combustion; other disinfectants (non-chlorine based) are now being used. Some of these alternatives include: aldehydes (such as formaldehyde and glutaraldehyde), calcium oxide, ozone, and others. Some of the most important requirements to achieve a high degree of chemical treatment in health care wastes are: 1) to have a sufficiently high concentration of the compound, 2) to have long enough time during which the wastes are in contact with the chemical (retention time), and 3) that the wastes have a small enough particle size. Small and large-scale systems have been designed and used for the treatment of health care wastes. These systems typically incorporate some type of size reduction equipment to shred the wastes before chemical treatment. The chemical that has been used for disinfection has

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 38
been a solution of chlorine. Eventually the treated solids are separated from the liquids. The addition of a liquid into the system implies that eventually the liquid has to be managed prior to discharge into the environment. In the past, the liquid has been discharged into the sewerage system (this implies that in some locations a special permit must be obtained). In other situations, it may be necessary to treat the liquid prior to discharge into the sewer (metals, organic contaminants, dissolved solids, and others). Aerosols and particulate matter that may be released from the process are managed by means of air pollution control devices; which include: enclosures, ducting, HEPA filters, and blowers providing negative pressure. A diagram showing a typical installation is presented in Figure 7.
HEPA FilterNegative PressureSystem Blower
ChlorineSolution
Pre-Shredder
Hammermill
SolidWaste
CollectionCart
LiquidEffluentto Sewer
ChlorineStorageTank
WasteConveyor
Waste
Source: U.S. Congress, 1990.
Figure 7. Diagram of Commercial Chemical Treatment Unit
Types of HCW that Can be Treated Chemical disinfectants generally are used to treat the following types of materials:
• sharps; • cultures and stocks; • items contaminated with blood; liquid human and animal wastes; • residues from surgery and from isolation wards; • bandages, gauze, linen, gowns, and other similar materials also known as "softs"; and • non-chemical laboratory wastes.
Types of HCW that Should Not be Treated Health care facilities produce a variety of chemical and hazardous substances that should not be treated with chemical compounds. These types of wastes include:

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 39
• wastes from chemotherapy treatment; • mercury; • volatile and semi-volatile organic compounds; • radioactive wastes; and • other hazardous chemical wastes.
In general, it is not advisable to treat large body parts, animal carcasses, or other large items that because of their mass and other characteristics which make it difficult or costly for the entire material to be properly treated.
Emissions and Residues from the Process The application of chemical disinfection for the treatment of health care wastes can result in liquid and gaseous emissions that may be hazardous to personnel in the health care facility, to personnel in the treatment facility or to those working in the waste collection system or at the final disposal site. In addition, if the treated materials are not properly contained in the final disposal site, any water that may percolate through the treated mass may become contaminated and eventually reach the groundwater or surface bodies of water. In several health care facilities in developing countries, it is common practice to use a recycled container from within the hospital and partially filled with a chemical disinfectant (usually a solution of sodium hypochlorite) to store used needles prior to disposal. This practice presents a risk to the medical staff and other personnel in the facility just by the mere fact that the containers must be filled. This compound and others that are similar are, at the very least, strong irritants to the skin and to the respiratory system. Furthermore, it has also been observed that at the time of collection, the containers with disinfectant and sharps are simply capped and taken to the storage facility prior to treatment or final disposal. Thus, the liquid remains in the container. The presence of sodium hypochlorite can cause occupational health problems and, in the event that the wastes are treated in an incinerator, contribute to the formation of dioxins and furans. The treatment facility can also pose occupational hazards because chemical processes generally require some type of size reduction. Thus, there is the possibility of pathogen release through the formation of aerosols. One of the most commonly used disinfectants, glutaraldehyde, has been associated with several health problems, including skin sensitization, asthma, and perhaps chemical sensitization.
Combustion Infectious health care waste may be treated by setting it on fire (combusting it) in a variety of methods. The "vessels" used for the combustion process range from simple open pits in the ground and metallic containers to sophisticated units which incorporate specialized equipment to control emissions.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 40
Any type of method used for the combustion of solid wastes generally produces three types of discharges: gaseous, liquid, and solid. The exception would be the use of combustion in the open air in which case water may not be used to quench the ashes. In a conventional, modern incinerator equipped with air pollution control equipment, a substantial concentration of heavy metals and dioxins would be present in the fine solid removed from the stack gas (this material is known as fly ash). In some countries, the fly ash collected from incinerators treating municipal solid waste is considered a hazardous waste. In this discussion, the combustion technologies are divided into three general types: low, medium, and high technologies.
Low Technology Combustion In many developing countries some fractions of health care wastes and in particular used injection equipment are commonly burned in the open air or in simple, often times improvised units such as pits, burners (made out brick or cement) and in drums. The units obviously are relatively inexpensive, are easy to build and require little or no maintenance. Because of the relatively uncontrolled conditions under which the combustion takes place, the process only reaches what is considered low temperatures (about 400°C or below). Combustion at these temperatures does not burn all of the wastes particularly if the wastes contain a relatively high moisture content. Some syringes and needles may remain relatively unchanged at the completion of the combustion process. Furthermore, the uncontrolled conditions may not destroy all of the pathogens. This type of combustion does not control any type of emissions (particulate matter, heavy metals, and others) and, in fact, may lead to the production of relatively high concentrations of toxic organic compounds. Whole vaccine vials and similar glass containers have the tendency to explode and thus pose and additional risk to the person tending to the combustion process. A schematic diagram of a low technology unit is shown in Figure 8.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 41
10 BOXES 5 liters each MAXIMUM
5 BOXES 10 liters each MINIMUM
Figure 8. Diagram of a Low-Technology Incineration Unit
Medium and High-Technology Combustion In this report, medium-technology combustion is defined as that which in some manner attempts to control the combustion process and provides slightly better conditions than those achieved by the low-technology options. There are some relatively simple and not excessively expensive units available in the market place that fit into this category. In essence, the units generally have a small capacity, are operated in batches and do not include any type of air pollution control equipment. High-technology combustion in this report is defined as the combustion of health care waste under controlled conditions, using equipment that operates at temperatures on the order of 900°C to 1000°C, and that includes air pollution control equipment as well as other components to manage the emissions from the unit. These units generally include a second chamber (known as secondary chamber) in which the off gases from the first chamber are treated at high temperatures by means of an ancillary burner. High-technology combustion essentially provides the necessary conditions (temperature, time, and turbulence) to achieve complete combustion and keep the concentration of undesirable compounds to a minimum. The burner normally is fuelled by means of diesel or gas. The incinerator may be operated in batches or in a continuous mode. A diagram of a high-technology controlled air incinerator is shown in Figure 9.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 42
Feed Ram
AshTransfer
RamAir Tube
AshDischarge Ram
Ash Sump
AshChute
PrimaryChamber
Fossil FuelBurner
SecondaryChamber
To Boiler
Ash Quench
Figure 9. Diagram of a Controlled Air Incinerator
Types of Risks Associated with Combustion The direct combustion (incineration) of HCW generates particulate matter and chemical compounds that can potentially affect human health and safety and have a negative impact on the environment. These materials can be emitted in gaseous, liquid, or solid form, and the impacts to humans can be direct or indirect. For example, inhalation of airborne particulate matter can be a direct source of exposure and may cause illness. An example of indirect exposure would be ingestion of metals by humans contained in meat originating from animals foraging on plants that received deposition of the metals from an incinerator situated upwind. Risks posed by airborne dispersion of incinerator emissions, i.e., exhaust gas emissions, generally are one of the primary environmental risks of waste combustion. The other primary risk is that associated with the solid residue, or combustion ash. Because of the concentration of certain toxic compounds in the solid residue produced by waste combustion, the risks posed by the ash also have several routes of exposure, e.g., direct inhalation of airborne ash particulates or indirect routes, such as ingestion of metals leached from ash into drinking water sources. Since many if not all of the chemicals found in HCW are also present in MSW, the analysis of the derivation and magnitude of health risks associated with incineration of HCW can draw upon similar analyses involving MSW as the feedstock. The analysis can also take advantage of some analyses specific to incineration of HCW. However, studies of HCW incineration have had the tendency to concentrate on those risks and measures of control that are associated with toxic organic compounds that exhibit high carcinogenicity, especially chlorinated dioxins and furans (dioxins/furans, or D/Fs).

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 43
In the case of certain types of gaseous emissions from incinerators combusting MSW, the risks to public health, and the safe levels that could be released into the ambient air, had been defined as a consequence of studies of health risks of airborne emissions generated by motor vehicles and by the combustion of coal. These air pollutants include particulate matter (PM), nitrogen oxides (NOx), sulfur oxides (SOx), carbon monoxide (CO), and unburned hydrocarbons. For certain other air emissions characteristic of the combustion of solid fuels, but not necessarily the subject of governmental regulation at the time, health risk assessments were sometimes performed during the process of obtaining local approval of projects involving the combustion of wastes. Air pollutants falling within this category include certain heavy metals and toxic organic compounds. Thus, there are well-developed methods of defining the routes of human exposure to incineration pollutants, and of analyzing the associated risks and determining safe concentrations in ambient air. The application of health risk assessment to waste incineration was developed over approximately a 20-year period and continues to evolve as of this writing. However, the main elements of the methodology have a firm foundation in science, including toxicology and dispersion modeling of stack gas plumes. It is fair to say that to date the risks to human health and safety posed by the incineration of waste probably have been given greater and longer quantitative analysis than have the risks associated with any other alternative available for managing solid wastes, including land disposal. Many industrialized countries have established risk-based limits of human exposure to airborne emissions that are characteristic of waste combustion. A detailed health risk assessment performed by the State of California Air Resources Board used a multi-pathway (inhalation, dermal absorption, etc.) health risk assessment model to evaluate potential acute, chronic, and cancer health risks from human exposure to airborne emissions generated by medical waste incinerators operating in California. The results of the assessment were used to support emission regulations promulgated by the State of California for medical waste incinerators. Eight medical waste incinerators were tested in California, ranging in processing capacities from approximately 115 to 7,100 kg/day. The incinerators that were tested reflected a variety of technology designs and operating conditions, and some of the units were equipped with air pollution control (APC) systems of various types. (Because the units were tested in the late 1980s, the results of the testing of the controlled incinerators did not reflect likely lower emissions that would have resulted from the imposition of modern emission control equipment required by regulation in the late 1990s.) The emissions were found to vary substantially, irrespective of whether or not an APC system was included in the design. As a result of the testing and analysis, the study concluded that the risk due to multi-pathway exposure to dioxins ranged from about 1 in one million from a controlled incinerator to approximately 250 per million in the case of an uncontrolled incinerator. The same study also found that the cancer risk from inhalation only of cadmium in emissions from a medical incinerator ranged from less than 1 in one million for a controlled incinerator to approximately 15 in one million for an uncontrolled unit (Air Resources Board, 1990). Combustion of HCW, and other types of solid waste, results in the production and emission of finely sized particulate matter and incomplete products of combustion. These emissions are inherent in the process of combustion, since in practice no large-scale combustion process for

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 44
solid matter is 100% thermally efficient. This situation exists because solid waste is composed of chemical compounds with additional elements to carbon and hydrogen, and because the combustion process cannot be ideally controlled. The other elements in solid waste include those of the family of heavy metals (lead, mercury, cadmium, and others) and the halogen family (chlorine, bromine, etc.). Some of these elements are precursors, under typical conditions of combustion, of chemical compounds that can present substantial risks to human health and safety. Chlorine and chlorinated compounds in particular are precursors of some very toxic chemicals, including chlorinated dioxins and furans. Depending on the molecular weight and boiling point of the compounds and on other factors, the compounds formed during the combustion process may exist in solid, liquid, or gaseous form upon entering the ambient environment. In addition to the combustion system (equipment) itself, a modern-day solid fuel-fired combustion facility also consists of post-combustion systems whose main functions are to control the emissions. Consequently, the post-combustion systems also can affect the form of the compounds that ultimately enter the environment. Thus, some emissions may initially exist after combustion in the form of gases and subsequently be converted to a solid form during a post-combustion process. Air pollution from sources of combustion has been associated with a wide variety of acute and chronic health effects. The health effects vary depending upon the type and concentration of the pollutants. Air pollution due to particulate matter is related to some of the most serious effects, including lung cancer and other cardiopulmonary mortality. Other components of air pollution, such as lead and ozone, also are associated with negative health impacts, and contribute to the burden of disease attributable to urban air pollution. Analyses based on particulate matter estimate that ambient air pollution causes about 5% of trachea, bronchus, and lung cancer; 2% of cardio-respiratory mortality; and about 1% of respiratory infections mortality globally. This amounts to about 0.8 million deaths and 7.9 million disability adjusted life years (DALYs). This burden of disease predominantly occurs in developing countries (WHO, 2002). The following discussion focuses on the emissions from the combustion system or facility and not upon the emissions that might be generated during the delivery, storage, or handling of MSW, HCW, or both prior to thermal processing. The emissions associated with those activities are assumed to be similar to the emissions generated during waste collection, or generated immediately before application of the waste to land or of other HCW treatment methods.
Potential Impacts
Airborne Pollutants (Stack Emissions)
Oxides of nitrogen, sulfur dioxide, hydrogen chloride, and hydrogen fluoride are referred to as acid gases. Acid gases degrade the quality of the ambient air and can affect other resources, such as building structures and fresh water lakes, as a result of acidification. While acid gases are emitted from MSW combustion, as a class they are less toxic and environmentally persistent than metals and to partially oxidized organic compounds, particularly halogenated organics (Washburn, et al., 1989). The incineration of HCW also emits airborne acid gases, as well as metals, particulate matter, and partially oxidized organic compounds.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 45
A summary of the stack emissions and their potential impacts is shown in Table 22. Typical airborne emissions from incineration of HCW in a developing country are given in Table 23.
Table 22. Pollutants in the Exhaust Gas from Waste Combustion Processes
Substances Potential Impact Heavy Metals Injury to human health, soil and water
contamination, loss/degradation of vegetation
Dioxins (PCDD/Fs and coplanar PCB) Injury to human health and ecosystem
SOx, NOx, HCl Injury to human health, acid rain
CO2 Global warming
Particulate matter Injury to human health Source: EX Corp., undated.
Airborne particulate matter (fly ash) represents a potential health risk due its very small particle size distribution and due to the possible high concentration of heavy metals, which tend to preferentially attach to the smaller particles. The size of the particles is important because if they are smaller than about 10 microns, they can be inhaled deep into the lungs of human beings. Emissions that are smaller than 10 microns in diameter are called "respirable particulate matter.� This category of emissions includes dusts, soot, liquids, acids from aerosols, smoke particles, and other materials. This limit in size (10 microns) has led to the abbreviation of respirable particulate matter as "PM10." Respirable particulate matter makes up approximately 55% of the total mass of suspended particles in air pollution in the United States. The U.S. Environmental Protection Agency (US EPA) has subdivided these particles into particles of 2.5 microns or less (fine particles) and particles of between 2.5 and 10 microns (coarse particles). The human nose and other components of the respiratory system are capable of removing relatively "large" particles from the inhaled air. However, PM10 and in particular PM2.5 particles can penetrate deep into the respiratory system and reach the lungs. The farther a particle penetrates into the lungs and the higher the concentration, the more likely it is to cause nose and throat irritation, bronchitis, and even physiologic damage to the lungs. Toxic chemicals adhered to respirable particulate matter can increase the potential for adverse health effects. Groups that are at high risk due to fine and coarse particles include children, the elderly, and people with heart diseases or with respiratory conditions like asthma and emphysema. In addition to these health hazards, fine particulate matter impairs visibility and can discolor property and clothing.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 46
Table 23. Measured Airborne Emissions from HCW Incinerators Tested in the Philippines a
Parameter Incinerator
#1 Incinerator
#2 Particulate 86.3 15.9
SO2 36.1 28.7
NOX 37.5 33.3
THCs b 0.6 3.6
CO - --
HCl 122.9 53.8
HF 0.27 0.2
Antimony 0.027 0.007
Arsenic 0.023 0.002
Barium 0.010 0.008
Beryllium <0.0001 <0.001
Chromium 0.015 0.005
Cobalt <0.0006 <0.005
Copper 0.073 0.022
Lead 0.852 0.173
Manganese 0.017 0.020
Nickel 0.018 0.008
Phosphorus 0.623 0.491
Selenium <0.0013 <0.001
Silver 0.002 0.001
Zinc 0.1123 0.312
Cadmium 0.021 0.009
Thallium <0.002 <0.001
Dioxins/Furansc 87 10.2 Source: CalRecovery, Inc., 2002. a All results are reported in mg/Ncm except those for dioxins/furans, which are reported in ng/Ncm. b Total (C14-C18) dioxins/furans. c Total hydrocarbons.
Some studies have analyzed the characteristics of particulate matter from HCW incineration. Lombardi, et al. (1998) measured particle sizes in the range of 99.73% smaller than 73 µm to 6.12% smaller than 1.1 µm for fly ash discharged from HCW incinerators in Rome, Italy. The same study reported concentrations of 3,000 mg of zinc/kg of fly ash and in the range of 6 to 964 mg/kg for certain other metals, as shown in Table 24. Particulate matter measured in ambient air downwind from a HCW incinerator operating in the United States has been shown to

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 47
be mutagenic, although less so than estimates of mutagenicity published for wood stoves, automobile gasoline engines, and residential furnaces (Driver, et al., 1990). The same study also reported that the incinerator fly ash and downwind ambient air particulate samples demonstrated a substantial increase in mutagenicity when the auxiliary burner failed during a portion of the sampling runs.
Table 24. Concentration of Metals in Fly Ash Generated from Incineration of HCW
Metal Mg Zn Pb Cu Cr Mn Cd Ni Sn As Sb
% 0.4 0.3
mg/kg 964 173 109 105 85 45 18 10 6 Source: Lombardi, et al., 1998.
The dominant metal emissions from HCW incinerators in the United States have been reported as As, Cd, Cr (carcinogenic metals), and Pb (toxic metal) (California Environmental Protection Agency, 1992). The results of research have identified some types of plastics as potential sources of Pb and Cd in HCW (Hickman, 1987). Some of the partially oxidized organic byproducts of waste combustion are persistent in the environment and are highly toxic and/or carcinogenic at low concentrations; thus, they have drawn the attention of the health care industry, regulators, and the public. These byproducts include dioxins and furans. The presence of dioxins and furans in air emissions from waste incineration has been known for approximately 25 years. Once dioxins are released through the stack of an incinerator, the dioxins may remain in the ambient air in the vapor phase or may be deposited on particulate matter. Eventually, the dioxins migrate onto surface soil and surface water through wet or dry deposition. Dioxins in soil are tightly bound to organic carbon in the soil particles and, due to relatively low solubility of dioxins in water, dioxins in soil mainly move attached to the soil particles. Precipitation falling on soil may transport dioxins either laterally to nearby surface waters or downward into the groundwater. Dioxins transported into surface water eventually settle to the bottom (EX Corp., undated). Wind action may promote horizontal as well as vertical movement of soil particles into the ambient air. Dioxins in ambient air may be deposited onto plants by wind action or by precipitation. Uptake of dioxins by plants takes place primarily in the vapor phase via aspiration. Due to the low water solubility of dioxins, plant uptake from the soil pore water via the root is less significant than via aspiration. Eventually, animals or humans may consume contaminated plants and thus would intake certain concentrations of dioxins. In addition, humans and animals may intake dioxins via inhalation of air, drinking water, ingesting soil or sediment, and other routes.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 48
Human exposure to dioxins can take place through the following pathways: • inhalation of dioxins in the vapor phase or of dust containing dioxins; • intake of contaminated water; • ingestion of contaminated soil; and • dermal contact with contaminated dust or soil.
It has been estimated that 90% of human exposure to dioxins is through food consumption. Inhalation of vapor or dust is one of the most significant pathways because:
• water solubility of dioxins is relatively low and therefore intake of dioxin through drinking water is very limited as long as particulate matter that may contain dioxins is properly removed;
• even though the highest levels of dioxins are found in soil samples, ingestion of soil is not common in terms of quantity and number of events that occur for the adult population; and
• skin penetration of dioxins is very limited since dioxins are closely bound to the organic carbon in soil particles (EX Corp., undated).
Leem and colleagues estimated the exposure status of PCDDs and PCCFs (D/Fs) and their effects on the health of workers and of residents living near MSW incinerators as well as of residents living near industrial waste incinerators (Leem, et al., 2003). In the study, 13 workers and 16 residents living around two MSW incinerators, and an additional 10 residents living close to an incinerator treating industrial wastes (suspected of emitting hazardous substances), were interviewed. The type of information collected during the survey dealt with socio-demographic parameters, personal habits and work history, as well as detailed gynecologic and other medical history. Blood samples were collected for analyses for D/Fs. Urine samples were also collected for analyses of oxidative injury biomarkers (8-hydroxydeoxyguanosine and malondialdehyde). The results of the analyses showed that the concentrations of D/Fs in residents from the area living around the industrial incinerator were higher than those in workers and residents living around the MSW incinerator. The average toxic equivalency (TEQ) concentrations of D/Fs in residents living near the industrial waste incinerator were 53.4 pg I-TEQ/g lipid. The average TEQ concentrations in workers and residents living near the MSW incinerator were 12.2 pg I-TEQs/g lipid. The estimated daily intake (EDI) of each person was calculated, and the EDI of all workers and residents living near the MSW incinerator were found to be within the tolerable daily intake range. However, only 30% of the 10 people living near the industrial waste incinerator had an EDI within the tolerable daily intake range (1 - 4 pg I � TEQ / kg b w/day) suggested by the WHO (Leem, et al., 2003). The oxidative stress of residents living near the industrial waste incinerator was higher than that in workers and residents living near the MSW incinerator. Descriptions of the type and capacity of the incinerators or of the type of air pollution control (APC) equipment used were not provided. The authors concluded that proper protection strategies against these hazardous chemicals were needed (Leem, et al., 2003). In September 1998, the Japanese Ministry of Health and Welfare reported that high concentrations of dioxins had been detected in soil samples collected near an incinerator located in the rural part of Osaka Prefecture and used for burning MSW. In addition, dioxins
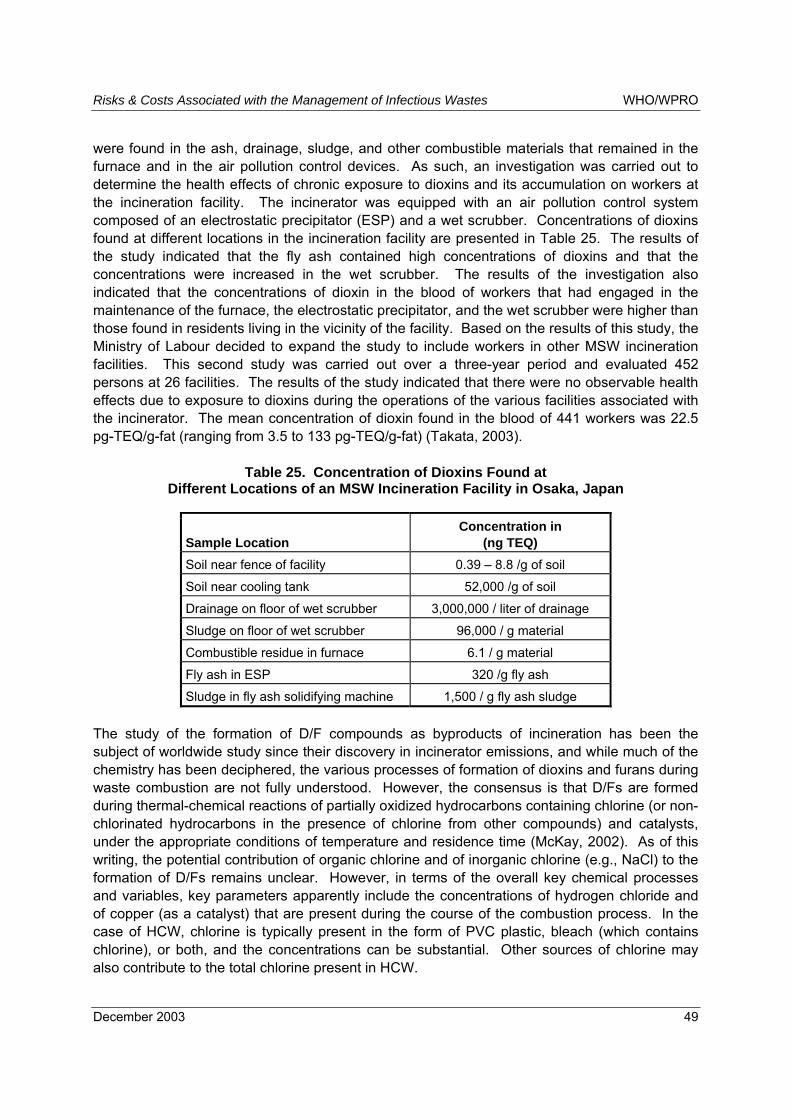
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 49
were found in the ash, drainage, sludge, and other combustible materials that remained in the furnace and in the air pollution control devices. As such, an investigation was carried out to determine the health effects of chronic exposure to dioxins and its accumulation on workers at the incineration facility. The incinerator was equipped with an air pollution control system composed of an electrostatic precipitator (ESP) and a wet scrubber. Concentrations of dioxins found at different locations in the incineration facility are presented in Table 25. The results of the study indicated that the fly ash contained high concentrations of dioxins and that the concentrations were increased in the wet scrubber. The results of the investigation also indicated that the concentrations of dioxin in the blood of workers that had engaged in the maintenance of the furnace, the electrostatic precipitator, and the wet scrubber were higher than those found in residents living in the vicinity of the facility. Based on the results of this study, the Ministry of Labour decided to expand the study to include workers in other MSW incineration facilities. This second study was carried out over a three-year period and evaluated 452 persons at 26 facilities. The results of the study indicated that there were no observable health effects due to exposure to dioxins during the operations of the various facilities associated with the incinerator. The mean concentration of dioxin found in the blood of 441 workers was 22.5 pg-TEQ/g-fat (ranging from 3.5 to 133 pg-TEQ/g-fat) (Takata, 2003).
Table 25. Concentration of Dioxins Found at Different Locations of an MSW Incineration Facility in Osaka, Japan
Sample Location Concentration in
(ng TEQ) Soil near fence of facility 0.39 � 8.8 /g of soil
Soil near cooling tank 52,000 /g of soil
Drainage on floor of wet scrubber 3,000,000 / liter of drainage
Sludge on floor of wet scrubber 96,000 / g material
Combustible residue in furnace 6.1 / g material
Fly ash in ESP 320 /g fly ash
Sludge in fly ash solidifying machine 1,500 / g fly ash sludge The study of the formation of D/F compounds as byproducts of incineration has been the subject of worldwide study since their discovery in incinerator emissions, and while much of the chemistry has been deciphered, the various processes of formation of dioxins and furans during waste combustion are not fully understood. However, the consensus is that D/Fs are formed during thermal-chemical reactions of partially oxidized hydrocarbons containing chlorine (or non-chlorinated hydrocarbons in the presence of chlorine from other compounds) and catalysts, under the appropriate conditions of temperature and residence time (McKay, 2002). As of this writing, the potential contribution of organic chlorine and of inorganic chlorine (e.g., NaCl) to the formation of D/Fs remains unclear. However, in terms of the overall key chemical processes and variables, key parameters apparently include the concentrations of hydrogen chloride and of copper (as a catalyst) that are present during the course of the combustion process. In the case of HCW, chlorine is typically present in the form of PVC plastic, bleach (which contains chlorine), or both, and the concentrations can be substantial. Other sources of chlorine may also contribute to the total chlorine present in HCW.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 50
No peer-reviewed studies describing mechanisms of D/F formation during the incineration of HCW in developing countries were found during this study. However, studies of incineration of MSW in barrels can be used to judge the influence of PVC concentration and D/F formation under poor combustion conditions, such as might be expected in the case of HCW incineration using simple and poorly controlled incineration equipment. A study conducted by the US EPA found that total concentrations of D/Fs were on the order of approximately 5 to 100 times greater in the case of combustion of solid waste that contained 4.5% PVC, compared to waste composed of only 0.2% PVC (Lemieux, et al., 2000). Uncontrolled emission D/Fs generated during the incineration of HCW have been measured and compared for several facilities in the United States (California Environmental Protection Agency, 1992). The concentrations were typically in the range of approximately 200 to 6,000 ng/Nm3 at 12% CO2. These emission concentrations were generally greater than uncontrolled concentrations of D/Fs measured for municipal solid waste incinerators during approximately similar historical time periods. However, the greater emission levels likely were the result of MSW incinerators as a class having generally better (more modern) design and operation at the time than HCW incinerators. Uncontrolled emissions for MSW incinerators were in the range of approximately 50 to 1,800 ng/Nm3 at 12% CO2. Tests of HCW incinerators in developing countries show that emissions of total D/Fs can be in the range of 10 (0.25) to 10,090 (252) ng (ng TEQ)/Nm3 based on stack testing in Cambodia and the Philippines. A summary of the test data is shown in Table 26. The incinerators tested did not possess modern post-combustion APC equipment, and control of pollutant emissions, if any, was imparted to the burning process through the use of combustion controls, e.g., residence time, turbulence, and temperature. The wide variations in measured values indicate the effect of incinerator design and operating conditions on emission levels. As a point of reference, total D/F emissions are also shown in Table 26 for open pit burning of HCW in Cambodia. The measured values were 7 (0.15) and 33 (0.49) ng (ng TEQ)/Nm3.
Table 26. Emissions of PCDDs and PCDFs from Incineration and Open Pit Burning of HCW in Developing Countries (ng/Nm3)
Total (PCDDs and PCDFs) Incinerator Model Location As Measured TEQ
SICIM Case 2 a Cambodia 10,090 252
Vulcam Case 2 a Cambodia 63 1.1
Hovalwerk AG CV1 b Philippines 87 2.4
Hovalwerk AG CV1 b Philippines 10.2 0.25
Open Pit Burning a Cambodia 7.0 0.15
Open Pit Burning a Cambodia 33 0.49 Sources: a Environmental Control Center, 2001. b CalRecovery, Inc., 2002.
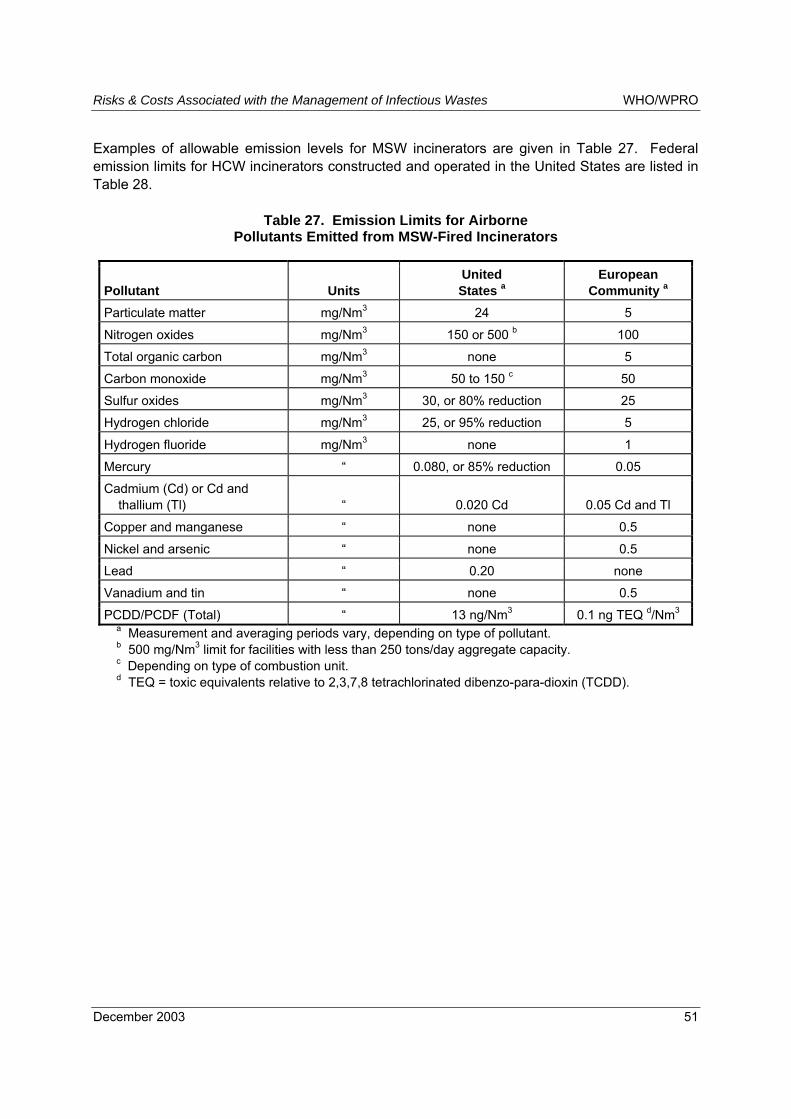
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 51
Examples of allowable emission levels for MSW incinerators are given in Table 27. Federal emission limits for HCW incinerators constructed and operated in the United States are listed in Table 28.
Table 27. Emission Limits for Airborne Pollutants Emitted from MSW-Fired Incinerators
Pollutant Units United States a
European Community a
Particulate matter mg/Nm3 24 5
Nitrogen oxides mg/Nm3 150 or 500 b 100
Total organic carbon mg/Nm3 none 5
Carbon monoxide mg/Nm3 50 to 150 c 50
Sulfur oxides mg/Nm3 30, or 80% reduction 25
Hydrogen chloride mg/Nm3 25, or 95% reduction 5
Hydrogen fluoride mg/Nm3 none 1
Mercury � 0.080, or 85% reduction 0.05
Cadmium (Cd) or Cd and thallium (Tl)
�
0.020 Cd
0.05 Cd and Tl
Copper and manganese � none 0.5
Nickel and arsenic � none 0.5
Lead � 0.20 none
Vanadium and tin � none 0.5
PCDD/PCDF (Total) � 13 ng/Nm3 0.1 ng TEQ d/Nm3 a Measurement and averaging periods vary, depending on type of pollutant. b 500 mg/Nm3 limit for facilities with less than 250 tons/day aggregate capacity. c Depending on type of combustion unit. d TEQ = toxic equivalents relative to 2,3,7,8 tetrachlorinated dibenzo-para-dioxin (TCDD).

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 52
Table 28. Emission Limits for Airborne Pollutants Discharged from Small, Medium, and Large HCW Incinerators -- United States
Processing Capacity of Incinerator
Pollutant Units a
Small (less than or
equal to 200 TPD)
Medium (201 to
500 TPD)
Large (greater than
500 TPD) Particulate matter mg/Nm3 69 34 34
Nitrogen oxides ppm by volume 250 250 250
Carbon monoxide ppm by volume 40 40 40
Sulfur dioxide ppm by volume 55 55 55
Hydrogen chloride ppm by volume, or
percent reduction
15 or 99% 15 or 99% 15 or 99%
Lead mg/Nm3, or percent
reduction
1.2 or 70% 0.07 or 98% 0.07 or 98%
Cadmium mg/Nm3, or percent
reduction
0.16 or 65% 0.04 or 90% 0.04 or 90%
Mercury mg/Nm3, or percent
reduction
0.55 or 85% 0.55 or 85% 0.55 or 85%
PCDD/PCDF ng/Nm3 or ng TEQ/Nm3
125 or 2.3 25 or 0.6 25 or 0.6
Source: U.S. Environmental Protection Agency, 2003. a Values are on a dry basis and 7% O2.
Radioactive Materials
Low levels (less than 100 µCi/g) of radioactive waste have been found in HCW produced in the United States (Thompson and Vavruska, 1989). The more common radionuclides used in medical treatment are tritium, 32P, 125I, and 14C. The radioactive isotopes of I can be major radioactive contaminants in HCW, and they are highly volatile (California Environmental Protection Agency, 1992). Incineration does not affect radioactivity. However, the combustion process does convert much of the radioactive material to the gaseous byproducts, which exit with the other combustion gases and reduces the mass of solid material that is radioactive.
Pathogens
Pathogen survival in modern HCW incinerators is highly unlikely, at least in the case where the technology is at least as controlled as in starved-air incinerators. The small size of many HCW combustion units apparently enables exposure of wastes, and therefore any pathogens in the wastes, to adequate residence times (greater than 30 minutes) and temperature (greater than 760°C). However, as shown in an investigation of pathogen survival in MSW incinerators (Klafka and Tierney, 1988), or if residence times and combustion chamber temperatures are too

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 53
low (e.g., 590°C) (California Environmental Protection Agency, 1992), survival of viable pathogens has been shown to occur.
Cytotoxic Compounds
No data were found on airborne emissions of cytotoxic compounds from HCW incinerators. This category of waste could be present in incinerator feedstocks in the form of contaminated containers or of residue in discarded syringes or other discarded equipment for delivering chemotherapy chemicals to patients.
Residual Solids (Ash)
The solid residue from the combustion of solid waste can take the form of fly ash, bottom ash, or a combination of the two. One determinant of the form of ash to be produced is whether or not particulate control equipment is used to collect airborne particulate matter. If no or insufficient particulate control is exercised, then the fine particulates (i.e., fly ash) that are generated during combustion are entrained in the combustion gas stream, exit the combustion system through the flue gas stack, and are discharged into the ambient air. The remaining solid residue is predominantly high-density particles and remains at the bottom of the combustion chamber, and is commonly referred to as �bottom ash.� Bottom ash is typically removed manually from low-capacity combustion systems and mechanically from large-capacity combustion systems. The bottom ash generated from MSW or HCW incineration is typically on the order of 20% to 30% of the mass of the infeed materials. Bottom ash is usually allowed to cool by natural convection or quenched using water so that the ash can be safely removed from the combustion chamber. Bottom ash may contain unburned or partially burned organic (i.e., hydrocarbons) matter, as well as inert materials. The residual ash (both fly ash and bottom ash) from combustion of radioactive solids may contain radioactive material, but the level of radiation is less than in the parent material due to vaporization of the radioactive material during the combustion process and discharge of the gases in the flue gas (California Environmental Protection Agency, 1992). If particulate control equipment is used to control airborne emissions of fly ash, then the captured ash usually is collected using a fabric filter or an electrostatic precipitator (ESP). Unless treated in some way (e.g., using chemical compounds), the captured ash is a low-density, hydroscopic material and therefore prone to dispersion if disturbed in any way. Sometimes, air pollution control systems add dry or liquid chemical compounds to control certain non-particulate constituents generated during combustion (examples of such constituents are hydrogen chloride and sulfur dioxide). The byproducts of the chemical reactions themselves become particulate matter in the exhaust gas stream, and are also collected in fabric filters or ESPs. After collection, fly ash may be managed separately or combined with bottom ash, depending on operator preferences, local environmental regulations, or both.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 54
Land Disposal Issues
Since fly ash typically has high concentrations of metals, its disposal on land can create a potential risk to the environment, the public health, or both. There are a number of factors that govern the potential of the metals in fly ash to enter the environment. The factors include the pH of the ash, characteristics of the waste that may be disposed along with the ash, if any, and local hydrogeological conditions. For example, burial of fly ash with MSW, presents the opportunity for organic acids generated by decomposing organic waste in the MSW to lower the overall local pH of the incinerator ash, thus freeing metal ions so that the ions may be transported by percolating water. Many studies in the United States have shown that the solubilities of a number of regulated metals in untreated MSW fly ash can exceed US EPA limits for designation of a waste as hazardous. In addition, data are available from a study that indicates that soluble concentrations of some metals in untreated fly ash from incinerated Malaysian HCW also exceed US hazardous waste standards, as shown in Table 29.
Table 29. Solubilities of Metals in Fly Ash Generated from the Incineration of HCW a
Acidity Metal pH 3 pH 5
US EPA Limit (mg/l) b
As 9.11 6 1.54 5.11 6 0.97 5
Ag 0.04 6 0.01 0.04 6 0.01 5
Ba 48.19 6 5.24 6.8 6 1.87 100
Cd 8.20 6 2.53 4.17 6 0.97 1
Cr 10.08 6 1.69 0.11 6 0.06 5
Cu 67.12 6 12.36 49.14 6 4.63 100
Hg 0.97 6 0.04 0.97 6 0.09 0.2
Ni 9.74 6 2.28 6.73 6 0.12 100
Pb 6.90 6 1.75 1.40 6 0.09 5
Se 2.83 6 0.19 0.97 6 0.05 1 Source: Idris and Saed, 2002. a All data are the means of six samples. b US EPA maximum limits for designation as solid, as opposed to hazardous, waste.
Methods of decreasing the potential of the metals found in the fly ash to leach into the environment have been proposed and tested. The methods include solidification and stabilization processes. These processes have been researched and/or applied to MSW fly ash for a number of years in industrialized countries. The application has been less in the case of HCW fly ash. However, some attention has been paid to treatment of HCW fly ash. For example, two researchers reported the use of a high temperature melting process to bind the metals in HCW fly ash so that they would exhibit low leaching potential (Idris and Saed, 2002). The results indicate that the solubilities of the metals were a factor of 2 to 1000 times less than those of the raw (i.e., unprocessed) ash alone, depending on the specific metal analyzed and the pH used in the analysis.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 55
Liquid Emissions
Both direct and indirect liquid emissions can be associated with the operation of incinerators. The primary example of a direct liquid emission is the uncontrolled discharge to the environment of water used to reduce the temperature of the ash (quench water) produced by incineration. Quench water can contain relatively high concentrations of any number of the pollutants characteristic of ash, including heavy metals and toxic, partially oxidized organics. These pollutants can be transported either as soluble or insoluble chemical compounds. The primary indirect liquid emission is leachate produced from land disposal of incinerator ash, fly ash, and/or bottom ash. The extent of inherent and/or percolated water in a land disposal site, the internal environment of the mass of waste, and the hydrogeological conditions at the boundary of the land disposal site all govern the polluting potential of incinerator ash. These parameters dictate the migration of ash constituents, whether the ash is disposed singularly or in combination with other waste, e.g., municipal solid waste. The mechanisms and effects of leachate formation and migration from land disposal sites have been previously described in the section on land disposal.
Emission Control Modern emission control systems for the combustion of solid waste, and coincidentally HCW, are derived primarily from those developed for MSW incinerators and in some cases complemented by those developed for hazardous waste combustion systems.
Particulate Matter, Acid Gases, CO, and Partially Oxidized Hydrocarbons
Regardless of the technology employed for post-combustion airborne pollution control, all modern solid waste incinerators employ complex combustion control systems whose goal is to achieve maximum oxidation (also referred to as "burnout") of the organic constituents in the waste feedstock. Maximum oxidation is achieved during the thermo-chemical reactions that occur in the combustion chamber by careful selection and regulation of residence time, turbulence, and temperature within the combustion zone(s). Regulation and control of combustion conditions is particularly important in minimizing generation of products of incomplete combustion, which, as previously mentioned, include toxic and carcinogenic compounds. Consequently, airborne pollutants remaining after the combustion products are primarily inorganic materials (e.g., ash and HCl) and oxidized compounds, e.g., SO2. Inefficiencies in the combustion process also result in the production of some partially oxidized chemical compounds. Combustion control is very important in minimizing the formation of nitrogen oxide compounds, CO, and toxic or carcinogenic compounds, including D/Fs. Additional control of emissions from incineration is achieved by using post-combustion air pollution control systems. The post-combustion emission control systems of modern incinerators consist of a set of integrated subsystems. Post-combustion control (PCC) is used primarily to capture any airborne particulate matter, acid gases (other NOx), and metals. Key PCC unit operations include wet scrubbers, dry scrubbers, electrostatic precipitators, and fabric filters.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 56
In the case of some airborne pollutants produced during waste incineration, namely NOx and D/Fs, special methods of control are used. These methods include catalytic or non-catalytic reduction systems for control of NOx and control of post-combustion temperature, and residence time of the exhaust gas to minimize formation of D/Fs. A listing of the primary methods used to control emissions of airborne pollutants from incineration of solid waste and HCW is given in Table 30.
Table 30. Air Pollutants from Solid Waste Incineration and Methods of Control
Pollutant Control Methods Typical Reduction (%) Oxides of nitrogen (NO2) • Selective catalytic reduction
• Selective non-catalytic reduction • Flue gas recirculation • Combustion control
10 to 60
SO2 and HCl acid gases • Wet scrubber • Dry scrubber • Fabric filter • Electrostatic precipitator
50 to 85 SO2 75 to 95 HCl
Carbon monoxide (CO) • Combustion control 50 to 90
Heavy metals • Dry scrubber • Fabric filter • Electrostatic precipitator
70 to 95
Particulates • Electrostatic precipitator • Fabric filter
95 to 99.9
Toxic organics (including dioxins and furans)
• Combustion control • Combination of dry scrubber and
fabric filter
50 to 99.9
Source: Savage, et al., 1988.
Radioactive Material
Levels of radioactivity in HCW usually are sufficiently low so that control of radioactive emissions can be exercised through good combustion practice. Good combustion practices ensures maximum burnout of ash and that radioactive material is gasified and properly discharged, diluted and dispersed so that safe levels are achieved in downwind ambient air (California Environmental Protection Agency, 1992).
Pathogens
Pathogens in the waste are destroyed if proper combustion control is exercised. Proper temperatures are those greater than 760°C. However, even if proper combustion conditions are enforced, viable pathogens can be emitted from incineration facilities if fugitive pathogens are inadvertently drawn into the stack, where the gas temperatures are much less than 760°C (California Environmental Protection Agency, 1992).
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 57
Cytotoxic Compounds
Since these compounds are organic, good combustion practice is considered to be the standard for achieving very efficient decomposition of the compounds into harmless byproducts, primarily CO2 and H2O. Some cytotoxic compounds are particularly resistant to thermal decomposition and require combustion temperatures above 900°C (Acurex Corp., 1989).
Emerging Technologies A few researchers and developers of waste treatment technologies are in the process of evaluating several approaches for treating the wastes. Most of these technologies are at various stages of development. For completeness, some of the approaches are presented here. However, it is important to emphasize that very few, if any, of these technologies have been demonstrated at full-scale facilities.
Plasma In physics, plasma is a gas of positive ions and free electrons with little or no overall electric charge. In this state, the ionized gas can conduct an electric current. However, due to its high resistance, the electric energy is converted to thermal energy. Thus, this process can result in reaching temperatures between about 1600°C and more than 11,000°C. The systems that are being developed for the treatment of solid wastes usually use a plasma-arc torch to produce the plasma energy. In this type of system, an arc is produced between two electrodes. This type of system could treat a wide variety of health care wastes. These systems may have high capital and high operating and maintenance costs. Available information indicates that these units have not been demonstrated on a continuous basis at any health care facility.
Pyrolysis Pyrolysis is defined as the degradation of organic matter in the material undergoing the process under high temperatures and pressures. The process results in the production of off-gases, a liquid and a solid residue. Depending upon the operating conditions (i.e., temperature and pressure), the relative quantity of the outputs can be changed. The pyrolysis process has been demonstrated at full scale for the production of a combustible gas from coal. The gas is known as syngas and consists primarily of CO and several other combustible gases. Several attempts have been made to develop a pyrolysis system capable of treating municipal solid wastes. Most of these processes have not been successful at large-scale systems. One manufacturer claims to have pyrolysis systems for the treatment of health care wastes installed in North America and in a country in the Caribbean. In the process, the organic fraction is first pyrolyzed using electricity as the source of energy. Pyrolysis is followed by two phases of oxidation of the gases produced. The remaining residue consists of essentially inert matter, and typically is about 5% of the original weight. The resulting air emissions consist of carbon dioxide, water vapor and trace gases. According to the manufacturer, the system is capable of processing between about 45 and 60 kg of health care waste per hour.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 58
Cost Costs associated with the construction of a final disposal site or a particular treatment facility play a critical role in the selection of a specific option. Furthermore, those involved in the decision-making process must take under consideration the costs associated with the operation and maintenance of the process. In the process of selecting a treatment option, the provider of the technology should be requested to submit detailed information regarding the costs for operation and maintenance. In some cases, the capital costs may be relatively low, but the operating and maintenance costs (O&M) can be substantially high. The data in the Tables 31 and 32 present estimated capital and operation and maintenance costs for the disposal of HCW in different types of landfills. For comparison purposes, the data in Table 31 also show the costs associated with the disposal of wastes in open dumps. In addition, the estimated capital and O&M costs for available treatment options are presented in Table 33. The data are given for a range of capacities for the treatment options. As shown in the table, the capital costs vary from as low as US$ 700 to about US$ 5 million. On the other hand, the O&M costs fluctuate from 0.022 to 0.638 US$/kg of material treated. It is important to keep in mind that the costs will be influenced by the local conditions such as labor rates as well as the costs of construction materials, the costs of energy and other factors.
Table 31. Estimated Costs for Land Disposal of HCW in Developing Countries
Cost
Type of Facility Capital US$/ha
O&M US$/tonne
Open dump 0 to 5,000 1 to 3
Controlled landfill 10,000 to 90,000 5 to 18
Sanitary landfill 100,000 to 150,000 20 to 45
Table 32. Estimated Costs for Additional Land Disposal Options
Type of Facility Capacity Estimated Construction
Cost (US$) Pit (soil) 4 m3 40 to 100*
Pit (cement) 4 m3 200 to 900**
Encapsulation 200 liter drum 50 to 100*** * Higher costs if pit is lined with impermeable plastic material. ** Range reflects costs for cement or for a reinforced concrete enclosure and depends
upon local material and labor costs. *** Range reflects differing local costs for materials and labor.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 59
Table 33. Estimated Capital and Operation and Maintenance Costs Available Treatment Methods
Method Capacity (kg/hr)
Capital Cost (US$ x 1000)
Operating Cost (US$/kg)
Autoclave 23 to 3600 30 to 1,780 0.13 to 0.36
Chemical 11 to 6800 20 to 890 0.15 to 2.2
Microwave 23 to 410 70 to 710 0.10 to 0.42
Incinerator (medium technology) 3 to 6 0.8 to 6.0 0.06 to 0.10
Incinerator (high technology) 250 to 4,000* 120 to 6,000 0.15 to 0.30 * There are incinerators with much higher capacities than these. For completeness in this discussion, the estimated costs related to the management of used syringes are presented in Table 34. The most common methods for managing the syringes include: needle removers, safety boxes, and needle destroyers.
Table 34. Estimated Capital and Operation and Maintenance Costs for the Management of Used Syringes
Method Capacity Capital Cost
(US$) Operating Cost
(US$) Needle remover ~ 30 min. continuous 20 to 50 N/A
Safety box ~100 syringes/5 liter box $1/box 0.01 per syringe
Needle destroyer 1 per second or less 150 to 1900 < $ 4/1000
Trends • Based on the results of this evaluation and on the experience of the authors, it has
become apparent that: • Most developing countries are becoming more and more aware that HCW require
special treatment; • At the present time, the major fraction of health care wastes collected in developing
countries either are disposed on the land or are incinerated; • There is a slow but concerted effort to discontinue the reliance on incineration for the
treatment of HCW. It is expected that the incineration of HCW will not be practiced within the next ten years.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 60
Conclusions 1. The review of the literature points out the need to reach consensus on a worldwide basis
on the definitions used to describe the various types of wastes generated in health care facilities. One reason for resolving this shortcoming is that comparative analyses such as this one, as well as the exchange of information, are severely compromised by ill-defined and ambiguous terms. Without well-defined terms, major difficulties and misunderstandings are bound to occur when discussing and analyzing HCW characteristics.
2. Based on data reviewed and analyzed in this study, the range of total hospital waste generation varied from 0.54 to 1.39 kg/bed-day. On the other hand, the reported amount of infectious (clinical, yellow bag) waste varied from 0.30 to 0.34 kg/bed-day.
3. The percentage of total health care waste of the total amount of municipal solid waste generated is on the order of 0.72% (the range can fluctuate from 0.36% to 1.44%) whereas the percentage of infectious waste of the municipal solid waste generated is about 0.27% (similarly the range can vary from about 0.14% to 0.54%).
4. Other characteristics of the components of the waste stream such as the bulk density and the calorific value have a substantial variability. This is probably due to different moisture contents of the waste.
5. The most common method of land disposal of solid wastes used in developing countries is the open dump. This method of waste disposal poses severe negative public and environmental health effects and must be discontinued.
6. A considerable amount of research has been carried out to determine the risks associated with land disposal and with the incineration of solid wastes. Only limited amount of information is available regarding risks due to alternative methods of treatment. Furthermore, the data are at least 20 years old.
7. Currently available alternative technologies for the treatment of HCW require that suitable land disposal facilities be available. Capital costs for the construction of a sanitary landfill in developing countries range from US$ 100,000 to 150,000. The O&M costs for these facilities range from US$ 20 to 45 per tonne of waste.
8. The capital costs for available treatment technologies fluctuate from about US$ 700 to 5 million and the O&M varies from 0.022 to 0.638 US$/kg.
9. Technically it is extremely difficult to build and operate and incinerator that can be "low-cost, and low technology" and at the same time maintain emissions to a minimum.
10. There are several international conventions and/or protocols that impact the management of health care wastes.
Recommendations Based on the information collected during the preparation of this report, the authors would like to make the following general recommendations for the management of health care wastes in developing countries in the Western Pacific region.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 61
1. The solid waste management system should be based on a comprehensive waste reduction program combined with careful segregation practices. Specialized personnel should continually monitor these programs since the practices lead to a substantial reduction in the quantity of infectious and hazardous wastes that would require special treatment. Waste reduction and segregation must be complemented by continuous and comprehensive information, education, and communication (IEC) campaigns aimed at every member of the health care facility and at the general public.
2. The use of open burning for the treatment and of open dumps for the final disposition of the wastes should be strictly prohibited due to the serious potential negative impacts on public health and on the environment.
3. Incineration of any type should be phased out as soon as practical, primarily due to the potential emissions of unacceptably high concentrations of toxic compounds such as dioxins, furans, and heavy metals and also due to the release of greenhouse gases (GHGs).
4. Pooling of resources should be explored for purposes of treating health care wastes generated by under-financed facilities such that the wastes are treated at better financed health care facilities or at treatment sites that have the requisite equipment, trained operators, and ancillary equipment.
In addition, the following specific recommendations are made aimed at three geographical areas: urban areas, rural areas, and small island communities. These recommendations are broadly subdivided such that they fall into two strategies: short- and long-term. Short-term strategies are urgently needed to address existing conditions. On the other hand, long-term strategies are proposed for the establishment of comprehensive, achievable, and practical goals for appropriate solid waste management and to put into practice a series of actions to achieve the goals.
Urban Areas The authors are well aware that there are many urban areas in developing countries that lack sufficient financial, human, and other resources and consequently the implementation of modern, non-combustion technologies for the treatment of health care wastes are not currently feasible nor practical. Where such technologies are not feasible, in the short-term, infectious and hazardous wastes should be properly isolated, stored, transported, and disposed in a special cell in a land disposal site. The cell must be properly lined with a material that will control leachate migration. Procedures should be put into place to make every effort to keep the moisture content of the wastes to a minimum. In the event that it is difficult to keep the moisture content low, then another waste (for example, one containing relatively high concentrations of paper products) can also be placed in the cell to absorb the excess moisture. The wastes should be covered immediately upon discharge into the cell. Furthermore, the entire area should be fenced off and clearly identified in order to prevent access by unauthorized personnel.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 62
In the long-term, the management of health care wastes in urban areas should be based on a general reduction on the use of incineration and a shift to non-combustion technologies as soon as practical. Proven non-combustion technologies include: autoclaves, chemical treatment, and microwave units. As indicated in other sections of this report, all of these technologies do not reduce the mass of the waste that requires disposal and thus a sound final disposal system (such as a sanitary landfill) must be in place. Furthermore, if technologies that rely on chemical treatment are considered, facility staff should make certain that a proper method for the treatment of the liquid residue from the system is operational. Emphasis should be placed on the use of centralized facilities strategically located such that potential negative impacts to the public and to the environment are maintained to a minimum. The centralized facilities must be developed in conjunction with a safe and reliable collection system.
Rural Areas Most rural areas are relatively isolated, consequently, in the short-term, infectious and potentially infectious wastes generated in rural areas can be disposed on the land or incinerated. Land disposal can be carried out in pits (lined with an impermeable material or composed of cement, as described in another section of this report) and following careful siting criteria (i.e., as far away from human receptors, at least 1.5 m above the groundwater table, and at least 200 m away from any source of water supply). This recommendation is based on the assumption that most clinics or health posts in rural areas would not generate large quantities of infectious wastes. If necessary, the wastes in these areas can also be incinerated provided that the combustion is conducted in a "controlled air" incinerator, which would be able to reach sufficiently high temperatures and detention times to keep toxic emissions to a minimum. Similarly to the land disposal site, the incinerator should be located as far away from human receptors as possible (such as children and the elderly), consider the local meteorology (i.e., wind direction), use the proper stack height, consider other factors, and must be operated by properly trained personnel using personal safety equipment. Manufacturers of the combustion units should demonstrate the performance and durability of the incinerators prior to the sale. The ash that results from the combustion process should be disposed in a lined pit or in a sanitary landfill. Ash must be managed in such a way that additional emissions during handling, transport, and final disposition are kept to a minimum. In the long-term, rural areas should make every effort to use non-combustion technologies or to establish a means to safely transport the wastes to centralized treatment facilities.
Small Island Communities These communities generally have very fragile ecosystems that must be carefully protected. In particular, efforts must be made to protect the sources of water supply (surface and underground). Furthermore, with a few minor exceptions, land on islands is a very important resource that must be protected and conserved.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 63
In the short-term, and recognizing the limitations faced by a great number of small island communities in the Western Pacific region, the wastes can be incinerated or disposed on the land. Incineration should be conducted in "controlled air" incinerators, which would be able to reach sufficiently high temperatures and detention times to keep toxic gaseous emissions to a minimum. The incinerators should be located as far away from human receptors as possible and must be operated by properly trained persons using safety equipment. Site selection for the incinerators should be carefully conducted, taking into consideration the location of sensitive human receptors, meteorological conditions, as well as geological, hydrological, and other factors. Manufacturers of these units should be required to demonstrate the performance and durability of the incinerators prior to the sale. Ash from the combustion device should be disposed in a lined pit or in a sanitary landfill. Ash must be managed so that additional emissions during handling, transport, and final disposition are reduced. Concerted efforts should be made to find suitable alternatives to incineration (such as transport to the nearest treatment facility). Land disposal can be carried out in pits (preferably composed of cement), as described in another section of this report, and following careful siting criteria (i.e., as far away from human receptors, at least 1.5 m above the groundwater table, and at least 200 m away from any source of current or potential water supply). In the long-term, the most appropriate technologies for the treatment of infectious wastes include autoclave and microwave. Chemical treatment is not recommended for small island countries unless a reliable method for managing the liquid residue from the treatment is in place and operating properly. In the event that there is a wastewater treatment system in operation, the manufacturer or the designer of the system should be contacted in order to ascertain if the system is capable of accepting and treating the effluents from the chemical treatment process. Autoclaves and microwaves should be installed in a central location so that more than one entity can avail of the services (a suitable means of collecting and transporting the wastes must be designed and implemented). In addition, a reliable method for final disposition of the wastes should be incorporated in the design.
Relevant International Conventions and Protocols In addition to the specific national and local laws and regulations that each country or region must follow, there are a number of international conventions and protocols that have an important impact on the management of health care wastes. Some of these agreements are summarized in the following paragraphs and include some of the pertinent sections. For more details on each of the agreements, the reader is invited to review the documentation and information prepared for the agreements.
Stockholm Convention (2001) The Stockholm Convention is a global treaty to protect human health and the environment from persistent organic pollutants (POPs). Persistent Organic Pollutants are chemicals that have the following characteristics: 1) remain unchanged in the environment for long periods of time, 2)

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 64
become widely distributed geographically, 3) accumulate in the fatty tissue of living organisms, and 4) are toxic to humans and wildlife. POPs circulate globally and can cause damage wherever they travel. In implementing the Convention, Governments will take measures to eliminate or reduce the release of POPs into the environment. The Convention was signed in May 22 to 23 2001 in Stockholm, Sweden. Some of the clauses of this convention that are relevant to this assessment include: The Parties included in Annex I of the convention agree to, individually or jointly, ensure that their aggregate anthropogenic carbon dioxide-equivalent emissions of the greenhouse gases listed in Annex A do not exceed their assigned amounts, calculated pursuant to their quantified emission limitation and reduction commitments inscribed in Annex B and in accordance with the provisions of this Article, with a view to reducing their overall emissions of such gases by at least 5 per cent below 1990 levels in the commitment period 2008 to 2012. Each Party included in Annex I shall, by 2005, have made demonstrable progress in achieving its commitments under this Convention. Greenhouse gases listed in Annex A of the Convention include:
• carbon dioxide (CO2); • methane (CH4); • nitrous oxide (N2O); • hydrofluorocarbons (HFCs); • perfluorocarbons (PFCs); and • sulfur hexafluoride (SF6).
Some of the relevant categories of the sectors or sources of green house gases include:
• fuel combustion; • manufacturing industries and construction; • transport; • fugitive emissions from fuels; • solid fuels; • oil and natural gas; • consumption of halocarbons and sulphur hexafluoride; • solvent and other product use; • waste; • solid waste disposal on land; • wastewater handling; and • waste incineration.
In addition, Annex C of the Protocol deals with Unintentional Production of some POPs. The annex specifically applies to Polychlorinated dibenzo-p-dioxins and dibenzofurans (PCDD/PCDF), Hexachlorobenzene (HCB), and Polychlorinated biphenyls (PCBs). These compounds are unintentionally formed and released from thermal processes involving organic matter and chlorine as a result of incomplete combustion or chemical reactions. Several

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 65
industrial source categories have been identified as having the potential for comparatively high formation and release of these chemicals to the environment. The most relevant source to this presentation is: waste incinerators, including co-incinerators of municipal, hazardous, or medical waste, or of sewage sludge. Relevant source categories include: open burning of waste, including burning of landfill sites; firing installations for wood and other biomass fuels; crematoria; and destruction of animal carcasses.
Montreal Protocol on Substances that Deplete the Ozone Layer (1987) The Montreal Protocol was adopted in Montreal, Canada on 16 September 1987 and subsequently adjusted and amended. Negotiations to reach agreement on the Protocol were very delicate and this is reflected in the final agreement. The final agreement contains clauses to cover the special circumstances of several groups of countries, especially developing countries with low consumption rates that do not want the Protocol to hinder their development. However, the Protocol is constructively flexible: it can be made more stringent or "adjusted" as the scientific evidence strengthens, without having to be completely renegotiated. Indeed, it sets the "elimination" of ozone-depleting substances as its "final objective." The Protocol came into force, as agreed, on January 1, 1989. At that time, 29 countries and the EEC representing approximately 82% of world consumption had ratified it. Since then, several other countries have joined. The Protocol was only a first step, as was realized at the time. Once it was agreed, events developed with astonishing speed. New scientific evidence showed that very much tighter and greater controls would be needed, and Governments and industry moved further, and faster, than anyone would have believed possible.
Convention on Long-Range Transboundary Air Pollution (1979) The history of the Convention on Long-Range Transboundary Air Pollution goes back to the 1960s, when scientists first demonstrated the interrelationship between sulfur emissions in continental Europe and the acidification of Scandinavian lakes. The 1972 United Nations Conference on the Human Environment in Stockholm signaled the start for active international cooperation to combat acidification. Between 1972 and 1977, several studies confirmed the hypothesis that air pollutants could travel thousands of kilometers before deposition and damage occurred. This also implied that international cooperation was necessary to solve problems such as acidification. In response to these serious problems, a High-level Meeting within the Framework of the ECE on the Protection of the Environment was held at the ministerial level in November 1979 in Geneva. The meeting resulted in the signing of the "Convention on Long-range Transboundary Air Pollution by 34 Governments and the European Community (EC).� The Convention was the first international legally binding instrument to deal with problems of air pollution on a broad regional basis. Besides laying down the general principles of international cooperation for air pollution abatement, the Convention sets up an institutional framework bringing together research and policy.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 66
The Convention is one of the central means for protecting our environment. It has, over the years, served as a bridge between different political systems and as a factor of stability in years of political change. It has substantially contributed to the development of international environmental law and has created the essential framework for controlling and reducing the damage to human health and the environment caused by transboundary air pollution. The Convention on Long-range Transboundary Air Pollution entered into force in 1983 and has been extended by the following eight protocols:
• The 1999 Protocol to Abate Acidification, Eutrophication, and Ground level Ozone, 31 Signatories and 6 ratifications. Not yet in force.
• The 1998 Protocol on Persistent Organic Pollutants (POPs), 36 Signatories and 17 ratifications. Will enter into force on 23 October 2003.
• The 1998 Protocol on Heavy Metals; 36 Signatories and 15 ratifications. Not yet in force.
• The 1994 Protocol on Further Reduction of Sulfur Emissions, 25 Parties. Entered into force 5 August 1998.
• The 1991 Protocol concerning the Control of Emissions of Volatile Organic Compounds or their Transboundary Fluxes, 21 Parties. Entered into force 29 September 1997.
• The 1988 Protocol concerning the Control of Nitrogen Oxides or their Transboundary fluxes; 28 Parties. Entered into force 14 February 1991.
• The 1985 Protocol on the Reduction of Sulfur Emissions or their Transboundary Fluxes by at least 30 per cent; 22 Parties. Entered into force 2 September 1987.
• The 1984 Protocol on Long-term Financing of the Cooperative Program for Monitoring and Evaluation of the Long-range Transmission of Air Pollutants in Europe (EMEP); 40 Parties. Entered into force 28 January 1988.
The United Nations Framework Convention on Climate Change
Background Due to concerns that a variety of human activities are resulting in an increase in concentrations of greenhouse gases in the atmosphere, most nations of the world joined together to sign the United Nations Framework Convention on Climate Change (UNFCCC) in 1992. The UNFCC included a legally non-binding, pledge that by the year 2000 the major industrialized nations would voluntarily reduce their greenhouse gas emissions to 1990 levels. However, as additional data were collected on the impact had on global climate systems due to human activities, which would possibly cause a warming of the Earth. The warming of the Earth could result in major impacts such as a rise of the sea level, changes in weather patterns and health effects. Furthermore, it became apparent that major nations such as the United States and Japan would not meet the voluntary stabilization target by 2000. As such, in 1995 Parties to the treaty decided to enter into negotiations on a protocol to establish legally binding limitations or reductions in emissions of greenhouse gases. It was decided by the Parties that this round of

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 67
negotiations would establish limitations only for the industrialized countries (those listed in Annex I to the UNFCCC, including the former Communist countries, and referred to as "Annex I countries." Developing countries are referred to as "non-Annex I countries."). During negotiations that preceded a meeting in Kyoto, Japan from December 1 to 11, 1997, little progress was made, and the most difficult issues were not resolved until the final hours of the Conference. There was wide disparity among key players especially on three items: 1) the amount of binding reductions in greenhouse gases to be required, and the gases to be included in these requirements; 2) whether or not developing countries should be part of the requirements for greenhouse gas limitations; and 3) whether or not to allow emissions trading and joint implementation, which allow credit to be given for emissions reductions to a country that provides funding or investments in other countries that bring about the actual reductions in those other countries or locations where they may be cheaper to attain. Following completion of the Protocol in December of 1997, details of a number of the more difficult issues remained to be negotiated and resolved. At the fourth Conference of the Parties (COP-4) held from November 2 to 13, 1998, in Buenos Aires, Argentina, it was apparent that these issues could not be resolved as had been expected during this meeting. Instead, parties established a two-year "Buenos Aires action plan" to deal with these issues, with a deadline for completion now set at the end of 2000 or in early 2001--at COP-6.
Major Provisions of the Kyoto Protocol The Kyoto Protocol was opened for signature March 16, 1998, for one year, and would enter into force when 55 nations have ratified it, provided that these ratifications include Annex I Parties that account for at least 55% of total carbon dioxide emissions in 1990. This provision is likely to be hard to meet in the absence of U.S. ratification. On November 12, 1998, the United States signed the Protocol, in part because the Clinton Administration wanted to revitalize what was seen as some loss of momentum during COP-4. As of February 2000, 84 countries had signed the treaty, including the European Union and most of its members, Canada, Japan, China, and a range of developing countries. Some 22 countries were reported by the UNFCCC Secretariat to have ratified the treaty. Nations are not subject to its commitments unless they have ratified it and it enters into force.
Status of Signatories & Ratification of the Convention The text of the Convention was adopted at the UN Headquarters in New York on May 9, 1992. It was open for signature at the Earth Summit in Rio de Janeiro from 4 to 14 June 1992, and thereafter at the UN Headquarters, from June 20 1992 to June 19 1993. By June 19, 1993, the Convention had received 166 signatures. The Convention entered into force on March 21 1994. Those States that have not signed the Convention may accede to it at any time. For those States that ratify, accept or approve the Convention or accede thereto after the date of entry into force, the Convention shall enter into force on the ninetieth day after the date of the deposit by such State of its instrument of ratification, acceptance, approval or accession.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 68
The Convention currently has received 188 instruments of ratification.
The Kyoto Protocol
Status of the Kyoto Protocol The text of the Protocol to the UNFCCC was adopted at the third session of the Conference of the Parties to the UNFCCC in Kyoto, Japan, on 11 December 1997. The Protocol was opened for signature from March 16 1998 to March 15 1999 at the UN Headquarters. As of February 2000, 84 countries had signed the treaty, including the European Union and most of its members, Canada, Japan, China, and a range of developing countries. Those Parties that have not as yet signed the Kyoto Protocol may accede to it at any time. The Protocol is subject to ratification, acceptance, approval, or accession by Parties to the Convention. The Protocol would enter into force on the ninetieth day after the date on which not less than 55 Parties to the Convention, incorporating Annex I Parties which accounted in total for at least 55% of the total carbon dioxide emissions for 1990 from that group, have deposited their instruments of ratification, acceptance, approval or accession. The six gases covered by the Protocol are carbon dioxide (CO2), methane (CH4), nitrous oxide (N2O), hydrofluorocarbons (HFCs), perfluorocarbons (PFCs), and sulfur hexafluoride (SF6). Each of these gases has very specific properties, and the overall emissions reduction targets for the six gases are weighted by the relative heat-trapping effect of each gas. The most prominent of all these gases, and perhaps the most pervasive in human economic activity is carbon dioxide. Carbon dioxide is produced when wood or fossil fuels such as oil, coal, and gas are burned. The major commitments in the treaty on the most controversial issues are:
• Emissions Reductions; • Developing Country Responsibilities; and • Emissions Trading and Joint Implementation.
As of 29 September 2003, 84 Parties have signed and 119 Parties have ratified or acceded to the Kyoto Protocol. Following is a list of the countries or regions that have ratified the Protocol:
• Czech Republic: Ratified November 2001; • Romania: Ratified March 2001; • European Union: Ratified May 2002; • Japan: Ratified June 2002; • Russia: Officially declared intention to ratify; and • Poland: Officially declared intent to ratify.
Total: 55.5% Complete Text of the Kyoto Protocol to the United Nations Framework Convention on Climate Change can be found at the following website: unfccc.int/resource/convkp.html.
Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 69
References Acurex Corp., Guidance on Setting Permit Conditions and Reporting Trial Burn Results, EPA/625/6-89/019, January 1989.
Adan, B.L., V.P. Cruz, and M. Palaypay, in Metro Manila Solid Waste Management Study, Draft Final Report, Volumes I and II, Norconsult A.S.; Cal Recovery Systems, Inc.; Engineering Science; Test Consultants, Inc.; DCCD Engineering Corporation; and Philnor Consultants and Planners, Inc. prepared for the Metropolitan Waterworks and Sewerage System, Manila, Philippines, July 7, 1982.
Air Resources Board, State of California, Proposed Dioxins Control Measure for Medical Waste Incinerators, Staff Report, prepared by Stationary Source Division, May 25, 1990.
Alvim-Ferraz, M. and S. Afonso, �Incineration of Different Types of Medical Wastes: Emission Factors for Particulate Matter and Heavy Metals,� Environmental Science & Technology, Vol. 37, No. 14, 2003.
Asian Development Bank, Metro Manila Solid Waste Management Project [TA 3848-PHI], Final Report, Volume 8, Medical Waste Management, September 2003.
Aulenbach, D.B., T.P. Glavin, and J.A.R. Rojas, �Protracted recharge of treated sewage into sand, Part I, Quality changes in vertical transport through sand,� Groundwater, 12:161-169, 1974.
Barker, J.F., �Volatile aromatic and chlorinated organic contaminants in groundwater at six Ontario landfills,� Water Pollut. Res. J. Can., 22(1):33-48, 1987.
Belgiorno, V., G. De Feo, C. Della Rocca, and R.M.A. Napoli, �Risk Assessment of Solid Waste Landfill,� Proceedings Sardinia 2003, Ninth International Waste Management and Landfill Symposium, Cagliari, Italy, October 2003.
Bell, D.M., �Occupational Risk of Human immunodeficiency virus infection in health care workers: an overview,� Am J Med., 102 suppl. 5B: 9-15, 1997.
Borden, R.C. and T.M. Yanoschak, �Ground and surface water quality impacts of North Carolina sanitary landfills,� Water Res. Bull., 26(2):269-277, 1990.
Butt, T.E. and K.O.K. Oduyemi, �A holistic approach to Concentration Assessment of hazards in the risk assessment of landfill leachate,� Environment International, 28:597-608, 2002.
California Environmental Protection Agency, Air Resources Board, Survey of Medical Waste Incinerators and Emissions Control, Volume I, Final Report, Contract No. A832-155, January 1992.
CalRecovery, Inc., Guidance for Landfilling Waste in Economically Developing Countries, in association with the U.S. Environmental Protection Agency, the International Solid Waste Association (ISWA), and U.S. Technology for International Environmental Solutions, 1998.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 70
CalRecovery, Inc., Medical Waste Incinerator Testing Study, Final Report, prepared for World Health Organization, June 2002.
CCOHS, Canadian Center for Occupational Health and Safety, Needlestick injuries, October 2000 (accessed at http://www.ccohs.ca/oshanswers/diseases/needlestick_injuries.html, September 2003).
Cimino, J.A., �Health and safety in the solid waste industry,� American Journal of Public Health, 65:38-46, 1975.
Clark, C.S., G.L. Van Meer, A.B. Bjornson, C.A. Linnemann, G.M. Schiff, and P.S. Gartside, Incidence of viral infections among waste collection workers, Cincinnati, Ohio, University of Cincinnati Medical Center, Institute of Environmental Health, Kettering Laboratory, 1979.
Clément, B. and G. Merlin, �The contribution of ammonia and alkalinity to landfill leachate toxicity to duckweed,� Sci. Tot. Environ., 170:71-79, 1995.
Cole, E.C., K.E. Leese, and R.M. Hall, Evaluation of Potential Biological Emissions from Alternative Medical Waste Treatment Technologies, prepared for U.S. EPA, Contract No. 68-WO-0032, July 1993.
Cooper, R.C., et al., Effect of Disposable Diapers on the Composition of Leachate from a Landfill, SERL Report No. 74-3, Sanitation Engineering Research Laboratory, University of California, Berkeley, pg. 97, 1974.
Diaz, L.F. Manejo de Residuos de Establecimientos de Salud en Guayaquil, Ecuador, (Management of Health Care Wastes in Guayaquil, Ecuador), Pan American Health Organization, January 2001.
Diaz, L.F., R.C. Cooper, L.P. Scarpace, G.J. Trezek, and C.G. Golueke, Public Health Aspects of Composting Combined Refuse and Sludge and of the Leachates Therefrom, Final Report, prepared for California Solid Waste Management Board, September 1977.
Donnelly, J.A., P.V. Scarpino, and D. Brunner, �The survival of bacterial indicators in lysimeters and landfills,� Water Sci. Technol., 14:1558-1559, 1982.
Driver, J.H., H.W. Rogers, and L.D. Claxton, �Metagenicity of Combustion Emissions from a Biomedical Waste Incinerator,� Waste Management, 10:177-183, 1990.
Environmental Control Center Company (The), Ltd., Report on “Testing of the emissions from two incinerators and one open pit in Cambodia,” Reference data, prepared for World Health Organization, September 2001.
EX Corp., Risk Evaluation of Dioxin Emission by Incineration of Syringes and Needles, Report prepared for the WHO, undated.
Först, C., L. Stieglitz, W. Roth, and S. Kuhmünch, �Quantitative analysis of volatile organic compounds in landfill leachates,� Int. J. Environ. Anal. Chem., 37:287-293, 1989.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 71
Garland, G.A. and D.C. Mosher, �Leachate effects of improper land disposal,� Waste Age, 6(42-48, 1975.
Gellin, G.A. and M.R. Zavon, Occupational dermatoses of solid waste workers, Arch. Environmental Health, 20:510-515, 1970.
Gerberding, J.L., Management of occupational exposures to blood-borne viruses, N. Engl J Med, 332:444-451, 1995.
Hickman, D.C., Cadmium and Lead in Bio-Medical Waste Incinerators, Master of Science Thesis, University of California, Davis, 1987.
Hutin, Y. A. Hauri, L. Chiarello, M. Catlin, B. Stilwell, T. Ghebrehiwet, J. Garner and the Members of the Injection Safety Best Practices Development Group, "Best infection control practices for intradermal, subcutaneous, and intramuscular needle injections", Bulletin of the World Health Organization, 81 (7): 491-500, 2003.
Idris, A. and K. Saed, �Characteristics of slag produced from incinerated hospital waste,� Journal of Hazardous Materials, 201-208, 2002.
Ippolito, G., V. Puro, G. De Carli, and the Italian Study Group on Occupational Risk of HIV infection, �The risk of immunodeficiency virus infection in health care workers: Italian multicenter study,� Arch Intern Med, 153:1451-1458, 1993.
Jones, K.H. and C.S. Konheim, A comparative life cycle risk assessment of regulated medical waste incineration and thermal treatment, Air & Waste Management Association, 87th Annual Meeting 94-RA123A.04, 1994.
Kamiya, A., Y. Ose, and Y. Sakagami, �The mutagenicity of refuse leachate from a municipal incinerator, Sci. Total Environ., 78:131-145, 1989.
Khare, M. and N.C. Dondero, �Fractionation and concentration from water of volatiles and organics on high vacuum system: Examination of sanitary landfill leachate,� Environ. Sci. Technol., 11(8):814-819, 1977.
Kjeldsen, P., M.A. Barlaz, A.P. Rooker, A. Baun, A. Ledin, and T.H. Christensen, �Present and long-term composition of MSW landfill leachate: A review,� Critical Review Env. Sci. Tech., 32:297-336, 2002.
Klafka, S. and M. Tierney, �Pathogen Survival at Hospital/Infectious Waste Incinerators,� Proceedings: Hospital/Infectious Waste Incineration and Hospital Sterilization Workshops, San Francisco-Baltimore, May 1988.
Lambolez-Michel, L., T. Gisbert, H. Billard, and J. Miralves, �Analysis of Atmospheric Pollutants from Two Municipal Solid Waste (MSW) Landfills: Determination of Exposure Levels and Research of Possible Effects on Human�s Health,� Proceedings Sardinia 2003, Ninth International Waste Management and Landfill Symposium, Cagliari, Italy, October 2003.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 72
Lance, J.C., �Fate of Pathogens in Saturated and Unsaturated Soils,� 1977 National Conference on Composting of Municipal Residues and Sludges, August 1977.
Leem, J.-H., Y.-C. Hong, K.-H. Lee, H.-J. Kwon, Y.-S. Chang, and J.-Y. Jang, �Health Survey on Workers and Residents Near the Municipal Waste and Industrial Waste Incinerators in Korea,� Industrial Health, National Institute of Industrial Health, Japan, Vol. 41, No. 3, 181-188, July 2003.
Lemieux, P.M., C.C. Lutes, J.A. Abbott, and K.M. Aldous, �Emissions of Polychlorinated Dibenzo-p-dioxins and Polychlorinated Dibenzofurans from the Open Burning of Household Waste in Barrels,� Environ. Sci. & Technol., 34:377-384, 2000.
Lombardi, F., T. Mangialardi, L. Piga, and P. Sirini, �Mechanical and leaching properties of cement solidified hospital solid waste incinerator fly ash,� Waste Management, 18:99-106, 1998.
McKay, G., �Dioxin characterization, formation and minimization during municipal solid waste (MSW) incineration: review,� Chemical Engineering Journal, 86:343-368, 2002.
Marttininen, S.K., R.H. Kettunen, K.M. Sormunen, R.M. Soimasuo, and J.A. Rintala, �Screening of physical-chemical methods for removal of organic material, nitrogen and toxicity from low strength landfill leachates,� Chemosphere, 46:851-858, 2002.
Meyer, J.E., Tutorials in Microbiology, Chemical Control of Microorganisms: Sterilization and Disinfection, 1997.
Ministerio de Salud, Direccion General de Salud Ambiental, Diagnostico Situacional del Manejo de los Residuos Solidos de Hospitales Administrados por el Ministerio de Salud (Diagnostic of the Current Situation of the Management of Solid Wastes from Hospitals Administered by the Ministry of Health), Lima, Peru, 1995.
Mitsui, T., K. Iwano, K. Masuko, C. Yamazaki, H. Okamoto, F. Tsuda, T. Tanaka, and S. Mishiro, �Hepatitis C virus infection in medical personnel after needlestick accident,� Hepatology, 16:1109-14, 1992.
Murray, J.P., J.V. Rouse, and A.B. Carpenter, �Groundwater contamination by sanitary landfill leachate and domestic wastewater in carbonate terrain: Principal source diagnosis, chemical transport characteristics and design implications,� Water Res., 15(6):745-757, 1981.
NaSH, The National Surveillance System for Hospital Care Workers, Summary Report for data collected from June 1995 through July 1999 (accessed at http://www.cdc.gov/ncidod/hip/nash/report99.PDF, September 2003).
Nath, K.J., et al., �Socio-economic and health aspects of recycling of urban solid wastes through scavenging,� All India Institute of Hygiene and Public Health, Calcutta, 1990.
NIOSH (National Institute for Occupational Safety and Health), Control of Aerosol (Biological and Non-biological) and Chemical Exposures and Safety Hazards in Medical Waste Treatment Facilities, Washington D.C., November 1997.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 73
Olson, R.W., A comparison between the emissions of 1993 permitted medical waste incinerator and a steam decontamination device, Air & Waste Management Association, 88th Annual Meeting, 95-TA40.06, 1995.
Öman, C., M. Malmberg, and C. Wolf-Watz, �Utveckling av metoder för karakterisering av lakvatten från avfallsupplag - Slutrapport,� RVF rapport 00:3, 2000.
Pahren, H.R., �Microorganisms in municipal solid waste and public health implications,� CRC Crit. Rev. Environ. Contam., 17(3):187-228, 1987.
Prüss, A., E. Giroult, and P. Rushbrook, Safe Management of wastes from health-care activities, World Health Organization, Geneva, 1999.
Puro V., G. De Carli, N. Petrosillo, G. Ippolito, �Risk of exposure to bloodborne infection for Italian health care workers, by job category and work area,� Studio Italiano Rischio Occupazionale da HIV Group, Infect. Control Hosp. Epidemiology, 22(4):206-10, 2001.
Romea S., et al., �Risk of occupational transmission of HIV infection among health care workers,� Study in a Spanish hospital, European Journal of Epidemiology, 11:225-9, 1995.
Savage, G.M., D.L. Bordson, and L.F. Diaz, �Important Issues Related to Air Pollution at Municipal Solid Waste Facilities,� presented at 25th Annual Governmental Refuse Collection and Disposal Association (GRCDA) Conference in St. Paul, Minnesota, August 1987, Environmental Progress, 7(2):123-130, May 1988.
Saw, C.B. and T. Hoo, Management of Hospital Wastes and Associated Risks to Health, World Health Organization, WPRO, Manila, August 1998.
Takata, T., �Survey on the Health Effects of Chronic Exposure to Dioxins and Its Accumulation on Workers of a Municipal Solid Waste Incinerator, Rural Part of Osaka Prefecture, and the Results of Extended Survey Afterwards,� Industrial Health, National Institute of Industrial Health, Japan, Vol. 41, No. 3, 189-196, July 2003.
Thompson, T.K. and J.S. Vavruska, �Design Features of the New Los Alamos Low Level Waste/Mixed Waste Incinerator,� Proceedings: The 1989 Incineration Conference, Knoxville, Tennessee, May 1989.
Torres, E.B., R.D. Subida, and L.B. Rabuco, The profile of child scavengers in Smokey Mountain, Balut, Tondo, University of Philippines College of Public Health, Manila, pp. 1-83 and annexes, 1991.
Turnberg, W., An Examination and Risk Evaluation of Infectious Waste in King County, Washington, Seattle-King County Department of Public Health, Seattle, Washington, March 1988.
Turnberg, W.L, and F. Frost, �Survey of occupational exposure of waste industry workers to infectious waste in Washington State,� American Journal of Public Health, Vol. 80, No. 10, 1262-1264, 1990.

Risks & Costs Associated with the Management of Infectious Wastes WHO/WPRO
December 2003 74
U.S. Congress, Office of Technology Assessment, Facing America’s Trash: What Next for Municipal Solid Waste?, OTA-O-425, U.S. Government Printing Office, Washington DC, October 1989.
U.S. Congress, Office of Technology Assessment, Finding the Rx for Managing Medical Wastes, OTA-O-459, Government Printing Office, Washington, DC, September, 1990.
U.S. Environmental Protection Agency, US Code of Federal Regulations, Title 40 (Protection of Environment), Volume 6, Part 60 (Standards of Performance for New Stationary Sources), Subpart Ec (Standards of Performance for Hospital/Medical/Infectious Waste Incinerators for Which Construction is Commenced After June 20, 1996), July 2003.
Waara, S., A.-S. Allard, M. Ek, and A. Svenson, "Chemical and Toxicological Characterization of Landfill Leachate After Treatment in a Pilot Scale Plant Using Different Treatment Methods,� Proceedings Sardinia 2003, Ninth International Waste Management and Landfill Symposium, Cagliari, Italy, October 2003.
Ware, S.A., A Survey of Pathogen Survival During Municipal Solid Waste and Manure Treatment Processes, EPA-600/8-80-034, August 1980.
Washburn, S.T., J. Brainard, and R.H. Harris, �Human Health Risks of Municipal Solid Waste Incineration,� Environ. Impact Assess. Rev., 9:181-198, 1989.
WHO, The World Health Report 2002: Reducing Risks, Promoting Healthy Life, World Health Organization, Geneva, Switzerland, 2002.