risk vs benefit - uk clinical pharmacy association
TRANSCRIPT

30/11/2017
1
Christina Nurmahi
Women & Newborn Lead Pharmacist
University Hospital Southampton
Why does it matter?
The Problem Manufacturers unlikely to do clinical trials in
pregnancy so we are dependent on post marketing surveillance.
Most studies are in animals - do not necessarily extrapolate to humans.
The harm may not be immediately apparent.
Other factors also contribute to fetal harm
Aims
RISK vs BENEFIT
By end of session:
be better equipped to make an informed decision
ObjectivesGain understanding of the:
The stages of fetal development and some of the risks associated with drug exposure in pregnancy
Factors that influence drug handling in pregnancy including impact of physiological changes in pregnancy
General principles of prescribing in pregnancy and how to reduce risk
Morbidity and mortality in pregnancy and the management of some of the high risk groups identified
TeratogenDefinition – a drug or other substance capable of
interfering with development of the fetus
Congenital malformation (structural or functional)
Failure of implantation of the conceptus
Miscarriage
Abnormal mental development
Development of Intra-uterine growth retardation
(IUGR)
Fetal death
30/11/2017
2
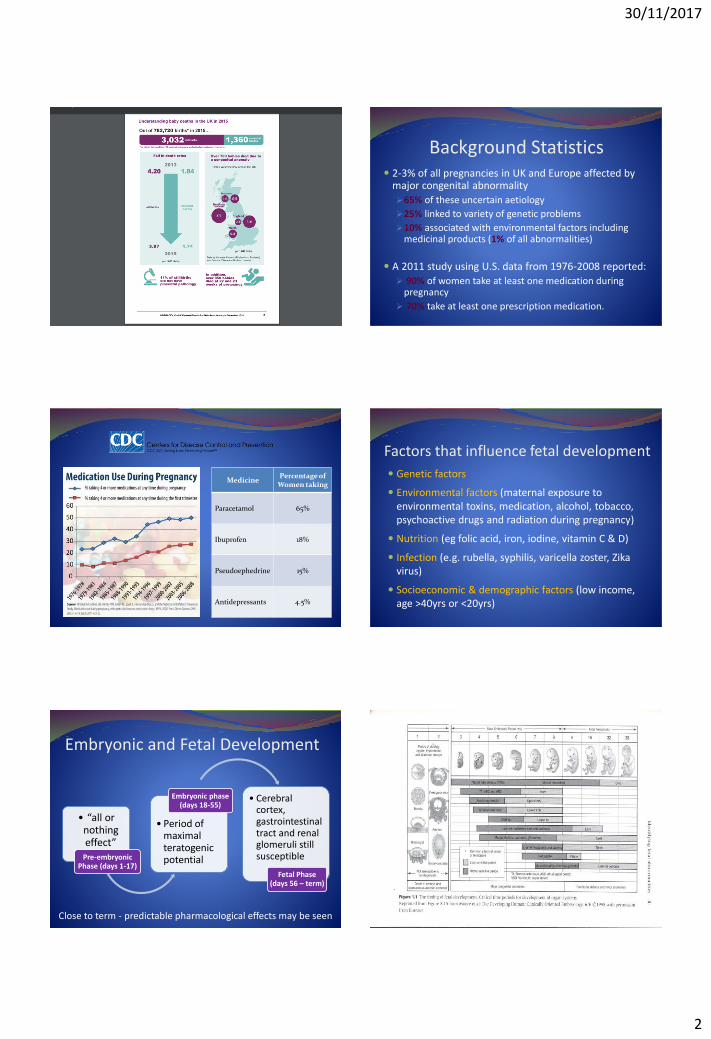
Background Statistics 2-3% of all pregnancies in UK and Europe affected by
major congenital abnormality
65% of these uncertain aetiology
25% linked to variety of genetic problems
10% associated with environmental factors including medicinal products (1% of all abnormalities)
A 2011 study using U.S. data from 1976-2008 reported:
90% of women take at least one medication during pregnancy
70% take at least one prescription medication.
MedicinePercentage of
Women taking
Paracetamol 65%
Ibuprofen 18%
Pseudoephedrine 15%
Antidepressants 4.5%
Factors that influence fetal development
Genetic factors
Environmental factors (maternal exposure to environmental toxins, medication, alcohol, tobacco, psychoactive drugs and radiation during pregnancy)
Nutrition (eg folic acid, iron, iodine, vitamin C & D)
Infection (e.g. rubella, syphilis, varicella zoster, Zikavirus)
Socioeconomic & demographic factors (low income, age >40yrs or <20yrs)
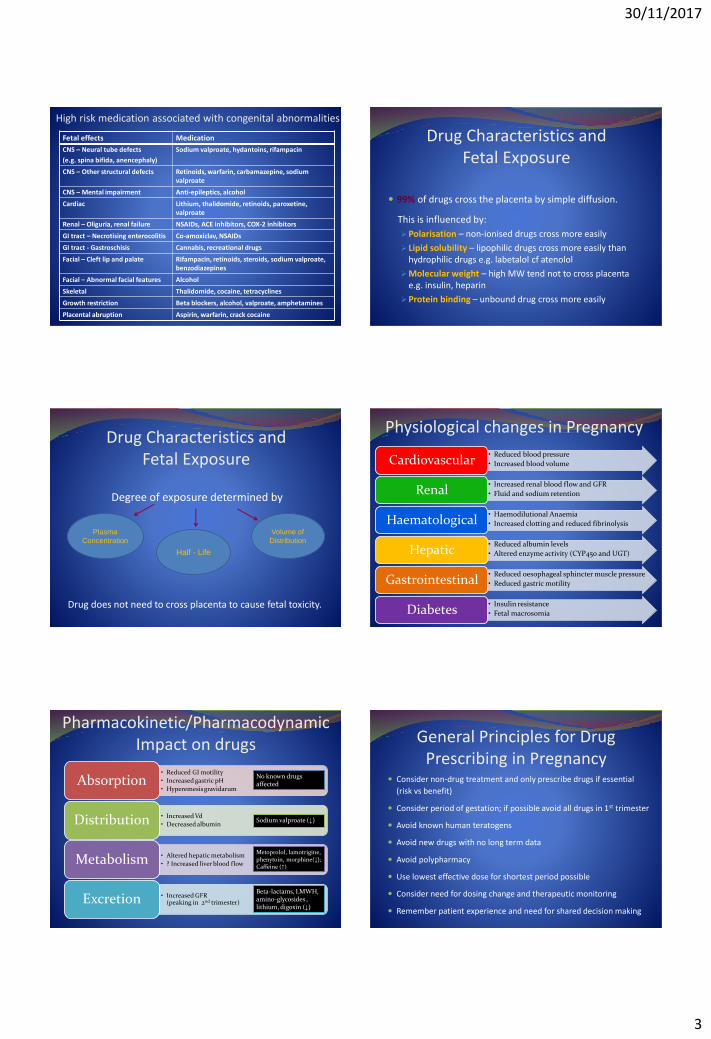
Embryonic and Fetal Development
• “all or nothing effect”
Pre-embryonic Phase (days 1-17)
• Period of maximal teratogenicpotential
Embryonic phase (days 18-55)
• Cerebral cortex, gastrointestinal tract and renal glomeruli still susceptible
Fetal Phase (days 56 – term)
Close to term - predictable pharmacological effects may be seen
30/11/2017
3
High risk medication associated with congenital abnormalities
CNS – Neural tube defects
(e.g. spina bifida, anencephaly)
Sodium valproate, hydantoins, rifampacin
CNS – Other structural defects Retinoids, warfarin, carbamazepine, sodium valproate
CNS – Mental impairment Anti-epileptics, alcohol
Cardiac Lithium, thalidomide, retinoids, paroxetine, valproate
Renal – Oliguria, renal failure NSAIDs, ACE inhibitors, COX-2 inhibitors
GI tract – Necrotising enterocolitis Co-amoxiclav, NSAIDs
GI tract - Gastroschisis Cannabis, recreational drugs
Facial – Cleft lip and palate Rifampacin, retinoids, steroids, sodium valproate, benzodiazepines
Facial – Abnormal facial features Alcohol
Skeletal Thalidomide, cocaine, tetracyclines
Growth restriction Beta blockers, alcohol, valproate, amphetamines
Placental abruption Aspirin, warfarin, crack cocaine
Fetal effects Medication Drug Characteristics and Fetal Exposure
99% of drugs cross the placenta by simple diffusion.
This is influenced by:
Polarisation – non-ionised drugs cross more easily
Lipid solubility – lipophilic drugs cross more easily than hydrophilic drugs e.g. labetalol cf atenolol
Molecular weight – high MW tend not to cross placenta e.g. insulin, heparin
Protein binding – unbound drug cross more easily
Drug Characteristics and Fetal Exposure
Degree of exposure determined by
Drug does not need to cross placenta to cause fetal toxicity.
Half - Life
Plasma
Concentration
Volume of
Distribution
Physiological changes in Pregnancy
• Reduced blood pressure
• Increased blood volumeCardiovascular
• Increased renal blood flow and GFR
• Fluid and sodium retentionRenal
• Haemodilutional Anaemia
• Increased clotting and reduced fibrinolysisHaematological
• Reduced albumin levels
• Altered enzyme activity (CYP450 and UGT)Hepatic
• Reduced oesophageal sphincter muscle pressure
• Reduced gastric motilityGastrointestinal
• Insulin resistance
• Fetal macrosomiaDiabetes
Pharmacokinetic/PharmacodynamicImpact on drugs
• Reduced GI motility
• Increased gastric pH
• HyperemesisgravidarumAbsorption
• Increased Vd
• Decreased albuminDistribution
• Altered hepatic metabolism
• ? Increased liver blood flowMetabolism
• Increased GFR (peaking in 2nd trimester)Excretion
No known drugs affected
Sodium valproate (↓)
Metoprolol, lamotrigine, phenytoin, morphine(↓); Caffeine (↑)
Beta-lactams, LMWH, amino-glycosides , lithium, digoxin (↓)
General Principles for Drug Prescribing in Pregnancy
Consider non-drug treatment and only prescribe drugs if essential
(risk vs benefit)
Consider period of gestation; if possible avoid all drugs in 1st trimester
Avoid known human teratogens
Avoid new drugs with no long term data
Avoid polypharmacy
Use lowest effective dose for shortest period possible
Consider need for dosing change and therapeutic monitoring
Remember patient experience and need for shared decision making
30/11/2017
4
Dddd indirect causes
direct causes
d
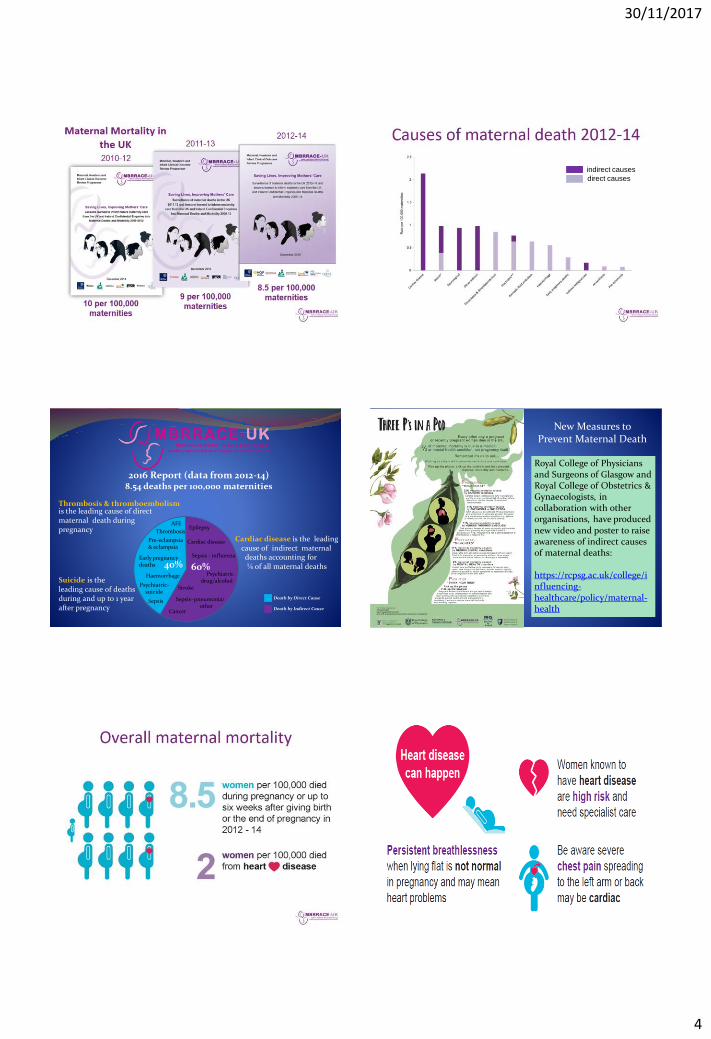
2016 Report (data from 2012-14)8.54 deaths per 100,000 maternities
Thrombosis & thromboembolismis the leading cause of direct maternal death during pregnancy
Cardiac disease is the leading cause of indirect maternal deaths accounting for ¼ of all maternal deaths
Suicide is the leading cause of deaths during and up to 1 yearafter pregnancy
Death by Direct Cause
Death by Indirect Cause
Haemorrhage
Cardiac disease
Epilepsy
Stroke
Sepsis–pneumonia/ other
Cancer
60%40%
Sepsis
Thrombosis
Pre-eclampsia& eclampsia
AFE
Early pregnancy deaths
Psychiatric-suicide
Psychiatric-drug/alcohol
Sepsis - influenza
Haemorrhage
Royal College of Physicians and Surgeons of Glasgow and Royal College of Obstetrics & Gynaecologists, in collaboration with other organisations, have produced new video and poster to raise awareness of indirect causes of maternal deaths:
https://rcpsg.ac.uk/college/influencing-healthcare/policy/maternal-health
New Measures to Prevent Maternal Death

30/11/2017
5
Cardiac DiseaseKey messages – how can we help as pharmacists?
Pre-pregnancy counselling, including dietary, smoking and contraceptive advice for women with pre-existing conditions
Lower threshold for referral and investigation of cardiac and respiratory symptoms, and chest/arm/back pain
Importance of continuing medication; restarting medicines postnatally if indicated e.g. ACE inhibitors, warfarin
Good interdisciplinary working and communication
Venous Thromboembolism 2009-2013 – 48 deaths from VTE
50% VTEs antenatally (though some died postnatally)
50% VTEs postnatally (up to 6 weeks postpartum)
83% of these women had risk factors for VTE
VTE risk assessment should be done for all women at booking, admission to hospital (up to 6 weeks postpartum), with any change in clinical situation, immediately post delivery (within 6 hours) and on discharge from hospital.
Venous ThromboembolismRoyal College of Obsteticians and Gynaecologists (RCOG)
Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium
Green-top Guideline No. 37a April 2015
Thromboembolic Disease in Pregnancy and the Puerperium: Acute Management
Green-top Guideline No. 37b April 2015

30/11/2017
6
Venous ThromboembolismProphylactic Dose of Low molecular weight heparin
*Can give BD if high prophylaxis dose required
Weight Enoxaparin dose Dalteparin dose Tinzaparin dose
<50kg 20mg OD 2500 units OD 3500 units OD
50-90kg* 40mg OD 5000 units OD 4500 units OD
91-130kg 60mg OD 7500 units OD 7000 units OD
131-170kg 80mg OD 10000 units OD 9000 units OD
>170kg 0.6mg/kg/day 75 units/kg/day 75 units/kg/day
Contraindications LMWH allergy Acute stroke within previous 4 weeks
Increased risk of major haemorrhage Active bleeding Uncontrolled BP (>200/120)
Planned delivery within 12hrs Bleeding disorder Severe liver disease with raised INR
Recent spinal anaesthesia or epidural catheter removal < 4hrs
Platelets<75 x 109/lRenal failure (Cr> 125 and rising; or eGFR<30mL/min/1.73m2)
Venous ThromboembolismTreatment dose of low molecular weight heparin
Enoxaparin 1mg/kg BD / Dalteparin 100units/kg BD *
*Insufficient evidence to recommend whether dose be given once daily or in two divided doses (RCOG 2015)
Doses titrated against woman’s booking or early pregnancy weight. Unfractionated heparin preferred for initial treatment of pulmonary embolism Treat during remainder of pregnancy and for at least 6 weeks postnatally and
until at least 3 months of treatment has been given in total.
Weight Enoxaparin dose Dalteparin dose
<50kg 40mg BD or 60mg OD 5000 units BD or 10000 units OD
50-69kg 60mg BD or 90mg OD 6000 units BD or 12000 units OD
70-89kg 80mg BD or 120mg OD 8000 units BD or 16000 units OD
90-109kg 100mg BD or 150mg OD 10000 units BD or 20000 units OD
110-125kg 120mg BD or 180mg OD 12000 units BD or 24000 units OD
>125kg Discuss with haematologist Discuss with haematologist
Venous Thromboembolism Warfarin – TERATOGEN
Avoid weeks 6-12 & week 36 onwards – give LMWH BD
Postpartum, can recommence day 5 post delivery
INR range aim for 2-3
Give vitamin K 10mg (phytomenadione) from 36 weeks till delivery once warfarin stopped
Aspirin 75mg given if Antiphospholipid syndrome (APL) + fixed dose LMWH
(give 1mg/kg OD if APL syndrome plus previous thrombosis)
NOACs Avoid in pregnancy and if breastfeeding
SepsisWomen who are pregnant, have given birth or had a termination of pregnancy or miscarriage in the last 6 weeks, are in a high risk group for sepsis. In particular, women who:
have impaired immune system because of illness or drugs
have gestational diabetes or diabetes
needed invasive procedures (for example, caesarean section, forceps delivery, removal of retained products of conception)
had prolonged rupture of membranes
have been in close contact with people with group A streptococcal infection e.g. scarlet fever
have continued vaginal bleeding or offensive vaginal discharge.(NICE Sepsis Guidelines July 2016)
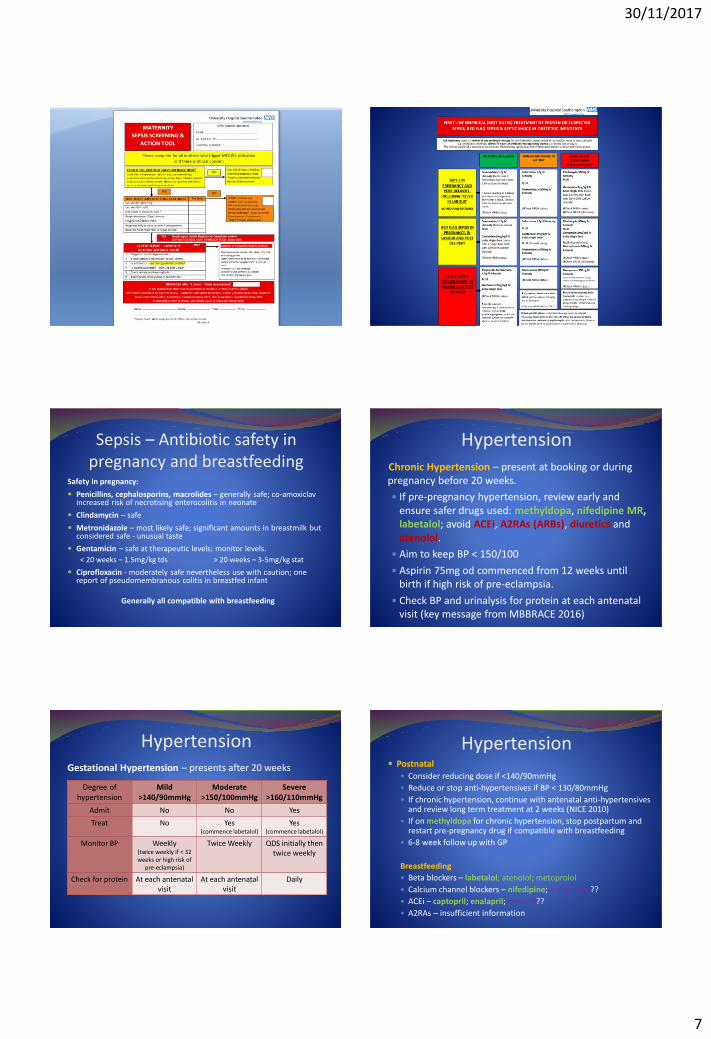
SEPSISKey actions for Doctors, Midwives and Allied Health Professionals for diagnosis and management of sepsis are:
Timely recognition and early diagnosis –‘THINK SEPSIS’
Rapid antibiotics – within 1 hr of suspected diagnosis
Review by senior doctors and midwives
30/11/2017
7
Sepsis – Antibiotic safety in pregnancy and breastfeeding
Safety in pregnancy:
Penicillins, cephalosporins, macrolides – generally safe; co-amoxiclavincreased risk of necrotising enterocolitis in neonate
Clindamycin – safe
Metronidazole – most likely safe; significant amounts in breastmilk but considered safe - unusual taste
Gentamicin – safe at therapeutic levels; monitor levels.
< 20 weeks – 1.5mg/kg tds > 20 weeks – 3-5mg/kg stat
Ciprofloxacin - moderately safe nevertheless use with caution; one report of pseudomembranous colitis in breastfed infant
Generally all compatible with breastfeeding
HypertensionChronic Hypertension – present at booking or during pregnancy before 20 weeks.
If pre-pregnancy hypertension, review early and ensure safer drugs used: methyldopa, nifedipine MR,labetalol; avoid ACEi, A2RAs (ARBs), diuretics and atenolol.
Aim to keep BP < 150/100
Aspirin 75mg od commenced from 12 weeks until birth if high risk of pre-eclampsia.
Check BP and urinalysis for protein at each antenatal visit (key message from MBBRACE 2016)
HypertensionGestational Hypertension – presents after 20 weeks
Degree of hypertension
Mild >140/90mmHg
Moderate >150/100mmHg
Severe >160/110mmHg
Admit No No Yes
Treat No Yes(commence labetalol)
Yes(commence labetalol)
Monitor BP Weekly (twice weekly if < 32 weeks or high risk of
pre-eclampsia)
Twice Weekly QDS initially then twice weekly
Check for protein At each antenatal visit
At each antenatal visit
Daily
Hypertension Postnatal
Consider reducing dose if <140/90mmHg
Reduce or stop anti-hypertensives if BP < 130/80mmHg
If chronic hypertension, continue with antenatal anti-hypertensivesand review long term treatment at 2 weeks (NICE 2010)
If on methyldopa for chronic hypertension, stop postpartum and restart pre-pregnancy drug if compatible with breastfeeding
6-8 week follow up with GP
Breastfeeding
Beta blockers – labetalol; atenolol; metoprolol
Calcium channel blockers – nifedipine; amlodipine??
ACEi – captopril; enalapril; ramipril??
A2RAs – insufficient information
30/11/2017
8
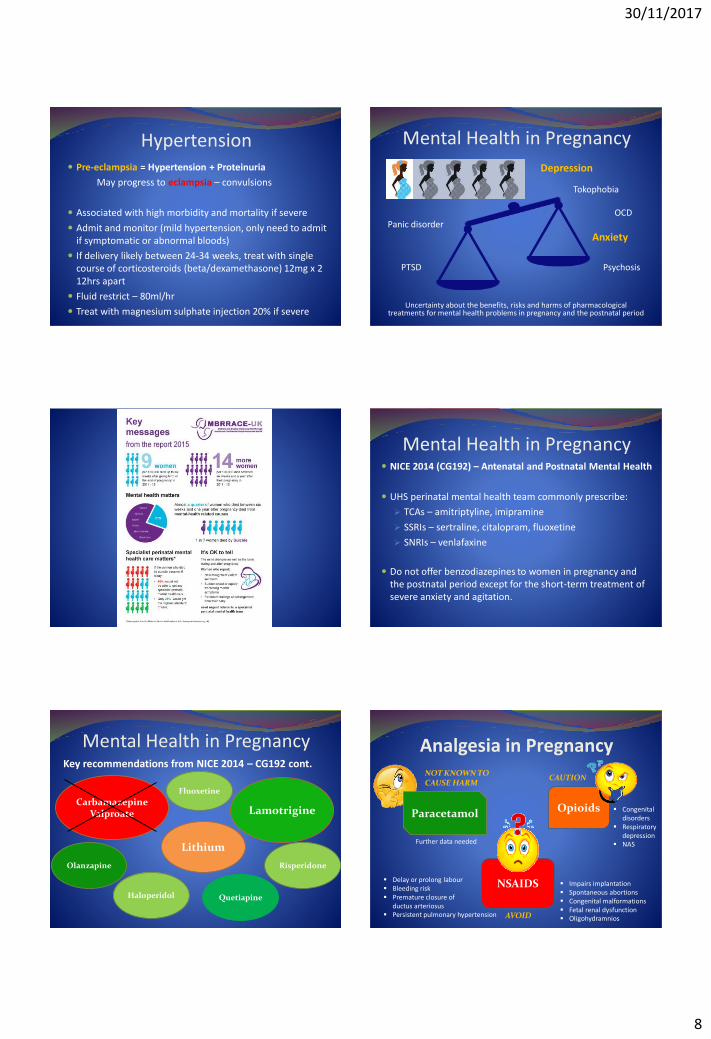
Hypertension Pre-eclampsia = Hypertension + Proteinuria
May progress to eclampsia – convulsions
Associated with high morbidity and mortality if severe
Admit and monitor (mild hypertension, only need to admit if symptomatic or abnormal bloods)
If delivery likely between 24-34 weeks, treat with single course of corticosteroids (beta/dexamethasone) 12mg x 2 12hrs apart
Fluid restrict – 80ml/hr
Treat with magnesium sulphate injection 20% if severe
Depression
Tokophobia
OCD Panic disorder
Anxiety
PTSD Psychosis
Uncertainty about the benefits, risks and harms of pharmacological treatments for mental health problems in pregnancy and the postnatal period
Mental Health in Pregnancy
Mental Health in Pregnancy NICE 2014 (CG192) – Antenatal and Postnatal Mental Health
UHS perinatal mental health team commonly prescribe:
TCAs – amitriptyline, imipramine
SSRIs – sertraline, citalopram, fluoxetine
SNRIs – venlafaxine
Do not offer benzodiazepines to women in pregnancy and the postnatal period except for the short-term treatment of severe anxiety and agitation.
Mental Health in PregnancyKey recommendations from NICE 2014 – CG192 cont.
Lithium
CarbamazepineValproate Lamotrigine
Olanzapine
Haloperidol Quetiapine
Risperidone
Fluoxetine
Analgesia in Pregnancy
NSAIDS Delay or prolong labour Bleeding risk Premature closure of
ductus arteriosus Persistent pulmonary hypertension
Impairs implantation Spontaneous abortions Congenital malformations Fetal renal dysfunction OligohydramniosAVOID
Opioids
CAUTION
Congenital disorders
Respiratory depression
NAS
NOT KNOWN TO CAUSE HARM
Paracetamol
Further data needed

30/11/2017
9
Anti-emetics Nausea and vomiting common in early pregnancy;
severe N&V can progress to hyperemesis gravidarum
Management consists of correction of fluid & electrolyte imbalances and treatment with anti-emetics
Antihistamines (promethazine, cyclizine)
Phenothiazines (prochlorperazine)
Dopamine antagonists (metoclopramide, domperidone)
Serotonin antagonists (ondansetron)
If uncontrolled hyperemesis, consider corticosteroids
If risk of Wernicke’s encephalopathy, consider thiamine
Useful ResourcesReference sources: Drugs in Pregnancy and Lactation – G. Briggs, R. Freeman, S. Yaffe
Drugs during Pregnancy and Lactation – C. Schaefer, P. Peters, R. Miller
Therapeutics in Pregnancy and Lactation – A. Lee, S. Inch, D. Finnigan
British National Formulary and BNF for children
Summary of Product Characteristics (www.emc.medicines.org.uk)
UKMI Q&A (www.ukmi.nhs.uk/activities/medicinesQAs/)
UK Teratology Service (UKTIS) (www.uktis.org or 0344-8920909)
Uktis BUMPS - http://www.medicinesinpregnancy.org/
NHS Choices - https://www.nhs.uk/Conditions/pregnancy-and-baby/Pages/medicines-in-pregnancy.aspx
http://www.motherisk.org/women/index.jsp
https://www.cdc.gov/pregnancy/meds/treatingfortwo/