right intervention, right time: managing medically complex
TRANSCRIPT

Right Intervention, Right Time: Managing Medically Complex Members
2
Medical labeling tends to oversimplify patient
health status, particularly in the case
of medically complex members. The
disproportionate impact of the high-risk,
high-cost population underscores the
importance of using strategic, specialized
care management to control the unsustainable costs attached to
treating chronic diseases — and their debilitating impact on
quality of life.
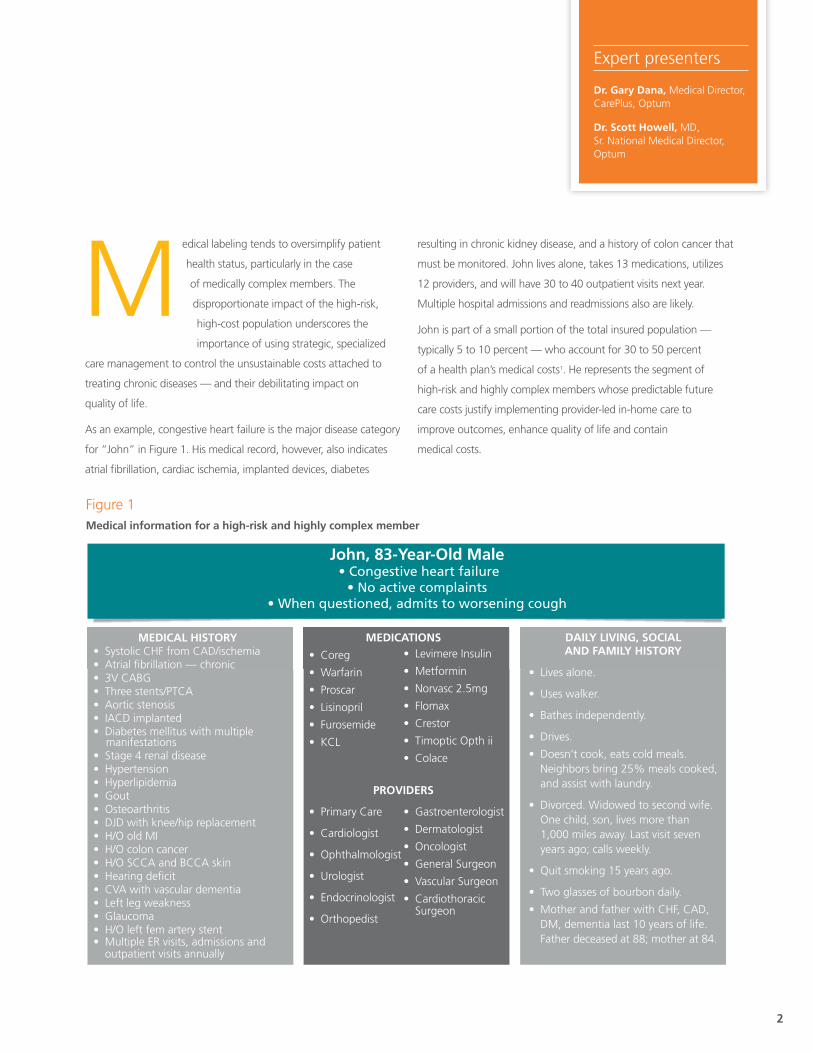
As an example, congestive heart failure is the major disease category
for “John” in Figure 1. His medical record, however, also indicates
atrial fibrillation, cardiac ischemia, implanted devices, diabetes
resulting in chronic kidney disease, and a history of colon cancer that
must be monitored. John lives alone, takes 13 medications, utilizes
12 providers, and will have 30 to 40 outpatient visits next year.
Multiple hospital admissions and readmissions also are likely.
John is part of a small portion of the total insured population —
typically 5 to 10 percent — who account for 30 to 50 percent
of a health plan’s medical costs1. He represents the segment of
high-risk and highly complex members whose predictable future
care costs justify implementing provider-led in-home care to
improve outcomes, enhance quality of life and contain
medical costs.
Expert presenters
Dr. Gary Dana, Medical Director, CarePlus, Optum
Dr. Scott Howell, MD, Sr. National Medical Director, Optum
John, 83-Year-Old Male • Congestive heart failure
• No active complaints• When questioned, admits to worsening cough
MEDICAL HISTORY• Systolic CHF from CAD/ischemia • Atrial fibrillation — chronic• 3V CABG• Three stents/PTCA• Aortic stenosis• IACD implanted• Diabetes mellitus with multiple manifestations• Stage 4 renal disease• Hypertension• Hyperlipidemia • Gout • Osteoarthritis • DJD with knee/hip replacement• H/O old MI • H/O colon cancer • H/O SCCA and BCCA skin • Hearing deficit• CVA with vascular dementia • Left leg weakness• Glaucoma• H/O left fem artery stent• Multiple ER visits, admissions and outpatient visits annually
MEDICATIONS
• Coreg
• Warfarin
• Proscar
• Lisinopril
• Furosemide
• KCL
PROVIDERS
• Primary Care
• Cardiologist
• Ophthalmologist
• Urologist
• Endocrinologist
• Orthopedist
• Levimere Insulin
• Metformin
• Norvasc 2.5mg
• Flomax
• Crestor
• Timoptic Opth ii
• Colace
• Gastroenterologist
• Dermatologist
• Oncologist
• General Surgeon
• Vascular Surgeon
• Cardiothoracic Surgeon
DAILY LIVING, SOCIALAND FAMILY HISTORY
• Lives alone.
• Uses walker.
• Bathes independently.
• Drives.
• Doesn’t cook, eats cold meals. Neighbors bring 25% meals cooked, and assist with laundry.
• Divorced. Widowed to second wife. One child, son, lives more than 1,000 miles away. Last visit seven years ago; calls weekly.
• Quit smoking 15 years ago.
• Two glasses of bourbon daily.
• Mother and father with CHF, CAD, DM, dementia last 10 years of life. Father deceased at 88; mother at 84.
Patients
• Avoid ER visits, inpatient admissions.• Reduce medications, unnecessary procedures.• Improve disease state understanding and self care.• Create closer relationships with providers.• Address advanced illness care goals including advance (directives).
• Improve patient understanding and outcomes.• Deliver timely, high-quality information.• Assistance in managing di�cult, complex patients.• Deliver preventive maintenance care, including disease education and intervention for clinical, functional, environmental, psychosocial and cultural triggers.
• Improve quality.• Lower costs for members.
Providers
HealthPlans
Heart Failure PalliativeCare/Hospice
COPDExacerbation
Urinary TractInfection
History and physical focusing on weight gain, fluid status and cardiopulmonary examination
Evaluation of current medications, adjustment as needed and provision of parenteral diuretics
Laboratory or imaging studies such as portable Chest X-ray (CXR) or blood tests
Coordination and follow-up with Primary Care Provider (PCP), nurse care manager
Primary Visiting Provider (PVP) - follow-up visits
History and physical focusing on vital signs, oxygenation status (pulse ox) andcardiopulmonary examination
Evaluation and adjustment of current medications; possible initiation of steroids
Laboratory studies such as portable CXR
Coordination and follow-up with PCP, nurse case manager
PVP follow-up visit
History and physical
Laboratory and evaluation including urinalysis and urine culture
Prescribing of oral or parenteral antibiotics
PCP notification, nurse care manager follow-up calls
PVP follow-up visit if indicated
Advance directives in place within 90 days of program enrollment
Review and adjust, or prescribe palliative care medications
Initiate hospice referral
Coordinate with PCP, nurse care manager
In-depth discussion with hospice team to determine next steps and responsible parties for ongoing management
Figure 1Medical information for a high-risk and highly complex member
3
The issue is not that a medically complex patient like John lacks
access to excellent doctors or committed caregivers. The needs of
this segment simply require heightened forms of care, collaboration
and coordination — along with specialized infrastructure and
systems — tailored to disease processes that place members in
categories like chronically high-risk, catastrophic and terminal.
Health plans use advanced analytics, predictive modeling and
referrals from primary care physicians, case managers or discharge
planners to identify and target members within their populations
who will benefit from a medically complex care delivery and
management strategy. One key selection parameter: more than
two acute admissions and two chronic conditions, or more than
eight chronic conditions.
Typical targeted disease processes include:
• COPD/chronic respiratory
• CHF/high-cost cardiac
• Frailty (end of life, MS, ALS)
• Social risk: homebound, socially isolated, transportation issues,
financial risk
• Comorbid conditions causing overutilization (anxiety,
depression, dementia)
Among members correctly identified for inclusion in a medically
complex care delivery and management program, approximately
35 percent will expire, while 50 percent slowly progress and worsen,
and 15 percent regress to the mean and can be discharged from
the program.
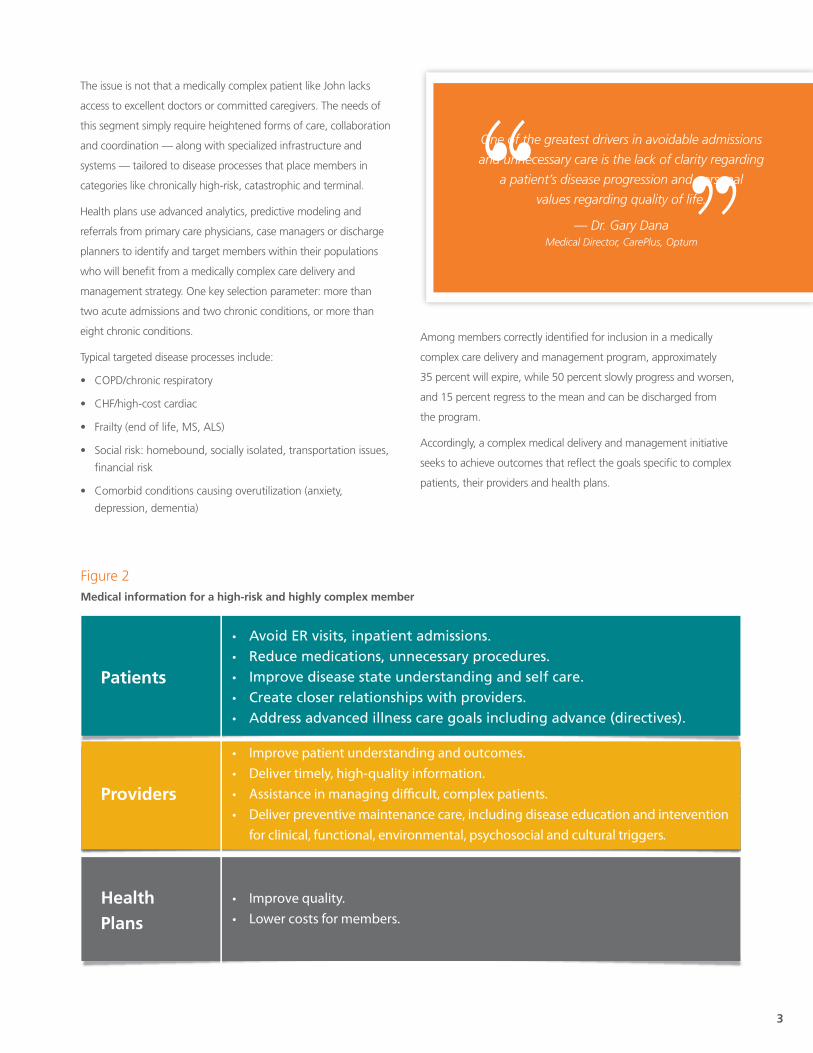
Accordingly, a complex medical delivery and management initiative
seeks to achieve outcomes that reflect the goals specific to complex
patients, their providers and health plans.
John, 83-Year-Old Male • Congestive heart failure
• No active complaints• When questioned, admits to worsening cough
MEDICAL HISTORY• Systolic CHF from CAD/ischemia • Atrial fibrillation — chronic• 3V CABG• Three stents/PTCA• Aortic stenosis• IACD implanted• Diabetes mellitus with multiple manifestations• Stage 4 renal disease• Hypertension• Hyperlipidemia • Gout • Osteoarthritis • DJD with knee/hip replacement• H/O old MI • H/O colon cancer • H/O SCCA and BCCA skin • Hearing deficit• CVA with vascular dementia • Left leg weakness• Glaucoma• H/O left fem artery stent• Multiple ER visits, admissions and outpatient visits annually
MEDICATIONS
• Coreg
• Warfarin
• Proscar
• Lisinopril
• Furosemide
• KCL
PROVIDERS
• Primary Care
• Cardiologist
• Ophthalmologist
• Urologist
• Endocrinologist
• Orthopedist
• Levimere Insulin
• Metformin
• Norvasc 2.5mg
• Flomax
• Crestor
• Timoptic Opth ii
• Colace
• Gastroenterologist
• Dermatologist
• Oncologist
• General Surgeon
• Vascular Surgeon
• Cardiothoracic Surgeon
DAILY LIVING, SOCIALAND FAMILY HISTORY
• Lives alone.
• Uses walker.
• Bathes independently.
• Drives.
• Doesn’t cook, eats cold meals. Neighbors bring 25% meals cooked, and assist with laundry.
• Divorced. Widowed to second wife. One child, son, lives more than 1,000 miles away. Last visit seven years ago; calls weekly.
• Quit smoking 15 years ago.
• Two glasses of bourbon daily.
• Mother and father with CHF, CAD, DM, dementia last 10 years of life. Father deceased at 88; mother at 84.
Patients
• Avoid ER visits, inpatient admissions.• Reduce medications, unnecessary procedures.• Improve disease state understanding and self care.• Create closer relationships with providers.• Address advanced illness care goals including advance (directives).
• Improve patient understanding and outcomes.• Deliver timely, high-quality information.• Assistance in managing di�cult, complex patients.• Deliver preventive maintenance care, including disease education and intervention for clinical, functional, environmental, psychosocial and cultural triggers.
• Improve quality.• Lower costs for members.
Providers
HealthPlans
Heart Failure PalliativeCare/Hospice
COPDExacerbation
Urinary TractInfection
History and physical focusing on weight gain, fluid status and cardiopulmonary examination
Evaluation of current medications, adjustment as needed and provision of parenteral diuretics
Laboratory or imaging studies such as portable Chest X-ray (CXR) or blood tests
Coordination and follow-up with Primary Care Provider (PCP), nurse care manager
Primary Visiting Provider (PVP) - follow-up visits
History and physical focusing on vital signs, oxygenation status (pulse ox) andcardiopulmonary examination
Evaluation and adjustment of current medications; possible initiation of steroids
Laboratory studies such as portable CXR
Coordination and follow-up with PCP, nurse case manager
PVP follow-up visit
History and physical
Laboratory and evaluation including urinalysis and urine culture
Prescribing of oral or parenteral antibiotics
PCP notification, nurse care manager follow-up calls
PVP follow-up visit if indicated
Advance directives in place within 90 days of program enrollment
Review and adjust, or prescribe palliative care medications
Initiate hospice referral
Coordinate with PCP, nurse care manager
In-depth discussion with hospice team to determine next steps and responsible parties for ongoing management
One of the greatest drivers in avoidable admissions
and unnecessary care is the lack of clarity regarding
a patient’s disease progression and personal
values regarding quality of life.
— Dr. Gary Dana Medical Director, CarePlus, Optum
Figure 2Medical information for a high-risk and highly complex member

4
One of the greatest drivers in avoidable admissions and unnecessary
care is the lack of clarity regarding a patient’s disease progression and
personal values regarding quality of life. This underdeveloped “health
literacy” on the part of all stakeholders — patients, caregivers
and family — causes inappropriate utilization, increases cost and
reduces the member’s quality of life. As a result, the core principle in
improving care for the medically complex is delivering the right care,
to the right patients, at the right time and in the right setting, often
their personal residence.
Member-centric and provider-driven health care solutions designed
for complex, high-risk populations have reduced inpatient admissions
by 40 to 50 percent while providing an average savings of $1,468
per member per month in acute care admissions.2 Successful
programs emphasize several elements critical to improving medically
complex outcomes:
• Selection of evidence-based practice guidelines, plus services
designed to facilitate patient disease management and
adherence to treatment plans.
• Regular, in-home visits to treat members where they live and
reduce exacerbations.
• High intensity through a team approach to education, telephonic
monitoring, in-home provider oversight and direct primary care/
specialist involvement.
• Frequent patient encounters with treatment team members.
• 24/7/365 patient access to care.
• Advanced data collection, analytics and reporting, including
routine reporting and feedback to providers.
• Ongoing adjustment and alignment that responds to data,
measured outcomes and evidence-based care gaps.
• Graduatingmemberswhoregresstothemean.
As an example, under the Optum CarePlus program, clinicians visit
the medically complex patient where he or she lives whether that is
a skilled nursing facility, an assisted living complex or the member’s
private residence.
An initial comprehensive assessment drives care planning and
hierarchical condition coding (HCC). Next, the Optum provider,
care manager and primary care physician (PCP) develop the care
management plan. Scheduled visits by the Optum CarePlus in-home
providers reflect the member’s acuity. On average, care teams visit
members 1.0 to 1.2 scheduled times per month. Unscheduled visits
occur as needed to keep members out of the hospital. Telephonic
care management and coordination are also key to symptom
monitoring, trigger management and member/family education.
Member-centric and provider-driven health care solutions designed for complex,
high-risk populations have reduced inpatient admissions by 40 to 50 percent
— Dr. Gary Dana Medical Director, CarePlus, Optum

5
John, 83-Year-Old Male • Congestive heart failure
• No active complaints• When questioned, admits to worsening cough
MEDICAL HISTORY• Systolic CHF from CAD/ischemia • Atrial fibrillation — chronic• 3V CABG• Three stents/PTCA• Aortic stenosis• IACD implanted• Diabetes mellitus with multiple manifestations• Stage 4 renal disease• Hypertension• Hyperlipidemia • Gout • Osteoarthritis • DJD with knee/hip replacement• H/O old MI • H/O colon cancer • H/O SCCA and BCCA skin • Hearing deficit• CVA with vascular dementia • Left leg weakness• Glaucoma• H/O left fem artery stent• Multiple ER visits, admissions and outpatient visits annually
MEDICATIONS
• Coreg
• Warfarin
• Proscar
• Lisinopril
• Furosemide
• KCL
PROVIDERS
• Primary Care
• Cardiologist
• Ophthalmologist
• Urologist
• Endocrinologist
• Orthopedist
• Levimere Insulin
• Metformin
• Norvasc 2.5mg
• Flomax
• Crestor
• Timoptic Opth ii
• Colace
• Gastroenterologist
• Dermatologist
• Oncologist
• General Surgeon
• Vascular Surgeon
• Cardiothoracic Surgeon
DAILY LIVING, SOCIALAND FAMILY HISTORY
• Lives alone.
• Uses walker.
• Bathes independently.
• Drives.
• Doesn’t cook, eats cold meals. Neighbors bring 25% meals cooked, and assist with laundry.
• Divorced. Widowed to second wife. One child, son, lives more than 1,000 miles away. Last visit seven years ago; calls weekly.
• Quit smoking 15 years ago.
• Two glasses of bourbon daily.
• Mother and father with CHF, CAD, DM, dementia last 10 years of life. Father deceased at 88; mother at 84.
Patients
• Avoid ER visits, inpatient admissions.• Reduce medications, unnecessary procedures.• Improve disease state understanding and self care.• Create closer relationships with providers.• Address advanced illness care goals including advance (directives).
• Improve patient understanding and outcomes.• Deliver timely, high-quality information.• Assistance in managing di�cult, complex patients.• Deliver preventive maintenance care, including disease education and intervention for clinical, functional, environmental, psychosocial and cultural triggers.
• Improve quality.• Lower costs for members.
Providers
HealthPlans
Heart Failure PalliativeCare/Hospice
COPDExacerbation
Urinary TractInfection
History and physical focusing on weight gain, fluid status and cardiopulmonary examination
Evaluation of current medications, adjustment as needed and provision of parenteral diuretics
Laboratory or imaging studies such as portable Chest X-ray (CXR) or blood tests
Coordination and follow-up with Primary Care Provider (PCP), nurse care manager
Primary Visiting Provider (PVP) - follow-up visits
History and physical focusing on vital signs, oxygenation status (pulse ox) andcardiopulmonary examination
Evaluation and adjustment of current medications; possible initiation of steroids
Laboratory studies such as portable CXR
Coordination and follow-up with PCP, nurse case manager
PVP follow-up visit
History and physical
Laboratory and evaluation including urinalysis and urine culture
Prescribing of oral or parenteral antibiotics
PCP notification, nurse care manager follow-up calls
PVP follow-up visit if indicated
Advance directives in place within 90 days of program enrollment
Review and adjust, or prescribe palliative care medications
Initiate hospice referral
Coordinate with PCP, nurse care manager
In-depth discussion with hospice team to determine next steps and responsible parties for ongoing management
The above scenarios (see Figure 3) demonstrate how care team
in-home interventions support medically complex members who are
facing disease processes, dealing with illnesses, or making
end-of-life decisions.
Taking a holistic approach to care extends beyond managing
chronic conditions. The care plan also includes a focus on relevant
preventative services and guideline-driven treatment (e.g., flu shot,
pneumonia vaccination) to avoid unnecessary hospitalization.
Historically, the health care industry has taken a disease-by-disease
approach to chronic illness treatment — identifying and managing
clinical interventions tied to particular clinical situations. Population-
based health management of complex members — using a program
that modifies utilization and curtails unnecessary costs — can
improve outcomes and enable a better quality of life, while lowering
medical costs.
Figure 3In-home interventions supporting medically complex members

Want to learn more?
Visit optum.com
or call 1-800-765-6807.
How Optum can helpOptum partners with health plans to provide in-home, provider-led clinical care and
care management to improve quality while reducing unnecessary health care costs, for
the most expensive, medically complex population. Our solutions provide:
• Healthcaredesignedspecificallyforhigh-riskmembers
• Improvedqualityandlowerhealthcarecosts
• Preventedavoidablehospitalizations
1 Stanton MW. The High Concentration of U.S. Health Care Expenditures. Research in Action, Issue 19. AHRQ Publication No. 06-0060, June
2006. Agency for Healthcare Research and Quality, Rockville, MD. ahrq.gov/research/ria19/expendria.htm
2 Optum CarePlus Outcomes Study on Acute Admissions, based on claims savings for the large-patient pool programs in Five Markets. 2011. Data compiled by Optum Data Analytics.
optum.com
13625 Technology Drive, Eden Prairie, MN 55344
OptumTM and its respective marks are trademarks of Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owner. Because we are continuously improving our products and services, Optum reserves the right to change specifications without prior notice. Optum is an equal opportunity employer.
OPTPRJ1804_Print 09/13 © 2013 Optum, Inc. All rights reserved.