richard duke basics of drug discovery and development
TRANSCRIPT

UCCCGlobeImmune
ApopLogicCID4
PeptiVirMenoGeniXAurora Onc
Taking an Idea from the Lab Bench to the Clinic
Drug Discovery and Development
Richard C. Duke, [email protected]
Building BiotechnologyOctober 2015

Serial Entrepreneur
• Definition:
“A person who doesn’t follow directions and is a slow learner”
- Larry Gold, PhD
2

The Constitution protects ideas
• “The Congress shall have the Power to promote the Progress of Science and useful Arts, by securing for limited Times to Authors and Inventors the exclusive Right to their respective Writings and Discoveries”
- Article 1, Section 8, Clause 8
3

The Bayh-Dole Act
• Federal grant recipients are required to maximize the use of their research findings either through dissemination to the research community and the public (publication) or through timely commercialization (patents and licenses)
4

It’s a good idea to patent your idea
• Product development is an extremely risky, time-consuming and expensive undertaking
• Without patent protection, there is no incentive for investment
• If you have an idea that could benefit the world, it has to be patented
• However, once patented, the clock starts ticking and the bills start accruing
5

Who really owns the idea?
6

Invention disclosure
• Upside• See if your idea works• Money for your research and pocket• The university pays for the initial patent
• Downside• Time consuming• May not count towards promotion/tenure• Unrealized expectations
7

Reality
• 9 out of 10 drugs that enter into phase 1 fail• They don’t actually fail to work• They fail to be better than what we
already have• It costs $50 - $200 million for each failure• Only 20 or so new drugs are approved by
the FDA each year
8

Research vs. development
• Research provides data that supports proof-of-concept and proof-of-principle for an idea. In the life sciences, funding comes almost exclusively from the NIH, NSF and philanthropic organizations. Take things apart.
• Development provides data that allows a product to be made and used. The NIH and NSF do not fund development for the most part. Development requires private investment. Put things together.
9

0 3 7 12
Feasibility studies
Drug discoveryTarget discovery
Timeline in years
IND enabling studiesPhase 1 clinical trials
Post-registration
0 $500K $5.5M $200 million $1BDevelopment costsCumulative burn
Phase 2/3 clinical trials
Proof-of-concept
Drug development timeline and cost(does not include IP costs)
10

0 3 7 12
Feasibility studies
Drug discoveryTarget discovery
Timeline in years
IND enabling studiesPhase 1 clinical trials
Post-approval
1980’s 1990’s 2000’s Today
1980’s Today
1990’s 2000’s Today
First VC financing
IPO
M&A
Timing of:
Phase 2/3 clinical trials
Proof-of-concept
Drug development timeline and cost
11

0 3 7 12
Feasibility studies
Drug discoveryTarget discovery
Timeline in years
IND enabling studiesPhase 1 clinical trials
Post-registration
0 $500K $5.5M $200 million $1BDevelopment costsCumulative burn
Phase 2/3 clinical trials
Proof-of-concept
Drug development timeline and cost
“Valley of Death”
12

0 3 7 12
Feasibility studies
Drug discoveryTarget discovery
Timeline in years
IND enabling studiesPhase 1 clinical trials
Post-registration
0 $500K $5.5M $200 million $1BDevelopment costsCumulative burn
Phase 2/3 clinical trials
Proof-of-concept
Don’t forget about patents…
“Valley of Death”
13Patent Filings

Research vs. development
• Research is empirical. The results from one experiment determine the design of the next experiment. Where you end up may be very far away from where you thought you were headed
• Development is methodical. You start with the “label” and work backwards. Once you start clinical trials it’s extremely costly to “tweak” the product.
14

Stage 1: Target Validation
• Establishes MOA and value of the target
• Knock-outs and knock-ins• iRNA and shRNA
• Resources• AMC• BioFrontiers
15

Stage 2: Drug Discovery
• Types of drugs• Small molecules• Peptides• Biologics• Monoclonal antibodies• Vaccines• Cells• Repurposed and abandoned drugs
16

Stage 2: Drug Discovery
• Small molecules• Need a good screening assay• Need a large library of compounds• Efficacy assessment
• Test tube• In vivo – cells• In vivo – animals
• Safety and drugability• What if it’s a pre-existing drug
17

Stage 2: Drug Discovery
• Entrepreneur’s concerns• I need proof-of-concept data• Can I make enough and is it soluble?
• Investor’s concerns• Is this the final product and formulation?• Is the composition patentable?
18

Stage 2: Drug Discovery
• Resources:• Drug discovery and formulation
• School of pharmacy HTS facility• Colorado Center for Drug Discovery (CSU)
• Biologics and Cells - Gates Center• Peptides – Hodges lab
19

Stage 3: Proof-of-concept
• Entrepreneur’s concerns• I need proof-of-concept data
• Investor’s concerns• I don’t believe the model you used• How pure is the drug?• Is this stuff soluble?• Is this stuff drugable?
20

Stage 4: FeasibilityLast chance to tweak
• Entrepreneur’s concerns• I gave you POC data, now what do you want?
• Investor’s concerns• I don’t believe the model you used• How pure is the drug?• Is this stuff soluble?• Is this stuff drugable?
21

Stage 5+: Development
• IND enabling studies• Toxicology and pharmacology ($500K - $2M)• Pilot GMP manufacturing ($50K - $1M)• GMP manufacturing ($250K - $2M)
• Phase 1 clinical trials ($10K - $30K per subject)• Phase 2 clinical trials• Phase 3 clinical trial
22

Stage 5+: What’s an IND
• Clinical Trial Protocol• Potential benefit to the patient, safety discussion,
starting dose, stopping rules
• CMC: Chemistry, Manufacturing and Controls• Purity, stability, QC, QA
• Non-clinical Pharmacology and Toxicology• Pre-clinical efficacy, safety in the appropriate animal
species, PK/PD, ADME
23

Being a biotech entrepreneur is getting a lot harder
• It costs a lot to develop a drug• Greater uncertainty regarding regulatory risk,
reimbursement and new patent rules• Unless you are a serial entrepreneur, venture
capital has all but disappeared for drugs that have not been in humans
• Greater reliance on alternative funding• Grants, Family, Friends, Angels• Need to be even more “virtual”
24

Resources
• Colorado infrastructure grants• CID4; C2D2; SOP-HTS; BioFrontiers
• Colorado advanced industry grants• POC ($200K); Early stage company ($250K)
• Federal grants• SBIR, STTR
• Philanthropy and angels
25

The problem: We aren’t getting enough drugs into the clinic (2010-2014)
• NIH funds ~4,000 research projects ($1.5 B)• ~200 drug invention disclosures are filed ($20M)• ~100 POC projects are funded ($15M)• ~20 start-up companies receive SBIR or ESC
funding ($20M)• ~10 drugs enter into clinical trials• 1 drug approved (4 total from CU last 30 years)• We can do better than this
26

Duke’s history
1985 Ph.D. in Immunology (UC-SOM)1987 First Faculty Position (UC-SOM; Tenured in Medicine)1990 Research Analyst at Janus Capital1993 First Patent Application1995 Founded GlobeImmune (3 faculty; >$180 million raised to date)2004 First phase I clinical trial at GlobeImmune (cancer)2008 Founded ApopLogic (7 faculty; >$2 million raised to date)2009 First IND filing at ApopLogic (cancer)2009 Founded CID4 to support early stage company creation & growth2010 Completion of first phase II trial at GlobeImmune (hepatitis C)2010 CID4 founds and funds its first company, PeptiVir (2 faculty)2010 Founded MenoGeniX (first clinical trial completed in 2013)2011 Helped found Aurora Oncology (4 faculty)2012 GlobeImmune files an IPO2013 GlobeImmune withdraws its IPO2014 GlobeImmune IPO
27
Case Study #1
GlobeImmune, Inc.
28

GlobeImmune, Inc.
• Ceres Pharmaceuticals, Ltd. was founded in 1995 by tenured UC-SOM faculty:
• Dr. Richard Duke (Medicine)• Dr. Alex Franzusoff (Cell Biology)• Dr. Don Bellgrau (Immunology)
• Mission: Take an invention from the lab bench to the clinic = Commercialization
29

GlobeImmune, Inc.Technology
• From 1993 to 1995, GlobeImmune’s Founder’s filed patents on three technologies:
• Fas ligand to prevent transplant rejection Nature; Scientific American Licensed to Novartis, GlobeImmune and ApopLogic
• T cell protease required for HIV infection PNAS Licensed to Glaxo
• Recombinant yeast-based immunotherapy Nature MedicineLicensed to GlobeImmune; 7 products in the clinic
30

GlobeImmune, Inc.Platform Technology
31

GlobeImmune, Inc.Lead Product Development
• Whole, heat-killed recombinant yeast-based immunotherapeutics and vaccines
• Our initial target was HIV• We built a small scale manufacturing facility,
made the product, vialed the product and carried out toxicology testing
• The NIH HIV vaccine trial network was supposed to do a clinical trial. At the last moment, they decided to delay. We couldn’t delay
32

33

Ceres becomes GlobeImmune
• In March 2002, the decision was made to obtain venture capital financing = become a real company
• VCs do not trust inventors or technology• VCs invest in management• We hired a seasoned CEO• HIV was no longer of interest• Cancer immunotherapy was the focus
34

GlobeImmune, Inc.Financing history
1995 Established operations with Duke as CEO1996 First SBIR + other NIH grants (Total = $4.3 million)1996 Colorado Advanced Technology Grant: $100,000)1997 Licensed Fas ligand to Novartis: $1.2 million1998 First patent issued2002 Angel investors: $425,0002002 Hired new CEO; Duke is President; Franzusoff is VP-R&D2003 Series A venture capital: $8 million2005 Series B venture capital: $38 million; Duke resigns as President2008 Series C venture capital: $41 million; Duke quits2009 Series D venture capital + Celgene R&D funding: $40 million2010 Series E private equity: $18 million2011 Gilead R&D funding: $10 million; Franzusoff quits2012 IPO filed and withdrawn2013 Gilead R&D license: $Not disclosed2014 Debt Financing: Aegis Capital: $7.5 million2015 IPO: $35 million 35

GlobeImmune, Inc.Pipeline Products - 2012
36

GlobeImmune, Inc.Pipeline Products - 2014
37

GlobeImmune20 years later
38

Case Study #2
ApopLogic Pharmaceuticals
39

ApopLogicPharmaceuticals

• Founded in 2008 to address the unmet need for new, less toxic, targeted anti-cancer drugs
• $900K in grants (NCI and AKC) – AP300
• $900K angel round (LSA, others) – B201
• Open IND for Breceptin (B201-acetate) – SCLC and other cancers with neuroendocrine features
• Seeking USDA approval for Fasaret (AP-300) in dogs – multiple human cancer applications
The CompanyCancer: the leading killer in the U.S.
41

• Richard Duke, PhD, Founder and CEO: Serial entrepreneur (GlobeImmune; ApopLogic, PeptiVir, CID4)
• Paul Bunn, MD, Founder and CMO: International KOL (lung cancer); Former Dir./Pres./Chair (UCCC; ASCO; IASLC; ODAC-FDA); UCCC
• Jaime Modiano, VMD, PhD, Founder and VP-Veterinary Oncology: Perlman Professor of Oncology and Comparative Medicine (UMN)
• Donald Bellgrau, PhD, Founder and VP-Immunolgy
• Jeffrey Rona, CBO/CFO: Biotech finance and BD (UBS Warburg; GlobeImmune, Antigenics, Coopers & Lybrand)
• Drs. Lajos Gera, John Stewart, Dan Chan, Founders
The teamExpertise in business and science
42

B201-acetate (Breceptin)
ApopLogicPharmaceuticals
43

• Chemotherapy is non-specific and toxic• Targeted drugs are less toxic but don’t work
in many cancers including small cell lung cancer (SCLC)
• Few new drugs in late stage development• Huge opportunity for new, less toxic,
targeted anti-cancer drugs = Breceptin
The problemCancer: the leading killer in the U.S.
44

• Small cell lung cancer is associated with a paraneoplastic syndrome• Over expression of neuropeptides• Do these act as growth factors?• Bradykinin receptors are the most highly
expressed receptors on SCLC• Target BK receptors?
The Idea
45

1948 Bradykinin discovered as mediator of snake venom pain & shock1959 Solid phase peptide synthesis invented by Merrifield (Nobel)1962 Bradykinin first active peptide to be synthesized by SPPS by
Stewart and Merrifield1965 Automated peptide synthesizer invented by Stewart and
Merrifield (Smithsonian)1984 First effective BK antagonist synthesized by Stewart & Vavrek1990 BK as a growth factor for lung cancer described by Bunn & Chan1996 Gera and Stewart make B9430 monomer and B9870 dimer, the
latter shown to have anticancer activity by Chan & Bunn2000 NCI starts development of Breceptin under the RAID program2006 NCI gives up on manufacturing Breceptin2008 ApopLogic in-licenses Breceptin2009 ApopLogic gets IND open in December to start clinical trials
Breceptin History
46

Bradykinin (BK)
47

• BK is produced in the tumor microenvironment due to tissue damage caused by the growing cancer and because many cancers produce kallikreins that cleave kininogen
• BK induces inflammation, invasion and neo-angiogenesis which potentiate cancer cell growth and metastasis
• Cancer cells over-express BK B1 and B2 receptors and BK acts as a cancer cell growth factor
Bradykinin (BK)
48

BreceptinPeptide dimer bradykinin biased agonist
Rationally-designed to have an extended half-life
Bradykinin (Pure agonist):Arg-Pro-Pro-Gly-Phe-Ser-Pro-Phe-Arg
B9430 (Pure antagonist):DArg-Arg-Pro-Hyp-Gly-Igl-Ser-DIgl-Oic-Arg
Breceptin (B9430 dimer) (Biased agonist)
APP NEP ACE CPNEndopeptidase cleavage sites
49

BK & BK receptorsBK is a growth factor
BKR gene copy number is a cancer biomarker
BDKRB2
Control
14q32.2
Ca++ flux in SCLC Gene duplication in SCLC
50

• Monomer and dimer are B1 and B2 receptor antagonists as measured in competitive binding, contractility, neo-angiogenesis and migration assays (anti-inflammatory) (IC50 1-10 nM)
• The dimer, but not the monomer, inhibits tumor cell growth (anti-proliferative) (LD50 ~1 uM)• Mechanism is biased agonism – discordant signaling• Linker length and chemistry are critical• Other peptide BK antagonists do not work as dimers
BreceptinHow it works – Part 2
5151
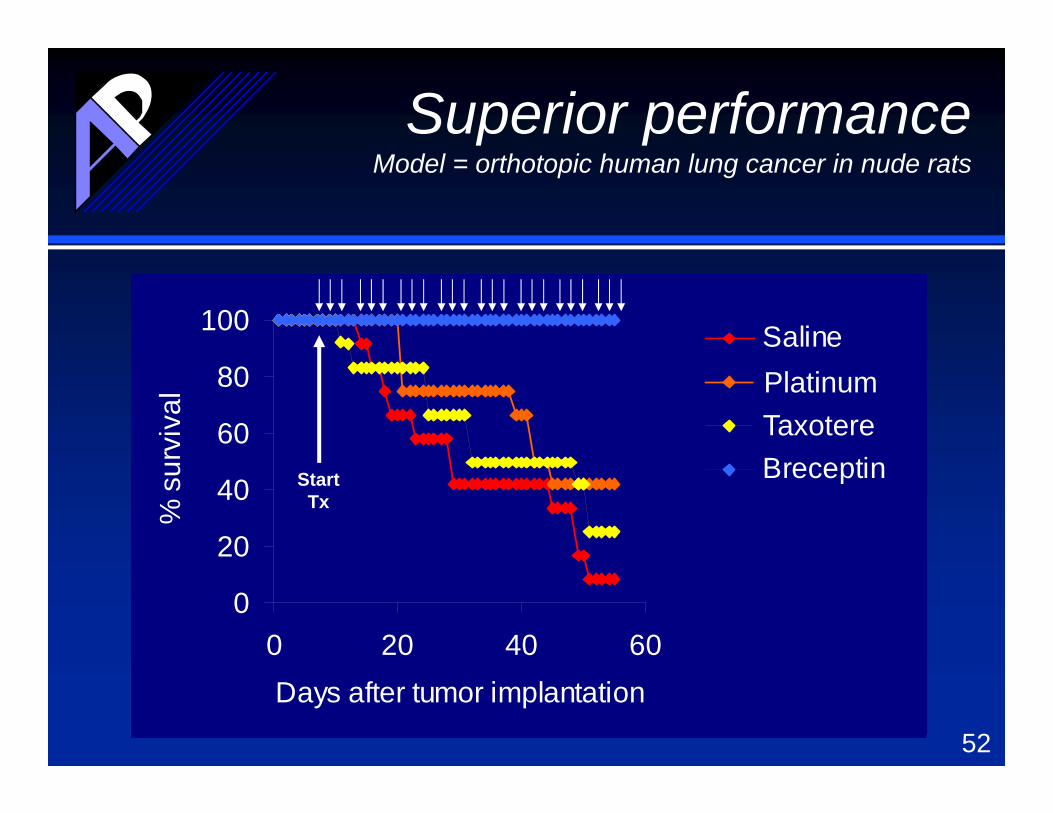
Superior performanceModel = orthotopic human lung cancer in nude rats
0
20
40
60
80
100
0 20 40 60Days after tumor implantation
% s
urvi
val
SalinePlatinTaxaneBreceptin
0
20
40
60
80
100
0 20 40 60Days after tumor implantation
% s
urvi
val
SalinePlatinTaxaneBreceptin
0
20
40
60
80
100
0 20 40 60Days after tumor implantation
% s
urvi
val
SalinePlatinTaxaneBreceptinStart
Tx
TaxoterePlatinum
52

Superior performance
* These results are consistent with inhibition of bradykinin-induced proliferation, neo-angiogenesis, and metastasis
Control lungs Treated lung(metastatic disease) (static primary tumor)
53

Superior performanceDelayed progression and tumor stasis in
subcutaneous human lung cancer in nude mice
0
1000
2000
3000
4000
5000
6000
0 15 30 45Days after tumor implantation
Mea
n tu
mor
vol
ume PBS
Breceptin
0
1000
2000
3000
4000
5000
6000
0 15 30 45Days after tumor implantation
Mea
n tu
mor
vol
ume PBS
Breceptin
0
1000
2000
3000
4000
5000
6000
0 15 30 45Days after tumor implantation
Mea
n tu
mor
vol
ume PBS
Breceptin
0
1000
2000
3000
4000
5000
6000
0 15 30 45Days after tumor implantation
Mea
n tu
mor
vol
ume PBS
Breceptin
StopTx
Daily Tx
Re-start Daily Tx
54

• Clinical Trial Protocol• Potential benefit to patient, safety discussion,
starting dose, stopping rules
• Non-clinical Pharmacology & Toxicology• Pre-clinical efficacy, PK/PD, safety in animals
• Chemistry, Manufacturing and Controls• Purity, Stability, QC, QA
IND packageInvestigational New Drug Application
55

• Phase 1 clinical trial in unselected cancer patients with solid tumors will start within 6 months of financing and establishes the phase 2 dose level and schedule
• Phase 2 trials establish POC in SCLC, extrathoracic SCC and/or carcinoid as second line therapy vs. SOC
• Phase 3 trials leading to NDA: first line maintenance therapy in SCLC (vs. placebo)
BreceptinPreferred clinical development scheme
56

• A phase 1 open-label, multiple dose study to assess the safety, tolerability and pharmacokinetics of repeated subcutaneous injection of B201-acetate (Breceptin) in patients with advanced cancer.
• Primary objective: Evaluate the safety profile of subcutaneously injected Breceptin including DLTs
• Primary objective: Evaluate the plasma pharmacokinetic profile after single and repeated dosing and compare systemic exposure levels to the predicted exposure parameters required for efficacy in the preclinical models.
BreceptinPhase 1 clinical trial
57

The secondary objectives are to:
• Determine the recommended phase 2 dose for further clinical trials
• Observe any evidence of anti-cancer activity in an unselected patient population
• Determine the presence of BKB1R and BKB2R receptors in patient tumor tissue and any relationship between receptor expression and anti-cancer activity.
BreceptinPhase 1 clinical trial
58

Cycle 1 (D1, 8, 15, 17, 19)
Cycle 2 and thereafter(D1, 3, 5, 8, 10, 12, 15, 17, 19)
Weeks
Breceptininjections
DLT assessment period
BreceptinPK (C1‐2 only)(*=trough levels only)
* * * **
BP (C1‐2 only)(^=extended monitoring)
^ ^ ^ ^ ^ ^
PD RP2D cohort only (C1‐2 only)
59

Accelerated Dose Escalation PhaseSingle patient cohorts
At least Grade 2 drug related toxicity in C1?
NO YES
100% dose increment
next cohort.Continue single patient cohorts
Does this meet DLT criteria?
NO YES
Add patients up to total of 3 evaluable
1 or more DLT occurs?
NO YES
33% dose increment next
cohort. 3+3 design from
now on
Add patients up to total of 6 evaluable
>1 DLT?
YES
NO
Non-tolerated dose
>1 DLT? YESNO
Non-tolerated dose
33% dose increment next
cohort. 3+3 design from
now on
60

• Accepted by the NCI-RAID program for development in 2000
• GMP manufactured under RFP by Advanced ChemTech (ACT) as TFA salt in 2001 and acetate salt in 2004
• Pharmacology and GLP toxicology studies performed with ACT drug
• During preparation of an IND application in 2005, the NCI discovers that the ACT product is highly contaminated. ACT files for bankruptcy
• ApopLogic considers license. NCI contracts with a new manufacturer in January 2006. New manufacturer produces the wrong drug
• University of Colorado requests that NCI deliver all existing product and study reports to Dr. Bunn and desist further development in Summer 2006. Materials received in 2008 and licensed to ApopLogic
BreceptinNCI-RAID involvement
61

• Clinical Trial Protocol• Potential benefit to patient, safety discussion,
starting dose, stopping rules
• Non-clinical Pharmacology & Toxicology• Pre-clinical efficacy, PK/PD, safety in animals
• Chemistry, Manufacturing and Controls• Purity, Stability, QC, QA
IND packageInvestigational New Drug Application
62

• B201-TFA salt was initially manufactured by Advanced ChemTech under contract to the NCI
• Initial pharmacology and toxicology testing were performed with B201-TFA by Battelle
• A rapid IV bolus of B201-TFA resulted in severe hypotension, rebound hypertension and tachycardia
• B201-acetate was subsequently manufactured by ACT and the toxicology studies were repeated
IND: Preclinical toxicology package
63

• The toxicology of B201-acetate was investigated in 28-day studies in rats and monkeys with daily subcutaneous injection
• The major toxicology findings were cardiovascular (hypotension followed by rebound hypertension) and reactogenicity at the injection site (NOAEL <5 mg/kg).
• PK studies indicated: Tmax =10-60 minutes, Cmax > 1 M; t1/2 = 4 hours; and t1/2 ~ 40 hours
IND: Preclinical toxicology package
64

0
500
1000
1500
2000
2500
0 10 20 30 40 50time (hours)
conc
entr
atio
n
Cmax
CminAUC
Cmax and AUC
65

• The NCI package supports daily, subcutaneous administration at super optimal doses
• A non-GLP study was performed by ApopLogic to establish the local toxicity and recovery period associated with a single sub-cutaneous dose
• An ongoing study is examining the relationship of Cmax vs. AUC to toxicity and efficacy in tumor-bearing rats to guide future formulation studies
IND update: Preclinical toxicology package
66

0
500
1000
1500
2000
2500
0 10 20 30 40 50time (hours)
conc
entr
atio
n
Cmax
CminAUC
Cmax and AUC
67
Toxic dose level
Efficacious dose level

• Clinical Trial Protocol• Potential benefit to patient, safety discussion,
starting dose, stopping rules
• Non-clinical Pharmacology & Toxicology• Pre-clinical efficacy, PK/PD, safety in animals
• Chemistry, Manufacturing and Controls• Purity, Stability, QC, QA
IND packageInvestigational New Drug Application
68

• B201 has been synthesized at phase 1 scale by Peptisynthta (>98% purity)
• Highly stable when stored as dry powder (>8 yr) and as refrigerated liquid formulation (>3 months)
• B201 will be formulated (Innovative Pharmacy Solutions) in sterile, non-buffered, physiological saline, sterile filtered, stored frozen, and shipped on dry ice to the clinical trial sites.
IND update Manufacture and Formulation
69

AP‐300 (Fasaret)
ApopLogicPharmaceuticals
70

• Fas ligand (FasL) delivered locally into tumors using recombinant adenovirus or other forms of vectors including plasmid DNA
• In the context of cancer, Fasaret is used in either the neo‐adjuvant or adjuvant setting to improve the outcome of standard of care irrespective of cancer type or therapeutic regimen
FasaretFas ligand‐mediated therapy
71

• Fas receptor is expressed on activated and dividing cells
• Fas ligand is involved in lymphocyte homeostasis but also directly kills Fas sensitive cancers
• Fasaret targets Fas‐resistant cancers by creating a potent pro‐inflammatory response and killing FasR+/CD4+/CD25+ regulatory T cells (T‐regs) thereby leading to a systemic tumor vaccine response that targets distant metastases.
FasaretMechanism of Action
72

FasaretHighly efficient killing of activated CD4+/CD25+ T cells by
tumor cells transduced with Ad‐FasL
-20
0
20
40
60
80
100
% k
illed
0.006:1 (0.6% of total cells)
0.03:1 (3%)
0.16:1 (16%)
0.8:1 (80%)
Ad-Ctrl Ad-FasL
73

FasaretPre‐clinical data: In vivo efficacy of Ad‐FasL
Human lung cancer cells in nude mice
0
1000
2000
3000
4000
5000
0 10 20 30 40
Days after tumor implantation
Tum
or v
olum
e (m
m3) Lung cancers + Ad-GFP
90:10 (GFP:FasL)Lung cancers + Ad-FasL
74

Control
0
40
80
120
160
0 5 10Days after implantation
Tum
or v
olum
e
Fas Ligand
0
40
80
120
160
0 5 10Days after implantation
Tum
or v
olum
e
FasaretPre‐clinical data in a syngeneic colorectal cancer model
Nabel et al. 1997, PNAS 94:13862
Control adenovirus or adenovirus encoding Fas ligand directly injected into a Fas‐resistant tumor
75

FasaretPre‐clinical data: Prevention of tumor metastasis to lung
PBS Fasaret Inactive Fasaret
76

• Involves adenovirus which implies gene therapy
• Needs to be injected directly into the tumor so it looks like an oncolytic virus
• Prevents metastasis so it looks like immunotherapy
• Systematic administration can cause liver hemorrhage!
• De‐risk for investors by demonstrating safety and efficacy in dogs with spontaneous cancer
FasaretReal problems for investors
77

Enhancing antimelanoma immune responses through apoptosisBianco SR, Sun J, Fosmire SP, Hance K, Padilla ML, RittMG, Getzy DM, Duke RC, Withrow SJ, Lana S, MatthiesenDT, Dow SW, Bellgrau D, Cutter GR, Helfand SC, Modiano JF.Cancer Gene Ther. 2003 10:726‐36
Fasaret
78

Day 1 Day 8
Phase 1 clinical trial in 5 dogs with oral melanoma: Results: 80% response rate including 2 cures
FasaretEfficacy of intratumoral injection of DNA encoding FasL
(Bianco et al. 2003. Cancer Gene Ther. 10:726‐736)
79

Inflammation, Apoptosis, and Necrosis Induced by Neoadjuvant Fas Ligand Gene Therapy Improves Survival of Dogs With Spontaneous Bone CancerJaime F Modiano, Donald Bellgrau, Gary R Cutter, Susan E Lana, Nicole P Ehrhart, EJ Ehrhart, Vicki L Wilke, J Brad Charles, Sibyl Munson, Milcah C Scott, John Pozniak, Cathy S Carlson, Jerome Schaack and Richard C DukeMol. Ther. 2012. 20: 2234‐2243
Fasaret
80

• Hypothesis: Intra‐tumoral administration of FasL in a delay of therapy/neo‐adjuvant setting will be safe and will produce anti‐tumor responses that will improve outcomes following SOC
• Open‐label study in 56 dogs at CSU and UMN. 50 dogs were treated at the highest allowable dose
• Single intratumoral injection of Fasaret ten days prior to limb amputation and initiation of SOC
FasaretPhase 1b/2a clinical trial in dogs with osteosarcoma
81

FasaretProlonged survival in 56 dogs with osteosarcoma with
intratumoral injection of rAd‐FasL followed by SOC
Days
% su
rvival
Phase 1b canine osteosarcoma survival data
82
Fas low
Fas high

AP‐300Fas expression is not predictive of survival in the absence of
Fasaret therapy
0
100
200
300
400
Fasaret + SOC SOC alone
Fas‐low
Fas‐high
83
• Initial data show efficacy in melanoma and bone cancer = seek conditional approval from USDA for limited sales and marketing
• Establish community trial to expand label to other tumor types including generally non‐metastatic cancers that are hard to treat (e.g., soft tissue sarcomas and some H&N)
• Can also be used for multiple human cancers
AP‐300Veterinary market opportunity
84

Targeted therapies for bladder cancerMike Glode, MDDan Theodorescu, MDTom Flaig, MDWon Park, PhDRick Duke, PhDAdam Wolach
10/23/2015 85
Jack Lemon Ray Bolger

Company
Companyand
Science
86
Aurora Oncology, Inc
10/23/2015

Company
• Spun out of University of Colorado School of Medicine in 2012 to address the unmet need for new, targeted therapies for superficial and metastatic bladder cancer
• Technologies developed with extensive NIH, NCI and NSF funding
87
Aurora Oncology, Inc
10/23/2015

Team
• Mike Glode, MD, Founder and President: Medical Oncology (GU) at UCD‐AMC and Serial entrepreneur (Gonex; ProTechSure)
• Dan Theodorescu, MD, Founder and Acting VP, Ral program: Director, UC Comprehensive Cancer Center , Institute of Medicine
• Tom Flaig, MD, Founder and Acting VP, DAB389EGF program: Medical Oncology (GU) at UCD‐AMC
• Won Park, PhD, Founder and Acting VP, Nano‐EGFR‐mAb program: Nanoparticle engineering – UC Boulder
• Rick Duke, PhD, Acting CEO: Serial entrepreneur (GlobeImmune; ApopLogic; PeptiVir; MenoGeniX) and Colorado Institute for Drug, Device and Diagnostic Development (CID4)
• Adam Wolach, Acting Sr. Director of Business Development: Serial entrepreneur (BioVantage Resources, Mentor InterActive, ProTechSure)
88
Expertise in Genitourinary Oncology and Business
10/23/2015

Problem: Bladder Cancer
• Bladder cancer is the 5th most common cancer
• Highest lifetime treatment costs per patient of all cancers
• New agents are needed to replace 30‐year old therapies
• Long‐term survival is not currently attainable
89
The unmet need
10/23/2015

The Problem: BCG Therapy
• Superficial bladder cancer is currently treated with intravesical BCG (attenuated TB bacteria)
• Disease recurrence after BCG therapy is high– 50% in some high‐risk series– Recurrence can lead to cystectomy and/or metastasis
• Local adverse events with BCG are common– Urinary frequency; cystitis; fever; hematuria; systemic infection and granulomas
10/23/2015 90
Current therapy is ineffective and toxic

The Solution
• The bladder is an accessible organ for direct drug administration
• The epidermal growth factor pathway and receptor (EGFR) play an important role in bladder cancer pathogenesis and proliferation. – Diffuse EGFR protein expression is seen in urothelial cancers (70%)
– EGFR protein expression is uncommon/rare in normal urothelium.
• DAB389EGF or Nano‐EGFR‐mAb are targeted, direct therapies
10/23/2015 91
Targeted intravesical therapy

Solution: Targeted Therapy
• DAB389EGF: Diphtheria toxin A chain –epidermal growth factor fusion protein to treat superficial bladder cancer via intravesical injection. ONTAK (DAB‐IL‐2) is FDA approved.
• Nano‐EGFR‐mAb: Gold nanorod – anti‐EGFR mAb fusion compound to treat superficial bladder cancer via intravesical injection/thermotherapy
92
Research and Development Programs
10/23/2015

Orthoptopic Model
10/23/2015 93
Killing of human bladder cancer cells in vitro
Seven day post cell implantation Two weeks after first drug treatment
DT-GMCSF DT-EGF
Examples of treatment response: DT‐GM‐CSF was used as a control treatment. Blue indicates viable xenograft by bioluminescence.‐ Cancer Research 2012, Yang et al

Additional Animal Studies
• DAB389EGF shows equivalent efficacy to BCG– Orthotopic model using highly aggressive syngeneic mouse bladder cancer cells
• Dog studies at CSU Animal Cancer Center– 3 healthy dogs treated to date with no evidence of systemic toxicity
– Dogs with bladder cancer are being recruited• These are typically not superficial so exploratory PK/PD/Toxicology only
94
Superficial bladder cancer
10/23/2015

DAB389EGF
• Phase Ib – Superficial bladder cancer patients who have failed BCG
• Safety• Establish phase 2 dose
• Phase II studies:– BCG‐failure
• Recurrence rate at 6 months– First line vs. BCG
• Recurrence rate at 6 months• Phase III ‐ TBD
10/23/2015 95
Clinical development plans

DAB389EGFIntellectual property
Development and Financing
96

DAB389EGFIntellectual property
Licensed IP covers composition and method of use including intravesical delivery• Pending patent (PCT/US10/52634)
• Use claims• Composition of matter on novel DAB389EGF construct
97

Drug Repurposing
• Examples
• MenoGeniX
• CU
98

Starting your own company
• Intellectual Property & Product Development Plan• Single vs. Multiple Founders• Managing Expectations• Funding
• Friends and Family• Grants• Angel Investors• Venture Capital
99

Managing Expectations
“Make meaning. Increase the quality of life.
Right a wrong. Prevent the end of something good”
- The Art of the Start- Guy Kawasaki
100

The Pitch10 slides, 20 minutes, 30-point font
• Title
• Problem
• Solution
• Business Model
• Underlying Magic
101
• Market
• Competition
• Team
• Financial Projections
• Timeline & Milestones

Negotiating a Term Sheet
Richard C. Duke, Ph.D.Founder and CSO, CID4
Founder and CEO, ApopLogic
102

“An entrepreneur tends to bite off a little more than he can chew hoping he'll quickly learn how to chew it.”
- Roy Ash
103

• Don’t assume that you know it all• If you don’t think that you need help, you really
need help• If you think you need help, you really need help• Your baby and/or your money deserve good
counsel and advice• You never really know an investor until you spend
quality time with them in your company when the roof is leaking
Before we dig in
104

“Business opportunities are like buses, there's always another one
coming.”- Richard Branson
105

• Entrepreneur• Intellectual Property• Needs cash• Has equity to sell•
• Angel Investor• Has money to burn• Likes the idea• Wants ROI•
Starting Point
106

Starting Point
• Entrepreneur• Extremely Valuable Intellectual Property • Desperately Needs cash • Has equity to sell but it’s “my baby”• LIKES TO BE IN CHARGE
• Angel Investor• Has money to burn but it’s my money• Likes the idea but not all angels are “angels”• Wants ROI• LIKES TO BE IN CHARGE
107

• How much money does the entrepreneur want to raise?
• How much equity is the entrepreneur willing to give up?
• Who is going to control the company after the investment is made?
The deal should be pretty straightforward
108

“The fellow who says he’ll meet you halfway usually thinks he’s standing
on the dividing line.”- Orlando Battista
109

• Amount of financing being sought
• Valuation• THE FIRST MAJOR ISSUE
• Control
The Basic DealFrom the top of the term sheet
110

• Amount of financing being sought• Entrepreneur vs. investor• How much money do you need to get to the next
milestone if things don’t go smoothly• How much do you need in the next round• Can your investors fund the next round• It’s all about mitigating risk
The Basic DealFrom the top of the term sheet
111

• Dilution of company ownership• Loss of managerial control• Adequacy of financing• Future capital requirements• Alliance with investors that have helpful industry
connections• Get help to close the deal• Don’t be afraid to ask dumb questions. They’re
easier to handle than dumb mistakes.
Preparing for the negotiation
112

“Make meaning. Increase the quality of life. Right a wrong. Prevent the end of something
good”- Guy Kawasaki
113