rezūm system reimbursement guide - rezum treatment for ... · rezūm system reimbursement guide...
TRANSCRIPT
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 2
table of contents
OVERVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Benign Prostatic Hyperplasia (BPH) . .. . .. . .. . .. . .. . .. . .. . 3
The Rezūm System . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . 3
Indications for Use . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . 3
CODING AND PAYMENT . . . . . . . . . . . . . . . . . . . .4
Diagnosis Coding .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . 4
Physician Coding and Payment . .. . .. . .. . .. . .. . .. . .. . .. . 6
Physician Billing in the Office .. . .. . .. . .. . .. . .. . .. . .. . .. . 7
Physician Billing in a Facility Setting . .. . .. . .. . .. . .. . .. . .. . 8
Outpatient Hospital Coding & Payment . . .. . .. . .. . .. . .. . .. . 9
Ambulatory Surgery Center (ASC) Coding & Payment . .. . .. . .. . 9
Inpatient Hospital.. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . .. . 9
BENEFITS AND COVERAGE . . . . . . . . . . . . . . . . 10
The Prior Authorization Process . .. . .. . .. . .. . .. . .. . .. . .. 10
FREQUENTLY ASKED QUESTIONS . . . . . . . . . . . . 11
SAMPLE PRIOR AUTHORIZATION REQUEST . . . 12
SAMPLE LETTER OF MEDICAL NECESSITY . . . . 13 THE REZŪM SYSTEM BIBLIOGRAPY . . . . . . . . . 14
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
DisclaimerThe information in this guide is provided for the benefit of NxThera customers and offers general coverage, coding and payment information for procedures associated with the use of the Rezūm System. The information provided is intended to facilitate appropriate coverage and reimbursement for providers in various sites of service. Users of this guide should understand that this is general information, not legal guidance nor is it advice about how to code completely or submit any particular claim for payment. Information provided is not intended to increase or maximize reimbursement by any payer. The information provided represents NxThera’s understanding of current reimbursement policies. The suggested codes are to be used only to facilitate appropriate coding and should not be construed as recommended guidelines in the establishment of policy or practice. Any descriptions of services contained in this guide are for the purpose of illustrating typical clinical services and not intended to represent practice guidelines or standards of care. NxThera makes no representations or warranties with respect to the contents of this guide and disclaims any implied guarantee or warranty of fitness for any particular purpose. NxThera will not be liable to any individual or entity for any losses or damages that may be incurred by the use of this guide. Furthermore, NxThera specifically disclaims any liability or responsibility for the results or consequences of any actions taken in reliance on the statements, opinions or suggestions in this guide. It is always the provider’s responsibility to determine coverage and submit appropriate codes and charges for services rendered. Providers should check and verify current policies and requirements with the payer for any particular patient. It is important to verify coverage for each patient as policies and guidelines can vary by payer and plan. The key in all coding and billing to payers is to be truthful and not misleading and make full disclosures to the payer about how the product has been used and the procedures necessary to use the product when seeking reimbursement for any product or procedure. In all cases, services billed must be medically necessary, actually performed as reported and appropriately documented.
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 3
overview
BENIGN PROSTATIC HYPERPLASIA (BPH)
BPH is a localized, enlargement of the prostate gland characterized by a proliferation of tissue within the prostate. This
excess growth of prostate tissue compresses and obstructs the urethra, reducing the flow of urine from the bladder and
sometimes blocking it entirely.
THE REZŪM SYSTEM
The Rezūm System includes a handheld delivery device and generator. The system uses radiofrequency (RF) power to
create thermal energy in the form of sterile water vapor (steam). During this transurethral needle ablation procedure,
controlled doses of the wet thermal energy created with RF power are convectively delivered directly to targeted
areas of the prostate gland through the tissue interstices. Condensation releases the stored thermal energy of the
RF water vapor directly against the walls of the tissue cells within the treatment zone, immediately denaturing the
cell membranes, and causing almost instantaneous tissue cell death. The body’s immune system response causes this
denatured tissue to be resorbed over a matter of weeks, and this reduction in hyperplastic prostate tissue volume
reduces the obstruction of the urethra, relieving the lower urinary tract symptoms associated with BPH and enabling
improved urinary flow.
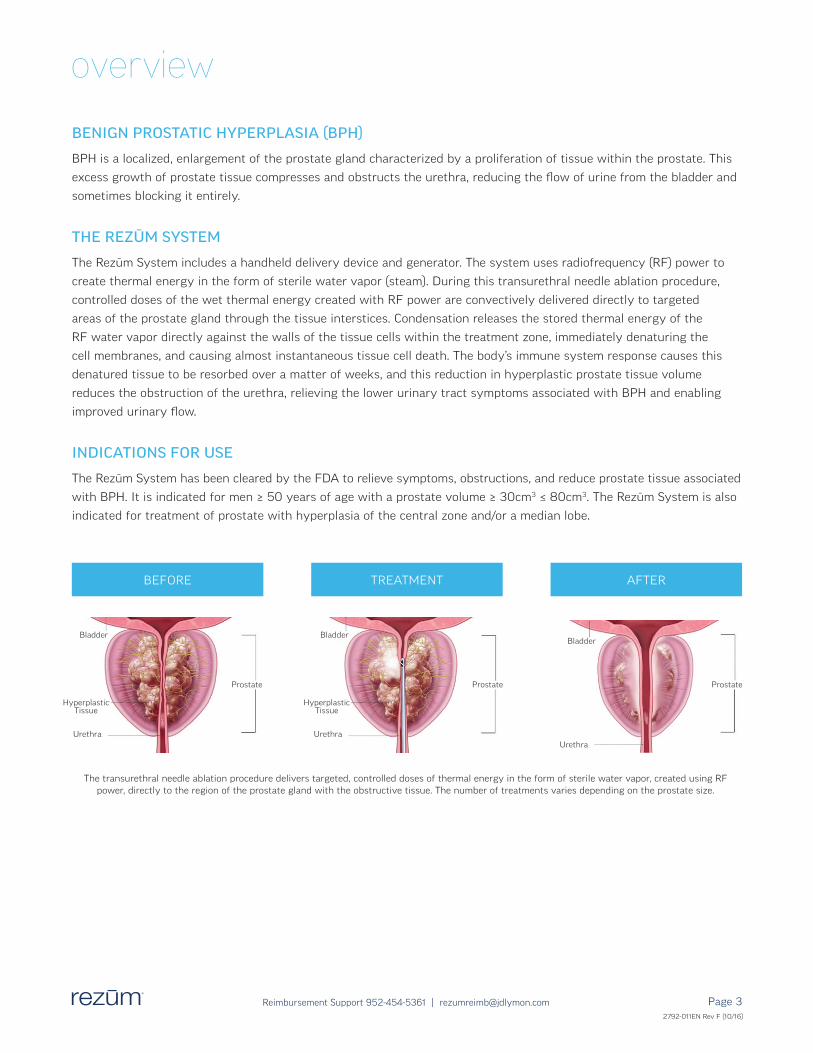
INDICATIONS FOR USE
The Rezūm System has been cleared by the FDA to relieve symptoms, obstructions, and reduce prostate tissue associated
with BPH. It is indicated for men ≥ 50 years of age with a prostate volume ≥ 30cm3 ≤ 80cm3. The Rezūm System is also
indicated for treatment of prostate with hyperplasia of the central zone and/or a median lobe.
The transurethral needle ablation procedure delivers targeted, controlled doses of thermal energy in the form of sterile water vapor, created using RF power, directly to the region of the prostate gland with the obstructive tissue. The number of treatments varies depending on the prostate size.
BEFORE AFTERTREATMENT
Bladder BladderBladder
Prostate Prostate Prostate
Urethra UrethraUrethra
Hyperplastic Tissue
Hyperplastic Tissue
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 4
coding and payment
This guide has been developed to assist you in reporting radiofrequency thermotherapy procedures to treat BPH using
the Rezūm System. It is important to understand that coding is specific to the procedure or services being performed,
not to the device being used. Ultimately it is the provider’s responsibility to choose codes that accurately describe the
patient’s condition and the procedure or services performed.
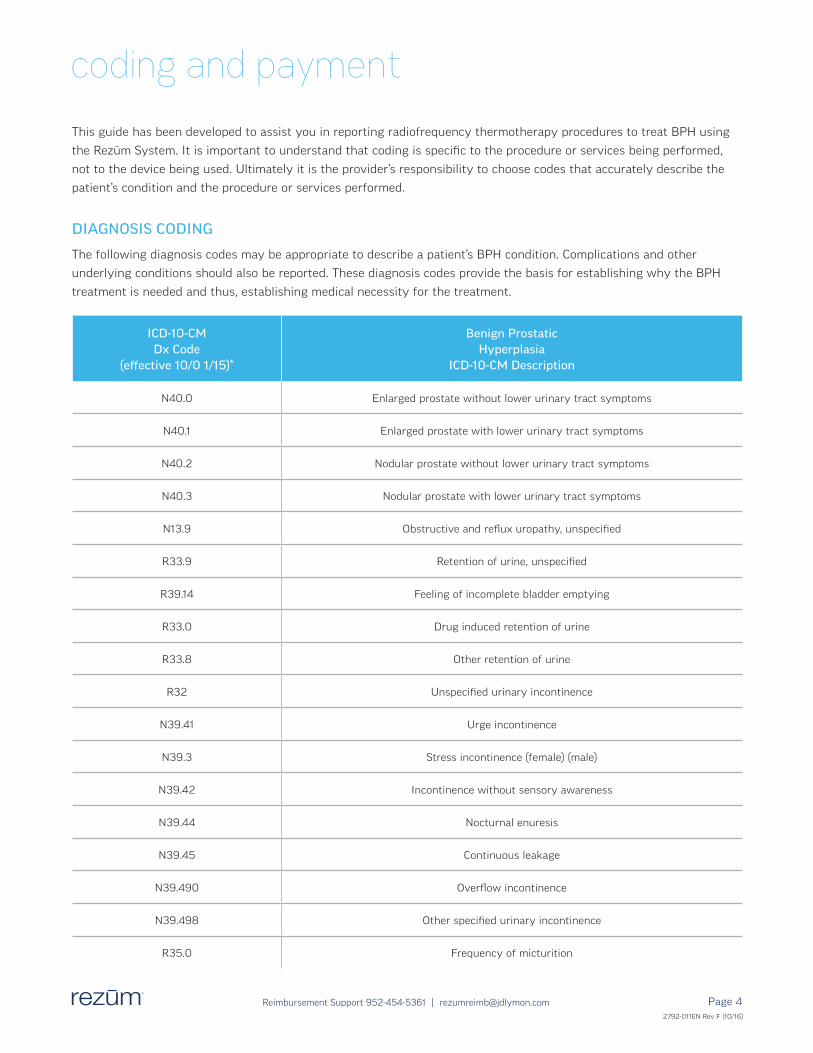
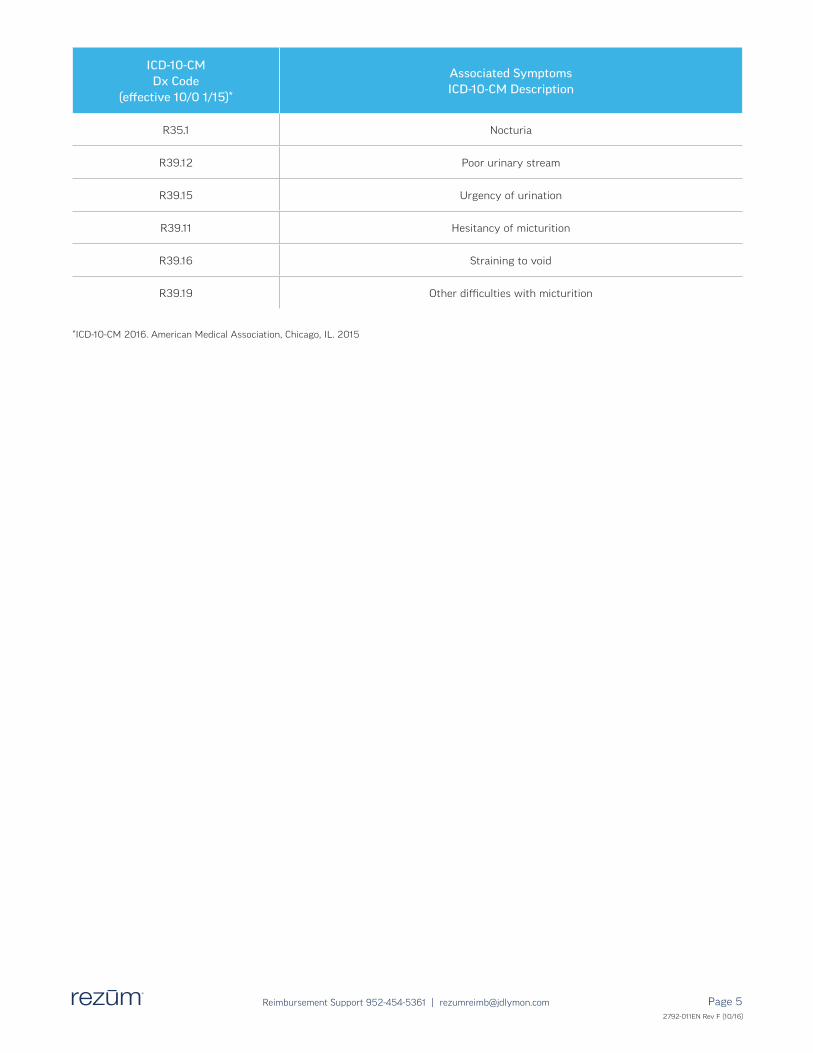
DIAGNOSIS CODING
The following diagnosis codes may be appropriate to describe a patient’s BPH condition. Complications and other
underlying conditions should also be reported. These diagnosis codes provide the basis for establishing why the BPH
treatment is needed and thus, establishing medical necessity for the treatment.
ICD-10-CM Dx Code
(effective 10/0 1/15)*
Benign Prostatic Hyperplasia
ICD-10-CM Description
N40.0 Enlarged prostate without lower urinary tract symptoms
N40.1 Enlarged prostate with lower urinary tract symptoms
N40.2 Nodular prostate without lower urinary tract symptoms
N40.3 Nodular prostate with lower urinary tract symptoms
N13.9 Obstructive and reflux uropathy, unspecified
R33.9 Retention of urine, unspecified
R39.14 Feeling of incomplete bladder emptying
R33.0 Drug induced retention of urine
R33.8 Other retention of urine
R32 Unspecified urinary incontinence
N39.41 Urge incontinence
N39.3 Stress incontinence (female) (male)
N39.42 Incontinence without sensory awareness
N39.44 Nocturnal enuresis
N39.45 Continuous leakage
N39.490 Overflow incontinence
N39.498 Other specified urinary incontinence
R35.0 Frequency of micturition
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 5
ICD-10-CM Dx Code
(effective 10/0 1/15)*
Associated Symptoms ICD-10-CM Description
R35.1 Nocturia
R39.12 Poor urinary stream
R39.15 Urgency of urination
R39.11 Hesitancy of micturition
R39.16 Straining to void
R39.19 Other difficulties with micturition
*ICD-10-CM 2016. American Medical Association, Chicago, IL. 2015
2792-011EN Rev F (10/16)

2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 6
PHYSICIAN CODING & PAYMENT
Physicians and other providers use CPT codes to report procedures and services. Medicare reimburses CPT codes
under a fee schedule based on the Relative Value Units (RVUs) assigned to each code. Private payers may base their
reimbursement rates on the RVUs published by Medicare, or on other provider contracted and/or negotiated amounts.
The Rezūm System uses radiofrequency power to create thermal energy. This thermal energy ablates the targeted
prostate tissue during a series of treatments delivered during each procedure. NxThera sought guidance on appropriate
coding for the radiofrequency thermotherapy ablation procedure using the Rezūm System through the American
Urological Association’s (AUA) Coding & Reimbursement Committee (CRC). Based on their thorough review, the AUA CRC
confirmed the procedure using the Rezūm system may be reported using CPT code 53852, transurethral destruction
of prostate tissue; by radiofrequency thermotherapy.* BPH treatment procedures using either the Prostiva™ or Rezūm
devices are appropriately reported with CPT code 53852 because CPT codes are developed to describe
procedures and services, not specific to any particular device or product brand.
To report the Rezum procedure on medical claims, use CPT® code 53852 Transurethral destruction of prostate tissue; by
radiofrequency thermotherapy. The Rezum System uses radiofrequency energy to transform sterile water into stored thermal
energy in the form of vapor, or steam. This water vapor is convectively delivered directly into the obstructive prostate tissue
that causes BPH, where condensation releases enough thermal energy to denature the targeted prostate tissue cells to cause
necrosis. The treated tissue is absorbed by the body’s natural immune system. It is intended to relieve symptoms, obstruction,
and reduce prostate tissue associated with benign prostatic hyperplasia (BPH). It is also indicated for treatment of prostates
with hyperplasia of the central zone and/or a median lobe.
https://www.auanet.org/resources/biopsy-procedures.cfm
* American Urological Association: Prostate Procedures Coding and Reimbursement Q&A. https://www.auanet.org/resources/biopsy-procedures.cfm
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 7
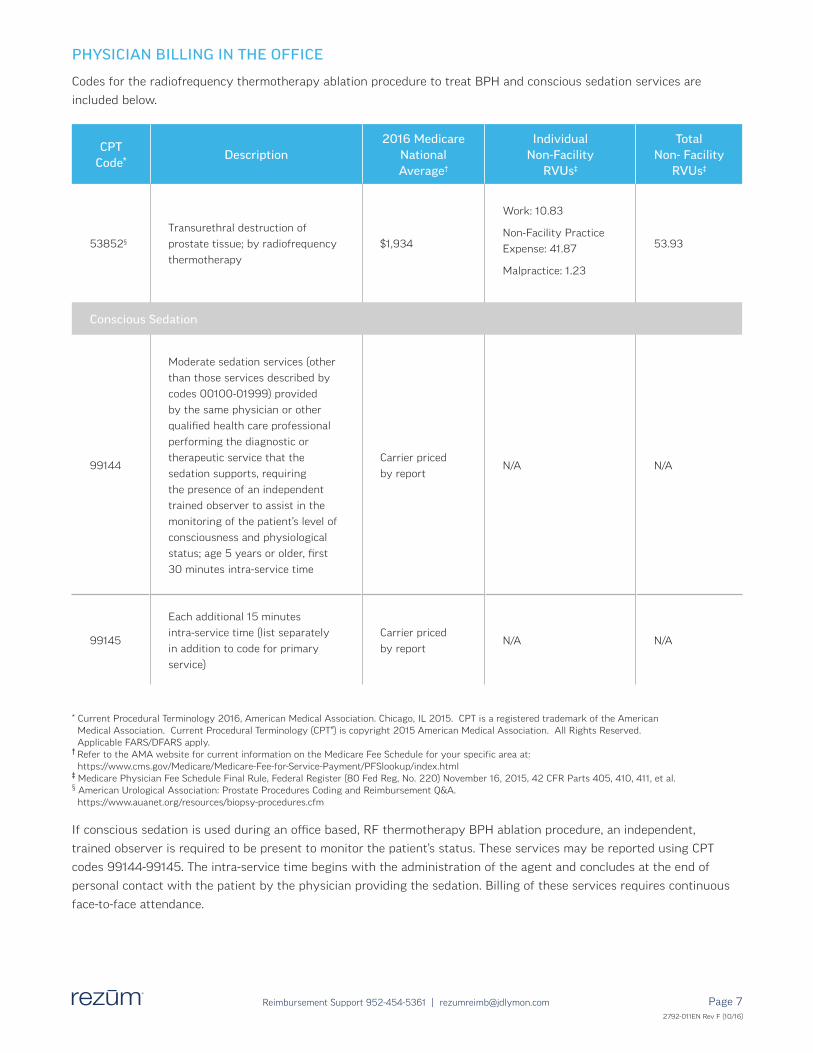
PHYSICIAN BILLING IN THE OFFICE
Codes for the radiofrequency thermotherapy ablation procedure to treat BPH and conscious sedation services are
included below.
CPT Code*
Description2016 Medicare
National Average†
Individual Non-Facility
RVUs‡
Total Non- Facility
RVUs‡
53852§
Transurethral destruction of
prostate tissue; by radiofrequency
thermotherapy
$1,934
Work: 10.83
Non-Facility Practice
Expense: 41.87
Malpractice: 1.23
53.93
Conscious Sedation
99144
Moderate sedation services (other
than those services described by
codes 00100-01999) provided
by the same physician or other
qualified health care professional
performing the diagnostic or
therapeutic service that the
sedation supports, requiring
the presence of an independent
trained observer to assist in the
monitoring of the patient’s level of
consciousness and physiological
status; age 5 years or older, first
30 minutes intra-service time
Carrier priced
by reportN/A N/A
99145
Each additional 15 minutes
intra-service time (list separately
in addition to code for primary
service)
Carrier priced
by reportN/A N/A
* Current Procedural Terminology 2016, American Medical Association. Chicago, IL 2015. CPT is a registered trademark of the American Medical Association. Current Procedural Terminology (CPT®) is copyright 2015 American Medical Association. All Rights Reserved. Applicable FARS/DFARS apply.† Refer to the AMA website for current information on the Medicare Fee Schedule for your specific area at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PFSlookup/index.html‡ Medicare Physician Fee Schedule Final Rule, Federal Register (80 Fed Reg, No. 220) November 16, 2015, 42 CFR Parts 405, 410, 411, et al.§ American Urological Association: Prostate Procedures Coding and Reimbursement Q&A. https://www.auanet.org/resources/biopsy-procedures.cfm
If conscious sedation is used during an office based, RF thermotherapy BPH ablation procedure, an independent,
trained observer is required to be present to monitor the patient’s status. These services may be reported using CPT
codes 99144-99145. The intra-service time begins with the administration of the agent and concludes at the end of
personal contact with the patient by the physician providing the sedation. Billing of these services requires continuous
face-to-face attendance.
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 8
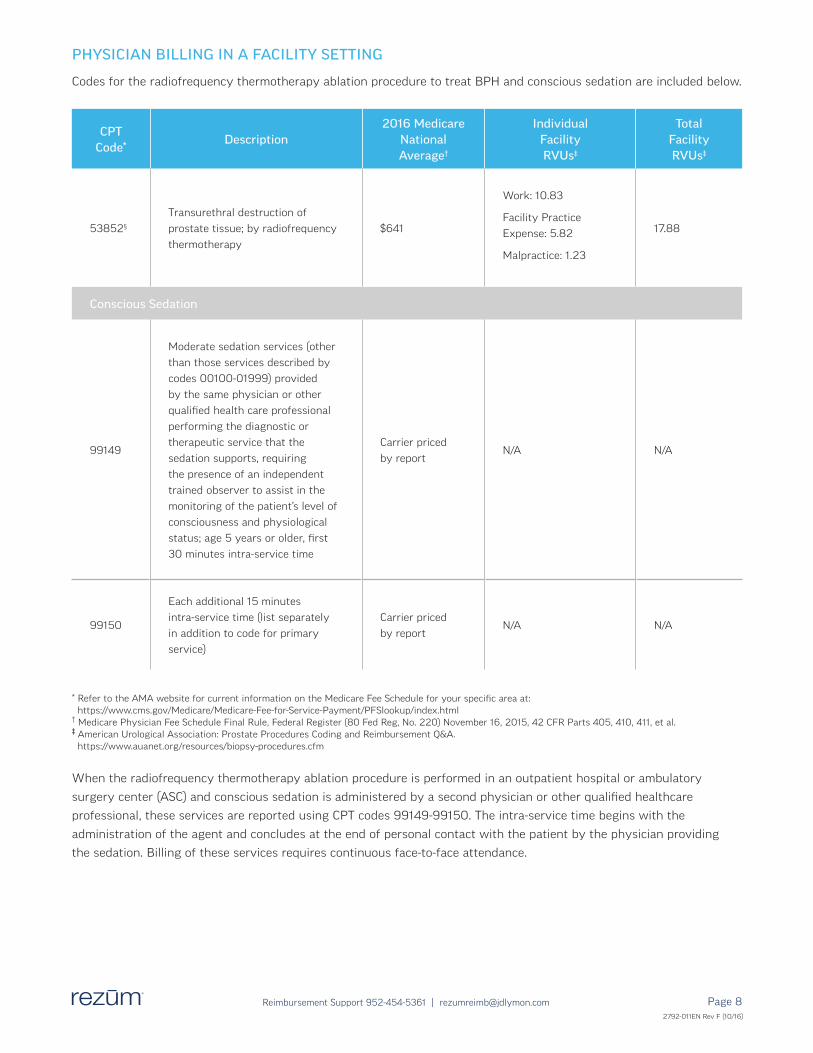
PHYSICIAN BILLING IN A FACILITY SETTING
Codes for the radiofrequency thermotherapy ablation procedure to treat BPH and conscious sedation are included below.
* Refer to the AMA website for current information on the Medicare Fee Schedule for your specific area at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PFSlookup/index.html† Medicare Physician Fee Schedule Final Rule, Federal Register (80 Fed Reg, No. 220) November 16, 2015, 42 CFR Parts 405, 410, 411, et al.‡ American Urological Association: Prostate Procedures Coding and Reimbursement Q&A. https://www.auanet.org/resources/biopsy-procedures.cfm
When the radiofrequency thermotherapy ablation procedure is performed in an outpatient hospital or ambulatory
surgery center (ASC) and conscious sedation is administered by a second physician or other qualified healthcare
professional, these services are reported using CPT codes 99149-99150. The intra-service time begins with the
administration of the agent and concludes at the end of personal contact with the patient by the physician providing
the sedation. Billing of these services requires continuous face-to-face attendance.
CPT Code*
Description2016 Medicare
National Average†
Individual Facility RVUs‡
Total Facility RVUs‡
53852§
Transurethral destruction of
prostate tissue; by radiofrequency
thermotherapy
$641
Work: 10.83
Facility Practice
Expense: 5.82
Malpractice: 1.23
17.88
Conscious Sedation
99149
Moderate sedation services (other
than those services described by
codes 00100-01999) provided
by the same physician or other
qualified health care professional
performing the diagnostic or
therapeutic service that the
sedation supports, requiring
the presence of an independent
trained observer to assist in the
monitoring of the patient’s level of
consciousness and physiological
status; age 5 years or older, first
30 minutes intra-service time
Carrier priced
by reportN/A N/A
99150
Each additional 15 minutes
intra-service time (list separately
in addition to code for primary
service)
Carrier priced
by reportN/A N/A
2792-011EN Rev F (10/16)
Page 92792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected]
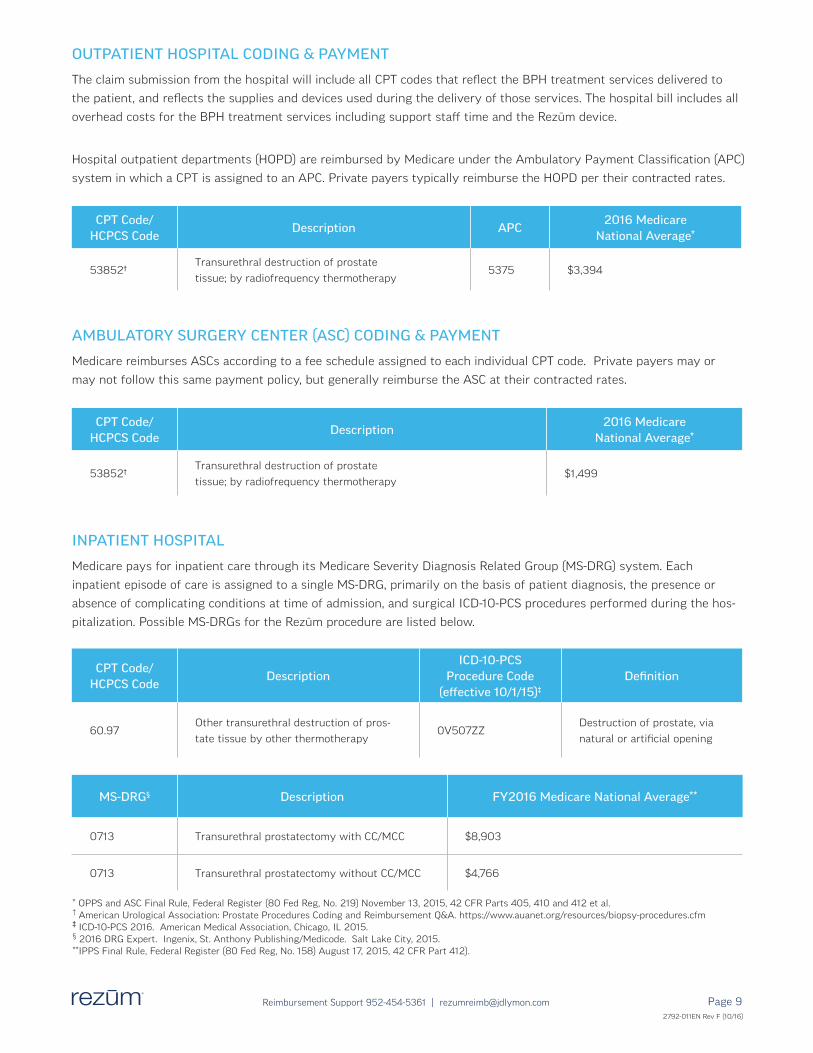
OUTPATIENT HOSPITAL CODING & PAYMENT
The claim submission from the hospital will include all CPT codes that reflect the BPH treatment services delivered to
the patient, and reflects the supplies and devices used during the delivery of those services. The hospital bill includes all
overhead costs for the BPH treatment services including support staff time and the Rezūm device.
Hospital outpatient departments (HOPD) are reimbursed by Medicare under the Ambulatory Payment Classification (APC)
system in which a CPT is assigned to an APC. Private payers typically reimburse the HOPD per their contracted rates.
CPT Code/ HCPCS Code
Description APC2016 Medicare
National Average*
53852†Transurethral destruction of prostate
tissue; by radiofrequency thermotherapy5375 $3,394
CPT Code/ HCPCS Code
Description2016 Medicare
National Average*
53852†Transurethral destruction of prostate
tissue; by radiofrequency thermotherapy$1,499
AMBULATORY SURGERY CENTER (ASC) CODING & PAYMENT
Medicare reimburses ASCs according to a fee schedule assigned to each individual CPT code. Private payers may or
may not follow this same payment policy, but generally reimburse the ASC at their contracted rates.
* OPPS and ASC Final Rule, Federal Register (80 Fed Reg, No. 219) November 13, 2015, 42 CFR Parts 405, 410 and 412 et al. † American Urological Association: Prostate Procedures Coding and Reimbursement Q&A. https://www.auanet.org/resources/biopsy-procedures.cfm‡ ICD-10-PCS 2016. American Medical Association, Chicago, IL 2015.§ 2016 DRG Expert. Ingenix, St. Anthony Publishing/Medicode. Salt Lake City, 2015.**IPPS Final Rule, Federal Register (80 Fed Reg, No. 158) August 17, 2015, 42 CFR Part 412).
CPT Code/ HCPCS Code
DescriptionICD-10-PCS
Procedure Code(effective 10/1/15)‡
Definition
60.97Other transurethral destruction of pros-
tate tissue by other thermotherapy0V507ZZ
Destruction of prostate, via
natural or artificial opening
INPATIENT HOSPITAL
Medicare pays for inpatient care through its Medicare Severity Diagnosis Related Group (MS-DRG) system. Each
inpatient episode of care is assigned to a single MS-DRG, primarily on the basis of patient diagnosis, the presence or
absence of complicating conditions at time of admission, and surgical ICD-10-PCS procedures performed during the hos-
pitalization. Possible MS-DRGs for the Rezūm procedure are listed below.
MS-DRG§ Description FY2016 Medicare National Average**
0713 Transurethral prostatectomy with CC/MCC $8,903
0713 Transurethral prostatectomy without CC/MCC $4,766
2792-011EN Rev F (10/16)

2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 10
benefits and coverage
THE PRIOR AUTHORIZATION PROCESS
MEDICARE
Since Medicare does not have a process to review prior authorization requests, it is up to the provider to determine
coverage guidelines either by checking an individual payer’s website or contacting the payer directly. The treatment
of BPH by radiofrequency thermotherapy is not new and is appropriately reported with CPT code 53852. A search of
Medicare’s Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) show that the Medicare
Administrative Contractors (MACs) are not managing the treatment of this disease by radiofrequency thermotherapy,
and consider it to be medically necessary for patients diagnosed with BPH.
COMMERCIAL PAYERS
Prior authorization, sometimes referred to as “pre-certification,” is the process used to confirm if a patient’s proposed
service or procedure is medically necessary. Whenever possible, prior authorization should occur before a procedure
is provided. You are advised to check with a patient’s individual health plan for their policy on prior authorization for
reporting procedures using CPT code 53852. Included in this Reimbursement Guide are sample letters which may be
used at different points during this process.
STEP 1: Allow up to 30 days for the payer to process the request
STEP 2: Allow an additional 30-45 days for each level of appeal
Up to four months may lapse before �nal approval
STEP 1
Follow payer process to request prior
authorization (or pre-determination)
of CPT code 53852.
Include:
• Patient history and medical
necessity for the procedure
• CPT and diagnosis codes
PRIOR AUTHORIZATION REQUEST
STEP 2
If the payer does not approve the
request for CPT 53852, the surgeon
and the patient may write appeal letters
to the payer.
If the appeal is denied, the patient
may request an external review with an
Independent Review Organization (IRO).
APPEALS PROCESS
STEP 3
Once authorization has been approved
by the payer, you may proceed with
the thermotherapy ablation procedure
and billing the payer.
PROCEDURE
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 11
frequently asked questions
Current Procedural Terminology 2016, American Medical Association . Chicago, IL 2015 . CPT is a registered trademark of the American Medical Association . Current Procedural Terminology (CPT®) is copyright 2015 American Medical Association . All Rights Reserved . Applicable FARS/DFARS apply .
Q . WHAT IS THE CPT CODE FOR THE REZŪM SYSTEM?
A. In December 2014, the American Urological
Association’s Coding and Reimbursement Committee
determined that CPT code 53852 (Transurethral
destruction of prostate tissue; by radiofrequency
thermotherapy) should be used to report the
transuretheral needle ablation procedure using the
Rezūm System.*
To report the Rezum procedure on medical claims, use CPT® code 53852 Transurethral destruction of prostate tissue; by radiofrequency thermotherapy. The Rezum System uses radiofrequency energy to transform sterile water into stored thermal energy in the form of vapor, or steam. This water vapor is convectively delivered directly into the obstructive prostate tissue that causes BPH, where condensation releases enough thermal energy to denature the targeted prostate tissue cells to cause necrosis. The treated tissue is absorbed by the body’s natural immune system. It is intended to relieve symptoms, obstruction, and reduce prostate tissue associated with benign prostatic hyperplasia (BPH). It is also indicated for treatment of prostates with hyperplasia of the central zone and/or a median lobe.
https://www.auanet.org/resources/biopsy-procedures.cfm
Q . DOES MEDICARE COVER CPT CODE 53852?
A. Medicare Administrative Contractors (MACs) consider
radiofrequency thermotherapy ablation reported using
CPT code 53852 medically necessary for treating
patients with BPH.
Q . DO PRIVATE PAYERS COVER CPT CODE 53852?
A. Most payers consider CPT code 53852 medically
necessary for patients with benign prostatic
hypertrophy (BPH). Providers should always verify
a patient’s benefits and any prior authorization
requirements prior to scheduling a procedure.
Q . IS PRIOR AUTHORIZATION OR PRE- CERTIFICATION REQUIRED FOR THE REZŪM SYSTEM?
A. The Rezūm System is a technology used to perform
the transurethral RF thermotherapy procedure to treat
BPH, and is reported using CPT code 53852. For the
majority of payers, this procedure code is not on their
prior authorization list. It is advised, however, that
you check with patients’ individual health plans for
their policy on prior authorization and pre-certification
requirements for CPT code 53852.If a patient’s payer
requires prior authorization, this should occur prior
to the procedure being provided. Remember you are
seeking authorization for the procedure under CPT
code 53852, not for the specific device being used
in the procedure. NxThera can provide information
that will help you with this process, including sample
letters. Should you need assistance, please contact
952-454-5361.
Q . HOW SHOULD CONSCIOUS SEDATION BE REPORTED IF USED IN THE PHYSICIAN OFFICE?
A. If conscious sedation is used during an office based,
RF thermotherapy BPH ablation procedure, an
independent, trained observer is required to be present
to monitor the patient’s status. These services may
be reported using CPT codes 99144-99145. The intra-
service time begins with the administration of the
agent and concludes at the end of personal contact
with the patient by the physician providing the
sedation. Billing of these services requires continuous
face-to-face attendance
Q . ARE OTHER PROCEDURES INCLUDED IN THE PAYMENT FOR CPT CODE 53852?
A. CPT code 53852 includes administration of a prostate
block and transrectal ultrasound, if performed. These
services should not be reported separately as they are
considered bundled and included in the payment for
the surgical procedure.
* American Urological Association: Prostate Procedures Coding and Reimbursement Q&A. https://www.auanet.org/resources/biopsy-procedures.cfm
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 12
SAMPLE PRIOR AUTHORIZATION REQUEST – CPT 53852
In lieu of a prior authorization request form, a physician can submit a formal letter requesting a prior authorization. The following letter can be modified with patient- and provider-specific information and attached to written prior authorization requests for the procedure:
[Insert Date]
VIA FACSIMILE: [insert insurer’s prior authorization fax number]
[Insert Health Insurer Name]
[Insert Street Address]
[Insert City, State Zip]
RE: Prior Authorization Request for [Patient’s Name/insurance I.D. Number]
To Whom It May Concern:
This letter is to request prior authorization for radiofrequency thermotherapy ablation of the prostate. I am writing on
behalf of [patient’s name], who suffers from [insert patient diagnosis]. He has been on BPH drug medications for [time
period] and these are not providing symptom relief. Therefore, I would like my patient to undergo a transurethral proce-
dure that uses thermal energy created with radiofrequency power to treat obstructive prostate tissue by delivering tar-
geted, controlled doses of thermal energy directly to the prostate gland tissue. The prostate tissue cell membranes are
denatured causing immediate cell death, and the necrotic tissue is absorbed over time by the body’s immune system
response. This treatment results in a reduction in the volume of obstructive prostate tissue, relieving the
symptoms of BPH by reducing the compression of the urethra.
Transurethral radiofrequency thermotherapy ablation of the prostate to treat BPH is the best option for my patient. It
enables a targeted and controlled treatment of the enlarged prostate tissue that is causing his BPH, and is designed to
minimize post-procedure complications.
I will perform this procedure in the [insert setting of care]. The procedure for [patient name] is scheduled for [date].
I will be reporting the following CPT code for performance of this procedure: 53852 (Transurethral destruction of
prostate tissue; by radiofrequency thermotherapy).
I request confirmation that this procedure is a covered benefit, and that associated professional fees will be covered.
If you require additional information, please contact me at [insert telephone number].
Sincerely,
[Physician Name]
[Provider number]
[Street Address]
[City, State Zip]
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 13
SAMPLE LETTER OF MEDICAL NECESSITY – CPT 53852
The following letter can be modified with patient- and provider-specific information and used to appeal a denial for prior authorization of the procedure for the treatment of BPH:
[Insert Date]
VIA FACSIMILE: [insert insurer’s prior authorization fax number]
[Insert Health Insurer Name]
[Insert Street Address]
[Insert City, State Zip]
RE: Appeal of Prior Authorization Denial for [Insert Patient’s Name/Insurance I.D. Number]
To Whom It May Concern:
I am writing on behalf of [patient’s name], who suffers from [insert patient diagnosis]. I am writing to request that you
reconsider your previous denial of the prior authorization for transurethral radiofrequency thermotherapy ablation of the
prostate to treat BPH. [Describe the patient’s current status and intended treatment pathway.]
As [patient’s name]’s treating physician, I believe this procedure is the best option to treat this patient’s BPH. He
has been on BPH drug medications for [time period] and these are not providing symptom relief. I have scheduled
the procedure for [date] in anticipation of a positive response from you. The following CPT code will be reported in
connection with performing this procedure: 53852 (transurethral destruction of prostate tissue; by radiofrequency
thermotherapy).
Radiofrequency thermotherapy ablation is a standard procedure for treating BPH. It is my professional preference to
use this procedure which enables a targeted and controlled treatment of the enlarged prostate tissue. This office-based/
outpatient therapy can be conducted under local anesthesia, avoids complications associated with other BPH treatments
and has clinically proven results with symptom improvement in as soon as two weeks1.
I request confirmation as soon as possible that you will respect my professional recommendation and preference to
perform this procedure with the prior authorization requested. I am very happy to discuss this request. Please contact
me at [insert telephone number].
Sincerely,
[Physician Name]
[Provider number]
[Street Address]
[City, State Zip]
1 McVary KT, Gange SN, Gittelman MC, et al. Minimally Invasive Prostate Convective Water Vapor Energy Ablation: A Multicenter, Randomized, Controlled Study for the Treatment of Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia. The Journal of Urology. 2016;195(5):1529-1538. doi:10.1016/j.juro.2015.10.181.
2792-011EN Rev F (10/16)
2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 14
the rezūm system bibliography
MANUSCRIPTS
1. McVary KT, Gange SN, Gittelman MC, Goldberg KA, Patel K, Shore ND, Levin RM, Rousseau M, Beahrs JR, Kaminetsky
J, Cowan BE, Cantrill CH, Mynderse LA, Ulchaker JC, Larson TR, Dixon CM, Roehrborn CG. Erectile and Ejaculatory
Function Preserved with Convective Water Vapor Energy Treatment of LUTS Secondary to BPH: Randomized
Controlled Study. J Sex Med 2016;13:924-33.
2. McVary KT, Gange SN, Gittelman MC, Goldberg KA, Patel K, Shore ND, Levin RM, Rousseau M, Beahrs JR, Kaminetsky
J, Cowan BE, Cantrill CH, Mynderse LA, Ulchaker JC, Larson TR, Dixon CM, Roehrborn CG. Minimally Invasive Prostate
Convective Water Vapor Energy (WAVE) Ablation: A Multicenter, Randomized, Controlled Study for Treatment of
Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia. J Urol 2016;195:1529-39.
3. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Wagrell L, Tornblom M, Mynderse L, Larson T. Efficacy and Safety of
Rezūm System Water Vapor Treatment for Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia.
UROLOGY. 2015;86:1042-1047.
4. Mynderse LA, Hanson D, Robb R, Pacik D, Vit V, Varga G, Wagrell L, Tornblom M, Rido Cedano E, Woodrum D, Dixon
CM, Larson TR. Rezūm System Water Vapor Treatment for Lower Urinary Tract Symptoms/Benign Prostatic
Hyperplasia: Validation of Convective Thermal Energy Transfer and Characterization with Magnetic Resonance
Imaging and 3D Renderings. UROLOGY. 2015;86:122-127.
5. Dixon CM, Cedano ER, Mynderse LA, Larson TR. Transurethral convective water vapor as a treatment for lower
urinary tract symptomatology due to benign prostatic hyperplasia using the Rezūm® system: evaluation of acute
ablative capabilities in the human prostate. Res Reports Urol. 2015;7:13-18.
REVIEW ARTICLES
1. Shore ND. An outcomes review of minimally invasive transurethral convective water vapor energy (WAVE) therapy
for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Curr Bladder Dysfunct Rep
2016;11:153-159.
2. Dixon C, Larson T, Hoey M. The Rezūm System: Minimally invasive treatment for BPH using water vapor (steam): why
consider it? Curr Bladder Dysfunct Rep 2015;10:156-159.
3. Ebbing J, Bachmann A. Anesthesia-free procedures for benign prostate obstruction: worth it? Curr Opin Urol
2015;25:32–39.
ABSTRACTS
1. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Mynderse L, Larson, T. Convective Water Vapor Energy (WAVE)
Ablation: Two-Year Results Following Treatment of Lower Urinary Tract Symptoms Secondary to Benign Prostatic
Hyperplasia. Abstract ID 16-5612. American Urological Association Annual Meeting 2016, San Diego, California.
2. McVary K, Gange, S, et al. Treatment of Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia with
Convective Water Vapor Energy Ablation: Preserved Erectile and Ejaculatory Function. Abstract ID 16-1219. American
Urological Association Annual Meeting 2016, San Diego, California.
3. McVary K, Roehrborn C, et al. Using the Thermal Energy of Convectively Delivered Water Vapor for the Treatment
of Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia: The Rezūm II Study. Abstract #15-8068.
Plenary II Late-Breaking Abstract Session. American Urological Association Annual Meeting 2015, New Orleans,
Louisiana.
2792-011EN Rev F (10/16)

2792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected] Page 15
4. Mynderse L, Hanson D, Robb R, Rijo Cedano E, Pacik D, Vit V, Varga G, Larson T, Dixon C. Rezūm® System Water
Vapor Treatment for Benign Prostatic Hyperplasia: Characterization with Magnetic Resonance Imaging and 3D
Rendering. Abstract #1890. American Urological Association Annual Meeting 2014, Orlando, Florida.
5. Wagrell L, Tornblom, M. Transurethral Water Vapor Therapy for BPH; A Single Center’s Experience Using the Rezūm®
System in an Office-based Setting. Abstract #1817. American Urological Association Annual Meeting 2014, Orlando,
Florida.
6. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Mynderse L, Larson, T. Transurethral Water Vapor Therapy for BPH;
1-year Clinical Results of the First-In-Man and Rezūm® I Clinical Trials Using the Rezūm® System. Abstract #1816.
American Urological Association Annual Meeting 2014, Orlando, Florida.
7. Wagrell L, Tornblom, M. Transurethral Water Vapor Therapy for BPH; A Single Center’s Experience Using the Rezūm®
System. Abstract #234. European Association of Urology 2014, Stockholm, Sweden.
8. Mynderse L, Hanson D, Robb R, Rijo Cedano E, Pacik D, Vit V, Varga G, Larson T, Dixon, C. Characterizing Rezūm®
System Water Vapor Treatments for Benign Prostatic Hyperplasia with Serial Magnetic Resonance Imaging and 3D
Rendering. Abstract #230. European Association of Urology 2014, Stockholm, Sweden.
9. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Mynderse L, Hanson D, Larson T. Transurethral High Energy Water
Vapor Therapy for BPH; Initial Clinical Results of the First-In-Man and Rezūm™ 1 Clinical Trials Using the Rezūm™
System. Journal of Endourology 2013, 27 (s1): A340. Abstract nr MP23-13.
10. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Mynderse L, Hanson D, Larson T. Serial MRI and 3D Rendering
Following Treatment of BPH Using High Energy Water Vapor Therapy and the Rezūm™ System; Initial Results from
the First-In-Man and Rezūm™ 1 Clinical Trials. Journal of Endourology 2013, 27 (s1): A69. Abstract nr MP03-08.
11. Dixon C, Pacik D, Huidobro C, Rijo Cedano E, Mynderse L, Hanson D, Hoey M, Larson T. Preliminary Data Following
Treatment with Vapor for BPH: The Rezūm System. Abstract #1476. World Congress of Endourology 2012, Istanbul,
Turkey.
12. Dixon C, Rijo Cedano E, Pacik D, Vit V, Varga G, Mynderse L, Hanson D, Larson T. Transurethral Water Vapor Therapy
for BPH; Initial Clinical Results of the First-In-Man and Rezūm I Pilot Study. Abstract #631. European Association of
Urology 2013, Milan, Italy.
13. Dixon C, Huidobro C, Rijo Cedano E, Hoey M, Larson T. Acute Effects in the Human Prostate Following Treatment
with High-Calorie Water Vapor (Rezūm). Abstract #0838. World Congress of Endourology 2012, Istanbul, Turkey.
WHITE PAPERS
1. Water Vapor for Tissue Ablation. Hoey MF. March 2009.
2792-011EN Rev F (10/16)

Page 162792-011EN Rev E (7/16)
Reimbursement Support 952-454-5361 | [email protected]
referencesCurrent Procedural Terminology 2016, American Medical Association. Chicago, IL 2015. CPT is a registered trademark
of the American Medical Association. Current Procedural Terminology (CPT®) is copyright 2015 American Medical
Association. All Rights Reserved. Applicable FARS/DFARS apply.
Medicare Physician Fee Schedule Final Rule, Federal Register (80 Fed Reg, No. 220) November 16, 2015, 42 CFR Parts
405, 410, 411, et al.
OPPS and ASC Final Rule, Federal Register (80 Fed Reg, No. 219) November 13, 2015, 42 CFR Parts 405, 410 and 412
et al.
Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective
Payment System Policy Changes and Fiscal Year 2016 Rates Final Rule, Federal Register (80 Fed Reg, No. 158) August
17, 2015, 42 CFR Part 412.
American Urological Association: Prostate Procedures Coding and Reimbursement Q&A.
https://www.auanet.org/resources/biopsy-procedures.cfm.
Hospital ICD-10-CM 2016. American Medical Association, Chicago, IL 2015.
ICD-10-PCS 2016. American Medical Association, Chicago, IL 2015.
ICD-10-CM 2016. American Medical Association, Chicago, IL 2015.
2792-011EN Rev F (10/16)
888-319-9691 | www.rezum.com
©2016 NxThera, Inc. All rights reserved. Rezūm is a registered trademark of NxThera, Inc.
Reimbursement Support952-454-5361