revised gleason grading system is a better predictor of indolent prostate cancer at the time of...
TRANSCRIPT
Original Study
Revised Gleason Grading System Is a BetterPredictor of Indolent Prostate Cancer at the Timeof Diagnosis: Retrospective Clinical-Pathological
Study on Matched Biopsy and RadicalProstatectomy Specimens
Francesca Giunchi,1 Eugenio Brunocilla,2 Marco Borghesi,2 Simona Rizzi,2
Martina Sofia Ricci,2 Daniele Romagnoli,2 Giuseppe Martorana,2
Riccardo Schiavina,2 Michelangelo Fiorentino1
AbstractWe showed that the application of the revised histological Gleason’s grade criteria identify patients withindolent prostate cancer better than the original scoring system. We enrolled for this purpose 134 men withhistologically diagnosed prostate cancer who would have suitable for active surveillance at the time of biopsybut invariably underwent radical prostatectomy.Introduction/Background: The increase of prostate cancer diagnosis after the introduction of prostate-specificantigen (PSA) screening resulted in overtreatment of patients with low risk tumors. The histological Gleason score(GS) revised in 2005 by the International Society of Urological Pathology (ISUP) is currently the most reliable tool toseparate aggressive from indolent prostate cancer. Materials and Methods: Using the new 2005 GS criteria weretrospectively evaluated biopsy and surgical samples of 1344 patients who underwent radical prostatectomy in ourinstitution. According to the new GS criteria we then selected 134 patients who would have been suitable for activesurveillance at the time of biopsy (at least 2 positive cores, PSA < 10 ng/mL, GS � 6). We finally assessed theaccuracy of the revised GS in biopsy to predict indolent cancer in the prostatectomy specimens. Results: The meanGS increased from 6 to 7 after histological revision in biopsy and prostatectomy specimens. Histological revisiondetermined a significant decrease of patients with GS � 6 and an increase of those with GS � 7 (all P < .001). Theaverage of pathologically indolent disease (organ-confined, GS � 6 at surgery, tumor of any volume) significantlydecreased after histological revision (P < .001). Conclusion: The revised ISUP 2005 criteria for Gleason gradingprovided better stratification of GS � 6 prostate cancer and improved the accuracy for the histological diagnosis ofindolent prostate cancer in biopsy and radical prostatectomy specimens.
Clinical Genitourinary Cancer, Vol. -, No. -, --- ª 2014 Elsevier Inc. All rights reserved.Keywords: Active surveillance, Gleason grading, Histopathology, Indolent tumor, Prostate cancer
IntroductionScreening with prostate-specific antigen (PSA) has disclosed the
issue of the overdiagnosis and the optimal treatment of clinicallyindolent prostate cancer. Considering the slow-growing behavior of
Michelangelo Fiorentino and Riccardo Schiavina contributed equally to this work.
1Pathology Service, Addarii Institute of Oncology, S. Orsola-Malpighi Hospital,University of Bologna, Bologna, Italy2Department of Urology, S. Orsola-Malpighi Hospital, University of Bologna,Bologna, Italy
1558-7673/$ - see frontmatter ª 2014 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.clgc.2014.01.009
indolent prostate cancer, active surveillance represents a safe alter-native treatment option for old subjects with comorbidities andshort life expectancy or a responsible approach to delay surgery inyoung motivated patients.1-3 The concept of active surveillance is
Submitted: Dec 10, 2013; Accepted: Jan 23, 2014
Address for correspondence: Michelangelo Fiorentino, MD, PhD, Pathology Service,Addarii Institute of Oncology, Viale Ercolani 4/2, 40138, S. Orsola-Malpighi Hospital,Bologna 40138, ItalyFax: þ39-0516363782; e-mail contact: [email protected]
Clinical Genitourinary Cancer Month 2014 - 1

Revised GS and Indolent Prostate Cancer
2 - Cli
based on the awareness that approximately 50% of newly diagnosedprostate cancers in the PSA era are small-size tumors that in mostinstances would not have been discovered without the screening.4,5
In the present post-PSA era, patients with indolent prostate cancershould avoid the adverse effects of radical prostatectomy, and thosewith aggressive tumors would benefit from radical therapy.6
However, a small percentage of patients with a diagnosis of in-dolent prostate cancer still develop aggressive disease, essentiallybecause a focus of high-risk cancer was already present but wasunderestimated at the time of diagnosis. Even if high-risk patientscan be identified with reasonable accuracy during the strict follow-up of active surveillance,7,8 and effectively treated in most cases,9
the key step is the initial diagnosis of indolent prostate cancer. Thedefinition of indolent (very low risk) prostate cancer greatly de-pends on the Gleason score (GS) that is currently the most reliableprognosticator of this tumor type. The original histopathologicalGleason grading was revised in 2005 and a further revision wasproposed in 2010.10,11 The 2005 revision of the Gleason systemgenerally resulted in an upgrade of at least 1 point in score, andmore importantly, in a better definition of the low grade (GS � 6)tumors.12 Unfortunately, these Gleason system updates have notbeen fully acknowledged in every institution with a significantinterobserver variability among pathologists in different centers.13
Centralized revision of the GS on biopsy by dedicated genitouri-nary pathologists is required by most active surveillance protocolsto warrant the reliability of the initial diagnosis that in most in-stances should fit within the GS � 6.14 Currently, the main reasonfor patient withdrawal from active surveillance protocols is theupgrading of the GS to � 7 in the repeated biopsy samples.15 Inthis proof-of-principle study, we investigated the ability of therevised GS to define a series of indolent prostate tumors throughcentralized histological revision. In particular, we retrospectivelyselected a population of prostate cancer patients who were eligiblefor entering an active surveillance protocol but invariably underwentradical prostatectomy. We reviewed the matched biopsy and sur-gical samples for GS and stage and compared it with the outcome.
Materials and MethodsPatient Population
Among 1344 patients who underwent radical prostatectomybetween March 2004 and May 2011 in our institution, we iden-tified 134 men (10%) with complete clinical and follow-up data,who would have fulfilled at the time of biopsy the inclusion criteriaof the Prostate Cancer Research International Active Surveillanceprotocol.9 These criteria comprised: (1) PSA level � 10.0 ng/mL;(2) clinical stage T1c/T2; (3) at least 10 biopsy cores taken; (4) � 2biopsy cores positive for cancer; (5) biopsy GS � 6; (6) PSAdensity < 0.2 ng/mL; and (7) availability of bioptic and radicalprostatectomy archival specimens.
HistopathologyTwo experienced genitourinary pathologists (MF and FG) blind
to each other and to the original histological reports reviewed his-tological slides for all of the enrolled patients. Discordance betweenthe 2 pathologists were resolved by applying the diagnosis of themost experienced of the 2 raters. GS was redetermined in biopsycores and radical prostatectomy specimens according to the 2005
nical Genitourinary Cancer Month 2014
International Society of Urological Pathology (ISUP) criteria.10 TheGS and the percentage of tumor involvement were calculated foreach biopsy core. GS, tumor stage, and the status of surgical marginswere also reassessed in the surgical specimens. Pathological andclinical staging were determined according to the 7th AmericanJoint Committee on Cancer regulations.16
Clinical EvaluationsAll patients underwent the clinical follow-up planned in our
institution for all patients after radical prostatectomy, which includedphysical and serum PSA examination every 3 months for the first2 years and every 6 months thereafter. Indolent prostate cancer inradical prostatectomy specimens was defined as: organ-confinedcancer, GS � 6 according to the ISUP 2005 criteria, and tumorof any volume according to the criteria proposed by Lee et al.14
The main end points of the study were to: (1) quantify thevariation of GS (in biopsy and surgical specimens) before and afterthe revision; (2) assess the accuracy of the revised GS in biopsy topredict indolent cancer in the radical prostatectomy specimens; (3)quantify the actual percentage of biopsies with GS � 6 after revisionand assess the pathologic and oncologic outcomes of these patients(group 1) versus patients with revised biopsy GS � 7 (group 2).
The study was performed in line with the Helsinki Declaration17
and the national regulations. The local institutional review board(IRB) approved the study (approval code STUD-OF by the S.Orsola-Malpighi Hospital IRB September 11, 2012).
Statistical AnalysisThe Student test, Mann-Whitney U test for continuous variables,
and the Pearson c2 test for categorical variables were used asappropriate.
ResultsTable 1 shows the clinical characteristics of the whole population
of 134 patients before the histological revision. The mean age, PSAlevel, and number of cores taken were 65.9 � 5.3 years, 5.9 � 1.8ng/mL, and 13.2 � 3.1, respectively. Eighty-five (63.4%) patientshad only 1 biopsy core positive for cancer and the average in-volvement of the main core was 21.5% (range, 10-30). The initialkappa of concordance between the 2 reviewing pathologists wask ¼ 0.856 for the biopsies and k ¼ 0.844 for the prostatectomies.Seventy-five (56.0%) patients were in clinical stage T1c and 49(36.6%) in stage T2a. The mean follow-up was 40.8 � 21.2months (range, 10-93 months).
Histological Revision Upgraded the GS of Approximately1 Point and Significantly Reduced the Number of CasesWith GS � 6
Table 2 shows the discrepancy between clinical and pathologicalcharacteristics of the 134 patients, before and after the histologicalrevision. The median GS of biopsy cores and surgical specimensincreased by 1 point, from 6 to 7 (P< .001). The number of patientswith GS � 6 after histological revision decreased from 114 (85.1%)to 44 (32.8%) in the biopsy samples and from 70 (52.2%) to25 (18.7%) in the radical prostatectomy specimens (all P < .001).In turn, the percentage of patients with GS � 7 significantlyincreased after histological revision. In particular, in the radical
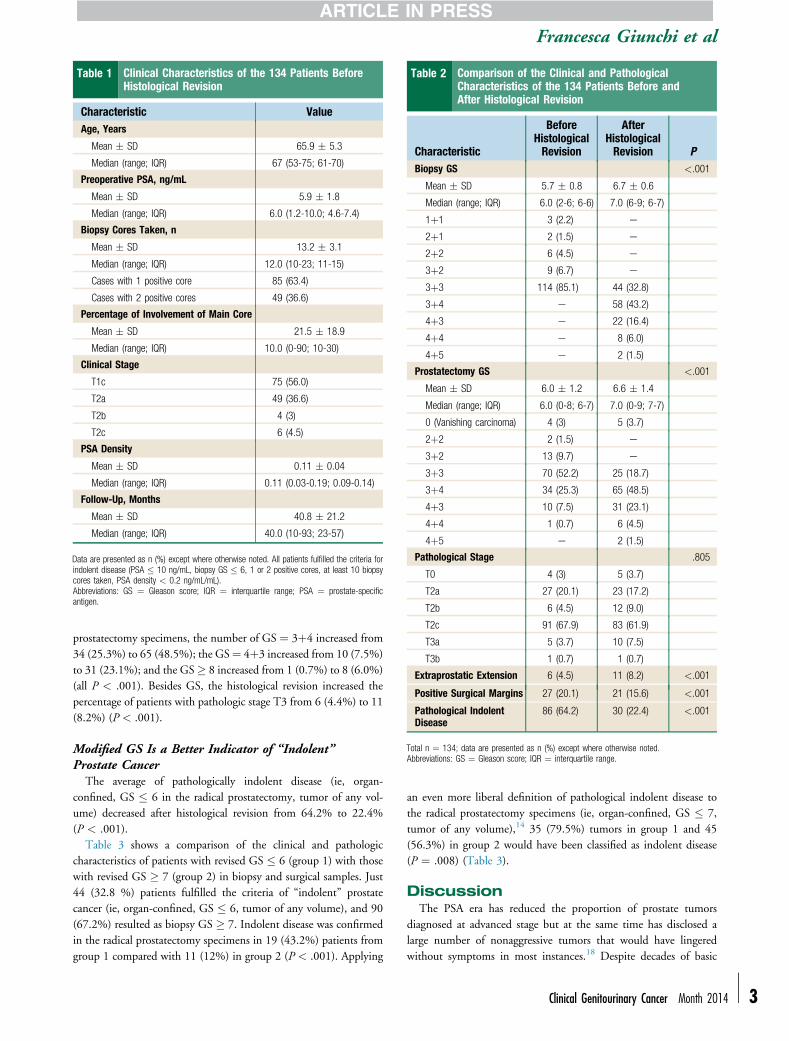
Table 2 Comparison of the Clinical and PathologicalCharacteristics of the 134 Patients Before andAfter Histological Revision
Characteristic
BeforeHistologicalRevision
AfterHistologicalRevision P
Biopsy GS <.001
Mean � SD 5.7 � 0.8 6.7 � 0.6
Median (range; IQR) 6.0 (2-6; 6-6) 7.0 (6-9; 6-7)
1þ1 3 (2.2) e
2þ1 2 (1.5) e
2þ2 6 (4.5) e
3þ2 9 (6.7) e
3þ3 114 (85.1) 44 (32.8)
3þ4 e 58 (43.2)
4þ3 e 22 (16.4)
4þ4 e 8 (6.0)
4þ5 e 2 (1.5)
Prostatectomy GS <.001
Mean � SD 6.0 � 1.2 6.6 � 1.4
Median (range; IQR) 6.0 (0-8; 6-7) 7.0 (0-9; 7-7)
0 (Vanishing carcinoma) 4 (3) 5 (3.7)
2þ2 2 (1.5) e
3þ2 13 (9.7) e
3þ3 70 (52.2) 25 (18.7)
3þ4 34 (25.3) 65 (48.5)
4þ3 10 (7.5) 31 (23.1)
4þ4 1 (0.7) 6 (4.5)
4þ5 e 2 (1.5)
Pathological Stage .805
T0 4 (3) 5 (3.7)
T2a 27 (20.1) 23 (17.2)
T2b 6 (4.5) 12 (9.0)
T2c 91 (67.9) 83 (61.9)
T3a 5 (3.7) 10 (7.5)
T3b 1 (0.7) 1 (0.7)
Extraprostatic Extension 6 (4.5) 11 (8.2) <.001
Positive Surgical Margins 27 (20.1) 21 (15.6) <.001
Pathological IndolentDisease
86 (64.2) 30 (22.4) <.001
Total n ¼ 134; data are presented as n (%) except where otherwise noted.Abbreviations: GS ¼ Gleason score; IQR ¼ interquartile range.
Table 1 Clinical Characteristics of the 134 Patients BeforeHistological Revision
Characteristic ValueAge, Years
Mean � SD 65.9 � 5.3
Median (range; IQR) 67 (53-75; 61-70)
Preoperative PSA, ng/mL
Mean � SD 5.9 � 1.8
Median (range; IQR) 6.0 (1.2-10.0; 4.6-7.4)
Biopsy Cores Taken, n
Mean � SD 13.2 � 3.1
Median (range; IQR) 12.0 (10-23; 11-15)
Cases with 1 positive core 85 (63.4)
Cases with 2 positive cores 49 (36.6)
Percentage of Involvement of Main Core
Mean � SD 21.5 � 18.9
Median (range; IQR) 10.0 (0-90; 10-30)
Clinical Stage
T1c 75 (56.0)
T2a 49 (36.6)
T2b 4 (3)
T2c 6 (4.5)
PSA Density
Mean � SD 0.11 � 0.04
Median (range; IQR) 0.11 (0.03-0.19; 0.09-0.14)
Follow-Up, Months
Mean � SD 40.8 � 21.2
Median (range; IQR) 40.0 (10-93; 23-57)
Data are presented as n (%) except where otherwise noted. All patients fulfilled the criteria forindolent disease (PSA � 10 ng/mL, biopsy GS � 6, 1 or 2 positive cores, at least 10 biopsycores taken, PSA density < 0.2 ng/mL/mL).Abbreviations: GS ¼ Gleason score; IQR ¼ interquartile range; PSA ¼ prostate-specificantigen.
Francesca Giunchi et al
prostatectomy specimens, the number of GS ¼ 3þ4 increased from34 (25.3%) to 65 (48.5%); the GS¼ 4þ3 increased from 10 (7.5%)to 31 (23.1%); and the GS� 8 increased from 1 (0.7%) to 8 (6.0%)(all P < .001). Besides GS, the histological revision increased thepercentage of patients with pathologic stage T3 from 6 (4.4%) to 11(8.2%) (P < .001).
Modified GS Is a Better Indicator of “Indolent”Prostate Cancer
The average of pathologically indolent disease (ie, organ-confined, GS � 6 in the radical prostatectomy, tumor of any vol-ume) decreased after histological revision from 64.2% to 22.4%(P < .001).
Table 3 shows a comparison of the clinical and pathologiccharacteristics of patients with revised GS � 6 (group 1) with thosewith revised GS � 7 (group 2) in biopsy and surgical samples. Just44 (32.8 %) patients fulfilled the criteria of “indolent” prostatecancer (ie, organ-confined, GS � 6, tumor of any volume), and 90(67.2%) resulted as biopsy GS � 7. Indolent disease was confirmedin the radical prostatectomy specimens in 19 (43.2%) patients fromgroup 1 compared with 11 (12%) in group 2 (P < .001). Applying
an even more liberal definition of pathological indolent disease tothe radical prostatectomy specimens (ie, organ-confined, GS � 7,tumor of any volume),14 35 (79.5%) tumors in group 1 and 45(56.3%) in group 2 would have been classified as indolent disease(P ¼ .008) (Table 3).
DiscussionThe PSA era has reduced the proportion of prostate tumors
diagnosed at advanced stage but at the same time has disclosed alarge number of nonaggressive tumors that would have lingeredwithout symptoms in most instances.18 Despite decades of basic
Clinical Genitourinary Cancer Month 2014 - 3

Table 3 Clinical and Pathologic Characteristics of PatientsWith Revised Biopsy GS £ 6 Compared With ThoseWith Revised Biopsy GS ‡ 7
Characteristic
Group 1: RevisedBiopsy GS £ 6(n [ 44; 32.8%)
Group 2: RevisedBiopsy GS ‡ 7(n [ 90; 67.2%) P
Prostatectomy GS .001
Mean � SD 6.3 � 1.5 6.77 � 1.3
Median (range;IQR)
7.0 (0-8; 6-7) 7.0 (0-9; 7-7)
0 (Vanishingcarcinoma)
2 (4.5) 3 (3.3)
3þ3 17 (38.6) 8 (8.9)
3þ4 18 (40.9) 47 (52.2)
4þ3 5 (11.3) 26 (28.8)
4þ4 2 (4.5) 4 (4.4)
4þ5 e 2 (2.2)
Indolent Diseaseat RadicalProstatectomya
19 (43.2) 11 (12.2) <.001
More LiberalDefinitions ofIndolent Diseasein ProstatectomySpecimensb
35 (79.5) 45 (56.3) .008
Data are presented as n (%) except where otherwise noted.Abbreviations: GS ¼ Gleason score; IQR ¼ interquartile range.aOrgan-confined, GS � 6; tumor of any volume.bOrgan-confined, GS � 7; tumor of any volume.
Revised GS and Indolent Prostate Cancer
4 - Cli
research on biomarkers, the histological Gleason grade still remainsthe most reliable prognosticator of prostate cancer and the revisionsrecently made to the Gleason system have further refined its dis-criminatory capability between aggressive and indolent tumors.11 Infact, the application of the modified Gleason grading according tothe 2005 criteria has been shown to better predict biochemicaltumor recurrence compared with the original Gleason system.19,20
To our knowledge, no one has investigated the power of themodified Gleason system to predict indolent tumor behavior in aselected series of very low risk prostate cancer. In this retrospectivestudy, we demonstrated that the histological revision of the GSaccording to the 2005 criteria in the biopsy specimens improved theaccuracy in predicting indolent disease at time of radical prosta-tectomy. As expected, the total GS after revision increased by at least1 point and the number of GS � 6 tumors at biopsy dropped from85% to 32%. The better discriminatory prognostic power of the2005 revised GS mostly relies in its capability of restricting the fieldof GS � 6 cases only to the very low aggressive tumors.12 In turn,the number of localized prostate cancers with GS � 6 in our radicalprostatectomy series also decreased after the histological revision.
The criteria proposed by the ISUP consensus in 2005 recentlyunderwent another revision that further restricted the diagnosticcriteria of the GS � 6.11 The application of these further revisedcriteria in a single institution correlated with a very low aggressivebehavior of the GS � 6 tumors diagnosed in this new way, leadingto the provoking conclusion that GS � 6 prostate cancer should notbe considered cancer.21 If these new criteria will be fully acknowl-edged and the predictive power confirmed in different cohorts it is
nical Genitourinary Cancer Month 2014
likely that active surveillance will become the therapy of choice forGS � 6 prostate cancer in the future. The safe implementation ofactive surveillance in these patients is also supported by the recentevidence that GS is not likely to progress over time.22 If the patientsin our series had been diagnosed using the revised GS criteria, atleast a third of them could have been assigned to active surveillancewith reasonable safety of this intervention.
The histological revision by dedicated genitourinary pathologistsof our data also improved the accuracy in the assessment of positivesurgical margins (decreased after revision) and extraprostatic tumorextension (increased after revision) (P < .001 for both). A nonsig-nificant trend toward upstaging was also observed after revision.Overall, these data confirm that the histological diagnosis of prostatecancer by dedicated genitourinary pathologists is relevant for diag-nosing not only biopsy cores but also the surgical specimens. Wecannot evaluate here the prognostic effects of the improved diag-nosis on radical prostatectomy and we realize that the follow-up inour series is too short to draw conclusions on survival, includingbiochemical relapse-free survival. However, survival analyses wereout of the scope of the present report and the decision to enrollpatients with short follow-up was justified by the need to homog-enize the pathological samples. In fact, the radical prostatectomyspecimens were not entirely submitted to histological examinationbefore 2004 in our institution. This would have led to certainunderestimation of organ-confined prostate cancer.
ConclusionOur study indicates that biopsy GS � 6 diagnosed using the
2005 revised criteria by experienced pathologists is a reliable indi-cator of indolent prostate cancer.
Clinical Practice Points
� In the era of PSA screening, there is a frequent risk of prostatecancer (PCa) overdiagnosis and overtreatment. Most Pca bear anindolent behavior that does not require an aggressive treatmentlike radical prostatectomy (RP). Several protocols of active sur-veillance have been recently implemented worldwide to avoid ordelay RP in patients with low risk PCa.� We retrospectively reviewed biopsy and surgical pathologyspecimens of all the 1344 PCa patients who underwent RP in thepast 7 years in our Institution. We revised the Gleason score(GS) of all specimens according to the ISUP 2005 recommen-dation and we selected only the 134 patients with PCa thatwould have been considered indolent at the time of biopsy butinvariably underwent RP. Histology and GS in RP and biopsyspecimens was compared to assess the actual power of the biopsyand the GS to predict indolent PCa.
� Our data indicate that biopsy diagnosis of indolent PCa is achiev-able only if experienced pathologists have applied the ISUP 2005GS criteria. Based on this observation we deem that active sur-veillance might be considered the definitive treatment for GS � 6PCa patients with life expectancy < 10 years and a candidatetherapeutic option for younger strongly motivated subjects.
DisclosureThe authors have stated that they have no conflicts of interest.

Francesca Giunchi et al
References1. Epstein JI, Chan DW, Sokoll LJ, et al. Nonpalpable stage T1c prostate cancer:
prediction of insignificance disease using free/total prostate-specific antigen levelsand needle biopsy findings. J Urol 1998; 160:2407-11.
2. Epstein JI, Walsh PC, Carmicheal M, et al. Pathologic and clinical findingsto predict tumor extent of nonpalpable prostate cancer. JAMA 1994; 271:368-74.
3. Stamey TA, Freiha FS, McNeal JE, et al. Localized prostate cancer. Relationship oftumor volume to clinical significance for treatment of prostate cancer. Cancer1993; 71:933-8.
4. Schroder FH, Hugosson J, Roobol MJ, et al. Screening and prostate cancermortality in randomized European study. N Engl J Med 2009; 360:1320-8.
5. Schröder FH. Screening for prostate cancer: an update on recent findings of theEuropean Randomized Study of Screening for Prostate Cancer (ERSPC). UrolOncol 2008; 26:533-41.
6. Brunocilla E, Pultrone C, Pernetti R, et al. Preservation of the smooth muscularinternal (vesical) sphincter and of the proximal urethra during retropubic radicalprostatectomy: description of the technique. Int J Urol 2012; 19:783-5.
7. Iremashvili V, Peleaz L, Manoharan M, et al. Pathologic prostate cancer charac-teristic in patients eligible for active surveillance: a head-to-head comparison ofcontemporary protocols. Eur Urol 2012; 62:462-8.
8. Tosoian JJ, Trock BJ, Landis P, et al. Active surveillance program for prostatecancer: an update of the Johns Hopkins Experience. J Clin Oncol 2011; 29:1-6.
9. Van der Bergh RC, Roemeling S, Roobol MJ, et al. Prospective validation ofactive surveillance in prostate cancer: the PRIAS study. Eur Urol 2007; 52:1560-3.
10. Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL; ISUP Grading Committee.The 2005 International Society of Urological Pathology (ISUP) Consensus Con-ference on Gleason grading of prostatic carcinoma. Am J Surg Pathol 2005; 29:1228-42.
11. Brimo F, Montironi R, Egevad L, et al. Contemporary grading for prostate cancer:implications for patient care. Eur Urol 2013; 63:892-901.
12. Zareba P, Zhang J, Yilmaz A, Trpkov K. The impact of the 2005 InternationalSociety of Urological Pathology (ISUP) consensus on Gleason grading incontemporary practice. Histopathology 2009; 55:384-91.
13. Egevad L, Ahmad AS, Algaba F, et al. Standardization of Gleason grading among337 European pathologists. Histopathology 2013; 62:247-56.
14. Lee MC, Dong F, Stephenson AJ. The Epstein criteria predict for organ-confinedbut not insignificant disease and a high likelihood of cure at radical prostatectomy.Eur Urol 2010; 58:90-5.
15. Van den Bergh RC, Vasarainen H, van der Poel HG, et al. Short-term outcomes ofthe prospective multicentre ‘Prostate Cancer Research International: Active Sur-veillance’ study. BJU Int 2009; 105:956-62.
16. Edge S, Byrd DR, Compton CC, Fritz AG, Green FL, Trotti A. American JointCommittee on Cancer. Cancer staging manual. 7th Edition. Newyork NY,Springer, 2010.
17. World Medical Association. Declaration of Helsinki. Ethical Principles for MedicalResearch Involving Human Subjects. Bull World Health Organ 2001; 79:373-4.
18. Center MM, Jemal A, Lortet-Tieulent J, et al. International variation in prostatecancer incidence and mortality rates. Eur Urol 2012; 61:1079-92.
19. Pierorazio PM,Walsh PC, PartinAW,Epstein JI. PrognosticGleason grade grouping:data based on the modified Gleason scoring system. BJU Int 2013; 111:753-60.
20. Billis A, Quintal MM, Meirelles L, et al. The value of the 2005 InternationalSociety of Urological Pathology (ISUP) modified Gleason grading system as apredictor of biochemical recurrence after radical prostatectomy. Int Urol Nephrol,Published online Oct 6, 2013; http://dx.doi.org/10.1007/s11255-013-0579-8.
21. Carter HB, Partin AW, Walsh PC, et al. Gleason score adenocarcinoma: should itbe labeled cancer? J Clin Oncol 2012; 30:4294-6.
22. Penney KL, Stampfer MJ, Jahn JL, et al. Gleason grade progression is uncommon.Cancer Res 2013; 73:5163-8.
Clinical Genitourinary Cancer Month 2014 - 5