review of claims status for the nhif phase one ad kiwara gradeline minja manfred störmer ulrika...
TRANSCRIPT
Review of claims status for the NHIF
Phase One
AD Kiwara Gradeline Minja
Manfred StörmerUlrika Enemark

Background
• Contributions and reimbursements 2004/5– Contributions collected 24.0 bn TSh– Claims lodged 4.9 bn TSh– Reimbursements paid 4.2 bn TSh
• NHIF accredited facilities (sept 2005)– 3,358 government facilities– 594 private facilities (mostly faith-based)– 68% of accredited facilites are active (june 05)

Overall aim
• Aim:
Strengthening the system of claims and reimbursement for the benefit of district health services
• Two phases– Situation analysis– Pilot implementation in selected districts

Objectives, Phase One
To analyse
• the relative importance of NHIF funding
• reasons for not registering with NHIF
• reasons for the low level of claims submitted
• flow of reimbursement to providers and the use of reimbursements

Methodology
• Document review
• Semi-structured interviews
• Field visits to Tanga and Mwanza Region– 7 districts– 24 health facilities at varying levels,
ownership and location
• Limitations

Findings

Importance of NHIF funding 1
• National level: – NHIF contributions: 4.8% of total on-budget
expenditures (2004/5)– Table 1. NHIF reimbursements compared to total
health sector expenditures 2001-04 Actual Budget
2001/02 2002/03 2003/04 2004/05
NHIF claims paid (mill TSh) 247.4 1345.9 3808.4 4204.6
NHIF reimbursement to total recurrent health exp 0.22% 0.98% 2.34% 1.82%
NHIF reimbursement to total domestic health exp. 0.26% 1.22% 2.54% 2.27%
Note: Total recurrent excluding AGO spending on NHIF.

Importance of NHIF funding 2
• District level
Table 1. NHIF reimbursements to districts compared to total health
care budget for selected districts District Average Annual
health budget Av. Annual NHIF reimbursements
NHIF to total health budget
Mill TSh Mill TSh %
Magu 1,608 24 1.5
Handeni 1,459 8 0.5
Sengerema 916 15 1.6

Importance of NHIF funding 3
• Facility level– The low end: At dispensaries NHIF
contribution is negligible: 0.5-3% of total cost sharing
– The high end: At faith-based facilities 20-50% of cost sharing is recovered through NHIF

R ei mbur s ements by l evel of c ar e. M wanz a, one quar ter 2005
0
10
20
30
40
50
60
70
80
90
100
Regional and referral hospitals Other hospitals Health Centres Dispensaries Pharmacies
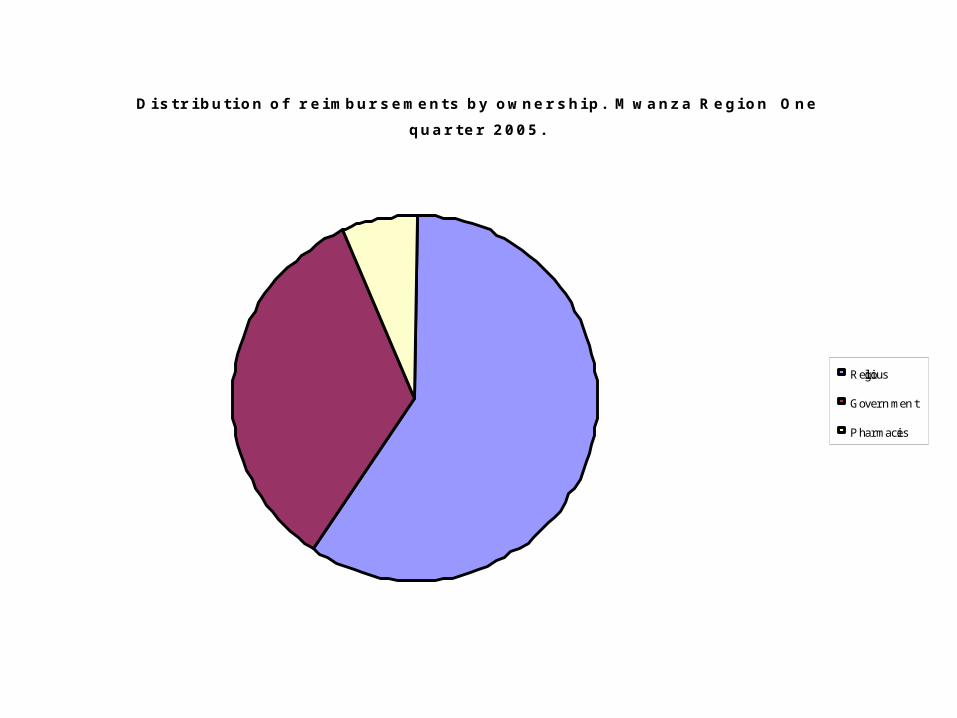
Di s tr i buti on of r ei mbur s ements by owner s hi p. M wanz a R egi on One
quar ter 2005.
Religious
Government
Pharmacies

Accreditation 1
Factors affecting # of privateaccredited facilities
• Accreditation process perceived as smooth• Level of rates
– FBOs, Pharmacies: Generally acceptable, but is needs revision more often
– PFP: On the low side• Low level of awareness in PFP sector• Some skepticism towards government operations
Accreditation 2
Factors affecting access to quality services
• Accreditation guideline for ideal rather than minimum criteria not useful– Few facilities meet criteria– Accreditation rarely denied or revoked
• Government facilites are given blanket accreditation• Pharmacies are accredited in only few places

Registration 1
• Process clearly defined by Act no. 8 of 1999 which established NHIF
• Eligibility well-defined
• Membership volume (sept 05)– Members 266,131 Beneficiaries 1,224,20
• Identity cards

Registration 2
Current issues in relation to registration
• Problems with cards
• Membership compliance problems
Claiming - Processing of Claim Forms
• Claim forms are generally filled in • Staff aware that funds will be earmarked
for their health facility• Some facilities do not have the summary
page of the coding list, price list• Lack of qualified staff creates problems
also for processing NHIF claims• Retraining of staff needed• Claim forms are appropriate
Claiming - Submission of Claim Forms, Feedback and Monitoring
• Claims are filled in but not always submitted (both at health facility and DMO level)
• NHIF provides feedback for rejected claims; for some dispensaries and h/centres difficult to understand
• No correction of mistakes allowed• Lacking monitoring instruments at health facility
and DMO level on claims and reimbursements• Districts with NHIF Co-ordinator had better quality
control and monitoring

Reimbursement and use of funds
• Delays in payment not caused by late claiming occur, especially in Tanga; Mwanza doing well; but improving
• Some health facilities, esp. at lower level, are not aware of how to access the NHIF reimbursement funds

Reimbursement and use of funds
• Hospitals have to deposit their funds at the sub-treasury at regional level => complicated and time consuming procedures
• Lower level health facilities use various options for depositing funds:• Account #6 at district level • HSF account in the sub-treasury at regional level • A common cost sharing account at district level • A cost sharing account at facility level
Benefit package
• Reimbursable drugs do not correspond to content of KIT
• Limitation of inpatient days can cause problems
• Awareness of package limitation among NHIF beneficiaries
• Bypassing of referral system

Recommendations