review article areviewoflutingagents
TRANSCRIPT

Hindawi Publishing CorporationInternational Journal of DentistryVolume 2012, Article ID 752861, 7 pagesdoi:10.1155/2012/752861
Review Article
A Review of Luting Agents
Cornelis H. Pameijer
Department of Reconstructive Sciences, School of Dental Medicine, University of Connecticut, Farmington,CT 06030, USA
Correspondence should be addressed to Cornelis H. Pameijer, [email protected]
Received 4 November 2011; Accepted 23 November 2011
Academic Editor: J. Anthony Von Fraunhofer
Copyright © 2012 Cornelis H. Pameijer. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Due to the availability of a large number of luting agents (dental cements) proper selection can be a daunting task and is usuallybased on a practitioner’s reliance on experience and preference and less on in depth knowledge of materials that are used for therestoration and luting agent properties. This review aims at presenting an overview of current cements and discusses physicalproperties, biocompatibility and other properties that make a particular cement the preferred choice depending on the clinicalindication. Tables are provided that outline the different properties of the generic classification of cements. It should be noted thatno recommendations are made to use a particular commercial cement for a hypothetical clinical situation. The choice is solelythe responsibility of the practitioner. The appendix is intended as a guide for the practitioner towards a recommended choiceunder commonly encountered clinical scenarios. Again, no commercial brands are recommended although the author recognizesthat some have better properties than others. Please note that this flowchart strictly presents the author’s opinion and is based onresearch, clinical experience and the literature.
1. Introduction
Proper selection of a luting agent is a last important decisionin a series of steps that require meticulous execution and willdetermine the long-term success of fixed restorations. Onehundred years ago this decision was easy with the availabilityof essentially only one luting agent, zinc phosphate cement.Currently, a plethora of luting agents is available. Now thechoice of the optimal luting agent can be confusing, evenfor the most experienced clinician. Restorations of metal,porcelain fused to metal, low-and high-strength ceramics,full or partial coverage, require a prudent approach and theproper cement selection should be based on knowledge ofphysical properties, biological properties and other attributesof both restorative materials and luting agents. This paperaims at providing an overview of currently available lut-ing agents (cements) and discusses their advantages anddisadvantages. Emphasis has been placed on composition,biocompatibility, physical properties, clinical indications,and clinical performance. A wide range of formulations has
been developed over the last 40 years, but here emphasis hasbeen placed on the contemporary most frequently used ones,whether used for luting or bonding.
2. Classification of Cements
Cements can be classified as follows:
(1) liners and bases;
(2) temporary (provisional) cements;
(3) permanent cements.
2.1. Liners and Bases. Preference seems to be given bythe dental profession to visible light curing materials, inparticular resin-modified glass ionomer (RMGI) cements(sometimes also referred to as resin reinforced glass ionomer(RRGI), when there is a need for a base or a liner. The reasonis based on simplicity and on the fast setting characteristics

2 International Journal of Dentistry
of light curing materials as well as the possibility of subse-quently etching them in order to establish strong adhesivebonds with dentin bonding agents. Furthermore, they adherewell to unetched hard tissue and exhibit sustained fluoriderelease.
2.2. Provisional Cements. Provisional cements can be eu-genol, noneugenol, resin, or polycarboxylate based. Cau-tion has to be exercised when using eugenol-containingcements as the eugenol can contaminate the preparation.This can inhibit the polymerization of certain resin com-posites subsequently used as permanent restorative fillingmaterial [1].
Eugenol-containing temporary cements that are usedprior to indirect bonding restorations reduce the bondstrength of both total- and self-etching adhesive systemsto dentin [2]. It is therefore advisable to use noneugenoltemporary cements. In another report, however, no differ-ence in bond strengths was observed when using eugenol-free and eugenol-containing provisional cements followed byself-adhesive resin cements [3].
Most subsequent publications report on a reduced bondstrength of luting agents when eugenol-containing tempo-rary cements are used [4, 5]. Nevertheless, the application ofany temporary cement, whether eugenol-containing or not,contaminates the dentin, which will interfere with adhesion.
2.3. Permanent Cements. Figure 1 shows the chronologicaldevelopment of luting agents from the late 1800 hundredsto today. It is significant in that for almost 100 years onlyzinc phosphate cement was available, which is still beingconsidered the “gold” standard.
With the introduction of cast restorations in the late1880s, the need for a luting agent or dental cement forcrowns and small bridges was readily recognized by thedental profession. The Dental Cosmos reported (in the late1800s), a technique for the fabrication of a 4-unit pin ledgebridge (Finley), which required cement for fixation. Whilegold shell crowns were introduced around 1883 it was notuntil 1907 that Taggert introduced cast crowns by meansof the lost wax technique. Around 1879, zinc phosphatecement was introduced and although the formulation hasbeen refined during more than a century of use, it is a lutingagent that has consistently been successful in clinical practiceand even today is still considered the “gold” standard.With the exception of silicate cement in the 1940s fewnew cements were introduced until around 1970. The wordsilicate cement, however, is a misnomer as it was not a lutingagent. It was used for anterior Cl III and Cl V estheticrestorations.
3. Zinc Phosphate Cement
The cement comes as a powder and liquid and is classifiedas an acid-base reaction cement. The basic constituent of thepowder is zinc oxide. Magnesium oxide is used as a modifier(±10%) while other oxides such as bismuth and silica may bepresent.
The liquid is essentially composed of phosphoric acid,water, aluminum phosphate, and sometimes zinc phosphate.The water content is approximately 33±5% and is an impor-tant factor as it controls the rate and type of powder/liquidreaction [6].
When the powder reacts with the liquid a considerableamount of heat is generated (exothermic reaction) andwhen the mixing is complete the cement reaches a pH of3.5. Since the cement is placed on and in prepared teethwhen it is in a “wet consistency” and not all the liquid hasreacted with the powder, unreacted phosphoric acid liquidwith a low pH ±1.5 comes in contact with the preparationand causes an immediate (within 5 s) dissolution of thesmear layer and smear plugs. Since cementation can causea considerable amount of hydraulic pressure, the unreactedacid is pressed in the dentinal tubules and, depending onthe remaining dentin thickness (RDT), the distance from thefloor of the preparation to the pulp, can cause greater orless irritation to the pulp. Therefore, the pulp has to copewith not only heat but low acidity as well. The greater theRDT, the more beneficial the buffering action of the fluidin the dentinal tubules is and the less the effect of the acid.Furthermore, a greater RDT also diminishes the thermaleffect. When fully reacted, the set cement reaches a pH = 6.7after 24 hours. Postcementation hypersensitivity is indeed afrequently occurring clinical problem, which either resolvesover time or may result in the need for endodontic treatment.If it resolves, it is through the protective action of secretionof secondary dentin by the odontoblasts, which increases theRDT. This however, does not start in humans until 3 weeksafter the insult has taken place and deposition of secondarydentin occurs in microns per day [7]. If the irritation cannotbe handled by the body, the pulp becomes necrotic, whichthen requires root canal treatment. Therefore, although theset luting material may be biocompatible, postcementationdiscomfort is a known unfavorable side effect when usingthis cement. Attempts at blocking access of the unreactedphosphoric acid to the dentinal tubules have been made inthe form of a varnish (Copalite). Unfortunately, Copalite canreduce the retention of the restoration by as much as 50%[8].
4. Zinc Polycarboxylate Cement
Polycarboxylate cement is also an acid-base reaction cement.The powder is composed of mainly zinc oxide, magnesiumoxide, bismuth, and aluminum oxide. It may also containstannous fluoride, which increases strength. The liquid iscomposed of an aqueous solution of polyacrylic acid or acopolymer of acrylic acid and other unsaturated carboxylicacids. Fluoride release by the cement is a small fraction (15–20%) of that released from materials such as silicophosphateand glass ionomer cements.
When mixed at the recommended P/L ratio the finalmix appears more viscous than zinc phosphate cement.However, this can be offset by vibratory action during seatingyielding a film thickness of ±25µm. At no time should theamount of liquid be increased, as it will adversely affect

International Journal of Dentistry 3
18801940 1972
19751986
1995
1976
2004
2009
Polymer based
Acid-base reaction cements
Hybrid acid-base reaction cement
• Zinc phosphate cement used for ±120 years• ±1940 silicate cement• Polycarboxylate cement (1972)• Composite resin cements (1975)• Glass ionomer cement (1976)• Resincement (Biomer-1986)• Resin modified glass ionomer cement (1995)• Self etching (adhesive) resin cements (±2004)• Ceramir C and B (2009)
Figure 1: An overview of the chronological development of luting agents starting around 1880 until today. The last 30–40 years havewitnessed the development of new cement systems and a large number of cements have become available. It was not until 2009 that aparadigm shift took place and a hybrid acid-base reaction cement was introduced, which offered physical and other properties that not onlydiffered from the polymer-based luting agents but also matched them. +1880—zinc phosphate cement, +1940—silicate cement∗, 1972—polycarboxylate cement, +1975—composite resin cements, 1976—glass ionomer cement, 1986—resin cement, +1995—resin-modified glassionomer cement, +2004—self-etching (adhesive) resin cements, 2009—hybrid-acid-base reaction cement, (∗the designation silicate cementis a misnomer as it was a restorative material for Cl III and Cl V restorations).
the compressive strength, which at 55 MPa is already lowerthan that of zinc phosphate cement. Biological propertiesof polycarboxylate cement are quite favorable and thecement causes little or no irritation to the pulp, even at aremaining dentin thickness of 0.2 mm (Unpublished data). Itis believed that the long molecular chains of the polyacrylicacid prevent penetration into the dentinal tubules. It is ofinterest to note that both zinc phosphate and polycarboxylatecements have a pH of about 3.5 immediately after mixing.Currently polycarboxylate cements are mostly used for long-term temporary cementation.
Polycarboxylate and glass ionomer cements exhibit aproperty that is called chelation, which is the ability to bondto the Ca ions.
5. Glass Ionomer Cement
Glass ionomer cements (GICs) were invented in the late1960s in the laboratory of the Government Chemist in GreatBritain and were first reported on by Wilson and Kent in 1971[9]). GICs set by means of chelation as a result of an acid-basereaction. They strongly adhere to enamel and to some extentto dentin and release fluoride. Initially used as a restorative
material, GI further evolved into a luting agent, which is nowthe predominant application of this class of material.
The powder consists of aluminosilicates with high flu-oride content. The material is formed by the fusion ofquartz, alumina, cryolite, fluortite, aluminum trifluoride,and aluminum phosphate at temperatures of 1100–1300◦C.This glass frit is cooled to a dull glow and quenched in water.It is subsequently ground into 45 µm particles.
The liquid is composed of polyacrylic acid and tartaricacid, the latter to accelerate the setting reaction. The re-action of the powder with the liquid causes decomposition,migration, gelation, postsetting hardening and further slowmaturation. The polyacrylic acid reacts with the outer surfaceof the particles resulting in release of calcium, aluminum,and fluoride ions. When a sufficient amount of metal ionshas been released, gelation occurs, and hardening continuesfor about 24 hours [9].
GIC display a relatively low curing shrinkage; within thefirst 10 minutes 40–50% of shrinkage has occurred.
However, with the use of GIC as a luting agent, frequentpostcementation sensitivity has been reported. The thenaccepted ANSI/ADA Specification 41, Recommended Stan-dard Practices for Biological Evaluation of Dental Materials

4 International Journal of Dentistry
stipulated that luting agents should be tested for pulpreaction in primates by passively inserting a heavier thanluting consistency mix in Class V restorations in primates.Indeed the results of these tests demonstrated that the cementwas biocompatible and nonirritating [10]. In a subsequentstudy, also in primates, crowns were cemented adhering to aclinically more relevant cementation protocol, with a cementmix that had a normal luting consistency [11].
In this study hydraulic pressure generated during cemen-tation and the resulting penetration of unreacted acid intothe dentinal tubules was responsible for the true postce-mentation reaction of the pulp under clinical conditions. Itwas clearly demonstrated that, depending on the RDT, GICcaused pulpal inflammation which, rather than subsidingover time, increased in severity. It was this study that resultedin a change in protocol in the ANSI/ADA Specification41 (2005) [12], which now calls for a pressure insertiontechnique. Rather than using a laborious indirect techniqueand cementing all metal cast crowns as was done in theaforementioned study, Cl V composite resin inlays are fab-ricated and cemented with the cement to be tested. With theuse of this technique, hydraulic pressure is generated that issimilar to complete crown cementation. In addition, the Cl Vinlays are usually closer to the pulp than crown preparationsand therefore result in a more reliable biocompatibilityreaction.
6. Resin Cements
As an alternative to acid-base reaction cements, resin ce-ments were introduced in the mid-1980s, these materialshave a setting reaction based on polymerization. Resincements are polymers to which a filler has been added aswell as fluoride. Cement film thickness is not favorable forsome materials, for example, C & B Metabond (Parkell Inc.)with a film thickness > 100 µm, while others have a reportedfilm thickness of 9 µm, for example, Permalute (UltradentProducts Inc). One of the first resin cements was marketedby Dentsply/Caulk under the name Biomer, around 1987.In two clinical studies by Pameijer (unpublished data), thecement performed well over a one-year period of evaluation.However, over time polymer degradation occurred due tohydrolysis, while a lack of bonding to enamel and dentinmade the cement unsuitable as a stand-alone luting agent,leading to leakage and failure of the restoration. Additionally,incomplete polymerization can lead to irritation of the pulpby unreacted monomers.
In combination with a dentin bonding agent, however,many resin cements have superior properties and are fre-quently used for the cementation (bonding) of porcelainlaminate veneers. The concept of a “monobloc” describedin endodontics [13] applies here as well. A combinationbonding agent that bonds to tooth structure and a resincement that adheres to the bonding agent and to silanetreated porcelain follows the same principles. Nevertheless,there is a reluctance on the part of practitioners to do a“total etch” of complete crown preparations, which is arequired step for many bonding agents. Even the self-etching
dentin bonding agents are not ideal because of concerns forpostoperative sensitivity.
7. Resin-Modified Glass Ionomer(RMGI) Cements
The RMGI or RRGI (resin-reinforced glass ionomer) ce-ments are indicated for the luting of crowns and bridges,as well as inlay and onlay restorations. They are essentiallyhybrid formulations of resin and glass ionomer components.The RMGI cements are relatively easy to handle and aresuitable for routine application with metal-based crown andbridgework. However, their use is limited when adhesivelycementing ceramics with smooth, nonretentive surfaces.Adhesion to tooth structure is not strong with these mate-rials. Additionally, some early formulations have displayedexcess water sorption, causing swelling frequently resultingin ceramic fracture. Commercial examples of the RMGIcements are: RelyX Luting, RelyX Luting Plus (3 M/ESPE),Fuji Plus (GC) and UltraCem RRGI Luting Cement.
In a recent article, the biological effects of resin-modifiedglass-ionomer cements as used in clinical dentistry weredescribed, and the literature reviewed on this topic [14].Information on resin-modified glass ionomers and on 2-hydroxyethyl methacrylate (HEMA), the most damagingsubstance released by these materials, was collected fromover 50 published papers. These were mainly identifiedthrough Scopus. It is known that HEMA is released fromthese materials, which has a variety of damaging biologicalproperties, ranging from pulpal inflammation to allergiccontact dermatitis. These are therefore potential hazardsfrom resin-modified glass ionomers. However, clinical resultswith these materials that have been reported to date aregenerally positive. According to the above authors, RMGIscannot be considered biocompatible to nearly the sameextent as conventional glass-ionomers. Care needs to betaken with regard to their use in dentistry and, in particular,dental personnel may be at risk from adverse effects suchas contact dermatitis and other immunological responses.Interestingly, RMGIs have a better clinical track record thanglass ionomer cements.
In general few complaints have been reported about post-operative cementation hypersensitivity. Yet, RMGIs are inthe category of resin cements and water sorption anddegradation through hydrolysis are negative features thatshould not be ignored or underestimated.
In spite of the numerous research methodologies that areat our disposal conflicting results are frequently reported,either using the same technique and tests on the samematerials, or using different techniques and testing the samematerials. RMGIs as shown above are such an example.While controversial data has been generated, successfulclinical use seems to contradict these findings.
8. Adhesive Resin Cements
The poor adhesive properties of the RMGIs have led tofurther development of resin-based luting agents, which

International Journal of Dentistry 5
have resulted in the introduction of adhesive resin cements.These cements do not require pretreatment and bondingagents to maximize their performance. In order for thesecements to be self-adhesive, new monomers, filler and ini-tiator technology were created. Examples of these materialsare: MaxCem (Kerr), RelyX Unicem (3 M/ESPE), Breeze(Pentron), Embrace Wet Bond (Pulpdent Corporation) toname a few. These cements enjoy great popularity as theyhave universal applications. As pointed out before underresin and RMGI cements, polymer degradation over timeis still an issue. Matrix metalloproteinases (MMPs) arefossilized within mineralized dentin and can be releasedand activated during bonding [15]. These endogenouscollagenolytic enzymes are on the collagen fibers and neededfor bonding and their slow degrading enzymatic action isbeyond the control of even the most meticulous clinician.Reports have appeared that recommend pretreatment of thedentin with 2.0% chlorhexidine gluconate with a pH of6.0, which prevents the action of the endogenous enzymes[16].
9. Hybrid-Acid-Based CaAl/Glass Ionomer
Only one formulation is presently known that is basedon calcium aluminate/glass ionomer. Ceramir C&B (DoxaDental AB, Uppsala, Sweden) is a new dental luting agentintended for permanent cementation of crowns and bridges,gold inlays and onlays, prefabricated metal, and cast postand cores and all-zirconia or all-alumina crowns. The cementis a water-based hybrid composition comprising of calciumaluminate and glass ionomer components that is mixed withdistilled water. The material has been demonstrated to bebioactive [17]. The setting mechanism of Ceramir C&B is acombination of a glass ionomer reaction and an acid-basereaction of the type occurring in hydraulic cements. Theincorporation of the calcium aluminate component providesseveral unique properties compared to conventional GIC’s.There are several features that strongly contribute to thebiocompatibility profile of the material. These include thefact that after setting, the material is slightly acidic, pH∼4. After 1 h, the pH is already neutral and after 3-4 hrsit reaches a basic pH of ∼8.5. This means that the fullyhardened material is basic and stays basic throughout itsservice. This basic pH is the most important prerequisite forthe material to be bioactive, that is, creating apatite on itssurface when in contact with phosphate-containing solutions[17]. The apatite forms during hardening but its formationcontinues when the hardened material is in contact withphosphate solutions. The basic pH is also an important factorin the biocompatibility profile of the material. Additionally,the material produces an excess of Ca2+ ions, which alsocontributes to its bioactivity. The incorporation of calciumaluminate fixes the GIC structure and hinders the ionomerglass from continuously leaking over time. Ceramir C&B hasan initial fluoride release comparable to a glass ionomer,although the release tapers off over time. Unique propertiessuch as apatite formation and remineralization developquickly and continue to be active.
10. Pulpal Reactions
Ultimately, a postcementation pulpal reaction under clinicalconditions is dependent on three factors:
(1) composition of the cement. Postoperative hypersen-sitivity for most cements can be problematic and isbased on their chemistry, while only a few do notpresent a problem;
(2) the RDT—the larger the RDT the less risk of pulpirritation due to the greater buffering capacity of thefluid in the dentinal tubules;
(3) time elapsed from preparation to moment of cemen-tation—the longer this period, the better the pulp isable to recover from the trauma of preparation andtherefore can tolerate a subsequent irritation better.
11. Biocompatibility
Luting agents for permanent cementation of crown andbridge restorations have to meet many requirements beforethey can safely be used in humans. The ANSI/ADA Rec-ommended Standard Practices for Biological Evaluation ofDental Materials, Specification 41 (2005) [12], and the ISO7405 provide a road map outlining tests that are required inorder to meet these requirements. Physical properties suchas hardness, flexural strength, and solubility are extremelyimportant but if the material lacks biocompatibility, excellentphysical properties are meaningless. For practitioner andpatient alike, a luting agent that causes no postcementationhypersensitivity is highly desirable. Dentistry is still perceivedby many, as being “a painful experience” and every effortshould be made on the part of the dentist to make thetreatment as comfortable as possible. One such step is thefinal cementation of a fixed crown and bridge work, whethera single unit or a bridge. A restoration may be estheticallypleasing and functional at the time of cementation, buta sequel of postcementation hypersensitivity can generatequestions from the patient as to the success of the treatment,time from the practitioner to address the problem, andpossible complications that require further treatment. Extravisits may be required, all of which constitute a loss of timeand money not only for the practitioner, but also for thepatient.
Although zinc phosphate cement is still the “gold”standard, advances in luting agents over the last 30 yearshave produced new luting agents, which most likely willeventually replace zinc phosphate cement altogether. If welook at the three acid-base reaction cements, zinc phosphate,polycarboxylate and glass ionomer cement and comparethem to the hybrid-acid-base reaction cement, two of thethree cements (zinc phosphate and glass ionomer cements)have well recognized postcementation hypersensitivity prob-lems. This has frequently resulted in the need for root canaltreatment after permanent cementation of the fixed unit.Typical complaints of a patient are sensitivity to hot andcold and chewing. Assuming that the occlusion is not acausative factor, the only explanation is irritation caused bythe cement. Clearly, if the patient was comfortable during

6 International Journal of Dentistry
Table 1: This Table compares properties of the various generic cements. (Biocomp: biocompatibility; Integr: integration, Oxy inh layer:oxygen inhibited layer, RRGI: resin reinforced glass ionomer).
Cement Universal Retention Biocomp Sensitivity Integr Self-Etch Self-Seal Bioactive Oxy inh layer
Zinc Phosph No Low/med ∗ Yes No No No No No
Polycarb No Low ∗∗∗∗ No No No No No No
Glass ion No Medium ∗∗∗ Yes No No No No No
Resin No Medium ∗∗∗ No No No No No Yes
RRGI Yes Med/high ∗∗∗ ? No No No No yes
Self-etch resin cement Yes High ∗∗∗∗ ? ? Yes No No Yes
Hybrid CaAl/GI Yes High ∗∗∗∗∗ No Yes Yes Yes Yes No
Table 2: Comparison of additional properties of the various generic cements.
Cement Nano crystals Hydroxy apatite Hydrolysis Water sorption Resin-based Mineralizing F-release
Zinc Phosph No No No No No No No
Polycarb No No No No No No No
Glass ion No No No No No Yes Yes
Resin No No Yes No Yes No Yes
RRGI No No Yes Yes Yes No Yes
Self-etch resin cement No No Yes Yes Yes No Yes
Hybrid CaAl/GI Yes Yes No No No Yes Yes
the interim with a provisional restoration the problems pointtowards the irritation caused by the permanent cement.Mostly the pain will subside, more so with zinc phosphatecement than glass ionomers, but this may take weeks orlonger, and the practitioner can only guess at the ultimateoutcome. In vivo research has shown that indeed aftercementation with zinc phosphate cement and glass ionomerscauses pulpal irritation, which would explain the complaintsfrom patients [11].
RMGIs also have a record of occasional postcementationhypersensitivity due to their questionable biocompatibility[14]. In particular, unreacted monomers are highly toxic andirritating.
The resin cements and self adhesive resin cements have agood track record, although there are few, if any, reports thatsupport their biocompatibility.
Little clinical data are available on self-adhesive cements.Empirical data suggest that they are tolerated by the pulp,perhaps based on the change in acidity upon completesetting.
The many properties that are exhibited by luting agentsare summarized in Tables 1 and 2.
Tables 1 and 2 clearly show the differences between thevarious generic cements. It is therefore important that thepractitioner is familiar not only with the composition andproperties of the luting/bonding agent, but also with thecomposition of the restoration to be cemented.
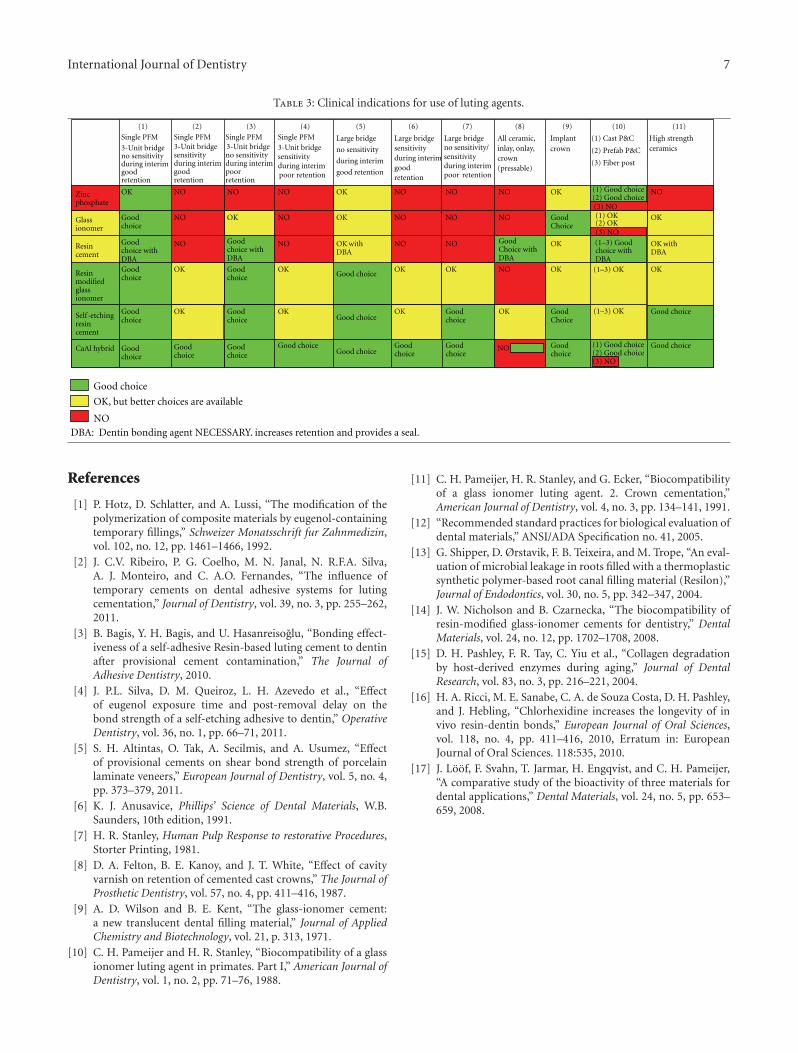
A separate flow chart is being presented in the appendix,which serves as a guide for the practitioner in the selectionof a final luting agent. Hypothetical clinical situations arebeing presented that can be cross-referenced with a choice ofa generic cement. The chart is based on clinical observations,research, and the literature.
12. Concluding Remark
The choice of an appropriate luting agent (cement) forfinal cementation of fixed crown and bridge units needscareful consideration as the ultimate success to a large extentdepends on the correct choice.
Appendix
See Table 3.
International Journal of Dentistry 7
Table 3: Clinical indications for use of luting agents.
Single PFM
3-Unit bridgeno sensitivityduring interimgood retention
Single PFM3-Unit bridgesensitivityduring interimgood retention
Single PFM3-Unit bridgeno sensitivityduring interimpoor retention
Single PFM3-Unit bridgesensitivityduring interimpoor retention
Large bridge
no sensitivity
during interim
good retention
Large bridgesensitivityduring interimgood retention
Large bridgeno sensitivity/sensitivityduring interimpoor retention
All ceramic, inlay, onlay, crown (pressable)
Implant crown
(1) Cast P&C
(2) Prefab P&C
(3) Fiber post
High strength ceramics
Zincphosphate
OK NO NO NO OK NO NO NO OK
(3) NO
NO
(1) OK(2) OKGlass
ionomer
Good choice
NO OK NO OK NO NO NO Good Choice
(3) NO
OK
Resin cement
Good choice withDBA
NO
NO
Good choice withDBA
NO OK withDBA
NO NO Good Choice withDBA
OKchoice withDBA
OK withDBA
Resin modified glass ionomer
Good choice
OK Good choice
OKGood choice
Good choice
OK OK NO OK OK
Self -etching resin cement
Good choice
OK
OK, but better choices are available
Good choice
OKGood choice
OK Good choice
OK Good Choice
Good choice
CaAl hybrid Good choice
Good Good choicechoice
Good choiceGood choice
Good choice
Good choice
NO Good choice
(1) Good choice(2) Good choice
(1) Good choice(2) Good choice
(3) NO
Good choice
DBA: Dentin bonding agent NECESSARY. increases retention and provides a seal.
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11)
(1–3) Good
(1–3) OK
(1–3) OK
References
[1] P. Hotz, D. Schlatter, and A. Lussi, “The modification of thepolymerization of composite materials by eugenol-containingtemporary fillings,” Schweizer Monatsschrift fur Zahnmedizin,vol. 102, no. 12, pp. 1461–1466, 1992.
[2] J. C.V. Ribeiro, P. G. Coelho, M. N. Janal, N. R.F.A. Silva,A. J. Monteiro, and C. A.O. Fernandes, “The influence oftemporary cements on dental adhesive systems for lutingcementation,” Journal of Dentistry, vol. 39, no. 3, pp. 255–262,2011.
[3] B. Bagis, Y. H. Bagis, and U. Hasanreisoglu, “Bonding effect-iveness of a self-adhesive Resin-based luting cement to dentinafter provisional cement contamination,” The Journal ofAdhesive Dentistry, 2010.
[4] J. P.L. Silva, D. M. Queiroz, L. H. Azevedo et al., “Effectof eugenol exposure time and post-removal delay on thebond strength of a self-etching adhesive to dentin,” OperativeDentistry, vol. 36, no. 1, pp. 66–71, 2011.
[5] S. H. Altintas, O. Tak, A. Secilmis, and A. Usumez, “Effectof provisional cements on shear bond strength of porcelainlaminate veneers,” European Journal of Dentistry, vol. 5, no. 4,pp. 373–379, 2011.
[6] K. J. Anusavice, Phillips’ Science of Dental Materials, W.B.Saunders, 10th edition, 1991.
[7] H. R. Stanley, Human Pulp Response to restorative Procedures,Storter Printing, 1981.
[8] D. A. Felton, B. E. Kanoy, and J. T. White, “Effect of cavityvarnish on retention of cemented cast crowns,” The Journal ofProsthetic Dentistry, vol. 57, no. 4, pp. 411–416, 1987.
[9] A. D. Wilson and B. E. Kent, “The glass-ionomer cement:a new translucent dental filling material,” Journal of AppliedChemistry and Biotechnology, vol. 21, p. 313, 1971.
[10] C. H. Pameijer and H. R. Stanley, “Biocompatibility of a glassionomer luting agent in primates. Part I,” American Journal ofDentistry, vol. 1, no. 2, pp. 71–76, 1988.
[11] C. H. Pameijer, H. R. Stanley, and G. Ecker, “Biocompatibilityof a glass ionomer luting agent. 2. Crown cementation,”American Journal of Dentistry, vol. 4, no. 3, pp. 134–141, 1991.
[12] “Recommended standard practices for biological evaluation ofdental materials,” ANSI/ADA Specification no. 41, 2005.
[13] G. Shipper, D. Ørstavik, F. B. Teixeira, and M. Trope, “An eval-uation of microbial leakage in roots filled with a thermoplasticsynthetic polymer-based root canal filling material (Resilon),”Journal of Endodontics, vol. 30, no. 5, pp. 342–347, 2004.
[14] J. W. Nicholson and B. Czarnecka, “The biocompatibility ofresin-modified glass-ionomer cements for dentistry,” DentalMaterials, vol. 24, no. 12, pp. 1702–1708, 2008.
[15] D. H. Pashley, F. R. Tay, C. Yiu et al., “Collagen degradationby host-derived enzymes during aging,” Journal of DentalResearch, vol. 83, no. 3, pp. 216–221, 2004.
[16] H. A. Ricci, M. E. Sanabe, C. A. de Souza Costa, D. H. Pashley,and J. Hebling, “Chlorhexidine increases the longevity of invivo resin-dentin bonds,” European Journal of Oral Sciences,vol. 118, no. 4, pp. 411–416, 2010, Erratum in: EuropeanJournal of Oral Sciences. 118:535, 2010.
[17] J. Loof, F. Svahn, T. Jarmar, H. Engqvist, and C. H. Pameijer,“A comparative study of the bioactivity of three materials fordental applications,” Dental Materials, vol. 24, no. 5, pp. 653–659, 2008.

Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral OncologyJournal of
DentistryInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
International Journal of
Biomaterials
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Case Reports in Dentistry
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral ImplantsJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Anesthesiology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Radiology Research and Practice
Environmental and Public Health
Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Dental SurgeryJournal of
Drug DeliveryJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral DiseasesJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PainResearch and TreatmentHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Preventive MedicineAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
OrthopedicsAdvances in