restless
TRANSCRIPT

Restless Leg Syndrome
D.M.W. Dharmakeerthi (MD)
Senior Registrar in Clinical Neurophysiology

Restless Leg Syndrome
•“The most common disorder some have never heard of.”
What are Restless legs? Neurological movement disorder Irresistible urge to move legs when at
rest Difficulty sleeping Involuntary periodic leg movements Uncomfortable sensation in limbs
subjective & difficult to describe Symptoms eased by movement

Why should we know about it? Excess 5 million in UK are sufferers (MEMO
2000)
Estimated prevalence 2-15% Sufferers will present to primary care Important physical cause of sleep
disturbance Clinical diagnosis which can be made in
primary care

Why should we know about it?
Unrecognised & under-diagnosed
Incorrectly labeled as stress / anxiety
Managed poorly

Wide spectrum Affects any age group
More common in middle age + women Mild
Minimal distress Severe
Episodes occur >2 per week Can be disabling

Why is it important? Large impact on quality of life: (REST Study)
Poor sleep Inability to get comfortable / relax Poor concentration / fatigue Pain Depression Problems in day to day functioning / employment Implications for partner

Common descriptive terms used by patients

How do we diagnose RLS? International Restless Legs Syndrome
Study Group - 2003

Supporting Features Positive FHx (50-92%)
Involuntary limb movements (80%)
Sleep disturbance

Classification Primary
No underlying cause found. Positive FHx >50% Earlier onset / slower progression
Secondary
Sudden onset.
Often occurs after the age of 40
Most associated with specific medical conditions or the use of certain drugs.

Pathophysiology Genetic
Susceptibility loci identified on 3 chromosomes
Genetic anticipation Positive FHx >50%
Neurochemical Dopaminergic dysfunction - universal
response to dopaminergic agents Ferritin level - inverse relation between
severity and serum ferritin

Primary RLS
Idiopathic. Familial in 25-75% of cases(AD). Progressive decrease in age at onset
with subsequent generations ( genetic anticipation).
Begins before approximately 40 to 45 years of age, and can even occur as early as the first year of life.

Primary RLS
Onset is often slow. RLS may disappear for months, or even
years. Often progressive and gets worse as
the person ages. RLS in children is often misdiagnosed
as growing pains.

Secondary RLS
Iron deficiency Varicose vein folate deficiency magnesium deficiency sleep apnea uremia diabetes thyroid disease

Secondary RLS
Auto-immune disorders ( Sjögren's syndrome, celiac disease and rheumatoid arthritis)
Acute intermittent porphyria Fibromyalgia Cholesterol peripheral microemboli. RLS can also worsen in pregnancy.

Neurologic conditions linked to RLS Parkinson disease Spinal cerebellar atrophy Spinal stenosis Lumbosacral radiculopathy Charcot-Marie-Tooth disease type 2.

What investigations should we do? Exclude secondary cause.
Vascular dx / Neuropathy / nocturnal cramp / anxiety
Examination Neuro / vascular
Bloods FBC, ferritin, B12, Folate, U&E, Glucose,
TFT, Auto immune screening etc.

What are the treatment options? Non Pharmacological
Preventative measures Symptomatic control
Pharmacological PRN treatment - mild / intermittent Maintenance treatment - moderate / severe Majority of treatments used ‘off license’
Non pharmacological treatment
Preventative Avoid caffeine / alcohol / nicotine Avoid medication which may aggravate
SSRI / antihistamine / antiemetic / CaChannel blockers Keep active into evening Good sleep hygiene
Symptom control Mental alerting activities Walking / stretching Massage Hot / cold bath Relaxation / biofeedback

Pharmacological optionsDrug Advantage Disadvantage
Iron Helpful if serum ferritin low
Slow response
Dopamine agonistPramipexole / ropinirole
High efficacy (70-100%)Less augmentation
Daytime sleepinessLong term effect not known
Dopaminergic agentCarbidopa / levodopa
Can be used PRN basisShown to be effective
Up to 80% develop augmentation
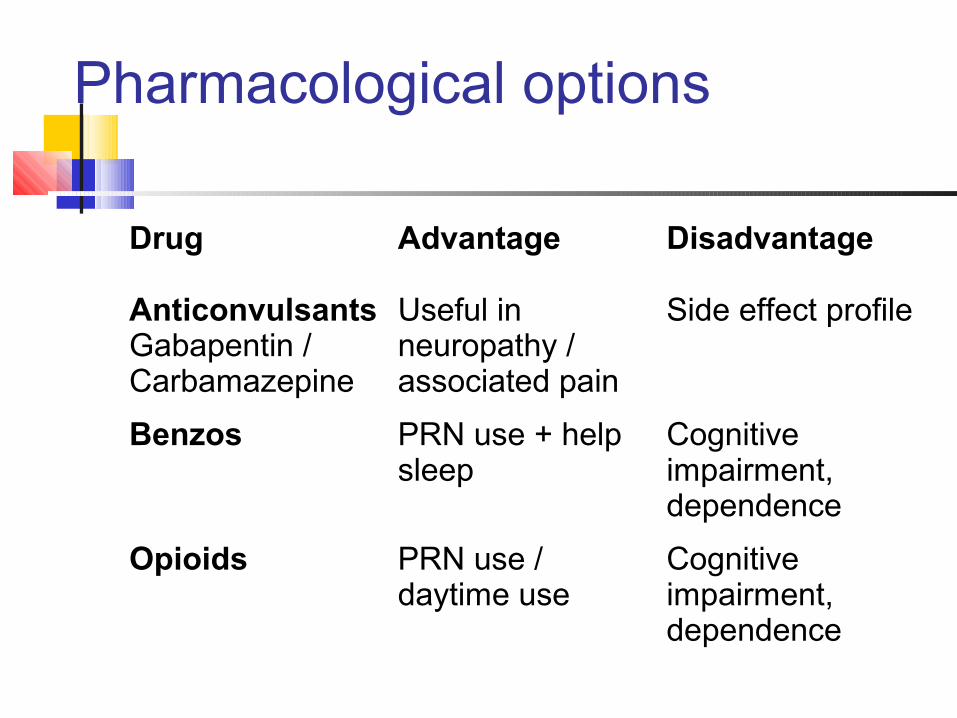
Pharmacological options
Drug Advantage Disadvantage
AnticonvulsantsGabapentin / Carbamazepine
Useful in neuropathy / associated pain
Side effect profile
Benzos PRN use + help sleep
Cognitive impairment,dependence
Opioids PRN use / daytime use
Cognitive impairment,dependence
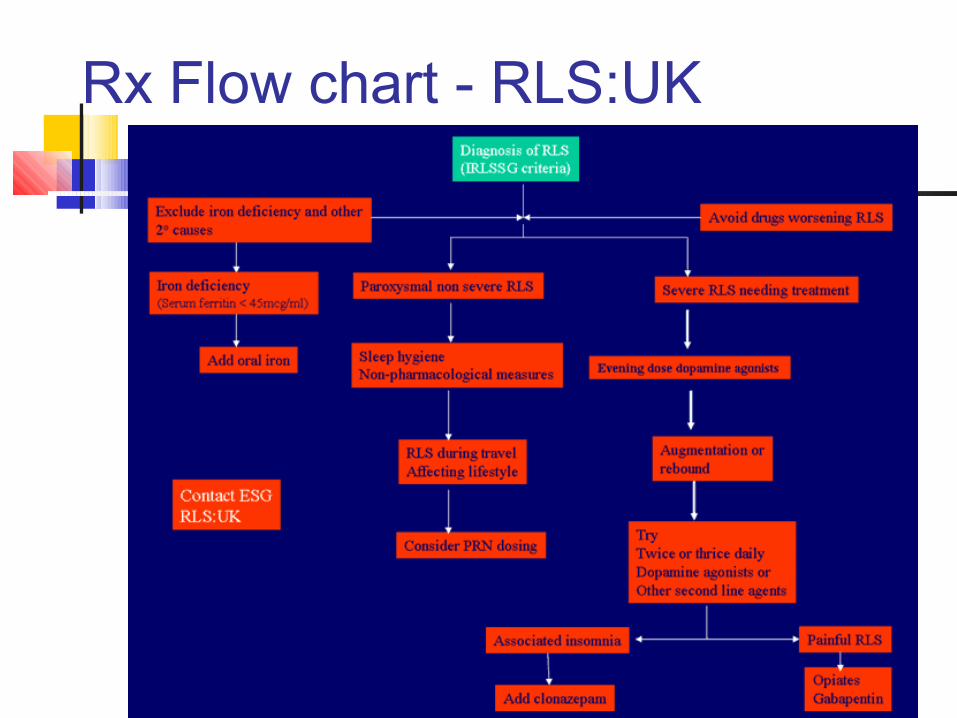
Rx Flow chart - RLS:UK
Mirapexin (pramipexole) First drug treatment / ONLY treatment
licensed in EU for RLS For use in moderate / severe disease Quick onset of symptom relief (<1/52) Start low dose 125mcg od Titrate up (max 750mcg od)

What should we be doing?
Have raised awareness about diagnosis Exclude / treat secondary causes Symptoms generally mild +
reassurance & non-pharmacological measures suffice
In moderate / severe cases consider onward referral

Useful Info Resources
www.ekbom.org.uk www.restlesslegs.org.uk www.restlesslegs.com
Review DTB Nov 2003 Bandolier 118
Thank you