respiratory tract infections. prof. azza elmedany department of pharmacology
TRANSCRIPT

Respiratory Tract Respiratory Tract infectionsinfections

PROF.PROF.
AzzA ELMedanyAzzA ELMedany
Department of pharmacologyDepartment of pharmacology
Objectives of the lectureObjectives of the lecture
At the end of lecture , students should At the end of lecture , students should be able to understand the following:be able to understand the following:
Types of respiratory tract infectionsTypes of respiratory tract infectionsAntibiotics commonly used to treat Antibiotics commonly used to treat
respiratory tract infections and theirrespiratory tract infections and their
side effects.side effects. Understand the mechanism of action, Understand the mechanism of action,
pharmacokinetics of individual drugs.pharmacokinetics of individual drugs.

The respiratory tractThe respiratory tract

Classification of Classification of respiratory tract respiratory tract
infectionsinfectionsUpper respiratory tract infections Upper respiratory tract infections
(URTI)(URTI)
Lower respiratory tract infections Lower respiratory tract infections (LRTI) (LRTI)

URTIURTIRhinitis- inflammation of the nasal Rhinitis- inflammation of the nasal
cavity cavity Sinusitis- inflammation of sinusesSinusitis- inflammation of sinusesPharyngitis- inflammation of the Pharyngitis- inflammation of the
pharynx,pharynx, uvula, tonsilsuvula, tonsilsLaryngitis- inflammation of the larynxLaryngitis- inflammation of the larynxLaryngotracheitis- inflammation of the Laryngotracheitis- inflammation of the
larynx & trachealarynx & tracheaTracheitis- inflammation of tracheaTracheitis- inflammation of tracheaOtitis media- inflammation of middle Otitis media- inflammation of middle
earear
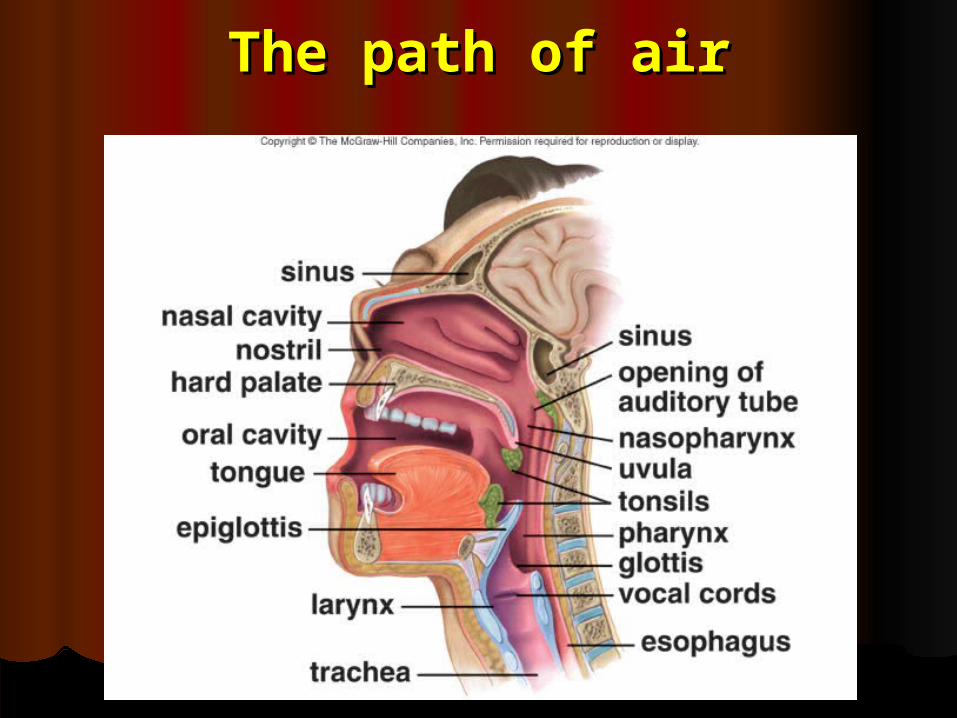
The path of airThe path of air

LRTILRTI
BronchitisBronchitis
AcuteAcute
ChronicChronic
Acute exacerbation of chronic Acute exacerbation of chronic bronchitisbronchitis
PneumoniaPneumonia
Community -acquired Community -acquired
Hospital-acquiredHospital-acquired
LRTILRTI,,ssAre more costly to treat and Are more costly to treat and
generally more serious than URTIgenerally more serious than URTI,,ss

Causes of URTICauses of URTI,,ss
Viruses ( over 200 different types Viruses ( over 200 different types have been isolated ) have been isolated )
Bacteria , mainly Group A Bacteria , mainly Group A streptococcus & H. influenzae streptococcus & H. influenzae

Causes of LRTICauses of LRTI,,ss
Bacteria mainly:Bacteria mainly:Streptococcus pneumoniaeStreptococcus pneumoniaeHaemophilus influenzaeHaemophilus influenzaeMoraxella catarrhalis Moraxella catarrhalis
Lines for treatment of Lines for treatment of respiratory tract respiratory tract
infectionsinfectionsAnalgesics ( NSAIDs)Analgesics ( NSAIDs)Nasal decongestant Nasal decongestant Vitamin CVitamin CDrinking plenty of fluidsDrinking plenty of fluidsAntiviralAntiviralAntibioticsAntibiotics
AntibioticsAntibiotics
First-line treatment ( given for 3-First-line treatment ( given for 3-10 days10 days))
For the treatment of moderate to For the treatment of moderate to severe infections severe infections
Broad spectrum penicillinsBroad spectrum penicillinsTrimethoprim-sulfamethoxazoleTrimethoprim-sulfamethoxazoleTetracyclines ( doxycycline ) Tetracyclines ( doxycycline )

Antibiotics ( continue)Antibiotics ( continue) Second-line treatmentSecond-line treatment Used in allergic patients to drugs of Used in allergic patients to drugs of
first –line or in antibiotic –resistant first –line or in antibiotic –resistant organismsorganisms
Macrolids Macrolids CephalosporinsCephalosporinsFluoroquinolonesFluoroquinolones

PenicillinsPenicillins
Mechanism of actionMechanism of action
Inhibits bacterial cell wall Inhibits bacterial cell wall synthesissynthesis
BactericidalBactericidal

PharmacokineticsPharmacokinetics
Given orally or parnterallyGiven orally or parnterallyNot metabolized in human.Not metabolized in human.Relatively lipid insoluble.Relatively lipid insoluble.Excreted mostly unchanged Excreted mostly unchanged in urine.in urine.Half-life 30-60 min Half-life 30-60 min ( increased in renal failure)( increased in renal failure). .

Broad- spectrum Broad- spectrum penicillinspenicillins
AmoxicillinAmoxicillinAmpicillinAmpicillin
Acts on both gram –positive & gram- Acts on both gram –positive & gram- negative bacteria negative bacteria
Destroy by Destroy by ββ-lactamase enzyme -lactamase enzyme produced by certain bacteriaproduced by certain bacteria

ββ-Lactamase inhibitors-Lactamase inhibitors
Such as : Such as : Clavulanic acidClavulanic acidSulbactam Sulbactam TazobactamTazobactam
Themselves have no antibacterial Themselves have no antibacterial activity.activity.
They inactivate They inactivate ββ-lactamase enzyme-lactamase enzyme

ββ-Lactamase inhibitors -Lactamase inhibitors (continue)(continue)
Given in combination with Given in combination with ββ - -lactamase sensitive antibiotics :lactamase sensitive antibiotics :
AmoxicillinAmoxicillin//clavulanic acid clavulanic acid ((augmentinaugmentin ) )
AmpicillinAmpicillin/ / sulbactamsulbactam

Therapeutic usesTherapeutic uses
Upper respiratory tract infectionsUpper respiratory tract infections
Lower respiratory tract infectionsLower respiratory tract infections

CephalosprinsCephalosprins

Mechanism of actionMechanism of action
Inhibit bacterial cell wall synthesisInhibit bacterial cell wall synthesis
BactericidalBactericidal

ClassificationClassification
11stst Generation Generation CephalosporinsCephalosporins
CephalexinCephalexinGiven orallyGiven orallyEffective against Gram positive Effective against Gram positive
bacteria & to some extent to bacteria & to some extent to Gram-negativeGram-negative
Effective in upper respiratory Effective in upper respiratory tract infectionstract infections


22ndnd Generation Generation CephalosporinsCephalosporins
Cefuroxime axetil (zinnat)Cefuroxime axetil (zinnat)Effective mainly on Gram –Effective mainly on Gram –
negative bacteria .negative bacteria .Given orallyGiven orally
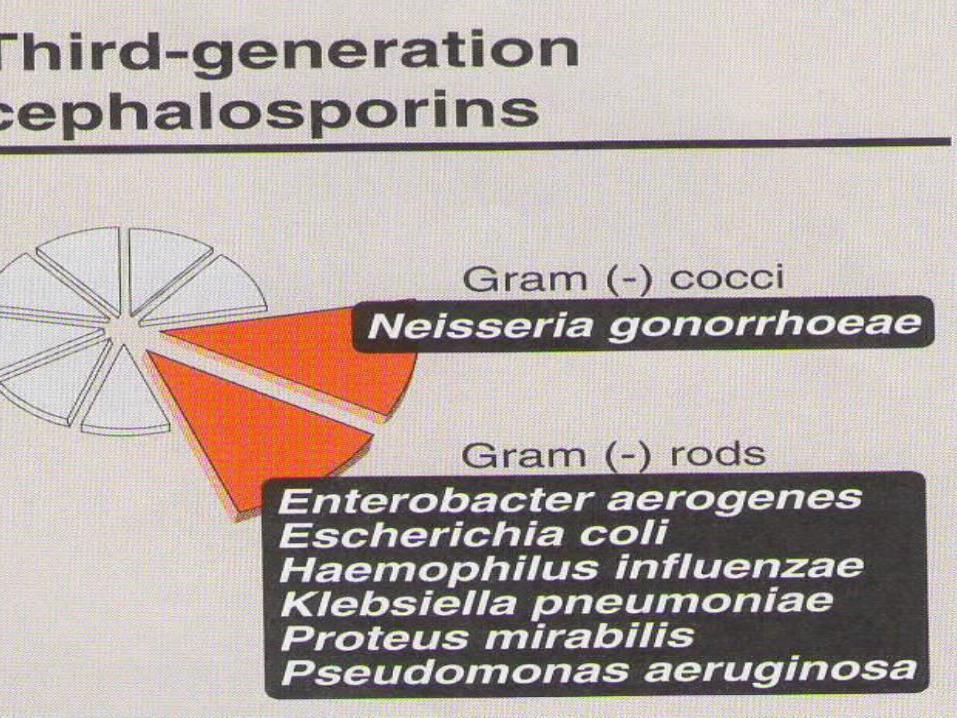
33rdrd Generation Generation CephalosporinsCephalosporins
Ceftriaxone / CefotaximeCeftriaxone / CefotaximeNot susceptible to hydrolysis by Not susceptible to hydrolysis by
ββ-lactamase.-lactamase.Effective against gram-negative Effective against gram-negative
bacteriabacteriaGiven by intravenous routeGiven by intravenous routeEffective in treatment of Effective in treatment of
pneumonia caused by pneumonia caused by ββ--lactamase producing bacterialactamase producing bacteria

Pharmacokinetics of Pharmacokinetics of cephalosporinscephalosporins
Given parnterally or orallyGiven parnterally or orally
Relatively lipid insolubleRelatively lipid insoluble
Excreted Mostly unchanged in the urine. Excreted Mostly unchanged in the urine. Half-life 30-90 min (increased in renal failure)Half-life 30-90 min (increased in renal failure)
Adverse effects of Adverse effects of cephalosporins cephalosporins

Mechanism of actionMechanism of action
Inhibit protein synthesis by binding to the Inhibit protein synthesis by binding to the 50 S subunit of the bacterial ribosomes 50 S subunit of the bacterial ribosomes
BacteriostaticBacteriostatic
Bactericidal at high concentrationBactericidal at high concentration

ClarithromycinClarithromycin
Stable to stomach acidityStable to stomach acidity
Inhibits cytochrome P-450 systemInhibits cytochrome P-450 system
Metabolized in liver to active Metabolized in liver to active metabolite metabolite (antibacterial (antibacterial activity)activity)
Half-life 6-8 hoursHalf-life 6-8 hours
AzithromycinAzithromycin
Rapidly absorbed from GITRapidly absorbed from GITFood delays absorptionFood delays absorptionStable against gastric acidityStable against gastric acidity
Undergo some hepatic metabolism ( inactive )Undergo some hepatic metabolism ( inactive )Biliary route is the major route of eliminationBiliary route is the major route of eliminationOnly 10-15% excreted unchanged in the urineOnly 10-15% excreted unchanged in the urineHalf- life ( 3 days)Half- life ( 3 days)Advantage over clarithromycinAdvantage over clarithromycin1- Once daily dosing1- Once daily dosing
2- No effect on cytochrome 2- No effect on cytochrome P- 450P- 450

Adverse effectsAdverse effects


Mechanism of actionMechanism of action
Inhibit DNA synthesis by Inhibit DNA synthesis by inhibiting inhibiting DNA Gyrase enzyme DNA Gyrase enzyme

CIPROFLOXACINCIPROFLOXACIN
Antibacterial spectrumAntibacterial spectrum
Mainly effective against G – Mainly effective against G – bacteria bacteria
** Not effective against G+ and ** Not effective against G+ and anaerobesanaerobes

PharmacokineticsPharmacokinetics
Well absorbed orally ( available i.v ) Di & tri- valent cations interfere with its absorption Concentrates in many tissues, esp. kidney, prostate, lung & bones/ joints Poorly crossing BBB Excreted mainly through the kidney Half-life average 3 hrs
GatifloxacinGatifloxacin
Is a new fluoroquinolonesIs a new fluoroquinolonesHas extended gram-positive activityHas extended gram-positive activityGiven once dailyGiven once daily11stst line treatment of LRTI line treatment of LRTI It is effective against community It is effective against community
acquiredacquired
pneumonia pneumonia

Adverse effects of Adverse effects of fluoroquinolonesfluoroquinolones
Nausea , vomiting & diarrheaNausea , vomiting & diarrhea
CNS effects – confusion, insomnia, CNS effects – confusion, insomnia, headache, dizziness & anxiety.headache, dizziness & anxiety.
Damage growing cartilageDamage growing cartilage
Phototoxicity (avoid excessive Phototoxicity (avoid excessive sunlight )sunlight )

ContraindicationsContraindicationsAdolescents ( under 18 years )Adolescents ( under 18 years )
During pregnancyDuring pregnancy
Breast feeding womenBreast feeding women
Clinical UsesClinical Uses

THANK YOUTHANK YOU