respiratory infections and the infant rees oliver md assistant professor department of pediatrics...
TRANSCRIPT
Respiratory Infections and the Infant
Rees Oliver MDAssistant Professor
Department of PediatricsDivision of NeonatologyUniversity of Alabama at
Birmingham

Disclosure statement:
I do speak as a consultant on behalf of MedImmune for the product Synagis.


With permission from Simoes EAF and Carbonell-Estrany X. Pediatr Infect Dis J. 2003;22:S13-S20.
Causes of Acute Respiratory Infections in Children <5 Years of Age
Data from the Belgian sentinel network’s epidemiology surveillance (2000–2001 season)
Adenovirus 7%
C. pneum. 0%
M. pneum. 9%
H. infl. 6%
Parainfluenza 2%
Infl. B 2%
Infl. A 3%
S. pneum. 8%
RSV 62%
3
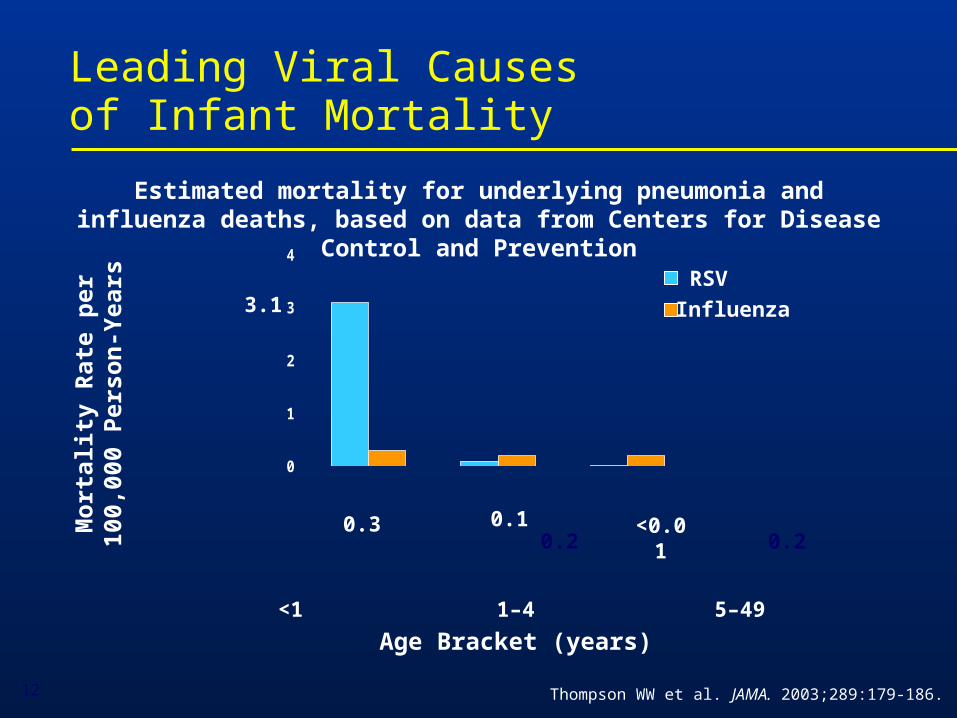
Leading Viral Causesof Infant Mortality
Thompson WW et al. JAMA. 2003;289:179-186.
<1 1–4 5–49
Age Bracket (years)
Mo
rtal
ity
Rat
e p
er10
0,00
0 P
erso
n-Y
ears
RSV
Influenza
0
1
2
3
4
Estimated mortality for underlying pneumonia and influenza deaths, based on data from Centers for Disease Control and Prevention
3.1
0.3 0.10.2 0.2
<0.01
12
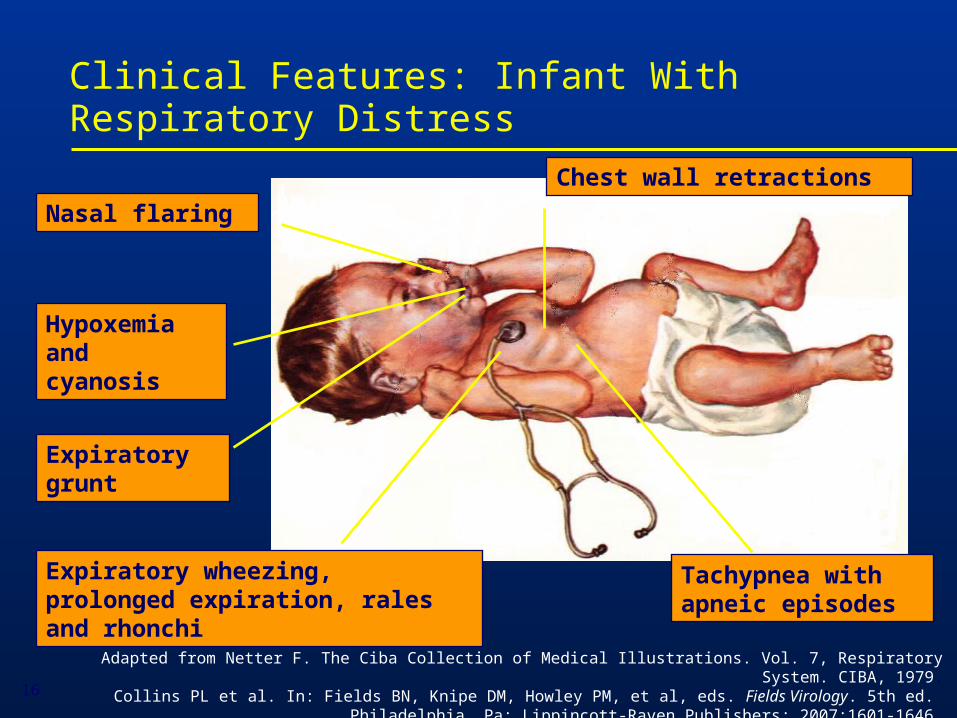
Expiratory wheezing, prolonged expiration, rales and rhonchi
Chest wall retractions
Tachypnea with apneic episodes
Nasal flaring
Hypoxemia and cyanosis
Expiratory grunt
Clinical Features: Infant With Respiratory Distress
Adapted from Netter F. The Ciba Collection of Medical Illustrations. Vol. 7, Respiratory System. CIBA, 1979.Collins PL et al. In: Fields BN, Knipe DM, Howley PM, et al, eds. Fields Virology. 5th ed.
Philadelphia, Pa: Lippincott-Raven Publishers; 2007:1601-1646.16
Signs and Symptoms of Respiratory Distress in Infants
Mild symptoms: moderate tachypnea, rhinorrhea, low-grade fever, and, frequently, otitis media. Recovery occurs after an illness of 7 to 12 days
Severe symptoms: coughing and wheezing followed by dyspnea; severe tachypnea is common; in cases of extreme hypoxemia, respiratory failure occurs
In high-risk infants, respiratory failure severe enough to require airway intubation can occur early in the course of illness
Collins PL et al. In: Fields BN, Knipe DM, Howley PM, et al, eds. Fields Virology. 5th ed. Philadelphia, Pa: Lippincott-Raven Publishers; 2007:1601-1646.
17

Transmission of Viruses
• Viruses can be transmitted by droplets, large particles, and fomites
• Can survive for as long periods of time on nonporous surfaces
• Medical personnel transmit these viruses readily
• Nosocomial infection remains an enormous problem
Blydt-Hansen T, et al. Pediatr Infect Dis J. 1999;18(2):164; Hall CB, et al. J Pediatr. 1980;141:98-102;
Hall CB. Clinical Infectious Diseases; 2000;31:590-6; Cohen B, et al. Pediatric Infectious Disease Journal. 2003;22:494-9

Epidemiology of Viral Processes
• Several of these viruses produce outbreaks each year particularly RSV
• In the case of these outbreaks they can vary in length from region to region, and from season to season and can last for months throughout much of the U.S.
• Year-round epidemics have been reported
Mavunda K, et al. Am J Crit Care Pulm Med. 2000;ATS Abstr # G55:348; Ledbetter JC, et al. Ped ResAPS/SPR/APA. 2002;Abstr #2787; Doraisingham S, Ling ,AE. Ann Acad Med Singapore. 1986;15:9-14
Viral Epidemiology
• During any given season a large portion of the population develops an upper or lower respiratory tract infection (LRTI), Bronchiolitis
• More than half of all children will be infected by their first birthday especially with RSV
• By two years of age essentially all children have been experienced Bronchiolitis
Glezen WP, et al. Am J Dis Child. 1986;140:543-6
Re-infection
• If you look at studies looking at these viruses there are reports that between 6% and 83% of children followed longitudinally have been re-infected each year
• Antibody response is sometimes not sufficient to prevent subsequent re-infection
• Infected lymphocytes and macrophages may suppress secondary immune responses
Feigin RD, Cherry JD, (Eds.). Textbook of Pediatric Infectious Diseases, 4th Ed. 1998. 185.2095; Hall CB, et al. Journal of Infectious Diseases. 163,no.4(1991):693-8;Openshaw, P.J.M. Respiratory Research 3, Suppl 1. (2002):S15

Recent Trends in Hospitalizations
• Up to 126,300 annual hospitalizations among U.S. infants for bronchiolitis or pneumonia may be attributed to RSV alone.
• Bronchiolitis hospitalizations 1980-1996
– 1.65 million hospitalizations
– 7 million inpatient days
– 57% were in children <6 mo
– 81% were in children <1 yo
– 239% increase in bronchiolitis hospitalizations in children less than six months of age
Shay DK, et al. J Infect Dis. 2001;183:16-22; Institute of Medicine. In: New Vaccine Development: Establishing Priorities. Vol I. Wash DC Nat Aca Press 1986: 397-409; Shay DK, et al. JAMA. 1999;282:1440-9
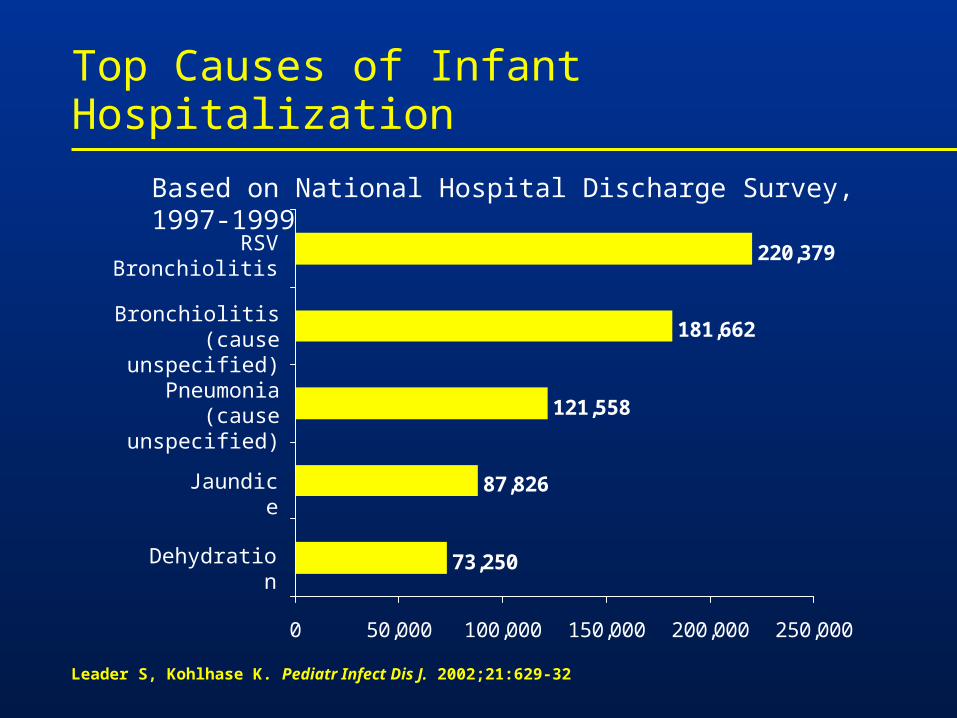
Leader S, Kohlhase K. Pediatr Infect Dis J. 2002;21:629-32
Top Causes of Infant Hospitalization
73,250
87,826
121,558
181,662
220,379
0 50,000 100,000 150,000 200,000 250,000
Dehydration
Jaundice
Pneumonia(cause unspecified)
Bronchiolitis(cause unspecified)
RSV Bronchiolitis
Based on National Hospital Discharge Survey, 1997-1999
• Several prospective studies have shown that even RSV bronchiolitis is associated with recurrent wheezing during subsequent years
• Recurrent wheezing tends to diminish by early adolescence (age 13)
• Conclusion: RSV bronchiolitis appears to be linked to recurrent childhood wheezing through early adolescence
Sigurs N, et al. Am J Crit Care Med. 2000;161:1501-7Taussig LM, et al. Am J Epidemiol. 1989;129:1219-31Stein RT, et al. The Lancet. 1999;354:541-5

Children at Highest Risk for Severe Respiratory Distress as an Infant
Adapted from a presentation by L Weisman, MD: 1st International Congress RSV, 2002
Premature birth
Chronic Lung Disease
Congenital Heart disease
Neuromuscular disease
Immune deficiency
• Altered airway anatomy• Absence of maternal antibody
• Bronchial hyper-responsiveness• Reduced lung capacity
• Pulmonary vascular hyper-responsiveness• Pulmonary hypertension• Increased pulmonary blood flow
• Decreased respiratory muscle strength and endurance
• Decreased host defenses• Impaired capacity to eliminate virus
Problems in Premature Infants
•Respiratory: Airway alteration, respiratory distress/failure, apnea, air leaks, CLD/BPD
•Cardiovascular: Patent ductus arteriosus
•CNS: Intraventricular hemorrhage, periventricular leukomalacia, seizures
•Renal: Electrolyte imbalance, acid-base disturbances, renal failure
•Ophthalmologic: Retinopathy of prematurity, strabismus, myopia
•Gastrointestinal-nutritional: Feeding intolerance, necrotizing enterocolitis, inguinal hernias, failure to thrive
•Immunologic: Poor defense to infection
Boyce TG, et al. J Pediatr. 2000;137:865-70; Law BJ, et al. Paediatr Child Health. 1998;3:402-4; Imaizumi S, Agarwal S, Pereira GR, et al. APS/SPR/APA – 2001 convention 4-28-2001. Abstract
Prematurity: Increased Disease Severity
• Several studies have confirmed the high-risk status of premature infants
• Among premature infants hospitalized with RSV and other viral pathogens:
– 28-34% were admitted to the ICU
– 7-22% required mechanical ventilation
Premature Infants are at High-Risk
Altered lung development
• Altered airway anatomy
• Reduced lung function through early childhood
Immature immune system
• Impaired humoral and cellular immunity

*Pictures are artistic renditions of lung development and are designed to emphasize terminal acinus development & not the entire conducting airway system
Behrman: Nelson Textbook of Pediatrics, 16th ed., 2000. Langston C, et al. Am Rev Respir Dis. 1984;129:607-13
Pseudoglandular Period
(7 to 16 weeks GA)
Canalicular Period
(16 to 26 weeks GA)
Saccular Period
(26 to 36 weeks GA)
Alveolar Period
(36 to 41 weeks GA)
Premature Term
• The lungs of premature infants are underdeveloped at birth
• Although alveoli are present in some infants as early as 32 weeks GA, they are not uniformly present until 36 weeks GA
Prematurity: Interrupts Lung Development
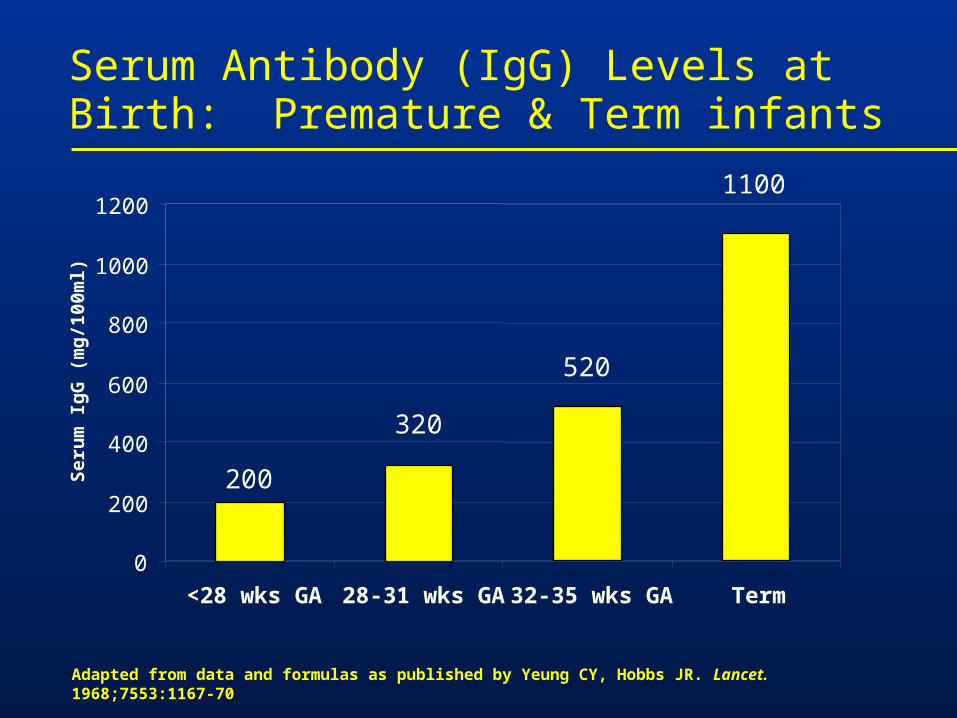
Adapted from data and formulas as published by Yeung CY, Hobbs JR. Lancet. 1968;7553:1167-70
Serum Antibody (IgG) Levels at Birth: Premature & Term infants
200
320
520
1100
0
200
400
600
800
1000
1200
<28 wks GA 28-31 wks GA 32-35 wks GA Term
Ser
um
Ig
G (
mg
/100
ml)
Summary: Risk of Severe Disease in Premature Infants
• Hospitalization rates demonstrate that premature infants up to 36 wks GA are potentially high risk for severe respiratory distress
• Premature infants, even those without a history of ventilation or oxygen use, are high risk due to
– Altered airway anatomy-significant obstruction seen throughout early childhood
– Immature immunity-impaired cellular and humoral immunity

Congenital Heart Disease
• Increased morbidity and mortality. Statistics among children hospitalized:
– 25-33% admission to PICU
– 11-24% mechanical ventilation
– 3.4% fatality rate
• CHD patients with associated pulmonary hypertension are at highest risk for complications.
Navas L, et al. J Pediatr. 1992;121:348-54; Altman CA, et al. Pediatr Cardiol. 2000;21:433-8;Moler FW, et al. Crit Care Med. 1992;20:1406-13; MacDonald NE, et al. N Engl J Med. 1982;307:397-400; Khongphatthanayothin A, et al. Crit Care Med. 1999;27:1974-81

Risk Factors in CHD Patients
• Compromised cardiorespiratory status at baseline
• Altered pulmonary mechanics may contribute to disease severity
• Pulmonary hypertension may exacerbate the adverse effects of respiratory disease
• Inability to properly compensate for intercurrent disease

Navas L, et al. J Pediatr. 1992;121:348-54
Chronic Lung Disease: Increased Risk of Severe Respiratory Distress
• Studies have confirmed the high-risk status of children with Chronic Lung Disease (CLD)
• Among CLD children hospitalized viral processes:
– 32% were admitted to the ICU
– 17% required mechanical ventilation
– 3.5% died within two weeks

Therapeutic Options for Bronchiolitis
• Prevention
– Limit exposure– Avoid daycare
– Excellent hand washing
– Passive immunoprophylaxis:Synagis® (palivizumab)
• Supportive care
• Overcoming airway obstruction and inflammation
Prophylaxis: Reserved for the Highest Risk Children
• RSV immunoprophylaxis is the only available safe and effective method for preventing severe RSV disease
• Prophylaxis is reserved for high risk infants and children
– Premature infants <36 wks GA are at a significantly elevated risk of severe RSV disease
– Children with chronic lung disease, congenital heart disease, immunodeficiencies, and other high-risk conditions
The IMpact-RSV Study Group. Pediatrics. 1998;102(3):531-7; Boyce TG, et.al. J. Pediatr. 2000;137:865-70;Imaizumi S, et al. Abstract # 2311:APS/SPR/APA-2001;Law BJ, et al. CAAC 1998 (abstract #MN-9);Meissner HC, et al. Pediatr Infect Dis J. 1999;18:223
IMpact-RSV Clinical Trial: Study Design
Multicenter, randomized, placebo-controlled trial
Infants 35 weeks gestational age (GA) or with bronchopulmonary dysplasia (BPD) were randomized (N=1502) to receive 5 injections of Synagis® (palivizumab) (15 mg/kg) or equivalent volume of placebo every 30 days
The IMpact-RSV Study Group. Pediatrics. 1998;102:531-537.Please see full prescribing information for Synagis® (palivizumab).
65

IMPACT-RSV TRIAL
RSV Hospitalization Rates by Subgroup
10.6 11.09.8
4.85.8
2.00
2
4
6
8
10
12
All patients All < 32 weeks GA All 32-35 weeks GA
Placebo: 1996-1997 IMpact-RSV trial (n=500)Synagis® (palivizumab): 1996-1997 IMpact-RSV trial (n=1,002)
55% 47% 80%
Reduction
The IMpact-RSV Study Group. Pediatrics. 1998;102(3):531-7
Summary
• There is significant viral pathogens, some producing annual epidemics and others that are common to our communities
• Bronchiolitis is a major threat to the health of all infants and can lead to hospitalization and death
• The threat of these viruses is greatest in high-risk groups, such as infants born prematurely and children with CLD or CHD
• Treatment options are limited