respiratory epithelium lined cysts presenting in the orbit without
TRANSCRIPT

British Journal of Ophthalmology, 1986, 70, 387-390
Respiratory epithelium lined cysts presenting in theorbit without associated mucocele formationC R H JAMES, R LYNESS, AND J E WRIGHT
From Moorfields Eye Hospital, City Road, London EC]V2PD
SUMMARY Three patients presented with orbital cysts lined with upper respiratory tractepithelium. In each case there was no evidence of an associated mucocele. Two patients had a pasthistory of orbital trauma, and the third had had preceding sinus surgery. It is postulated that thesecysts were caused by traumatic herniation of nasal sinus epithelium cells into the orbit.
The usual pathological route for upper respiratorytract epithelium to find its way into the orbit is inassociation with mucocele formation. Mucocelesaccount for up to 10% of unilateral proptosis. I2 Theycommonly present in the fourth and fifth decades oflife in association with chronic sinus disease, thoughthey may also occur in children with cystic fibrosis.34
It is generally accepted that mucoceles form as aresult of blockage of the normal drainage pathway ofa sinus. Increased pressure, from continuing secre-tion by the lining of respiratory epithelium, causessinus expansion and may eventually be associatedwith osteoclastic resorption of its bony wall. Thisallows the enlarging respiratory epithelium lined cystto enter the orbit, with ensuing ocular displacementand proptosis (Fig. 1).When the diagnosis of mucocele is suspected
clinically, radiology is the most useful investigation.The classical signs are well described by Lloyd.5 Aswell as radiological evidence of an increase in size,which may not have been obvious clinically, theremay also be pacification of the sinus. The charac-teristic scalloped margin of the frontal sinus is oftenlost, and in the ethmoid sinus the typical septatepattern may be eroded. Finally the bony deficit in thesinus wall may become visible.
Successful treatment involves a combined sinusand orbital approach, for it is vital to strip therespiratory epithelium from the wall of the offendingsinus and to re-establish a drainage pathway to thenose in order to prevent recurrence.6 However, ourthree patients with orbital respiratory epitheliumlined cysts had no evidence of a mucocele-or underly-ing sinus disease at the time of presentation, and noevidence of bony dehiscence or destruction wasCorrespondence to Mr C R H James.
found radiologically or at the time of surgery.Effective treatment consisted in excision withoutrecourse to sinus surgery, and there have been no
a.
C.
1~~4
b if
d. at
Fig. 1 Proposedpathogenesis ofpost-traumatic respiratoryepithelium lined cysts in the orbit contrasted with orbitalmucocele development. (a) Normal orbit and nasal sinuses.(b) Frontalsinus mucocele developmentfollowing blockageofthe sinus drainagepathway. (c) Trauma to the sinus regionresults in the transfer ofsinus epithelial cells to the orbitthrough a small dehiscencelfracture ofthe orbital wall, (d)with the subsequent development ofa respiratory epitheliumlined cyst.
387

CRHJames, R Lyness, andJ E Wright
Fig. 2 Case 1. Right eye with massin the superonasal quadrant oftheorbit.
recurrences. We consider that another mechanismmust be invoked to explain the presence of respira-tory epithelium in the orbit.
Case reports
CASE 1A 26-year-old man presented with a faintly blue cysticmass in the superonasal quadrant of his right orbit.At the age of 12 he had received a blow to his facerequiring sutures to a laceration of his right eyebrow.Since then he had noticed a small lump beneath thescar. During the year before he presented the lumphad slowly increased in size (Fig. 2). His visual acuitywas 6/5. There was no proptosis or ocular displace-ment. Orbital and sinus x-rays were normal. Atsurgery a postseptal brown cystic lesion was revealedwhich leaked oily brown fluid as it was being re-moved. Posteromedially there was a thin 'tail' fromthe cyst to the medial wall of the orbit, but no bonydefect was seen. Postoperative recovery was un-complicated.
CASE 2A 23-year-old man presented with a four-year historyof a slowly increasing mass in the superomedialquadrant of his left orbit. Ten years previously he hadreceived a blow to the left brow requiring sutures.The visual acuity was 6/6, and the left eye wasdisplaced inferolaterally but not proptosed. A palp-able cystic lesion was present superomedially. Orbitaland sinus x-ray views were normal. A CT scanshowed an ill defined soft tissue mass in the left orbit(Fig. 3).At surgery a subperiosteal cystic lesion was re-
vealed overlying the ethmoid sinus. It was dissectedfree and found to contain brown oily fluid. There was
no obvious bony defect. The patient made an un-complicated recovery.
CASE 3A 20-year-old man presented with a 10-month historyof a slowly increasing mass in the inferomedialquadrant of his right orbit. Eighteen months pre-viously he had had a right sided maxillary sinuswashout procedure. There had been several episodesof painful increase in size of the mass over the 10months before presentation. The visual acuity was6/6 and the right eye was displaced superolaterallyand proptosed 2 mm. A faintly blue cystic lesion waspresent inferomedially (Fig. 4).
Orbital and sinus x-rays were normal; in particular
Fig. 3 Case2. Axial CTscan with ill-defined soft tissue massmedial to the left eye (arrowed).
388

Respiratory epithelium lined cysts presenting in the orbit without associated mucoceleformation
Fig. 4 Case3. Right eye with massin the lower inner quadrant oftheorbit.
there was no sinus clouding. CT scans revealed a softtissue mass in the right orbit. At surgery a postseptalbrown cystic lesion was revealed. It contained brownoily fluid and there was a thin 'tail' from the cyst to themedial wall, but no bony defect was seen. Post-operative recovery was uncomplicated.
PATHOLOGYThe histopathological examination of the threeorbital lesions showed each to be a thin walledcyst lined by a pseudostratified columnar epi-thelium containing scattered mucin-producing cells(Fig. 5).There was evidence of focal epithelial atrophy,
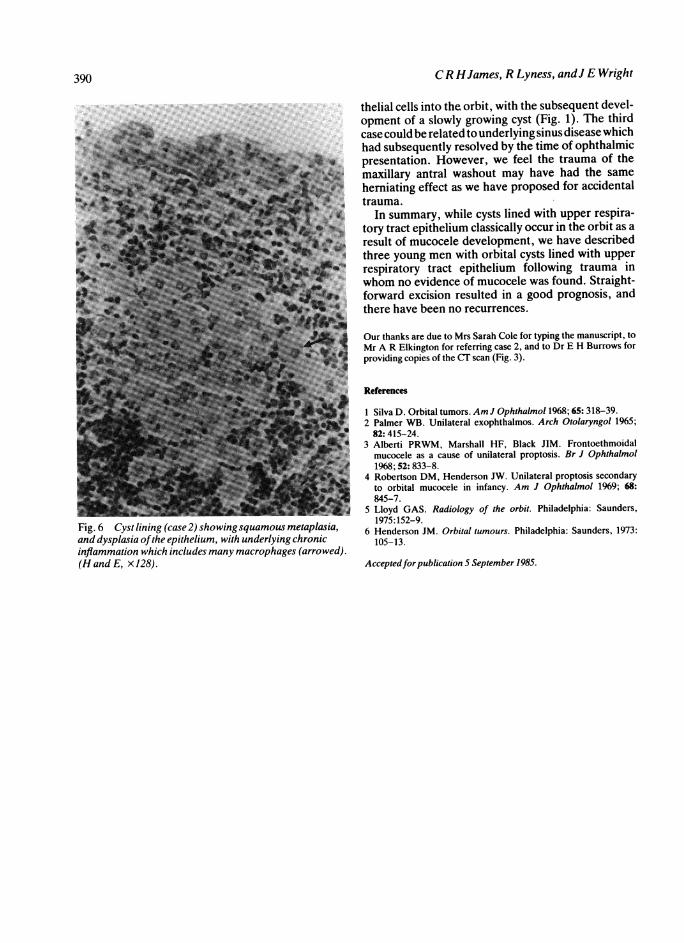
possibly due to pressure effects. In case 2 there weresubepithelial foci of active chronic inflammation,with many macrophages containing lipoid material,indicating a response to leaked cyst contents (Fig. 6).In areas of the epithelium associated with a heavychronic inflammatory response there was metaplasia
of the pseudostratified columnar epithelium tosquamous epithelium. No epidermis or dermal ap-pendages were present within the wall of any of thesecysts, ruling out a diagnosis of dermal inclusion cystor dermoid.
Discussion
The preoperative differential diagnosis in our firsttwo cases included orbital varices or an implantationcyst, and we were surprised to find cysts lined byupper respiratory tract epithelium in the absence ofan underlying mucocele. However, the characteristicclinical picture of a young man presenting with a post-traumatic, faintly blue cystic lesion lying in themedial orbit, with normal orbital x-rays, enabled usprovisionally to diagnose our third case pre-operatively. In the two cases preceded by trauma tothe region our hypothesis is that a tiny fracture ordehiscence allowed herniation of nasal sinus epi-
1v..Fig. 5 Microscopic appearance ofthe cyst lining casee3, comprisingpseudostratified columnarepithelium with an occasionalmucin-secreting goblet cell (arrow)(HandE, x122).
389
CR HJames, R Lyness, andJ E Wright
Fig. 6 Cyst lining (case 2) showingsquamous metaplasia,and dysplasia ofthe epithelium, with underlying chronicinflammation which includes many macrophages (arrowed).(H and E, xJ28).
thelial cells into the orbit, with the subsequent devel-opment of a slowly growing cyst (Fig. 1). The thirdcase could be related to underlying sinus disease whichhad subsequently resolved by the time of ophthalmicpresentation. However, we feel the trauma of themaxillary antral washout may have had the sameherniating effect as we have proposed for accidentaltrauma.
In summary, while cysts lined with upper respira-tory tract epithelium classically occur in the orbit as aresult of mucocele development, we have describedthree young men with orbital cysts lined with upperrespiratory tract epithelium following trauma inwhom no evidence of mucocele was found. Straight-forward excision resulted in a good prognosis, andthere have been no recurrences.
Our thanks are due to Mrs Sarah Cole for typing the manuscript, toMr A R Elkington for referring case 2, and to Dr E H Burrows forproviding copies of the CT scan (Fig. 3).
References
1 Silva D. Orbital tumors. Am J Ophthalmol 1968; 65: 318-39.2 Palmer WB. Unilateral exophthalmos. Arch Otolaryngol 1965;82:415-24.
3 Alberti PRWM, Marshall HF, Black JIM. Frontoethmoidalmucocele as a cause of unilateral proptosis. Br J Ophthalmol1968; 52: 833-8.
4 Robertson DM, Henderson JW. Unilateral proptosis secondaryto orbital mucocele in infancy. Am J Ophthalmol 1969; 68:845-7.
5 Lloyd GAS. Radiology of the orbit. Philadelphia: Saunders,1975:152-9.
6 Henderson JM. Orbital tumours. Philadelphia: Saunders, 1973:105-13.
Acceptedfor publication 5 September 1985.
390