resistance to beta-lactams in enterobacteriaceae ... · spm, sim cephs inhib-r pens cephs inhib-s...
TRANSCRIPT

1
Resistance to beta-lactams in Enterobacteriaceae:
mechanisms and detection
Y. Glupczynski
National Reference Center for Antimicrobial Resistance of
Gram-negative bacteria, CHU Mont-Godinne-UCL, 5530 Yvoir
Classification
Extended-Spectrum β-Lactamases
(ESBLs)
• OXA
Class DClass A
• SHV
• TEM
mutations
Ser70
What is an ESBL?
Serine ß-lactamases Metallo-enzymes
Group 1 Group 2dGroup 2 Group 3
AmpC TEM/SHVCTX-M, Others
OXA IMP,VIM, GIM,SPM, SIM
CephsInhib-R
Pens CephsInhib-S
Pens (Oxa++)Inhib-R/S
CarbapenemsInhib-R
K Bush, curr. Opin. Invest. Drugs 3-1284 (2002)
ESBLs
Plasmid encoded
R to all ß-lactams, except temocillin, (cephamycins),
carbapenems
inhibited by clavulanic acid
Evolution of extended-spectrumβ-lactamases (ESBLs)
Activity vsoxyimino cephs(3rd Gen Cephs)
TEM-11964
TEM-21970
Gln39→→→→Lys
TEM-31987
Gln39→→→→Lys Glu104→→→→Lys Gly238→→→→Ser
First ESBL
Epidemiology of ESBLs
Pre –2000
Mostly Klebsiella spp. with TEM/SHV
Nosocomial, often ICU / specialist units
1998: c. 25% of Klebs from European ICUs ESBL+
Few epidemic strains - e.g K. pneumoniae K25 SHV-4 in France & Belgium
Occasional local outbreaks in Belgian hospitals(Brussels, Gent, Leuven)
c. 5-15% of Klebsiella spp.; 40-60% E. aerogenes;
<2% E. coli
Plasmid encoded
1983 SHV-type (>130)
1985 TEM-type (> 180)
1989 CTX-M-type (> 100)
1988 SFO-1 Serratia FOnticola
1991 TLA-1 TLAhuicas (indian tribe)
1991 PER (7) Pseudomonas Extended Resistance
1996 VEB (7) Vietnam Extended-spectrum ß-lactamase
1996 BES-1 Brazilian Extended-Spectrum ß-lactamase
1998 GES (16) Guyana Extended-Spectrum ß-lactamases
2005 BEL (2) Belgium Extended-spectrum ß-Lactamase
2005 TLA-2 ???? (Plasmid, waste water)
1998 KPC (10) Klebsiella pneumoniae Carbapenemase
1991 OXA-ESBL (18) (OXA-2, -10, -13 derivatives, OXA-18, OXA-45)
ß-lactamases (>600) > 50% ESBLs
“The oldies”
“ESBLs of growing importance”
“infrequent
ESBLs”
“peculiar
ESBLs”
� http://www.lahey.org/studies/webt.asp
� Naas et al., 2008, CMI, Suppl 1:42-52)

2
K. georgiana- related
K. ascorbata- related
CTX-M ββββ-lactamases
- Cefotaximases rather than ceftazidimases
- Predominant ESBLs in Argentina since 1990
- Disseminating worldwide since 2000’s
>100 types, 5 clusters: evolved via escape
of chromosomal β-lactamase genes from Kluyvera spp.
ESBLs in the 21st Century
Major shift from TEM/SHV to CTX-M
Often in E. coli; (variable degree of clonality)
Often in community patients with no/little HC contact
Deaths; high attributable mortality
CTX-M Producers often multi-resistant (quinolones, cotrimox, AGs);
-> major driver of carbapenem use
Epidemiology of CTX-M β-Lactamases Transmission
bla genes mobilized from chromosomes to plasmids:
• transposases, insertion sequences, integrases involved
• blaCTX-M mobilizes 10x more frequently than blaSHV & blaTEM
Horizontal & vertical transmission of plasmids:
• Horizontal transmission: plasmid-mediated conjugation
• Vertical transmission: clonal transmission by normal cell division
ESBL transmission
Diversity of Mobiles Genetic Elements (MGE)
carrying ESBL genes
Smet A et al. FEMS Microbiol Rev 2009
Transposon
blaTEM-144
IR IR
blaSHV-5 IS26IS26
Specific IS (ISEcp1), Complex integrons (ISCR1)
Phage related elements
blaCTX-M-15ISEcp1/tnpA
blaCTX-M-14ISCR1
blaCTX-M-10
blaTEM-52
Tn3
Tn2
Insertion sequence
TEM
SHV
CTX-M
ESBL transmissionESBL transmission routes

3
Classification
Extended-Spectrum β-Lactamases
(ESBLs)
• OXA
Class DClass A
• SHV
• TEM
mutations
Ser70
Carbapenemases
Rising threat of multi-drug antibiotic resistance
Back to the pre-antibiotic era
PLASMID-ENCODED CLASS A
KPC ENZYMES: KLEBSIELLA PNEUMONIAE CARBAPENEMASE
Located on large plasmids;
• conjugative and nonconjugative
blaKPC is usually identified within a Tn3-type transposon (Tn4001).
blaKPC reported on plasmids with:
• Normal spectrum b-lactamases
• Extended spectrum b-lactamases
• Aminoglycoside resistance
GENETIC APPARATUS OF TRANSFERABLE MBLs
Plasmids, integrons and transposons
carbapenemase-produing Enterobacteriaceae isolates
Escherichia coli Klebsiella pneumoniae
Increased mortality with Infections caused by KPC producers
• A high invasive-device score was a predictor of IRE isolation (P 0.02).
• The mortality in the IRE group was 33%, compared to 9% among controls (P 0.043)
• Delay in effective therapy did not affect the in-hospital mortality but was found to increase the length of hospitalization among survivors (34+/-3.2 days versus 26.5 +/-5.4 days; P 00.2)
Why are carbas in the top chart of ß-lactamases?
•Case patients were more likely than control patients to �die during hospitalization (48% vs 20%; P < .001) �die from infection (38% vs 12%; P < .001).
• The timely administration of antibiotics with in vitro activity against CR-KP was not associated with patient survival.

4
KPC: Klebsiella Pneumoniae Carbapenemase
Source: Patrice Nordmann, Thierry Naas, and Laurent Poirel . Global Spread of Carbapenemase producing
Enterobacteriaceae. Emerging Infectious Diseases , October 2011: Vol. 17, No. 10, pp. 1791-1798.
Mortality rate:
> 50%
VIM: Verona Integron–encoded Metallo-β-lactamase
Source: Patrice Nordmann, Thierry Naas, and Laurent Poirel . Global Spread of Carbapenemase producing
Enterobacteriaceae. Emerging Infectious Diseases , October 2011: Vol. 17, No. 10, pp. 1791-1798.
Mortality rate:
18-62%
NDM: New-Delhi Metallo-β-lactamase
Source: Patrice Nordmann, Thierry Naas, and Laurent Poirel . Global Spread of Carbapenemase producing
Enterobacteriaceae. Emerging Infectious Diseases , October 2011: Vol. 17, No. 10, pp. 1791-1798.
Balkan countries, Middle east
Indian subcontinent
North Africa
OXA-48 : OXAcillinase
Source: Patrice Nordmann, Thierry Naas, and Laurent Poirel . Global Spread of Carbapenemase producing
Enterobacteriaceae. Emerging Infectious Diseases , October 2011: Vol. 17, No. 10, pp. 1791-1798.
Evolution of the distribution of resistance mechanisms of carbapenemase-
producing Enterobacteriaceae isolates, National Reference Centre, Belgium,
January 2007–October 2011 (n=80)
0
5
10
15
20
25
30
35
40
45
50
2007 2008 2009 2010 2011 oct
Year
Nu
mb
er
of
CP
E i
so
late
s O XA -48
K P C -2
NDM-1
V IM-2
V IM-1
x3
x3
x3
The rule of 3… as rule of thumb
With courtesy from T-D. Huang
Geographical origin (by country of cross-border transfer) and type
of carbapenemase-encoding genes detected in patients carrying
carbapenemase-producing Enterobacteriaceae,
Belgium, January 2007–October 2011 (n=73)
Patients Carbapenemase
Country /
Region VIM-1 VIM-2 NDM-1 KPC-2 OXA-48
VIM-1
and
KPC-2 Total
No travel
abroad 11 1 4 35 51
Greece 3 6 1 10
Italy 1 3 4
Morocco 3 3
Iraq 1 1
Kosovo 1 1
Montenegro 1 1
England 1 1
Pakistan 1 1
Total 16 1 3 13 39 1 73
5
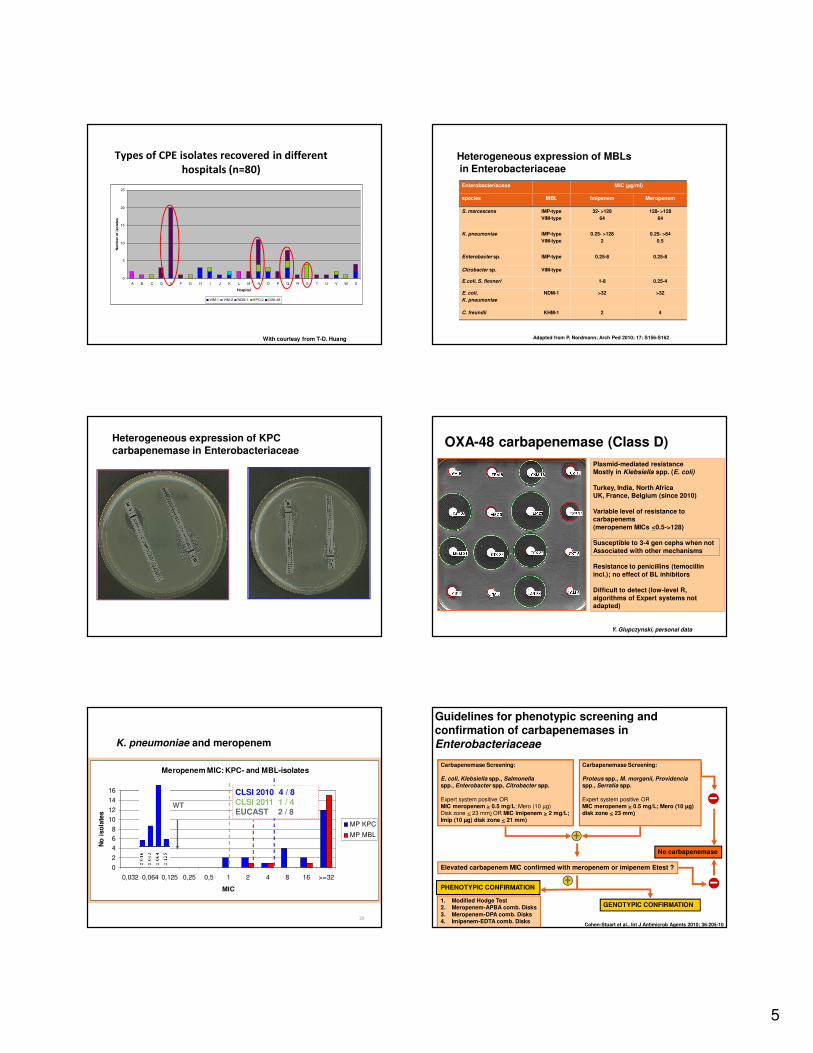
Types of CPE isolates recovered in different
hospitals (n=80)
0
5
10
15
20
25
A B C D E F G H I J K L M N O P Q R S T U V W X
Hospital
Nu
mb
er
of
iso
late
s
VIM-1 VIM-2 NDM-1 KPC-2 OXA-48
With courtesy from T-D. Huang
Heterogeneous expression of MBLs
in Enterobacteriaceae
Enterobacteriaceae MIC (µg/ml)
species MBL Imipenem Meropenem
S. marcescens IMP-type
VIM-type
32- >128
64
128- >128
64
K. pneumoniae IMP-type
VIM-type
0.25- >128
2
0.25- >64
0.5
Enterobacter sp. IMP-type 0.25-8 0.25-8
Citrobacter sp. VIM-type
E.coli, S. flexneri 1-8 0.25-4
E. coli,
K. pneumoniae
NDM-1 >32 >32
C. freundii KHM-1 2 4
Adapted from P. Nordmann; Arch Ped 2010; 17: S156-S162
Heterogeneous expression of KPC
carbapenemase in EnterobacteriaceaeOXA-48 carbapenemase (Class D)
Plasmid-mediated resistance Mostly in Klebsiella spp. (E. coli)
Turkey, India, North AfricaUK, France, Belgium (since 2010)
Variable level of resistance to carbapenems
(meropenem MICs <0.5->128)
Susceptible to 3-4 gen cephs when not
Associated with other mechanisms
Resistance to penicillins (temocillin
incl.); no effect of BL inhibitors
Difficult to detect (low-level R,
algorithms of Expert systems not adapted)
Y. Glupczynski, personal data
29
Meropenem MIC: KPC- and MBL-isolates
0
2
4
6
8
10
12
14
16
0,032 0,064 0,125 0,25 0,5 1 2 4 8 16 >=32
MIC
No
iso
late
s
MP KPC
MP MBL
WT
K. pneumoniae and meropenem
CLSI 2010 4 / 8
CLSI 2011 1 / 4EUCAST 2 / 8
PHENOTYPIC CONFIRMATION
1. Modified Hodge Test2. Meropenem-APBA comb. Disks
3. Meropenem-DPA comb. Disks4. Imipenem-EDTA comb. Disks
Guidelines for phenotypic screening and confirmation of carbapenemases in
Enterobacteriaceae
Carbapenemase Screening:
E. coli, Klebsiella spp., Salmonellaspp., Enterobacter spp, Citrobacter spp.
Expert system positive ORMIC meropenem > 0.5 mg/L; Mero (10 µg)Disk zone < 23 mm) OR MIC imipenem > 2 mg/L;Imip (10 µg) disk zone < 21 mm)
No carbapenemase
Elevated carbapenem MIC confirmed with meropenem or imipenem Etest ?
GENOTYPIC CONFIRMATION
Cohen-Stuart et al., Int J Antimicrob Agents 2010; 36:205-10
Carbapenemase Screening:
Proteus spp., M. morganii, Providenciaspp., Serratia spp.
Expert system positive ORMIC meropenem > 0.5 mg/L; Mero (10 µg) disk zone < 23 mm)

6
K. pneumoniae KPC-positive (class A
carbapenemase)
IMI+DPA IMI IMI+EDTAMERO + APBA
MERO+DPA MERO MERO+CLMERO+EDTA
MEROMERO +DPA MERO +CL
MERO +BOR
ERTAIMI IMI + EDTA
KPC-2
With courtesy from TD Huang
DDST for detection of MBLs
IMI IMI + EDTA
EDTA (420 µg)
1.
2.
NDM-1
Detection of asymptomatic carriage of carbapenemase in the gut flora
From rectal swabs (stools)
Chromogenic selective culture media- Chrom ID BLSE (cefpodoxime)
- CHROMagar KPC (Carbapenem)- Brilliance CRE (Oxoid) (Carbapenem)
- ChromID CARBA (bioMérieux) (Carbapenem)
- MAC+ IMI (1 mg/L)- MAC + 10-µg disks (ERTA/MERO/IMP)
Limit of sensitivity of detection (102 to 103)
(Chrom ID BLSE > CHROMagar KPC)
Enrichment broth culture not superior to direct plating
CHROMagar KPC(carbapenemase producers)
Gold standard: molecular biology +++
Multiplex PCR; IMP, VIM, KPC, OXA-48, NDM….
NDM-1, KPC, AmpC and ESBL Check-MDR CT101*
NDM-1 KPC, OXA-48, VIM, IMP and ESBL Check-MDR CT102*
Molecular confirmatory tests
(Naas et al. AAC, 2010; JCM, 2011)
Spectrophotometric assays for Carbapenem-hydrolysis +++
Rapid Molecular detection tools
ß-lactamases (>600) > 50% ESBLs
SHV-type (> 150), TEM-type (> 190), CTX-M-type (> 100)
TLA-1, PER (7) , VEB (7), BES-1, GES (17), BEL (3), TLA-2, KPC (10), OXA-ESBL
PCR and sequencing•The gold standard• Can detect all variants• Easy to perform but labor intensive and costly
� PCR, Multiplex-PCR, Real-time PCR (Sybr green, Taqman, Hybridization probes), Real time
PCR coupled with pyrosequencing, PCR-ESI (Maldi)….⇒ Only seeked genes can be found ⇒ Only detection of DNA (not expressed genes)
⇒ Requires isolation of the strain for identification and susceptibility testing⇒ Most of the presently used assays are confirmative tests (on cultures)
detection-ligation
PCR
Hybridisation
detection

7
Array: summary
DNA
extraction
1 h
Identification
Amplification
3 h
Detection
2 h
Results
on line
Hands on time:- 3 samples: 1 h
-15 samples: 1 ½ h- 72 samples: 2 ½ h
72 samples/day, cost effective run: minimum 3 samples Patient transferred from Montenegro –
Colonization (resp.) – Clinical outcome: curedPatient transferred from Pakistan –Wound infection – Clinical outcome: deceased
Example: 2 patients in western Europe with pan-drug resistant Enterobacteriaceae isolates
Escherichia coli Klebsiella pneumoniae
Case: 2 Patients in western Europe
K.pneumoniae from
wound infection
(NDM-1; SHV-12; CTX-M-1 gr)
E.coli from faeces
(NDM-1; CMY-2 like
like; CTX-M-1 gr)
NDM-1
CTX-M- group1
SHV-12
CMY-2 like
Combination of resistance mechanisms detected in single experiment
Distinction between TEM/SHV ESBLs or non ESBLsCourtesy from W. de Levita
Result ESBL - KPC Array:
Naas et al. AAC 2010
Evaluate novel molecular assays
Molecular test based on micro-array (results in < 7 h)
Identification of ESBLs
• of TEM and SHV type
• non-ESBL TEM and SHV type
• CTX-M type
Identification of KPC
and KPC, OXA-48, NDM, VIM, IMP
and KPC, NDM, CMY-1, CMY-2, ACT, ACC, DHA, FOX
and KPC, OXA48, NDM, VIM, IMP, CMY-1 /-2, ACT, ACC, DHA, FOX
Cohen S, JAC, 2010
Naas, AAC, 2010Endimiani, JCM, 2010
Naas, JCM, 2011
Bogaerts, AAC
Multiplex end-point PCR assays
Genotypic detection of carbapenemase-encoding genes and other important β-lactamases (ESBLs, AmpC, OXA…)
Multiple protocols (3-7 sets, 11-25 target genes)
Design of specific group of primers
• Definition of different reaction mixtures
• Optimization of PCR conditions (one single amplification protocol)
• Distinct amplicon sizes for the different genes
Rapid (<4 h), reliable (specific)
Screening of clinical isolates, epidemiological surveys
Customizable to local needs (endemic/non endemic settings)
Lower costs (Vs multiple PCR assays)
Dalenne et al., JAC 2010Poirel et al., Diag. Microb. Infect Dis 2011Voets et al. IJAA 2011

8
Diag Microbiol Infect Dis 2011; 70: 119-123
Rapid (<4 h), reliable (specific)Screening of clinical isolates, epidemiological surveysCustomizable to local needs
(endemic/non endemic settings)Lower costs (Vs multiple PCR assays
Real-time Multiplex PCRDesign of specific primers and fluorescent probes (TaqMan)
Rapid (<2 h), one amplification reaction in single tube
Less prone to contamination (closed system, no tube opening)
Different ways for identification of amplicons
− Real-time probe-based PCR
− Amplicon melt-curve analysis (intercalating dye – LCGreen)
− Capillary electrophoresis of amplicons (QIAxcel –QIAGEN)
− DNA sequencing of amplicons (confirmation, identification of specific alleles –e.g: GES 170 Gly-Ser with carbapenemase activity)
Would allow more rapid guidance of antibiotic treatment and infection control measures
Swayne et al., IJAA 2011
Real time pentaplex PCR
Melt-curve analysis
of amplicons - LCGreenCapillary electrophoresis
of amplicons
Cycles
A
Fluor
esc
enc
e
106 105 104 103 102 101 100
No NDM-bacteria
B
Fluor
esc
enc
e
Cycles
106 105 104 103
102
101
No spiked NDM-bacteria
NDM-1-qPCRA: Serially diluted Kp NDM-1 in 108 E. coli WT
B: Serially diluted Kp NDM-1 in stool
Number of Kp NDM-1 in PCR tube
Number of Kp NDM-1 / 100 mg of stool
T Naas*, A Ergani, A Carrer, and P Nordmann, AAC 2011
Isolate
#
Bacteria MIC
(µg/ml)
Lowest limit of
detection in water
(CFU/ml)
Lowest limit of detection in
stool (CFU/ml of stool)a
Lowest detection limit of NDM-1
qPCR
IMPa ChromID
ESBL
CHROMag
ar KPC
ChromID
ESBL
CHROMagar
KPC
(CFU/ml of
stoola)
(DNA copies/ml
of stoolb)
23 K. pneumoniae A >32 1 x 101 1 x 10
1 2 x 10
1 1 x 10
2 10
1 1 x 10
2
24 K. pneumoniae B >32 2 x 101 1 x 10
1 2 x 10
1 5 x 10
1 2 x 10
1 2x 10
2
25 K. pneumoniae D >32 3 x 101 2 x 10
1 2 x 10
1 2 x 10
1 10
1 4 x 10
2
26 K. pneumoniae F >32 1 x 101 2 x 10
1 1 x 10
1 2 x 10
1 2 x 10
1 2 x 10
2
27 K. pneumoniae G 2 2 x 101 3 x 10
2 1 x 10
2 4 x 10
3 10
1 2 x 10
2
28 K. pneumoniae I >32 1 x 101 3 x 10
1 2 x 10
1 6 x 10
1 10
1 6 x 10
2
29 C. freundii A >32 1 x 101 1 x 10
1 1 x 10
1 1 x 10
1 3 x 10
1 6 x 10
2
30 E. coli A 6 2 x 101 4 x 10
1 2 x 10
1 3 x 10
2 10
1 2 x 10
2
31 E. coli B 3 1 x 101 2 x 10
3 1 x 10
1 3 x 10
3 10
1 2 x 10
2
32 E. cloacae A 8 4 x 101 3 x 10
2 2 x 10
1 8 x 10
1 3 x 10
1 10
3
Real-Time PCR for Detection of
NDM-1-carbapenemase genes from Stools
T Naas*, A Ergani, A Carrer, and P Nordmann (submitted AAC)
Real-Time PCR for Detection of
NDM-1-carbapenemase genes from Stools
Highly specific and sentitive qPCR (limit of detection +/-101 bacteria /
100 mg of stool=> use of enrichment culture (increased detection?)
Useful tool for outbreak management (rapid cohorting of patients, infection control measure evaluation, ….)
At least as sensitive as culture on stool samples, but 4h turn around time vs 48h-72h for culture
Needs to be evaluated on rectal swabs &/ in outbreak situationExtraction can be automated (less hands on time)

9
Multiplex PCR-ELISA
Direct Screening for MRSA / ESBL / VRE from 1 swab!Enrichment by culture is not necessary!Economical test system for 1 to 94 samples per run Simple test performance; Automation possible hyplex® TAT: 2-4 hoursReliable, secure, fast
1. DNA extraction2. Multiplex PCR3. Reverse hybridization of PCR products
to specific capture oligonucleotide probes
4. Detection of hybridization complex by peroxidaseconjugated antibody
Results in less than 2 hours!
hyplex® (Multiplex-PCR-ELISA)
Multiplex PCR-ELISA Evaluation of hyplex® MBL ID Multiplex PCR-ELISA(AmplexDiagnostics)
Avlami et al., J Microbiol Methods 2010; 83: 185-187
Clinical specimens (n) MBL-producers (n) Hyplex (+)
TP TN FP FN Sens (%)
Spec (%)
PPV (%)
NPV (%)
Blood (n=90) P. aeruginosa (8)K. pneumoniae (9)P. stuartii (1)E. aerogenes (1)
19 19 71 0 0 100 100 100 100
Other specimens (n=236)- Urine (60)- Bronchial/sputum (n=85)
P. aeruginosa (2)K. pneumoniae (3)P.aeruginosa (26)A. baumannii (6)K. pneumoniae (6)P. stuartii (2)
58742
53540
1775343
522
100
98 97 91 99
- Wound/Pus (n=91) P. aeruginosa (6)K. pneumoniae (2)E. aerogenes (1)
9 8 81 1 1
Total (n=326) 77 72 248 5 1 98.6 98 93.5 99.5
Identification of MBL (VIM/IMP) genes directly from clinical specimens326 samples, 3 hospitals (Athens)
73 VIM + (22.4%); no IMP found
Timely, reliable detection of MBL-producers
Need for multicentric studies (lower prevalence settings, IMP-positive organisms)
Conclusions
The epidemiology of carbapenemase (sources of acquisition, risk
factors, real prevalence/incidence) is poorly known and most
probably largely underestimated because of difficulties in their detection. It is obvious that carbapenemase–producing organisms
are distributed worldwide and their prevalence is increasing
•This rapid spread of carbapenemases will be a major heathcare issue for the next decades
•The « fight » against MDR carbapenemase-producing bugs, will require:
•Fast detection and identification of the reservoirs
•Reduced (appropriate) consumption of antimicrobials
•Strict adherence to standard hygiene practice
Acknowledgments
CHU Mont Godinne (UCL)
National Reference Laboratory
- Daniel Huang
- Alexia Verroken
- Pierre Bogaerts
- Caroline Bauraing
- Catherine Berhin
- Roberta Rezende de Castro
- Warda Boucharhouf
- Amélie Guisset
- Farid El Garch
Hôpital ULB-Erasme
Associated Ref. laboratory
- Ariane Deplano
- Sandrine Roisin
- Claire Nonhoff
- Ricardo De Mendonca
- Marie Hallin
- Olivier Denis
Institute of Public Health
- Bea Jans
- Boudewijn Catry
- Sophie Quoilin
MONT-
GODINNE