research article changes in cerebrospinal fluid...
TRANSCRIPT

Research ArticleChanges in Cerebrospinal Fluid Biomarkers in HumanHerpesvirus-6-Associated Acute EncephalopathyFebrile Seizures
Naoyuki Tanuma12 Rie Miyata2 Keisuke Nakajima2 Akihisa Okumura3 Masaya Kubota4
Shin-ichiro Hamano5 and Masaharu Hayashi2
1 Department of Pediatrics Tokyo Metropolitan Fuchu Medical Center for the Disabled 2-9-2 Musashidai FuchuTokyo 183-8553 Japan
2Department of Brain Development and Neural Regeneration Tokyo Metropolitan Institute of Medical ScienceTokyo 156-8506 Japan
3Department of Pediatrics School of Medicine Juntendo University Tokyo 113-8421 Japan4Department of Neurology National Center for Child Health and Development Tokyo 157-8535 Japan5Division of Neurology Saitama Childrenrsquos Medical Center Saitama 339-8551 Japan
Correspondence should be addressed to Naoyuki Tanuma naoyuki tanumamembermetrotokyojp
Received 20 June 2014 Revised 2 September 2014 Accepted 3 September 2014 Published 11 September 2014
Academic Editor Yung-Hsiang Chen
Copyright copy 2014 Naoyuki Tanuma et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
To determine the involvement of oxidative stress in the pathogenesis of acute encephalopathy associated with human herpesvirus-6(HHV-6) infection we measured the levels of oxidative stress markers 8-hydroxy-21015840-deoxyguanosine (8-OHdG) and hexanoyl-lysine adduct (HEL) tau protein and cytokines in cerebrospinal fluid (CSF) obtained from patients with HHV-6-associated acuteencephalopathy (HHV-6 encephalopathy) (119899 = 16) and complex febrile seizures associated with HHV-6 (HHV-6 complex FS)(119899 = 10) We also examined changes in CSF-8OHdG and CSF-HEL levels in patients with HHV-6 encephalopathy before and aftertreatment with edaravone a free radical scavenger CSF-8-OHdG levels in HHV-6 encephalopathy and HHV-6 complex FS weresignificantly higher than in control subjects In contrast CSF-HEL levels showed no significant difference between groups Thelevels of total tau protein in HHV-6 encephalopathy were significantly higher than in control subjects In six patients with HHV-6infection (5 encephalopathy and 1 febrile seizure) the CSF-8-OHdG levels of five patients decreased after edaravone treatment Ourresults suggest that oxidative DNA damage is involved in acute encephalopathy associated with HHV-6 infection
1 Introduction
Viral infection-associated acute encephalopathyencephalitisis a serious complication with neurological sequelae Themain symptoms of the acute phase are impaired conscious-ness and convulsive status epilepticuswith hyperpyrexia Sev-eral subtypes of acute encephalopathy have been establishedbased on clinical radiologic and laboratory findings Acuteencephalopathy with biphasic seizures and late reduced dif-fusion (AESD) is a new subtype characterized by a prolongedfebrile seizure (FS) on day 1 which usually lasts longer than30min as the initial neurological symptom [1 2] The initialseizures are followed by secondary seizures most often acluster of complex partial seizures on days 4ndash6 Magneticresonance imaging (MRI) shows no acute abnormalities
until day 1 or 2 but reveals reduced subcortical diffusionfrom day 3 onwards Hoshino et al reported that AESDwas the most frequent syndrome in a nationwide surveyon the epidemiology of acute encephalopathy in Japan andthat human herpesvirus-6 (HHV-6) was the most commonpreceding pathogenic infection in AESD [3] Recent studiesdemonstrated three potential major pathomechanisms ofviral associated encephalopathy metabolic error cytokinestorm and excitotoxicity [4] However the exact pathogen-esis remains unknown
Oxidative stress originates from an imbalance betweenthe production of reactive oxygen species (ROS) and toa lesser extent reactive nitrogen species (RNS) and theantioxidant capacities of cells and organs [5] Recently
Hindawi Publishing CorporationMediators of InflammationVolume 2014 Article ID 564091 8 pageshttpdxdoiorg1011552014564091
2 Mediators of Inflammation
oxidative stress was confirmed to play a role in adult-onset neurodegenerative diseases such asAlzheimerrsquos diseaseParkinsonrsquos disease and amyotrophic lateral sclerosis [6 7]We confirmed the involvement of oxidative neuronal damagein child-onset neurodegenerative diseases such as subacutesclerosing panencephalitis [8] xeroderma pigmentosum [9]Cockayne syndrome [10] and spinal muscular atrophy [11]
In the present study we measured the levels of oxidativestress markers (8-hydroxy-21015840-deoxyguanosine 8-OHdG andhexanoyl-lysine adduct HEL) tau protein and cytokines incerebrospinal fluid (CSF) obtained from patients with HHV-6-associated encephalopathy and complex FS associated withHHV-6 infection
2 Patients and Methods
21 Patients We analyzed CSF obtained in the acute phaseof inpatients with HHV-6-associated encephalopathy (HHV-6 encephalopathy) (119899 = 16) and complex FS associatedwith HHV-6 (HHV-6 complex FS) (119899 = 10) during theperiod from 2008 to 2010 Laboratory diagnoses of HHV-6 infection were based on a virus-specific polymerase chainreaction (PCR) assay or detection of virus-specific antibod-ies Diagnosis of acute encephalopathy or complex FS wasperformed by the attending physician and later confirmed byexamination of available clinicoradiological information Allcases of HHV-6-associated encephalopathy were diagnosedbased on the clinical course and MRI findings The complexFS group consisted of children who presented with fever andseizure butwere later found to be free fromacute neurologicaldamage based on the clinical course laboratory data andbrain imaging Another 16 children (15with fever but not cen-tral nervous system infection and 1 with hypoglycemia) werealso enrolled as control subjects Parent consent was obtainedin all subjects in accordance with the Helsinki Declarationand all protocols were approved by the institutional ethicscommittee of the Tokyo Metropolitan Fuchu Medical Centerfor the Disabled
22 Sample Collection and Measurement of CSF BiomarkersCSF samples were obtained from each patient at any pointduring the disease and immediately stored atminus80∘Cuntil theywere analyzed The amount of DNA oxidative stress marker8-hydroxy-21015840-deoxyguanosine (8-OHdG) and the early stagelipid peroxidation marker hexanoyl-lysine adduct (HEL)was examined using commercially available enzyme-linkedimmunosorbent assay (ELISA) kits (Japan Institute for theAging Shizuoka Japan) Total tau protein was determinedusing sandwich ELISA (Invitrogen Corporation CamarilloCA) The levels of cytokines were evaluated by multiplexbead-based immunoassay (BioPlex 200 system) (Bio-RadLaboratories Inc Hercules CA) All assays were carried outaccording to themanufacturerrsquos protocolsThedetection limitfor each ELISA kit was 006 ngmL (8-OHdG) 26 ngmL(HEL) and 15 pgmL (total tau protein)
23 Edaravone Treatment Edaravone (3-methyl-1-phenyl-2-pyrazolin-5-one) is a free radical scavenging drug that
is clinically used in Japan for treatment of acute ischemicstroke [12 13] Several studies have shown that edaravonehas preventive effects on brain injury following ischemiaand reperfusion in patients with brain attack [14 15] Basedon these observations six patients with HHV-6 infection(5 patients with encephalopathy and 1 patient with complexFS) received free radical scavenger edaravone treatment inaddition to conventional therapy for acute encephalopathyA standard treatment protocol is edaravone 05mgkg every12 hours (1mgkg daily) intravenously for 7ndash12 days Parentconsent was obtained in all patients before the treatment
24 Statistical Analysis Data were analyzed by GraphPadPrism version 50 Differences in oxidative stress markerstau protein and cytokine levels among each group wereanalyzed by one-way analysis of variance (ANOVA) andDunnrsquos multiple comparison test Correlations between CSF-8OHdG and other biomarkers were evaluated using Spear-manrsquos rank correlation coefficient We used Fisherrsquos exacttest to examine the relationship between increased levels ofeach biomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy Comparisons of levels ofCSF biomarkers before and after edaravone treatment wereperformed by paired 119905-test A 119875 value of less than 005 wasconsidered statistically significant
3 Results
31 Study Population and Clinical Features The characteris-tics of the patients included in the study are summarized inTable 1 There were no significant differences of age amongeach group Thirteen of 16 patients (813) with HHV-6encephalopathy were AESD and only five patients (313)recovered without sequelae from HHV-6 encephalopathy Incontrast all patients with complex FS associated with HHV-6infection were without neurological sequelae
32 Oxidative DNADamage and Lipid Peroxidation inHHV-6Encephalopathy and Complex FS TheCSF-8-OHdG levels inHHV-6 encephalopathy (0129plusmn007 ngmLmean plusmn SD119875 lt001) and HHV-6 complex FS (0116 plusmn 0061 ngmL mean plusmnSD 119875 lt 005) patients were significantly higher than in con-trol subjects (0063 plusmn 001 ngmL mean plusmn SD) (Figure 1(a))CSF-HEL levels (mean plusmn SD) in HHV-6 encephalopathyHHV-6 complex FS and control subjects were 359 plusmn187 nmolL 524 plusmn 363 nmolL and 362 plusmn 108 nmolLrespectively There were no significant differences in CSF-HEL levels between all groups (Figure 1(b)) These data aresummarized in Table 2
33 Total Tau Protein Levels in HHV-6 Encephalopathy andComplex FS Total tau protein levels in HHV-6 encephalopa-thy patients (119899 = 16) (13 9056 plusmn 14 2011 pgmL mean plusmnSD)were significantly higher than in control subjects (6090plusmn3420 pgmL mean plusmn SD) (119875 lt 005 Figure 2) Howeverthere were no significant differences in CSF tau protein levelsbetween the HHV-6 encephalopathy group and HHV-6 FSgroup (6547 plusmn 2137 pgmL mean plusmn SD) We then divided
Mediators of Inflammation 3
Table 1 Clinical characteristics of HHV-6 encephalopathy and febrile seizure patients
HHV-6 encephalopathy HHV-6 complex febrile seizures ControlsNumber of patients 16 10 16Age (months) 151 plusmn 54 126 plusmn 39 111 plusmn 108
Sex ratio (M F) 8 8 5 5 11 5Sampling time (day of illness) 1ndash8 1 mdashMRI abnormality 1416 ND NDOutcome (without sequelae) 516 1010 mdashHHV human herpesvirus No number ND not done M male F female MRI magnetic resonance imaging
Con
trol (n=16
)
HH
V-6
com
plex
FS
(n=10
)
HH
V-6
ence
phal
opat
hy(n=16
)
00
01
02
03
04
8-O
HdG
(ng
mL)
lowast
lowastlowast
(a)
Con
trol (n=15
)
HH
V-6
com
plex
FS
(n=7
)
HH
V-6
ence
phal
opat
hy(n=14
)
0
2
4
6
8
10
12
14
HEL
(nm
olL
)
(b)
Figure 1 Cerebrospinal fluid (CSF) levels of oxidative stress markers in HHV-6 encephalopathy HHV-6 complex febrile seizures (FS) andcontrols (a) 8-hydroxy-21015840-deoxyguanosine 8-OHdG (b) hexanoyl-lysine adduct HEL lowast119875 lt 005 lowastlowast119875 lt 001 The horizontal bar indicatesthe mean value of each group CSF-8OHdG levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6 complex FS and controls are 0129 plusmn007 ngmL 0116 plusmn 0061 ngmL and 0063 plusmn 001 ngmL respectively CSF-HEL levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6complex FS and control subjects are 359 plusmn 187 nmolL 524 plusmn 363 nmolL and 362 plusmn 108 nmolL respectively
Table 2 Descriptive statistics for the biomarkers examineda
Biomarkers Controls HHV-6complex FS
HHV-6encephalopathy
119875
GlobalControlsversus
HHV-6 FS
Controls versusHHV-6
encephalopathy
HHV-6 FSversus HHV-6encephalopathy
8-OHdGngmL 0063 (001) 0116 (0061) 0129 (007) 00025 lt005 lt001 ns
HEL nmolL 362 (108) 524 (363) 359 (187) 01863 ns ns nsTau pgmL 6090 (3420) 6547 (2137) 139056 (142011) 00028 ns lt005 nsIL-6 pgmL 32 (30) 58 (53) 746 (1169) 00349 ns lt001 nsIL-10 pgmL 04 (03) 06 (08) 14 (21) 01663 ns ns nsTNF-120572 pgmL 01 (01) 03 (05) 34 (40) 00036 ns lt001 lt0058-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct HHV-6 human herpesvirus-6 FS febrile seizure ns not significant IL interleukinTNF tumor necrosis factoraValues are expressed as the mean (standard deviation)
4 Mediators of Inflammation
Con
trol (n=8
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy to
tal
(n=16
)
HH
V-6
ence
phal
opat
hy d
ays1
-2(n=5
)
HH
V-6
ence
phal
opat
hy d
ays3
ndash8(n=11
)
Tau
(pg
mL)
100
1000
10000
100000
lowast
lowastlowast
lowastlowast
lowastlowast
Figure 2 Cerebrospinal fluid (CSF) tau protein levelsThe horizon-tal bar indicates the mean value of each group CSF levels (meanplusmn SD) of tau protein in HHV-6 encephalopathy HHV-6 complexfebrile seizures (FS) and controls are 13 9056 plusmn 14 2011 pgmL6547plusmn2137 pgmL and 6090plusmn3420 pgmL respectively Total tauprotein levels in HHV-6 encephalopathy patients are significantlyhigher than in control subjects (lowast119875 lt 005) The levels of tau proteinin HHV-6 encephalopathy at days 3ndash8 (19 8569 plusmn 13 1219 pgmL)are significantly higher than those of HHV-6 encephalopathy atdays 1-2 (5204 plusmn 2296 pgmL) HHV-6 complex FS and controls(lowastlowast119875 lt 001)
the HHV-6 encephalopathy group into two groups accordingto sampling time at days 1-2 (119899 = 5) and days 3ndash8 (119899 = 11)respectively Consequently we found that the levels of tauprotein were significantly increased at days 3ndash8 in HHV-6encephalopathy (19 8569 plusmn 13 1219 pgmL mean plusmn SD)compared with those of HHV-6 encephalopathy at days 1-2 (5204 plusmn 2296 pgmL mean plusmn SD) (119875 lt 001) HHV-6complex FS (119875 lt 001) and controls (119875 lt 001) (Figure 2)
34 CSF Cytokine Profile in Acute Encephalopathy and Com-plex FS We next confirmed the elevation of CSF IL-6 andTNF-120572 in patients with HHV-6 encephalopathy (Figure 3)The CSF IL-6 levels in patients with HHV-6 encephalopathy(746 plusmn 1169 pgmL mean plusmn SD) were significantly higherthan in controls (32 plusmn 30 pgmL mean plusmn SD) (119875 lt 001)(Figure 3(a)) The CSF TNF-120572 levels in patients with HHV-6 encephalopathy (34 plusmn 40 pgmL mean plusmn SD) were also
significantly higher than those with complex FS (03 plusmn05 pgmL mean plusmn SD) and in controls (010 plusmn 01 pgmLmean plusmn SD) (119875 lt 005 and 119875 lt 001 resp) (Figure 3(c))In contrast there were no significant differences of CSF IL-10levels among patients with HHV-6 encephalopathy or HHV-6 complex FS and controls (Figure 3(b))
35 Correlation Analysis of CSF Biomarkers in HHV-6Encephalopathy We next examined correlations betweenCSF-8OHdG and other biomarkers in the HHV-6encephalopathy group (Table 3) There was a significantpositive correlation between IL-6 and TNF-120572 (Spearman119903 = 0783 119875 = 00006) However there were no significantcorrelations among other biomarkers In addition therewas no correlation between the increased levels of eachbiomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy (data not shown)
36 Changes in CSF-8-OHdG and CSF-HEL Levels beforeand after Edaravone Treatment in HHV-6-Associated AcuteEncephalopathy and Complex FS Finally we compared theCSF levels of oxidative stress markers in six patients withHHV-6 infection (5 patients with encephalopathy and 1patient with febrile seizures) before and after edaravone treat-ment Clinical profile of patients with edaravone treatmentis shown in Table 4 The mean initiation time of edaravonetreatment was day 48 for the HHV-6 encephalopathy groupOne patient with febrile seizures associated with HHV-6 infection who received edaravone treatment from day1 did not develop encephalopathy and recovered withoutsequelae (patient 6) The CSF-8-OHdG levels decreased afteredaravone treatment (119875 = 00202 paired 119905-test) (Figure 4(a))Regarding the CSF-HEL levels there were no significantdifferences between before and after edaravone treatmentWe also compared the mean CSF levels of other biomarkersbefore and after treatment and observed no significant differ-ences of mean values (data not shown)
4 Discussion
In the present study we demonstrated that CSF-8-OHdGlevels in HHV-6 encephalopathy and HHV-6 complex FSpatients were significantly higher than in controls suggestingincreased oxidative stress is induced by HHV-6 infectionRecent studies revealed that oxidative damage is an emerginggeneral mechanism of nervous system injury caused by viralinfection For example oxidative injury is a component ofacute encephalitis caused by herpes simplex virus type 1(HSV-1) [16] HSV-1 infection of nervous system tissues inmice was associated with the expression of inducible nitricoxide synthase (iNOS) and the release of cytokines includingTNF-120572 from inflammatory cells Thus increased generationof ROS and RNS can be caused by the direct effects ofvirus on cells and the indirect effects of host inflammatoryresponses [17] Regarding HHV-6 infection Fukuda et alreported that urinary 8-OHdG concentrations in a patientwith HHV-6 encephalopathy on the first day of hospital-ization were 15 times higher than the mean concentration
Mediators of Inflammation 5
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)01
1
10
100
1000
IL-6
(pg
mL)
lowastlowast
(a)C
ontro
l (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
01
1
10
IL-10
(pg
mL)
(b)
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
001
01
1
10
100
TNF-120572
(pg
mL)
lowast
lowastlowast
(c)
Figure 3 Cerebrospinal fluid (CSF) cytokine levels The horizontal bar indicates the mean value of each group (a) Levels of CSF IL-6 inpatients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 746plusmn1169 pgmL 58plusmn53 pgmL and 32plusmn30 pgmLrespectively The CSF IL-6 levels in patients with HHV-6 encephalopathy are significantly higher than in controls (lowastlowast119875 lt 001) (b) Levelsof CSF IL-10 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 14 plusmn 21 pgmL 06 plusmn 08 pgmL and04 plusmn 03 pgmL respectively (c) Levels of CSF TNF-120572 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controlsare 34 plusmn 40 pgmL 03 plusmn 05 pgmL and 01 plusmn 01 pgmL respectively The CSF TNF-120572 levels in patients with HHV-6 encephalopathy aresignificantly higher than those with complex FS and in controls (lowast119875 lt 005 and lowastlowast119875 lt 001 resp)
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Mediators of Inflammation
oxidative stress was confirmed to play a role in adult-onset neurodegenerative diseases such asAlzheimerrsquos diseaseParkinsonrsquos disease and amyotrophic lateral sclerosis [6 7]We confirmed the involvement of oxidative neuronal damagein child-onset neurodegenerative diseases such as subacutesclerosing panencephalitis [8] xeroderma pigmentosum [9]Cockayne syndrome [10] and spinal muscular atrophy [11]
In the present study we measured the levels of oxidativestress markers (8-hydroxy-21015840-deoxyguanosine 8-OHdG andhexanoyl-lysine adduct HEL) tau protein and cytokines incerebrospinal fluid (CSF) obtained from patients with HHV-6-associated encephalopathy and complex FS associated withHHV-6 infection
2 Patients and Methods
21 Patients We analyzed CSF obtained in the acute phaseof inpatients with HHV-6-associated encephalopathy (HHV-6 encephalopathy) (119899 = 16) and complex FS associatedwith HHV-6 (HHV-6 complex FS) (119899 = 10) during theperiod from 2008 to 2010 Laboratory diagnoses of HHV-6 infection were based on a virus-specific polymerase chainreaction (PCR) assay or detection of virus-specific antibod-ies Diagnosis of acute encephalopathy or complex FS wasperformed by the attending physician and later confirmed byexamination of available clinicoradiological information Allcases of HHV-6-associated encephalopathy were diagnosedbased on the clinical course and MRI findings The complexFS group consisted of children who presented with fever andseizure butwere later found to be free fromacute neurologicaldamage based on the clinical course laboratory data andbrain imaging Another 16 children (15with fever but not cen-tral nervous system infection and 1 with hypoglycemia) werealso enrolled as control subjects Parent consent was obtainedin all subjects in accordance with the Helsinki Declarationand all protocols were approved by the institutional ethicscommittee of the Tokyo Metropolitan Fuchu Medical Centerfor the Disabled
22 Sample Collection and Measurement of CSF BiomarkersCSF samples were obtained from each patient at any pointduring the disease and immediately stored atminus80∘Cuntil theywere analyzed The amount of DNA oxidative stress marker8-hydroxy-21015840-deoxyguanosine (8-OHdG) and the early stagelipid peroxidation marker hexanoyl-lysine adduct (HEL)was examined using commercially available enzyme-linkedimmunosorbent assay (ELISA) kits (Japan Institute for theAging Shizuoka Japan) Total tau protein was determinedusing sandwich ELISA (Invitrogen Corporation CamarilloCA) The levels of cytokines were evaluated by multiplexbead-based immunoassay (BioPlex 200 system) (Bio-RadLaboratories Inc Hercules CA) All assays were carried outaccording to themanufacturerrsquos protocolsThedetection limitfor each ELISA kit was 006 ngmL (8-OHdG) 26 ngmL(HEL) and 15 pgmL (total tau protein)
23 Edaravone Treatment Edaravone (3-methyl-1-phenyl-2-pyrazolin-5-one) is a free radical scavenging drug that
is clinically used in Japan for treatment of acute ischemicstroke [12 13] Several studies have shown that edaravonehas preventive effects on brain injury following ischemiaand reperfusion in patients with brain attack [14 15] Basedon these observations six patients with HHV-6 infection(5 patients with encephalopathy and 1 patient with complexFS) received free radical scavenger edaravone treatment inaddition to conventional therapy for acute encephalopathyA standard treatment protocol is edaravone 05mgkg every12 hours (1mgkg daily) intravenously for 7ndash12 days Parentconsent was obtained in all patients before the treatment
24 Statistical Analysis Data were analyzed by GraphPadPrism version 50 Differences in oxidative stress markerstau protein and cytokine levels among each group wereanalyzed by one-way analysis of variance (ANOVA) andDunnrsquos multiple comparison test Correlations between CSF-8OHdG and other biomarkers were evaluated using Spear-manrsquos rank correlation coefficient We used Fisherrsquos exacttest to examine the relationship between increased levels ofeach biomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy Comparisons of levels ofCSF biomarkers before and after edaravone treatment wereperformed by paired 119905-test A 119875 value of less than 005 wasconsidered statistically significant
3 Results
31 Study Population and Clinical Features The characteris-tics of the patients included in the study are summarized inTable 1 There were no significant differences of age amongeach group Thirteen of 16 patients (813) with HHV-6encephalopathy were AESD and only five patients (313)recovered without sequelae from HHV-6 encephalopathy Incontrast all patients with complex FS associated with HHV-6infection were without neurological sequelae
32 Oxidative DNADamage and Lipid Peroxidation inHHV-6Encephalopathy and Complex FS TheCSF-8-OHdG levels inHHV-6 encephalopathy (0129plusmn007 ngmLmean plusmn SD119875 lt001) and HHV-6 complex FS (0116 plusmn 0061 ngmL mean plusmnSD 119875 lt 005) patients were significantly higher than in con-trol subjects (0063 plusmn 001 ngmL mean plusmn SD) (Figure 1(a))CSF-HEL levels (mean plusmn SD) in HHV-6 encephalopathyHHV-6 complex FS and control subjects were 359 plusmn187 nmolL 524 plusmn 363 nmolL and 362 plusmn 108 nmolLrespectively There were no significant differences in CSF-HEL levels between all groups (Figure 1(b)) These data aresummarized in Table 2
33 Total Tau Protein Levels in HHV-6 Encephalopathy andComplex FS Total tau protein levels in HHV-6 encephalopa-thy patients (119899 = 16) (13 9056 plusmn 14 2011 pgmL mean plusmnSD)were significantly higher than in control subjects (6090plusmn3420 pgmL mean plusmn SD) (119875 lt 005 Figure 2) Howeverthere were no significant differences in CSF tau protein levelsbetween the HHV-6 encephalopathy group and HHV-6 FSgroup (6547 plusmn 2137 pgmL mean plusmn SD) We then divided
Mediators of Inflammation 3
Table 1 Clinical characteristics of HHV-6 encephalopathy and febrile seizure patients
HHV-6 encephalopathy HHV-6 complex febrile seizures ControlsNumber of patients 16 10 16Age (months) 151 plusmn 54 126 plusmn 39 111 plusmn 108
Sex ratio (M F) 8 8 5 5 11 5Sampling time (day of illness) 1ndash8 1 mdashMRI abnormality 1416 ND NDOutcome (without sequelae) 516 1010 mdashHHV human herpesvirus No number ND not done M male F female MRI magnetic resonance imaging
Con
trol (n=16
)
HH
V-6
com
plex
FS
(n=10
)
HH
V-6
ence
phal
opat
hy(n=16
)
00
01
02
03
04
8-O
HdG
(ng
mL)
lowast
lowastlowast
(a)
Con
trol (n=15
)
HH
V-6
com
plex
FS
(n=7
)
HH
V-6
ence
phal
opat
hy(n=14
)
0
2
4
6
8
10
12
14
HEL
(nm
olL
)
(b)
Figure 1 Cerebrospinal fluid (CSF) levels of oxidative stress markers in HHV-6 encephalopathy HHV-6 complex febrile seizures (FS) andcontrols (a) 8-hydroxy-21015840-deoxyguanosine 8-OHdG (b) hexanoyl-lysine adduct HEL lowast119875 lt 005 lowastlowast119875 lt 001 The horizontal bar indicatesthe mean value of each group CSF-8OHdG levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6 complex FS and controls are 0129 plusmn007 ngmL 0116 plusmn 0061 ngmL and 0063 plusmn 001 ngmL respectively CSF-HEL levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6complex FS and control subjects are 359 plusmn 187 nmolL 524 plusmn 363 nmolL and 362 plusmn 108 nmolL respectively
Table 2 Descriptive statistics for the biomarkers examineda
Biomarkers Controls HHV-6complex FS
HHV-6encephalopathy
119875
GlobalControlsversus
HHV-6 FS
Controls versusHHV-6
encephalopathy
HHV-6 FSversus HHV-6encephalopathy
8-OHdGngmL 0063 (001) 0116 (0061) 0129 (007) 00025 lt005 lt001 ns
HEL nmolL 362 (108) 524 (363) 359 (187) 01863 ns ns nsTau pgmL 6090 (3420) 6547 (2137) 139056 (142011) 00028 ns lt005 nsIL-6 pgmL 32 (30) 58 (53) 746 (1169) 00349 ns lt001 nsIL-10 pgmL 04 (03) 06 (08) 14 (21) 01663 ns ns nsTNF-120572 pgmL 01 (01) 03 (05) 34 (40) 00036 ns lt001 lt0058-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct HHV-6 human herpesvirus-6 FS febrile seizure ns not significant IL interleukinTNF tumor necrosis factoraValues are expressed as the mean (standard deviation)
4 Mediators of Inflammation
Con
trol (n=8
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy to
tal
(n=16
)
HH
V-6
ence
phal
opat
hy d
ays1
-2(n=5
)
HH
V-6
ence
phal
opat
hy d
ays3
ndash8(n=11
)
Tau
(pg
mL)
100
1000
10000
100000
lowast
lowastlowast
lowastlowast
lowastlowast
Figure 2 Cerebrospinal fluid (CSF) tau protein levelsThe horizon-tal bar indicates the mean value of each group CSF levels (meanplusmn SD) of tau protein in HHV-6 encephalopathy HHV-6 complexfebrile seizures (FS) and controls are 13 9056 plusmn 14 2011 pgmL6547plusmn2137 pgmL and 6090plusmn3420 pgmL respectively Total tauprotein levels in HHV-6 encephalopathy patients are significantlyhigher than in control subjects (lowast119875 lt 005) The levels of tau proteinin HHV-6 encephalopathy at days 3ndash8 (19 8569 plusmn 13 1219 pgmL)are significantly higher than those of HHV-6 encephalopathy atdays 1-2 (5204 plusmn 2296 pgmL) HHV-6 complex FS and controls(lowastlowast119875 lt 001)
the HHV-6 encephalopathy group into two groups accordingto sampling time at days 1-2 (119899 = 5) and days 3ndash8 (119899 = 11)respectively Consequently we found that the levels of tauprotein were significantly increased at days 3ndash8 in HHV-6encephalopathy (19 8569 plusmn 13 1219 pgmL mean plusmn SD)compared with those of HHV-6 encephalopathy at days 1-2 (5204 plusmn 2296 pgmL mean plusmn SD) (119875 lt 001) HHV-6complex FS (119875 lt 001) and controls (119875 lt 001) (Figure 2)
34 CSF Cytokine Profile in Acute Encephalopathy and Com-plex FS We next confirmed the elevation of CSF IL-6 andTNF-120572 in patients with HHV-6 encephalopathy (Figure 3)The CSF IL-6 levels in patients with HHV-6 encephalopathy(746 plusmn 1169 pgmL mean plusmn SD) were significantly higherthan in controls (32 plusmn 30 pgmL mean plusmn SD) (119875 lt 001)(Figure 3(a)) The CSF TNF-120572 levels in patients with HHV-6 encephalopathy (34 plusmn 40 pgmL mean plusmn SD) were also
significantly higher than those with complex FS (03 plusmn05 pgmL mean plusmn SD) and in controls (010 plusmn 01 pgmLmean plusmn SD) (119875 lt 005 and 119875 lt 001 resp) (Figure 3(c))In contrast there were no significant differences of CSF IL-10levels among patients with HHV-6 encephalopathy or HHV-6 complex FS and controls (Figure 3(b))
35 Correlation Analysis of CSF Biomarkers in HHV-6Encephalopathy We next examined correlations betweenCSF-8OHdG and other biomarkers in the HHV-6encephalopathy group (Table 3) There was a significantpositive correlation between IL-6 and TNF-120572 (Spearman119903 = 0783 119875 = 00006) However there were no significantcorrelations among other biomarkers In addition therewas no correlation between the increased levels of eachbiomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy (data not shown)
36 Changes in CSF-8-OHdG and CSF-HEL Levels beforeand after Edaravone Treatment in HHV-6-Associated AcuteEncephalopathy and Complex FS Finally we compared theCSF levels of oxidative stress markers in six patients withHHV-6 infection (5 patients with encephalopathy and 1patient with febrile seizures) before and after edaravone treat-ment Clinical profile of patients with edaravone treatmentis shown in Table 4 The mean initiation time of edaravonetreatment was day 48 for the HHV-6 encephalopathy groupOne patient with febrile seizures associated with HHV-6 infection who received edaravone treatment from day1 did not develop encephalopathy and recovered withoutsequelae (patient 6) The CSF-8-OHdG levels decreased afteredaravone treatment (119875 = 00202 paired 119905-test) (Figure 4(a))Regarding the CSF-HEL levels there were no significantdifferences between before and after edaravone treatmentWe also compared the mean CSF levels of other biomarkersbefore and after treatment and observed no significant differ-ences of mean values (data not shown)
4 Discussion
In the present study we demonstrated that CSF-8-OHdGlevels in HHV-6 encephalopathy and HHV-6 complex FSpatients were significantly higher than in controls suggestingincreased oxidative stress is induced by HHV-6 infectionRecent studies revealed that oxidative damage is an emerginggeneral mechanism of nervous system injury caused by viralinfection For example oxidative injury is a component ofacute encephalitis caused by herpes simplex virus type 1(HSV-1) [16] HSV-1 infection of nervous system tissues inmice was associated with the expression of inducible nitricoxide synthase (iNOS) and the release of cytokines includingTNF-120572 from inflammatory cells Thus increased generationof ROS and RNS can be caused by the direct effects ofvirus on cells and the indirect effects of host inflammatoryresponses [17] Regarding HHV-6 infection Fukuda et alreported that urinary 8-OHdG concentrations in a patientwith HHV-6 encephalopathy on the first day of hospital-ization were 15 times higher than the mean concentration
Mediators of Inflammation 5
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)01
1
10
100
1000
IL-6
(pg
mL)
lowastlowast
(a)C
ontro
l (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
01
1
10
IL-10
(pg
mL)
(b)
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
001
01
1
10
100
TNF-120572
(pg
mL)
lowast
lowastlowast
(c)
Figure 3 Cerebrospinal fluid (CSF) cytokine levels The horizontal bar indicates the mean value of each group (a) Levels of CSF IL-6 inpatients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 746plusmn1169 pgmL 58plusmn53 pgmL and 32plusmn30 pgmLrespectively The CSF IL-6 levels in patients with HHV-6 encephalopathy are significantly higher than in controls (lowastlowast119875 lt 001) (b) Levelsof CSF IL-10 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 14 plusmn 21 pgmL 06 plusmn 08 pgmL and04 plusmn 03 pgmL respectively (c) Levels of CSF TNF-120572 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controlsare 34 plusmn 40 pgmL 03 plusmn 05 pgmL and 01 plusmn 01 pgmL respectively The CSF TNF-120572 levels in patients with HHV-6 encephalopathy aresignificantly higher than those with complex FS and in controls (lowast119875 lt 005 and lowastlowast119875 lt 001 resp)
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Mediators of Inflammation 3
Table 1 Clinical characteristics of HHV-6 encephalopathy and febrile seizure patients
HHV-6 encephalopathy HHV-6 complex febrile seizures ControlsNumber of patients 16 10 16Age (months) 151 plusmn 54 126 plusmn 39 111 plusmn 108
Sex ratio (M F) 8 8 5 5 11 5Sampling time (day of illness) 1ndash8 1 mdashMRI abnormality 1416 ND NDOutcome (without sequelae) 516 1010 mdashHHV human herpesvirus No number ND not done M male F female MRI magnetic resonance imaging
Con
trol (n=16
)
HH
V-6
com
plex
FS
(n=10
)
HH
V-6
ence
phal
opat
hy(n=16
)
00
01
02
03
04
8-O
HdG
(ng
mL)
lowast
lowastlowast
(a)
Con
trol (n=15
)
HH
V-6
com
plex
FS
(n=7
)
HH
V-6
ence
phal
opat
hy(n=14
)
0
2
4
6
8
10
12
14
HEL
(nm
olL
)
(b)
Figure 1 Cerebrospinal fluid (CSF) levels of oxidative stress markers in HHV-6 encephalopathy HHV-6 complex febrile seizures (FS) andcontrols (a) 8-hydroxy-21015840-deoxyguanosine 8-OHdG (b) hexanoyl-lysine adduct HEL lowast119875 lt 005 lowastlowast119875 lt 001 The horizontal bar indicatesthe mean value of each group CSF-8OHdG levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6 complex FS and controls are 0129 plusmn007 ngmL 0116 plusmn 0061 ngmL and 0063 plusmn 001 ngmL respectively CSF-HEL levels (mean plusmn SD) in HHV-6 encephalopathy HHV-6complex FS and control subjects are 359 plusmn 187 nmolL 524 plusmn 363 nmolL and 362 plusmn 108 nmolL respectively
Table 2 Descriptive statistics for the biomarkers examineda
Biomarkers Controls HHV-6complex FS
HHV-6encephalopathy
119875
GlobalControlsversus
HHV-6 FS
Controls versusHHV-6
encephalopathy
HHV-6 FSversus HHV-6encephalopathy
8-OHdGngmL 0063 (001) 0116 (0061) 0129 (007) 00025 lt005 lt001 ns
HEL nmolL 362 (108) 524 (363) 359 (187) 01863 ns ns nsTau pgmL 6090 (3420) 6547 (2137) 139056 (142011) 00028 ns lt005 nsIL-6 pgmL 32 (30) 58 (53) 746 (1169) 00349 ns lt001 nsIL-10 pgmL 04 (03) 06 (08) 14 (21) 01663 ns ns nsTNF-120572 pgmL 01 (01) 03 (05) 34 (40) 00036 ns lt001 lt0058-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct HHV-6 human herpesvirus-6 FS febrile seizure ns not significant IL interleukinTNF tumor necrosis factoraValues are expressed as the mean (standard deviation)
4 Mediators of Inflammation
Con
trol (n=8
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy to
tal
(n=16
)
HH
V-6
ence
phal
opat
hy d
ays1
-2(n=5
)
HH
V-6
ence
phal
opat
hy d
ays3
ndash8(n=11
)
Tau
(pg
mL)
100
1000
10000
100000
lowast
lowastlowast
lowastlowast
lowastlowast
Figure 2 Cerebrospinal fluid (CSF) tau protein levelsThe horizon-tal bar indicates the mean value of each group CSF levels (meanplusmn SD) of tau protein in HHV-6 encephalopathy HHV-6 complexfebrile seizures (FS) and controls are 13 9056 plusmn 14 2011 pgmL6547plusmn2137 pgmL and 6090plusmn3420 pgmL respectively Total tauprotein levels in HHV-6 encephalopathy patients are significantlyhigher than in control subjects (lowast119875 lt 005) The levels of tau proteinin HHV-6 encephalopathy at days 3ndash8 (19 8569 plusmn 13 1219 pgmL)are significantly higher than those of HHV-6 encephalopathy atdays 1-2 (5204 plusmn 2296 pgmL) HHV-6 complex FS and controls(lowastlowast119875 lt 001)
the HHV-6 encephalopathy group into two groups accordingto sampling time at days 1-2 (119899 = 5) and days 3ndash8 (119899 = 11)respectively Consequently we found that the levels of tauprotein were significantly increased at days 3ndash8 in HHV-6encephalopathy (19 8569 plusmn 13 1219 pgmL mean plusmn SD)compared with those of HHV-6 encephalopathy at days 1-2 (5204 plusmn 2296 pgmL mean plusmn SD) (119875 lt 001) HHV-6complex FS (119875 lt 001) and controls (119875 lt 001) (Figure 2)
34 CSF Cytokine Profile in Acute Encephalopathy and Com-plex FS We next confirmed the elevation of CSF IL-6 andTNF-120572 in patients with HHV-6 encephalopathy (Figure 3)The CSF IL-6 levels in patients with HHV-6 encephalopathy(746 plusmn 1169 pgmL mean plusmn SD) were significantly higherthan in controls (32 plusmn 30 pgmL mean plusmn SD) (119875 lt 001)(Figure 3(a)) The CSF TNF-120572 levels in patients with HHV-6 encephalopathy (34 plusmn 40 pgmL mean plusmn SD) were also
significantly higher than those with complex FS (03 plusmn05 pgmL mean plusmn SD) and in controls (010 plusmn 01 pgmLmean plusmn SD) (119875 lt 005 and 119875 lt 001 resp) (Figure 3(c))In contrast there were no significant differences of CSF IL-10levels among patients with HHV-6 encephalopathy or HHV-6 complex FS and controls (Figure 3(b))
35 Correlation Analysis of CSF Biomarkers in HHV-6Encephalopathy We next examined correlations betweenCSF-8OHdG and other biomarkers in the HHV-6encephalopathy group (Table 3) There was a significantpositive correlation between IL-6 and TNF-120572 (Spearman119903 = 0783 119875 = 00006) However there were no significantcorrelations among other biomarkers In addition therewas no correlation between the increased levels of eachbiomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy (data not shown)
36 Changes in CSF-8-OHdG and CSF-HEL Levels beforeand after Edaravone Treatment in HHV-6-Associated AcuteEncephalopathy and Complex FS Finally we compared theCSF levels of oxidative stress markers in six patients withHHV-6 infection (5 patients with encephalopathy and 1patient with febrile seizures) before and after edaravone treat-ment Clinical profile of patients with edaravone treatmentis shown in Table 4 The mean initiation time of edaravonetreatment was day 48 for the HHV-6 encephalopathy groupOne patient with febrile seizures associated with HHV-6 infection who received edaravone treatment from day1 did not develop encephalopathy and recovered withoutsequelae (patient 6) The CSF-8-OHdG levels decreased afteredaravone treatment (119875 = 00202 paired 119905-test) (Figure 4(a))Regarding the CSF-HEL levels there were no significantdifferences between before and after edaravone treatmentWe also compared the mean CSF levels of other biomarkersbefore and after treatment and observed no significant differ-ences of mean values (data not shown)
4 Discussion
In the present study we demonstrated that CSF-8-OHdGlevels in HHV-6 encephalopathy and HHV-6 complex FSpatients were significantly higher than in controls suggestingincreased oxidative stress is induced by HHV-6 infectionRecent studies revealed that oxidative damage is an emerginggeneral mechanism of nervous system injury caused by viralinfection For example oxidative injury is a component ofacute encephalitis caused by herpes simplex virus type 1(HSV-1) [16] HSV-1 infection of nervous system tissues inmice was associated with the expression of inducible nitricoxide synthase (iNOS) and the release of cytokines includingTNF-120572 from inflammatory cells Thus increased generationof ROS and RNS can be caused by the direct effects ofvirus on cells and the indirect effects of host inflammatoryresponses [17] Regarding HHV-6 infection Fukuda et alreported that urinary 8-OHdG concentrations in a patientwith HHV-6 encephalopathy on the first day of hospital-ization were 15 times higher than the mean concentration
Mediators of Inflammation 5
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)01
1
10
100
1000
IL-6
(pg
mL)
lowastlowast
(a)C
ontro
l (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
01
1
10
IL-10
(pg
mL)
(b)
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
001
01
1
10
100
TNF-120572
(pg
mL)
lowast
lowastlowast
(c)
Figure 3 Cerebrospinal fluid (CSF) cytokine levels The horizontal bar indicates the mean value of each group (a) Levels of CSF IL-6 inpatients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 746plusmn1169 pgmL 58plusmn53 pgmL and 32plusmn30 pgmLrespectively The CSF IL-6 levels in patients with HHV-6 encephalopathy are significantly higher than in controls (lowastlowast119875 lt 001) (b) Levelsof CSF IL-10 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 14 plusmn 21 pgmL 06 plusmn 08 pgmL and04 plusmn 03 pgmL respectively (c) Levels of CSF TNF-120572 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controlsare 34 plusmn 40 pgmL 03 plusmn 05 pgmL and 01 plusmn 01 pgmL respectively The CSF TNF-120572 levels in patients with HHV-6 encephalopathy aresignificantly higher than those with complex FS and in controls (lowast119875 lt 005 and lowastlowast119875 lt 001 resp)
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Mediators of Inflammation
Con
trol (n=8
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy to
tal
(n=16
)
HH
V-6
ence
phal
opat
hy d
ays1
-2(n=5
)
HH
V-6
ence
phal
opat
hy d
ays3
ndash8(n=11
)
Tau
(pg
mL)
100
1000
10000
100000
lowast
lowastlowast
lowastlowast
lowastlowast
Figure 2 Cerebrospinal fluid (CSF) tau protein levelsThe horizon-tal bar indicates the mean value of each group CSF levels (meanplusmn SD) of tau protein in HHV-6 encephalopathy HHV-6 complexfebrile seizures (FS) and controls are 13 9056 plusmn 14 2011 pgmL6547plusmn2137 pgmL and 6090plusmn3420 pgmL respectively Total tauprotein levels in HHV-6 encephalopathy patients are significantlyhigher than in control subjects (lowast119875 lt 005) The levels of tau proteinin HHV-6 encephalopathy at days 3ndash8 (19 8569 plusmn 13 1219 pgmL)are significantly higher than those of HHV-6 encephalopathy atdays 1-2 (5204 plusmn 2296 pgmL) HHV-6 complex FS and controls(lowastlowast119875 lt 001)
the HHV-6 encephalopathy group into two groups accordingto sampling time at days 1-2 (119899 = 5) and days 3ndash8 (119899 = 11)respectively Consequently we found that the levels of tauprotein were significantly increased at days 3ndash8 in HHV-6encephalopathy (19 8569 plusmn 13 1219 pgmL mean plusmn SD)compared with those of HHV-6 encephalopathy at days 1-2 (5204 plusmn 2296 pgmL mean plusmn SD) (119875 lt 001) HHV-6complex FS (119875 lt 001) and controls (119875 lt 001) (Figure 2)
34 CSF Cytokine Profile in Acute Encephalopathy and Com-plex FS We next confirmed the elevation of CSF IL-6 andTNF-120572 in patients with HHV-6 encephalopathy (Figure 3)The CSF IL-6 levels in patients with HHV-6 encephalopathy(746 plusmn 1169 pgmL mean plusmn SD) were significantly higherthan in controls (32 plusmn 30 pgmL mean plusmn SD) (119875 lt 001)(Figure 3(a)) The CSF TNF-120572 levels in patients with HHV-6 encephalopathy (34 plusmn 40 pgmL mean plusmn SD) were also
significantly higher than those with complex FS (03 plusmn05 pgmL mean plusmn SD) and in controls (010 plusmn 01 pgmLmean plusmn SD) (119875 lt 005 and 119875 lt 001 resp) (Figure 3(c))In contrast there were no significant differences of CSF IL-10levels among patients with HHV-6 encephalopathy or HHV-6 complex FS and controls (Figure 3(b))
35 Correlation Analysis of CSF Biomarkers in HHV-6Encephalopathy We next examined correlations betweenCSF-8OHdG and other biomarkers in the HHV-6encephalopathy group (Table 3) There was a significantpositive correlation between IL-6 and TNF-120572 (Spearman119903 = 0783 119875 = 00006) However there were no significantcorrelations among other biomarkers In addition therewas no correlation between the increased levels of eachbiomarker and the presence or absence of neurologicalsequelae in HHV-6 encephalopathy (data not shown)
36 Changes in CSF-8-OHdG and CSF-HEL Levels beforeand after Edaravone Treatment in HHV-6-Associated AcuteEncephalopathy and Complex FS Finally we compared theCSF levels of oxidative stress markers in six patients withHHV-6 infection (5 patients with encephalopathy and 1patient with febrile seizures) before and after edaravone treat-ment Clinical profile of patients with edaravone treatmentis shown in Table 4 The mean initiation time of edaravonetreatment was day 48 for the HHV-6 encephalopathy groupOne patient with febrile seizures associated with HHV-6 infection who received edaravone treatment from day1 did not develop encephalopathy and recovered withoutsequelae (patient 6) The CSF-8-OHdG levels decreased afteredaravone treatment (119875 = 00202 paired 119905-test) (Figure 4(a))Regarding the CSF-HEL levels there were no significantdifferences between before and after edaravone treatmentWe also compared the mean CSF levels of other biomarkersbefore and after treatment and observed no significant differ-ences of mean values (data not shown)
4 Discussion
In the present study we demonstrated that CSF-8-OHdGlevels in HHV-6 encephalopathy and HHV-6 complex FSpatients were significantly higher than in controls suggestingincreased oxidative stress is induced by HHV-6 infectionRecent studies revealed that oxidative damage is an emerginggeneral mechanism of nervous system injury caused by viralinfection For example oxidative injury is a component ofacute encephalitis caused by herpes simplex virus type 1(HSV-1) [16] HSV-1 infection of nervous system tissues inmice was associated with the expression of inducible nitricoxide synthase (iNOS) and the release of cytokines includingTNF-120572 from inflammatory cells Thus increased generationof ROS and RNS can be caused by the direct effects ofvirus on cells and the indirect effects of host inflammatoryresponses [17] Regarding HHV-6 infection Fukuda et alreported that urinary 8-OHdG concentrations in a patientwith HHV-6 encephalopathy on the first day of hospital-ization were 15 times higher than the mean concentration
Mediators of Inflammation 5
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)01
1
10
100
1000
IL-6
(pg
mL)
lowastlowast
(a)C
ontro
l (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
01
1
10
IL-10
(pg
mL)
(b)
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
001
01
1
10
100
TNF-120572
(pg
mL)
lowast
lowastlowast
(c)
Figure 3 Cerebrospinal fluid (CSF) cytokine levels The horizontal bar indicates the mean value of each group (a) Levels of CSF IL-6 inpatients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 746plusmn1169 pgmL 58plusmn53 pgmL and 32plusmn30 pgmLrespectively The CSF IL-6 levels in patients with HHV-6 encephalopathy are significantly higher than in controls (lowastlowast119875 lt 001) (b) Levelsof CSF IL-10 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 14 plusmn 21 pgmL 06 plusmn 08 pgmL and04 plusmn 03 pgmL respectively (c) Levels of CSF TNF-120572 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controlsare 34 plusmn 40 pgmL 03 plusmn 05 pgmL and 01 plusmn 01 pgmL respectively The CSF TNF-120572 levels in patients with HHV-6 encephalopathy aresignificantly higher than those with complex FS and in controls (lowast119875 lt 005 and lowastlowast119875 lt 001 resp)
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Mediators of Inflammation 5
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)01
1
10
100
1000
IL-6
(pg
mL)
lowastlowast
(a)C
ontro
l (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
01
1
10
IL-10
(pg
mL)
(b)
Con
trol (n=12
)
HH
V-6
com
plex
FS
(n=9
)
HH
V-6
ence
phal
opat
hy(n=15
)
001
01
1
10
100
TNF-120572
(pg
mL)
lowast
lowastlowast
(c)
Figure 3 Cerebrospinal fluid (CSF) cytokine levels The horizontal bar indicates the mean value of each group (a) Levels of CSF IL-6 inpatients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 746plusmn1169 pgmL 58plusmn53 pgmL and 32plusmn30 pgmLrespectively The CSF IL-6 levels in patients with HHV-6 encephalopathy are significantly higher than in controls (lowastlowast119875 lt 001) (b) Levelsof CSF IL-10 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controls are 14 plusmn 21 pgmL 06 plusmn 08 pgmL and04 plusmn 03 pgmL respectively (c) Levels of CSF TNF-120572 in patients with HHV-6 encephalopathy HHV-6 febrile seizures (FS) and controlsare 34 plusmn 40 pgmL 03 plusmn 05 pgmL and 01 plusmn 01 pgmL respectively The CSF TNF-120572 levels in patients with HHV-6 encephalopathy aresignificantly higher than those with complex FS and in controls (lowast119875 lt 005 and lowastlowast119875 lt 001 resp)
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
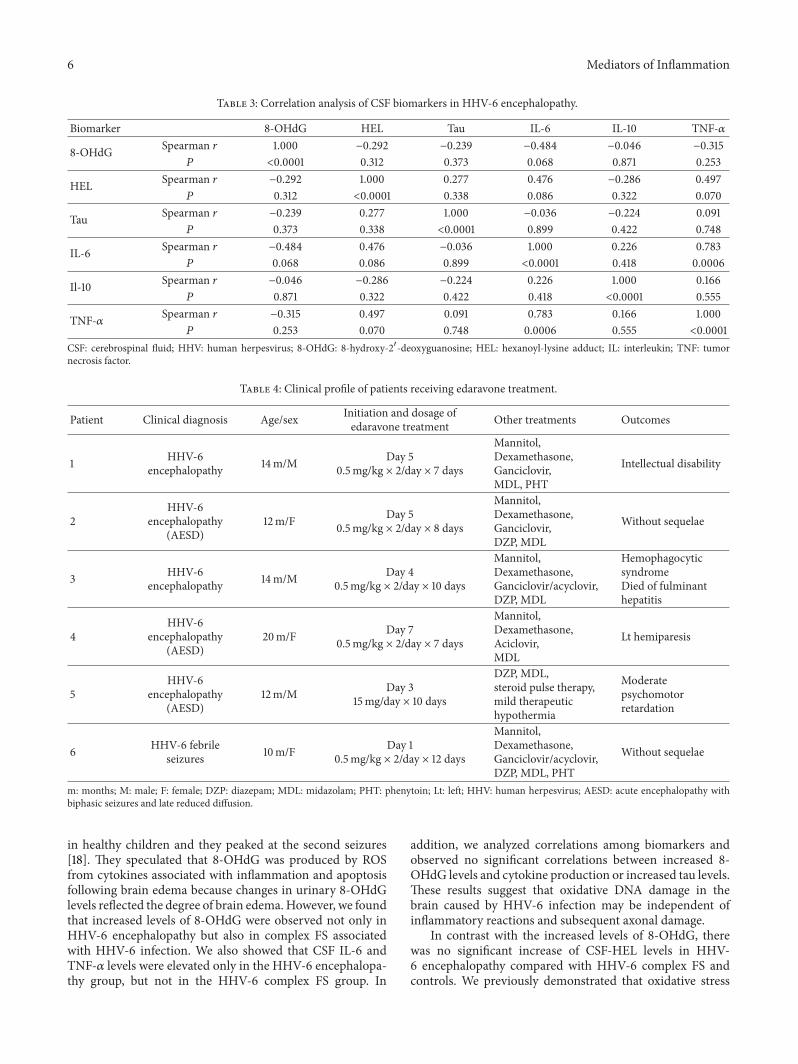
6 Mediators of Inflammation
Table 3 Correlation analysis of CSF biomarkers in HHV-6 encephalopathy
Biomarker 8-OHdG HEL Tau IL-6 IL-10 TNF-120572
8-OHdG Spearman 119903 1000 minus0292 minus0239 minus0484 minus0046 minus0315119875 lt00001 0312 0373 0068 0871 0253
HEL Spearman 119903 minus0292 1000 0277 0476 minus0286 0497119875 0312 lt00001 0338 0086 0322 0070
Tau Spearman 119903 minus0239 0277 1000 minus0036 minus0224 0091119875 0373 0338 lt00001 0899 0422 0748
IL-6 Spearman 119903 minus0484 0476 minus0036 1000 0226 0783119875 0068 0086 0899 lt00001 0418 00006
Il-10 Spearman 119903 minus0046 minus0286 minus0224 0226 1000 0166119875 0871 0322 0422 0418 lt00001 0555
TNF-120572 Spearman 119903 minus0315 0497 0091 0783 0166 1000119875 0253 0070 0748 00006 0555 lt00001
CSF cerebrospinal fluid HHV human herpesvirus 8-OHdG 8-hydroxy-21015840-deoxyguanosine HEL hexanoyl-lysine adduct IL interleukin TNF tumornecrosis factor
Table 4 Clinical profile of patients receiving edaravone treatment
Patient Clinical diagnosis Agesex Initiation and dosage ofedaravone treatment Other treatments Outcomes
1 HHV-6encephalopathy 14mM Day 5
05mgkg times 2day times 7 days
MannitolDexamethasoneGanciclovirMDL PHT
Intellectual disability
2HHV-6
encephalopathy(AESD)
12mF Day 505mgkg times 2day times 8 days
MannitolDexamethasoneGanciclovirDZP MDL
Without sequelae
3 HHV-6encephalopathy 14mM Day 4
05mgkg times 2day times 10 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL
HemophagocyticsyndromeDied of fulminanthepatitis
4HHV-6
encephalopathy(AESD)
20mF Day 705mgkg times 2day times 7 days
MannitolDexamethasoneAciclovirMDL
Lt hemiparesis
5HHV-6
encephalopathy(AESD)
12mM Day 315mgday times 10 days
DZP MDLsteroid pulse therapymild therapeutichypothermia
Moderatepsychomotorretardation
6 HHV-6 febrileseizures 10mF Day 1
05mgkg times 2day times 12 days
MannitolDexamethasoneGancicloviracyclovirDZP MDL PHT
Without sequelae
m months M male F female DZP diazepam MDL midazolam PHT phenytoin Lt left HHV human herpesvirus AESD acute encephalopathy withbiphasic seizures and late reduced diffusion
in healthy children and they peaked at the second seizures[18] They speculated that 8-OHdG was produced by ROSfrom cytokines associated with inflammation and apoptosisfollowing brain edema because changes in urinary 8-OHdGlevels reflected the degree of brain edema However we foundthat increased levels of 8-OHdG were observed not only inHHV-6 encephalopathy but also in complex FS associatedwith HHV-6 infection We also showed that CSF IL-6 andTNF-120572 levels were elevated only in the HHV-6 encephalopa-thy group but not in the HHV-6 complex FS group In
addition we analyzed correlations among biomarkers andobserved no significant correlations between increased 8-OHdG levels and cytokine production or increased tau levelsThese results suggest that oxidative DNA damage in thebrain caused by HHV-6 infection may be independent ofinflammatory reactions and subsequent axonal damage
In contrast with the increased levels of 8-OHdG therewas no significant increase of CSF-HEL levels in HHV-6 encephalopathy compared with HHV-6 complex FS andcontrols We previously demonstrated that oxidative stress
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
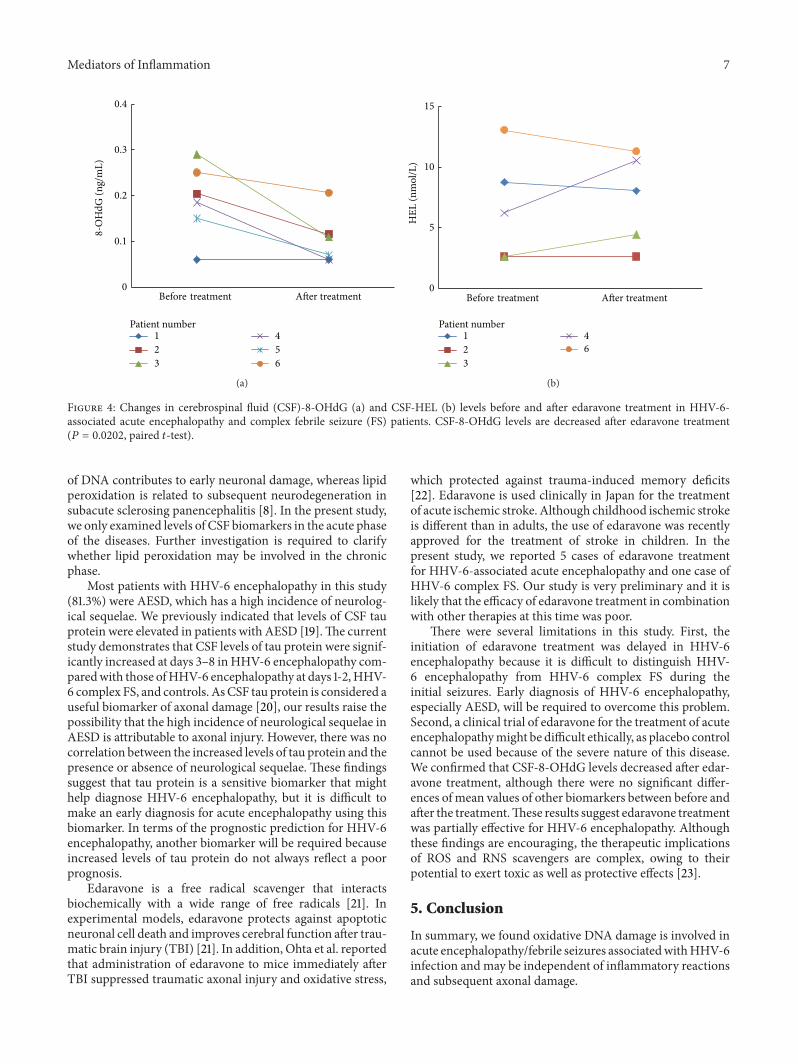
Mediators of Inflammation 7
0
01
02
03
048
-OH
dG (n
gm
L)
Before treatment After treatment
1
2
3
4
5
6
Patient number
(a)
0
5
10
15
HEL
(nm
olL
)
1
2
3
4
6
Patient number
Before treatment After treatment
(b)
Figure 4 Changes in cerebrospinal fluid (CSF)-8-OHdG (a) and CSF-HEL (b) levels before and after edaravone treatment in HHV-6-associated acute encephalopathy and complex febrile seizure (FS) patients CSF-8-OHdG levels are decreased after edaravone treatment(119875 = 00202 paired 119905-test)
of DNA contributes to early neuronal damage whereas lipidperoxidation is related to subsequent neurodegeneration insubacute sclerosing panencephalitis [8] In the present studywe only examined levels of CSF biomarkers in the acute phaseof the diseases Further investigation is required to clarifywhether lipid peroxidation may be involved in the chronicphase
Most patients with HHV-6 encephalopathy in this study(813) were AESD which has a high incidence of neurolog-ical sequelae We previously indicated that levels of CSF tauprotein were elevated in patients with AESD [19]The currentstudy demonstrates that CSF levels of tau protein were signif-icantly increased at days 3ndash8 inHHV-6 encephalopathy com-paredwith those ofHHV-6 encephalopathy at days 1-2HHV-6 complex FS and controls AsCSF tau protein is considered auseful biomarker of axonal damage [20] our results raise thepossibility that the high incidence of neurological sequelae inAESD is attributable to axonal injury However there was nocorrelation between the increased levels of tau protein and thepresence or absence of neurological sequelae These findingssuggest that tau protein is a sensitive biomarker that mighthelp diagnose HHV-6 encephalopathy but it is difficult tomake an early diagnosis for acute encephalopathy using thisbiomarker In terms of the prognostic prediction for HHV-6encephalopathy another biomarker will be required becauseincreased levels of tau protein do not always reflect a poorprognosis
Edaravone is a free radical scavenger that interactsbiochemically with a wide range of free radicals [21] Inexperimental models edaravone protects against apoptoticneuronal cell death and improves cerebral function after trau-matic brain injury (TBI) [21] In addition Ohta et al reportedthat administration of edaravone to mice immediately afterTBI suppressed traumatic axonal injury and oxidative stress
which protected against trauma-induced memory deficits[22] Edaravone is used clinically in Japan for the treatmentof acute ischemic stroke Although childhood ischemic strokeis different than in adults the use of edaravone was recentlyapproved for the treatment of stroke in children In thepresent study we reported 5 cases of edaravone treatmentfor HHV-6-associated acute encephalopathy and one case ofHHV-6 complex FS Our study is very preliminary and it islikely that the efficacy of edaravone treatment in combinationwith other therapies at this time was poor
There were several limitations in this study First theinitiation of edaravone treatment was delayed in HHV-6encephalopathy because it is difficult to distinguish HHV-6 encephalopathy from HHV-6 complex FS during theinitial seizures Early diagnosis of HHV-6 encephalopathyespecially AESD will be required to overcome this problemSecond a clinical trial of edaravone for the treatment of acuteencephalopathymight be difficult ethically as placebo controlcannot be used because of the severe nature of this diseaseWe confirmed that CSF-8-OHdG levels decreased after edar-avone treatment although there were no significant differ-ences of mean values of other biomarkers between before andafter the treatmentThese results suggest edaravone treatmentwas partially effective for HHV-6 encephalopathy Althoughthese findings are encouraging the therapeutic implicationsof ROS and RNS scavengers are complex owing to theirpotential to exert toxic as well as protective effects [23]
5 Conclusion
In summary we found oxidative DNA damage is involved inacute encephalopathyfebrile seizures associatedwithHHV-6infection andmay be independent of inflammatory reactionsand subsequent axonal damage
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
8 Mediators of Inflammation
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This study was supported by grants from theMinistry of Edu-cation Culture Sports Science and Technology (22591147)and the Ministry of Health Labour andWelfare (H23-Nanji-Ippan-107) Japan
References
[1] J Takanashi H Oba A J Barkovich et al ldquoDiffusionMRI abnormalities after prolonged febrile seizures withencephalopathyrdquo Neurology vol 66 no 9 pp 1304ndash1309 2006
[2] J-I Takanashi ldquoTwo newly proposed infectious encephali-tisencephalopathy syndromesrdquo Brain and Development vol 31no 7 pp 521ndash528 2009
[3] A Hoshino M Saitoh A Oka et al ldquoEpidemiology of acuteencephalopathy in Japan with emphasis on the association ofviruses and syndromesrdquo Brain and Development vol 34 no 5pp 337ndash343 2012
[4] M Mizuguchi ldquoOverview of acute encephalitis andencephalopathyrdquo Nippon Rinsho Japanese Journal of ClinicalMedicine vol 69 no 3 pp 391ndash398 2011
[5] M Hayashi ldquoOxidative stress in developmental brain disor-dersrdquo Neuropathology vol 29 no 1 pp 1ndash8 2009
[6] J Emerit M Edeas and F Bricaire ldquoNeurodegenerative dis-eases and oxidative stressrdquo Biomedicine and Pharmacotherapyvol 58 no 1 pp 39ndash46 2004
[7] K Dasuri L Zhang and J N Keller ldquoOxidative stress neurode-generation and the balance of protein degradation and proteinsynthesisrdquo Free Radical Biology and Medicine vol 62 pp 170ndash185 2013
[8] M Hayashi N Arai J Satoh et al ldquoNeurodegenerative mecha-nisms in subacute sclerosing panencephalitisrdquo Journal of ChildNeurology vol 17 no 10 pp 725ndash730 2002
[9] M Hayashi M Itoh S Araki et al ldquoOxidative stress anddisturbed glutamate transport in hereditary nucleotide repairdisordersrdquo Journal of Neuropathology amp Experimental Neurol-ogy vol 60 no 4 pp 350ndash356 2001
[10] M Hayashi S Araki J Kohyama K Shioda and R FukatsuldquoOxidative nucleotide damage and superoxide dismutaseexpression in the brains of xeroderma pigmentosum group Aand Cockayne syndromerdquo Brain and Development vol 27 no 1pp 34ndash38 2005
[11] M Hayashi S Araki N Arai et al ldquoOxidative stress anddisturbed glutamate transport in spinal muscular atrophyrdquoBrain and Development vol 24 no 8 pp 770ndash775 2002
[12] E Otomo H Tohgi K Kogure et al ldquoEffect of a novel freeradical scavenger edaravone (MCI-186) on acute brain infarc-tion Randomized placebo-controlled double-blind study atmulticentersrdquo Cerebrovascular Diseases vol 15 no 3 pp 222ndash229 2003
[13] B J Lee Y Egi K van Leyen E H Lo and K AraildquoEdaravone a free radical scavenger protects components ofthe neurovascular unit against oxidative stress in vitrordquo BrainResearch vol 1307 pp 22ndash27 2010
[14] Y Kitagawa ldquoEdaravone in acute ischemic strokerdquo InternalMedicine vol 45 no 5 pp 225ndash226 2006
[15] Y Higashi ldquoEdaravone for the treatment of acute cerebralinfarction role of endothelium-derived nitric oxide and oxida-tive stressrdquo Expert Opinion on Pharmacotherapy vol 10 no 2pp 323ndash331 2009
[16] T Valyi-Nagy and T S Dermody ldquoRole of oxidative damagein the pathogenesis of viral infections of the nervous systemrdquoHistology and Histopathology vol 20 no 3 pp 957ndash967 2005
[17] T Akaike ldquoRole of free radicals in viral pathogenesis andmutationrdquo Reviews in Medical Virology vol 11 no 2 pp 87ndash1012001
[18] M Fukuda H Yamauchi H Yamamoto et al ldquoThe evaluationof oxidative DNA damage in children with brain damage using8-hydroxydeoxyguanosine levelsrdquo Brain amp Development vol30 no 2 pp 131ndash136 2008
[19] N Tanuma R Miyata S Kumada et al ldquoThe axonal damagemarker tau protein in the cerebrospinal fluid is increased inpatients with acute encephalopathy with biphasic seizures andlate reduced diffusionrdquo Brain and Development vol 32 no 6pp 435ndash439 2010
[20] M Ost K Nylen L Csajbok et al ldquoInitial CSF total taucorrelates with 1-year outcome in patients with traumatic braininjuryrdquo Neurology vol 67 no 9 pp 1600ndash1604 2006
[21] T Itoh T Satou S Nishida et al ldquoEdaravone protects againstapoptotic neuronal cell death and improves cerebral functionafter traumatic brain injury in ratsrdquo Neurochemical Researchvol 35 no 2 pp 348ndash355 2010
[22] M Ohta Y Higashi T Yawata et al ldquoAttenuation of axonalinjury and oxidative stress by edaravone protects against cogni-tive impairments after traumatic brain injuryrdquo Brain Researchvol 1490 pp 184ndash192 2013
[23] T Satoh and S A Lipton ldquoRedox regulation of neuronalsurvival mediated by electrophilic compoundsrdquo Trends in Neu-rosciences vol 30 no 1 pp 37ndash45 2007
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom