research article assessment of bone healing during
TRANSCRIPT

Dow
nloadedfrom
https://journals.lww.com
/jaaosby
BhDMf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD3XG
JiJSDa6kLdjliR
zOOsR
+bI3gZWJ99prw
iH9JO
uTYY=on
09/11/2018
Downloadedfromhttps://journals.lww.com/jaaosbyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3XGJiJSDa6kLdjliRzOOsR+bI3gZWJ99prwiH9JOuTYY=on09/11/2018
Research Article
Assessment of Bone HealingDuring Antegrade IntramedullaryRod Femur Lengthening UsingRadiographic Pixel Density
Abstract
Introduction: Premature full weight bearing after femur lengtheningcan lead to implant failure, telescopic nail shortening, and regeneratefracture. This study aimedat performing a retrospective analysis of thecorrelation between pixel density ratio (PDR) calculations and clinicalreadiness for weight bearing in patients undergoing intramedullarynail–mediated femoral distraction osteogenesis.Methods: Thirty-two patients who underwent antegrade femurlengtheningwere included in this study.ThePDRwascalculatedon femurradiographs in a picture archiving and communication system for eachcortex (ie, medial, lateral, anterior, and posterior) at each postoperativevisit. Thesevalueswere thencorrelatedwithsubjectiveevaluationof bonehealing by the treating physician with expertise in bone lengthening.Results: Bone regenerate healingwas clinically declared by the treatingsurgeons (S.R.R. and A.T.F.) at a mean of 8.5 weeks (range, 4 to 18weeks). No implant failure, nail shortening, or regenerate fracture wasobserved. The overall mean PDR corresponding to clinical bone healingwas 0.90, which was significantly (P , 0.001) greater than the meanvalue at the previous visit (0.82), when the bone was not clinicallydeclared to be healed. The PDR increased in all cortices at allpostoperative visits.Conclusions: The findings of the present study suggest that theremay be a correlation between the PDR and clinical bone healing. Thisobservational pilot study should be followed by additional studies tounderstand the relationship between the PDR and bony union.
The use of telescopic intra-medullary (IM) rods for femur
lengthening is quickly gaining inpopularity. IM rods decrease the highcomplication rates of pin track in-fections, joint stiffness contracturesdue to tethering of the muscles bythe pins, and large pin track scarsthat occur with external fixators.1,2
Weight bearing must be limitedduring distraction as per the device’sbiomechanical testing and the man-
ufacturer’s recommendations. Oneof the challenges that orthopaedicsurgeons face is the decision as towhen a bone has sufficiently healedto allow a patient to begin bearingweight fully. The main tool used toassess bone healing in clinical prac-tice today is standard radiography intwo planes, which is commonlychosen because it is widely availableand inexpensive. The presence ofthree of four continuous cortices at
Ettore Vulcano, MD
Jonathan S. Markowitz, BS
Shabaz Ali
Joseph Nguyen, MPH
Austin T. Fragomen, MD
S. Robert Rozbruch, MD
From the Icahn School of Medicineat Mount Sinai, New York, NY(Dr. Vulcano), and Hospital forSpecial Surgery, New York, NY(Mr. Markowitz, Mr. Ali, Mr. Nguyen,Dr. Fragomen, Dr. Rozbruch).
Correspondence to Dr. Vulcano:[email protected]
J Am Acad Orthop Surg 2018;26:e388-e394
DOI: 10.5435/JAAOS-D-16-00949
Copyright 2018 by the AmericanAcademy of Orthopaedic Surgeons.
e388 Journal of the American Academy of Orthopaedic Surgeons
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

least 2 mm thick on AP and lateralradiographs is a commonly citedcriterion for the removal of theexternal fixator.3 This method ofidentifying three of four cortices ismost applicable to lengthening withexternal fixation and not necessarilyapplicable to the use of a lengtheningnail. Furthermore, identification ofcortices on radiographs is subjectiveand surgeon dependent, and thevariation in the assessment of thenumber of cortices present is slightlybetter than chance.4,5
Various indirect quantitative meth-ods, including dual-energy x-ray ab-sorptiometry (DEXA) and quantitativeCT (QCT), have been explored andevaluated as feasible options for as-sessing bone healing after distractionosteogenesis. Although they exposepatients to less radiation, these meth-ods have various pitfalls, includinginability to assess for bone alignmentand implant integrity, high cost, andless accessibility.There is a need for a quick, inex-
pensive, reproducible, and simplequantitative method to help ortho-paedic surgeons determine when it isappropriate to allow patients to bearweight after distraction osteogenesisusing an IM rod. The pixel densityratio (PDR) method may provide amore accurate means for assessingthe regenerate bone healing afterdistraction osteogenesis than thesubjective evaluation of the corticalbridging method. Authors who haveassessed the PDR method have eval-uated only the method for bonehealing of the tibia after applicationof an external fixator.6,7 Studies haveshown that the PDR method has lowinterobserver variability and high
intraobserver reproducibility andthat this method is a useful way toindicate callus stiffness to judge bonehealing.6,7 Some authors have shownthat pixel density (PD) is an effectivemethod in determining when to re-move an external fixator after dis-traction osteogenesis of the tibia, butlittle is known on its efficacy indetermining bone healing after dis-traction osteogenesis of the femurusing an IM rod.6,7 The goal of thepresent study was to correlate PDRvalues and clinical readiness forweight bearing in patients undergo-ing femur lengthening with an ante-grade motorized IM nail. Theauthors hypothesize that the PDRwill correlate with progressive bonehealing, and there will be a notablethreshold above which patients willbe allowed to safely bear full weight.
Methods
An institutional review board–approved retrospective study wasconducted on 32 consecutive pa-tients who underwent antegradefemur lengthening using a motorizedIM rod from February 2012 to May2015 at the Icahn School of Medicineat Mount Sinai. We excluded allpatients who did not meet the mini-mum requirement of 1-year follow-up. Indications for limb lengtheningincluded congenital in 26 patients(81%) (short stature in 6 patients,hence 12 femurs) and posttraumaticleg-length discrepancy in 6 patients(19%). Twenty-two (69%) weremen, and 10 (31%)were women. Themean age was 26 years (range, 12 to52 years). The mean amount of
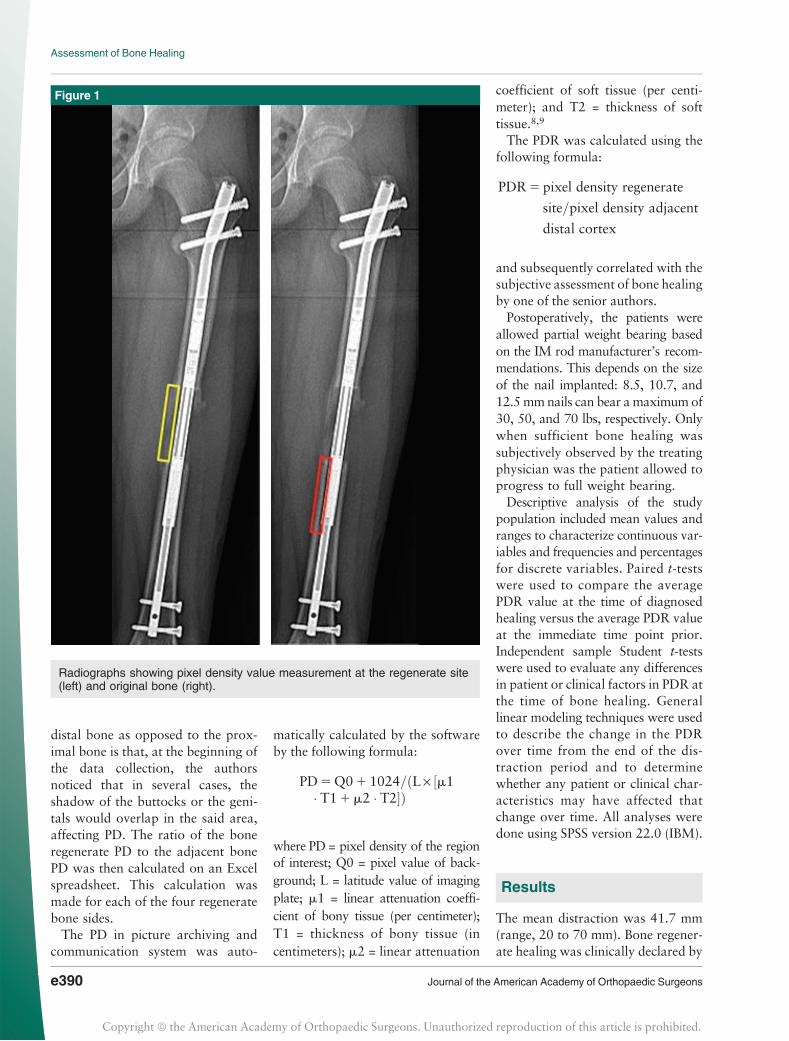
lengthening was 41.7 mm (range, 20to 70mm). Themean bony union timewas 8.5 weeks (range, 4 to 18 weeks)and was based on the surgeon’s ex-perience. Serial, non–weight bearing,two-view 36-inch radiographs of thefemur (performed at 3 feet from thepatient and with the use of a 1-inchmagnification marker) were assessedby a single operator starting at thecompletion of lengthening (week 0).The pixel densities of the lateral andmedial cortices were measured onAP radiographs, and the anterior andposterior cortices were measured onlateral radiographs. All four corticeswere measured for each patient atevery postoperative visit. These val-ues were then compared with theadjacent 2 cm of original bone justdistal to the regenerate site (Figure 1).Any picture archiving and com-
munication system provides a tool tomeasure the PD on the radiographs.Typically, this tool is labeled as“ROI” (region of interest). Once thetool has been selected, the operatorwill need to delineate the regeneratebone being studied (ie, medial, lat-eral, anterior, and posterior) withmultiple mouse clicks. To avoidcompromising the ultimate PD value,it is crucial not to incorporate anypart of the metal rod in the region ofinterest. The same applies to theadjacent bone and to the area outsidethe regenerate site. The use of mul-tiple mouse clicks will allow one toaccurately select the area of interest.The delineation of the bone regen-erate will ultimately provide a PDvalue. The next step is to perform thesame measurement on the adjacentdistal 2 cm of bone (not including theregenerate). The reason to use the
Dr. Fragomen or an immediate family member has received royalties from Stryker; serves as a paid consultant to NuVasive, Smith &Nephew, and Synthes; and serves as a board member, owner, officer, or committee member of the Limb Lengthening Research Society.Dr. Rozbruch or an immediate family member has received royalties from Stryker; is a member of a speakers’ bureau or has made paidpresentations on behalf of NuVasive, Smith & Nephew, and Stryker; serves as a paid consultant to NuVasive, Smith & Nephew, and Stryker;and serves as a board member, owner, officer, or committee member of the Limb Lengthening Reconstruction Society. None of the followingauthors or any immediate family member has received anything of value from or has stock or stock options held in a commercial company orinstitution related directly or indirectly to the subject of this article: Dr. Vulcano, Mr. Markowitz, Mr. Ali, and Mr. Nguyen.
Ettore Vulcano, MD, et al
September 15, 2018, Vol 26, No 18 e389
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
distal bone as opposed to the prox-imal bone is that, at the beginning ofthe data collection, the authorsnoticed that in several cases, theshadow of the buttocks or the geni-tals would overlap in the said area,affecting PD. The ratio of the boneregenerate PD to the adjacent bonePD was then calculated on an Excelspreadsheet. This calculation wasmade for each of the four regeneratebone sides.The PD in picture archiving and
communication system was auto-
matically calculated by the softwareby the following formula:
PD5Q01 1024=ðL· ½m1� T11m2 � T2�Þ
where PD = pixel density of the regionof interest; Q0 = pixel value of back-ground; L = latitude value of imagingplate; m1 = linear attenuation coeffi-cient of bony tissue (per centimeter);T1 = thickness of bony tissue (incentimeters); m2 = linear attenuation
coefficient of soft tissue (per centi-meter); and T2 = thickness of softtissue.8,9
The PDR was calculated using thefollowing formula:
PDR5 pixel density regenerate
site=pixel density adjacent
distal cortex
and subsequently correlated with thesubjective assessment of bone healingby one of the senior authors.Postoperatively, the patients were
allowed partial weight bearing basedon the IM rod manufacturer’s recom-mendations. This depends on the sizeof the nail implanted: 8.5, 10.7, and12.5mmnails can bear a maximum of30, 50, and 70 lbs, respectively. Onlywhen sufficient bone healing wassubjectively observed by the treatingphysician was the patient allowed toprogress to full weight bearing.Descriptive analysis of the study
population included mean values andranges to characterize continuous var-iables and frequencies and percentagesfor discrete variables. Paired t-testswere used to compare the averagePDR value at the time of diagnosedhealing versus the average PDR valueat the immediate time point prior.Independent sample Student t-testswere used to evaluate any differencesin patient or clinical factors in PDR atthe time of bone healing. Generallinear modeling techniques were usedto describe the change in the PDRover time from the end of the dis-traction period and to determinewhether any patient or clinical char-acteristics may have affected thatchange over time. All analyses weredone using SPSS version 22.0 (IBM).
Results
The mean distraction was 41.7 mm(range, 20 to 70 mm). Bone regener-ate healing was clinically declared by
Figure 1
Radiographs showing pixel density value measurement at the regenerate site(left) and original bone (right).
Assessment of Bone Healing
e390 Journal of the American Academy of Orthopaedic Surgeons
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
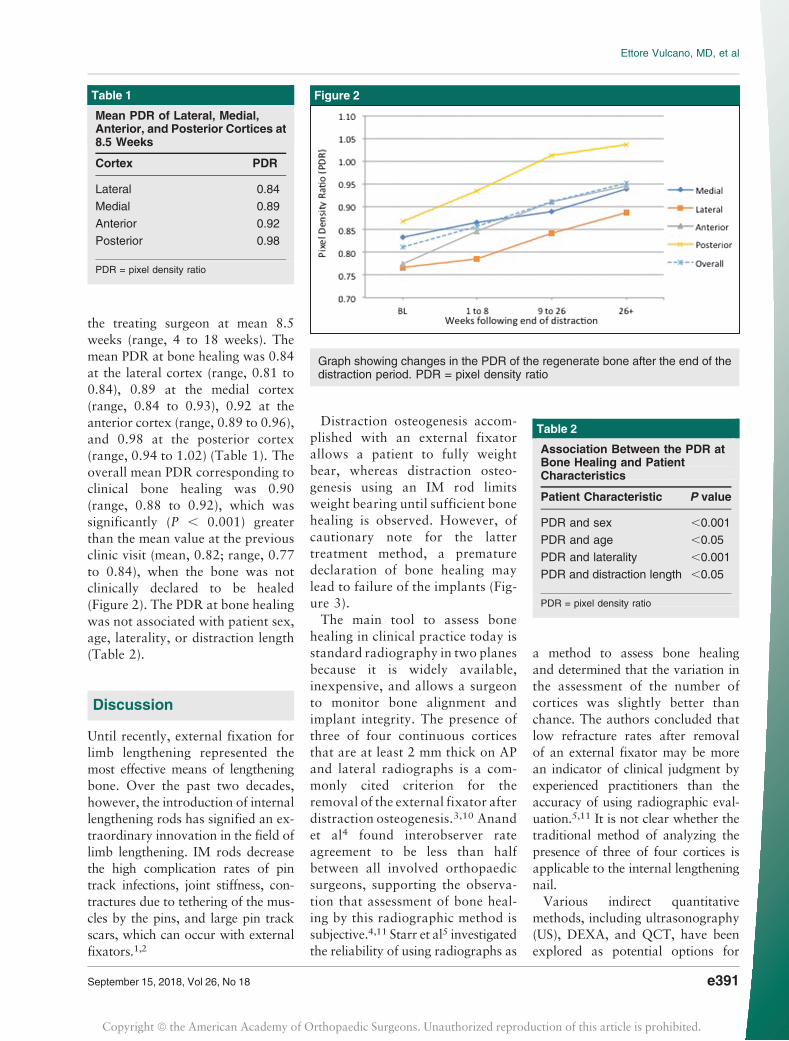
the treating surgeon at mean 8.5weeks (range, 4 to 18 weeks). Themean PDR at bone healing was 0.84at the lateral cortex (range, 0.81 to0.84), 0.89 at the medial cortex(range, 0.84 to 0.93), 0.92 at theanterior cortex (range, 0.89 to 0.96),and 0.98 at the posterior cortex(range, 0.94 to 1.02) (Table 1). Theoverall mean PDR corresponding toclinical bone healing was 0.90(range, 0.88 to 0.92), which wassignificantly (P , 0.001) greaterthan the mean value at the previousclinic visit (mean, 0.82; range, 0.77to 0.84), when the bone was notclinically declared to be healed(Figure 2). The PDR at bone healingwas not associated with patient sex,age, laterality, or distraction length(Table 2).
Discussion
Until recently, external fixation forlimb lengthening represented themost effective means of lengtheningbone. Over the past two decades,however, the introduction of internallengthening rods has signified an ex-traordinary innovation in the field oflimb lengthening. IM rods decreasethe high complication rates of pintrack infections, joint stiffness, con-tractures due to tethering of the mus-cles by the pins, and large pin trackscars, which can occur with externalfixators.1,2
Distraction osteogenesis accom-plished with an external fixatorallows a patient to fully weightbear, whereas distraction osteo-genesis using an IM rod limitsweight bearing until sufficient bonehealing is observed. However, ofcautionary note for the lattertreatment method, a prematuredeclaration of bone healing maylead to failure of the implants (Fig-ure 3).The main tool to assess bone
healing in clinical practice today isstandard radiography in two planesbecause it is widely available,inexpensive, and allows a surgeonto monitor bone alignment andimplant integrity. The presence ofthree of four continuous corticesthat are at least 2 mm thick on APand lateral radiographs is a com-monly cited criterion for theremoval of the external fixator afterdistraction osteogenesis.3,10 Anandet al4 found interobserver rateagreement to be less than halfbetween all involved orthopaedicsurgeons, supporting the observa-tion that assessment of bone heal-ing by this radiographic method issubjective.4,11 Starr et al5 investigatedthe reliability of using radiographs as
a method to assess bone healingand determined that the variation inthe assessment of the number ofcortices was slightly better thanchance. The authors concluded thatlow refracture rates after removalof an external fixator may be morean indicator of clinical judgment byexperienced practitioners than theaccuracy of using radiographic eval-uation.5,11 It is not clear whether thetraditional method of analyzing thepresence of three of four cortices isapplicable to the internal lengtheningnail.Various indirect quantitative
methods, including ultrasonography(US), DEXA, and QCT, have beenexplored as potential options for
Table 1
Mean PDR of Lateral, Medial,Anterior, and Posterior Cortices at8.5 Weeks
Cortex PDR
Lateral 0.84
Medial 0.89
Anterior 0.92
Posterior 0.98
PDR = pixel density ratio
Figure 2
Graph showing changes in the PDR of the regenerate bone after the end of thedistraction period. PDR = pixel density ratio
Table 2
Association Between the PDR atBone Healing and PatientCharacteristics
Patient Characteristic P value
PDR and sex ,0.001
PDR and age ,0.05
PDR and laterality ,0.001
PDR and distraction length ,0.05
PDR = pixel density ratio
Ettore Vulcano, MD, et al
September 15, 2018, Vol 26, No 18 e391
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

assessing bone healing after distrac-tion osteogenesis. Studies haveshown that US cannot differentiatechanges in bone stiffness and strengthafter a certain point during heal-ing.11,12 In addition, because most ofthe energy of US is transmittedthrough soft tissue, variable amountsof soft tissue overlying the bone maylead to fluctuations in measure-ments.11,13 DEXA is expensive anddoes not allow for assessment ofalignment and implant integrity.Although US and DEXA providevaluable information about the dis-tribution and quantity of new boneformed during limb lengthening,Eyres et al12 found that the high-resolution images of radiographywere useful in the detection of smallcortical defects, which were not
identified by the other imagingtechniques. QCT may have theunique advantage of providing high-resolution images of the healing bonewhile providing quantitative analy-sis. Babatunde et al11 report that themajor disadvantages of QCT are itslimited availability, high cost, andrelatively higher radiation exposureto patients.Radiographic pixel values ex-
pressed as PDR indicate ossificationor calcification of bone. Although thepixel value is not absolute, the rela-tive pixel value of the distraction sitecompared with the pixel value of theoriginal bone may provide informa-tion regarding biological steps ofbone gap healing8 (Figure 4). ThePDR at each of the four corticesessentially monitors the maturationof the regenerate by comparing itsdensity—in pixels—to that of theadjacent native bone.The relative pixel value ratios at
the declared time of clinical bonehealing were .0.89 in three of thefour cortices. The average PDR of0.90 may represent the circumfer-ential bone density after distractionosteogenesis. Treating surgeonsmay use this value as a method tomonitor regenerate maturation andas a guide to decide for full weightbearing. The PDR can be used aloneor as an adjunct to the subjectivemethod of deciding whether thebone is healed based on multiplebridging cortices. In addition, wefound that the PDR associated withclinical bone healing was notaffected by patient sex, age, later-ality, or distraction length. A valueof 0.90 may be used as a guide forbone healing for a broad range ofpatients irrespective of age, sex, andamount of lengthening.We recognize that our study has
several limitations. This study relieson visualization and it is potentiallymisleading. The authors did notmeasure or test the mechanical envi-ronment suitable for weight bearing.
Other limitations include the retro-spective nature of the study, the lackof a control group, and the relativelysmall cohort size. The use of theadjacent healthy bone whose PD wascalculated may have potentiallyaffected the results as it may havebeen affected by disuse osteopenia.Perhaps the contralateral femurshould have been measured, but thiswould have led to higher costs andexposure to radiation. However, it isnot clear whether creating a ratiowith contralateral bone would besuperior. The radiographic techniquemay differ from side to side, andcontralateral radiographs were notroutinely done. This may be an ideafor a future study. Another limitationis that the surgeons may have beentoo conservative with respect to al-lowing full weight bearing. Conse-quently, even lower PDR maycorrespond to safe full weight bear-ing. Another limitation is the fact thatdespite E.V.’s recommendation topartially or to fully bear weight,there were no means to identify howmuch weight each patient effectivelyput on the surgical extremity. Aweight-bearing monitoring devicewould be ideal to account for this.There is no doubt that stronger
nails may become available that mayallow earlier weight bearing withdifferent risks of implant failure. Forthe time being, the only titaniumtelescopic nail available in the UnitedStates is the one discussed in thisarticle. The findings in the presentstudy should assist, not replace, clin-ical judgment.When a stronger nail isdeveloped, the mechanics and timingof bone healing and full weightbearing will likely change. It will bean opportunity to study the PDR inthe new setting and see if and how itchanges.The findings of this pilot observa-
tional study introduce the PDR as apossibleobjectiveaid thatmaybeusedto monitor bone healing. The PDR isa rapid, objective, inexpensive, and
Figure 3
Radiograph showing failure of theimplant after premature declarationof bone healing.
Assessment of Bone Healing
e392 Journal of the American Academy of Orthopaedic Surgeons
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

simple method for the detection ofbone density changes in distractionosteogenesis of the femur usinga specific antegrade IM rod. Thismethod may assist less experiencedsurgeons and serve as a valuableaid to senior orthopaedic surgeonsin unclear cases. Furthermore, thePDR may be used as an objectivemeasurement in clinical research,increasing measurement uniformity.Future studies should focus on as-sessing the intra- and inter-reliabilityof the method, in addition to morerigorous methodology to establish athreshold value for bone healing.Multicenter studies will help achieve
more scientifically sound conclusionsas to the objective assessment of bonehealing and its correlation withweight-bearing status in the setting ofinternal bone lengthening. Further-more, the introduction to the marketof newer and stronger nails will pre-sent anopportunity to test the validityof the PDR method with differentimplants. The PDR may be implant-specific or perhaps universal. Thisremains to be seen. The methodologymay be used as a standardized mea-surement of bone regenerate healing,which may help limb-lengtheningsurgeons to report results and com-municate more effectively.
References
References printed in bold type arethose publishedwithin the past 5 years.
1. Kirane Y, Fragomen AT, Rozbruch SR:Precision of the precice internal lengtheningnail. Clin Orthop Relat Res 2014;472:3869-3878.
2. Rozbruch SR, Birch JG, Dahl MT,Herzenberg JE: Motorizedintramedullary nail for treatment oflimb length discrepancy and deformity.J Am Acad Orthop Surg 2014;22:403-409.
3. Skaggs DL, Leet AI, Money MD, Shaw BA,Hale JM, Tolo VT: Secondary fracturesassociated with external fixation inpediatric femur fractures. J Pediatr Orthop1999;19:582-586.
Figure 4
Radiographs showing progression of bone healing of the medial cortex from week 3 to 12 months from the end of distraction.PDR = pixel density ratio
Ettore Vulcano, MD, et al
September 15, 2018, Vol 26, No 18 e393
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

4. Anand A, Feldman DS, Patel RJ, et al:Interobserver and intraobserver reliabilityof radiographic evidence of bone healing atosteotomy sites. J Pediatr Orthop 2006;15:271-272.
5. Starr KA, Fillman R, Raney EM: Reliabilityof radiographic assessment of distractionosteogenesis site. J Pediatr Orthop 2004;24:26-29.
6. Hazra S, Song HR, Biswal S, et al:Quantitative assessment of mineralizationin distraction osteogenesis. Skeletal Radiol2008;37:843-847.
7. Song SH, Sinha S, Kim TY, Park YE, Kim SJ,Song HR: Analysis of corticalization using the
pixel value ratio for fixator removal in tibiallengthening. J Orthop Sci 2011;16:177-183.
8. Shim JS, Chung KH, Ahn JM: Value ofmeasuring bone density serial changes on apicture archiving and communicationsystems (PACS) monitor in distractionosteogenesis. Orthopedics 2002;25:1269-1272.
9. Swaton N: Learn from experience: Insightsof 2001 PACS customers. Radiol Manage2002;24:22-27.
10. Fischgrund J, Paley D, Suter C: Variablesaffecting time to bone healing during limblengthening. Clin Orthop Relat Res 1994;301:31-37.
11. Babatunde OM, Fragomen AT, RozbruchSR: Noninvasive quantitative assessment ofbone healing after distraction osteogenesis.HSS J 2010;6:71-78.
12. Eyres KS, Bell MJ, Kanis JA: Methods ofassessing new bone formation during limblengthening: Ultrasonography, dual energyx-ray absorptiometry and radiographycompared. J Bone Joint Surg Br 1993;75:358-364.
13. Markel MD, Chao EY: Noninvasivemonitoring techniques for quantitativedescription of callus mineral content andmechanical properties. Clin Orthop RelatRes 1993;293:37-45.
Assessment of Bone Healing
e394 Journal of the American Academy of Orthopaedic Surgeons
Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.