res update final
TRANSCRIPT
Therapeutic monoclonal antibodies -Why they are becoming so common-Some perspectives for internal medicine
BRIAN SKAUG
RESIDENT UPDATE TALK
MARCH 2N D-3R D 2015
Most internal medicine specialties have monoclonal antibodies at their disposal
Hematology/Oncology: rituximab (Rituxan), bevacizumab (Avastin), many more
Rheumatology: infliximab (Remicade), adalimumab (Humira), many more
Gastroenterology: Remicade, Humira
Endocrinology: denosumab (Prolia)
Cardiology: abciximab (ReoPro), PCSK9 inhibitors soon
Allergy/Pulmonary: Omalizumab (Xolair)
Nephrology: basilixumab for certain transplant recipients
Also Dermatology (Humira, others), Ophthalmology (Avastin), Neurology (natalizumab/Tysabri)
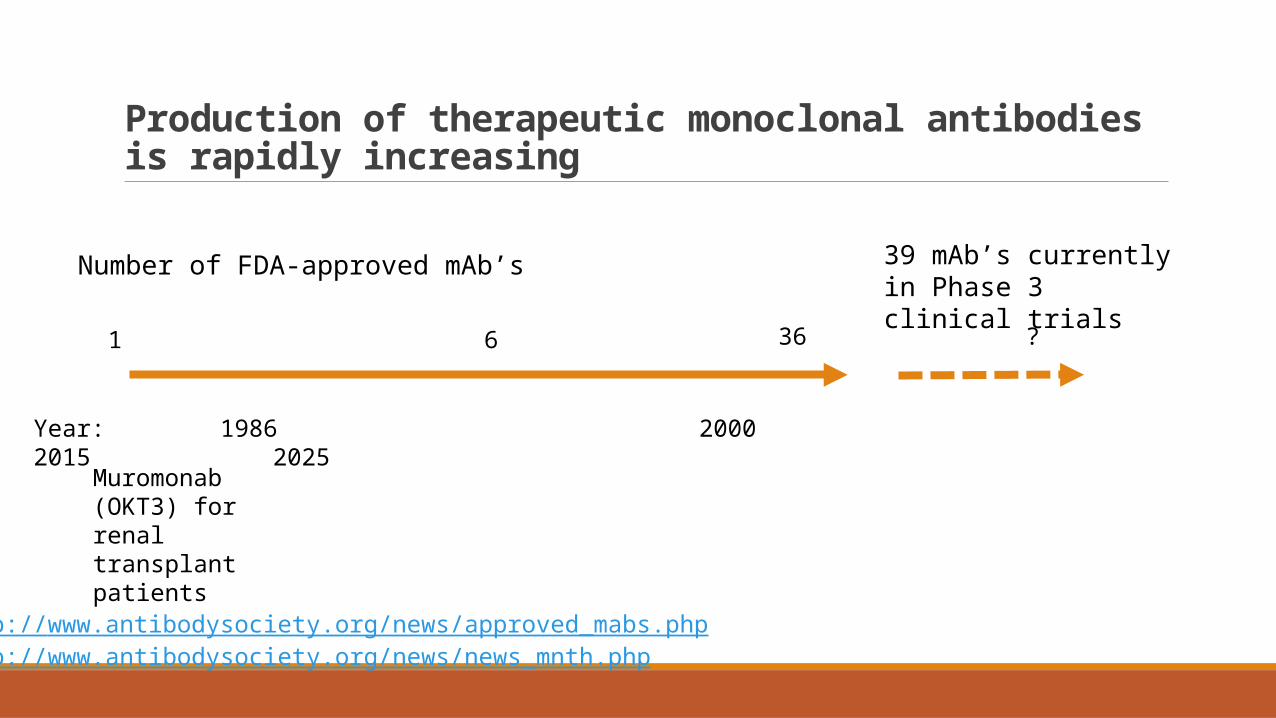
Production of therapeutic monoclonal antibodies is rapidly increasing
Year: 1986 20002015 2025
Number of FDA-approved mAb’s
1 6 ? 36
39 mAb’s currently in Phase 3 clinical trials
Muromonab (OKT3) for renal transplant patients
http://www.antibodysociety.org/news/approved_mabs.phphttp://www.antibodysociety.org/news/news_mnth.php
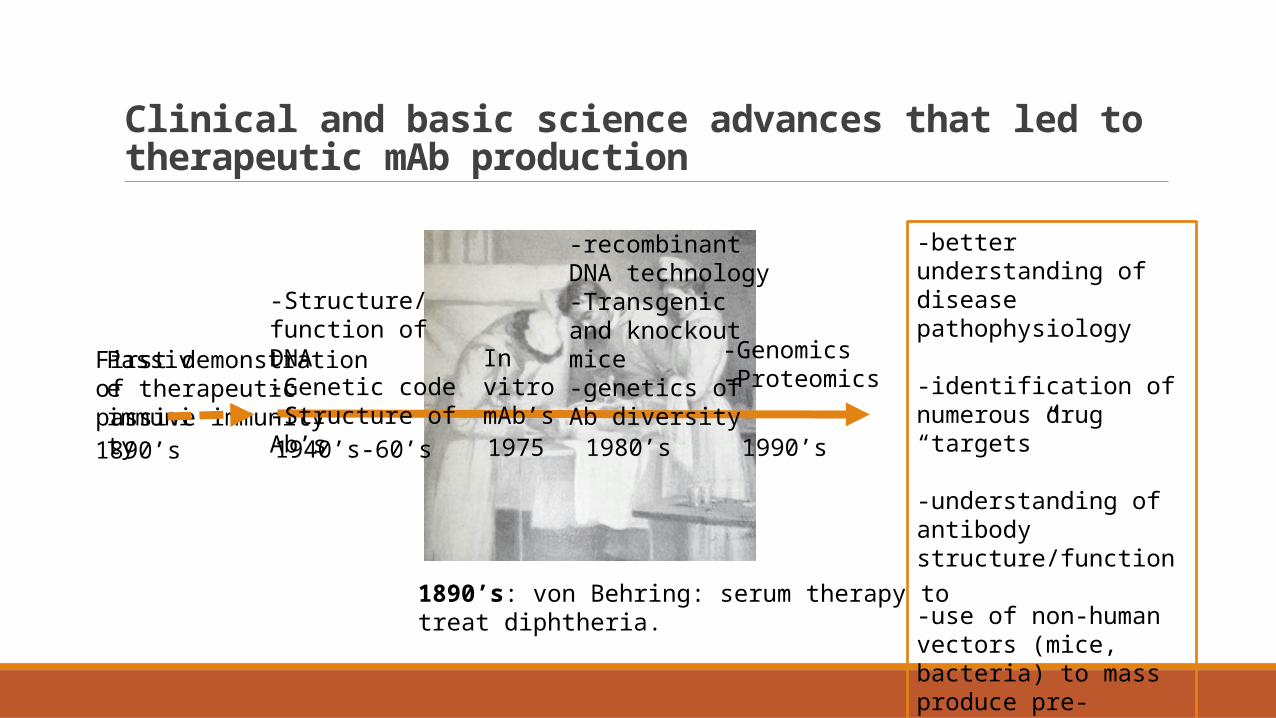
Clinical and basic science advances that led to therapeutic mAb production
1890’s: von Behring: serum therapy to treat diphtheria.
First demonstration of therapeutic passive immunity
Passive immunity
1890’s
In vitro mAb’s
1975
-Structure/function of DNA-Genetic code-Structure of Ab’s
1940’s-60’s
-recombinant DNA technology-Transgenic and knockout mice -genetics of Ab diversity
1980’s 1990’s
-Genomics-Proteomics
-better understanding of disease pathophysiology
-identification of numerous drug “targets”
-understanding of antibody structure/function
-use of non-human vectors (mice, bacteria) to mass produce pre-specified proteins or antibodies
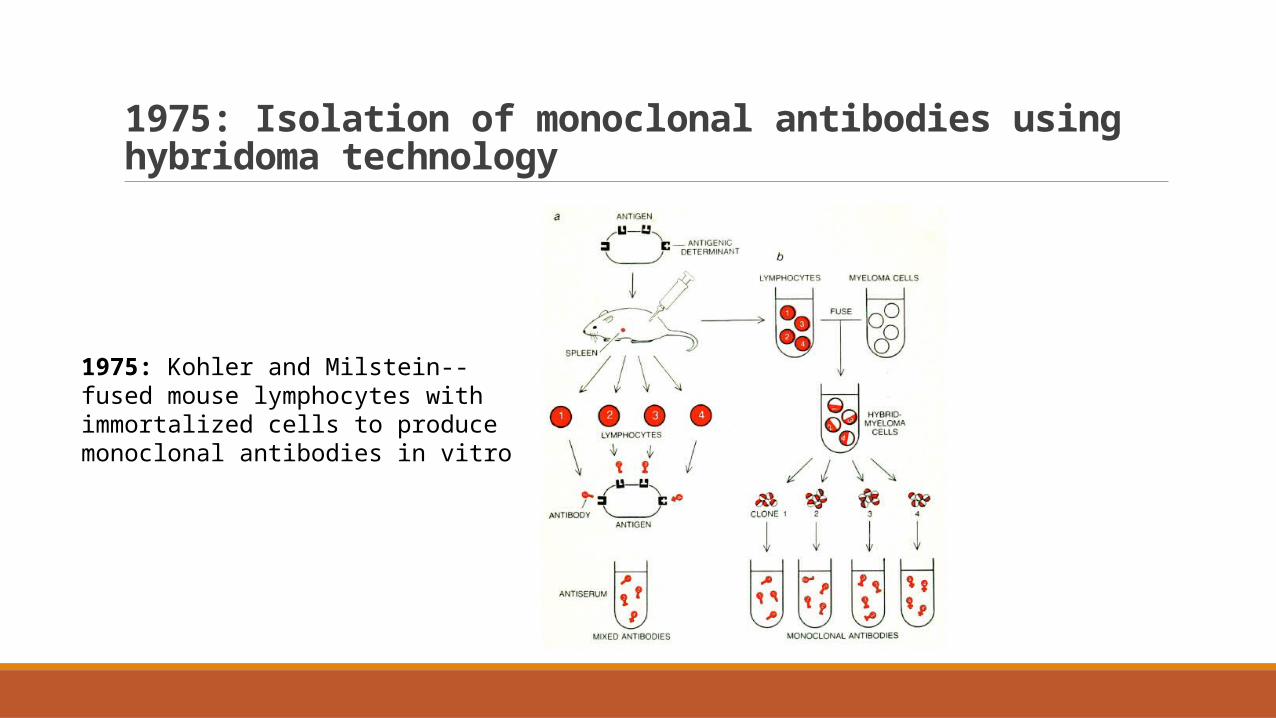
1975: Isolation of monoclonal antibodies using hybridoma technology
1975: Kohler and Milstein--fused mouse lymphocytes with immortalized cells to produce monoclonal antibodies in vitro
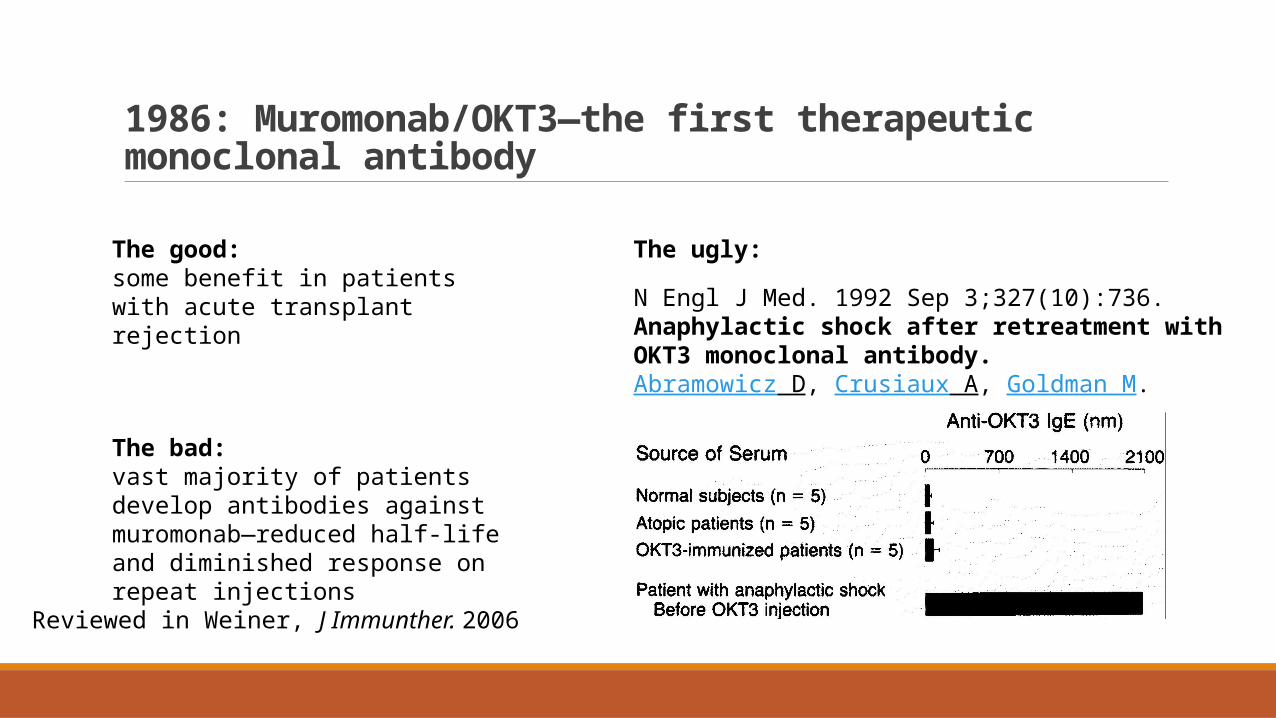
1986: Muromonab/OKT3—the first therapeutic monoclonal antibody
The good: some benefit in patients with acute transplant rejection
The bad: vast majority of patients develop antibodies against muromonab—reduced half-life and diminished response on repeat injections
N Engl J Med. 1992 Sep 3;327(10):736.Anaphylactic shock after retreatment with OKT3 monoclonal antibody.Abramowicz D, Crusiaux A, Goldman M.
The ugly:
Reviewed in Weiner, J Immunther. 2006
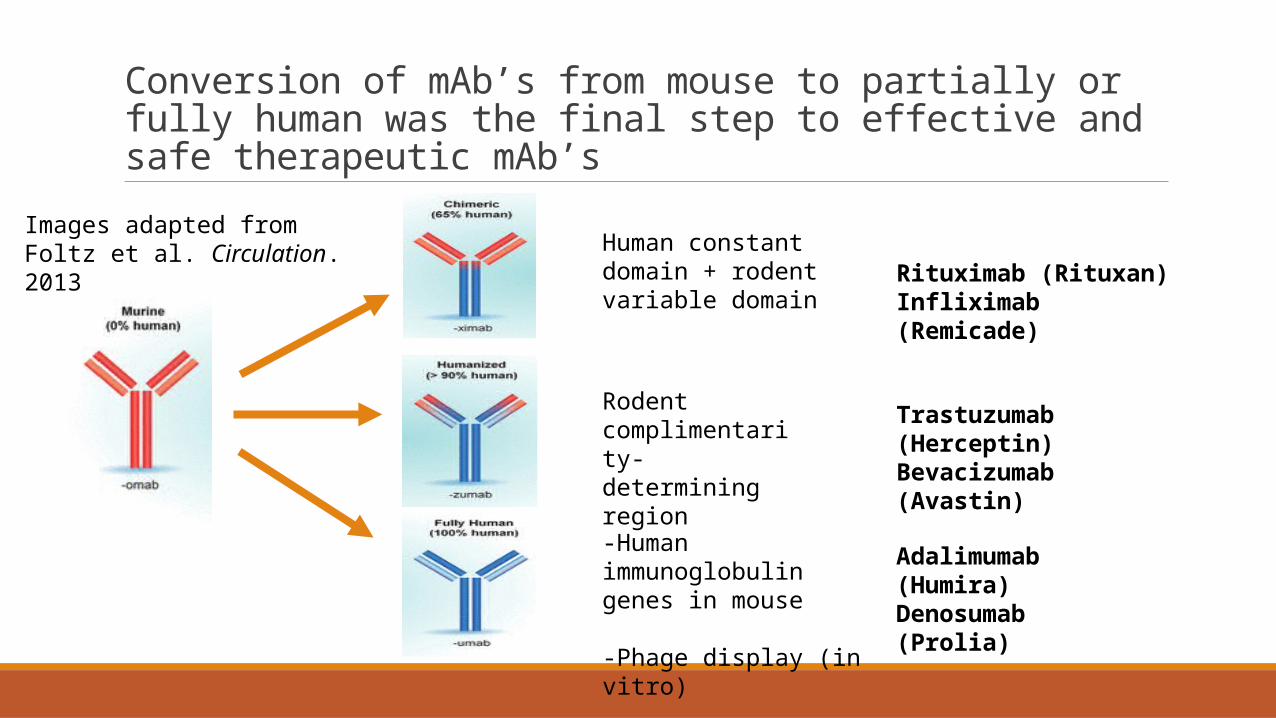
Conversion of mAb’s from mouse to partially or fully human was the final step to effective and safe therapeutic mAb’s
Rituximab (Rituxan) Infliximab (Remicade)
Human constant domain + rodent variable domain
Trastuzumab (Herceptin)Bevacizumab (Avastin)
Rodent complimentarity-determining region
-Human immunoglobulin genes in mouse
-Phage display (in vitro)
Adalimumab (Humira)Denosumab (Prolia)
Images adapted from Foltz et al. Circulation. 2013
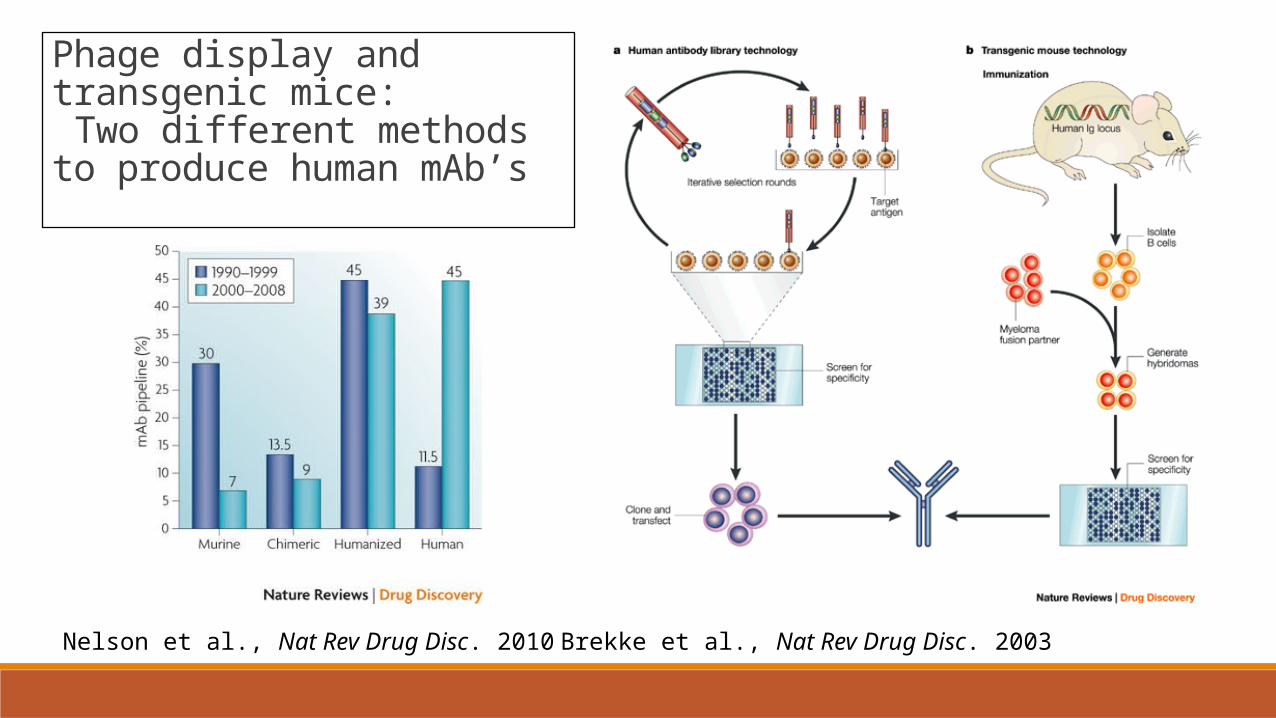
Phage display and transgenic mice: Two different methods to produce human mAb’s
Nelson et al., Nat Rev Drug Disc. 2010 Brekke et al., Nat Rev Drug Disc. 2003
2003: PCSK9 mutations identified as a cause of autosomal dominant hypercholesterolemia.Abifadel et al., Nat Gen. 2003
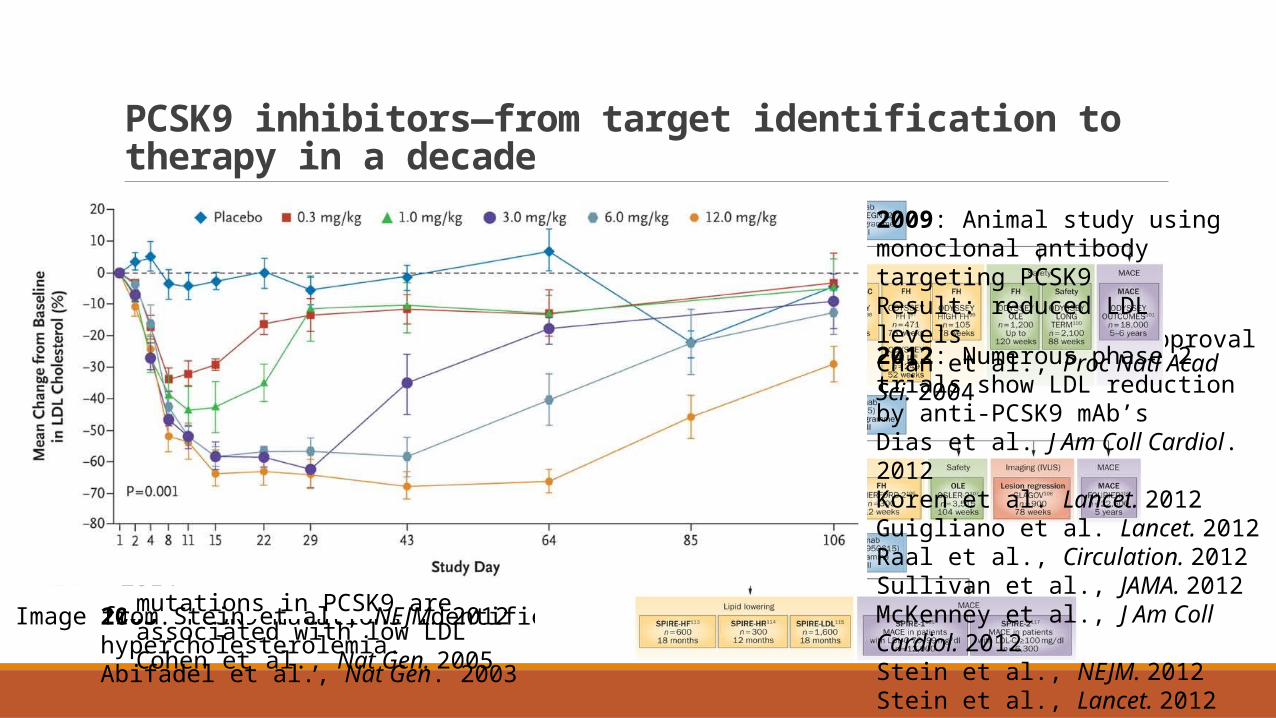
PCSK9 inhibitors—from target identification to therapy in a decade
2003-2006: identification and characterization of target
2009: mAb produced and studied in animals
2011-2014: Human trials
applications for FDA approval2004: Mouse studies show PCSK9 downregulates LDL receptor, raising serum LDL
Maxwell et al., Proc. Natl. Acad. Sci., 2004Park et al., J. Biol. Chem. 2004Benjannet et al., J. Biol. Chem. 2004
Image adapted from Mullard., Nat Rev Drug Disc. 2012 2005: loss of function mutations in PCSK9 are associated with low LDLCohen et al., Nat Gen. 2005
And…2006: reduced risk of coronary heart diseaseCohen et al., NEJM. 2006
2014: 3 different mAbs against PCSK9 being tested in phase 3 clinical trialsDadu et al., Nat Rev Cardiol. 2014
2009: Animal study using monoclonal antibody targeting PCSK9Result: reduced LDL levelsChan et al., Proc Natl Acad Sci. 2004
2012: Numerous phase 2 trials show LDL reduction by anti-PCSK9 mAb’sDias et al. J Am Coll Cardiol. 2012Koren et al. Lancet. 2012Guigliano et al. Lancet. 2012Raal et al., Circulation. 2012Sullivan et al., JAMA. 2012McKenney et al., J Am Coll Cardiol. 2012Stein et al., NEJM. 2012Stein et al., Lancet. 2012Roth et al., NEJM. 2012
Image from Stein et al., NEJM. 2012
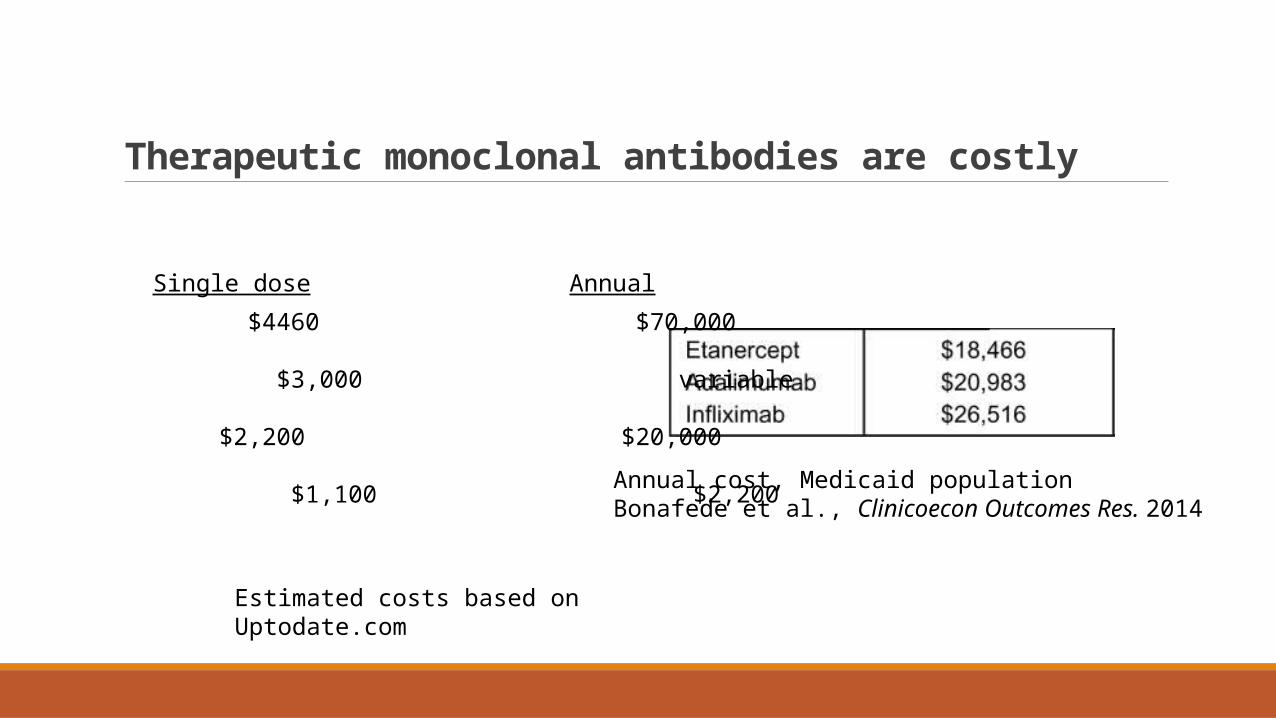
Therapeutic monoclonal antibodies are costly
Annual cost, Medicaid populationBonafede et al., Clinicoecon Outcomes Res. 2014
Estimated costs based onUptodate.com
Herceptin $4460 $70,000
Avastin $3,000 variable
Remicade $2,200 $20,000
Prolia $1,100 $2,200
Single dose Annual
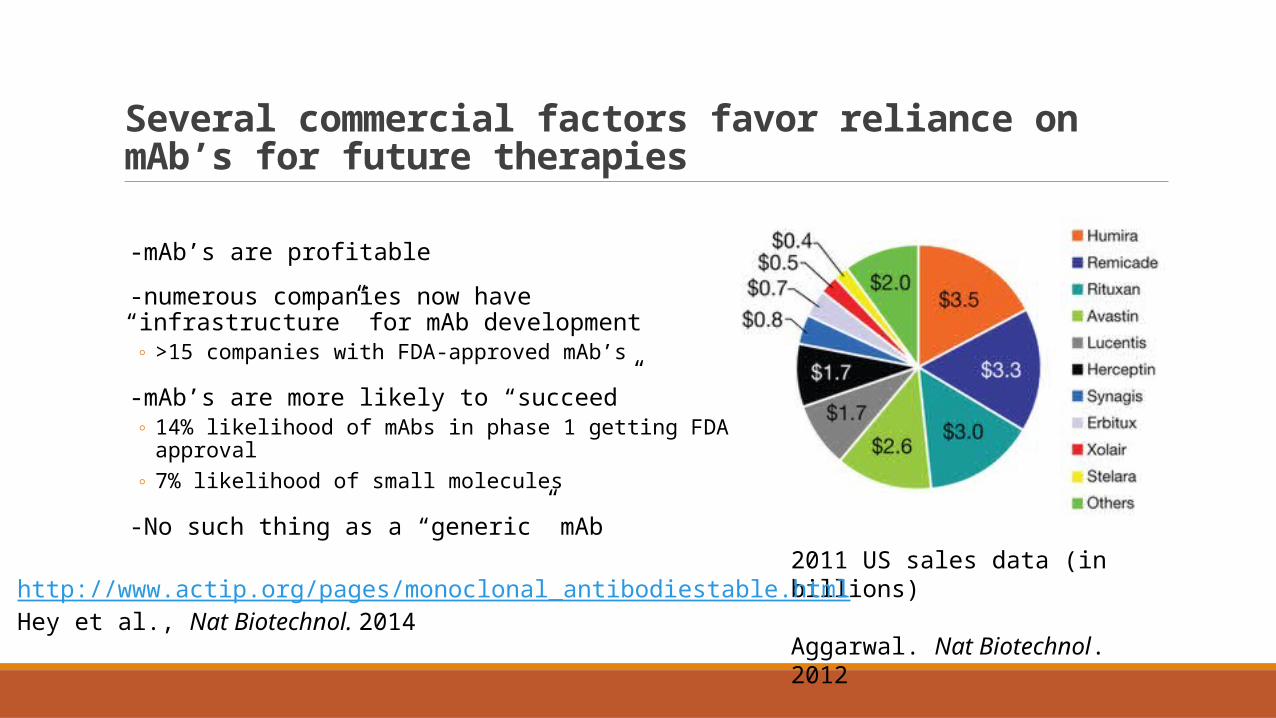
Several commercial factors favor reliance on mAb’s for future therapies
-mAb’s are profitable
-numerous companies now have “infrastructure” for mAb development
◦ >15 companies with FDA-approved mAb’s
-mAb’s are more likely to “succeed”◦ 14% likelihood of mAbs in phase 1 getting FDA approval◦ 7% likelihood of small molecules
-No such thing as a “generic” mAb
2011 US sales data (in billions)
Aggarwal. Nat Biotechnol. 2012http://www.actip.org/pages/monoclonal_antibodiestable.htmlHey et al., Nat Biotechnol. 2014
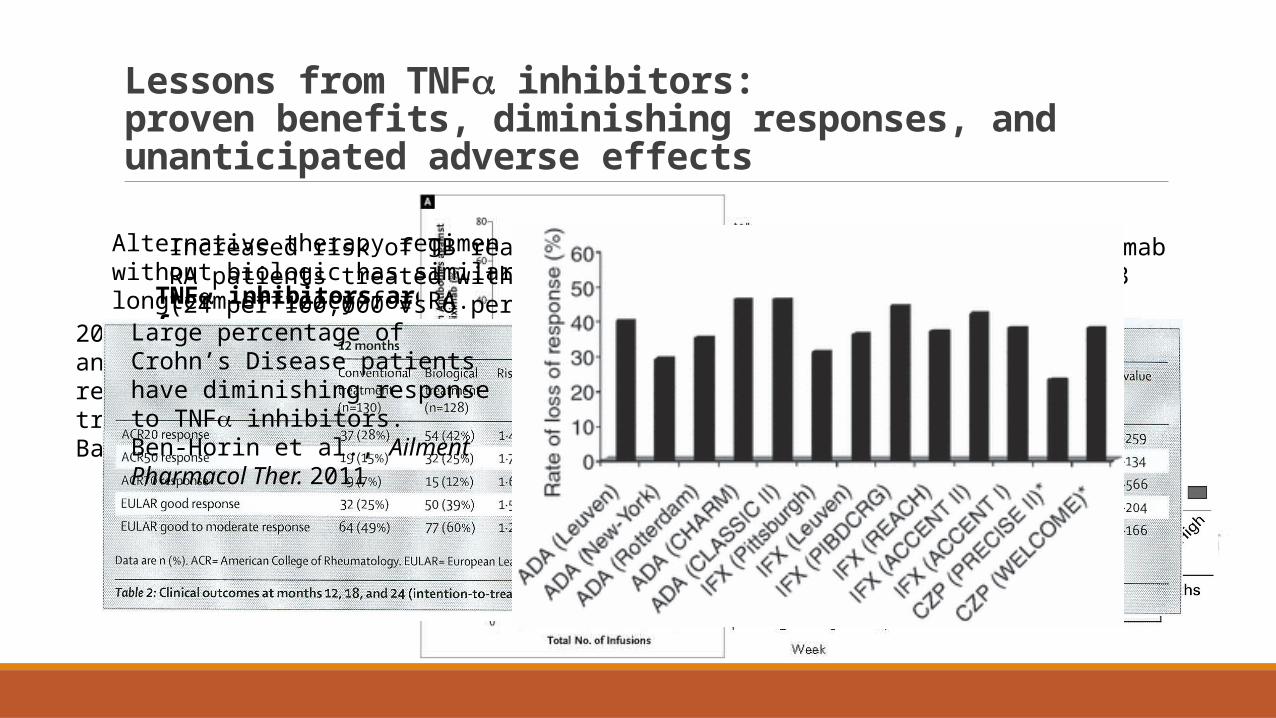
Lessons from TNFa inhibitors: proven benefits, diminishing responses, and unanticipated adverse effects
1997: Infliximab effective in refractory Crohn’s DiseaseTargan et al., NEJM. 1997
TNFa inhibitors are currently FDA approved for:-Crohn's disease, ulcerative colitis-Rheumatoid arthritis-Ankylosing spondylitis -Psoriatic arthritis-Plaque psoriasis
http://www.drugs.com
2003: Anti-infliximab antibodies, infusion reactions, and loss of treatment responseBaert et al., NEJM. 2003
2009: Adalimumab (human) has lower but still large percentage of anti-mAb Ab formation and treatment failure compared to infliximab in RA patientsRadstake et al., Ann Rheum Dis. 2009
Increased risk of TB reactivation in RA patients treated with infliximab (24 per 100,000 vs 6 per 100,000)Keane et al., NEJM. 2001
Worsening of CHF by infliximabChung et al., Circulation. 2003
Alternative therapy regimen without biologic has similar longterm efficacy for RA.van Vollenhoven et al. Lancet. 2012
Roughly 17,000 euro difference in cost at 21 month follow up.Eriksson et al., Ann Rheum Dis. 2014
Large percentage of Crohn’s Disease patients have diminishing response to TNFa inhibitors.Ben-Horin et al., Ailment Pharmacol Ther. 2011
Some perspectives for Internal Medicine
-Lots of mAb’s already available, many more on the way
-Potential for meeting some unmet medical needs
-Universally expensive
-Diminishing therapeutic response is a problem even with human mAbs
-Require same stringency for safety, efficacy, and cost-effectiveness as “traditional” drugs
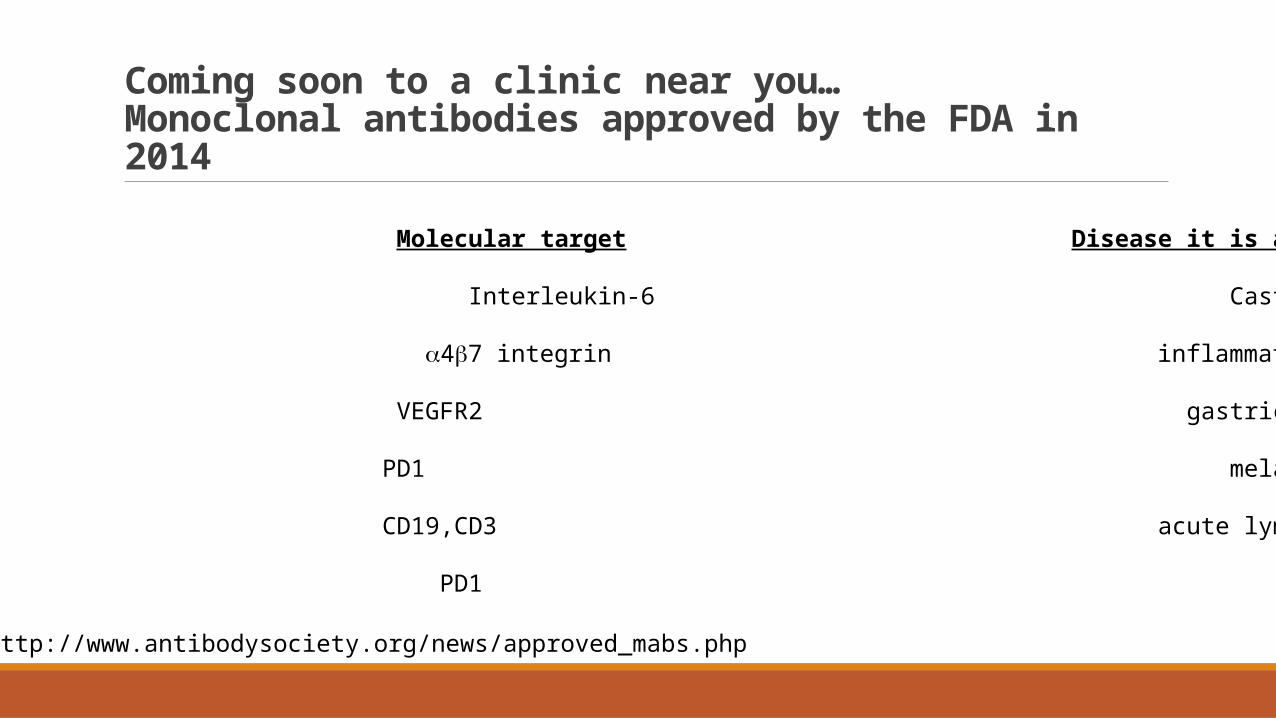
Coming soon to a clinic near you…Monoclonal antibodies approved by the FDA in 2014
Name of mAb Molecular target Disease it is approved for
Siltuximab Interleukin-6 Castleman Disease
Vedolizumab a4b7 integrin inflammatory bowel disease
Ramucirumab VEGFR2 gastric cancer
Pembrolizumab PD1 melanoma
Blinatumomab CD19,CD3 acute lymphoblastic leukemia
Nivolumab PD1 melanoma
http://www.antibodysociety.org/news/approved_mabs.php